1 Chaired by Lord ClementJones CBE The House of Lords 15 th February 2012 In association with the TEAM Partnership Together Everyone Achieves More Maintaining Patient Safety and Preventing Harm
Transcript
1
Chaired by Lord Clement-‐Jones CBE
The House of Lords 15th February 2012
In association with the TEAM Partnership
Together Everyone Achieves More
Maintaining Patient Safety
and Preventing Harm
2
Maintaining Patient Safety and Preventing Harm The House of Lords 15th February 2012
Chaired by Lord Clement-‐Jones CBE
Produced with funding support from the Department of Health
3
Content
Speakers Biographies Page 4
Participants Page 8
Report Of The Seminar, With Interspersed Q&A Sessions
Welcome And Opening Remarks Lord Clement-‐Jones Page 10
Raising The Bar On Patient Safety Maxine Power PhD, MPH National Improvement Advisor & Safe Care National Work Stream Lead, QIPP, Department of Health
Page 11
Hospital-‐Acquired Clots
Professor Beverley Hunt PhD MPH Medical Director, Lifeblood: The Thrombosis Charity; Professor of Thrombosis & Haemostasis, King's College; Consultant, Departments of Haematology, Pathology and Lupus, Guy's & St Thomas' NHS Foundation Trust
Page 16
National Patient Safety Strategy Dr Suzette Woodward Director of Patient Safety, NPSA
Page 22
The Role Of The Community Health Services In Preventing Avoidable Harm
Lynn Young Primary Care Advisor, Royal College of Nursing of the United Kingdom
Page 27
Maintaining Personal Safety After Discharge For SCI People Through Collaborative Care
Paul Harrison Spinal Injuries Association, Sheffield SCI Centre
Page 31
Maintaining The Safety Of Disabled People While In Hospital
Sister Hannah Elizabeth Community of Corpus Christi
Page 34
Patient Falls, The Challenge To Getting The Balance Right
Ruth Liley Assistant Director of Quality Improvement, Marie Curie Cancer Care
Page 36
Final Q & A Session And Closing Remarks Page 39
Appendices
Appendix 1: TEAM: Patient Partnership For Quality Care Page 43
Appendix 2: Paper Submitted On Behalf Of the Spinal Injuries Association Page 44
Appendix 3: Contributions From People Unable To Attend In Person Page 48
4
Speaker Biographies
Maxine Power PhD MPh National Improvement Advisor & QIPP Safe Care National Work Stream Lead, Quality, Innovation, Productivity and Prevention, Department of Health, England
Following a 20 year clinical career as a Speech and Language Therapist) Maxine was awarded a Health Foundation Quality Improvement Fellowship in 2006, spent one year at the Institute for Healthcare
Improvement in Boston, USA and completed a Masters in Public Health at Harvard University. Since her return to the UK Maxine has undertaken three substantive roles leading improvement in organisations and regions. Whilst her initial focus was in the improvement of care for patients following stroke, she now works with healthcare systems wishing to improve patient safety. In January 2010, Maxine was appointed by the Department of Health's Quality Innovation, Productivity and Prevention team (QIPP) as the National Improvement Advisor, in this role she is leading the design and delivery of a national programme for safety improvement and cost reduction. Maxine is also a governor on the Board of the Health Foundation, a UK charity which supports the improvement of healthcare delivery through individuals, programmes, advocacy and research.
Professor Beverley J Hunt FRCP, FRCPath, MD Professor of Thrombosis & Haemostasis, King's College; Consultant, Departments of Haematology, Pathology and Lupus, Guy's & St Thomas' NHS Foundation Trust
Professor Beverley Hunt is Professor of Thrombosis & Haemostasis at King’s College London and is a Consultant in the Departments of Haematology, Pathology and Rheumatology.
She is a Co-‐Founder and Medical Director of the thrombosis charity, ‘Lifeblood: the thrombosis charity’, which was Health Charity of the Year 2010 at the charity awards and “Patient group of 2010” at the Communiqué awards for their work in campaigning for mandated prevention of hospital-‐acquired clots in England.
Beverley is a national and international expert in thrombosis and acquired bleeding disorders. In England, she sits on the National VTE (venous thromboembolism) board where she is co lead of the “Patient awareness and experience” workstream.
5
She also sits on the National VTE prevention clinical advisory group, the NICE Guidelines Development group for the management of VTE and the NICE VTE standards development committee. She sat on the NICE guidelines development group for the prevention of venous thromboembolism in hospitalised patients.
She has huge clinical experience of thrombotic and acquired bleeding disorders and runs a very active research group with over 200 peer-‐reviewed publications to her name and won the BMJ Research paper of the year with the CRASH-‐2 team. Her Thrombosis committee have produced a free award-‐winning, downloadable iphone app containing a multitude of thrombosis guidelines in elegant algorithms:
Dr Suzette Woodward Director of Patient Safety, National Patient Safety Agency
Dr Suzette Woodward is Director of Patient Safety at the National Patient Safety Agency. Suzette is a qualified nurse, training at St Thomas Hospital and Guys Hospital. She specialised in paediatric intensive care. Over the last decade Suzette has led a number of national patient safety programmes; in particular she was Implementation Director for Patient Safety First. She has extensive knowledge of all aspects of patient safety and is the author of over 25 articles, book chapters, blogs, opinion pieces and podcasts. She has an MSc in Clinical Risk and a Professional Doctorate in Patient Safety Implementation. She is currently leading on the design of the national patient safety function of the NHS Commissioning Board
Lynn Young Primary Care Adviser, Royal College of Nursing of the United Kingdom
Lynn has held the post of Primary Healthcare Adviser for the Royal College of Nursing since October 1990. During the last decade the major part of her work has focused on the development of primary healthcare policy and practice within the context of health and social care reform.
This includes the development of PHC organisations, clinical governance, commissioning, nurse leadership in primary and public health, public and patient involvement, the GMS contract 2004, the prevention of coronary heart disease, nutrition and tobacco control.
Sister Hannah Elizabeth Community of Corpus Christi; Disability Equality Trainer, Leonard Cheshire Disability
Sr Hanna Elizabeth is a 66 year old Nun, having been disabled from birth with a rare progressive disease and taken vows in the Single Consecrated Life on 17.11.1995.
Qualified Leonard Cheshire Disability Equality Trainer, writer and Quiet Day leader.
Paul has worked as a Registered Nurse within the speciality of Spinal Cord Injuries since 1987 and has been employed as Clinical Development Officer since 1991 at the Princess Royal Spinal Cord Injuries Centre.
His areas of expertise encompass the lifetime care of SCI people including the pre-‐transfer and post-‐discharge management of SCI patients. He originated and manages the Lifetime Care of Individuals with Spinal Cord Injuries course at Sheffield and coordinator the SCI-‐Link scheme which trains and supports SCI Link-‐Workers in NHS Hospital Trusts.
Paul is a committee member and of the Multidisciplinary Association of Spinal Cord Injury Professionals and an honorary member of the Spinal Injuries Association. He has published several books relating to the management of SCI outside of specialist SCI Centres in collaboration with the Spinal Injuries Association.
More recent work includes, Transforming Community Services, world class commissioning and the provision of primary care services in the light of the demand to separate provider and commissioning functions. Currently Lynn is involved in a number of issues relating to the English Health and Social Care Bill, and in particular the development of the clinical commissioning groups.
The provision of end of life care and the development of the community nursing workforce are also within her work portfolio. In November 2004 Lynn was awarded an Honorary Fellowship Royal College General Practitioners FRCGP (Hons) and has a place on the RSM General Practice Council.
She is a director of Acton Care Centre and the National Heart Forum.
Paul was a member of the NPSA working group that produced the statement on the provision of manual evacuation for people with SCI and also advised within the Department of Health’s National Service Framework for People with Long-‐Term Conditions. Currently he is working as a member of the Information Management Group of the National SCI Strategy Board.
Paul Harrison RGN, ONC, MAEd Clinical Development Officer, Princess Royal Spinal Injuries Centre
Maintaining Patient Safety and Preventing Harm
7
Fully involved in various Church activities; weekly visits to Erlestoke prison, Royal United Hospital, Bath – Chaplaincy – plus remaining ward at local hospital.
Would now like to establish a training agency, for potential support workers.
Ruth Liley Assistant Director of Quality Improvement, Marie Curie Cancer Care
Ruth Liley has worked in Clinical Governance and quality assurance in both the NHS and voluntary sector.
Her current role is as the Assistant Director for Quality Assurance at Marie Curie Cancer Care which provides end of life care to patients through its 9 hospices and nationwide community nursing service.
Key elements include ensuring that all services delivered are compliant with each country’s regulator, standards and legislation.
Ruth has worked at Marie Curie for 7 years and continues to input into key external pieces of work such as the Care Quality Commission Quality risk profiles for the voluntary sector and the National End of Life Care Intelligence Network Quality Markers self assessment tool.
Maintaining Patient Safety and Preventing Harm
8
Participants
Baroness Jolly Baroness Masham Baroness Thornton Abi Flanagan Patient representative, Macmillan Cancer Support Ailsa Brotherton
Programme Director, National Safe Care Team, Quality, Innovation, Productivity and Prevention, Department of Health
Alison Tongue Programme Manager, Safer Care; NHS Institute for Innovation and Improvement
Angela Killip Quality Manager, Sue Ryder Care Anita Maullin Head of Customer Support, Leonard Cheshire Disability Ann Bisbrown Lee HealthWatch Advisory Panel (lay representative) Anna Dyktynska Care Supervisor, Leonard Cheshire Disability Dr Anna McGee Head of Research, Sense Dr Anne Godier Research Fellow, Thrombosis and Vascular Biology Group, Rayne Institute, St
Thomas' Hospital; Service d’Anesthésie Réanimation, Université Paris Descartes, Hôtel Dieu, Paris
Bernard Reed OBE Trustee, GIRES Dr Briony Cutts Haematology Fellow, Guy's & St Thomas' NHS Foundation Trust Catrin Fletcher Director of Operations, Wales, Leonard Cheshire Disability Clare Trott PEM Friends UK Daniel Burden Head of Public Affairs, Spinal Injuries Association Professor David Oliver National Clinical Director for Older People, Department of Health Diane Tolley Patient representative, Coventry Eddie Chan BME Health Forum and Chinese National Healthy Living Centre Elaine Inglesby Executive Nurse Director, Salford Royal NHS Foundation Trust Elizabeth Wright MNC Programme Director, NHS London Graham Tanner Chair, National Concern for Healthcare Infections Gill Stancer Service User Network Association, Leonard Cheshire Disability Helen Bronstein Vice Chair, MRSA Action UK Dr Jackie Morris MB FRCP
British Geriatrics Society Dignity Champion; Honorary Research Associate, Research Department of Primary Care and Population Health, UC London Medical School; Honorary Senior Fellow, School of Community and Health Sciences, City University London
Jane Plumb MBE Chief Executive, Group B Strep Support Jenny Brooks Matron, Infection Prevention and Control; Deputy Director of Infection
Prevention and Control, Milton Keynes Community Health Services Jenny Drew Associate, Safer Care; NHS Institute for Innovation and Improvement Juliette Millard UK Nursing and Health Professions Advisor, Leonard Cheshire Disability Kate Jones Interim Director, Safer Care; NHS Institute for Innovation and Improvement Katherine Fenton Chief Nurse, Professor of Nursing Leadership -‐ London City and London
Southbank Universities; University College London Hospitals NHS Foundation Trust
Kristina Earle Practical support, Leonard Cheshire Disability
Maintaining Patient Safety and Preventing Harm
9
Dr Louise Teare Director of Infection Prevention and Control, Mid Essex Hospital Services NHS Trust
Lyn McIntyre Head of Operations -‐ Quality and Nursing, NHS East of England Mark Platt Policy Advisor, Patient and Public Involvement; RCN Policy and International Dr Martyn Diaper Primary Care Team, NHS Institute for Innovation and Improvement May Li Clinical Governance and Regulatory Manager, Livability Mike Murnane Infectious Diseases and Blood Policy Branch, Department of Health Nadra Ahmed OBE Chairman, National Care Association Poonam Arora Lifeblood advisor and Secretariat to All-‐Party Parliamentary Thrombosis Group Rose Gallagher Nurse Advisor Infection Prevention and Control, Royal College of Nursing Rosemarie Mitchell Managing Director, Operations, Leonard Cheshire Disability Ruth Somerville External Communications Officer, Leonard Cheshire Disability Sally Deacon National Programme Delivery Manager, Harm Free Care, NHS Institute for
Innovation and Improvement Samantha Riley Director of Information for Service Improvement; The Quality Observatory, NHS
South of England Sheila Scott OBE Chief Executive, National Care Association Prof Simon Smail CBE, FRCP, FRCGP, FRSPH, FRSA
Emeritus Professor, Cardiff University and Non-‐Executive Director, Public Health Wales NHS Trust
Stevie Slade RN Nurse Adviser, National IPC Lead Susan Wilson Clinic Secretary Department of Haemostasis and Thrombosis, Guy's & St
Thomas' NHS Foundation Trust Susan Went
Health Foundation Quality Improvement Fellow; Senior Expert In Healthcare Quality Improvement RCP/RCGP/RCPsych
Suzie Hughes Patient and Carer Network, Royal College of Physicians Patient Involvement Unit Terry Reed OBE Trustee, GIRES Vicci Chittenden Service User Network Association, Leonard Cheshire Disability
Maintaining Patient Safety and Preventing Harm
10
Report of the Seminar Welcome and opening remarks Lord Clement-‐Jones CBE Ladies and Gentlemen, it is a delight to welcome you here today. I am very pleased that you have come together as part of the TEAM project -‐ Together Everyone Achieves More. I suspect that many of you will know a great deal about TEAM. This is a two-‐year project funded by the Department of Health’s Third Sector Investment Programme, which funds selective projects in its Innovation, Excellence and Strategic Development work-‐stream. That might sound slightly opaque, but I am sure we will find out a great deal more about it as we go along!
