Major Depressive Disorder: Understanding the Significance of Residual Symptoms and Balancing Efficacy with Tolerability Larry Culpepper, MD, MPH, a Philip R. Muskin, MD, b Stephen M. Stahl, MD c,d,e a Department of Family Medicine, Boston University School of Medicine, Boston Medical Center, Boston, Mass; b Department of Psychiatry, Columbia University Medical Center, New York, NY; c Department of Psychiatry, University of California San Diego, San Diego; d Neuroscience Education Institute, Carlsbad, Calif; e Department of Psychiatry, University of Cambridge, Cambridge, United Kingdom. ABSTRACT INTRODUCTION: Major depressive disorder is a complex and frequent psychiatric condition that poses significant challenges to both the patients who experience it and the physicians who treat them. The goal of therapy is for patients to achieve remission, which requires identifying and measuring symptoms at the outset and throughout treatment to document both response and resistance to treatment. A number of validated instruments are available both for diagnosis of and response to treatment. Many factors affect a patient’s ability to achieve remission, but although many patients do achieve remission, a significant number continue to have residual symptoms that cause functional impairment. METHODS: Review of the literature for treatment of major depression, including mechanisms of action, individualized treatment optimization, residual symptom reduction, and minimization of side effects. RESULTS: For sustained remission, all symptoms must be treated until they are undetectable. Patients who do not achieve remission after adequate treatment trials should be evaluated for adherence to treatment, as well as comorbid psychiatric and medical disorders. In these cases, consideration should be given to changing therapy by switching, combining, or augmenting initial therapy, as well as referring some patients to a psychiatrist for treatment with specialized modalities. Linking symptoms with malfunctioning brain circuits and neurotransmitters provides a targeted approach for achieving sustained remission. Neurobi- ology also provides a rational basis for combination therapy in patients with treatment-resistant depression, because it can aid selection of different drugs with different mechanisms of action or of multifunctional/ multimodal antidepressant drugs that target more than 1 molecular mechanism. DISCUSSION: Recent advances and better understanding of neurobiology provide a rational basis for individualizing treatment of patients with major depression. Ó 2015 Elsevier Inc. All rights reserved. The American Journal of Medicine (2015) 128, S1-S15 KEYWORDS: Efficacy; Individualized Treatment; Major depression; Measurement based care; Multimodal antidepressants; Residual Symptoms Major depressive disorder is widespread, with an estimated 12-month prevalence of 6.7%. 1 It is associated with signif- icant costs in quality of life and lost work productivity largely due to absenteeism/sick days, short-term disability, and performance deficits. 2,3 The estimated economic burden of depression in 2000 was 83.1 billion dollars, of which 51.5 billion dollars were workplace costs. 4 Treating depression is cost-effective because the cost of treatment is offset by increased work productivity associated with symptom remission. 2 Major depressive disorder is complex. If one considers the diagnostic criteria—depressed mood or apathy/loss of interest plus 4 additional symptoms (Figure 1)—there are >60 forms of major depressive disorder given the various Funding: None. Conflict of Interest: None. Authorship: All authors had access to the data and played a role in writing this manuscript. Requests for reprints should be addressed to Larry Culpepper, MD, MPH, Department of Family Medicine, 1 BMC Place, Boston, MA 02118. E-mail address: [email protected]0002-9343/$ -see front matter Ó 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.amjmed.2015.07.001
Transcript
Major Depressive Disorder: Understanding theSignificance of Residual Symptoms and BalancingEfficacy with TolerabilityLarry Culpepper, MD, MPH,a Philip R. Muskin, MD,b Stephen M. Stahl, MDc,d,eaDepartment of Family Medicine, Boston University School of Medicine, Boston Medical Center, Boston, Mass; bDepartment of Psychiatry,Columbia University Medical Center, New York, NY; cDepartment of Psychiatry, University of California San Diego, San Diego;dNeuroscience Education Institute, Carlsbad, Calif; eDepartment of Psychiatry, University of Cambridge, Cambridge, United Kingdom.
ABSTRACT
INTRODUCTION: Major depressive disorder is a complex and frequent psychiatric condition that posessignificant challenges to both the patients who experience it and the physicians who treat them. The goal oftherapy is for patients to achieve remission, which requires identifying and measuring symptoms at theoutset and throughout treatment to document both response and resistance to treatment. A number ofvalidated instruments are available both for diagnosis of and response to treatment. Many factors affect apatient’s ability to achieve remission, but although many patients do achieve remission, a significantnumber continue to have residual symptoms that cause functional impairment.METHODS: Review of the literature for treatment of major depression, including mechanisms of action,individualized treatment optimization, residual symptom reduction, and minimization of side effects.RESULTS: For sustained remission, all symptoms must be treated until they are undetectable. Patients whodo not achieve remission after adequate treatment trials should be evaluated for adherence to treatment, aswell as comorbid psychiatric and medical disorders. In these cases, consideration should be given tochanging therapy by switching, combining, or augmenting initial therapy, as well as referring some patientsto a psychiatrist for treatment with specialized modalities. Linking symptoms with malfunctioning braincircuits and neurotransmitters provides a targeted approach for achieving sustained remission. Neurobi-ology also provides a rational basis for combination therapy in patients with treatment-resistant depression,because it can aid selection of different drugs with different mechanisms of action or of multifunctional/multimodal antidepressant drugs that target more than 1 molecular mechanism.DISCUSSION: Recent advances and better understanding of neurobiology provide a rational basis forindividualizing treatment of patients with major depression.� 2015 Elsevier Inc. All rights reserved. � The American Journal of Medicine (2015) 128, S1-S15
KEYWORDS: Efficacy; Individualized Treatment; Major depression; Measurement based care; Multimodalantidepressants; Residual Symptoms
Major depressive disorder is widespread, with an estimated12-month prevalence of 6.7%.1 It is associated with signif-icant costs in quality of life and lost work productivity
largely due to absenteeism/sick days, short-term disability,and performance deficits.2,3 The estimated economic burdenof depression in 2000 was 83.1 billion dollars, of which 51.5billion dollars were workplace costs.4 Treating depression iscost-effective because the cost of treatment is offset byincreased work productivity associated with symptomremission.2
Major depressive disorder is complex. If one considersthe diagnostic criteria—depressed mood or apathy/loss ofinterest plus �4 additional symptoms (Figure 1)—there are>60 forms of major depressive disorder given the various
Funding: None.Conflict of Interest: None.Authorship: All authors had access to the data and played a role in
writing this manuscript.Requests for reprints should be addressed to Larry Culpepper, MD,
MPH, Department of Family Medicine, 1 BMC Place, Boston, MA 02118.E-mail address: [email protected]
0002-9343/$ -see front matter � 2015 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.amjmed.2015.07.001
possible unique combinations of symptoms.5 Effectivelytreating patients with major depressive disorder to completeresolution of all symptoms presents a challenge to physi-cians. All antidepressant drugs have similar efficacy rates,but response among patients varies.
As our understanding of the neurobiology of majordepressive disorder has increased,individualizing treatment toimprove outcomes has improved.It is now recognized that psychi-atric symptoms correlate withmalfunctioning brain circuits. Anunderstanding of a patient’ssymptom profile is key to indi-vidualizing treatment becausedifferent symptoms may reflectdifferences in underlying neuro-pathology, including differencesin neurotransmitter-related abnor-malities. Such understanding sup-ports the selection of medicationsor other treatments that have themechanisms of action appropriatefor the patient. Applying neurobi-ology principles provides a ratio-nale for individualized treatmentselection.
DEFINING TREATMENTOUTCOMES: IMPORTANCEOF RESIDUAL SYMPTOMSOver the last 3 decades, the desired outcome for the treat-ment of major depressive disorder has shifted from responseto remission (Table 1).6 The definition of response—�50%reduction in total symptom severity—allows for the pres-ence of significant residual symptoms, which may predis-pose patients to recurrence, chronicity, and suicidality. Theoptimal outcome for patients with major depressive disorderis now considered to be symptomatic remission, a markerof wellness that is critical to return to premorbid levelof functioning. It may be defined as minimal residualsymptoms as measured by a �80% reduction in symptom-atology using one of the accepted rating scales or as anabsolute cutoff score, such as �7 on the 17-item HamiltonRating Scale for Depression (HAM-D).
The concept of remission more closely matches, butfalls short of, what patients are trying to achieve withtreatment. The factors most frequently identified bypatients as being very important for achieving remissionwith treatment are listed in Table 2.7 These factors relateto the concept of well-being, which is defined as havingachieved at least 1 item in each of 6 dimensions, includingenvironmental mastery, personal growth, purpose in life,autonomy, self-acceptance, and positive relations withothers.8 Recovery from a major depressive episode also is
suggested as a desirable treatment outcome. However,the definition of recovery includes the criterion that thepatient remains in full remission despite discontinuationof treatment, which may not be reasonable given thechronicity of and biological basis for major depression inmany patients.8
Patients who achieve fullremission are more likely to returnto normal psychosocial func-tioning.9 Thus, the consequencesof not achieving remission aremany, affecting both the course ofthe disease and the healthcare andsocietal costs (Table 3).10-12 Pa-tients who achieve remissionbut have residual symptoms aremore likely to relapse than thosewithout residual symptoms(Figure 2).13,14 A literature reviewthat assessed the burden oftreatment-resistant depression inthe United States concluded thatup to 20% of patients withdepression are treatment resistantand that annual added societalcosts related to treatment-resistantdepression are in the range of$29 to $48 billion.16
Patients who respond to treat-ment—�50% reduction in symp-toms—are more likely to havesignificant functional impairment
than those who achieve remission.9,17 Nonetheless, somepatients who attain symptomatic remission also experiencesignificant functional impairment after treatment.9,17-19
Although a criterion for major depressive episodes is func-tional impairment, clinical studies almost universally haverelied on symptoms or symptom profiles as outcome mea-sures.18 Patients may report improvement in global func-tioning measures with treatment, but changes in specificfunctional domains (eg, social, occupational, physical)generally have not been studied. An analysis of the literatureconcluded that functional outcomes tend to be less respon-sive to treatment than are symptom outcomes.18 The pres-ence of some residual symptoms, such as core moodsymptoms, correlate more strongly with functional impair-ment in patients who achieved remission than do otherresidual symptoms.19
The degree of remission appears to influence theimprovement in the level of functionality. The accepteddefinition of remission on the 17-item HAM-D, a cutoff of�7, is now considered too high, because global psychoso-cial functioning and quality of life are still impaired.20-22
Scores of �520 and even 0 to 222 are suggested as bettertarget scores for identifying normal levels of functionality.Even patients who scored �7 on the HAM-D did notconsider themselves to be in remission.21
CLINICAL SIGNIFICANCE
� Treatment to remission of depression iskey to recovery of full function and pre-venting relapse.
