Page 1
MACs, MICs, RACs and ZPICs: Latest Developments Preparing for Medicare and Medicaid Audits and Appealing Unfavorable Results
Today’s faculty features:
1pm Eastern | 12pm Central | 11am Mountain | 10am Pacific
The audio portion of the conference may be accessed via the telephone or by using your computer's
speakers. Please refer to the instructions emailed to registrants for additional information. If you
have any questions, please contact Customer Service at 1-800-926-7926 ext. 10.
WEDNESDAY, OCTOBER 3, 2012
Presenting a live 90-minute webinar with interactive Q&A
Paula G. Sanders, Principal,Post & Schell, Harrisburg, Pa.
Anna M. Grizzle, Member, Bass Berry & Sims, Nashville, Tenn.
Page 2
Sound Quality
If you are listening via your computer speakers, please note that the quality of
your sound will vary depending on the speed and quality of your internet
connection.
If the sound quality is not satisfactory and you are listening via your computer
speakers, you may listen via the phone: dial 1-866-720-2805 and enter your PIN
when prompted. Otherwise, please send us a chat or e-mail
[email protected] immediately so we can address the problem.
If you dialed in and have any difficulties during the call, press *0 for assistance.
Viewing Quality
To maximize your screen, press the F11 key on your keyboard. To exit full screen,
press the F11 key again.
Page 3
For CLE purposes, please let us know how many people are listening at your
location by completing each of the following steps:
• In the chat box, type (1) your company name and (2) the number of
attendees at your location
• Click the word balloon button to send
FOR LIVE EVENT ONLY
Page 4
4
MACs, MICs, RACs and ZPICs:
Latest Developments
October 3, 2012
Paula G. Sanders Anna M. Grizzle
Post & Schell, PC Bass, Berry & Sims PLC
[email protected] [email protected]
Page 5
5
http://www.hms.com/our_services/services_program_integrity.asp
Page 6
6
60 Day Repayment Rule
Page 7
7
Mandatory Refunding of
Overpayments (3/2010) • Providers, suppliers, Medicaid MCOs, Medicare
Advantage plans, and PDP sponsors must report and return overpayments to HHS, the State, or a Medicare intermediary or carrier by the later of:
− 60 days of identification of overpayment, or
− Due date of cost report
• Treble damages and CMPs up to $50K for knowing failure to return overpayments on time
• Knowing failure also a false claim under the Federal False Claims Act
Page 8
8
CMS Proposed Rule On 60 Day
Repayment Obligation
Page 9
9
CMS Proposed Rules:
Knowledge Of The Overpayment • Overpayment is “identified” if the provider has
“actual knowledge of the existence of the overpayment or acts in reckless disregard or deliberate ignorance of the overpayment”
• Rule creates an incentive to exercise reasonable diligence to determine whether an overpayment exists
• Provider may receive information about a potential overpayment; the provider must make “reasonable inquiry”
Page 11
11
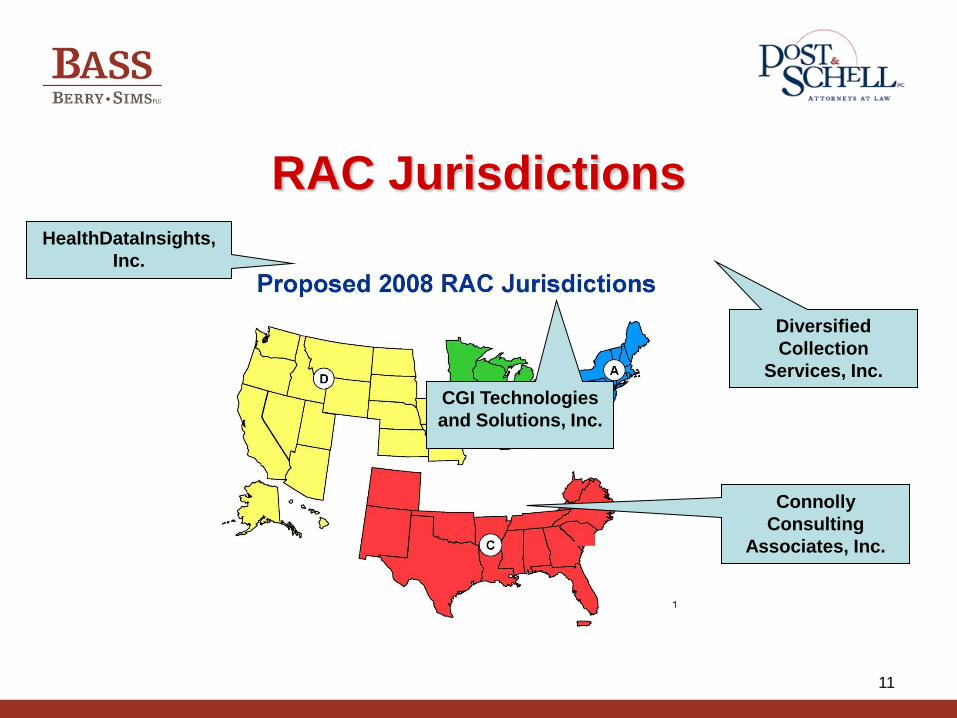
RAC Jurisdictions
Diversified
Collection
Services, Inc.
