73
PARAGANGLIOMAS By DR EUNICE RABIATU ABDULAI ENT DEPARTMENT KBTH DATE:05/12/16
| Date post: | 22-Jan-2018 |
| Category: |
Health & Medicine |
| Upload: | eunice-abdulai |
| View: | 350 times |
| Download: | 0 times |

PARAGANGLIOMASBy
DR EUNICE RABIATU ABDULAI
ENT DEPARTMENT KBTH
DATE:05/12/16
OUTLINE
• Introduction
• Epidemiology
• Definition
• Classifications
• Anatomy
• Aetiology
• pathogenesis
• Clinical characteristics{signs and symptoms}
• Investigations
• Treatment
• Conclusion

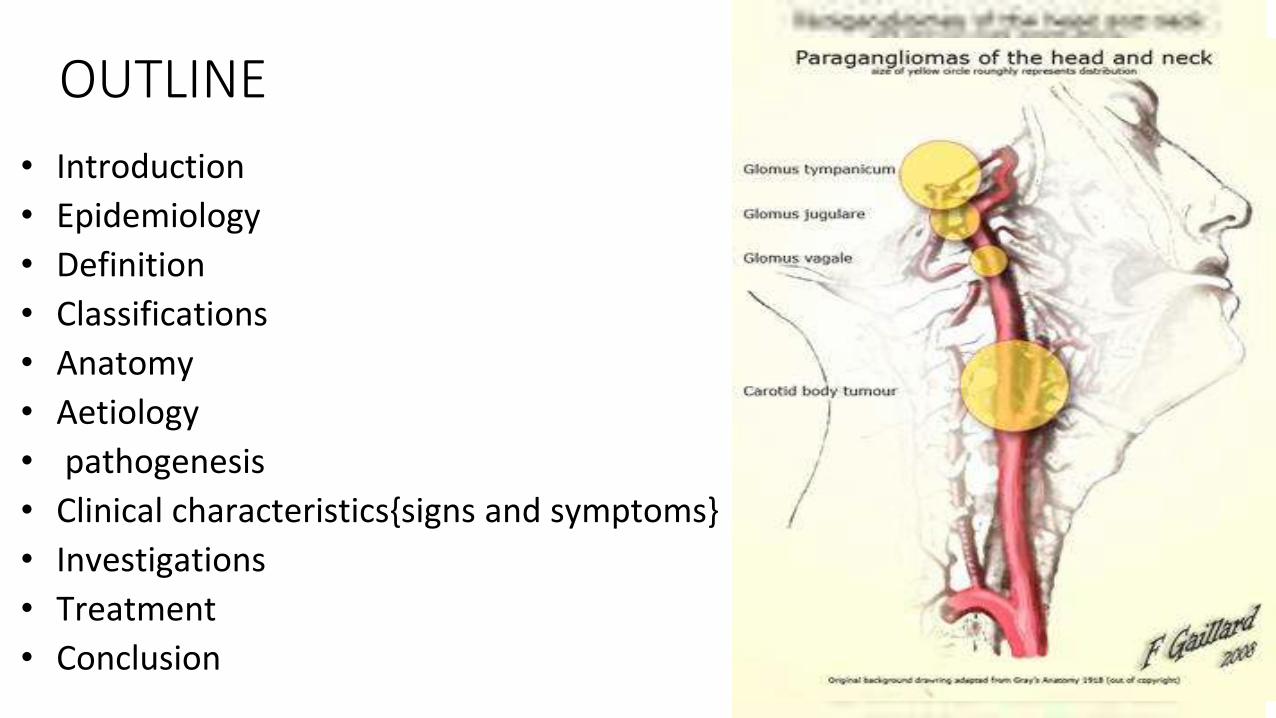
Introduction
• Nomenclature
• Glomus tumours, • chemodectoma, • nonchromaffin tumours, • carotid body tumours
• Correct terminology of paraganglionic tissue : by location
• Carotid body, glomus tympanicum, glomus jugulare

IntroductionNomenclature {Chromaffin cells/ pheochromocytes}
• word 'CHROMAFFIN' comes from chromium and affinity.
• Visualized by staining with chromium salts.
• Chromium salts oxidize and polymerize catechol amines to form a brown colour, most strongly in the cells secreting noradrenaline.
• ENTER CHROMAFFIN CELLS ……histological similarity to chromaffin cells (stain yellow when treated with chromium salts), but functions quite different and not derivatives of neural crest.
• PARAGANGLIA are clusters of either chromaffin cells or glomus cells near sympathetic ganglia.
• Neoplasms arising from these cells are pheochromocytomas

glomus cell Chromaffin cells, also pheochromocytes
Glomus cell( type 1) : peripheral chemoreceptor, mainly located in the carotid bodies and aortic bodies, helps the body regulate breathing.
neuroendocrine cellsfound mostly in the medulla of the adrenal glandfor flight- or –fight response
Blood (↓ pH, ↓pO2, or ↑pCO2 ) →carotid bodies and the aortic bodies signal → medulla oblongata (dorsal inspiratory centre in the medulla oblongata) to increase the volume and rate of breathing.
Chromaffin cells →→ release catecholamines: ~80% of Epinephrine (Adrenaline) and ~20% of Norepinephrine (Noradrenaline) into→→ systemic circulation for →→systemic effects on multiple organs (similarly to secretory neurons of the hypothalamus), and can also send paracrine signals. Hence they are called neuroendocrine cells.
called non-chromaffin or parasympathetic paraganglia
high metabolic rate and good blood perfusion T/4 sensitive to changes in arterial blood gas tension
. Chromaffin cells also settle near sympathetic ganglia, vagusnerve, paraganglia, and carotid arteries. largest extra-adrenal cluster of chromaffin cells is organ of
Zuckerkandl.
glomus cell Chromaffin cells, also pheochromocytes
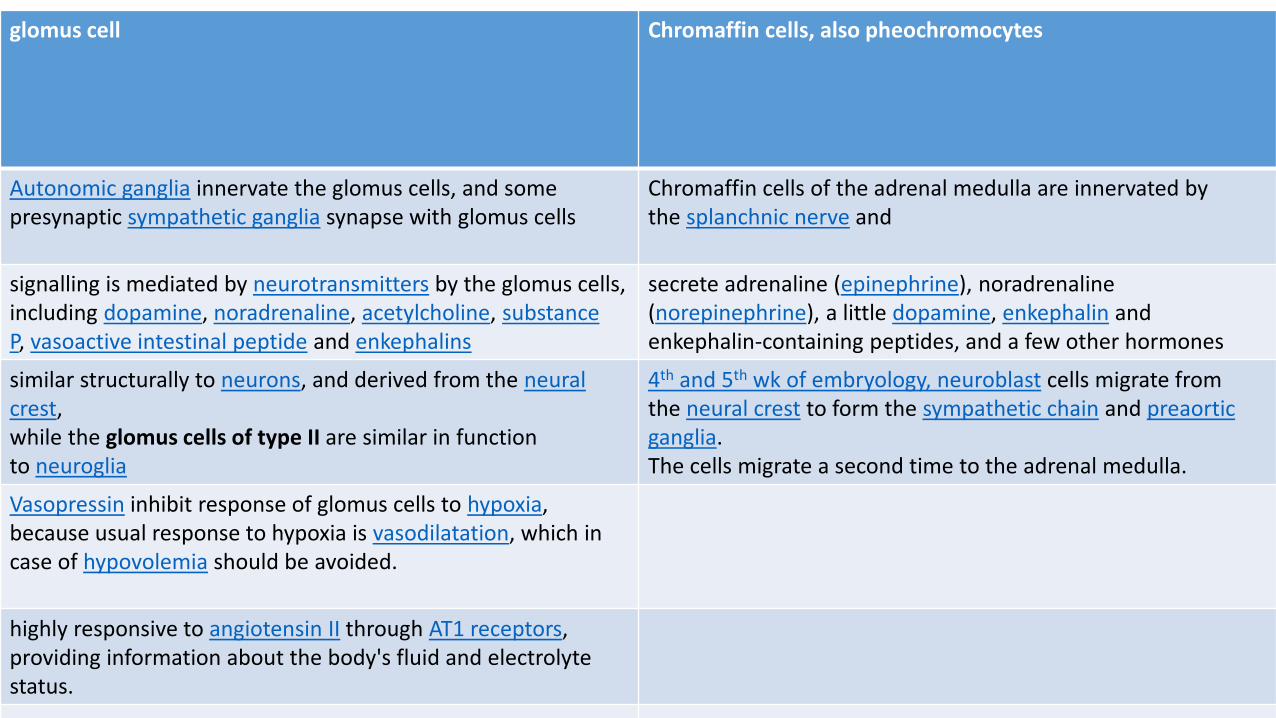
Autonomic ganglia innervate the glomus cells, and some presynaptic sympathetic ganglia synapse with glomus cells
Chromaffin cells of the adrenal medulla are innervated by the splanchnic nerve and
signalling is mediated by neurotransmitters by the glomus cells, including dopamine, noradrenaline, acetylcholine, substance P, vasoactive intestinal peptide and enkephalins
secrete adrenaline (epinephrine), noradrenaline (norepinephrine), a little dopamine, enkephalin and enkephalin-containing peptides, and a few other hormones
similar structurally to neurons, and derived from the neural crest, while the glomus cells of type II are similar in function to neuroglia
4th and 5th wk of embryology, neuroblast cells migrate from the neural crest to form the sympathetic chain and preaorticganglia. The cells migrate a second time to the adrenal medulla.
Vasopressin inhibit response of glomus cells to hypoxia, because usual response to hypoxia is vasodilatation, which in case of hypovolemia should be avoided.
highly responsive to angiotensin II through AT1 receptors, providing information about the body's fluid and electrolyte status.

glomus cell (type I)