� Even in remission patients experienceresidual symptoms that impairfunctioning.
� Individualized treatment matchingtherapy to specific symptom clusters maybe most effective.
� Matching treatment to symptoms targetsdysfunctional brain networks and theirneurotransmitters.
� Multimodal treatment is often requiredto target multiple neurotransmitters.
� Multimodal antidepressants may provideless adverse effects than use of multiplesingle modality antidepressants.
S2 The American Journal of Medicine, Vol 128, No 9A, September 2015
Measuring Residual Symptoms and FunctionalImpairmentAssessment of treatment response using measurement-basedassessment and rating scales is necessary to determine whento adjust therapy.23 Among the tools to measure the severityof major depressive disorder are the 16-item QuickInventory of Depressive Symptomatology (QIDS), whichhas both patient self-report and clinician-rated versions, the9-item Patient Health Questionnaire (PHQ-9), the HAM-D,the Montgomery Asberg Depression Rating Scale, and
specific symptom scales (eg, Epworth Sleepiness, insomnia,and pain severity scales). To enable full recovery in patientswith major depressive disorder, physicians must be awareof functional impairments that the patient is experiencing.Because the QIDS, HAM-D, and Montgomery AsbergDepression Rating Scale do not directly assess functionalimpairments, they often are coupled with validated in-struments that can identify impairments and measure thechange in impairments over time with treatment.
One instrument that is feasible for use in routine clinicalpractice is the Sheehan Disability Scale, a brief patient-ratedmeasure of functional disability in work, social, and familylife.24 A total score (the sum of the 3 domain scores ranging
Figure 1 Symptom dimensions of a major depressive episode.5 In addition to depressed moodand agitation, �4 other symptoms are required to make the diagnosis of major depressive disorder.This indicates that there are many types of major depression and that treatment needs to beindividualized to the specific symptoms present. From Stahl SM. Stahl’s Essential Psychophar-macology: Neuroscientific Basis and Practical Applications. 4th ed. New York, NY: CambridgeUniversity Press; 2013, with permission.
Table 2 Outcomes Important to Patients with Depression inDetermining Remission7
� Absence of symptoms of depression� Presence of positive mental health (eg, optimism, vigor,self-confidence)
� Feeling like your usual, normal self� Return to usual level of functioning at work, home, or school� Feeling in emotional control� Participating in, and enjoying, relationships with familyand friends
Table 1 Treatment Outcomes in Major Depressive Disorder6,25
� Response �50% reduction in total symptom severity� Remission Minimal residual symptoms as measured by
�80% reduction in symptoms using anaccepted rating scale
orAbsolute cutoff score, such as �7 on the17-item HAM-D
or <5 on the PHQ-9� Recovery Includes criterion that the patient remains
in full remission despite discontinuationof treatment
HAM-D ¼ Hamilton Rating Scale for Depression; PHQ-9 ¼ 9-ItemPatient Health Questionnaire.
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S3
from 0 [unimpaired] to 30 [highly impaired]) of �6 isindicative of functional impairment. The Sheehan DisabilityScale has been validated in clinical trials, in various psy-chiatric disorders, and in patients aged >60 years forboth baseline impairment and change in impairment withtreatment.
Other screening instruments, such as the PHQ-9, identifythe impact of residual symptoms on impairment.25,26 ThePHQ-9 asks patients about problems experienced over thelast 2 weeks and how difficult those problems made it to dowork, take care of things at home, or get along with otherpeople on a 4-point scale ranging from not difficult toextremely difficult. The level of functional impairmenton the PHQ-9 was shown to significantly correlate withseverity of depression and with remission in a retrospectivelogistic regression analysis of 1083 patients enrolled incollaborative care management for depression.27 Severedepression was more common in patients with the highestlevels of functional impairment (PHQ-9 score �20): 6.4%of patients in the somewhat difficult group, 22.3% of pa-tients in the very difficult group, and 52.3% of patients in
the extremely difficult group. In addition, the odds ofachieving normal functional status at 6 months correlatedhighly with clinical remission (PHQ-9 score <5) with anodds ratio of 218.53 (P < .001) or with improvement tomild depressive symptoms (PHQ-9 score 5-9) with an oddsratio of 12.301 (P < .001).
The Work and Social Adjustment Scale (WSAS) is a5-item self-report measure that assesses the ability to work,to manage home and social affairs, and to form and maintainclose relationships rated on a 0 to 8 Likert scale.28 Scores<10 on the WSAS are associated with subclinical disease,scores 10 to 20 indicate significant functional impairment,and scores >20 suggest at least moderately severe func-tional impairment. In an analysis of the Sequenced Treat-ment Alternatives to Relieve Depression trial, higher WSASscores were associated with greater risk for poorer quality oflife.28 The WSAS was shown to be a reliable and validmeasure of impaired functioning.29
The Quality of Life Enjoyment and Satisfaction Ques-tionnaire is a 16-item instrument that asks how satisfiedpatients have been during the past week with such things asphysical health, mood, work, social and family relation-ships, and ability to function in daily life on a scale of 1 to 5(numeric score corresponds to descriptive terms from verypoor to very good).30 Fourteen of the 16 items are summedfor a total score ranging from 14 to 70. The last 2 questionsare stand-alone ones that relate to medication and a ratingof overall life satisfaction and contentment during the pastweek. The scale scores are reliable, valid, and related toquality of life measures.
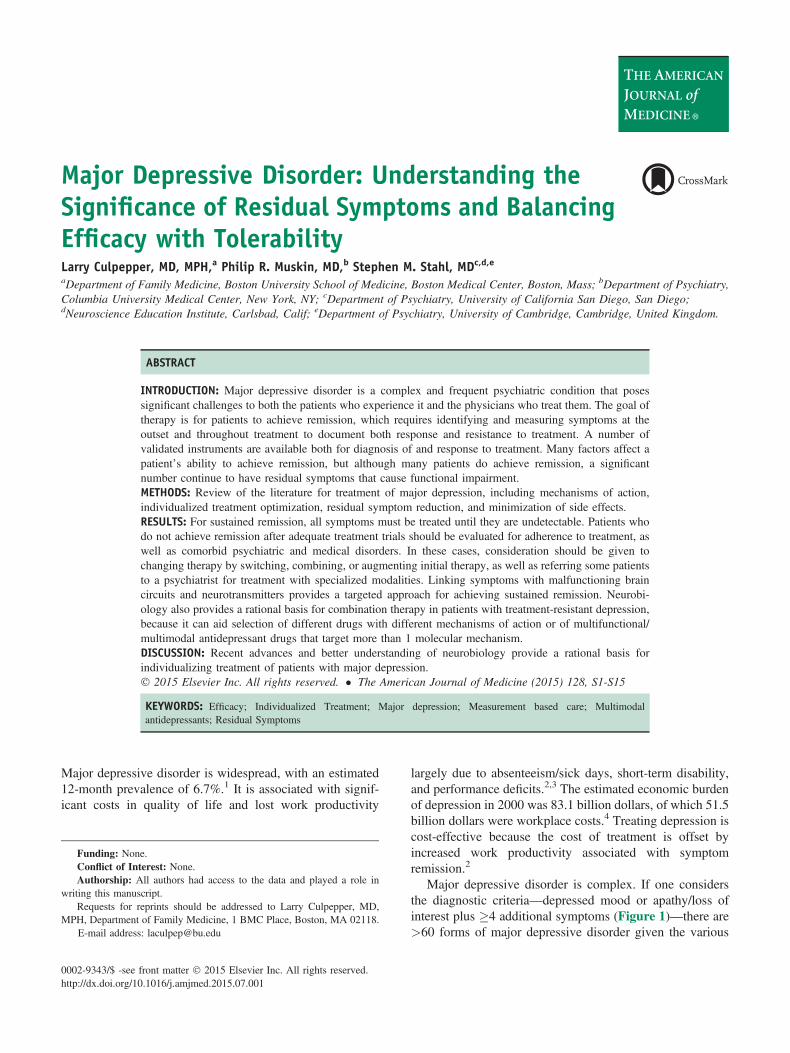
Residual Symptoms and Functional ImpairmentStudies have shown consistently that a high proportion ofpatients with major depressive disorder who experiencefull symptomatic remission still have at least 1 (median,2-4) residual symptom after treatment.14,31,32 The mostcommonly reported residual symptoms are sleep distur-bances, appetite/weight disturbances, cognitive problems,and lack of energy. Symptoms that were present duringthe course of the depressive episode also were presentapproximately half of the time during periods of remis-sion.32 A higher proportion of patients who do not experi-ence remission have residual symptoms compared withthose who achieve remission (Figure 3).19
Recent work confirms that individual depressive symp-toms have differential effects on impairments.34 Among thesymptoms shown to have strong associations with impair-ment were sadness, concentration problems, fatigue, andinterest loss, whereas hypersomnia had little association.Patients’ characteristics, including age and sex, also hadlittle association with impairment. Overall, sad mood andconcentration problems had the highest associations withimpairment and were among the most debilitating symptomsin each of the 5 domains (work impairment, home man-agement, close relationships, social activities, and privateactivities). The 3 most debilitating symptoms included
Figure 2 Proportion of patients with and without residualsymptoms: relapse after remission.13 Of patients with residualsymptoms, 76% relapsed in 10 months compared with 25% ofthose without residual symptoms, with permission from LesLaboratoires Servier.15
Table 3 Consequences of Not Achieving Remission ofDepression10-12
Disease Course Costs
� Higher risk of relapse� More rapid relapse� Increased rate ofrecurrence
� Shorter course of wellintervals
� Fewer symptom-free weeks� Increased risk of suicide
� Medical, psychiatric,emergency care
� More psychiatric hospitalizations� Increased welfare ordisability insurance benefits
� Associated work impairment
S4 The American Journal of Medicine, Vol 128, No 9A, September 2015
1 affective (sad mood), 1 cognitive (concentration prob-lems), and 1 somatic (fatigue) symptom, which suggest theneed to monitor all kinds of symptoms of depression ratherthan focusing on 1 domain or factor score.