CGI Technologies
and Solutions, Inc.
Connolly
Consulting
Associates, Inc.
HealthDataInsights,
Inc.
Page 12
12
RAC Overview
• Objective to recover overpayments, not
fraud hunters
• Extensive use of data mining
• All issues must be pre-approved by
CMS and posted on RAC website
• http://www1.cms.gov/RAC/01
Overview.asp#TopOfPage
Page 13
13
Prepare for Additional
Development Requests (ADRs) • As of 3/15/2102, annual limit for records requested
every 45 days is 2 percent of all claims submitted in
the prior year, divided by eight, capped at 400 per 45
days
• For SNFs, 1 ADR represents a beneficiary’s entire
episode of care
− All medical records for all services rendered from
admission to discharge http://www.cms.gov/Recovery-Audit-
Program/Downloads/Providers_ADRLimit_Update-03-12.pdf
Page 14
14
Prepare for ADRs
• 3 year look back: do you know where
your records are?
– Storage, soft files, filing back log
• Request extension if needed
• Copy entire medical record and all
relevant documents, and keep a copy
Page 15
15
Prepare for ADRs
• Follow document production
requirements http://dcsrac.com/Documentation.aspx
• Proof of mailing/proof of receipt
• Monitor deadlines
• Consider appeal options
Page 16
16
Claims Review
• Review claims on post-payment basis
• Uses same Medicare policies as FIs, Carriers, and
MACs including LCDs, NCDs and Medicare Manuals
• Areas of focus chosen based on data mining
techniques, OIG / GAO reports, CERT reports, and
experience and knowledge of staff
• Approved audit issues posted on RAC contractor
website
Source: Statement of Work for the Recovery Audit Program; available at:
http://www.cms.gov/RAC/downloads/Final%20RAC%20SOW.pdf
Page 17
17
Automated Review
• Uses data analysis to determine improper
payments
• Does not involve a review of medical records
• Contacts providers directly to collect any
overpayments or repay any underpayments
• Consumes less resources than a complex
review and conducted more frequently
Page 18
18
Complex Review
• Uses medical records to further analyze the claim when data analysis is insufficient
• Identifies discrepancies between the medical records and the claim
• Provider has 45 days to submit medical records
• Review must be completed within 60 days of receipt of medical records
• Sends the hospital a determination letter with its findings
Page 19
19
Expansion of RAC Program
• Expands RAC program to Medicare
Parts C and D and Medicaid
• States required to contract with a RAC
for review of Medicaid claims by
December 31, 2010
– RACs paid on contingency basis
– States required to have appeals process
Source: Section 6411 of the Patient Protection and Affordable Care Act (Pub. L. 111-148)
Page 20
20
Medicaid RACs
• Contracts with state Medicaid agency
• Typically paid on contingency
• Must have a licensed medical director
and certified coders
• States determine record limits, medical
necessity reviews and extrapolation
• National 3 year look-back
Page 21
21
Be Alert for RAC-Like Auditors
• Medicare Advantage and commercial
insurance doing RAC-like audits
• ~ 20% Medicare beneficiaries enrolled
in Medicare Part C
• Medicare Advantage plans have
different appeals processes
Page 22
22
Prepayment Demonstration Project
• Time Period: Aug. 27, 2012-Aug. 26, 2015
• States Subject to Review − Fraud and error-prone states (FL, CA, MI, TX, NY, LA, IL)
− States with high volumes of inpatient stays (PA, OH, NC,
MI)
• Focus on claims with high improper payment
rates
Page 23
23
Prepayment Demonstration Project
• ADR issued by MAC
• Records response due within 30 days
• Results sent to providers within 45 days
• Providers have appeal rights
Page 24
24
Current Areas of Focus
• http://www.connolly.com/healthcare/pages/ApprovedIssues.aspx
• https://www.dcsrac.com/IssuesUnderReview.aspx
• https://racinfo.healthdatainsights.com/home.aspx?ReturnUrl=%2fPublic%2fNewIssues.aspx
• http://racb.cgi.com/Issues.aspx?st=1
Page 25
25
RAC Trends (AHA, 8/22/2012)
• Medical records requests increased
22% from first to second quarter 2012
• 14% increase in automated denials