Chromaffin cells, also pheochromocytes
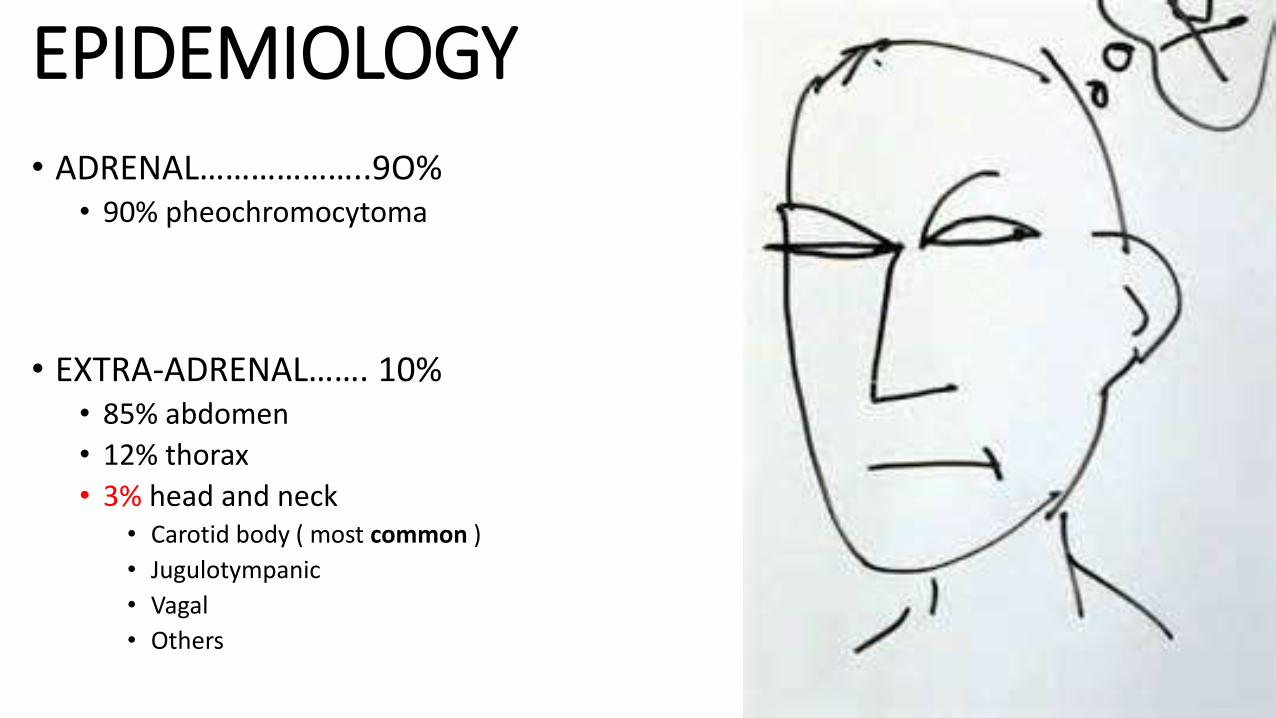
EPIDEMIOLOGY
• ADRENAL………………..9O%• 90% pheochromocytoma
• EXTRA-ADRENAL……. 10%• 85% abdomen
• 12% thorax
• 3% head and neck • Carotid body ( most common )
• Jugulotympanic
• Vagal
• Others
EPIDEMIOLOGY
• 1:30,000 head and neck tumours
• Malignancy determined by metastasis(possible in all locations)• 6% carotid body
• 5% jugulotympanic
• 10 to 19% vagal
• 3% laryngeal
• 17% sinonasal
• Survival data • 60% 5-year regional mets
• Distant mets worse
DEFINITION
• PARAGANGLIOMA is a type of noncancerous (benign) tumour that occurs in structures called paraganglia.
• PARAGANGLIA are groups of cells that are found near nerve cell bunches called ganglia.
• Paragangliomas are usually found in the head, neck, or torso.
• However, a type of paraganglioma known as PHEOCHROMOCYTOMA develops in the adrenal glands. (produce hormones in response to stress).

CLASSIFICATIONS
• Adrenal/extraadrenal
• Benign (97%)/ malignant (3%)…..produce distance metastasis. • Extra-adrenal paragangliomas become malignant than other paraganglioma or
pheochromocytoma.
• Sympathetic/parasympathetic
• Syndromic/ non syndromic

CLASSIFICATIONS• ADRENAL
• PHEOCHROMOCYTOMA
• EXTRA-ADRENAL• BRANCHIOMERIC
• AORTICOPULMONARY• CORONARY• INTERCAROTID• JUGULOTYMPANIC• LARYNGEAL• NASAL• ORBITAL• PULMUNARY• SUBCLAVIAN
• INTRAVAGAL• AORTICOSYMPATHETIC• VISEROAUTONOMIC
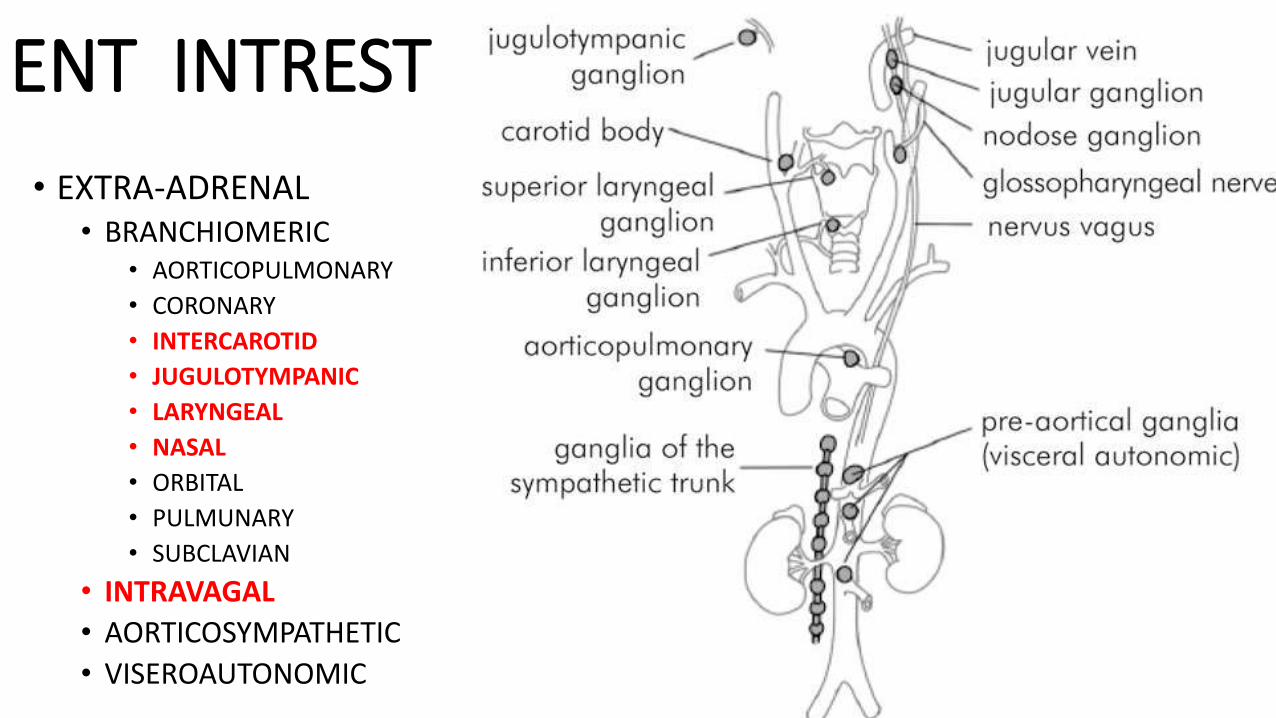
ENT INTREST
• EXTRA-ADRENAL• BRANCHIOMERIC
• AORTICOPULMONARY
• CORONARY
• INTERCAROTID
• JUGULOTYMPANIC
• LARYNGEAL
• NASAL
• ORBITAL
• PULMUNARY
• SUBCLAVIAN
• INTRAVAGAL
• AORTICOSYMPATHETIC
• VISEROAUTONOMIC

ANATOMY

ANATOMY

ANATOMY

ANATOMY
Aetiology
• 75% ------ sporadic
• 25% are hereditary
Aetiology(Familial paragangliomas)
• 10% of cases
• Most commonly bilateral CBP
• Chromosomes 11q13.1, 11q22-q23
• Autosomal dominant
• Genomic imprinting • Only expressed if father passes gene
• ? Higher incident with hypoxia due to altitude or medical conditions
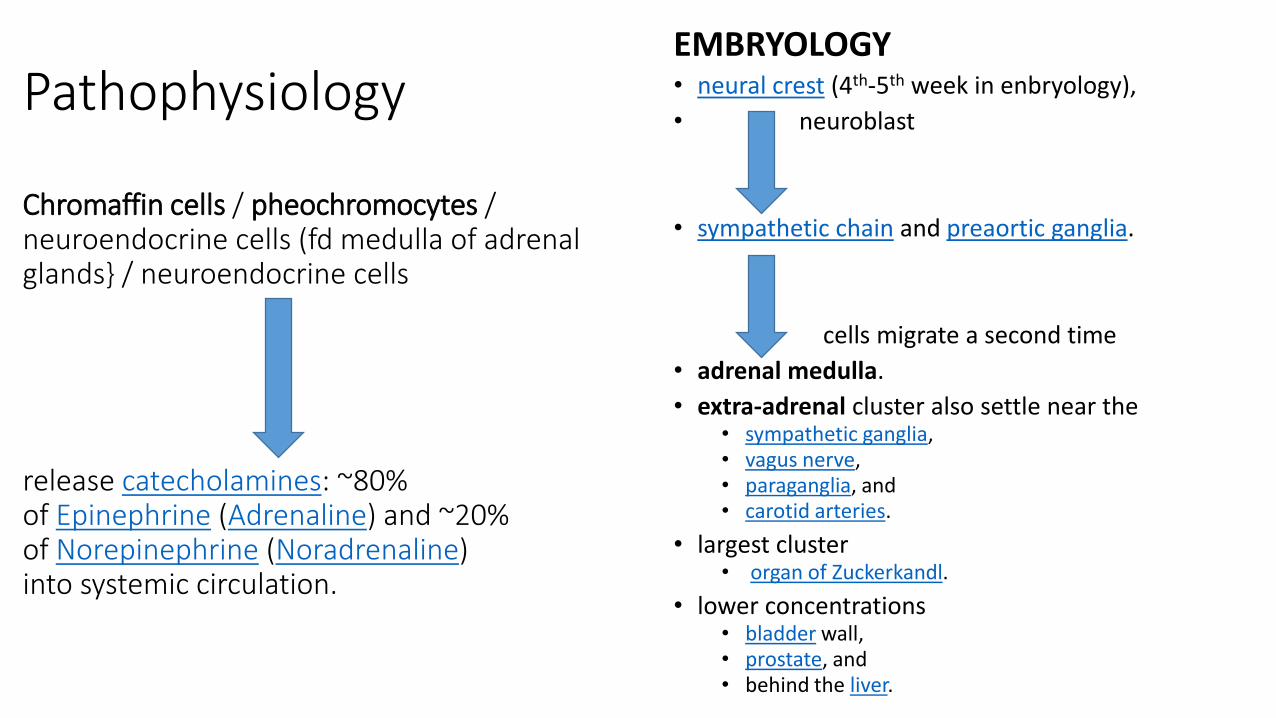
Pathophysiology
Chromaffin cells / pheochromocytes / neuroendocrine cells (fd medulla of adrenal glands} / neuroendocrine cells
release catecholamines: ~80% of Epinephrine (Adrenaline) and ~20% of Norepinephrine (Noradrenaline) into systemic circulation.
EMBRYOLOGY• neural crest (4th-5th week in enbryology),
• neuroblast
• sympathetic chain and preaortic ganglia.
cells migrate a second time
• adrenal medulla.
• extra-adrenal cluster also settle near the• sympathetic ganglia,• vagus nerve,• paraganglia, and• carotid arteries.
• largest cluster • organ of Zuckerkandl.
• lower concentrations• bladder wall,• prostate, and • behind the liver.