Another factor that affects the chance of remissionis concomitant medical conditions.35 Patients with �1concomitant medical condition are likely to achieve remis-sion at 6 months, whereas the odds of achieving remissionfor patients with �4 concomitant conditions is <0.5.
The goal of treatment for major depressive disorder is forpatients to achieve sustained remission. A number of vali-dated instruments are available both for diagnosis of andresponse to treatment for major depressive disorder. Manyfactors affect a patient’s ability to achieve remission, and asignificant number of patients continue to have residualsymptoms that cause functional impairment. For sustainedremission, all symptoms must be treated until they are gone.Attaining remission is key to patients returning to fullfunctioning in their premorbid roles, including at work andin their family and social networks.
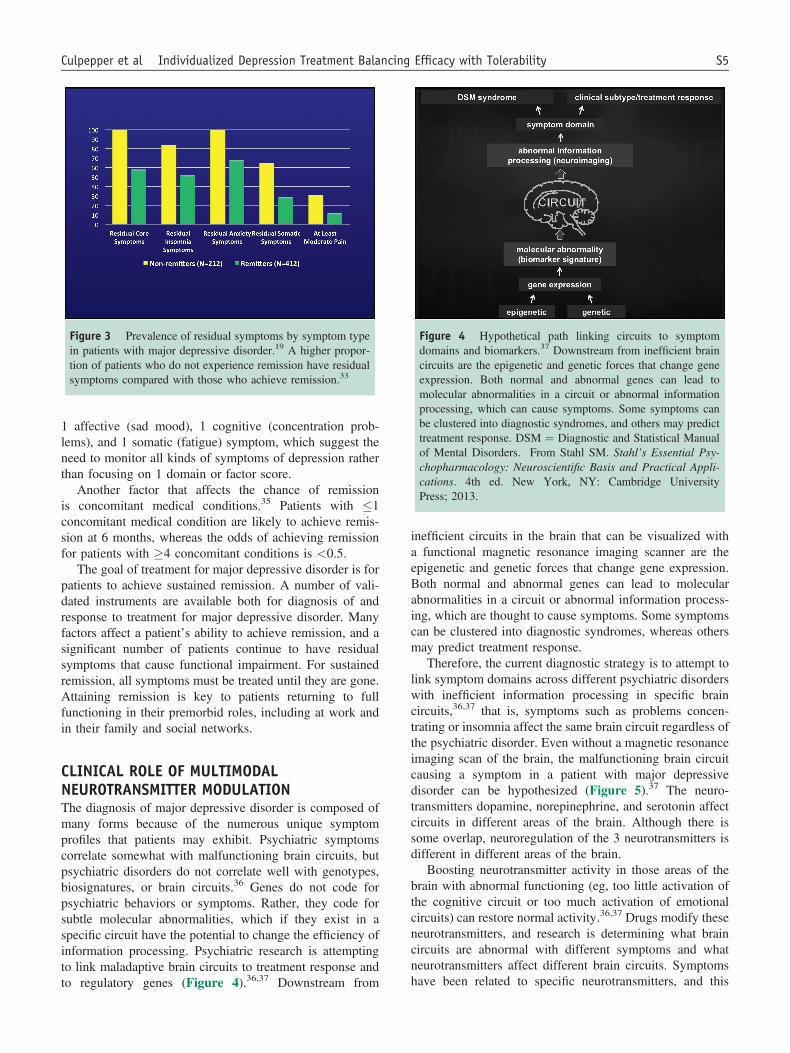
CLINICAL ROLE OF MULTIMODALNEUROTRANSMITTER MODULATIONThe diagnosis of major depressive disorder is composed ofmany forms because of the numerous unique symptomprofiles that patients may exhibit. Psychiatric symptomscorrelate somewhat with malfunctioning brain circuits, butpsychiatric disorders do not correlate well with genotypes,biosignatures, or brain circuits.36 Genes do not code forpsychiatric behaviors or symptoms. Rather, they code forsubtle molecular abnormalities, which if they exist in aspecific circuit have the potential to change the efficiency ofinformation processing. Psychiatric research is attemptingto link maladaptive brain circuits to treatment response andto regulatory genes (Figure 4).36,37 Downstream from
inefficient circuits in the brain that can be visualized witha functional magnetic resonance imaging scanner are theepigenetic and genetic forces that change gene expression.Both normal and abnormal genes can lead to molecularabnormalities in a circuit or abnormal information process-ing, which are thought to cause symptoms. Some symptomscan be clustered into diagnostic syndromes, whereas othersmay predict treatment response.
Therefore, the current diagnostic strategy is to attempt tolink symptom domains across different psychiatric disorderswith inefficient information processing in specific braincircuits,36,37 that is, symptoms such as problems concen-trating or insomnia affect the same brain circuit regardless ofthe psychiatric disorder. Even without a magnetic resonanceimaging scan of the brain, the malfunctioning brain circuitcausing a symptom in a patient with major depressivedisorder can be hypothesized (Figure 5).37 The neuro-transmitters dopamine, norepinephrine, and serotonin affectcircuits in different areas of the brain. Although there issome overlap, neuroregulation of the 3 neurotransmitters isdifferent in different areas of the brain.
Boosting neurotransmitter activity in those areas of thebrain with abnormal functioning (eg, too little activation ofthe cognitive circuit or too much activation of emotionalcircuits) can restore normal activity.36,37 Drugs modify theseneurotransmitters, and research is determining what braincircuits are abnormal with different symptoms and whatneurotransmitters affect different brain circuits. Symptomshave been related to specific neurotransmitters, and this
Figure 3 Prevalence of residual symptoms by symptom typein patients with major depressive disorder.19 A higher propor-tion of patients who do not experience remission have residualsymptoms compared with those who achieve remission.33
Figure 4 Hypothetical path linking circuits to symptomdomains and biomarkers.37 Downstream from inefficient braincircuits are the epigenetic and genetic forces that change geneexpression. Both normal and abnormal genes can lead tomolecular abnormalities in a circuit or abnormal informationprocessing, which can cause symptoms. Some symptoms canbe clustered into diagnostic syndromes, and others may predicttreatment response. DSM ¼ Diagnostic and Statistical Manualof Mental Disorders. From Stahl SM. Stahl’s Essential Psy-chopharmacology: Neuroscientific Basis and Practical Appli-cations. 4th ed. New York, NY: Cambridge UniversityPress; 2013.
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S5
may be useful in individualizing treatment (Table 4).38-40
It may be necessary to try a drug that targets a differentneurotransmitter if the symptom does not resolve, or it maybe necessary to target all 3 neurotransmitters.
Molecular TargetsThere are 5 potential molecular targets for psychotropicdrugs. Approximately 30% of psychotropic drugs and 90% ofantidepressants target the 12-transmembrane region trans-porter (Figure 6).5,41 Serotonin, dopamine, and norepi-nephrine reuptake inhibitors all target the 12-transmembraneregion transporter. Psychotropic drugs that act at G-proteinlinked receptors often are added to antidepressant drugs.Psychotropic drugs acting on ligand-gated and voltage-gatedion channels are sometimes used to treat anxiety and bipolardisorder.
Psychotropic drugs may have a single mode of action,may be multifunctional, or may be multimodal.5,41 Exam-ples of antidepressants with a single or selective mode ofaction include the selective serotonin reuptake inhibitors,which selectively inhibit the 12-transmembrane regiontransporter, and the monoamine oxidase inhibitors, whichtarget an enzyme. Although they have a single mode ofaction, they also may have downstream effects that increaseall 3 neurotransmitters.
Multifunctional and multimodal psychotropic drugshave more than 1 mode of action.5,41 A multifunctionalantidepressant class is the serotonin-norepinephrine
reuptake inhibitors, which block 2 neurotransmitter pumps.Several atypical antipsychotic drugs block numerousG-protein linked receptors, including aripiprazole andquetiapine, and are approved for augmentation of antide-pressant drugs. Multimodal psychotropic drugs affect 2different molecular targets, such as a neurotransmitterpump and a G-protein linked receptor. Examples ofmultimodal antidepressants are the serotonin partialagonist reuptake inhibitor vilazodone, vortioxetine (whichtargets 5 different receptors with 3 modes of action), andagomelatine, which is a melatonergic agonist and serotoninantagonist.42-44 The benefit of using a drug with multi-modal action is to administer 1 drug with 2 modes of actionrather than 2 drugs.
Combination Treatment Based on NeurobiologyIt is notable that all antidepressants are similarly effective:Approximately one third of patients get better with theirfirst-line therapy.45 The challenge is what to do for thosepatients who do not respond to initial therapy. It is importantto treat the residual symptoms by switching to a drug with adifferent mechanism of action or by adding a second drugwith a different mechanism of action based on the potentialmolecular targets discussed earlier.