• 29% increase in complex denials
• $5.3 billion targeted
Page 26
26
Automated Denials
• Outpatient billing errors - 39%
• Outpatient coding errors -17%
• Inpatient coding errors - 9%
• Duplicate payments - 6%
• Incorrect discharge status - 4%
• Other – 25%
Page 27
27
Complex Denials – 97% of Denied $
• Medically unnecessary short stays –
78%
• Incorrect MS-DRG or other code error -
12%
• Outpatient coding or billing error – 4%
• Medically unnecessary inpatient stays
lasting >3 days – 1%
Page 28
28
Average $ Value of Denials
• Automated denial = $548
• Complex denial = $5,564
Page 29
29
Underpayments
• ~75% hospitals received at least 1
underpayment determination
• Underpayments totaled ~$75 million
• 63% - incorrect MS-DRG
• 18% - discharge disposition
Page 30
30
It Pays to Appeal
• >1/3 hospitals had a denial reversed
during discussion period
• $507.1 million appealed claims
• Hospitals average 118 appealed denials
• >40% of denials appealed
• 75% of completed appeals overturned
in favor of hospital
Page 31
31
It Pays to Appeal
• Nearly ¾ of all appealed claims still in process
• $76.6 million in overturned denials
• 56% of denials overturned on medical necessity
• 43% of denials overturned for additional information substantiating claim
http://www.aha.org/aha/issues/RAC/ractrac.html
Page 33
33
Zone Program Integrity
Contractors (ZPICs) • Consolidation of PSCs and MEDICs
• Coordination of claims processing and benefit integrity activities
• Ensure integrity of ALL Medicare-related claims – Parts A, B, C, D, Home Health, DME, Hospice and
coordination of Medi-Medi data matches
• Use “innovative data analysis methodologies” for early fraud detection and prevention
Source: Chapter 4 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c04.pdf
Page 34
34
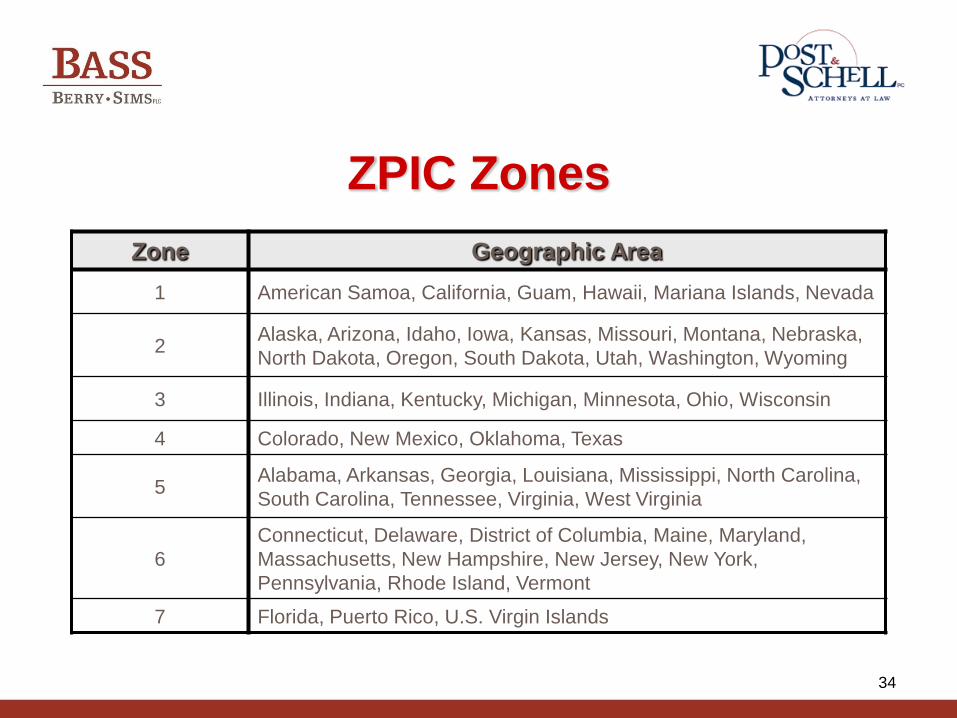
ZPIC Zones
Zone Geographic Area
1 American Samoa, California, Guam, Hawaii, Mariana Islands, Nevada
2 Alaska, Arizona, Idaho, Iowa, Kansas, Missouri, Montana, Nebraska,
North Dakota, Oregon, South Dakota, Utah, Washington, Wyoming
3 Illinois, Indiana, Kentucky, Michigan, Minnesota, Ohio, Wisconsin
4 Colorado, New Mexico, Oklahoma, Texas
5 Alabama, Arkansas, Georgia, Louisiana, Mississippi, North Carolina,
South Carolina, Tennessee, Virginia, West Virginia
6
Connecticut, Delaware, District of Columbia, Maine, Maryland,
Massachusetts, New Hampshire, New Jersey, New York,
Pennsylvania, Rhode Island, Vermont
7 Florida, Puerto Rico, U.S. Virgin Islands
Page 35
35
ZPICs
• Zone 1 – SafeGuard Services, LLC
• Zone 2 – NCI, Inc. (previously AdvanceMed)
• Zone 3 – Cahaba Safeguard Administrators, LLC
• Zone 4 – Health Integrity, LLC
• Zone 5 – NCI, Inc. (previously AdvanceMed)
• Zone 6 – Cahaba Safeguard Administrators, LLC
• Zone 7 – SafeGuard Services, LLC
Page 36
36
ZPIC Responsibilities
• Fraud case development
• Fraud complaint processing
• Provider education related to fraud
investigations
• Ability to initiate payment suspensions
and provider exclusions
Source: Chapter 4 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c04.pdf
Page 37
37
ZPIC Audits
• Unannounced or limited notice
• Review of claims
– Prepayment or post payment
» Potential for payment suspension
– Probe sample or statistical sampling and
extrapolation
• Employee or beneficiary interviews
Source: Chapter 4 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c04.pdf
Page 38
38
ZPIC Triggers
• Aberrant patterns
– Statistical deviations from the norm
– Changes in facility’s historical patterns
– High utilization (e.g., RU/RV therapy)
– High cost services or items
Page 39
39
Audit Results
• Referral to law enforcement – Baptist Healthcare Systems, Inc. and Hardin County,
Kentucky d/b/a Hardin Memorial Hospital 8/2011 Settlement
• Forward findings to MAC for
overpayment recoupment action
• Provider education
Source: Chapter 4 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c04.pdf
Page 40
40
Use of Statistical Sampling for
Overpayment Estimation
• A Medicare contractor may not use
extrapolation to determine overpayment
amounts . . . . unless . . .
