٠٤/٠٣/١٤٤١ Presented by Dr.MaissaEid Afifi Consultant of Psychiatry Ain Shams University Treasurer of Alzheimer’s Egypt Contents Introduction Mental competence Guardianship Screening for cognitive impairment Introduction Populations around the world are rapidly aging. Aging presents both challenges and opportunities. Cognitive abilities rise steeply from infancy to young adulthood and then are either maintained or decline to old age, depending on the specific ability. The normal cognitive changes with age are important to understand because, first, they can affect an older adult’s day to day function and, second, they can help us distinguish normal from disease states. Memory decline is the core of Dementia mostly Alzheimer’s disease . As the dementia progresses, the patient's ability to carry out everyday tasks diminishes and he may not be able to look after himself. Deficits in orientation, memory, abstraction, concentration, calculation, and thought process may be associated with mental incompetence. Diagnosis of cognitive impairment generally, and MCI and AD specifically, should signal possible financial impairment and prompt the physician to encourage patients and families to proactively engage in financial and legal advance planning. Alzheimer’s disease is identified by the National Bioethics Advisory Commission (Sweden)as one of the “mental disorders that may affect decision making capacity”. Few studies have addressed the relationship between dementia and crime. Understanding the impact of dementia has not been in focus in forensic psychiatry since criminal behaviour often starts at young age. Few studies have focussed on the mental condition of elderly criminals. BMC Geriatric. 2017; ١ ٢ ٣ ٤ ٥ ٦
Transcript
٠٤/٠٣/١٤٤١
Presented by Dr.MaissaEid Afifi
Consultant of Psychiatry Ain Shams University
Treasurer of Alzheimer’s Egypt
Contents Introduction
Mental competence
Guardianship
Screening for cognitive impairment
Introduction Populations around the world are rapidly aging. Aging
presents both challenges and opportunities.
Cognitive abilities rise steeply from infancy to young adulthood and then are either maintained or decline to old age, depending on the specific ability.
The normal cognitive changes with age are important to understand because, first, they can affect an older adult’s day to day function and, second, they can help us distinguish normal from disease states.
Memory decline is the core of Dementia mostly Alzheimer’s disease .
As the dementia progresses, the patient's ability to carry out everyday tasks diminishes and he may not be able to look after himself.
Deficits in orientation, memory, abstraction, concentration, calculation, and thought process may be associated with mental incompetence.
Diagnosis of cognitive impairment generally, and MCI and AD specifically, should signal possible financial impairment and prompt the physician to encourage patients and families to proactively engage in financial and legal advance planning.
Alzheimer’s disease is identified by the National Bioethics Advisory Commission (Sweden)as one of the “mental disorders that may affect decision making capacity”.
Few studies have addressed the relationship between dementia and crime. Understanding the impact of dementia has not been in focus in forensic psychiatry since criminal behaviour often starts at young age.
Few studies have focussed on the mental condition of elderly criminals.
BMC Geriatric. 2017;
١ ٢
٣ ٤
٥ ٦
٠٤/٠٣/١٤٤١
A Swedish study found that only <3% forensic psychiatric examinations concerned persons 60 years or older . In 7% of those, dementia was found.
In a register-based study from Finland, homicide offenders aged 60 or older had less drug dependence and personality disorders and more dementia and physical illnesses than younger homicide offenders .
In forensic psychiatric examinations in Turkey, most persons >60 years of age were diagnosed with schizophrenia or delusional disorder .
In South Carolina, violent crimes were common among persons >60 years of age that went through a forensic psychiatric examination .
Does dementia actually decrease the risk of committing crimes? Neurocognitive symptoms like memory impairment, reduced executive
function, lack of judgement and language difficulties are hall-marks of dementia.
Symptoms vary over time and with the type of dementia, comorbid diseases, medication, environment and care provided.
Symptoms can separately or in combination contribute to criminal behaviour and actions.
Some persons with dementia become withdrawn and careful since they experience their shortcomings.
Reduced executive function, that is common in Alzheimer’s disease, results in a passive behaviour, not likely to enhance planning and organizing a crime.
Focal prefrontal damage seems associated with an impulsive subtype of aggressive behaviour and persons with Frontal Lobe Dementia are at increased risk for violent crimes.
There are a few reports on persons with dementia committing murder. In murder-suicide cases by elderly couples, the victim often suffers from
dementia and not the spouse committing the murder .
From a forensic point of view, a “severe mental disorder” is not related to diagnoses but to effects of disorders:
1)Psychotic effects or
2) Severe depression with suicidal behaviorat the time of the crime or
٧ ٨
٩ ١٠
١١ ١٢
٠٤/٠٣/١٤٤١
3) Severe personality disorder with recurrent episodes of psychotic behaviorand decreased psychosocial functioning or
4) Mental disorder with marked compulsiveness and decreased psychosocial functioning or
5) Severe dementia, severe mental retardation and severe brain damage.
Mental disorders may be considered severe by the public and by the general health care system and but not from a forensic psychiatric point of view.
If the person was in a state of severe psychiatric disorder at the time of the crime, the verdict can be forensic psychiatric care instead of prison.