What I find of particular interest today is the fact that this event is very much about the involvement of the third sector – the voluntary sector – and patients in healthcare. Obviously, as we all know the Health and Social Care Bill is a pretty controversial Bill in many aspects. It is being debated more or less as we speak – we are half way through the report stage. But the two pieces which are not particularly controversial are the whole area of the public health and the whole area of the new arrangements for patient involvement. That is great because it means we have some form of consensus going forward on how that should happen.
It is a good start for today that we know that the new arrangements coming down the track have broad public and political acceptance, and I think that we can work into the new arrangements the things we will talk about today. Of course, public involvement arrangements, such as patient forums and community health councils, have had many different structures over the last 15 years. This is very much a plea to this Government and future Governments; I very much hope that we will have some stability in the way that we contribute to healthcare as members of the public. I hope we can achieve a consensus which will last, in order to allow this to develop in an appropriate fashion.
I am going to hand over to Dr Maxine Power, who has an extraordinarily impressive CV and who is now with the Department of Health. I have the advantage of having all the biographies in front of me, which I will follow. Following a 20 year clinical career as a speech and language therapist, Maxine was awarded a Heath Foundation Quality Improvement Fellowship in 2006, spent one year at the Institute for Healthcare Improvement in Boston USA and completed a Masters in Public Health at Harvard University. Since her return to the UK, Maxine has undertaken substantive roles leading improvement in organisations and regions. Currently, she is the National Improvement Advisor and Safe Care National Work Stream Lead, Quality, Innovation, Productivity and Prevention (QIPP), Department of Health. I hope that Maxine will spend just a little bit of time explaining exactly what that means.
Maintaining Patient Safety and Preventing Harm
11
‘Raising the Bar on Patient Safety’ Maxine Power PhD, MPH National Improvement Advisor & Safe Care National Work Stream Lead, QIPP, Department of Health Introduction Thank you very much Lord Clement-‐Jones and thank you to the organisers for inviting me to come and speak. I would like to share the experiences that I have had leading a national programme to improve patient safety as part of QIPP. For those of you who work in the NHS this will be a very familiar acronym. It is being led centrally by the Director General, Jim Easton, and also sponsored by Earl Howe. I want to spend some time bringing to life the piece of work that we have been doing as a coalition. My brief today is to talk about safety policy, which has come out of the QIPP Safe Care programme, to describe what good care looks like and, hopefully, also to identify some challenges on which, working together, we can achieve more.
As Lord Clement-‐Jones said, I have been working in the Department of Health at the centre of Government for the last two years, but still really consider myself to be a student of health policy, especially in respect of patient safety and healthcare. I am really interested in the discussion that we are going to have today, to reflect and learn more from the distinguished audience we have here with us, and to engage in a debate about how that can be improved and moved forward.
Patient Harm In 2007 I was involved in the Patient Safety First Campaign, which was really my first experience of a large-‐ scale change programme in patient safety. That was led by Suzette Woodward, who is sitting here at the Speakers’ Panel. Basically, I learnt an enormous amount. Since then I have been working with about 1,000 NHS frontline healthcare professionals with a team of colleagues from the regions. We have been undertaking a national demonstration project called Safety Express, which aims to deliver higher quality healthcare at lower cost by doing some very specific things – reducing harm from pressure ulcers, falls, urinary tract infection and blood clots. Clearly, we have not been doing that in divine isolation; we have had a coalition of partners who have significant expertise in these areas. What many of you will know and I learnt was that these are very common complications of healthcare that affect at least 200,000 people every year in England alone and cost the taxpayer roughly £400 million a year to treat. In the programme, which started in 2010, one of the first things I learnt was that there is almost an acceptance of these particular harms as complications of care or unavoidable, inevitable consequences of healthcare interventions. Actually, when you talk to people this assumption is not based on any irrational belief; it is based on very logical things, such as, “How could these harms possibly be avoidable if they are
There is a genuine trust between the public and healthcare providers that every effort will be made to
keep them safe from harm.
Maintaining Patient Safety and Preventing Harm
12
happening to so many people?” Furthermore, there is a genuine trust between the public and healthcare providers that every effort will be made to keep them safe from harm. We know now, as we have never known before, that this trust is a very precious gift.
We need transparency in the data, an honest discussion of current performance and partnerships with partners and providers, to move forward and improve together. I have to say, I think this has never been more important than it is now. Over the last decade, through the work of Suzette, Sir Liam Donaldson and many others in this room, we have collected information that we did not have before.
We know that despite the vigilance and hard work from healthcare professionals, every day we have a silent epidemic of harm. This is largely attributable to poorly developed systems in healthcare, not bad people. At the most severe end of the spectrum this results in serious harm or death to over 3,000 patients per year, and I am sure many of the speakers today will refer to that. However, I must stress that this is not a UK-‐specific issue. This is a global challenge. This is something that is happening in every healthcare system across the word – developed and developing.
Preventing Patient Harm Safety Express and the people who have committed to work in it during the pilot stage have, for me, been absolutely inspirational. They are starting a mindset change or a cultural revolution in the NHS. They believe that the prevailing mindset of ‘unavoidable’ is fundamentally flawed and that potentially over 50% of the harms that we have identified in those four areas alone (pressure ulcers, falls, urinary tract infection and blood clots) could be avoided with the collective sharing of ideas and the replication of best practice performance. Their courage and conviction to change this prevailing culture is astonishing; it is gaining momentum because we have had different experiences in the last decades. In 2005 MRSA Bacteraemia was very
common in hospitals. At the hospital where I worked in Salford, there were more than 50 patients a year with a MRSA Bacteraemia and now, in less than five years, the number of patients affected each year is in single figures and continues to reduce year on year, despite our claims that maybe we have reached the minimum that we can achieve. Elaine Inglesby, who was scheduled to be here, has led this work as the Director of Nursing at Salford as part of a large safety
improvement transformation programme to prevent 10,000 harmful events. Basically, leaders like her and many others in this room have shown us that tomorrow’s healthcare will be different from yesterday’s and we can be safe if we work together.
In fact, we know that many organisations in the NHS have gone more than two years without a single Bacteraemia. Last month one hospital in the north of England, Trafford General, who have been in the middle of the eye of the storm, reported 1,000 days since their last MRSA Bacteraemia. Mindsets are changing as a consequence and people are beginning to realise that we can change. If we can change for infection prevention then we can do it in other complications in healthcare.
We know that despite the vigilance and hard work from healthcare professionals, every day we have
a silent epidemic of harm.
Maintaining Patient Safety and Preventing Harm
13
New Ways Of Looking At Complications In the Safety Express programme, we have identified new ways of looking at complications that we believe are pivotal for patients and carers to deliver rapid change programmes. Our lessons have been learnt not simply through scrutiny of healthcare literature, although this has been critical, but predominantly through listening to patients. Our programme involved multi-‐disciplinary teams from across the health economy coming together for three days 90 days apart over an eight-‐month period during 2011 to learn together about improvements they could make and improvements being made by colleagues in the regions. I want to tell you a story about the day that I went to the first of these meetings in London and the South East coast because I think it is relevant to this meeting. We had about 300 people gathered in the room all eager to learn more about the content areas and we had a really impressive schedule of speakers from the Department of Health, the Royal Colleges and local healthcare organisations. The teams were really energised by the meeting and in this session, like in all our other sessions, we asked for teams to bring their patients with them. A small number did, but many did not. As part of the programme of presenters, though, we had asked a gentleman called Stephen Lightbown to come and talk about the experiences he had had with his pressure ulcers. On that day, Stephen came into the room and sat in front of 300 people in his wheelchair and told his story.
Stephen, at the age 17, had a sledging accident which resulted in him having a severe spinal injury. His recovery, whilst bumpy, was peppered with the kinds of story that we hear very commonly – fabulous healthcare, a sense of abandonment at transitions, in particular the transition home, and a young man grappling to understand exactly how to move forward with his life. None of this is uncommon, but the most compelling part of Stephen’s story for me was that he had been asked to talk to the group about his experience of having developed a pressure ulcer on discharge from hospital. He actually started his presentation by saying, “I’m not at risk of one of these. At some point in time and even maybe now I’m at risk of all four of them!”
For me and for many people in that room on that day, there was a dawning realisation that in healthcare we compartmentalise people into risks of falling, risks of skin damage or risks of blood clots. In fact, many of the most vulnerable in society are at risk of all those and some more besides. These harms are biologically interconnected, affecting the same patients and requiring similar interventions. Moreover, we send patients to specialists in these areas who have enormous expertise but who may also prioritise their issue when the person in front of them actually needs and wants to be treated as a whole person.
Pilot Study My job in the programme was to nurture excellence and change momentum. In parallel with the change, it became apparent very quickly that all four of our harms were not simply an issue for hospitals but that we needed to engage with people in the places that they spent time and felt safe – their homes, communities, support services, day centres, nursing and care facilities. We invited people to come and join in teams in localities based on common populations or geographies. We had no idea how difficult this would be. Even
The number of people affected by new pressure ulcers in the pilot had reduced by 42%. If this change could be replicated across all providers then
this could result in 50,000 fewer pressure ulcers each year in England
alone.
Maintaining Patient Safety and Preventing Harm
14
the most proactive organisations create barriers and our teams were constantly trying to break them down for patient benefit, sometimes with success but often not. Despite this, I can report that the pilot produced results that were beyond all current expectations. By September, just eight months after the start and eight months after Stephen had told his story, the number of people affected by new pressure ulcers in the pilot had reduced by 42%. If this change could be replicated across all providers then this could result in 50, 000 pressure ulcers avoided each year. Moreover the number of patients receiving harm free care – the term that we then use to describe patients without any of these harms – had increased by 5%, which may sound like a small percentage but if this could be delivered across England could mean that we had an additional 470,000 patients year on year who travel through our healthcare systems harm free. Safety Thermometer This brings us to our current challenge. From April 2012, the NHS Safety Thermometer, which is the measurement instrument that was developed by teams and measures these harms in any setting across the
health and home care system, has been included in the Operations Framework and is now part of the national CQUIN (Commissioning for Quality and Innovation) profile, which many of you will be familiar with. For others, what that means is collecting information about these harms on patients. Organisations that deliver NHS care will
receive incentivised payments in year one and then in year two will be able to talk to their local Commissioners about setting health economy-‐wide goals for improvement that are meaningful and relevant to patients. It is clear that there is much to be worked through. Community and third sector organisations are struggling to understand how this act of measurement could be useful. How can this be more than just a box checking exercise? We have started to work with them by saying, “It’s not counting; it’s caring”.
I want to finish today by sharing a story with you. We have asked all district nursing services to use the NHS Safety Thermometer on one day a month for the patients they see on that day as a test. In NHS London we are working with nurses to test this, and there are many people in this room who have experience in this too. On the first day we went to a local community service and received a fairly frosty but open-‐minded reception. There was one experienced nurse, Linda, who, unconvinced that this instrument was of any use whatsoever, agreed reluctantly to test it on a patient she was seeing that day. She went to see her first patient of the day, a lady called Brenda, 76, with limited mobility, who she had seen every month for six months following a referral from a GP for a treatment of leg ulcers. The ulcers were healing nicely and this would probably be the last visit. She really could not see the point in asking this lady about her pressure ulcers; it just did not seem relevant. As instructed in the Thermometer, though, she got out her checklist and asked about areas of reddening on her shoulders, back and ankles. To her surprise, Brenda said that she had been a little bit uncomfortable in bed because of her lower back. Linda asked her
It’s not counting; it’s caring!
Maintaining Patient Safety and Preventing Harm
15
to lie on her bed so she could inspect her skin more closely and what she found was a grade four pressure ulcer, a lesion which exposed the bone of the coccyx and which was in serious danger of becoming infected.
Linda came back and told her story to the rest of the team. Their response was typical, because healthcare professionals are there to heal: “This isn’t counting; this is caring”. My question to you is how can we do this together? We have set the policy; we have the instruments; we have evidence on the website. How can we get a national campaign together to engage patients to protect Stephen, Brenda and the 200,000 others just like them to deliver harm-‐free care from pressure ulcers, falls, catheters and blood clots to the 500,000 people who deserve that every year?
Short Question and Answer Session
Graham Tanner (Chair, National Concern for Healthcare Infections) I am Chair of the National Concern for Healthcare Infections, but I am also a WHO Patient for Patient Safety Champion, which was brought forward some time ago by Sir Liam Donaldson. Thank you, Maxine, for an excellent presentation. The MRSA Bacteraemia have gone down, but the point is that other infections have increased and become more severe. That is the problem. You mentioned pressure ulcers. I did a little bit of work on this about two years ago and communicated that to the then Secretary of State. A grade four pressure ulcer is already infected. As you are probably aware, the total cost of an infected ulcer in terms of money is around £10,000 to £10,500. If you include the community, we spend somewhere in the region of £4 billion on dealing with ulcers of some description. We have looked at the hospital situation; there was a very good thing that came out of South Wales, where they put a clock at the end of the bed so that they would turn the patient and move the patient every two hours. You are absolutely right that what we have not done is to look at the community situation and to look at what can be done within the community. If we look to the future of the NHS, that is where things lie.
We have a population that is rapidly ageing, with an extra three million people over 65 by this time next year. Hospitals are running out of hospital beds; therefore, we need to move more care into the community, and that involves the third sector. The only thing that can actually be done is to move some of these people out and deliver community care, but that needs investment. It needs investment in the nursing teams and in training for community nurses. It needs people within third sector organisations to be able to disseminate information to the patients that they represent. There is a lot that can be done, but the lack of investment actually counters that.