– There is a sustained or high level of
payment error; or
– Documented educational intervention has
failed to correct the payment error
42 U.S.C. §1395ddd(f)(3)
Page 41
41
Use of Statistical Sampling for
Overpayment Estimation • Sustained or high level of payment error can be
determined by:
– Error rate determinations by MR unit, PSC, ZPIC
– Probe samples
– Data analysis
– Provider/supplier history
– Information from law enforcement investigations
– Allegations of wrongdoing by current or former employees of provider or supplier
– Audits or evaluations conducted by the OIG
Source: Chapter 8 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c08.pdf
Page 42
42
Use of Statistical Sampling for
Overpayment Estimation
• Additional Factors to Consider
– Number of claims in universe
– Dollar values associated with claims
– Available resources
– Cost effectiveness of expected sampling
results
Source: Chapter 8 – Benefit Integrity; Medicare Program Integrity Manual; available at:
http://www.cms.gov/manuals/downloads/pim83c08.pdf
Page 43
43
Payment Suspensions
• OIG analyzed 253 payment suspensions 2007-2008
• Majority of suspended providers exhibited characteristics that suggest fraud
• 250 received no advance notice, indicating suspected fraud or willful misrepresentation
Page 44
44
Payment Suspensions
• 74% had questionable billing patterns
• 63% supported by information from beneficiaries or other providers that raised questions
• 55% failed to submit medical records
• 24% billed Medicare from vacant physical locations
OIG: The Use of Payment Suspensions to Prevent Inappropriate Medicare
Payments, 0EI-01-09-00180 (11/1/2010)
Page 45
45
Affordable Care Act Expands
Suspension Authority
• Payments suspended pending an
investigation of a credible allegation of
fraud unless good cause not to suspend
payments
• CMS to consult with OIG regarding
credible allegation of fraud
Page 46
46
“Discretionary” Payment
Suspensions
• Based on “credible allegation of fraud”
• Indicia of reliability
– Fraud hotline complaints
– Data mining
– Patterns of problems identified thru audits
– Civil false claims cases
Page 47
47
Payment Suspensions Difficult to
Challenge
• Exhaustion of administrative review
required
• All claims must be presented to HHS
• No real remedy under Medicare statute
• Nichole Medical Equipment & Supply,
Inc. v. Tricenturion, Inc., 2012 U.S. App.
LEXIS 19218 (3d Cir., Sept. 13, 2012)
Page 49
49
Medicare Administrative Contractors
(MAC)
• Medicare Prescription Drug, Improvement
and Modernization Act of 2003 (MMA), Pub.
Law 108-173, Subtitle B, Section 911 (42
USC 1395kk-1)
• Consolidated Fiscal Intermediaries (FI) and
Carriers
• Regional Hospice and Home Health
Intermediary (RHHI)
Page 50
50
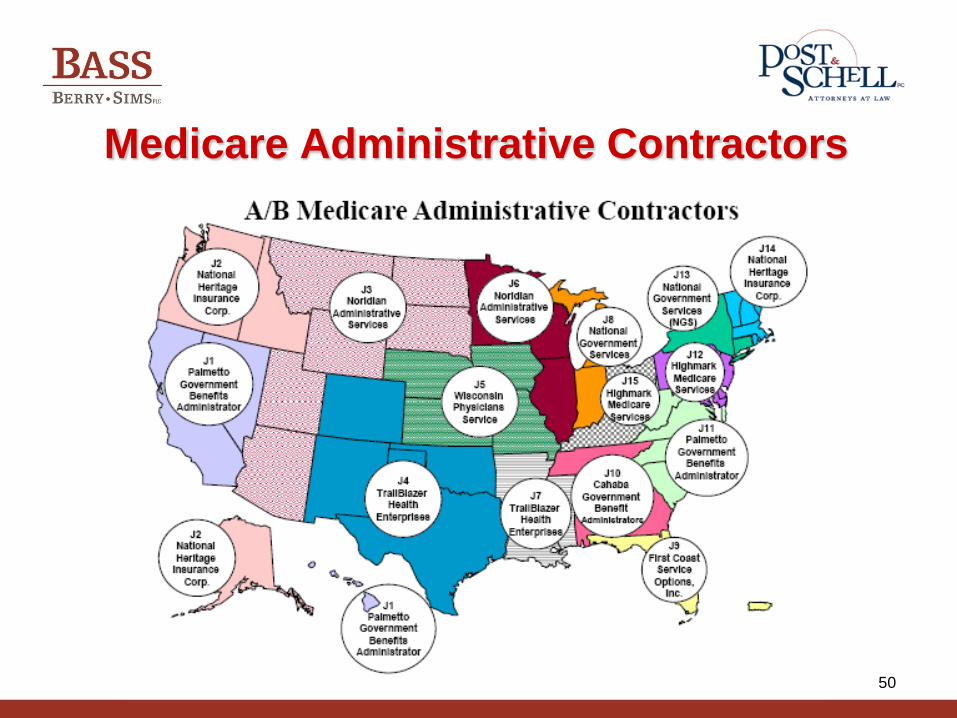
Medicare Administrative Contractors
Page 51
51
Coming Soon: Consolidated A/B MAC
Jurisdictions
Page 52
52
MACs Are. . .