Brain circuits are regulated by more than 1 neurotrans-mitter, suggesting that perhaps combination treatment formajor depressive disorder is justified on the basis ofneurobiology. There is evidence that combining drugs withdifferent mechanisms is effective when a single mechanismfails.45-47 It is not so much about which drug to add, butmore about when to initiate combination therapy. Any of theantidepressant drugs are more effective earlier in the courseof depression, and no drug works well after several failedtreatments. Interest has shifted to giving the most effectivetreatments first, either alone or in combination, which isanalogous to the treatment of tuberculosis, human immu-nodeficiency virus infection, or cancer for which multipledrugs may be given early.
Figure 5 Match each diagnostic symptom for a majordepressive episode to hypothetically malfunctioning brain cir-cuits.37 The same topographic area or circuit of the brain isresponsible for specific symptoms regardless of the psychiatricdisorder. For example, sleep and appetite disturbances involvethe hypothalamus, and mood disturbances involve anotherarea of the brain. A ¼ Amygdala; BF ¼ Basal forebrain;C ¼ Cerebellum; H ¼ Hippocampus; Hy ¼ Hypothalamus;NA ¼ nucleus accumbens; NT ¼ brainstem neurotransmittercenters; PFC ¼ Prefrontal cortex; S ¼ Striatum; T ¼ Thalamus.From Stahl’s Essential Psychopharmacology, 4th ed. 2013,copyright Neuroscience Education Institute, with permission.
Table 4 Common Residual Symptoms by NeurotransmitterActivity38-40
Serotonin Related� Anxiety� Inhibited communication� Dysfunctional attitude� High neuroticism* Social maladjustment* Insomnia� Psychic and somatic anxiety
� Guilt and loweredself-esteem
� Hopelessness� Impaired work andinterests
� Psychosocial disability� Sexual symptoms� Anhedonia� Lack of motivation
Norepinephrine Related* Excessive reactivity to social stress� Fatigue
� Interpersonal friction� Irritability
S6 The American Journal of Medicine, Vol 128, No 9A, September 2015
A double-blind trial of 105 patients who met the Diag-nostic and Statistical Manual of Mental Disorders IV criteriafor major depressive disorder assessed whether combinationtherapy from initiation of treatment was superior to single-drug therapy.48 Patients were randomized to 6 weeks oftreatment with fluoxetine (20 mg/d) alone or mirtazapine (30mg/d) in combination with fluoxetine (20 mg/d) or bupro-pion (150 mg/d) or venlafaxine (225 mg/d titrated in 14days). The reduction in the HAM-D score was significantly(P ¼ .011) greater with the combination regimens than withfluoxetine monotherapy. The proportion of patients achievingsustained remission (HAM-D score, �7) was significantlygreater for the mirtazapine/fluoxetine (52%) and mirtaza-pine/venlafaxine (58%) combinations but not for the mirta-zapine/bupropion (46%) compared with fluoxetinemonotherapy (25%). Combination regimens were as welltolerated as fluoxetine monotherapy. This study demon-strates the benefit of targeting multiple molecular targets atthe initiation of treatment for major depressive disorder:Fluoxetine targets the serotonin pump, whereas mirtazapinetargets G-protein linked receptors and venlafaxine targetsboth serotonin and norepinephrine pumps.
A second single-blind randomized study evaluatedacute (12 weeks) and long-term (7 months) outcomes with
escitalopram (�20 mg/d) plus placebo monotherapy com-pared with those of combination regimens of escitalopram(�20 mg/d) and sustained-release bupropion (�400 mg/d)or mirtazapine (�45 mg/d) and venlafaxine (�300 mg/d).49
Remission rates at both 12 weeks and 7 months were similaramong the groups: 12 weeks, 38.8% for escitalopram-placebo vs 38.9% for escitalopram-bupropion vs 37.7%for mirtazapine-venlafaxine. At 7 months, remission ratesranged from 41.8% to 46.6%. Unlike in the previousstudy, combination regimens were not as well tolerated asescitalopram monotherapy. Severe or intolerable adverseevents were reported by 4.2% of patients treated withescitalopram vs 10.0% of patients treated with escitalopram-bupropion and 15.2% of patients treated with mirtazapine-venlafaxine.
Therefore, clinical trial results are mixed regarding theuse of combination therapy in treatment-naive patients anddo not support its use at initiation of therapy because theriskebenefit ratio tends to favor monotherapy. However,combination therapy is becoming more common practicein patients with prior treatment failures. Combiningmechanisms of action provides a synergistic effectparticularly for those patients who have failed on 1 or 2drugs.45 Combining psychotherapy or cognitive behavioral
Figure 6 The 5 molecular targets of psychotropic drugs.5,41 Approximately 30% of psychotropicdrugs and 90% of antidepressants target the 12-transmembrane region transporter. Another 30% ofpsychotropic drugs are G-protein linked, and these often are added to antidepressants. Othermolecular targets targeted by fewer psychotropic drugs are enzyme inhibitors, which include themonoamine oxidase inhibitors, as well as the 6-transmembrane region voltage gated ion channeland the 4-transmembrane region ligand-gated ion channel transporters. From Stahl SM. Stahl’sEssential Psychopharmacology: Neuroscientific Basis and Practical Applications. 4th ed. NewYork, NY: Cambridge University Press; 2013, with permission.
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S7
therapy with psychopharmacology also may be effectivebecause it combines different mechanisms.45,50,51 Anotherway to target several mechanisms yet prescribe only 1 drugis to use multifunctional or multimodal antidepressantdrugs.
Neurobiology provides a rational basis for individual-izing treatment of patients with major depressive disorder.Linking symptoms with malfunctioning brain circuits andneurotransmitters provides a targeted approach for achievingsustained remission. Neurobiology also provides a rationalbasis for combination therapy by prescribing 2 differentdrugs with different mechanisms of action or by usingmultifunctional/multimodal antidepressant drugs becausethey target different molecular target mechanisms.
IMPROVING OUTCOMESDespite advances in our understanding of the science ofmajor depressive disorder and its treatment, 75% to 90% ofpatients experience >1 episode of depression. As thenumber of recurrences increase, there is a tendency forepisodes to increase in frequency and become less respon-sive to treatment.52 Table 3 lists the consequences ofnot achieving remission in major depressive disorder.10-12
Obstacles to attaining remission include both physiciansand patients settling for a treatment response although thepatients may still be experiencing residual symptoms, poortolerance to drug treatment, medication dose or length oftherapy, or the failure to recognize residual symptoms.52,53
In addition to antidepressant drugs, nonpharmacologicapproaches such as support, exercise, informal counseling,and psychotherapy are beneficial in patients with a majordepressive episode.54,55
Because all antidepressant drugs have similar efficacyrates and mechanisms of action, other factors affect treat-ment choices (Table 5).54 The perceptions of the patient orfamily and friends regarding a specific antidepressant theyhave received may influence the patient’s comfort levelwith taking that medication. Comorbidities and other drugsthat the patient is taking affect treatment decisions for adepressive episode. After selecting therapy, frequentfollow-up is necessary for managing both efficacy andtolerability of the drug (Table 6).56 It is important to pro-vide education and occasionally provide educational
materials at the initial visit. This aids in ensuring that thepatient recognizes that depression is a biological illness, thatthe drugs to treat depression can increase suicidality, andthat they have the potential to cause adverse effects before atherapeutic effect. At 2 to 3 weeks, after an initial responseto therapy, patients may realize that troublesome side effectsare not going away. It may be necessary to considerchanging drug therapy. At 3 to 6 weeks, patients should benoticeably improved, but there may be a need to change thedrug or adjust dosing. Continued monitoring shouldcontinue out to 12 weeks with considerations for changingtherapy or adding nonpharmacologic therapies such aspsychotherapy if there is only a partial response. If thepatient achieves a full response, the patient enters thecontinuation phase of treatment.
Approximately two thirds of patients have residualsymptoms after 12 weeks of treatment, and as much as20% will have severe or very severe symptoms.39,57 Manypatients have >1 symptom and will meet criteria for minoror subsyndromal depression. Residual symptoms of fatigueor mood and sleep disturbances represent dysfunctionalchanges that patients do not consider normal and add to theeconomic burden of depression.39,57,58 In addition, comor-bid anxiety is a predictor of lower remission rates.59 Themost common reasons for an inadequate response aremisdiagnosis, inappropriate treatment, or failure to addressconcurrent disorders (Table 7).60,61
Therapeutic Options for Patients withResidual SymptomsDifficult-to-treat or refractory depression can be treatedsuccessfully with many patients achieving remission.62 Forpatients who do not achieve remission after 12 weeks ofinitial therapy, there are several therapeutic options fromchanging to another antidepressant drug, to combinationantidepressant therapy, to augmentation therapies and spe-cial treatment programs (Table 8).56 It is necessary to firstevaluate those factors that may contribute to lack of treat-ment response, such as comorbid medical or psychiatric
Table 5 Factors to Consider in Antidepressant Drug Selection54
� Patient comfort level with use of medication� Efficacy of prior treatments or treatment of family members� Insurance coverage, cost to patient� Medical comorbidities� Psychiatric comorbidities� Drugedrug interactions� Side effects� Tolerability, both early and long term� Dosing and cost potential of using higher thanFDA-approved doses
FDA ¼ Food and Drug Administration.
Table 6 Active Management Guide After Initiation of Therapy
� Initial presentation— Provide education/durable material— 48- to 72-h assessment for adverse effects and suicidality
� 2-3 wks— Assess initial response, side effects, suicidality— Consider dose or treatment (same class or different
mechanism of action) change if necessary� 3-6 wks— Assess response trajectory— Consider dose or treatment (same class or different
mechanism of action) change if necessary� 6-12 wks— Further monitoring
S8 The American Journal of Medicine, Vol 128, No 9A, September 2015
conditions. After this evaluation, one could begin using the4 classic strategies for enhancing antidepressant efficacy:optimization, augmentation, combination therapy, andswitching agents.54,63 Table 9 provides an overview of theefficacy of the pharmacologic options for treatment-resistantdepression.11,54,64 Selected strategies with data for their usein major depressive disorder are discussed next.