Dr Maxine Power I concur. You make your point really well, Graham, and I could not agree more. We need to move beyond this simply being NHS professionals in acute care settings doing this work. These are system issues and there are population issues. Similarly, there is an element that we really need to tackle as a leadership community, and that is this notion of blame, because that tends to get in the way of improvement. If I spend all my time figuring out whether this happened here because of something I did, albeit a legitimate thing to scrutinise, that then makes the change process quite difficult. Therefore, it is absolutely critical to make sure that not only do we get patients to be cared for closer to home, but that the accountability lies with the community and the population rather than an individual organisation being penalised.
Maintaining Patient Safety and Preventing Harm
16
Lord Clement-‐Jones Great, and we may be talking more about that later on. Now let us move on to our second speaker, which is Professor Beverley Hunt. She is the Professor of Thrombosis and Haemostasis at King’s College and a consultant at the Department of Haematology, Pathology and Lupus at Guy’s and St Thomas’ NHS Foundation Trust. She is a co-‐founder and medical director of the thrombosis charity, Lifeblood, which was awarded Health Charity of the Year 2010 at the Charity Awards and Patient Group of 2010 at the Communiqué Awards, for their work in campaigning for mandated prevention of hospital-‐acquired clots in England. As you have gathered from that, Beverley is a national and international expert in thrombosis and acquired bleeding disorders. Professor Hunt’s throat is not in fantastic shape today, so as an auxiliary Poonam Arora will be supporting her in her capacity as advisor to Professor Hunt’s charity, Lifeblood, and as secretariat to the All-‐Party Parliamentary Thrombosis Group. Take it away!
‘Hospital-‐Acquired Costs’ Professor Beverley Hunt PhD MPH Medical Director, Lifeblood: The Thrombosis Charity; Professor of Thrombosis & Haemostasis, King's College; Consultant, Departments of Haematology, Pathology and Lupus, Guy's & St Thomas' NHS Foundation Trust Introduction I will talk a little bit about hospital-‐acquired clots and what they are, talk about Lifeblood’s story, what is happening in NHS England and some of the devolved regions, where we are with national policy and what we think ought to happen next.
What Is A Blood Clot? A clot in the deep veins of your leg is known as a deep vein thrombosis or DVT. I know that the general public is very aware of DVT; they associate it with long-‐haul flights. What we are trying to do through the charity is increase awareness of the fact that it is actually very unusual to have a DVT after a flight, but it is very common to have one after hospital admission. The trouble with having a clot in your leg is that, as it grows, bits of it can break off and move to block the blood supply to the lungs. If it is a really big clot, ‘that’s it’ – sadly, it can be fatal! If it is a slightly smaller one you might have chest pain and shortness of breath. Estimates And Facts People die from blood clots. We do not know the total number of
We know that about 25,000 of the 32,000 deaths due to hospital-‐ acquired clots can be prevented
Maintaining Patient Safety and Preventing Harm
17
people who die from them, because it is very much under-‐diagnosed. Dying of a pulmonary embolism, which is the bit that has broken off and blocks the blood supply to the lungs, is very similar to dying of a heart attack. We think that quite often a death certificate will say ‘heart attack’ when they mean pulmonary embolism. We know from lots of international studies that there probably are an estimated 60,000 deaths due to blood clots in the UK and we know that of all those deaths two-‐thirds are due to being in hospital, very few are due to traveller’s thrombosis. If we do not risk-‐assess patients for their risk of hospital acquired clots on admission, and provide those patients identified as being at risk with the appropriate preventative treatment (thromboprophylaxis), then we would be in trouble. Thromboprophylaxis includes injections of blood thinners, stockings and pneumatic compression. We know that about 25,000 of the 32,000 deaths due to hospital-‐acquired clots can be prevented. Hospital-‐Acquired Clots A hospital-‐acquired clot is a clot that happens within 90 days of discharge or during admission. I have to say that most of the clots happen after discharge. What we do know is that there are about 17,000 deaths every
year registered to pulmonary embolism, and that studies from autopsies would suggest that for every death where a doctor says, “Oh, I think this patient died of a pulmonary embolism” there are another two cases where they thought, “Oh, they’ve died of something else” and then the post-‐mortem has shown that they died of a pulmonary embolism. What are the symptoms? Well they are few most of the time; it is a silent disease. Most individuals have a little bit of pain in the leg – and that is about it for 80% of them. People can die of a pulmonary
embolism with no warning at all: about 50% of people who die with a pulmonary embolism just drop dead. We call them hospital-‐acquired clots because although 10% of hospital deaths are due to pulmonary embolism, in actual fact most of these clots happen after discharge. At St Thomas’ Hospital we turn around our patients very fast, so they can be in, after a hip replacement, for three to five days. The average DVT shows up from day 7 after an operation – when patients are at home. The average pulmonary embolism shows up on day 22 – three weeks later. If you present with a bit of chest pain and shortness of breath, quite often you will get treated with antibiotics because the doctor thinks you might have an infection, and the diagnosis gets forgotten.
Let’s just talk about how it can impact on life. This is the story of a Deputy Head Teacher, who is 45. She unfortunately had an ankle fracture and she went up to Accident and Emergency; she got strapped up and put in plaster, and sent home. She was given little or no advice about aftercare. Two weeks later she was readmitted, absolutely gasping for breath, through the same A&E with a pulmonary embolism. She was taken to coronary care and luckily she had clot busters and she survived. Then, because she is a highly intelligent woman, she started to look at why this had happened and she said, “Since having the pulmonary
The problem with hospital-‐acquired clots is that they are silent. 80% of
DVTs do not show up at all and do not have any leg swelling or redness as
they show in the textbooks.
Maintaining Patient Safety and Preventing Harm
18
embolism I have discovered that it is surprisingly common, and the fracture clinic advice is either contradictory or virtually non-‐existent”.
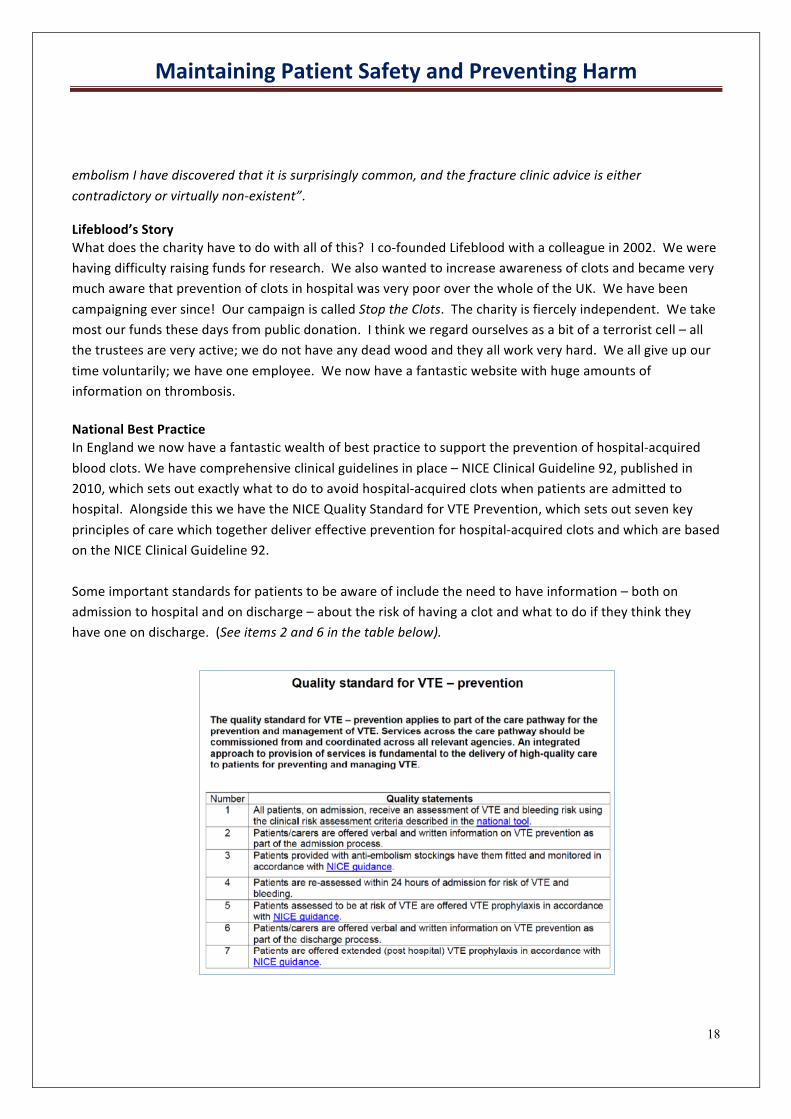
Lifeblood’s Story What does the charity have to do with all of this? I co-‐founded Lifeblood with a colleague in 2002. We were having difficulty raising funds for research. We also wanted to increase awareness of clots and became very much aware that prevention of clots in hospital was very poor over the whole of the UK. We have been campaigning ever since! Our campaign is called Stop the Clots. The charity is fiercely independent. We take most our funds these days from public donation. I think we regard ourselves as a bit of a terrorist cell – all the trustees are very active; we do not have any dead wood and they all work very hard. We all give up our time voluntarily; we have one employee. We now have a fantastic website with huge amounts of information on thrombosis. National Best Practice In England we now have a fantastic wealth of best practice to support the prevention of hospital-‐acquired blood clots. We have comprehensive clinical guidelines in place – NICE Clinical Guideline 92, published in 2010, which sets out exactly what to do to avoid hospital-‐acquired clots when patients are admitted to hospital. Alongside this we have the NICE Quality Standard for VTE Prevention, which sets out seven key principles of care which together deliver effective prevention for hospital-‐acquired clots and which are based on the NICE Clinical Guideline 92. Some important standards for patients to be aware of include the need to have information – both on admission to hospital and on discharge – about the risk of having a clot and what to do if they think they have one on discharge. (See items 2 and 6 in the table below).
Maintaining Patient Safety and Preventing Harm
19
In addition, patients should be aware that, if you have stockings fitted, they need to be fitted properly by somebody who is trained. You should not end up, as you used to, seeing people on the wards who are wearing anti-‐embolic stockings, half of which are around their ankles, like Nora Batty!
At this point, Professor Hunt lost her voice and asked Poonam Arora from the All-‐Party Parliamentary Thrombosis Group to speak on her behalf.
National Policy: Overview It has been recognised globally that the UK is in a leading position through supporting the prevention of hospital-‐acquired clots in national policy. The issue has been termed the National Clinical Priority for the NHS for the past two years, in recognition of the number of preventable deaths that occur every year in England and following a concerted lobbying campaign led by Lifeblood, fellow health professionals and the All-‐Party Parliamentary Thrombosis Group. There are a number of policy levers in place to try to incentivise quality care for blood clot prevention. I will not go into too much detail about what these individual levers are, but I will aim to provide a picture of what patients should expect when they are admitted to hospital, and how well people are complying within the healthcare service with each of these goals. CQUIN (Commissioning for Quality and Innovation) The CQUIN goal has been touched on already by Maxine when she talked about the introduction of a financial incentive – a national CQUIN goal – to report in line with the Safety Thermometer, which includes the need to report whether blood clot prevention measures have been administered to patients in order for hospital to receive some CQUIN money. In addition to this, CQUIN money can be provided to Trusts if they can demonstrate that they have risk-‐assessed 90% of patients on admission to hospital. This financial incentive has worked wonders in improving the number of patients who are risk-‐assessed for their risk of developing a hospital-‐acquired clot. Two years ago when first introduced, about 40% of patients were being risk-‐assessed, but by the end of 2011, 90% of all NHS patients were risk-‐assessed for hospital acquired clots on admission to hospital. This is great news for patient safety. NHS Standard Contract We also have the NHS Standard Contract, which is an agreed contract between commissioners (currently PCTs) and Hospital Trusts. This requires every single Trust to provide a monthly report on the number of patients who receive appropriate prophylaxis once they have been assessed as being at risk of a blood clot. Then for every hospital-‐acquired clot that has been confirmed, there has to be a root cause analysis looking back into the patient’s notes. This covers whether or not they have received a risk-‐assessment, whether they received the appropriate prophylactic treatment and whether it was an avoidable blood clot or not. Risk Management Standards The NHS Risk Management Standards are used by the NHS Litigation Authority (NHSLA) to assess Hospital Trusts’ activity in reducing risk and improving their standards. Performance against these Standards affects the insurance premium that Hospital Trusts pay – essentially, acting as a ‘stick’ whereas the CQUIN goal acts like a ‘carrot’. VTE prevention policies are included within these Standards.
It has been recognised globally that the UK is in a leading position through supporting the prevention of hospital-‐
acquired clots in national policy.
Maintaining Patient Safety and Preventing Harm
20
All-‐Party Parliamentary Thrombosis Group Annual Audit The All-‐Party Parliamentary Thrombosis Group carries out annual audits of every single Hospital Trust, assessing their VTE prevention policies as a while. The Group found that hospitals have tended to focus very much on the financial incentive that comes with the CQUIN goal, since of all the policy levers addressed above, this is the one which has really had an impact on the ground. The next challenge is to ensure that patients, once assessed as being at risk of hospital acquired clots in line with the CQUIN goal for VTE, then go on to receive the appropriate prophylactic treatment as outlined in NICE Clinical Guideline 92 and the NICE Quality Standard for VTE Prevention. What does Lifeblood do? We run a public awareness campaign, especially around National Thrombosis Week (May 28th). Lifeblood's most recent campaigns have centred around the shockingly high number of deaths caused by VTE in the under 40s, which amount to over one thousand in the last 4 years. When the under 50s are taken into the equation the numbers rise frighteningly higher to almost three thousand.