• Responsible for:
– Provider enrollment
– Processing claims
– Auditing providers
• Authorized to make Local Coverage Determinations (LCD)
42 USC 1395kk-1(a)(4)
• Re-bid every five (5) years 42 USC 1395kk-1(b)(1)(B)
Page 53
53
MAC Audits
• Conducting data analysis comparing
providers to peers
• Outliers receiving audit requests
• High error rates can result in
prepayment reviews
Page 55
55
Three Types of MICs
• Review-of-Provider MICs
• Audit MICs
• Education MICs
Page 56
56
Current MIC Audit Targets
Physicians/Practitioners DME
Home Health/ Transportation/
Skilled Nursing Ambulance
Hospice Lab/X-ray
Hospital Pharmacy
Nursing Facility Renal Dialysis
Page 57
57
How Are Providers Selected For
Audit?
• MICs select based on data analysis by
other CMS contractors and/or referrals
from state agencies
• Efforts to ensure that MIC audits do not
duplicate state MA audits or interfere
with potential law enforcement
investigations
• No MIC/RAC audit is “random”
Page 58
58
What Are the MICs Looking For?
• Did Medicaid pay for a “covered service?”
• Was the service actually provided?
• Was the service properly billed?
• Was the service properly documented?
• Was the service reimbursed appropriately according to state policies, rules and regulations?
Page 59
59
Records Requests
• Length of time to respond to record
requests expanded to 30 days
– MIC can give 15 day extension
– CMS approval needed for further
extensions
– Extensions typically given as long as
neither the integrity nor the timeliness of
the audit is compromised
Page 60
60
Records Requests
• Requests may include demand for color
copies or scanned documents on CD
• Unlike RACs, no apparent limit on
number of documents that may be
requested
• National 5 year look-back period for
audits
Page 61
61
What Happens After MIC Audit?
• MIC prepares draft report, shares with
state and then with provider
• State and provider may comment on
draft findings
• CMS considers comments and prepares
a revised draft audit report which is then
shared only with state for final
comments
Page 62
62
What Happens After MIC Audit?
• CMS issues final audit report and
specifies overpayment, if any
• State pursues collection of overpayment
• Providers have full appeal rights under
state law
– No explicit federal right of appeal
• Audit MIC supports state during appeal
process
Page 63
63
OIG Reviews MICs
• Review MICs had problems with data and analyses
• 81% of audits did not identify overpayments
• 11% audits completed: $6.9 M in overpayments
– $6.2M resulted from 7 completed collaborative audits involving Audit MICs, Review MICs, States and CMS
• States invalidated more than one-third of sampled potential overpayments
• Medicaid Statistical Information System needs additional data elements important to detecting Medicaid fraud, waste and abuse
• http://oig.hhs.gov/oei/reports/oei-05-10-00200.pdf (2/22/2012)
• http://oig.hhs.gov/oei/reports/oei-05-10-00210.pdf (2/22/2012)
Page 64
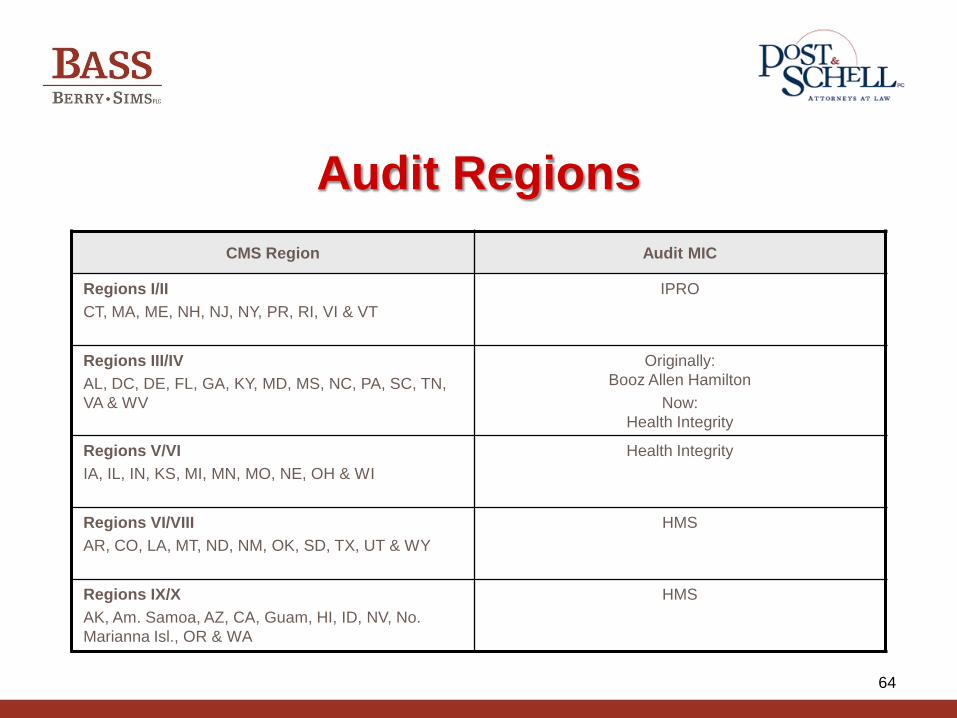
64
Audit Regions
CMS Region Audit MIC
Regions I/II
CT, MA, ME, NH, NJ, NY, PR, RI, VI & VT