PATHOGENESIS• Pheochromocytomas and some paragangliomas associated with ganglia of the sympathetic nervous
system. • "fight-or-flight" ……response 2⁰ hormones released in response to stress.
• Although most sympathetic paragangliomas are pheochromocytomas
• some are found outside the adrenal glands------extra-adrenal paragangliomas.
• Most sympathetic paragangliomas, including pheochromocytomas, produce• Catecholamines
• epinephrine (adrenaline) or • norepinephrine.
• Excess catecholamines cause• hypertension,• palpitations, • headaches, or • sweating.
PATHOGENESIS
• Most paragangliomas are associated with ganglia of the parasympathetic nervous system, which controls • involuntary functions eg. digestion and saliva formation.
•
• Parasympathetic paragangliomas, • typically found in the head and neck• usually do not produce hormones. • large tumors may cause:
• coughing, • hearing loss in one ear, or • difficulty swallowing.
• Paragangliomas originate from paraganglia in chromaffin-negative glomus cells derived from the embryonic neural crest.

PATHOLOGY• GROSSLY
• sharply circumscribed polypoid masses
• firm to rubbery consistency.
• highly vascular tumours
• may have a deep red colour.
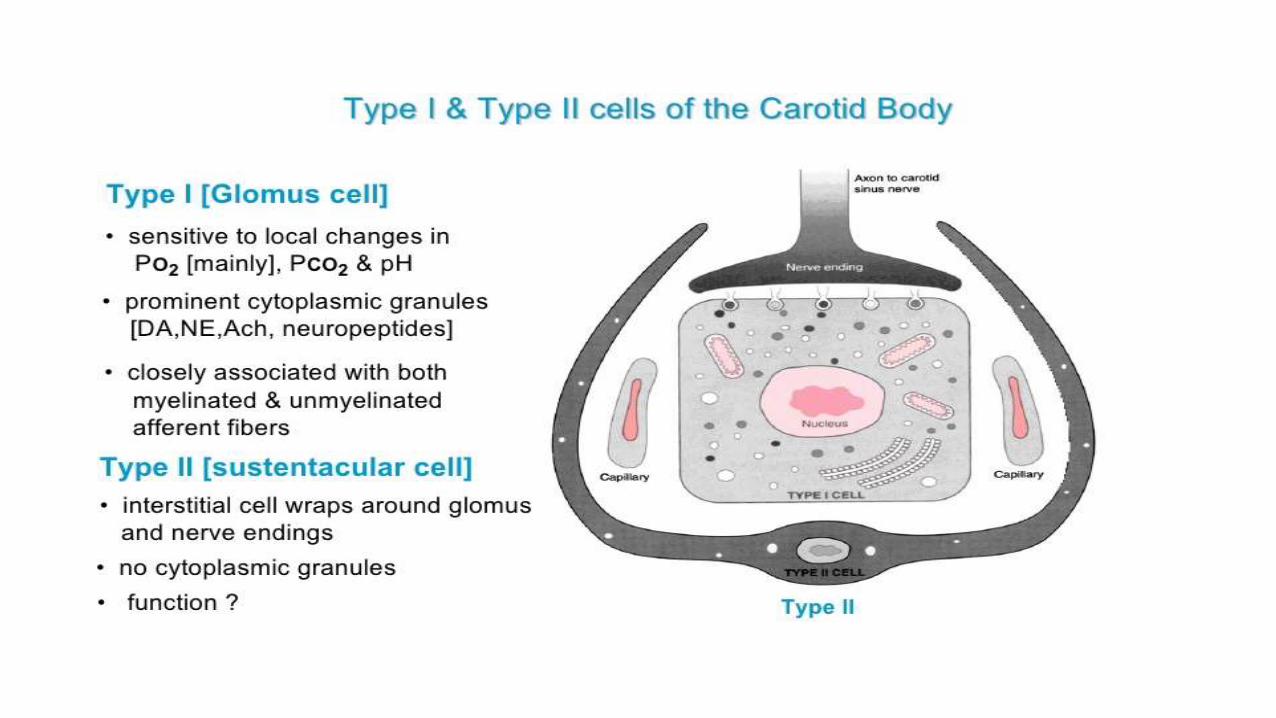
• MICROSCOPIC INSPECTION• Type 1 :Individual tumour cells are polygonal
to oval and are arranged in distinctive cell balls, called Zellballen(organoid nested pattern).chief/grannuler cells
• Cell balls are separated by fibro vascular stroma and surrounded by sustentacular cells.
• Type 2: intracytoplasmic organelles ,dense-core granules: catecholamine tryptophan containing protein: diffuse neuroendocrine system
• LIGHT MICROSCOPY,
• ΔΔ• neuroendocrine tumours
• carcinoid tumour,
• neuroendocrine carcinoma, and
• medullary carcinoma of the thyroid.