Also in the spotlight are the escalating costs of litigation in this avoidable area of harm. Blood cost failings cost the NHS £112m in 2010.
Maintaining Patient Safety and Preventing Harm
21
We run political and policy campaigns aiming to improve professional education as well as have VTE prioritised in the NHS, with the right outcomes being measured.
Conclusion from Professor Beverley Hunt Our campaign to Stop the Clots is a very good example of how charities, working with health professionals and politicians can improve patient safety. You have heard about all the different ways we have tried to embed the culture of prevention in England in healthcare. Now if you are a health professional, whichever way you turn there is a penalty to pay or some demand to risk-‐assess the patient to ensure they receive appropriate thromboprophylaxis. We hope very much that the rate of death due to pulmonary embolism will start to go down. Thank you very much. Lord Clement-‐Jones Beverley and Poonam, thank you very much for that very concise but hugely informative presentation. Now for somebody who really is in the ‘hot seat’. Dr Suzette Woodward is Director of Patient Safety with the National Patient Safety Agency. Suzette is a qualified nurse, having trained at St Thomas’ Hospital and Guy’s Hospital. She specialised in paediatric intensive care. Over the last decade, Suzette has led a number of national patient safety programmes; in particular, she was Implementation Director for Patient Safety First. She has extensive knowledge of all aspects of patient safety and is the author of over 25 articles, books, chapters, blogs, opinion pieces and podcasts, so we will hear a fraction of that, I am sure, today, Suzette. Thank you.
Maintaining Patient Safety and Preventing Harm
22
‘National Patient Safety Strategy’ Dr Suzette Woodward Director of Patient Safety, NPSA Introduction Thank you very much. I have thoroughly enjoyed the speakers so far but I am going to lift us a little to the slightly higher zone -‐ quality and strategy. I wanted to remind everyone of just what we mean by quality and safety. I bet you, if you asked every single person in this room what quality and safety meant, we would probably have at least 25 different definitions. What we currently use, and will continue to use, is the definition defined by Lord Darzi, which is that quality is about patient safety, patient experience and effectiveness. It is important that we remember those three things because, too often, people refer to quality and forget that that means those different components.
Effectiveness is very much about providing the right treatment and doing the right things, but safety is about doing those right things right. You can have effective care but it can be unsafe; you can also have unsafe care that is potentially effective, in a rather strange way. What the NPSA has done is raised a massive amount of awareness of patient safety over the last 10 years. It was very much the baby of Sir Liam Donaldson, as has been mentioned. One of the things that we have struggled to do, which is highlighted, in a way, by some of these talks, is to understand exactly how safe the system is now and after various interventions. Data on safety is really poor, as is compliance against initiatives, interventions and NICE guidance etc, as you have alluded to, and I want to explore that a little in terms of ‘why?’
Seven Steps to Patient Safety: Creating the Right Culture We can describe safety as ‘a body of individual actions’. We call them the Seven Steps to Patient Safety. We suggest that the foundation of everything is about creating the right culture – Maxine alluded to that – which is open, fair and just. What we mean by ‘just’ is that there is a right response to harm and error, which is of improvement and learning, rather than seeking to blame. There is absolutely no problem in accountability and responsibility for patient safety and, of course, if individuals are found not to be competent, that needs to be addressed. In the main, however, as many people say, people do not tend to come to work to do harm, but to care. We know that, and what we need to do is ensure that people, when things go wrong, have felt that they are treated proportionately in accordance with the error or the harm that has occurred. Creating the safety culture, then, is the platform for everything that you need to do. Clearly Demonstrable Leadership Then you absolutely have to have clearly demonstrable leadership. I can walk into a Trust that has a Chief Executive who both ‘gets’ patient safety and leads it from the top. I can sense and feel the difference from a Trust that does not. Board leadership is crucial but another key component is the importance of that
Quality is about patient safety, patient experience and effectiveness.
Effectiveness is very much about providing the right treatment and doing the right things.
Safety is about doing those right things right.
Maintaining Patient Safety and Preventing Harm
23
leadership all the way down the organisation. What we find is that, sometimes, the voice at the top is not heard at the bottom and that there is a middle-‐messaging that gets mixed up. It turns something very positive into something potentially negative. What I mean by that is that you could have a Board approach that is,”Yes, we want our staff to be open. We want to talk to our patients about when things have gone wrong”. But, halfway down the organisation, it turns into something like a target. We need to think about how we embed the safety culture all the way through an organisation. That is certainly something that the public inquiry into the Mid Staffordshire NHS Trust will be picking out: the role of leaders throughout and the crucial role that matrons and ward sisters play in the safety of the care provided.
Interaction And Integration Of Safety Systems Our third step is all about interaction and integration of all safety systems. What I want to say at this point is that that should be incredibly broader than just simply an organisation. The national system needs to think about how it integrates and brings together all of the aspects of safety into one system. That is one thing that I will be talking about in relation to the way forward. Monitoring Information The fourth step is to monitor your information. You are creating a safety culture, you have your leaders on board and they are saying that this is a really fantastically important thing. You are integrating all your knowledge and your systems around complaints, claims, incident reporting, audits and walkabouts etc, and then you need to monitor that patient safety information. What is it telling you? Not how many, not the numbers -‐ we are not interested in 300 of this and 200 of that -‐ but in what it is telling you about your organisation. How many of the same things are happening time and time again? How many things are going from small to really bad? How many things are you stopping going to really bad? How many things are you preventing? Monitoring patient safety information, then, is a really important step. Creating A Culture Of Openness And Transparency With Patients And The Public The fifth step is about creating a culture of being open and transparent with your patients and the wider public. Being open and transparent is very important in general, but very much in terms of openness with patients. When something has gone wrong, patients have an absolute right to know that that thing has gone wrong. If the patient has died, the relatives, carers or loved ones of that patient absolutely must know what has gone wrong. Somebody has to say sorry and somebody has to explain what has gone wrong, and then tell them what they are going to do about it. That has to be done as soon as possible. It is a highly skilled thing to do. I have done that myself. I have stood up in front of the parents of a child who has died in an organisation I was working at, and had to explain that their child died as a result of something that happened in the hospital and not because of the child’s disease or illness. It is incredibly hard to do but it is something that is vital and that needs to be taught and trained. We run training programmes on what we call ‘being open’ to help people do that.
We need to think about how we embed the safety culture all the way
through an organisation.
Maintaining Patient Safety and Preventing Harm
24
Identifying Contributory And Causal Factors To Harm The sixth step is about identifying contributory and causal factors to harm. You are gathering your information and integrating it, and you are talking to your patients and learning about these things. But the crucial thing is that you need to learn from those things and identify the contributory and causal factors, if at all possible. All too often we think that we have addressed the problem by sending out an edict to staff to say, “It would be brilliant if you did not do x” or we might change a policy document and say, “Please read this policy document, because that will make you safer”. That just skims the surface of safety. What we are talking about is redesigning systems and processes to make them safer and to design out the possibilities for error and harm. Using Knowledge And Evidence To Create Interventions To Improve The Safety Of Patient Care The seventh step to safety is using this knowledge and evidence base to create interventions, such as that which Maxine has been doing, which is an incredibly impressive programme. This is to improve the safety of patient care. So you have gone all the way through, from creating a safety culture to solutions. There are numerous ways in which you can create a safety culture, but fundamentally you need people to speak out. You need the ability to prevent something bad from happening, the ability to prevent something bad from becoming worse, and the ability to recover from something bad, once it has happened. Learnings: Preoccupation With Failure One of the things that we find is that good organisations have a preoccupation with failure. They expect
things to fail so they start looking at their systems to see if they can address failure. Therefore, they start to have early warning systems set up to pick those up, and we know that the NHS is not great at doing that. The other thing around integrating all of your systems is to make sure that you use them as a way of learning as opposed to blaming.
Reporting And Learning From Incidents Our National Reporting and Learning System at the centre is going to continue to operate. That is a key message if people are worried about what is happening to the NPSA. In fact, the Secretary of State has asked for that system to be reviewed over the next year and a half to two years to see if we could create a single system for aligning all patient-‐safety incident-‐reporting on one system. This is in order to reduce the burden on the NHS in terms of reporting and to enable learning from the different pieces of information. We have more than a million incidents reported a year, so we have a good reporting culture in acute care, in the main. However, there is a poor reporting culture in primary care and GP practices, in that one in 300 of our patients is seriously harmed by the care that they receive. That is a significant amount. Around 69% of these incidents result in no harm, for example a patient being given double the dose of paracetamol, which, while it is an incident, is not judged to be harmful. Twenty-‐four percent result in low harm but 6% result in moderate harm, and 5,000 cases, or 1%, result in death or severe harm, every quarter. Every three months, 5,000 people are severely harmed, for which the definition is permanently harmed for life, or they die.
Every three months, 5,000 people are severely harmed, for which the
definition is permanently harmed for life, or they die.
Maintaining Patient Safety and Preventing Harm
25
It is, then, exceptionally important that we start to learn about these things and to use the examples that Maxine and others have used to drive home the message of harm-‐free care. Why is it acceptable that one in 10 people is harmed? Why is it acceptable that I could sit in a GP surgery looking at 10 people and wonder which one is going to be harmed? It is not acceptable! It is also not acceptable in terms of compliance with initiatives, which I will come on to.
Contributory Factors Contributory factors have already been alluded to around patient safety, but the interesting thing about them is that they are not really hard to identify or address, because they are things that are quite simple: Patient identification; for example, wrong patient identification or the wrong identification of a limb. In
theatre that can mean that the person’s wrong leg is removed. Everyone always talks about communication and then they put it to one side as if it is too hard to do.
Poor communication and a poor handover of a patient could mean that, for example, a person who is allergic to penicillin will receive penicillin during that shift.
Lost or missing test results can lead to patients not being followed up at times when urgent care is needed.
Medication can cause significant harm in terms of wrong doses – overdoses and underdoses – and wrong routes etc.
Failure to observe patients may lead to them deteriorating. The Challenge My message here is that we know where the problems and the harms are, and we know what to do to address them, because there is a massive body of evidence. Our challenge is not the ‘what’ and ‘the evidence’, but the ‘how’ and ‘the implementation’. Our challenge is the massively difficult art of implementation. Many people say to us, “Tell us what to do, but do not tell us what to do”. What they mean by that is that they want direction but they do not want you to tell them to do it, which is a complex issue to deal with at a national level. There is also a big myth that telling people what to do creates long-‐term change. There is a lot of demotivation around change, as has been evident over the last year or so. There are two million research papers – where do you start and where do you prioritise? There are numerous things that come out from agencies like ours – which ones do you listen to? This is another thing around the opportunities of the future in terms of integrating these different initiatives. We suggest a blended change strategy with: A combination of top-‐down and bottom-‐up initiatives. The use of social movement methodology plus pragmatic approaches driving a lot of this change. Creating frameworks for people to adapt the national approaches locally. Measuring your baseline, measure constantly over time and then use that for improvement.
My message here is that we know where the problems and the harms are, and we know what to do to address them, because there is a
massive body of evidence.
Maintaining Patient Safety and Preventing Harm
26
Lessons Learned The lessons that we have learned over the last 10 years are numerous, and there are lots of documents to show that. Organisation for impact is incredibly crucial. You cannot just say, “It would be really nice if you could do
x”; you have to organise around a cause or a passion. Increased reporting is a really good indicator of a good safety culture, but you need to start
understanding what is happening in those reports and to learn from similar things all of the time. You need to be open with your patients. You also need to be very positive with both staff and patients to provide some level of hope. Talking
about how bad it is all the time is really hard to hear. You need to say, “This is bad, but bad plus all of these interventions can mean good”. Provide some hope for people!
Reward and celebrate all of the good practice that is going on in the NHS and show people that it can and does work well.
What Is Happening? The NPSA was set to be abolished in the arm’s-‐length body review that came out on 26 July 2010. Since then, the NPSA has been split up and disaggregated from its different systems: The Clinical Assessment Service is going to be a self-‐funding organisation but is currently being hosted by
NICE. The Research Ethics Service has become part of the Healthcare Research Authority. Confidential Inquiries has moved to the Healthcare Quality Improvement Partnership (HQIP). The Central Alerting System has moved to the Medicines and Healthcare products Regulatory Agency
(MHRA). What is left behind is the patient safety function, which is the one that I lead and which was the original NPSA in 2001. That is divided into two. One is the National Reporting and Learning System – this database is connected to every single organisation in the NHS, whatever care setting it may be. There is a group of people whom you might describe loosely as ‘patient safety experts’ who develop advice, guidance and solutions etc. The National Reporting and Learning System is going to be hosted and run by the Imperial College Healthcare NHS Trust on behalf of the NHS Commissioning Board. These are the current proposals, subject to the Health and Social Care Bill.
The patient safety function of the NPSA is proposed to be transferred to the NHS Commissioning Board, to sit within the Nursing Directorate of the NHS Commissioning Board and alongside Patient Experience and Nursing. It will be integrated with the Medical Directorate of the NHS Commissioning Board, which deals with the effectiveness side of the quality agenda
Increased reporting is a really good indicator of a good safety culture, but you need to start understanding what is happening in those reports and to learn from similar things all of the
time.