IPRO
Regions III/IV
AL, DC, DE, FL, GA, KY, MD, MS, NC, PA, SC, TN,
VA & WV
Originally:
Booz Allen Hamilton
Now:
Health Integrity
Regions V/VI
IA, IL, IN, KS, MI, MN, MO, NE, OH & WI
Health Integrity
Regions VI/VIII
AR, CO, LA, MT, ND, NM, OK, SD, TX, UT & WY
HMS
Regions IX/X
AK, Am. Samoa, AZ, CA, Guam, HI, ID, NV, No.
Marianna Isl., OR & WA
HMS
Page 65
65
Medicaid RACs and MICs
• States required to contract with contingency-fee paid RACs to conduct audits of Medicaid providers
• Recent OIG report concluded that RACs should have been incentivized to make fraud referrals
• Unclear how RACs will interface with Medicaid Integrity Contractors (MICs)
Page 66
66
Responding to an Audit
Page 67
67
Preparation Before Audit is Key.
• Develop effective policies and
procedures by:
– Establishing company policy
– Training your employees
– Identifying your team
– Knowing the issues and your exposure
– Preparing for extensive document
production
Page 68
68
Review Your Contracts
• What are your obligations regarding notice of claims?
• An audit may not be the same as a claim denial
• Define cooperation obligations
• When is your claim final?
• Do you have to complete the entire appeals process?
• What are you entitled to recover?
• Who is ultimately responsible?
Page 69
69
Internal Audits and Monitoring
• Gather disclosure information
• Review denied claims for legitimacy, rebuttal or appeal—root cause analyses
• Identify and fix any internal control or procedural deficiencies
• Refile corrected claims where appropriate
• Consult with counsel as necessary
• Remember the 60 Day Repayment Rule
Page 70
70
The Importance of the Mail Room
Page 71
71
Responding to Audits
• Provide complete documentation
• Don’t rush the process BUT meet deadlines
• Don’t sign statements certifying completeness
of records until confirming that all documents
have been provided
• Retain or request a copy of all documents
provided to contractor
Page 72
72
Best Practices
• Select an Audit Coordinator to manage all
inquiries and coordinate evaluation of all
records sent out for audit/review
• Tell the RA the name and address of your
coordinator
– http://dcsrac.com/ProviderContactInformati
on.aspx
• Make sure your MAC has the right address
Page 73
73
Timeliness Is Important
• Implement systems for timely responses to audit
• Develop a log
– Date stamp all correspondence and monitor electronic remittance advices
– Track requests for information, deadlines, extensions and dates sent
– Log all contacts with the RA (names, dates, times and summary of conversation)
– Log notices of overpayments, dates for repayment, dates for appeals
Page 74
74
Timeliness Is Important
• Do you know where your records are?
– Storage, soft files, filing back log
• Request extension if needed
• Copy entire medical record and all relevant
documents, and keep a copy
• Follow instructions from the auditor (e.g. DCS--
http://dcsrac.com/Documentation.aspx)
• Proof of mailing/proof of receipt
Page 75
75
Letters Requesting Self-Audit
• Engage counsel
• Assess risk
• Hospice of the Comforter, Inc.