PATHOLOGY
• IMMUNOHISTOCHEMISTRY,• Chief cells in the cell balls are positive for
• chromogranin,• synaptophysin,• neuron specific enolase,• serotonin,• neurofilament and• Neural cell adhesion molecule; • they are S-100 protein negative.
• The sustentacular cells are S-100 positive and focally positive for glial fibrillary acidic protein. By
• HISTOCHEMISTRY, • paraganglioma cells are argyrophilic,• periodic acid Schiff negative,• mucicarmine negative, and• argentaffin negative
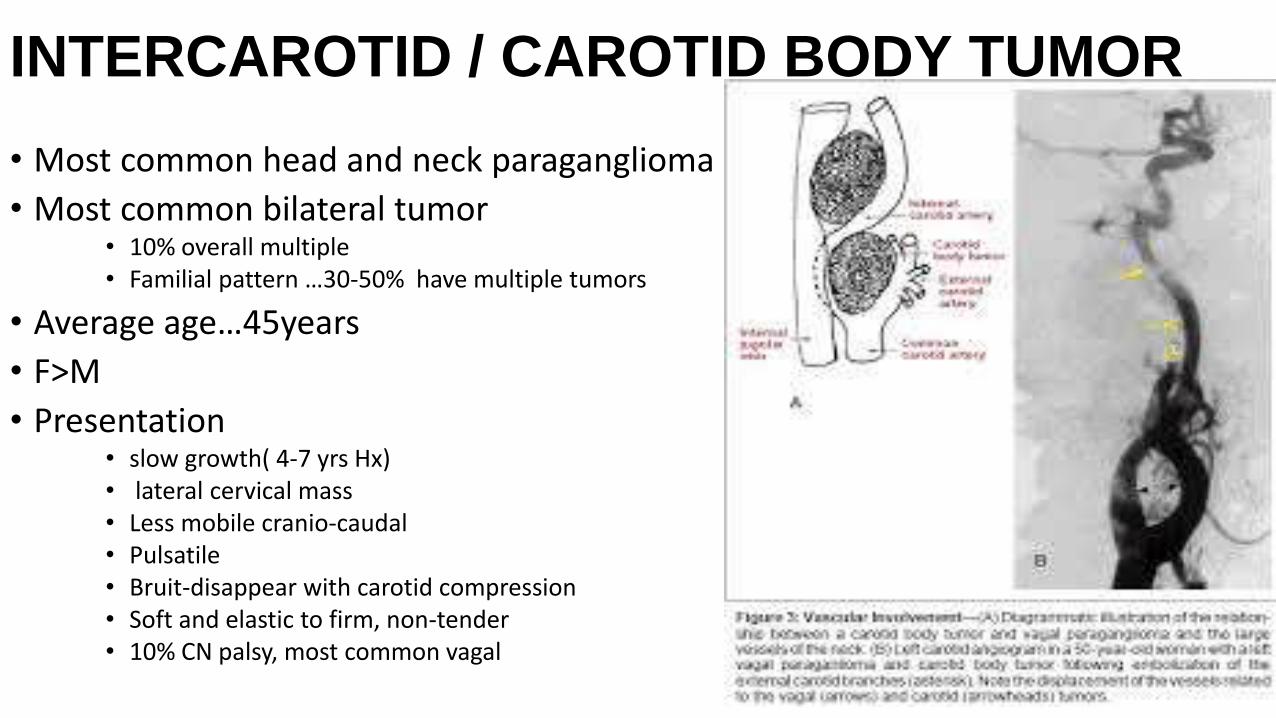
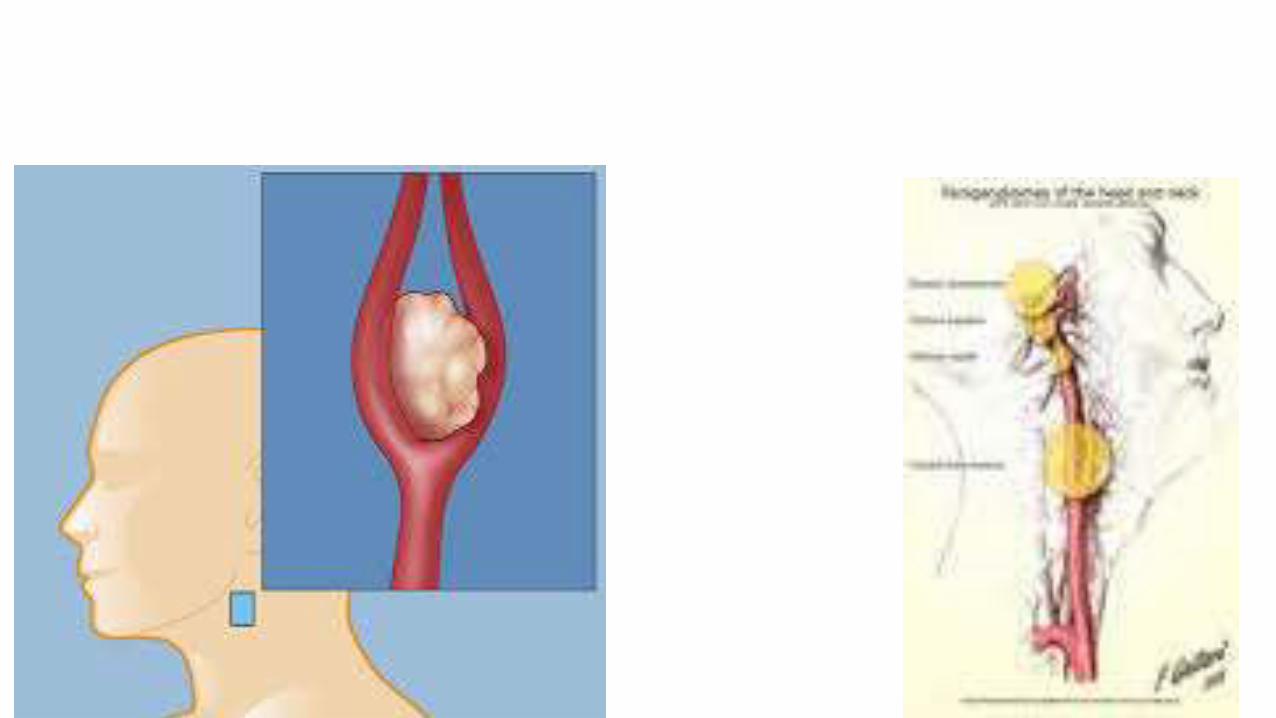
INTERCAROTID / CAROTID BODY TUMOR
• Most common head and neck paraganglioma
• Most common bilateral tumor• 10% overall multiple • Familial pattern …30-50% have multiple tumors
• Average age…45years
• F>M
• Presentation • slow growth( 4-7 yrs Hx)• lateral cervical mass • Less mobile cranio-caudal • Pulsatile • Bruit-disappear with carotid compression • Soft and elastic to firm, non-tender • 10% CN palsy, most common vagal
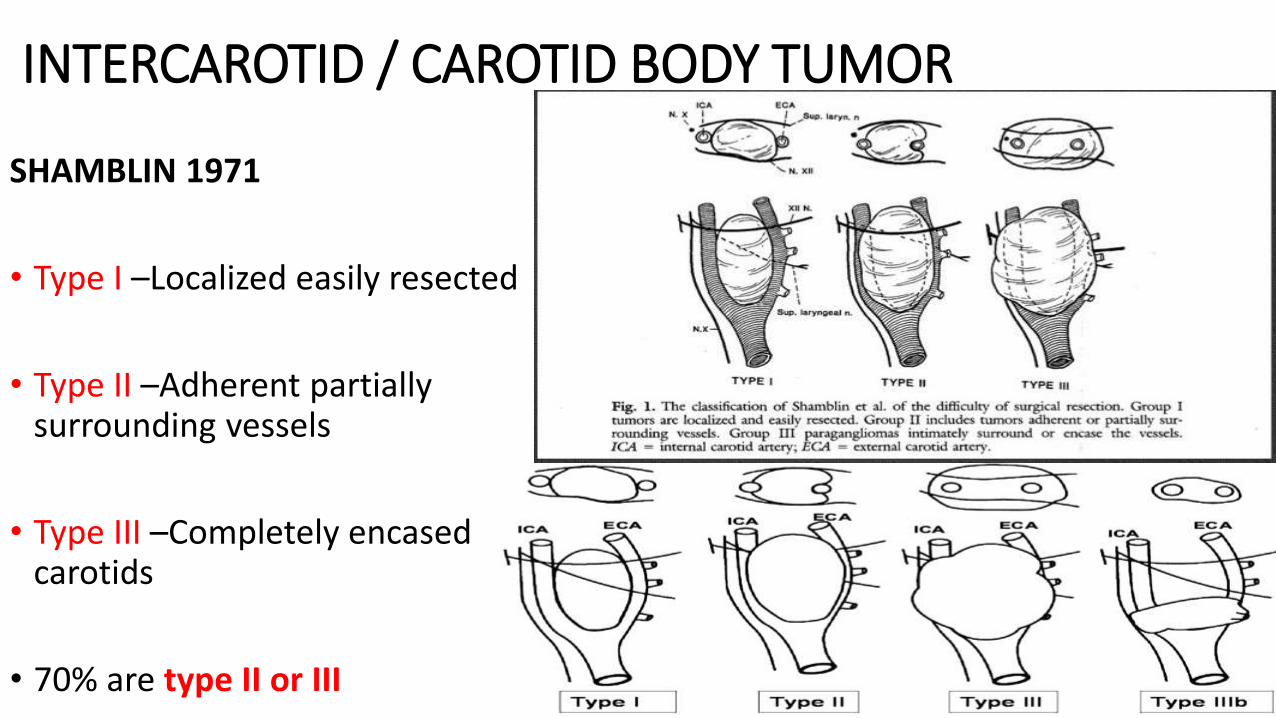
INTERCAROTID / CAROTID BODY TUMOR
SHAMBLIN 1971
• Type I –Localized easily resected
• Type II –Adherent partially surrounding vessels
• Type III –Completely encased carotids
• 70% are type II or III

Carotid Body Tumors: Objective Criteria to Predict the Shamblin Group on MR Imaging
Published online before print
April 16, 2008, doi:
10.3174/ajnr.A1092 AJNR
August 2008 29: 1349-1354

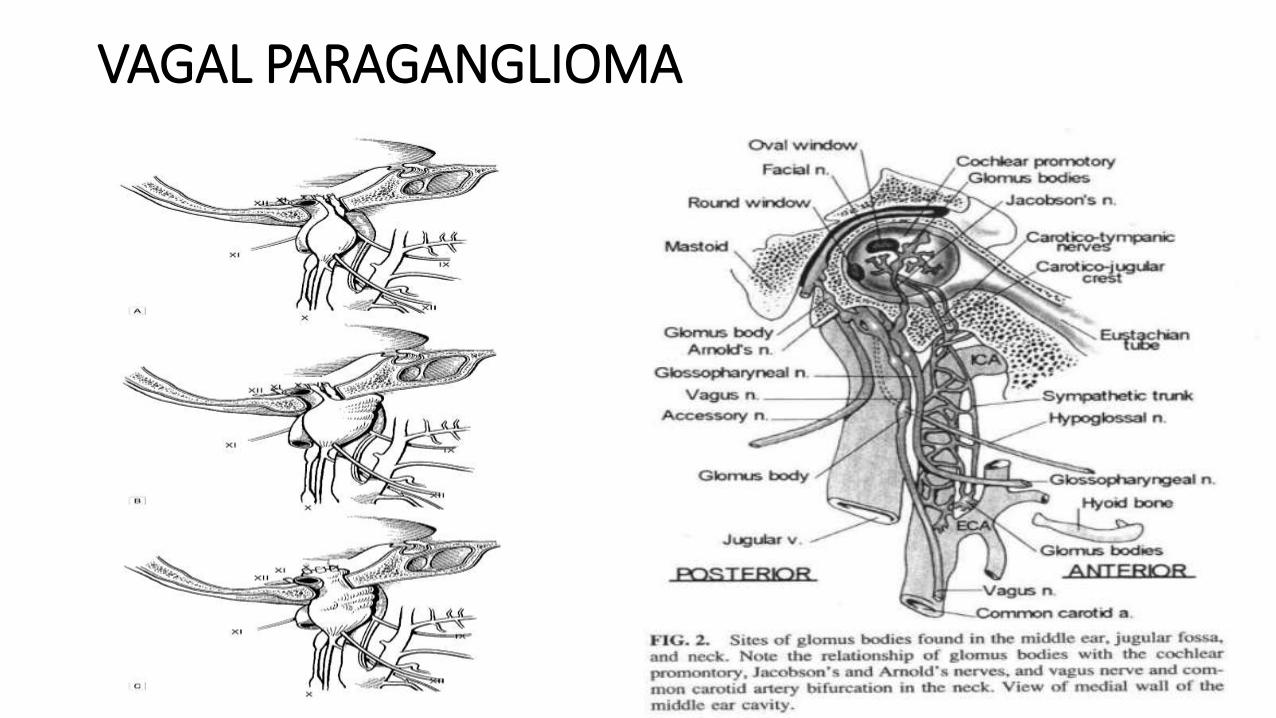
VAGAL PARAGANGLIOMA
• Rare
• 5% all H&N paragangliomas
• Most commonly nodose ganglion
• 200 cases in literature
• limited to cervical region
• attached to skull base, or intracranial
• Presentation • Neck mass, • pulsatile tinnitus, • pharyngeal mass, • hoarseness –36% • cranial nerve deficits at presentation
• X-28%, XII-17%, XI-11%, IX-11%, VII-6%
VAGAL PARAGANGLIOMA