Maintaining Patient Safety and Preventing Harm
27
There are, however, some opportunities with that, because currently the NPSA sits a little to one side. Sometimes it is heard and sometimes it is not; sometimes it is listened to and sometimes it is not! It has had areas in which it could have done better: it could have improved safety in primary care; it could have improved information-‐gathering from GP practices; and it could have been embedded across the system so that safety was not just one organisation’s piece of work. Shifting the functions of safety to the NHS Commissioning Board will, therefore, enable it to just do that. It will enable it to start creating all of these linkages all the way from standard setting to commissioning, and from regulation to improvement. Good safety culture is one where it’s part of everybody’s practice and everyday practice, and not that of an organisation or of the Director of Patient Safety. It has to be embedded so that it is not dependent on a few or on a single champion, and so that it retains the same intensity, regardless of personnel turnover, reconfigurations and reorganisations.
Lord Clement-‐Jones Suzette, thank you very much for that strategic and practical approach. We now come to Lynn Young, the Primary Care Advisor for the Royal College of Nursing. She has held that post since October 1990 and has seen a few healthcare reform bills! During the last decade, the major part of her work has focused on the development of primary healthcare policy and practice within the context of health and social reform. This includes the development of primary healthcare organisations, clinical governance, commissioning, nurse leadership in primary and public health, public and patient involvement, the General Medical Services contract of 2004, the prevention of coronary heart disease, and nutrition and tobacco control. I will not go on, but she is also a director of Action Care Centre and the National Heart Forum.
‘The Role of the Community Health Services in Preventing Avoidable Harm’ Lynn Young Primary Care Advisor, Royal College of Nursing of the United Kingdom Introduction Thank you for the opportunity to come and talk to you today. I am very reflective at the moment because I have worked for 21 years at the Royal College of Nursing and had a wonderful time, but am about to leave. So, it is easy for me to be reflective in terms of what has been going in the community during the last 20 years. The last time I was a nurse in a hospital was 1972, so I am jolly old! It is therefore a good time for me to honestly look back at the lessons I have learned, so forgive me if emotion takes over and I stray away from the policy side but focus instead on what happens to people’s lives. This is how it is when you move from the hospital to the community.
Good safety culture is one where it’s part of everybody’s practice and everyday practice, and not that of an organisation or of the Director of Patient Safety.
Maintaining Patient Safety and Preventing Harm
28
Experience In The Community All my experience of the last 30 years is that of the community, which is different from that of working in the hospital and this can often be quite humbling. On my first day out with the district nurse, it was almost shocking to me to see how ill people could be at home; that people die at home and that profoundly disabled people can live quite well at home. In 1948 Nye Bevan said that the NHS is, sadly, obsessed with hospitals, so it is high time that we moved on and make efforts to build a culture of patient safety within the
whole of the community. Every round of reforms brings another opportunity and I think, “Here comes another one! Maybe this time, we will have more attention paid to the community and what happens to people’s lives, rather than their particular diseases”. My mother is 93 and has never spent a night in hospital. She and her family hope that she is going to die without having to go into hospital -‐ so far we are managing jolly well, thank you. Obsession With Patient Safety
Looking back, there are people who I have heard and I remember what they said, as if it was yesterday. It was some years ago when Professor Aidan Halligan, who was then Assistant Chief Medical Officer, gave a talk. He stood there, speaking with his lovely Irish accent and declared, “Of course, wherever we are working in health and social care, we all -‐ whether it is the cleaner or the consultant -‐ have to be absolutely obsessed with patient safety”. It is an obsession! I have also learned over the years that policies can often mean very little. Sorry, Maxine, I am not being disrespectful, but it is the people who do the work and it is the work that matters. We do not go around with our policies attached to our chests; we take ourselves to work. It is who we are that matters most. Safety depends on what level of care we give. Of course, I could not leave this afternoon without mentioning Florence Nightingale who said, “The hospital shall do the patient no harm”. Another quote which is rarely heard is, “Every visitor to a hospital (patient) is an honoured guest”. I rather like that and it would be quite something if all people who looked after patients were reminded of it.
Complex Needs I come from a very different perspective from my colleagues here today, but there is some overlap of what has been said, which is quite comforting. Many people living in our communities have a very diverse range of highly complex needs. Of course, Maxine, you mentioned Stephen. I love the story of Stephen as he was so challenging in terms of his health and wellbeing and also in terms of providing health and social care services. I do not know any more details about Stephen and what kind of life he now has, but there are all kinds of challenges within his story. Linda might have been quite a mature district nurse, but she had the humility to be prepared to learn, which is attractive. We have an obsession with quality, and Suzette mentioned this. It is about the Holy Grail of quality. Quality is different things to different people. We keep seeking it and, when we feel it, we know it and we have that wonderful experience of what high quality care brings to us. I have come up with five themes which underpin quality, and they focus on the big picture, rather than the confines of the hospital building.
Wherever we are working in health and social care, we all -‐ whether it is the cleaner or the consultant -‐ have to be absolutely obsessed with patient
safety”.
Maintaining Patient Safety and Preventing Harm
29
The Community Nursing Workforce Above and beyond absolutely everything, patient safety relies upon the quality of the workforce. Of course, I am utterly attached and devoted to the community nursing workforce, which I have laboured so hard to make as good as it can be, but I have to admit to this audience that I have spectacularly failed! In the last decade, the number of district nurses has reduced from 14,000 to 9,500. The future is not looking good for district nursing. I wish I knew more on the tricks one needs to learn; how do you get your message heard? I have shouted, screamed, written, lobbied and campaigned. Sadly there has been little appetite in the last 10 years to invest in the district nursing workforce. If you want a safe community, if you want to prevent hospital admission, if you want to enable people to get out of that sometimes rather dangerous hospital as quickly as they can -‐ to maybe their rather dirty but actually quite safe home -‐ we have to significantly invest in the community nursing workforce. At a time when we need more skills, knowledge, expertise and competence in the community, these essential attributes are rapidly on the decline. The community needs urgent and remedial action.
Quality Of The Interface Maxine mentioned that Stephen suffered during the transition from one setting to another. The problem is that health and social care are fragmented into a number of bits and pieces. For the safety of many of our patients and community citizens, we have to bring all the different parts together. This does not have to be one organisation, but patients certainly need the people working within the different parts to have very trustful, honest and open relationships. We need connectedness between the different parts. Social care, the hospital, the community and general practice have very different priorities, perspectives and cultures, and yet, for our communities to be safe we must work sublimely well together. Think of a garden patio: if it has cracks between the slabs we fall through them. The cracks trip us up. Patients are harmed when, even if everybody does their bit right, they fall through the cracks, or rather the lack of interface and have to be helped. Quality Of The Integration My mantra is ‘integration, integration, integration’. All health and social reform should lead to a better pathway and supreme integration. This is not a new ambition. Florence Nightingale urged district nurses to work more closely with the workforce of the parish council. She was a wise woman and there is much to learn from her teachings. That tricky transition from one setting to another goes hopelessly wrong far too often, and patients are damaged as a result. I have been so lucky and met some fantastic people in my auspicious career: some interesting, clever people who have been absolutely driven to make things just a little better. One of those people was the Australian Professor Arthur Brownlow; anthropologist, sociologist and economist. He travelled the world trying to help different parts of organisations work better together. We need many more Arthur Brownlows to help us all -‐ nurses, doctors, therapists and social care people -‐ to come together and work in a much more cohesive way.
Social care, the hospital, the community and general practice have very different priorities, perspectives
and cultures, and yet, for our communities to be safe we must work
sublimely well together.
Maintaining Patient Safety and Preventing Harm
30
Patients who are profoundly ill or who have complex disabilities have to flow through the system. They do not want doors jammed up against them as they go from one setting to another; they need to flow like streams. Information has to flow rapidly. In these days of such fabulous technology, why are we not doing better? We really have a long way to go. The safe flow of information helps to promote fabulous integrated care.
Quality Of The Incentives Some of our incentives in the system are absolutely perverse and wrong. We fund hospitals for doing more. There is absolutely no incentive in place for a Foundation Trust to do what is required to help build a more resilient, healthy community. Foundation Trusts should be passionately driven to play their part in helping to build healthy communities. Of course hospitals are important. While my heart lies in the community I still acknowledge the nation’s need for safe hospitals. They are very much the centre of the community, but there needs to be far better collaboration so that, between the hospitals and community based services we are well placed to build healthier communities. If Mr Lansley was sitting here, I would suggest to him that, “He needs to look once more at the current incentives as they are not going to work”. Suzette mentioned the importance of good management. Healthcare needs the best, most talented, high-‐quality management. I grieve for my community nurses who, because of constant health reform, have a change of management almost every two years. Such change brings instability. It puts the work environment into chaos and causes high-‐level anxiety. Managers are just beginning to find their feet, they are looking after and nurturing their staff, only for someone to say, “Hey, let’s reorganise”. Off they go and in come a new group of people, which fails to enhance quality and patient safety.
Leadership, Leadership, Leadership We need to bottle leadership! It is like manna from heaven. Everybody calls for high-‐level clinical leadership, but where do we get it? If we find it, what do we do with it? How do we make it contagious? We need to nurture our leaders as being a leader can be lonely, especially when the times get tough. The tougher the times get the higher quality and the more talented your leadership has to be, if patient safety is to flourish.
Political Will The quality of the politics of the day matters. Without the political will, it is really difficult to get the good and the right things achieved. The carers As a district nurse, what stunned me during my early days was the heroism, the capacity, the capability and the sheer tenacity and resilience of our carers. We have millions of informal carers and, if it was not for them our patients who require nursing and care in the community would be very fragile indeed. Our formal services need to be absolutely committed to doing all they can to work with and make lives easier for carers. I do not know how they do it but they work 24/7, seven days a work, with very poor financial remuneration.
As a district nurse, what stunned me during my early days was the
heroism, the capacity, the capability and the sheer tenacity and resilience
of our carers.
Maintaining Patient Safety and Preventing Harm
31
They carry on simply because they are devoted to the people they love and care for, but carers need our support. We are moving into a very different time. Graham Tanner talked about the increasing number of older people, and that we will need more carers. We should be talking about how the system -‐ hospital, community, general practice and social care-‐ is going to support our willing carers.
I was surprised to learn how quickly carers were willing to learn. They could do anything that I could do. Carers simply needed to be taught and supported. They are fantastic people and must not be forgotten. I was turned on to carers by Baroness Jill Pitkeathley in the early 1990s, who really did some fabulous work for carers, and her legacy must continue.
My final advertisement is for the Royal College of Nursing. I am holding up our Principles of Nursing. http://www.rcn.org.uk/development/practice/principles/the_principles. We have principles from (a) through to (h) and if every single one of those principles were embedded throughout the system, no harm would be done to our patients, regardless of where they are being cared for. Thank you very much. Lord Clement-‐Jones Lynn, thank you very much for that extremely useful community perspective. Now we come to some short presentations from speakers from the third sector. Starting with Paul Harrison; he has worked as a registered nurse within the speciality of spinal cord injuries since 1987 and has been employed as Clinical Development Officer since 1991 at the Princess Royal Spinal Injuries Centre. His areas of expertise encompass the lifetime care of spinal cord injury people, including the pre-‐transfer and post-‐discharge management of spinal cord injury patients. He originated and manages the Lifetime Care of Individuals with Spinal Cord Injuries course at Sheffield and co-‐ordinates the SCI-‐LINK scheme, which trains and supports SCI-‐LINK workers in NHS hospital trusts.
‘Maintaining personal safety after discharge for SCI people through collaborative care’ Paul Harrison Spinal Injuries Association, Sheffield SCI Centre Introduction I am appreciative that this is a very short verbal presentation – and we have a lot to say! (A full paper on behalf of the Spinal Injuries Association is included in Appendix 2). There is a lot of information for people to look at on the Spinal Injuries Association website and also, for professionals, on the Multidisciplinary Association of Spinal Cord Injury Professionals (MASCIP) website.
We have millions of informal carers and, if it was not for them our
patients who require nursing and care in the community would be very
fragile. indeed.
Maintaining Patient Safety and Preventing Harm
32
I want to talk about spinal cord injuries and their management both in hospital and the community. This is a low-‐incidence but high-‐impact service within the NHS and qualifies as a ‘specialised service’. The NHS calls it a ‘specialised service’ because it has to be organised. However, within the modern NHS, everything that you have heard today can be applied to spinal cord injuries. We too need co-‐ordination. We need investment and we need a recognition that complex care does not always fit into the mainstream planning and provision of the NHS. We need alternative ways of thinking and we need people to recognise their limitations which exist, and can act on them.
The spinal cord injury service is currently being organised into a national care pathway that will provide, in the near future, a spinal cord injury service which extends from the point of diagnosis to the end of life. Spinal cord injury is a disability that does not change. There is a low incidence of cure, but a growing investment in research that is searching to improve survivability and quality of life. It happens and you are left to live with it for the rest of your life. But it is a stable and predictable disability with a growing longevity of survival after diagnosis.
Avoidable Harms In People With Spinal Cord Injury The avoidable harms that we have been talking about today are related to people with spinal cord injuries. The commonest cause of death after spinal cord injury in its early years was urinary tract infection and infected pressure ulcers. The commonest cause of death today, in a well managed care pathway, is cardiovascular disease. The second commonest cause of death is cancer. This means that, by putting in place a strategy that supports people with spinal cord injuries, we can ‘norm’ these people against the complications of the normal population, not against their disability. Death following spinal cord injury is expected to be as a result of old age or lifestyle choices.
However, the wheels have come off the wagon! The incidence of pressure ulcers within the spinal cord injuries population is now increasing, due to a lack of awareness. The incidence of urinary tract infections in people with spinal cord injuries is soaring, because of a lack of appreciation of the specialist condition within the guidelines. I will make a representation on the basis that, from what Dr Woodward said, we do not go around telling people what to do, but
how they are to do it within the restraints and the remit of their care.