Whistleblower Lawsuit
Page 76
76
Appealing Unfavorable Results
Page 77
77
Medicare Appeal Process
• Redetermination from the
Intermediary/Carrier
• Reconsideration from a Qualified
Independent Contractor
• Appeal to an administrative law judge
• Appeal to the Medicare Departmental
Appeals Board
• Appeal to a federal district court Source: 42 C.F.R. Part 405, Subpart I
Page 78
78
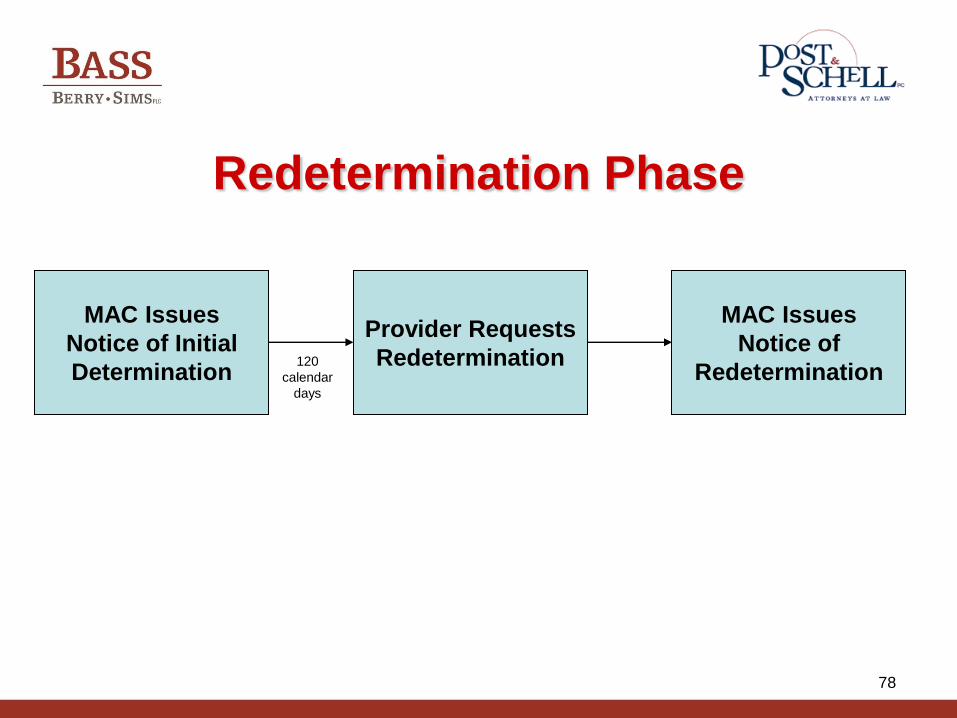
Redetermination Phase
MAC Issues
Notice of Initial
Determination
Provider Requests
Redetermination
MAC Issues
Notice of
Redetermination 120
calendar
days
Page 79
79
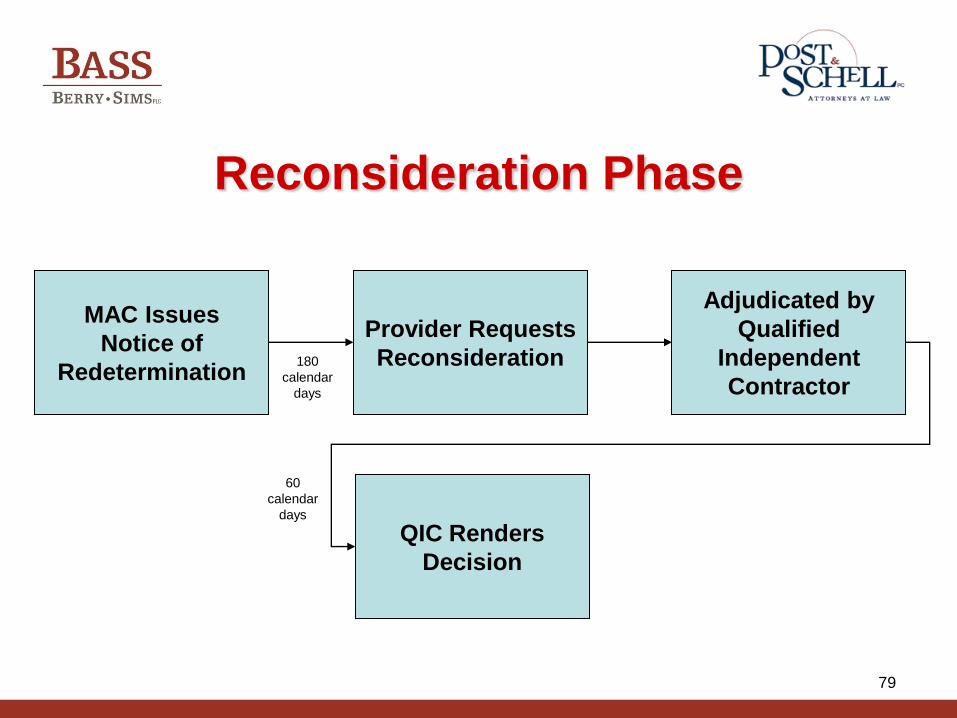
Reconsideration Phase
MAC Issues
Notice of
Redetermination
Provider Requests
Reconsideration
Adjudicated by
Qualified
Independent
Contractor
180
calendar
days
QIC Renders
Decision
60
calendar
days
Page 80
80
Appeal to an Administrative
Law Judge
QIC Renders
Decision
Provider Requests
ALJ Hearing
ALJ Renders
Decision 60
calendar
days
90
calendar
days
Page 81
81
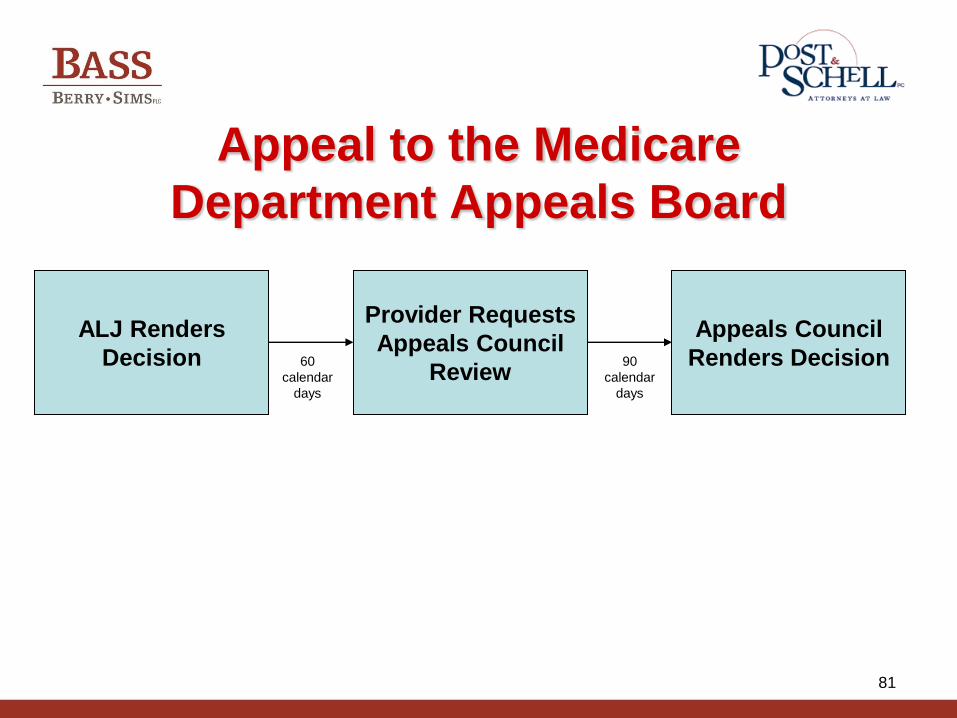
Appeal to the Medicare
Department Appeals Board
ALJ Renders
Decision
Provider Requests
Appeals Council
Review
Appeals Council
Renders Decision 60
calendar
days
90
calendar
days
Page 82
82
Appeal to a Federal District Court
Appeals Council
Renders Decision
Appeal to Federal
District Court 60
calendar
days
Page 83
83
Beware of Recoupment
• Redetermination
• Reconsideration
• Subsequent levels of appeal
Source: 42 C.F.R. Part 405, Subpart C
Page 84
84
Tips for Appeals
• Be prepared to appeal
• Know appeal timelines and
requirements for each appeal level
• Understand reasons for denial at each
level of appeal