Strategies with Clear Efficacy. Monoamine oxidaseinhibitors. The monoamine oxidase inhibitors were the firstantidepressant drugs and block monoamine oxidase-A ormonoamine oxidase-B isoenzymes. The A isoenzyme isfound in the brain but also is found throughout the body,including the intestines. The B isoenzyme is found in thebrain, lymphocytes, platelets, and norepinephrine neu-rons.65,66 Inhibition of monoamine oxidase-A in the brain isnecessary for an antidepressant effect; however, inhibitionof monoamine oxidase-A in the intestinal tract can result inextensive absorption of tyramine, which can lead to hyper-tensive crisis.54,67-69 Older monoamine oxidase inhibitorsare irreversible nonselective blockers (inhibit both A and B)and metabolize serotonin, dopamine, norepinephrine, andtyramine. Primary care physicians do not commonly pre-scribe them, in large part because of their drug and foodinteractions. Nevertheless, monoamine oxidase inhibitorsare useful drugs for patients with difficult-to-treat depressionand can be used safely because many of the interactions areoverstated.69,70
Inhibiting monoamine oxidase-B, which primarily me-tabolizes dopamine, has anti-Parkinson effects. The selec-tive monoamine oxidase-B inhibitor selegiline is prescribedfor Parkinson’s disease, and it is the first drug approved as atransdermal patch for the treatment of depression.66,68 Thearea under the 24-hour concentration time curve isapproximately the same for the 6-mg patch (dose deliveredover 24 hours) and a 10-mg oral dose.66 Because trans-dermal delivery bypasses the gastrointestinal tract and thehepatic first-pass metabolism that occurs with orallyadministered drugs, the 6 mg/24-hour selegiline patch canbe used without the dietary restrictions common formonoamine oxidase inhibitors; at higher doses, the dietary
restrictions for monoamine oxidase inhibitors are recom-mended.68 It is important to keep in mind that selegilineshares the same drugedrug interactions and medicationcontraindications as the other monoamine oxidase inhibitors(Table 10).68,69
Atypical antipsychotics. The atypical antipsychotic agents,quetiapine and aripiprazole, have been shown in clinicaltrials to augment the response to initial antidepressanttreatment.71-74 Remission rates with quetiapine extended-release 300 mg per day as adjunctive therapy were 42.5%compared with 24.5% with placebo adjunctive therapy(P < .01),71 whereas those for aripiprazole (mean dose,w11 mg/d) were approximately 25% to 26% compared with15% to 16% for placebo adjunctive therapy.72,73 The addi-tion of these drugs to preexisting therapy increases the riskof adverse effects. Common adverse effects with quetiapineinclude dry mouth, somnolence, dizziness, gastrointestinalsymptoms, insomnia, headache, and fatigue. Aripiprazolecan cause akathisia, headache, insomnia, and fatigue. Themedications are also associated with an increased risk oftardive dyskinesia, weight gain, and adverse metabolic,endocrine, and electrocardiographic effects.
Mirtazapine. Mirtazapine is a multifunctional antidepressantdrug in that it enhances release of norepinephrine and se-rotonin.54 It has been used as an across-class switch fromselective serotonin reuptake inhibitor therapy and toaugment selective serotonin reuptake inhibitor therapy,although it is not Food and Drug Administration approvedfor this use.75-77 Common adverse effects are sedation andweight gain, but it is less likely to cause sexual and sleep-related side effects than are selective serotonin reuptakeinhibitors.54
Table 7 Reasons for Inadequate Treatment Response60,61
� Misdiagnosis resulting in inappropriate treatment— Unipolar vs bipolar depression— Substance abuse— Undiagnosed medical disorder
� Inadequate treatment— Duration and dose— Poor adherence and adverse effects— Combination antidepressant use at subtherapeutic doses
� Failure to address known concurrent disorders— Alcohol or substance use disorders— General medical conditions— Other psychiatric disorders
Table 8 Possible Next Therapeutic Options for the Treatmentof Major Depressive Disorder56,63
� Switch antidepressants— Within class— Across class
� Referral for special treatments— Inpatient care— Day treatment programs— Crisis team approaches
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S9
Within-class vs across-class switch. A meta-analysis comparingwithin- vs across-class switches of selective serotonin re-uptake inhibitor therapy found that pooled remission ratesfor across-class switches (to bupropion, mirtazapine, orvenlafaxine) were greater compared with a within selectiveserotonin reuptake inhibitor class switch (28% vs 23.5%;P ¼ .007).75 Another review concluded that an across-classswitch may offer greater benefits than a within-classswitch.76
Strategies with Suggested Efficacy. S-adenosylmethionine.The nutraceutical S-adenosylmethionine works by addinga methyl group to neurotransmitters.78 It has shown promisein studies of patients with mild-to-moderate and moderate-to-severe depression, with most studies reporting a positiveeffect with doses of 400 to 1600 mg per day.79 The studies dohave methodological flaws (eg, small size, short-termanalyses). Although many of the studies did not reportadverse events, psychomotor excitation, mania, and insomnia
are among the reported behavioral-related adverse eventswith S-adenosylmethionine. Because S-adenosylmethioninereadily interacts with oxygen, only containers of foil-wrapped tablets should be purchased.
Omega-3 fatty acids. In addition to cardiovascular benefits, arecent meta-analysis showed that levels of polyunsaturatedfatty acids, including omega-3 fatty acids, are lower in pa-tients with depression.80,81 Studies have shown that addingomega-3 fatty acids to current antidepressant treatment wasmore effective than antidepressant monotherapy.82,83
Omega-3 fatty acids generally are well tolerated, but theoptimum dose is unknown. The ratio of eicosapentaenoicacid to docosahexaenoic acid is important for efficacy:supplements containing �60% eicosapentaenoic acid wereeffective for primary depression.84 The dose range foreicosapentaenoic acid was 200 to 2200 mg in excess ofdocosahexaenoic acid. There are online sites that report theeicosapentaenoic acid/docosahexaenoic acid ratio to help inselecting a suitable supplement. Omega-3 fatty acids are notapproved as a treatment for major depressive disorder.
L-methylfolate. Patients treated for depression who cannotconvert folate to L-methylfolate may have worse outcomesthan those without this abnormality. A study of 75 patientswho had an inadequate response to selective serotonin re-uptake inhibitors found that those with a genomic biomarkerassociated with an abnormality in L-methylfolate synthesisand metabolism treated with L-methylfolate supplementa-tion had significantly greater improvement in both HAM-Dscores and the Clinical Global Impressions Severity ofIllness Scale compared with patients treated with placebo.85
L-methylfolate is classified as a medical food and thereforedoes not require the same Food and Drug Administrationreview and approval as antidepressants. Additional studiesare necessary to confirm the link between depression andL-methylfolate.
Modafinil. Modafinil, a mood enhancer and wakefulnessdrug, is used in some patients with major depressive dis-order as an adjunct treatment, but it is a nonapproved use.When added to existing treatment, modafinil may resolve
Table 9 Overview of Pharmacologic Options for Treatment-Resistant Depression11,54,64
*Aripiprazole and quetiapine are approved by the Food and Drug Administration as augmentation agents only, not as monotherapy.†Not approved by the Food and Drug Administration for the treatment of major depressive disorder, either as monotherapy or in combination.
Table 10 Medications Contraindicated with MonoamineOxidase Inhibitors Because of DrugeDrug Interactions68
S10 The American Journal of Medicine, Vol 128, No 9A, September 2015
symptoms of depression in patients with residual symptomsof somnolence and fatigue.11,64,86
Bupropion and buspirone. Both bupropion and buspironewere evaluated as augmentation therapy to citalopram in theSequenced Treatment Alternatives to Relieve Depressionstudy.87 Remission rates based on HAM-D scores wereapproximately 30% for both drugs. The higher remissionrates based on the self-reported QIDS scores for bupropion(39% and 33%, bupropion and buspirone) and the lowerQIDS total scores at the end of the study suggest thatbupropion use may be more advantageous. Neither drug isapproved for augmentation therapy of major depression.
Strategies with Unclear Efficacy. Pindolol. The resultsare mixed for pindolol, a serotonin receptor antagonist, as anaugmentation strategy for patients receiving selective sero-tonin reuptake inhibitor therapy.88,89 A meta-analysis ofpindolol plus selective serotonin reuptake inhibitor therapyfound that outcomes favored pindolol early (at 2 weeks) inthe treatment but not at 4 to 6 weeks.90 Efficacy and safetyoutcomes do not suggest a role for pindolol as augmentationtherapy, and it is not approved for this use.
Switch antidepressants. Switching within or to a differentantidepressant class may increase remission rates andminimize the risks associated with polypharmacy.54 Pa-tients who switch from one selective serotonin reuptakeinhibitor to another have a 40% to 70% chance ofresponding to a second selective serotonin reuptake in-hibitor.91 In one study of a switch from tricyclic antide-pressant to selective serotonin reuptake inhibitor therapyand vice versa after 12 weeks of initial treatment, a further12 weeks of crossover drug therapy benefited more than50% of chronically depressed patients who had notresponded to their initial treatment.92 A switch to selectiveserotonin reuptake inhibitor therapy resulted in a higherproportion of responders than a switch to tricyclic anti-depressant therapy (60% vs 44%), and the selective sero-tonin reuptake inhibitor was better tolerated. Onlyapproximately one half of the responders achieved fullremission after the switch, that is, half had significant re-sidual symptoms after an additional 12 weeks of antide-pressant therapy. Switching antidepressant drug classesmay provide additional benefit in some patients, butadverse effects may limit patient acceptance.11
Lithium. Lithium is an older drug used to treat mania andbipolar disorder and as a mood stabilizer to prevent suicidein bipolar depression.54,93 It has been studied as anaugmentation strategy in treatment-resistant depression, butit is not approved for this use. A meta-analysis of placebo-controlled studies found that, with a minimum treatmentduration of 2 weeks, the absolute improvement in responserate was 27% with lithium augmentation therapy.94 Lithiumtherapy has disadvantages, including adverse effects(cognitive effects, weight gain, tremor), need for monitoringof blood levels to prevent lithium toxicity, and drugedrug
interactions that may lead to increased lithium levels andtoxicity.93 The studies for lithium augmentation therapy areolder and often studied tricyclic antidepressants, which arenot used commonly today. Lithium is recommended bysome clinicians64,94 but not others11 as an augmentationstrategy for treatment-resistant depression.