When we talk about pressure ulcers, we talk about turning patients. However, an acute spinal cord injury patient needs five people to turn them. The ward has four staff because the ward is staffed for the prevalent patients, conditions and services, and a spinal cord injury is something that is a very rare event. Some hospitals may see only two or three spinal cord injury patients a year, yet they have to have a plan to increase their staffing. They need awareness that you can turn somebody with a spinal cord injury safely. There is only a 1% incidence of somebody with a spinal injury transforming into a spinal cord injury because of inappropriate moving and handling, but there is a 30% incidence of grade III pressure ulcers occurring in the acute period before that person transfers to a spinal cord injury centre.
The incidence of pressure ulcers within the spinal cord injuries population is now increasing, due to a lack of
awareness.
Maintaining Patient Safety and Preventing Harm
33
People with spinal cord injuries use catheters. There are a lot of people who live with catheters. These are long-‐term catheters. The NHS Guidance on how you manage catheters against urinary tract infection is based on research for short-‐term catheters. The presence of a catheter is seen as a pariah; it is something to be avoided. When you do not have somebody who is fully informed about the two care pathways, a short-‐term catheter is something that should be avoided wherever possible. It should be removed as soon as possible. When somebody’s option for continence management is a long-‐term catheter, however, it must be supported, it must be understood, and it must be managed in accordance with a plan of care, which, for a spinal cord injured person, is supervised by a consultant urologist.
When you have a consultant urologist and his team prescribing care in collaboration with a patient to give them a quality of life that they desire, but they are challenged by a district nurse or a community nurse continence advisor, we are not working together; we are working in opposition. One of the frustrations of being a professional in spinal cord injuries is that, every time a change comes around, my workload goes up. I have wins and successes but then I see them all disappear! We heard the one word ‘sustainability’. So often we experience the needs of the minority specialised conditions being overlooked within quality initiatives being targeted for the greater service population. Do not let the baby get thrown out with the bathwater!
Working Together There are topics within the presentations today that are contained in the paper (Appendix 2) on which I will highlight how we can work together. In spinal cord injuries, I wish to extend the list that Dr Woodward provided from four to six. In spinal cord injuries, we have two additional concerns. One is a condition called autonomic dysreflexia and another is bowel management requiring digital interventions. Bowel Care The Spinal Injuries Association and the NPSA worked in 2004 to provide guidelines for the appropriate use of digital bowel procedures in people with spinal cord injuries, but it is not working. We have guidance but we have no enforcement. We have no audit and we have nobody going around asking, “Is this happening?” We are saying that it is not. Every time we discharge a patient, we are faced with the fact that someone says, “We cannot do that”. You can do it – it is legitimate, appropriate and well documented in the literature. Most hospital and community trusts have policies and personnel to support this technique. But every time we discharge somebody, we have to go through the process of justifying this particular form of bowel care, even after it has been agreed with the people in authority that it is a legitimate and appropriate process.
Another aspect of bowel care is that this is seen as something that can be done only by a registered nurse. I can reduce the work of district nurses if we have an investment in personal carers. There are numerous registered nurses ‘running themselves ragged’ trying to provide a service in the community that can be provided competently by personal carers. Those carers are present and can be trained. For the person with a spinal cord injury, bowel care is something that enables.
We can reduce the work of district nurses if we have an investment in
personal carers.
Maintaining Patient Safety and Preventing Harm
34
We have people with spinal cord injuries who could go to work, but they cannot because they are waiting at home for the convenience of a community nurse to come in and undertake bowel care. We have the expert in Lynn Young. She says the poor district nurse has to prioritise her work, and her priority is people with diabetes. By the time you find the time to get around to your spinal cord injury patient, it is about 11 o’clock in the morning. I cannot find anybody who can find an employer who will give them a job that regularly starts at 12 o’clock! If bowel management was provided by a service that provided bowel care at a time appropriate to the work schedule of the person with spinal cord injury we could have more of them returning to work or full-‐time education.
Autonomic dysreflexia If bladder and bowel care is not done properly, it can lead to autonomic dysreflexia. The catheter must be changed routinely, and the right size of catheter used. We use wide-‐bore indwelling catheters because the paralysed bladder produces more sediment. We do not use size 12 Foley gauge, but size 16 as a standard. It is proper and in accordance with the research. It does not harm the patient. A size 12 catheter blocks about every two days, which is a huge avoidable expense in care and equipment.
We have to make people understand that autonomic dysreflexia kills. The reason why I have chosen autonomic dysreflexia as an example is because the people that it most affects are those with higher lesions of spinal cord injury. The commonest level of lesion in new patients is a C5 – the fifth cervical vertebra – creating tetraplegics. Seventy percent of our current population is at risk of autonomic dysreflexia and it is still not understood outside of the specialist centres. When the new centre in Middlesbrough was being commissioned, they surveyed every A&E department in the North-‐East, yet not one knew what autonomic dysreflexia was or how it is treated. Every patient’s community care plan says: “If you get the symptoms, take yourself to A&E”. No: you have to find a plan where you can manage yourself at home. In order for the patient to receive prompt and appropriate attention in A&E or following a 999 call, organisations such as The Spinal Injuries Association, working with the NPSA, need to produce an information card, like a passport which prompts action, rather than bemusement.
We cannot go around and educate every health professional as much as we desire to, but we can enable somebody to present themselves with legitimate documentation that says, “I have this problem and this is how I want you to manage it”. As I said before, I am not giving you a policy but a piece of paper that says, “This is from the NHS; this
is my problem and this is what I need you to do with it”. They can do everything that we are asking them to: the request is, “I want you to change my catheter”. The response comes back; “I cannot change your catheter. It increases the risk of infection”. Then we have to say, “No, I want you to change my catheter because I am presenting with these symptoms and the longer you delay, the more likely they are to kill me”.
Lord Clement-‐Jones
Thank you very much indeed. That was quite a moving testimony. Now to Sister Hannah Elizabeth, who has been disabled from birth with a rare progressive disease. In 1995, she took her vows in the single consecrated life. She is qualified Leonard Cheshire Disability Equality trainer, writer and quiet daily leader.
We have to have people who understand that autonomic
dysreflexia kills.
Maintaining Patient Safety and Preventing Harm
35
She is fully involved in various church activities, weekly visits to Erlestoke Prison, Royal United Hospital Bath and a ward at her local hospital. She now, I gather, would like to establish a training agency for potential support workers.
‘Maintaining the safety of disabled people while in hospital’ Sister Hannah Elizabeth Community of Corpus Christi Introduction Starting when I was five, I have had over 60 hospital admissions. Many changes have taken place during that time, including diet, and not all for the best! I have a very rare progressive disease called Charcot Marie Tooth type II, involving most symptoms, including paralysed vocal cords causing intense breathing problems. At this point, due to the difficulty of hearing Sister Hannah, she asked that her assistant Kristina Earle read her prepared text on her behalf. Drawbacks Of Hospital Facilities For People With Disabilities I have been told, “You will be fine. Hospitals are geared for disabled people”. I dispute that. On my recent admission to intensive care, I was told there was no accessible toilet. As with other wards, where bedside lockers include a lockable section for patients’ drugs, here is another example of a huge loss of independence. Being in control of one’s medication is not allowed on admission and is frequently queried and/or changed during the duration of admission. This can lead to various complications and/or discomfort. At home, I have been prescribed a children’s weight mattress. My weight is currently three stone 12 lb. In hospital, all mattresses seem to be of the same nature, that is, more suited to heavy men -‐ no offence intended to gentlemen present! After my recent hospitalisation, I returned home with three new pressure ulcers, which had not been noticed by my medical staff. These continue to be extremely painful and continue to require twice-‐weekly dressing.
A very scary experience concerns patients who are admitted for seemingly unrelated problems and end up being tube-‐fed -‐ a very real sense of being out of control -‐ when the real problem is anorexia, an imprisoning condition. On the subject of food and drink, it is not uncommon for such basic items to be placed out of reach.
On a personal level, I dread the appearance of the PATSLIDE, which is excruciatingly painful. This is a patient transfer board, a device for transferring patients between bed and a trolley, for example.
What is the problem and possible solution? The problem, as I see it, is a severe lack of communication and basic training for all involved in the medical profession. Attitude and understanding are vitally important to get right. There must be many service users willing and able to assist in such a learning experience.
After my recent hospitalisation, I returned home with three new
pressure ulcers, which had not been noticed by my medical staff. These continue to be extremely painful and continue to require twice-‐weekly
dressing.
Maintaining Patient Safety and Preventing Harm
36
Lord Clement-‐Jones Thank you very much indeed. Now, as our final speaker from third sector organisations on the Panel, we have Ruth Liley, Assistant Director of Quality Improvement at Marie Curie Cancer Care. Ruth has worked in clinical governance and quality assurance in both the NHS and the voluntary sector. Marie Curie Cancer Care provides end-‐of-‐life care to patients through its nine hospices and nationwide community nursing service. Key elements include ensuring that all services delivered are compliant with each country’s regulator, standards and legislation.
‘Patient Falls, the challenge to getting the balance right’ Ruth Liley Assistant Director of Quality Improvement, Marie Curie Cancer Care Introduction Thank you very much indeed, and thank you for the invitation to come and speak today. I am going to be focusing on patient falls and the challenge of getting the balance right. As you have just heard, we provide end-‐of-‐life care through our hospices and community nursing services. We have five hospices in England, two in Scotland, one in Wales and one in Northern Ireland, giving us the dubious pleasure of working under six healthcare regulators, and trying to meet all of their standards and requirements is quite a challenge! In addition to that, we have the nursing service, which covers 95% of the population of England. It is provided by over 2,000 nurses and healthcare assistants throughout the country. We are registered both as a nursing care agency and a domiciliary care agency, again with two different sets of standards for each country, and you can imagine how complicated that can become.
The Scale Of Care Provided Last year Marie Curie Cancer Care spent £39 million on community nursing, £36 million on hospice care and £5 million on research and development. We are part-‐funded by the NHS, so probably about 50% of our
national spend is matched by the NHS -‐ although not for research and development, I have to say. We have over 6,500 regular volunteers who help us deliver what we do, and that number is far exceeded by volunteers who dip in and out of the organisation at particular times of the year. For example, we have thousands of people helping us out around the Great Daffodil Appeal. We could not do what we do without any of them. I wanted to raise that to acknowledge what our volunteers do for us.
Data Capture For Driving Safer Care As a regulated care provider, we need to ensure that we have robust clinical governance systems in place. As part of that, we make sure, just as the NHS does, that we capture data on any incidents that happen, including patient falls. We collect this information on a central database for analysis every quarter. We look at the themes and trends of the incidents and we use that to improve the services we provide. Falls
Every year, every hospice and every nursing region takes part in the
annual audit and we look at working practices and the way in which we
are improving patient care.
Maintaining Patient Safety and Preventing Harm
37
prevention and management form part of our annual clinical audit programme. Every year, every hospice and every nursing region takes part in the annual audit and we look at working practices and the way in which we are improving patient care.
We have a multidisciplinary approach to patient care within the hospices and the community. We had a small working group that included physiotherapists, occupational therapists, doctors, nurses and others to develop our falls assessment toolkit. That forms the basis of our falls prevention and management strategy, and that is what is audited every year -‐ and has been for the last three years. What that year-‐on-‐year analysis has shown us is that we have a very defined patient caseload. All our patients are very frail, often elderly, with complex medical problems and on multiple medications. They are prone to falling: they are often dizzy, weak and very frail. We risk-‐assess every single patient, and what the audit showed us every year was that 80% of our patients were at high risk of falling. We knew that we could count the incidents, fill in forms and assess that 80% of patients were at high risk. Our medical lead at the time of that audit asked why we kept on measuring and getting the same thing, instead of spending more time on planning how to make that safer! It seems logical now; at the time, we were going through the process of understanding what our audits were showing us.
Balancing Risk And Quality of Life We assumed that people would fall, given their high risk. Now we to try to reduce the impact of that risk on them as much as possible. The balance for us, however, is that we try to let every patient live as well as they can, for as long as they can, as independently as they want to be. We could put every patient into a bed and say, “If you stay there, you will be perfectly safe. No one will ever have a fall again and our numbers will be zero”. Our trustees and our boards do not want that. We want patients to be independent. We have physiotherapists and occupational therapists running rehabilitation programmes in our in-‐hospice gymnasiums to try to get people active and moving.
With that sort of culture, trying to let people be independent and as good as it can be, for as long as they can, we accept that some patients will have a fall. You cannot reduce these things to zero, but this comes down to patient quality of life and choice. If the patient’s choice is to be up and independent, we will help them to do that. One of the things we warned our trustees about was this: “This is what the patients are telling us they want to be able to do” versus “Do you want to get down to zero falls?” It is a balance and getting down to zero is never going to happen in fact. We have to ask our trustees, “Do you accept that we are helping patients live the life they want to live?” That is the judgment that has to be made.
Investing For Safe Care We have invested in specially designed falls rooms as we are rebuilding some of our hospices. For those patients who we know are at high risk, and for whom the impact of a fall could be extreme, we put them into a ‘falls risk room’. There they have a low-‐rise bed; the floor space is completely clear, everything is wall-‐mounted as far as possible and they are within eye-‐line of the nurses’ station. We try to minimise the impact, should a fall occur, while still allowing patients their independence, privacy and dignity. These rooms may be more expensive, you could argue, but I think they are very worthwhile.
We try to minimise the impact, should a fall occur, while still allowing
patients their independence, privacy and dignity.
Maintaining Patient Safety and Preventing Harm
38
The gymnasiums at the hospices are remarkable. We have drop-‐in gym sessions for patients, who will have gone from being quite poorly to building up their strength and improving. You see patients walking along the corridor, and you have a tendency to want to walk behind them in order to protect them! But they want to be independent, so that is what we let them be. One of the rooms that gets lots of use in the hospices is the gym. One could argue that gyms are expensive, but they are very worthwhile.