The court should also decide on whether cessation of forensic care be decided by the forensic psychiatrist or by a court procedure (“forensic care with separate discharge review”).
Mental Competence Mental competence is the basis for many activities in
life.
For example a person must be mentally competent to: enter contracts, consent to medical treatment, make a will or drive a vehicle.
The laws assume every adult is mentally competent until a court decides otherwise.
What exactly is mental incompetency? Legal terms defines a mentally incompetent person as someone whose
mind is affected either from birth, disease, injury or by a disorder to such a degree that they require care, supervision, and control for their own protection, the protection of others, or the protection of their property.
A finding of mental incompetency could mean that somebody will have to get legal authority to make decisions for the person.
When this happens, the assessment may be presented as evidence in court. The court would use this information to help it decide what kinds of decisions the guardian can or cannot make on behalf of the other person.
Egyptian Law
١٣ ١٤
١٥ ١٦
١٧ ١٨
٠٤/٠٣/١٤٤١
Who conducts a mental competency assessment? An experienced health care professional conducts the
assessment. It usually takes place in a person’s home and often there is more than one assessment.
Can a person refuse to have an assessment?
Yes. However, if a person refuses an assessment, a family
member or caregiver can ask a court to order a competency assessment.
How is mental competency assessed? Mental competency is assessed through a series of questions that try to
determine if a person is capable of making decisions.
The questions may vary and health care professionals may have different methods of assessment.
Generally an assessment examines a person’s
Thoughts Awareness Perceptions
Judgment Mood Memory
Medical and neurological examinations, laboratory evaluation, brain imaging, and neuropsychological testing may all provide essential information linked to the forensic question.
For example, in an elderly patient with cognitive impairment who is being assessed for decision-making ability, differentiating focal deficits from global impairment and progressive cognitive deterioration from reversible deficits may be central to issues that involve different forms of capacity and competency, safety, and advanced planning.
One model of the assessment of capacity involves the examination of 4 functional areas:• The ability to communicate a stable choice• The ability to understand relevant factual information within the context of the treatment decision• The ability to appreciate how the situation and outcome affect one’s personal life• The ability to weigh the risks and benefits of options in the process of making a decision
(Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988; 319:1635-1638.)
١٩ ٢٠
٢١ ٢٢
٢٣ ٢٤
٠٤/٠٣/١٤٤١
The approach to assessing the need for guardianship starts with an evaluation of capacity, determination whether capacity is impaired temporarily or permanently, the causes of any diminished capacity, and what types of decisions or actions a guardian will make.
A number of disorders can result in the need for either temporary or permanent guardianship, including delirium, dementia, stroke, traumatic brain injury, neurodevelopmental disorders, and psychoses.
Areas in which capacity to make decisions are assessed and for which a guardian may be needed include routine health care, decisions about finances and business, and decisions about medical care that can be state specific and include use of antipsychotic medication and electroconvulsive therapy.
Related to the issue of capacity, an individual may have impaired decision-making ability in one area, yet retain capacity or competency in another area, and the responsibilities of a substitute decision-maker may be focused and context specific.
For example, an impaired individual with a history of poor capacity related to treatment decisions, who is now in good health and lives in a supportive setting, may not have an immediate need for a guardian of person to make treatment decisions.
The clinical team, attorneys, and court may take into account the urgency and valence of the need for a substitute decision maker in the guardianship application process.
Here is some bedside tests to help in assessment of the degree of cognitive impairment.
Screening for cognitive impairment Mini Mental State Examination (MMSE): It takes 8 min to perform in hospitalized elderly patients (range 4–21 min).
There is some inter-user difference in scoring tests, and some variation in the questions; for example, the calculation task can use either serial 7s (subtracting 7s from 100) or spelling of the word ‘WORLD’ backwards—in some cases both are performed, and the highest result is used.
٢٥ ٢٦
٢٧ ٢٨
٢٩ ٣٠
٠٤/٠٣/١٤٤١
Screening for cognitive impairment Mini Mental State Examination (MMSE):
Various cut-off values have been advocated for the maximum sensitivity and specificity in differing populations. Scores can be biased by baseline educational level, language and cultural barriers.
Values of 23 or less for those with education up to high school, and 25 or less for those who underwent higher education are commonly used to indicate significant impairment.
Screening for cognitive impairment Mini Mental State Examination (MMSE):
It does not contain much capacity to test frontal/executive or visuospatial (typically right parietal) functions.
The pentagon task of the MMSE simply requires the patient to copy the image, and does not assess planning skills
As a consequence it may have a limited ability to detect non-Alzheimer’s dementias, such as post-stroke cognitive impairment, frontotemporal or subcortical dementias in their early phases.
Screening for cognitive impairment Montreal cognitive assessment tool: a brief 30-question test that takes around 10 to 12 minutes to complete and
helps assess people for dementia. The MoCA's advantages include its brevity, simplicity, and reliability as a
screening test for Alzheimer's disease. In addition, it measures an important component of dementia that's not measured by the MMSE, namely executive function. It seems to work well in Parkinson's disease dementia.