VAGAL PARAGANGLIOMA
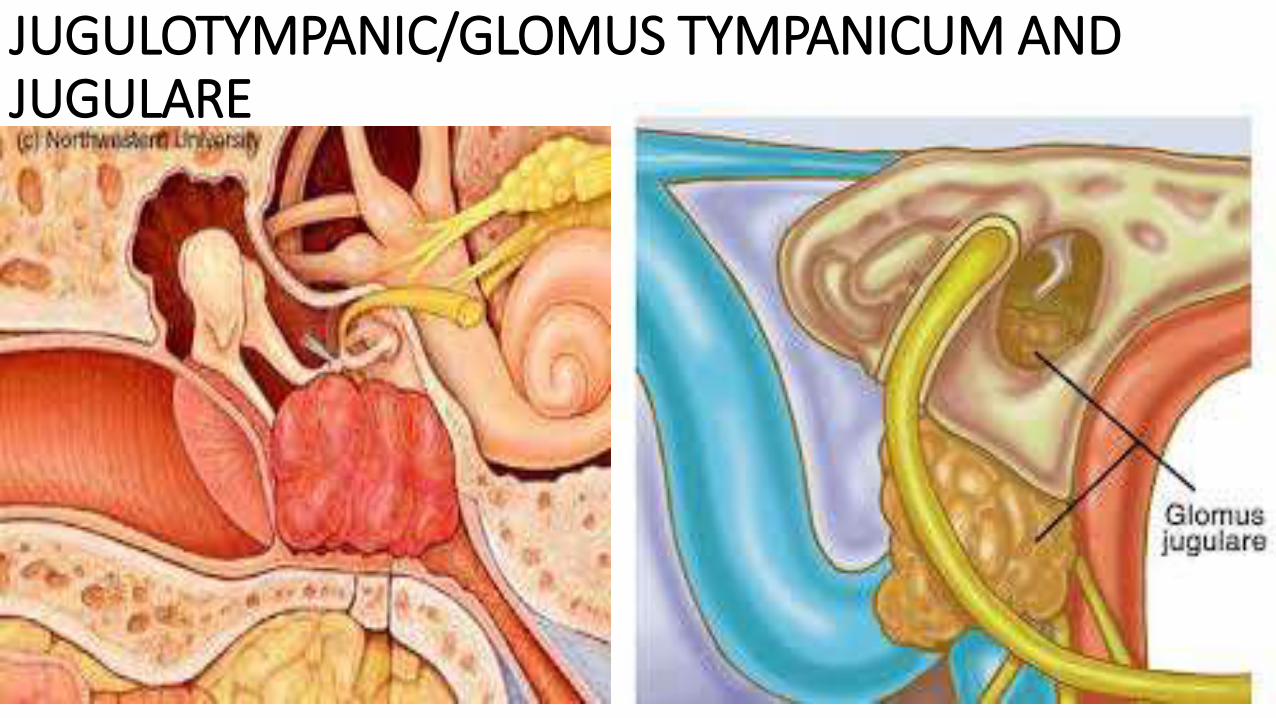
JUGULOTYMPANIC/GLOMUS TYMPANICUM AND JUGULARE

GLOMUS TUMUOR
JUGULOTYMPANIC/GLOMUS TYMPANICUM AND JUGULARE
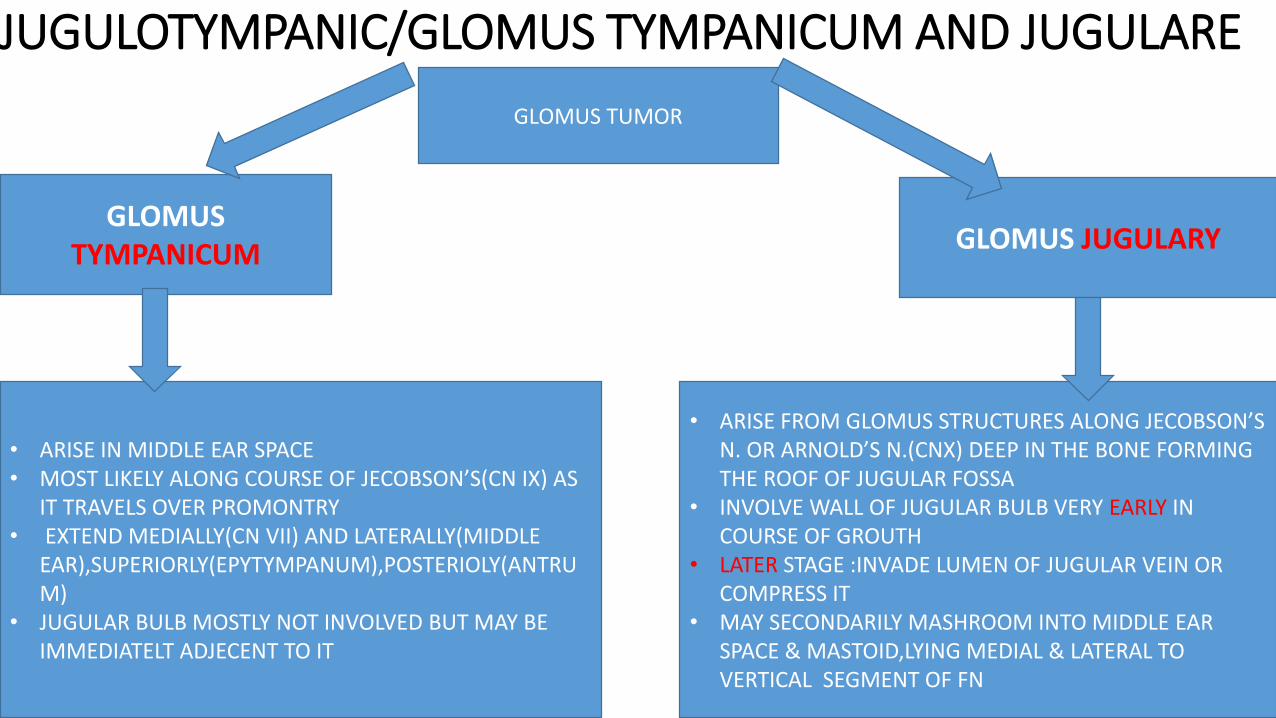
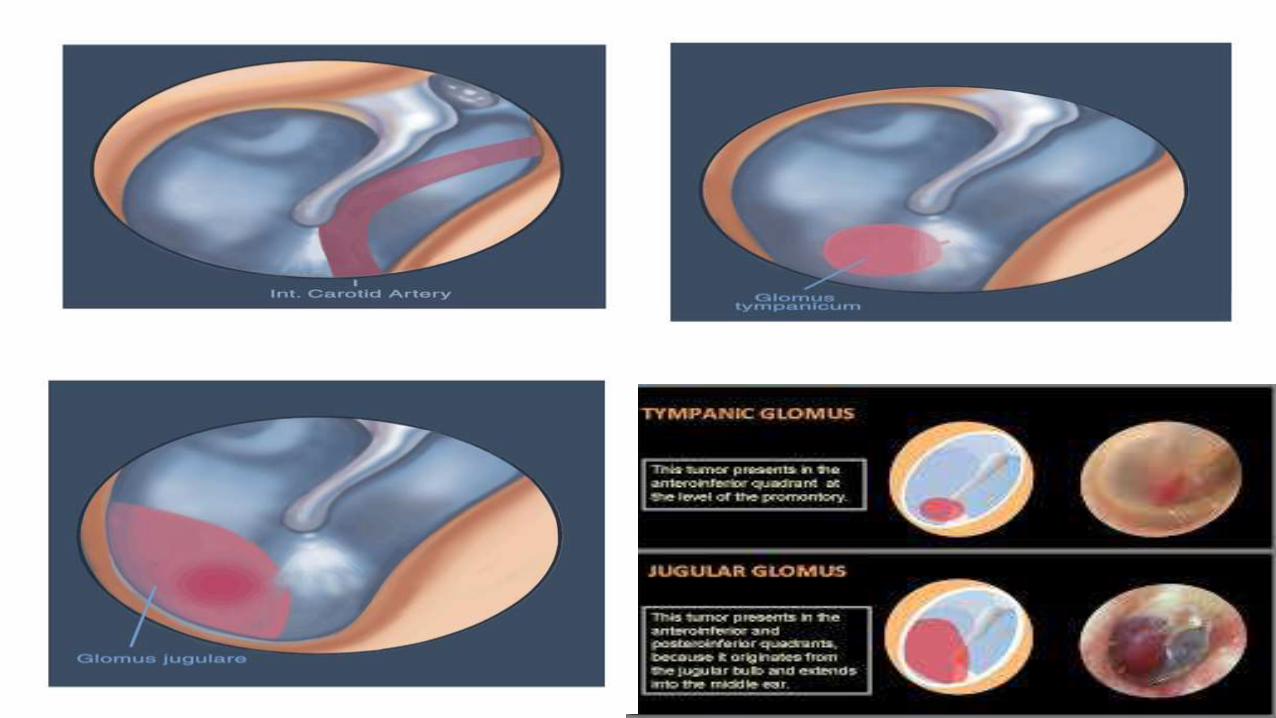
GLOMUS TUMOR
GLOMUS TYMPANICUM GLOMUS JUGULARY
• ARISE IN MIDDLE EAR SPACE• MOST LIKELY ALONG COURSE OF JECOBSON’S(CN IX) AS
IT TRAVELS OVER PROMONTRY• EXTEND MEDIALLY(CN VII) AND LATERALLY(MIDDLE
EAR),SUPERIORLY(EPYTYMPANUM),POSTERIOLY(ANTRUM)
• JUGULAR BULB MOSTLY NOT INVOLVED BUT MAY BE IMMEDIATELT ADJECENT TO IT
• ARISE FROM GLOMUS STRUCTURES ALONG JECOBSON’S N. OR ARNOLD’S N.(CNX) DEEP IN THE BONE FORMING THE ROOF OF JUGULAR FOSSA
• INVOLVE WALL OF JUGULAR BULB VERY EARLY IN COURSE OF GROUTH
• LATER STAGE :INVADE LUMEN OF JUGULAR VEIN OR COMPRESS IT
• MAY SECONDARILY MASHROOM INTO MIDDLE EAR SPACE & MASTOID,LYING MEDIAL & LATERAL TO VERTICAL SEGMENT OF FN
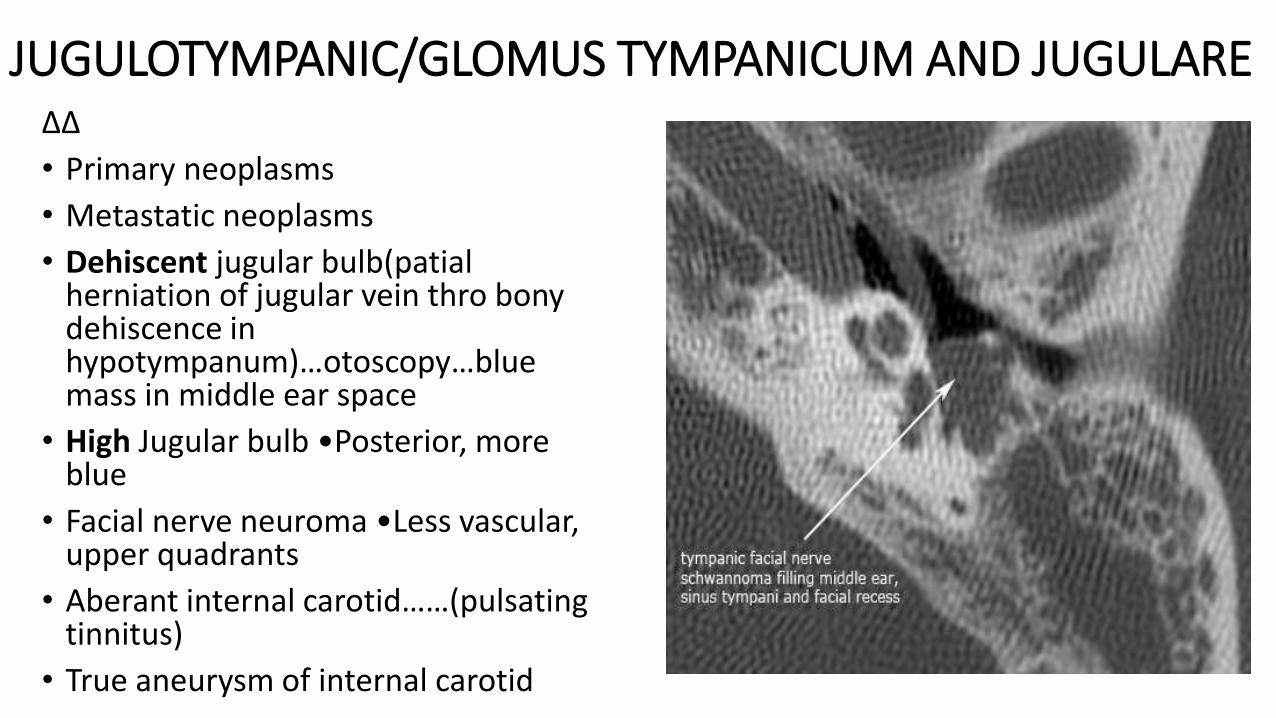
JUGULOTYMPANIC/GLOMUS TYMPANICUM AND JUGULAREΔΔ
• Primary neoplasms
• Metastatic neoplasms
• Dehiscent jugular bulb(patialherniation of jugular vein thro bony dehiscence in hypotympanum)…otoscopy…blue mass in middle ear space
• High Jugular bulb •Posterior, more blue
• Facial nerve neuroma •Less vascular, upper quadrants
• Aberant internal carotid……(pulsating tinnitus)
• True aneurysm of internal carotid