Within the hospices, the environment is relatively controlled by us. We work with patients to give them the care that they want in that environment. Our new builds are superb. We still have challenges in some of our older buildings that are not as ideal. Sometimes it is very difficult to see the patients at all times. This is reflected in the shift to single rooms that we now have. We have tried, where we can, to provide patients with single rooms with en suite bathrooms, and even to give them guest beds if they want their relatives to stay with them.
What that does mean, however, is that you cannot have nurses sitting at a nursing station keeping an eye on the patients. They will often have their door shut. If they have their family with them, they want some privacy, and quite rightly. What it means is that our nurses and doctors have to get up and go around and see them much more regularly. It is a different culture, mindset and way of working. You do not sit and wait to be called; you get up and see the patients regularly and routinely.
We try to make the rooms within the hospices a ‘home from home’. For some patients, it is going to be the last room they are in, so we do not want too many clinical things around. We try to make it homely, but that produces more challenges, because a homely environment is not always the best anti-‐falls environment. Again, the balance has to be made.
Challenges Some patients are determined to get up and be independent. Some do it by choice; others because they are
confused. We have an increasing elderly population, as we have heard. We have more patients with dementia. It is not always easy to say to somebody, “Do not move without ringing your bell first” if, five minutes later, they have forgotten what you have told them. Those sorts of challenges are increasing. In any care environment -‐ be it in NHS hospitals, care homes or within our hospices -‐ the change in the nature of the patients we treat will give us extra challenges in the future.
One of the bigger things that we have to deal with is patient care in the patient’s home. We cannot control the environment that a patient lives in, and nor should we even try. We try to provide the best care with advice and multidisciplinary support to make their care as safe as possible. In a patient’s own home, which is often where a patient wants to be, we have to rely on external agencies providing the equipment that those patients require.
I will give you an example: one of our hospices works within a six-‐PCT catchment area, which was quite enlightening when I visited it recently. If a patient comes from one particular PCT and wants to be
In any care environment -‐ be it in NHS hospitals, care homes or within our hospices -‐ the change in the nature of the patients we treat will give us extra challenges in the future.
Maintaining Patient Safety and Preventing Harm
39
discharged, getting equipment can happen really easily and quickly in a really slick process. For a patient from the same hospice being discharged to a different PCT, it is like ‘pulling teeth’ to get the basic equipment to help the patient get home safely, quickly and effectively. That is one hospice. If you multiply that across the country, you can see the challenges that some of our staff face and the inequity of the service that they receive. Most patients want to have the ability to go home at some point. Fifty percent of our patients are discharged because they have come for symptom care rather than end-‐of-‐life care, but those challenges shape the care plan that we can provide to our patients. It is not always within our remit to control this.
Patient Choice Ultimately, we need to remember patient choice in all of this. We can have guidelines, procedures, policy and clinical judgment, but the patients will determine what they want and we will do our very best to try to deliver that for their end-‐of-‐life care. It does, however, mean that you make balanced judgments with the patient for the care that they want to have. It is not always necessarily going to reduce our statistics to zero, but hopefully we are giving people what they need at a time that is very important to them.
Question and Answer Session
Lord Clement-‐Jones We have had a fascinating, high-‐speed run-‐through of the issues in this seminar. We have looked at specific areas of patient safety in relation to falls, urinary tract infection, clots and ulcers. We have also considered strategy in secondary care, in primary care and in the community. We have investigated some of the issues in terms of leadership, culture, integration and the use of carers in terms of working together with all the different disciplines. It has been quite a journey! I am sure that there are people in the audience who would like to have some input here. We will take a few questions before asking our Panel to respond. Questions raised: Dr Louise Teare (Director of Infection Prevention and Control, Mid Essex Hospital Services NHS Trust) I am a consultant and Director of Infection Prevention and Control in a district general hospital, and also chairman of the Hand Hygiene Alliance. Thank you to all speakers for excellent talks. Organisational culture and leadership were key concepts identified by several speakers. One of the ways in which we have captured these concepts in my organisation is by engaging our board -‐ both executive directors and non-‐executive directors -‐ and senior doctors and nurses in safety ward rounds. All aspects of patient safety -‐ everything that has been mentioned today -‐ are included. Increasingly, we are trying to get very clear standards expected, with follow-‐up and gap analysis in terms of where things go wrong. This is very much in terms of the blame-‐free culture and celebration of good practice.
Maintaining Patient Safety and Preventing Harm
40
Professor Simon Smail (Emeritus Professor, Cardiff University, and Non-‐Executive Director, Public Health Wales NHS Trust) I am a trustee of Leonard Cheshire Disability, where I chair the Quality and Compliance Committee, which is a board sub-‐committee for quality. I am also an Emeritus Professor of Medical Education. My question is quite specific and is for Professor Hunt, but it does cover the interests both of the secondary-‐care community and the primary-‐care community. It is about DVT prevalence and incidence in situations within the community outside the hospital, where the risks are likely to be higher. You very clearly described the very high level of incidence of DVT and pulmonary embolism within the hospital community, but the last time I looked at the literature around care homes and care homes with nursing, it seemed to be very unclear what the situation was in these locations. Yet you would think that the risks are likely to be really quite high. This leads us into a difficult area as to what we do in terms of policy and guidelines for prevention of DVT and pulmonary embolism within those kinds of situation within the community. Here we are, at the moment, trying to promote community care for people who might otherwise have been in hospital, and a lot of people who, in similar kinds of situations as them, might be in hospital. I would be very interested in your comment there. I suspect that the literature is not going to be terribly helpful.
Dr Jackie Morris (Dignity Champion, British Geriatrics Society) Thank you for introducing what I was going to say! I am very interested in patient safety in care homes generally. There are nearly 500,000 people in care homes at present. A significant number of studies, although some of them are old, show that about a third of people die within the first few months of arriving in a care home. What are the policies for people in care homes for pressure sores, thrombosis, falls, medication and bowel and bladder care? These are essential challenges that people in care homes face. What are we doing about them, or what do you want to do about them in the future? Lady Masham What is going to happen when the NPSA disappears? We are very concerned about it. We who are working on the Health Bill are concerned about fragmentation. Reponses: Lynn Young Dr Teare, congratulations for involving people from the board to the ward. This is absolutely the right approach! It feels as though your hospital is trying to do the right thing. But what is the relationship between your hospital and the rest of the community? Are the wonderful things that you are trying to do reaching out to other parts of your community? I would then give you 10 out of 10! Lord Clement-‐Jones I am going to ask Suzette to deal with Sue Masham’s question specifically, although I thought you gave us some rather good news at the end of what you said. There is no need to be pessimistic about this, Sue!
Maintaining Patient Safety and Preventing Harm
41
Dr Suzette Woodward Probably the part of the NPSA that you are most interested in is the patient safety element. What is happening at the moment is that I have about 40 staff, 20 of whom lead on the National Reporting and Learning System. That is going to be run by the Imperial College Healthcare Trust, to capture all the incidents in the same way that it always has. It is going to run it for two years. In parallel, it is proposed that the NHS Commissioning Board will take on nearly 40 staff in order to create the patient safety function of the NHS Commissioning Board. This will lead on the NHS Outcomes Framework Domain 5 aspects and on aggregating all that information from the National Reporting and Learning System with all other patient safety sources. They will turn the information into learning, alerts, advice, guidance and solutions through the Improvement Department of the NHS Commissioning Board. Lord Clement-‐Jones I sense that the care home issue is quite a big one for people, so I am going to ask Beverley first of all to kick off on this, and then we will spread it out among the panel. Professor Beverley Hunt It is very simple: there is no data on DVT and pulmonary embolism in care homes, so we do not know if people are developing DVTs in this setting. We do not know if stockings might be harmful or useful. We do not know if low doses of anticoagulation would be harmful or useful. I would suggest that, until we get data, there is a serious risk that we could do harm, because stockings in people who have strokes do harm and low doses of anticoagulants cause people to bleed. Until we know what the risk-‐benefit analysis is, we need to wait for some data, and I would encourage you to do some research. Paul Harrison We have done some research into care homes for people with spinal cord injuries. The trigger for it came when I did a mortality study and we found that somebody who lived with a spinal cord injury for 10 years in their own home lasted six months in a nursing home before they died. The commonest form of death was an infected pressure ulcer. The problem with a pressure ulcer – and with respiratory infections too – is not the care home’s fault, but rather the fact that there is no provision in the care home to support them afterwards. Our biggest problem was that, when a care home took on complex care for spinal cord injuries, we had to invest an awful lot of our time in preparing that care home to take those cases. And then we had to keep going back in to maintain that level of knowledge and understanding. We have changed tack. We are now trying to work with the PCTs to identify singular care homes acceptable to the family in terms of travel distance. The family always want the care home closest to where they are. This means we then have to cover every care home in the counties. Some patients say, “I want to go into a care home because I am struggling at home”. It is a voluntary decision, not a forced one. “I have looked at the care homes and I have found a really nice one. I have gone there and talked to them about my condition and they understand it. They even have a couple of other people with a spinal cord injury”. The problem is funding. We can very quickly identify at discharge care homes that can look after a complex spinal cord injury, but the charges are above what the PCT funds.
Maintaining Patient Safety and Preventing Harm
42
Dr Maxine Power I completely agree that we absolutely have to protect our patients in care homes and work with care homes. In the Safety Express programme, we had an organisation that worked with us in eight care homes to look at whether the change programmes that we were trying to work through in NHS healthcare settings were applicable and relevant to them. One of the things that we learned was that it was really helpful for us to measure together. Again, I am back to this issue of measurement. Interestingly, I talked about the NHS Safety Thermometer, which measures the four areas that we talked about today, being part of the NHS Operations Board commitment. For the first time, they will be looking at data from the NHS Safety Thermometer at the Operations Board, once it starts to come out. Organisations are being incentivised to collect information, and care homes that provide NHS-‐funded care will also have those incentives available to them. For the first time, there is something of a level playing field, where we can start to look at pressure ulcers, falls and catheters etc in care homes, and get data. My guess is that, over the next two years, the data that is required for clinical care, but also potentially could be used for research purposes, will be there. It is up to us to do something about it. Dr Suzette Woodward In terms of the seven steps that I alluded to, there is a Seven Steps for Primary Care. It was specifically written for the community. The principles for patient safety apply everywhere, and you do not have to think about acute care or acute provision to apply those key principles. I urge you to have a look at the Seven Steps to Patient Safety on the NPSA website http://www.nrls.npsa.nhs.uk/resources/collections/seven-‐steps-‐to-‐patient-‐safety/.
Lynn Young I am rapidly putting on my care home director hat! We must return to the workforce and remember that you only enter a care home because you need nursing. Funding is a huge issue and is likely to become more difficult. Care homes need to provide the very best, most excellent nursing care and this can be difficult to achieve. Some areas, such as London have an enormous recruitment problem, but it is probably far less severe than in Hull. The reality of good staffing can be a tough order. Our care home has been awarded the Gold Standard Framework for end-‐of-‐life care, which is a fabulous achievement. It just shows that we are, within our home, able to provide exemplary nursing. If a care home can provide excellent end-‐of-‐life care, the nursing skills are there for other domains of care. So, look for the Gold Standard Framework -‐ it is a quality marker. But the recruitment of the very best of nursing is the challenge. Ruth Liley I think it is down to respecting patients’ choices and wishes, and making sure we give the best possible care to let them live as well as they can, for as long as they can. Paul Harrison We have not mentioned the Expert Patients Programme (http://www.nhs.uk/conditions/Expert-‐patients-‐programme-‐/Pages/Introduction.aspx). This needs to be put in, because care homes do appreciate people who can inform their care. SIA hopes that this is also a service that can be provided by their evolving Community Peer Support Service.
Maintaining Patient Safety and Preventing Harm
43
Lord Clement-‐Jones We have, at a canter, accomplished an awful lot this afternoon. We have had some great contributors and it has been a fascinating afternoon. Thank you very much to all our panel. I am sure that this debate will continue and, clearly, a huge amount of work is being done. We must be grateful to everybody in each of their different ways for all that they are doing. Thank you very much indeed to everybody who has come along today, contributed and asked questions.
Maintaining Patient Safety and Preventing Harm
44
Appendix 1
Patient Partnership for Quality Care The goal of the TEAM project is to enhance the influence of third sector organisations on health care services in England. A proposal outlining some activities and materials designed to achieve this goal was submitted to the Department of Health by the charity Leonard Cheshire Disability, supported by twelve partner third sector organisations. They were successful in gaining a grant under the Voluntary Sector Investment Programme Innovation, Excellence and Strategic Development Fund 2012–13, which will run for up to two years.
TEAM aims to extend links with many other groups; the current target is 150 third sector organisations. People across the diversity of the population will be included, paying particular attention to the different equality strands. Over the next two years, participating voluntary sector organisations will hopefully work together to help each other to empower and motivate patients and the public to participate more actively and effectively in healthcare. The project will focus on four areas:
o Healthcare-‐associated infections o Patient safety o Patient privacy and dignity o Patient engagement
This new TEAM project also aims to help build a strong foundation for HealthWatch, the new independent consumer champion and statutory part of the Care Quality Commission, to stand up for service users and carers across health and social care.