T3. There is an established link between thyroid function anddepression: Patients with thyroid disorders are more prone todevelop symptoms of depression, and depression may beaccompanied by abnormalities in thyroid function.95
Augmentation with T3 has been studied, but T3 is notapproved for this indication. A meta-analysis of 8 controlledclinical trials of tricyclic antidepressant augmentation with T3found a 23% absolute improvement in response rates with T3augmentation; however, limiting the analysis to 4 double-blindcontrolled studies yielded no significant effect for T3 augmen-tation.96 An analysis of double-blind studies of selective sero-tonin reuptake inhibitor augmentation with T3 concluded thatsimultaneous initiation of T3 and selective serotonin reuptakeinhibitor therapy is not significantly more likely to accelerate aclinical response in patients with depression compared withselective serotonin reuptake inhibitor monotherapy.97
Studies comparing lithium and T3 as augmentationstrategies show improvement over tricyclic antidepressant orselective serotonin reuptake inhibitor monotherapy. A small,2-week, randomized controlled study of tricyclic antide-pressant augmentation found similar improvement inresponse rates (HAM-D score <10 or �50% reduction inHAM-D score) with T3 (10/17 patients) and lithium (9/17patients).98 A 14-week study of selective serotonin reuptakeinhibitor augmentation with T3 or lithium as a third-steptreatment for major depressive disorder reported remissionrates of 24.7% with T3 and 15.9% with lithium.99 Asignificantly higher proportion of patients randomized tolithium compared with T3 discontinued treatment becauseof adverse effects (23.2% vs 9.6%; P ¼ .027). Augmenta-tion with lithium or T3 may be a useful strategy for somepatients with treatment-resistant depression, but neither isapproved for this indication.
Nonpharmacologic Interventions. Some patients initiallytreated by primary care physicians will require referral to apsychiatrist. Patients to consider for referral are those whohave severe depression or are suicidal, have a history oftreatment resistance, have comorbidities (eg, substanceabuse, personality disorder, eating disorder), or need mo-dalities not available to primary care physicians (inpatient orday hospital care, intensive community support team,specialized interventions).
New treatment modalities used by psychiatrists that mayameliorate treatment-resistant depression include repetitivetranscranial magnetic stimulation, electroconvulsive ther-apy, magnetic seizure therapy, vagal nerve stimulation, anddeep brain stimulation.100 Of these, repetitive transcranialmagnetic stimulation is the least invasive and has beenshown to provide significant benefit in short-term studies.101
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S11
A meta-analysis of 24 studies reported pooled response andremission rates of 25% and 17%, respectively, with repeti-tive transcranial magnetic stimulation compared with 9%and 6% response and remission rates, respectively, for shamtreatment.101 Discontinuations from treatment due toadverse events were low.
Continuation/Maintenance Treatment. After achievingremission, patients should continue therapy for an additional6 to 9 months.56 Patients with multiple (�3) lifetime episodesof depression, or 2 episodes if 1 was severe or difficult to treat,may require an even longer treatment period. Other factorsthat may necessitate a longer duration of maintenance therapyare brief remission periods between episodes, incompleteinter-episode recovery, treatment resistance during the cur-rent episode, and patient preference. The same drug at thesame dose should be continued asmaintenance treatment, andconsideration may be given to adjunctive cognitive behav-ioral therapy or interpersonal psychotherapy. Patients shouldcontinue to be monitored and treated for adverse events, re-sidual symptoms, and withdrawal symptoms, as well as otherpsychiatric and medical problems. Psychoeducation,including management of inter-current life events andrecognition of recurrence of depression, adverse events, re-sidual symptoms, and withdrawal symptoms, should beprovided to patients during maintenance treatment.
Patient Adherence. Adherence to antidepressant treatmentis not optimal. Studies report 25% to 42% of patients dis-continue therapy within 1 month, and up to 72% discontinuetherapy within 3 months.102-104 Use of newer antidepres-sants with improved adverse event profiles and educationregarding antidepressant drug use (eg, take daily, require 2-4weeks for noticeable effect, continue even if feel better,do not stop without consulting physician) help improveadherence with therapy. Adherence to antidepressant treat-ment in older adults may be affected by visual and auditoryimpairments, memory deficits, medication regimen com-plexity due to comorbid conditions, and a sense of hope-lessness and despair.
Treatment beliefs and patientephysician communicationinfluence patient adherence. One study identified thedemographic and clinical characteristics that accounted forpatient beliefs about antidepressants, characteristics thatinfluence adherence to treatment (Figure 7).105 Youngerpatients are more likely to be at risk for poor adherencebecause of their harmful beliefs. Frequent physician contact(eg, �3 follow-up visits) was shown in one study toimprove adherence with the initially prescribed antidepres-sant, as well as discussions about expected duration oftherapy and patient willingness to discuss adverse effects.106
Multifaceted interventions that increase the intensity(medication monitoring, patient education) and frequency of
Figure 7 Factors explaining antidepressant beliefs.105 Lower adherence to antidepressantmedication use is associated with beliefs that are harmful, whereas higher adherence is associatedwith necessity beliefs. Older patients are more likely to have necessity beliefs, whereas youngerpatients tend to have harmful beliefs about antidepressant use. Aikens JE, Nease DE Jr, KlinkmanMS. Explaining patients’ beliefs about the necessity and harmfulness of antidepressants. Ann FamMed. 2008;6:23-29, with permission from Annals of Family Medicine, Inc.
S12 The American Journal of Medicine, Vol 128, No 9A, September 2015
visits (2 with primary care physician, 2 with psychiatrist)during the initial 6 weeks of treatment improve adherenceand outcome measures compared with usual care by aprimary care physician.107
Improving outcomes in patients with major depressivedisorder requires identifying and measuring symptoms at theoutset and throughout treatment to document remission orresistance to treatment. Adequate treatment trials of anti-depressant therapy (sufficient dose and duration) arenecessary to achieve remission. If patients do not achieveremission, they should be evaluated for adherence to treat-ment and comorbid psychiatric and medical disorders, andconsideration should be given to changing therapy byswitching, combining, or augmenting initial therapy. It maybe necessary to refer some patients to a psychiatrist fortreatment with specialized modalities. Once patients achieveremission, it is important to continue with maintenancetherapy.
CONCLUSIONSMajor depressive disorder is complex, taking many formsbecause of the various possible unique symptom combina-tions. Although the desired outcome of treatment is remis-sion of all symptoms, a high proportion of patients whoachieve remission have at least 1 residual symptom.Symptoms of depression that have strong associationswith functional impairments include sad mood, difficultyconcentrating, fatigue, and loss of interest, and these add tothe economic burden of depression. All antidepressant drugshave similar efficacy, although some may not be effectivein a given patient. A better understanding of the neurobi-ology of depression now provides a rationale for how toindividualize drug selection both initially and in patientswith treatment-resistant depression to optimize outcomes.It is now known that symptom domains correlate some-what with malfunctioning brain circuits and that restoringneurotransmitter activity in the circuits with impairedinformation processing restores function. Applying neuro-biology principles to treatment selections may assist physi-cians in determining whether to switch antidepressants,add another antidepressant medication, or augment antide-pressant therapy with another pharmacologic agent ora nonpharmacologic treatment such as psychotherapy.Throughout a treatment course for major depressive disor-der, antidepressant medications must be given for a suffi-cient duration at a sufficient dose and patients monitoredfor response to and adverse events with treatment andpsychiatric and medical comorbidities. Patients withresidual symptoms or treatment-resistant depression canachieve complete remission of their symptoms and regainfunctionality.
and comorbidity of twelve-month DSM-IV disorders in the National
Comorbidity Survey Replication (NCS-R). Arch Gen Psychiatry.2005;62:617-627.
2. Kessler RC, Barber C, Birnbaum HG, et al. Depression in the work-place: effects on short-termdisability.Health Affairs. 1999;18:163-171.
3. Adler DA, McLaughlin TJ, Rogers WH, Chang H, Lapitsky L,Lerner D. Job performance deficits due to depression. Am J Psychi-atry. 2006;163:1569-1576.
4. Greenberg PE, Kessler RC, Birnbaum HG, et al. The economic burdenof depression in the United States: how did it change between 1990 and2000? J Clin Psychiatry. 2003;64:1465-1475.
5. Stahl SM. Stahl’s Essential Psychopharmacology: NeuroscientificBasis and Practical Applications. 4th ed. New York, NY: CambridgeUniversity Press; 2013.
6. McIntyre RS, Fallu A, Konarski JZ. Measurable outcomes in psy-chiatric disorders: remission as a marker of wellness. Clin Ther.2006;28:1882-1891.
7. Zimmerman M, McGlinchey JB, Posternak MA, Friedman M,Attiulah N, Boerescu D. How should remission from depression bedefined? The depressed patient’s perspective. Am J Psychiatry.2006;163:148-150.
8. Fava GA, Ruini C, Belaise C. The concept of recovery in majordepression. Psychol Med. 2007;37:307-317.
9. Miller IW, Keitner GI, Schatzberg AF, et al. Psychosocial functioningbefore and after treatment with sertraline or imipramine. J Clin Psy-chiatry. 1998;59:608-619.