JUGULOTYMPANIC/GLOMUS TYMPANICUM AND JUGULAREFisch classification (GLOMUS TYMPANICUM)
• Type A : Tumor limited to middle ear cleft
• Type B : Tumor limited to tympanomastoid area
• Type C : Tumors involving infralabyrinthine
• Type D₁ : Tumor with intracranial extension < 2cm
• Type D₂ : Tumor with intracranial extension > 2cm
Glasscock-Jackson classification
• Type I : small mass limited to promontry
• Type II : Tumor completely filling the middle ear space
• Type III : middle ear filled and extending into mastoid process
• Type IV : middle ear filled, extending into mastoid or thro TM to fill EAC,mayextend anteriorly to ICA
JUGULOTYMPANIC/GLOMUS TYMPANICUM AND JUGULARE
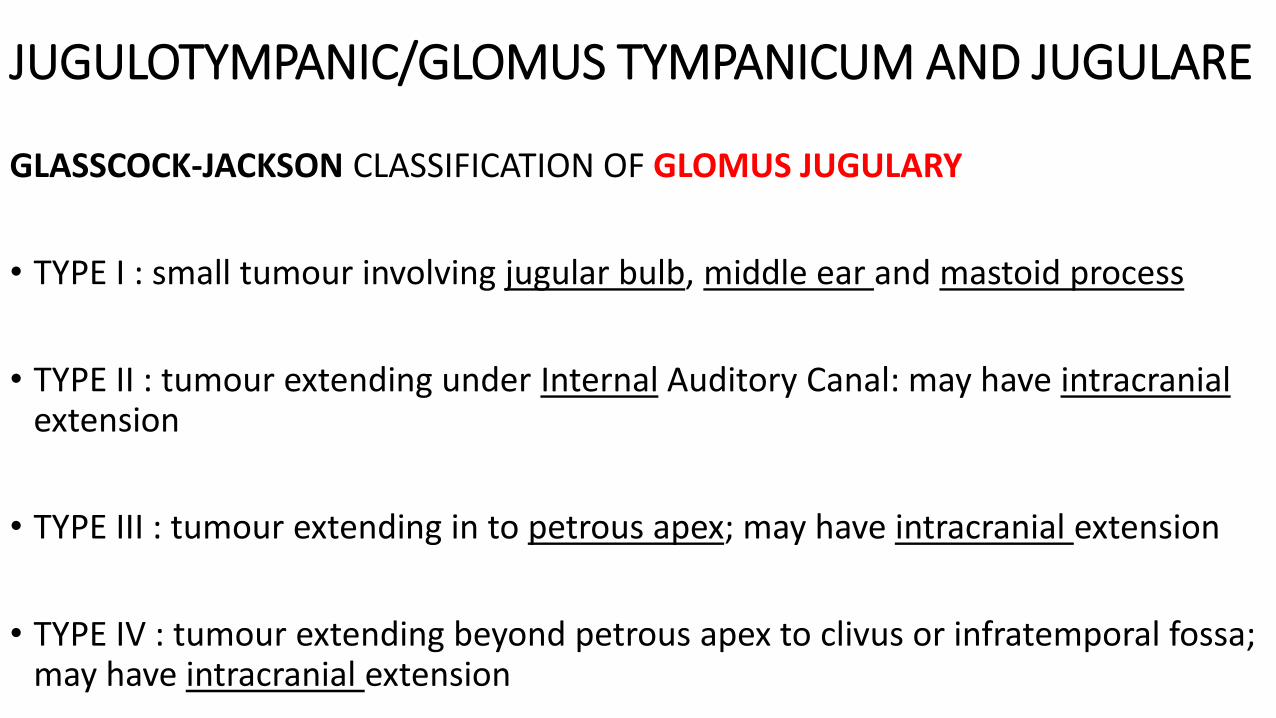
GLASSCOCK-JACKSON CLASSIFICATION OF GLOMUS JUGULARY
• TYPE I : small tumour involving jugular bulb, middle ear and mastoid process
• TYPE II : tumour extending under Internal Auditory Canal: may have intracranial extension
• TYPE III : tumour extending in to petrous apex; may have intracranial extension
• TYPE IV : tumour extending beyond petrous apex to clivus or infratemporal fossa; may have intracranial extension

LARYNGEAL PARAGANGLIOMAS
• Supraglottic or infraglottic
• No cases of multicentricity, familial, or secreting
SUPRAGLOTTIC• hoarseness, SOB, odynophagia
• True Vocal Cord paresis not common
• Diagnosis usually at time of surgical biopsy• brisk bleeding
• May require tracheotomy and laryngeal packing
• Image all submucous laryngeal lesions pre-operatively
• Hemisupraglottic laryngectomy • thro lateral laryngotomy, or pharyngotomy

LARYNGEAL PARAGANGLIOMASINFRAGLOTTIC
• rare
• Inner surface cricoid cartilage, outer surface, in CT membrane, in capsule of thyroid gland
• Symptoms • hoarseness,
• airway obstruction,
• haemoptysis
• Rx• External surgical excision

SINONASAL PARAGANGLIOMAS • Very rare
• Signs of obstructing nasal lesion
• Epistaxis
• May appear as nasal polyps
• Excision intranasally or external approach

Clinical characteristics{symptoms} HISTORY
EARS
• Pulsating tinnitus
• Bloody otorrhoea
• Otalgia (uncommon)
• Hearing loss
• Aural fullness
• Vertigo (rare)
CLINICAL CHARACTERISTICS{SYMPTOMS} HISTORYNOSE
• snoring
• Nasal congestion
• Purulent rhinorrhoea
• Epistasis
• Anosmia
• Nasal mass
• Swelling or deviation of nasal pyramide
Clinical characteristics{symptoms} HISTORY
THROAT
• Altered speech (rhinolalia clausa, hot potato speech, hoarse)
• Swelling
• Dysphagia
• Odynophagia(rare)
• Dyspnoea
• Mouth breathing
• Cough
• Haemoptysis
• Coughs whiles feeding (aspiration)
Clinical characteristics{symptoms} HISTORY
HEAD AND NECK
• headache
• Facial swelling(frontal, ethmoidal or maxillary sinus region)
• Neck swelling
• Facial pain, anaesthesia, weakness
• Epiphora
• Diplopia
• Loss of vision
• Inability to lift arm
Clinical characteristics{symptoms} HISTORY
GENERAL
• Headache,
• Palpitations,
• flushing,
• perspiration,
• cough
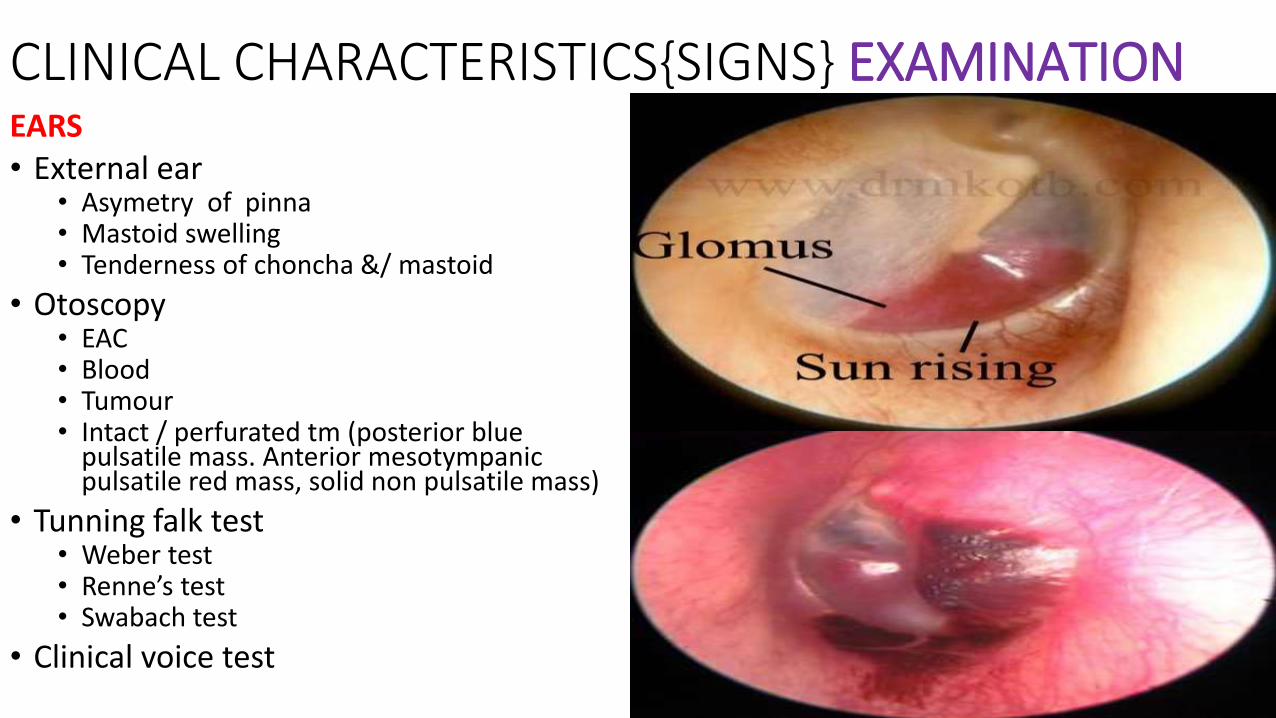
CLINICAL CHARACTERISTICS{SIGNS} EXAMINATIONEARS• External ear
• Asymetry of pinna• Mastoid swelling• Tenderness of choncha &/ mastoid
• Otoscopy• EAC• Blood• Tumour• Intact / perfurated tm (posterior blue
pulsatile mass. Anterior mesotympanicpulsatile red mass, solid non pulsatile mass)
• Tunning falk test• Weber test • Renne’s test • Swabach test
• Clinical voice test