The TEAM project host, partners and supporting third sector organisations Leonard Cheshire Disability (Host) MRSA Action UK (Partner) St John Ambulance (Partner) C. difficile Support Changes 12 Steps to Mental Health Gender Identity Research and Education Society Kidney Alliance Muslim Council of Britain National Civil Service Pensioners’ Alliance National Concern for Healthcare Infection National Pensioners’ Convention PEM Friends Spinal Injuries Association
Maintaining Patient Safety and Preventing Harm
45
Appendix 2
Paper submitted on behalf of the Spinal Injuries Association
‘Maintaining Personal Safety after Discharge for SCI People through Collaborative Care’ Paul Harrison, RGN, ONC MAEd The NHS National SCI Strategy Board has evolved a series of National Care Pathways for the Initial and Lifetime Care of SCI people (http://www.secscg.nhs.uk/home/national-‐spinal-‐cord-‐injury-‐strategy-‐board/) that has the potential to reduce inappropriate spending within community care packages, the potential and the actual incidence of avoidable complications leading to early readmission after discharge and later secondary hospital admission. Unfortunately, many of the associate hospital departments and community agencies required to populate the pathway outside of the specialist SCI Centres are failing to realise their contributions through a reluctance to grasp the need for exceptional guidelines to support SCI people with complex care needs. As a result, the national and local health and social care budget holders are failing to realise a wide range of potential efficiency savings in time, money and human resources whilst increasing NHS costs due to penalties imposed by delayed hospital admissions and discharges and the consequences of avoidable health complications. Our National Health and Social Care Services need to integrate Complex Care Pathways within or in parallel to their current acute, reintegration, community and secondary admission care strategies so that the NHS, the Nation and the National Exchequer can realise the same benefits within this patient population as with the majority. A shift in strategic thinking by a few important individuals, with the power and authority to enable change at both national and local level has the potential to influence the personal safety and life satisfaction of tens of thousands of SCI people and to save the Government millions of pounds. The problems I will raise are uniform across this population, the solutions I propose are reasonable and achievabIe. However, the realisation of these ideas requires a pro-‐active shift in strategic thinking and budgeting and inter-‐agency, inter-‐disciplinary collaboration. The principal concerns of SCI people regarding personal safety are bladders, bowel and skin problems so I have requested the opportunity to include autonomic dysreflexia and neurogenic bowel management within this presentation which SIA perceive as risks to SCI people and the NHS on a scale equivalent to those previously identified in the agenda for this meeting. Autonomic Dysreflexia: Autonomic Dysreflexia (AD) is a condition-‐specific complication of SCI at or above the level of the sixth thoracic spinal nerve (T6). AD manifests as a gross, malignant, hypertension in response to any visceral pain or discomfort in the paralysed regions of the body. The most mortal effects are in response to bladder and bowel distension due to urinary outlet obstruction and protracted constipation. Venous thromboembolism, urinary tract infections and pressure ulcers can also trigger AD. The perceived risk of AD is established with the SCI patient, their family and carers during the initial inpatient rehabilitation and discharge preparation education programmes. Unfortunately, when the SCI person is transferred to a specialist SCI Centre they enter an essentially safe environment within which the individual care plans, pathways and procedural guidelines are specifically orientated to the risks inherent within a diagnosis of SCI. As a consequence, the actual incidence of AD within a SCI Centre admission is minimised to
Maintaining Patient Safety and Preventing Harm
46
the extent that a SCI person may never actually experience this complication, even though their inpatient admission is for between 3 -‐ 8 months duration. The real problem for the SCI population at risk of AD begins when the SCI Centre tries to arrange their discharge back into the community. The current Decision Support Tool and the process for Continuing Health Care funding is not sufficiently informed to address the potential risk of AD or the real need of a physically dependent SCI person to source the help needed to resolve an AD episode in a timely and efficient manner. AD is an unpredictable and potentially mortal complication for the population at risk as much as hypoglycaemia is for people living with diabetes and grand mal fits are for people living with epilepsy. Specifically at decision making panels, SCI professionals or patients are being asked to provide a record of the incidence of AD events since admission to the SCI centre. This is a highly inappropriate request given that the SCI patient has been managed almost entirely within a controlled environment up until the point of discharge. During the discharge preparation process the SCI Centre staff will endeavour to create and deliver a transitional care plan that mimics as far as possible the level of personal care, supervision and carer presence which they would reasonably expect to be provided after discharge. The management of AD events is usually restricted to the removal of the noxious stimulus such as replacing a catheter. However, in the event of an unresolved episode, the SCI person is provided with a prescribed vaso-‐dilator medicine to take to keep the symptoms under control until medical help arrives. If this issue is not addressed during discharge preparation then it may prove problematic in some instances for GP’s or pharmacists to provide because the British National Formulary (BNF) carries no advisory information regarding the role of these drugs in the treatment of AD. Vaso-‐dilators such as GTN spray need to be prescribed as ‘For use in the event of unresolved Autonomic Dysreflexia’ to avoid this problem. SIA wants Continuing Health Care panels to rule more appropriately on the provision of personal assistance by enabling them to become properly informed of the potential risk of AD and the realistic need for the presence of a carer who can not only summon help but also undertake first-‐aid interventions up to and including changing a urinary catheter is properly accommodated. Enabling a more appropriate awareness of AD amongst health and social care professionals has the potential to save lives and reduce the incidence of avoidable secondary readmission to hospital. SIA wants increase awareness of AD amongst principal care providers such as GPs, Continence Nurses, Community Nurses, Case Managers, Paramedics and Hospital Emergency Departments SIA want to enable the provision and recognition of an Emergency Alert Card or ‘Patient Passport’ for the SCI population at large which would includes a specific ‘Dysreflexia Alert’ component for use by those at risk Neurogenic Bowel Management: ‘Continence care is problematic and requires timely and skilled intervention, beyond routine care’. This phrase, extracted from the current Decision Support Tool is an exact description of the care required to support a dependent SCI person in the community. How unfortunate then that the SCI Centre Discharge Coordinators are faced with panel decisions that suggest that bowel care for SCI people is merely ‘routine’. If only this were so. Despite the efforts of the Royal College of Nursing and the Association of Continence Advisors, hospital and community nurses are still proving reluctant to recognise digital bowel procedures as a legitimate and essential requirement within the routine care and management of SCI people. The essential need for appropriate bowel care after SCI to prevent AD was established in a collaboration between the SIA and the NPSA in 2004 and resulted in the issuing of appropriate guidance to professionals.
Maintaining Patient Safety and Preventing Harm
47
The launch event was held on the Parliament terrace. I return to Parliament after eight years to report that little has changed and SIA appeals to the NPSA to revisit the issue to see if a more enabling form of guidance can be created. It is within this topic that I offer an example of how a collaboration between PCTs and SCI professionals during the planning of complex discharges can result in significant resource savings. A particular PCT required that SCI patients discharged into their geographical area were required to receive their bowel care from a Community Nurse, even if the SCI person was provided with a personal carer funded within their health care package. This was because the PCT Continence Advisor had deemed that digital bowel procedures were outside of the skill-‐set of the personal carer. The greatest complaint within this arrangement was the need for the SCI person to be left waiting for the Community Nurse to undertake the bowel care at her convenience rather than at a time appropriate to the SCI person’s daily life routines. This was so detrimental that it was actually preventing SCI people from returning to work. An intervention by the Community Liaison and Education Teams of the local SCI Centre direct to the Regional Continence Care Team resulted in a recognition that personal carers could be enabled to undertake routine digital bowel procedures at a time convenient to the SCI person. The result when applied across the region to remove the need for avoidable Community Nurse interventions was a time saving equivalent to £1.6 million pounds per year. This nursing time was then better deployed to those tasks that definitively required the presence of a Community Nurse. For the SCI people involved it meant an improved quality of life, improved continence, a reduction in episodes of unplanned bowel emptying and for several, the opportunity to return to work or education that was previously denied them under the old arrangements. Pressure Ulcers Pressure Ulcers (PU) are also a well established complication within the initial and continuing care of SCI people. However, local and national initiatives to improve quality of care within this domain have failed to address many of the specific needs of SCI people with the consequence that PU incidence in the SCI population has actually increased in recent years. The principle cause of this increase is simply that the availability and contribution of specialist Community Liaison Teams within the SCI Centres is not recognised or accommodated within the PU prevention and management guidelines promoted within Community Care. By failing to recognise the advantage of involving specialist peers in the first instance, community care teams are failing to reduce the human and economic consequences of PUs within the SCI population. SIA has successfully campaigned to have SCI people and SCI Centre professionals included within the next review of the NICE PU guidelines. Urinary Tract Infections: When an SCI patient is discharged into the community it is with the knowledge that their bladder management programme has been established with their full involvement and was informed by a continence team led by a consultant urologist experienced in the management of the paralysed bladder and robustly tested over a minimum of 3 months to be sustainable after discharge. Unfortunately, community care guidelines do not easily accommodate specialist care needs and so local continence are teams strive to interpret long-‐term catheterisation issues within guidelines intended for managing short-‐term catheterisation. Urinary Tract Infections (UTIs) are a recurrent problem for SCI people and a potential cause of Autonomic Dysreflexia. Specialist clinicians are struggling to maintain SCI people within the SCI care pathway against the interference created by local and national strategic initiatives which once again fail to recognise or encompass the exceptional needs of patients with SCI. The principle cause is a failure to separate short and
Maintaining Patient Safety and Preventing Harm
48
long-‐term catheter use into clear and distinct guidelines for non-‐specialist carers. SCI people utilising long-‐term indwelling urinary catheters will present with a bacterial contamination akin to the normal skin flora. It is present but not harmful and like resident skin flora may actually reduce the potential for pathogens to achieve colonisation. Every hospital and community care trust has their own guidelines regarding catheterisation, including the use of suprapubic catheters but most of these fail to recognise the essential differences with regard to the prevention or management of clinically symptomatic UTI and bacterial colonisation. This results in a significant over-‐use of antibiotics with resulting bacterial resistance over the lifetime. Infection is related to the method of bladder management but the rate of symptomatic UTI in SCI people is primarily related to inappropriate or poorly informed changes in established methods of bladder management. Paralysed bladders do not work properly so the best solution for long-‐term care is to enable the SCI person to make an informed choice regarding a sustainable bladder management programme and then to ensure that this choice is understood and supported by community continence teams after discharge. Venous Thromboembolism (VTE) The presence of SCI paralysis reduces the potential for general hospital and community clinicians to interpret the available evidence of VTE during clinical examination in the same way with the result that there may be a delay in diagnosis and treatment. Guidelines for GPs and hospital clinicians when examining SCI people should include pointers to potential indicators of VTE in SCI people and the need to consult with specialist SCI clinicians in a timely and proficient manner whenever diagnosis is uncertain. Conclusion AD has a constant lifetime potential for morbidity and mortality in the at-‐risk SCI population. The actual AD incidence fluctuates over time because bladder and bowel management methods are expected to change over the lifetime of the SCI individual requiring a constant review of care needs in the dependent SCI population. Skin care programmes and the risk of pressure ulcers increases with advancing age and so does the need for additional interventions and equipment. The National SCI Care Pathway promotes the lifetime care needs of SCI people from initial diagnosis to end-‐of-‐life care. In order to achieve the quality of life possible after SCI specialist and generalist care providers must establish a collaboration in practice unlike any achieved previously. Current austerity measures mean that there is little money available to finance the launch of any new initiatives so SIA has set itself the ambition, along with the National SCI Strategy Board to promote AD as an example of where improved collaboration between service providers and alternative strategic thinking are all that is required to make significant improvements in both resource savings and patient reported outcomes measures within the existing care provision along with financial savings that can be reinvested in those parts of the pathway that genuinely need additional funding in order to improve.
Maintaining Patient Safety and Preventing Harm
49
Appendix 3
Contributions From People Unable To Attend In Person Simon Lawton-‐Smith Head of Policy, Mental Health Foundation
Patient safety is a key issue in mental health, as people’s experience both in psychiatric units, and also sometimes in the community, can at times be very frightening and unsafe. This involves not just high levels of self-‐harm and risk of suicide as a result of a mental disorder, but also, in inpatient settings, the possibility of harm from other unwell patients.
Much has been done to reduce avoidable harm in psychiatric units over the past few years, leading to a very welcome reduction in suicides, for example. However these settings remain potentially volatile places where good staff training in risk management and de-‐escalation techniques is absolutely essential.
A key issue is discharge planning for mental health patients – making sure people have access to rapid support when they leave hospital from the very start (whether in terms of clinical care, employment, housing or welfare benefits). It’s the first few days and weeks when there are the highest rates of suicides of discharged mental health patients. We also know that there are very high levels of self-‐harm in the community, not least among among older children and younger adults, and we would like to see more effective preventative strategies targeting these age groups in particular. Our Truth Hurts Inquiry set out what can be done to help young people who self-‐harm – one of its publications can be seen at
In addition, the evidence tells us that people with mental disorders often experience poorer physical health than they should. This is partly because they may lead chaotic lifestyles or their disorder (eg chronic depression) may lead them to neglect themselves – and we know there are very high levels of smoking among psychiatric patients. But in addition, co-‐morbidity among mental health patients can be ignored or missed by healthcare staff who focus exclusively on the mental disorder diagnosis. For example, an anxious person is up to six times more likely to die of coronary heart disease; people with bipolar disorder and schizophrenia are at increased risk for a range of physical illnesses, and are twice as likely to die from coronary heart disease as the general population; cumulative stress at work has been associated with an increased risk of heart disease, cardiovascular death or angina. It is therefore essential that patient safety strategies take into account the need to support both the physical and mental health needs of patients. Of course the Government’s 2011 mental health strategy has improving the physical health of mental health patients as one of its key objectives.
Finally, we recently collated responses to Mental Health Foundation ‘same sex wards’ questionnaire among members of the Foundation’s Policy Panel, June 2009. There were 19 responses in all, 13 from people who have used mental health services and 6 from people who have worked in the mental health system. While most mental health inpatients do now have access to same-‐sex facilities and their own bedrooms, we can see from the testimony of the patients who contacted us that there were some very real safety issues in the psychiatric facilities they had used.