٣١ ٣٢
٣٣ ٣٤
٣٥ ٣٦
٠٤/٠٣/١٤٤١
Screening for cognitive impairment
Go/no-go Test The patient is asked to make a response to one signal (the Go signal) and not to respond to another signal (the no-go signal). The most basic is to ask the patient to tap their knee when the examiner says, “Go” and to make no response when the examiner says, “Stop”.
The task may be made more demanding by reversing the customary meaning of signals. An example is to ask the patient to tap the knee when the examiner says "Stop" and not to tap when the examiner says "Go"
(Malloy and Richardson, 1994).
Screening for cognitive impairment The Stroop Test This is a neuropsychological test which examines the ability of the patient to
inhibit responses. Patients are asked to state the color in which words are printed rather than the
words themselves, e.g., yellow may be printed in blue, blue may be printed in red.
(Stroop, 1935).
Screening for cognitive impairment Clock Drawing Test (CDT):
The Clock Drawing Test (CDT) is a screen for visuospatial, constructional abilities and frontal/ executive impairment.
The patient is first asked to draw a circle , and then put on numbers as though it were a clock face. Or a pre-drawn circle is presented to the patient and he is asked to fill the numbers and then set the time to ten past eleven.
Inability to correctly space the numbers around the circle can be due to a visuospatial impairment, neglect, or a planning deficit.
Screening for cognitive impairment Mini-Cog: The Mini-Cog adds a three-word recall test to the CDT, thus improving memory
testing. It takes around 3 min to perform.
The result obtained is thus that cognitive impairment is absent or present, rather than a numerical scale. This adds to its simplicity as a screening test, but means the test has no value in either monitoring disease progression or rating severity
٣٧ ٣٨
٣٩ ٤٠
٤١ ٤٢
٠٤/٠٣/١٤٤١
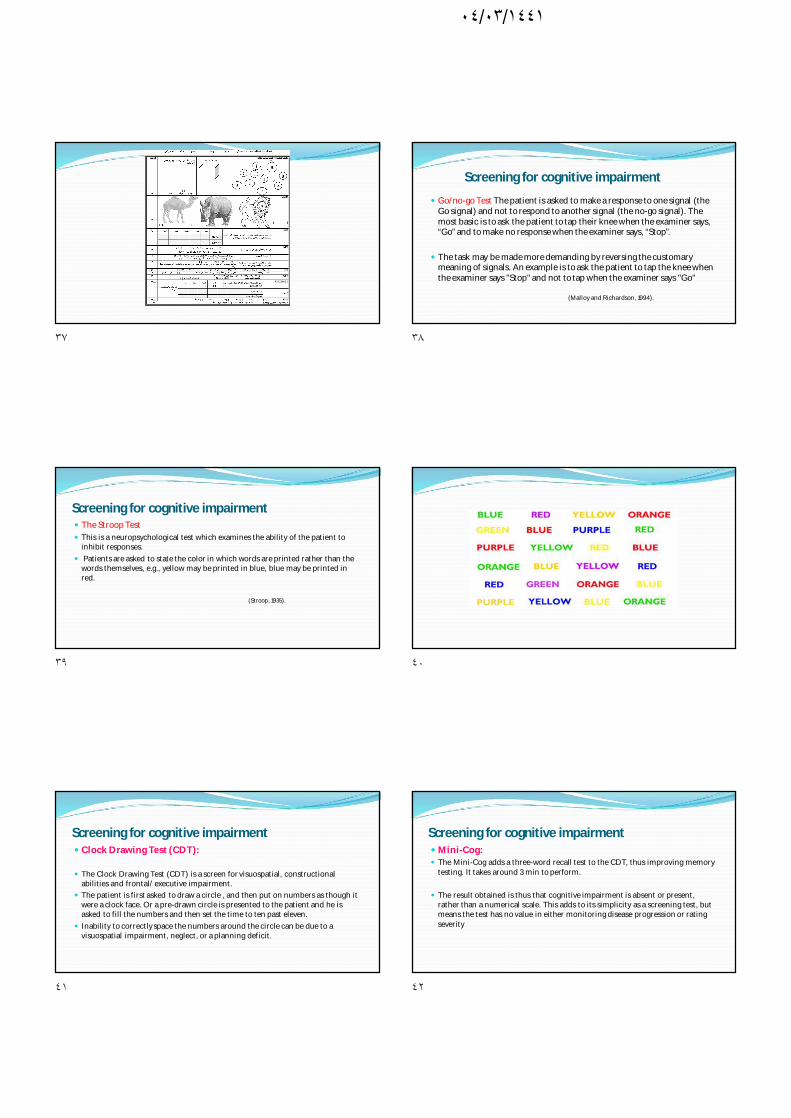
Assessing Patients’ Functional Status Functional impairment is defined as difficulty performing, or requiring the assistance of another
person to perform, one or more of the following Activities of Daily Living (ADL):
A summary score ranges from 0 (low function, dependent) to 8 (high function, independent) for women and 0 through 5 for men to avoid potential gender bias.