10. Judd LL, Paulus MJ, Schettier PJ, et al. Does incomplete recoveryfrom first lifetime major depressive episode herald a chronic course ofillness? Am J Psychiatry. 2000;157:1501-1504.
11. Papakostas GI. Managing partial response or nonresponse: switching,augmentation, and combination strategies for major depressive dis-order. J Clin Psychiatry. 2009;70(suppl 6):16-25.
12. Thase ME. Update on partial response in depression. J Clin Psychi-atry. 2009;70(suppl 6):4-9.
13. Paykel ES. Residual symptoms and relapse in depression. Medi-cographia. 2009;31:157-163.
14. Nierenberg AA, Husain MM, Trivedi MH, et al. Residual symptomsafter remission of major depressive disorder with citalopram and riskof relapse: a STAR*D report. Psychol Med. 2010;40:41-50.
15. Paykel ES, Ramana R, Cooper Z, Hayhurst H, Kerr J, Barocka A.Residual symptoms after partial remission: an important outcome indepression. Psychol Med. 1995;25:1171-1180.
16. Mrazek DA, Hornberger JC, Altar CS, Degtiar I. A review of theclinical, economic, and societal burden of treatment-resistant depres-sion: 1996-2013. Psychiatr Serv. 2014;65:977-987.
17. Trivedi MH, Corey-Lisle PK, Guo Z, Lennox RD, Pikalov A, Kim E.Remission, response without remission, and nonresponse in majordepressive disorder: impact on functioning. Int Clin Psychopharma-col. 2009;24:133-138.
18. McKnight PE, Kashdan TB. The importance of functional impairmentto mental health outcomes: a case for reassessing our goals indepression treatment research. Clin Psychol Rev. 2009;29:243-259.
19. Romera I, Pérez V, Quail D, Berggren L, Lenox-Smith A, Gilaberte I.Individual residual symptoms and functional impairment in patientswith depression. Psychiatry Res. 2014;220:258-262.
20. Romera I, Pérez V, Menchón JM, Polavieja P, Gilaberte I. Optimalcutoff point of the Hamilton Rating Scale for Depression according tonormal levels of social and occupational functioning. Psychiatry Res.2011;186:133-137.
21. Zimmerman M, McGlinchey JB, Posternak MA, Friedman M,Boerescu D, Attiulah N. Differences between minimally depressedpatients who do and do not consider themselves to be in remission.J Clin Psychiatry. 2005;66:1134-1138.
22. Zimmerman M, Posternak MA, Chelminski I. Is the cutoff to defineremission on the Hamilton Rating Scale for Depression too high?J Nerv Ment Dis. 2005;193:170-175.
23. Trivedi MH. Evaluating and monitoring treatment response indepression using measurement-based assessment and rating scales.J Clin Psychiatry. 2013;74:e14.
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S13
24. Sheehan KH, Sheehan DV. Assessing treatment effects in clinicaltrials with the Discan metric of the Sheehan Disability Scale. Int ClinPsychopharmacol. 2008;23:70-83.
25. Spitzer RL, Kroenke K, Williams JBW, the Patient Health Ques-tionnaire Primary Care Study Group. Validation and utility of a self-report version of PRIME-MD: the PHQ Primary Care Study. JAMA.1999;282:1737-1744.
26. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic andseverity measure. Psychiatric Ann. 2002;32:1-7.
27. Angstman KB, Rasmussen NH, MacLaughlin KL, Staab JP. Inter-relationship of the functional status question of the PHQ-9 anddepression remission after six months of collaborative care manage-ment. J Psychiatr Res. 2013;47:418-422.
28. Daly EJ, Trivedi MH, Wisniewski SR, et al. Health-related quality oflife in depression: a STAR*D report. Ann Clin Psychiatry. 2010;22:43-55.
29. Mundt JC, Marks IM, Shear MK, Greist JH. The Work and SocialAdjustment Scale: a simple measure of impairment in functioning. BrJ Psychiatry. 2002;180:461-464.
30. Endicott J, Nee J, Harrison W, Blumenthal R. Quality of life enjoy-ment and satisfaction questionnaire: a new measure. Psychopharma-col Bull. 1993;29:321-326.
31. Iovieno N, van Nieuwenhuizen A, Clain A, Baer L, Nierenberg AA.Residual symptoms after remission of major depressive disorder withfluoxetine and risk of relapse. Depress Anxiety. 2011;28:137-144.
32. Conradi HJ, Ormel J, de Jonge P. Presence of individual (residual)symptoms during depressive episodes and periods of remission: a3-year prospective study. Psychol Med. 2011;41:1165-1174.
33. Romera I, Pérez V, Ciudad A, et al. Residual symptoms and func-tioning in depression, does the type of residual symptom matter? Apost-hoc analysis. BMC Psychiatry. 2013;13:51.
34. Fried EI, Nesse RM. The impact of individual depressive symptoms onimpairment of psychosocial functioning. PLoS One. 2014;9:e90311.
35. Muskin PR. Major depressive disorder and other medical illness: atwo-way street. Ann Clin Psychiatry. 2010;22(suppl 3):S15-S20.
36. Stahl SM. Psychotherapy as an epigenetic ‘drug’: psychiatric thera-peutics target symptoms linked to malfunctioning brain circuits withpsychotherapy as well as with drugs. J Clin Pharmacol Ther.2012;37:249-253.
37. Stahl SM. The last Diagnostic and Statistical Manual (DSM):replacing our symptom-based diagnoses with a brain circuit-basedclassification of mental illness. CNS Spectrums. 2013;18:65-68.
38. Shelton RC, Tomarken AJ. Can recovery from depression be ach-ieved? Psychiatric Serv. 2001;52:1469-1478.
39. Nierenberg AA, Keefe BR, Leslie VC, et al. Residual symptoms indepressed patients who respond acutely to fluoxetine. J Clin Psychi-atry. 1999;60:221-225.
40. Nierenberg AA, DeCecco LM. Definitions of antidepressant treatmentresponse, remission, nonresponse, partial response, and other relevantoutcomes: a focus on treatment-resistant depression. J Clin Psychia-try. 2001;62(suppl 16):5-9.
41. Stahl SM. Classifying psychotropic drugs by mode of action and notby target disorder. CNS Spectrums. 2013;18:113-117.
42. Stahl SM. Mechanism of action of the SPARI vilazodone: serotonin1A partial agonist and reuptake inhibitor. CNS Spectrums. 2014;19:105-109.
43. Montgomery SA, Nielson RZ, Poulsen LH, Häggström L.A randomized, double-blind study in adults with major depressivedisorder with an inadequate response to a single course of selectiveserotonin reuptake inhibitor or serotoninenoradrenaline reuptake in-hibitor treatment switched to vortioxetine or agomelatine. HumanPsychopharmacol. 2014;29:470-482.
44. Pehrson AL, Sanchez C. Serotonergic modulation of glutamateneurotransmission as a strategy for treating depression and cognitivedysfunction. CNS Spectrums. 2014;19:121-123.
45. Schwartz TL, Stahl SM. Optimizing antidepressant management ofdepression: current status and future perspectives. Mod TrendsPharmacopsychiatry. 2010;27:254-267.
46. Stahl SM. Combining antidepressant therapies from initiation oftreatment: a paradigm shift for major depression. J Clin Psychiatry.2009;70:1493-1494.
47. Stahl SM. Enhancing outcomes from major depression: using anti-depressant combination therapies with multifunctional pharmacologicmechanisms from the initiation of treatment. CNS Spectrums.2010;15:79-94.
48. Blier P, Ward HE, Tremblay P, Laberge L, Hébert C, Bergeron R.Combination of antidepressant medications from treatment initiationfor major depressive disorder: a double-blind randomized study. Am JPsychiatry. 2010;167:281-288.
49. Rush AJ, Trivedi MH, Stewart JW, et al. Combining medicationsto enhance depression outcomes (CO-MED): acute and long-termoutcomes of a single-blind randomized study. Am J Psychiatry.2011;168:689-701.
50. Wiles N, Thomas L, Abel A, et al. Clinical effectiveness and cost-effectiveness of cognitive behavioural therapy as an adjunct to phar-macotherapy for treatment-resistant depression in primary care: theCoBalT randomized controlled trial. Heath Technol Assess. 2014;18:1-167.
51. Hollon SD, DeRubeis RJ, Fawcett J, et al. Effect of cognitive therapywith antidepressant medications vs antidepressants alone on the rate ofrecovery in major depressive disorder: a randomized clinical trial.JAMA Psychiatry. 2014;71:1157-1164.
52. Culpepper L (ed). Academic highlights: recognizing and treating thephysical symptoms of depression in primary care. Prim Care Com-panion J Clin Psychiatry. 2004;6:168-188.
53. Zajecka JM. Treating depression to remission. J Clin Psychiatry.2003;64(suppl 15):7-12.
54. Mann JJ. The medical management of depression. N Engl J Med.2005;353:1819-1834.
55. Tylee A. Identifying and managing depression in primary care in theUnited Kingdom. J Clin Psychiatry. 2006;67(suppl 6):41-45.
56. American Psychiatric Association (APA). Practice guidelines for thetreatment of patients with major depressive disorder. 3rd ed. Am JPsychiatry. 2010;167(suppl):1-152.
57. TrivediMH,RushAJ,Wisniewski SR, et al. Evaluationof outcomeswithcitalopram for depression using measurement-based care in Star*D:implications for clinical practice. Am J Psychiatry. 2006;163:28-40.
58. Robinson RL, Stephenson JJ, Denney EB, et al. The importance ofunresolved fatigue in depression: costs and comorbidities. Psycho-somatics. 2015;56:274-285.