Facial n neuroma
High JugulaB
Petrous cholesteat
oma
Aberrant carotid artery
Clinical characteristics{signs} EXAMINATION
NOSE
• Nasal pyramid• Deviated
• Nasal cavity• Tumour
• Normal/Deviated nasal septum
• Nasal turbinate's (inflamed,/atrophy 2⁰ compression by tumour)
• Postnasal rhinos copy/ rigid or flexible rhinoendoscopy• Tumour in postnasal space or nasopharynx,
nasal cavity , antrum

Clinical characteristics{signs} EXAMINATION
THROAT• Tenting of soft palate
• Deviation of ovula
• Para pharyngeal tumour
• Deviation of tongue
IDL/flexible laryngoscopy• Normal IDL findings
• Supraglottic/subglottic tumour
• Immobile vocal cord
• Hypopharyngeal bulge
• Dysplaced larynx

Clinical characteristics{signs} EXAMINATION
HEAD AND NECK
• Asymmetry of head and neck• Swelling on forehead , cheek , mastoid region, neck
• Facial weakness
• Lymph nodes
• Cranial nerves

C F : Syndromes
•MEN IIA-Sipple’s syndrome • RET proto-oncogene chromosome 10
• Medullary thyroid carcinoma, pheochromocytoma, parathyroid hyperplasia
•M E N I I B • RET but different site
• Mucosal neuromas
•Von Hipple-Lindau• Retinal angiomas, cerebellar hemangioblastomas
• Carney’s complex • Gastric leiomyosarcoma,
• pulmonary chondroma,
• extraadrenal functional paragangliomas
INVESTIGATIONS• HEAMATOLOGY :
• (FBC, Clotting profile, sickling, HB electrophoresis, Grouping and cross matching, ESR)
• BIOCHEMISTRY:• (BUNCr electrolyte, LFT,RBS,FBS)• 24-hour urine
• Norepinephrine, metabolites: vanillylmandelic acid, normetanephrine• Excess epinephrine, metanephrine suspect pheochromocytoma
• MICROBIOLOGY:• (C/S(purulent aural/nasal discharge/blood c/s),urine R/E,)
• BIOPSY:( eg:Therapeutic Excisional biopsy)
• IMAGING(X-Ray,CT-SCAN,MRI,SESTAMIBI NECK SCAN,U/S,ECHO)• (Depends on pathology)
• OTHERS :• (hormonal(eg TFT,))

IMMAGING (glomus tumour)
• PLAIN FILM OF TEMPORAL BONE(X-RAY)• Modified base view(beam directed underneath mandible/ thro oral cavity towards jugular foramen)
• Gives details of jugular foramen , erosive changes /distortion of normal contour
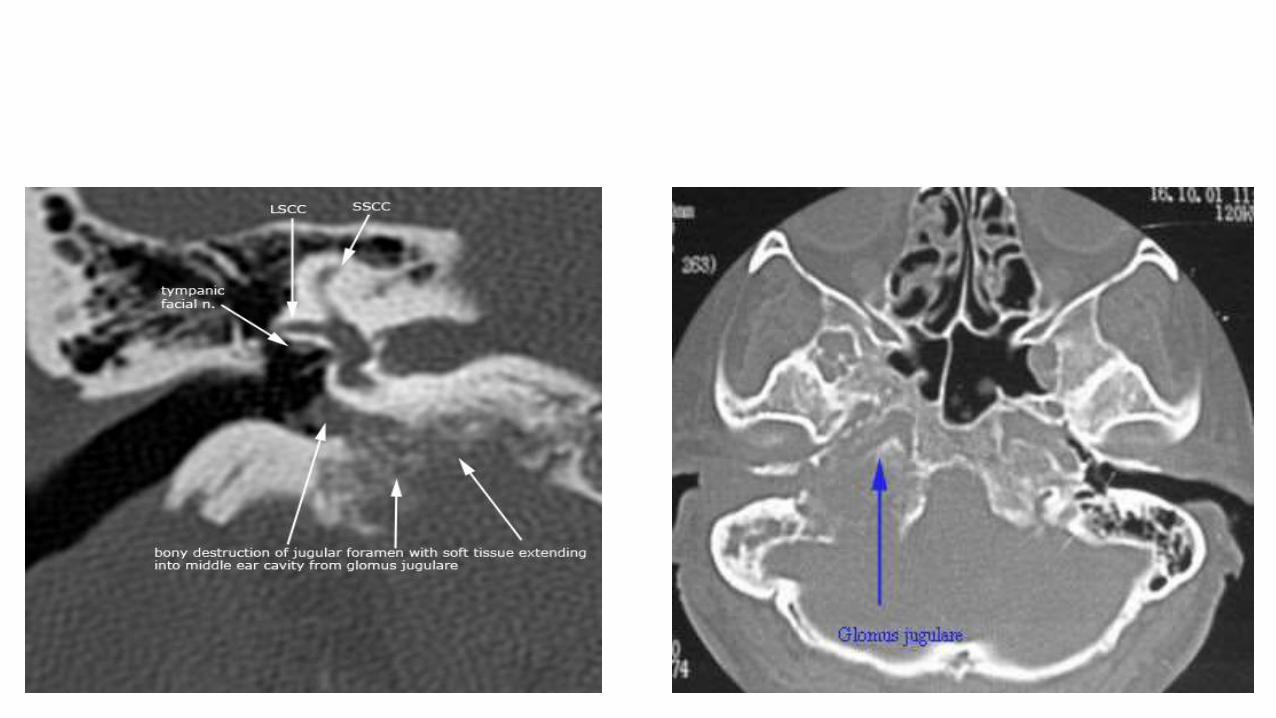
• STANDARD TOMOGRAPHIC TECHNIGUES(POLYTOME APPROACH)• Delineate bony destruction
• Contour of jugular foramen• Bone structure in hypo tympanum• Vertical/ descending portion of FN• Normal course of bony canal of ICA(R/O Aberrant ICA)
• ANGIOGRAM• Attention directed towards feeding vessels
• Ascending pharyngeal artery• Characteristic of tumour
• Late injection films- demonstrate. Normal/blocked venous drainage thro jugular bulb
• CT-SCAN• Demarcates bony details and major blood vessels, Intracranial extension, extend of temporal bone involvement and plan for surgery
• BALLOON OCCLUSION- EEG and Technetium 99 SPECK SCANNING : 99% specificity to tolerance of collateral cerebral circulation.
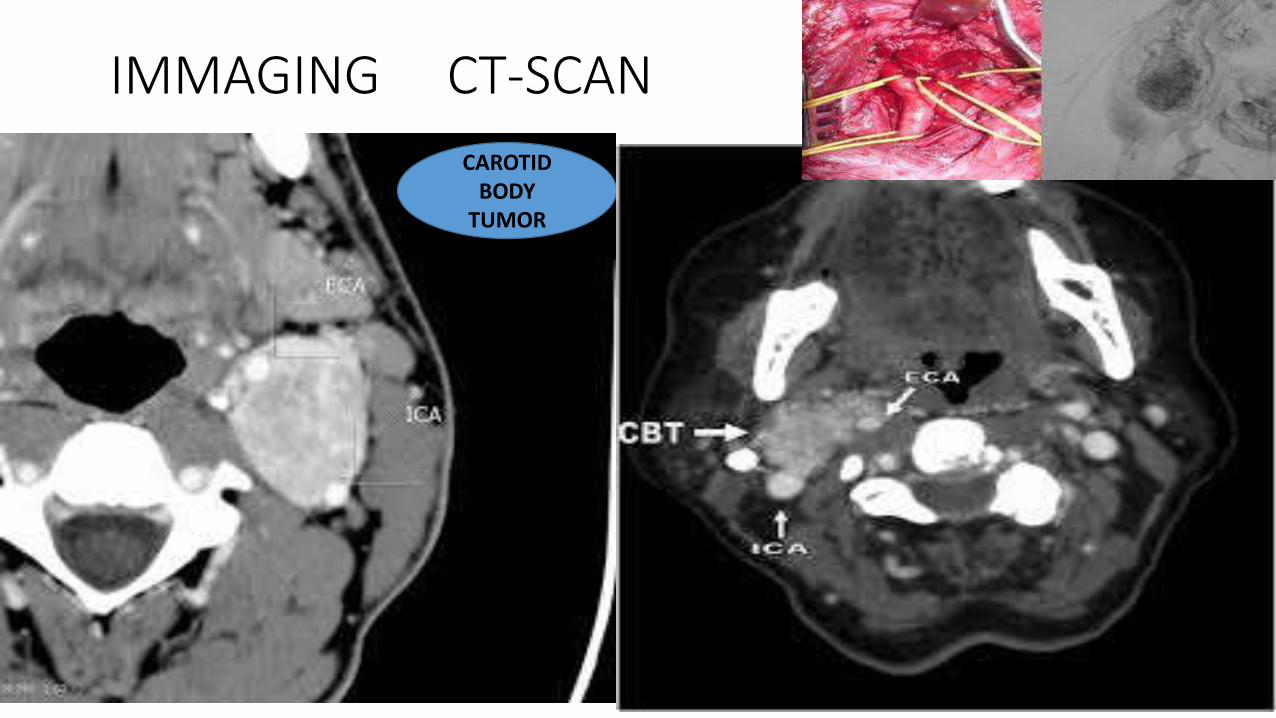
IMMAGING CT-SCAN
CAROTID BODY
TUMOR