• Look out for contractor participation
Page 85
85
Tips for Appeals
• Develop multi-disciplinary appeals team
• Establish tracking system
• Review EVERY claim for possible appeal
– Procedural – Did the contractor follow rules?
– Substantive – Was claim medically necessary?
Page 86
86
Tips for Appeals
• Consider Legal Defenses
– Provider Without Fault (SSA Section 1870)
– Waiver of Liability (SSA Section 1879(a))
– Treating Physician’s Rule
– Reopening Regulations
– Constitutional Challenges
Page 87
87
Tips for Appeals
• If extrapolation is used, consider:
– Were allowed claims included in
overpayment sample calculation?
– Were calculations performed correctly at
each level?
Page 88
88
Tips for Appeals
• Challenging Sampling Methodology
– No administrative or judicial review of determination of high level of payment error BUT determination must be made
– Failure to follow one or more requirements in Benefit Integrity Manual does not necessarily affect validity
– Not sufficient to argue better or more precise methods are available
Page 89
89
Tips for Appeals
• Challenging Sampling Methodology
– Can challenge validity of sampling
methodology based on “the actual
statistical validity of the sample as drawn
and conducted”
– Contractor has burden of establishing
sample was in fact random and statistically
valid
Page 90
90
Tips for Appeals
• When submitting appeal:
– Obtain internal and external reviews
(medical, coding, statistical) as appropriate
– Develop position paper with supporting
medical records and expert opinions
Page 91
91
Contact Information
Anna M. Grizzle
Bass, Berry & Sims PLC
[email protected]
Paula G. Sanders
Post & Schell, PC
[email protected]