59. Saveanu R, Etkin A, Duchemin AM, et al. The International Study toPredict Optimized Treatment in Depression (ISPOT-D): outcomesfrom the acute phase of antidepressant treatment. J Psychiatry Res.2015;61:1-12.
60. Hirschfeld RMA, Keller MB, Panico S, et al. The National Depressiveand Manic-Depressive Association consensus statement on theundertreatment of depression. JAMA. 1997;277:333-340.
61. Corey-Lisle PK, Nash R, Stang P, Swindle R. Response, partialresponse and nonresponse in primary care treatment of depression.Arch Intern Med. 2004;164:1197-1204.
62. Stewart JW, Delivannides DA, McGrath PJ. How treatable isrefractory depression? J Affect Disord. 2014;167:148-152.
63. Berlim MT, Fleck MP, Turecki G. Current trends in the assessmentand somatic treatment of resistant/refractory major depression: anoverview. Ann Med. 2008;40:149-159.
64. DeBattista C. Augmentation and combination strategies for depres-sion. J Psychopharmacol. 2006;20(3 suppl):11-18.
66. Patkar A, Pae CU, Massand PS. Transdermal selegiline: the newgeneration of monoamine oxidase inhibitors. CNS Spectrums.2006;11:363-365.
67. Vandenberg CM. MAOIs and transdermal delivery. J Clin Psychiatry.2012;73:e28.
68. Culpepper L, Kovalick LJ. A review of the literature on the selegilinetransdermal system: an effective and well-tolerated monoamine
S14 The American Journal of Medicine, Vol 128, No 9A, September 2015
oxidase inhibitor for the treatment of depression. Prim Care Com-panion J Clin Psychiatry. 2008;10:25-30.
69. Grady MM, Stahl SM. Practical guide for prescribing MAOIs:debunking myths and removing barriers. CNS Spectrums. 2012;17:2-10.
70. Culpepper L. Reducing the burden of difficult-to-treat major depres-sive disorder: revisiting monoamine oxidase inhibitor therapy. PrimCare Companion CNS Disorders. 2013;15(5), pii: PCC.13r01515.
71. El-Khalili N, Joyce M, Atkinson S, et al. Extended-release quetiapinefumarate (quetiapine XR) as adjunctive therapy in major depressivedisorder (MDD) in patients with an inadequate response to ongoing an-tidepressant treatment: amulticentre, randomized, double-blind, placebo-controlled study. Int J Neuropsychopharmacol. 2010;13:917-932.
72. Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety ofaripiprazole as adjunctive therapy in major depressive disorder: amulticenter, randomized, double-blind, placebo-controlled study.J Clin Psychiatry. 2007;68:843-853.
73. Marcus RN, McQuade RD, Carson WH, et al. The efficacy and safetyof aripiprazole as adjunctive therapy in major depressive disorder: asecond multicenter, randomized, double-blind, placebo-controlledstudy. J Clin Psychopharmacol. 2008;28:156-165.
74. Nelson JC, Papakostas GI. Atypical antipsychotic augmentation inmajor depressive disorder: a meta-analysis of placebo-controlledrandomized trials. Am J Psychiatry. 2009;166:980-991.
75. Papakostas GI, Fava M, Thase ME. Treatment of SSRI-resistantdepression: a meta-analysis comparing within- versus across-classswitches. Biol Psychiatry. 2008;63:699-704.
76. Connolly KR, Thase ME. If at first you don’t succeed: a review of theevidence for antidepressant augmentation, combination, and switch-ing strategies. Drugs. 2011;71:43-64.
77. Carpenter LL, Yasmin S, Price LH. A double-blind, placebo-controlled study of antidepressant augmentation with mirtazapine.Biol Psychiatry. 2002;51:183-188.
78. Bottiglieri T. Folate, vitamin B12, and s-adenosylmethionine. Psy-chiatr Clin North Am. 2013;36:1-13.
79. Carpenter DJ. St. John’s wort and s-adenosyl methionine as “natural”alternatives to conventional antidepressants in the era of the suici-dality boxed warning: what is the evidence for clinically relevantbenefit? Altern Med Rev. 2011;16:17-39.
80. Freeman MP. Omega-3 fatty acids in major depressive disorder.J Clin Psychiatry. 2009;70(suppl 5):7-11.
81. Lin PY, Huang SY, Su KP. A meta-analytic review of poly-unsaturated fatty acid compositions in patients with depression. BiolPsychiatry. 2010;68:140-147.
82. Peet M, Horrobin DF. A dose-ranging study of the effects of ethyl-eicosapentaenoate in patients with ongoing depression despiteapparently adequate treatment with standard drugs. Arch Gen Psy-chiatry. 2002;59:913-919.
83. Gertsik L, Poland RE, Bresee C, Rapaport MH. Omega-3 fatty acidaugmentation of citalopram treatment for patients with majordepressive disorder. J Clin Psychopharmacol. 2012;32:61-64.
84. Sublette ME, Ellis SP, Geant AL, Mann JJ. Meta-analysis: effects ofeicosapentaenoic acid in clinical trials in depression. J Clin Psychi-atry. 2011;72:1577-1584.
85. Papakostas GI, Shelton RC, Zajecka JM, et al. Effect of adjunctiveL-methylfolate 15 mg among inadequate responders to SSRIs indepressed patients who were stratified by biomarker levels andgenotype: results from a randomized clinical trial. J Clin Psychiatry.2014;75:855-863.
86. Fava GA, Thase ME, DeBattista C, Doghramji K, Arora S,Hughes RJ. Modafinil augmentation of selective serotonin reuptakeinhibitor therapy in MDD partial responders with persistent fatigueand sleepiness. Ann Clin Psychiatry. 2007;19:153-159.
87. Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentationafter the failure of SSRIs for depression. N Engl J Med. 2006;354:1243-1252.
88. Maes M, Libbrecht I, van Hunsel F, Campens D, Meltzer HY.Pindolol and mianserin augment the antidepressant activity offluoxetine in hospitalized major depressed patients, including thosewith treatment resistance. J Clin Psychopharmacol. 1999;19:177-182.
89. Perry EB, Berman RM, Sanacora G, Anand A, Lynch-Colonese K,Charney DS. Pindolol augmentation in depressed patients resistantto selective serotonin reuptake inhibitors: a double-blind, random-ized, controlled trial. J Clin Psychiatry. 2004;65:238-243.
90. Ballesteros J, Callado LF. Effectiveness of pindolol plus serotoninreuptake inhibitors in depression: a meta-analysis of early and lateoutcomes from randomised controlled trials. J Affect Disord. 2004;79:137-147.
91. Thase ME, Rush AJ. When at first you don’t succeed: sequentialstrategies for antidepressant nonresponders. J Clin Psychiatry.1997;58(suppl 13):23-29.
92. Thase ME, Rush AJ, Howland RH, et al. Double-blind switch study ofimipramine or sertraline treatment of antidepressant-resistant chronicdepression. Arch Gen Psychiatry. 2002;59:233-239.
93. Freeman MP, Freeman SA. Lithium: clinical considerations in internalmedicine. Am J Med. 2006;119:478-481.
94. Bauer M, Dopfmer S. Lithium augmentation in treatment-resistantdepression: meta-analysis of placebo-controlled studies. J Clin Psy-chopharmacol. 1999;19:427-434.
95. Hage MP, Azar ST. The link between thyroid function and depres-sion. J Thyroid Res. 2012;2012:1-8.
96. Aronson R, Offman HJ, Joffe RT, Naylor CD. Triiodothyronineaugmentation in the treatment of refractory depression: a meta-analysis. Arch Gen Psychiatry. 1996;53:842-848.
97. Papakostas GI, Cooper-Kazaz R, Appelhof BC, et al. Simultaneousinitiation (coinitiation) of pharmacotherapy with triiodothyronine anda selective serotonin reuptake inhibitor for major depressive disorder:a quantitative synthesis of double-blind studies. Int Clin Psycho-pharmacol. 2009;245:19-25.
98. Joffe RT, Singer W, Levitt AJ, MacDonald C. A placebo-controlledcomparison of lithium and triiodothyroninie augmentation of tricyclicantidepressants in unipolar refractory depression. Arch Gen Psychia-try. 1993;50:387-393.
99. Nierenberg AA, Fava M, Trivedi MH, et al. A comparison oflithium and T(3) augmentation following two failed medicationtreatments for depression: a STAR*D report. Am J Psychiatry.2006;163:1519-1530.
100. Kennedy SH, Giacobbe P. Treatment-resistant depression—advancesin somatic therapies. Ann Clin Psychiatry. 2007;19:279-287.
101. Lam RW, Chan P, Wilkins-Ho M, Yatham LN. Repetitive trans-cranial magnetic stimulation for treatment-resistant depression: asystematic review and metaanalysis. Can J Psychiatry. 2008;53:621-631.
102. Olfson M, Marcus SC, Tedeschi M, Wan GJ. Continuity of antide-pressant treatment for adults with depression in the United States. AmJ Psychiatry. 2006;163:101-108.
103. Simon GE, Von Korff M, Wagner EH, Barlow WL. Patterns ofantidepressant use in community practice. Gen Hosp Psychiatry.1993;15:399-408.
104. Lin EHB, Von Korff M, Katon W, et al. The role of the primary carephysician in patients’ adherence to antidepressant therapy. Med Care.1995;33:67-74.
105. Aikens JE, Nease DE Jr, Klinkman MS. Explaining patients’ beliefsabout the necessity and harmfulness of antidepressants. Ann FamMed. 2008;6:23-29.
106. Bull SA, Hu XH, Hunkeler EM, et al. Discontinuation of use andswitching of antidepressants: influence of patient-physician commu-nication. JAMA. 2002;288:1403-1409.
107. Katon K, Von Korff M, Lin E, et al. Collaborative management toachieve treatment guidelines: impact on depression in primary care.JAMA. 1995;273:1026-1031.
Culpepper et al Individualized Depression Treatment Balancing Efficacy with Tolerability S15