VAGAL

JUGULOTYMPANIC


IMMAGING MRI

IMMAGING ANGIOGRAM
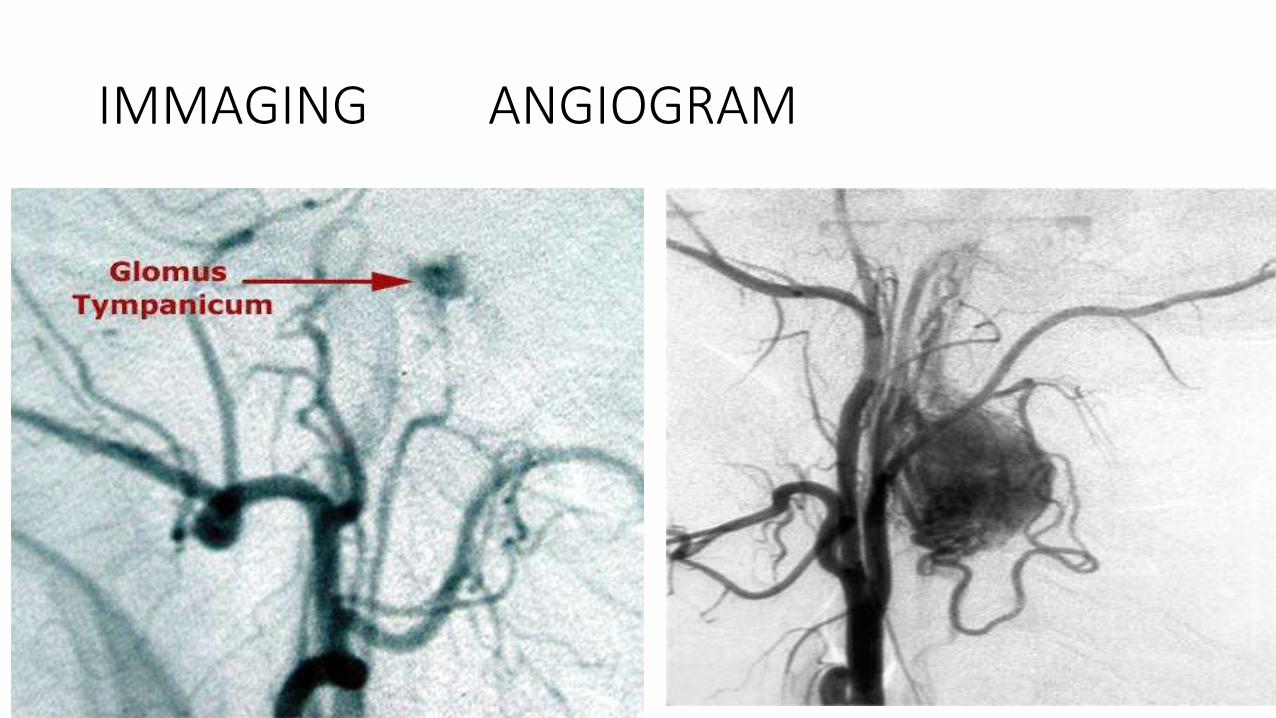
IMMAGING ANGIOGRAM

DIFFERENTIAL DIAGNOSIS
• W.H.O CLASSIFICATION OF NEUROENDOCRINE NEOPLASMS
• EPTHELIAL ORIGIN• TYPES
• CLASICAL CARCINOID
• ATYPICAL CARCINOID
• SMALL CELL NEUROENDOCRINE CARCINOMA• OAT CELL
• INTERMEDIATE CELL
• COMBINED
• NEURONAL ORIGIN• TYPES
• PARAGANGLIOMS

TREATMENT
• Medical
• Surgical
• radiotherapy
• Combined treatment
MEDICAL TREATMENT
• alpha and beta antagonists
• Observation
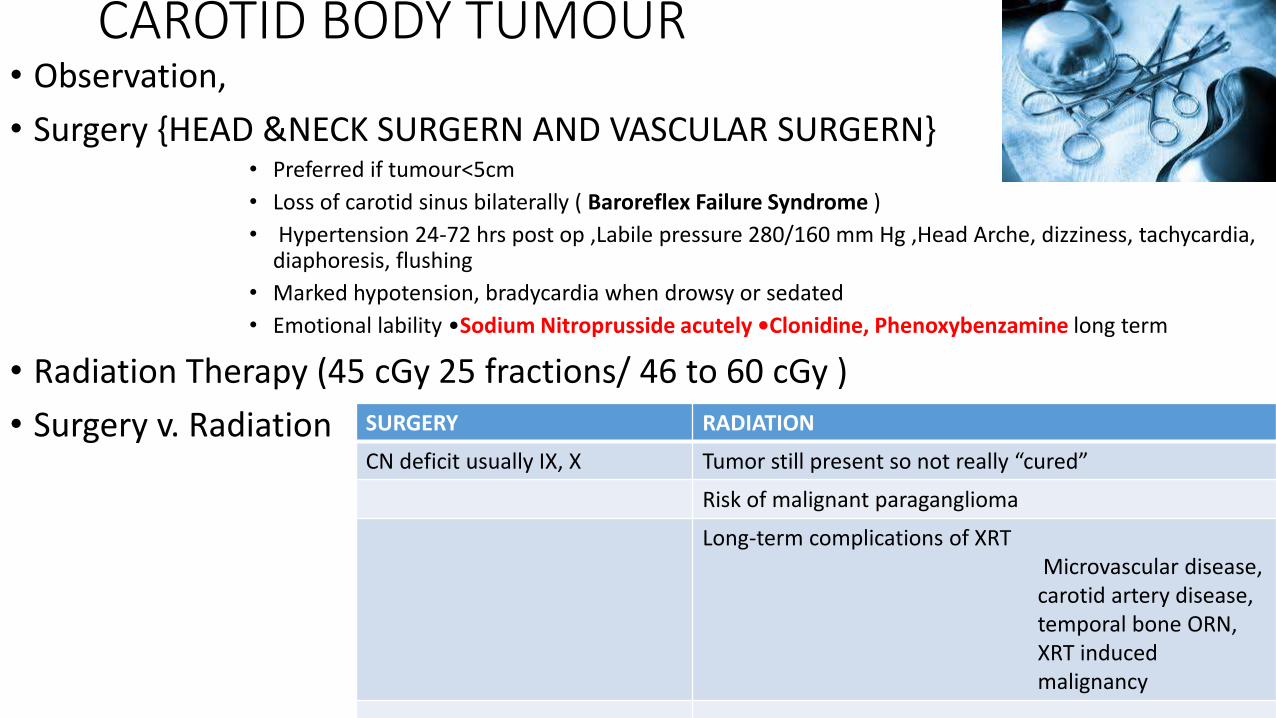
CAROTID BODY TUMOUR • Observation,
• Surgery {HEAD &NECK SURGERN AND VASCULAR SURGERN}• Preferred if tumour<5cm
• Loss of carotid sinus bilaterally ( Baroreflex Failure Syndrome )
• Hypertension 24-72 hrs post op ,Labile pressure 280/160 mm Hg ,Head Arche, dizziness, tachycardia, diaphoresis, flushing
• Marked hypotension, bradycardia when drowsy or sedated
• Emotional lability •Sodium Nitroprusside acutely •Clonidine, Phenoxybenzamine long term
• Radiation Therapy (45 cGy 25 fractions/ 46 to 60 cGy )
• Surgery v. Radiation SURGERY RADIATION
CN deficit usually IX, X Tumor still present so not really “cured”
Risk of malignant paraganglioma
Long-term complications of XRTMicrovascular disease,
carotid artery disease, temporal bone ORN, XRT inducedmalignancy
GLOMUS TUMOUR
• Radiation• effects
• Slows tumour• Temporary ↓size of tumour(last years)• Very little change if any detected in tumour cells themselves• Indication
• Total surgical resection not feasible because of • anatomical extent of tumour• Medical contraindication
• Surgery• Trans canal approach• Trans canal and trans mastoid approach• Trans canal and trans mastoid approach with upper neck dissection• Modified or extended infratemporal fossa approach(± dislocation or resection of
mandible or zygoma (CSF Leak---trapezius/rectus abdominals free flap))

Glomus tumour
• JT paraganglioma-Treatment• Observation
• Lifespan not affected by tumour morbidity or mortality
• Annual imaging
• Radiation : 35 Gy, followed 10 yrs median
• surgery

Vagal Paraganglioma
•Surgery :
• Lateral temporal bone resection • Netterville
• 37/40(patients) CN X sacrifice, • All 40 permanent vocal cord paralysis
• Jackson IX-39%, X-25%, XI-26%, XII-21%
•Radiation :consideration same as for CBP with equal local control

others
• Laryngeal– partial or total laryngectomy
• Nose/paranasal sinuses--- trans nasal excision or lateral rhinotomy

CONCLUSION
• Para ganglomas are rare but important tumours in ENT that require good knowledge of the pathology for effective management

















