35
Making it happen Evonne Curran Nurse Consultant
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | tyler-stevens |
| View: | 221 times |
| Download: | 0 times |

Making it happenEvonne Curran
Nurse Consultant

Unknown but limited ingredientsVariable talent
Time limitGoal: Make the best possible output with the above
At the end of the day..... It would be good to say..
• I can show that because of me (xxxxxxxxxxxx ) – Is now performed more safely– Has improved the patient experience– Has reduced risks to the organisation – Has resulted in fewer infections– Has resulted in less waste (money, time,
resources)

LAND MINES
Lack of visionLack of informationLack of inclusionLack of strategic thinkingLack of strategic alignment Participation as an endLack of productive conflictUntested assumptionsLack of alignmentLack of communication and accommodation Focus on results – not the steps to the results http://www.rexroundtables.com/showbriefs-yplansfail.php

Very high High Moderate LowDevasting
SevereModerate
Minor
Very likely Likely Low likelihood UndetectableReduce harm / risksImprove pt experienceReduce costsFaesible
Risk assessment
Potential benefits assessment

Potential topics - what is important to
• You • Your IPCT • Those at the front line• The antimicrobial pharmacist• Those who hold the purse strings• The patients• The HAI executive lead

What makes hospital infections
• Invasive Devices– Urinary Catheter– PVCs
• Norovirus• Antibiotics• Contaminated equipment• Failure to comply with SICPs
Topic Review
• The problem?• How big is it?• What is driving the problem?• What is achievable?• Benefit Assessment?
Urinary catheters
• We use too many of them!• We keep them in too long• We don’t know about alternatives• By pass defence mechanism• Perfect culture medium• Alternatives – not accessible
– Scales to weigh urine– Female slipper pans– Suitable inco pads
Habits
• Habits emerge because the brain is constantly looking for ways to save effort (system 1 / 2 thinking)
• When a habit emerges the brain stops fully participating in decision making.– The order you wash in the morning
• Unless you deliberately fight a habit – find new routines – the habit will unfold automatically
• Habits work on cues• Habits are driven by ‘cravings’• Willpower becomes a habit when certain behaviours are
chosen ahead of time – routine followed when cue arrives
The Power of Habit – why we do what we do and how to change, Duhigg

Q How man animals of each kind did Moses take on to the ark?

Habits in healthcare just as in life
• Serve us well• Allow us to do things swiftly and
consistently• But… from time to time we need to
break old habits and create new ones
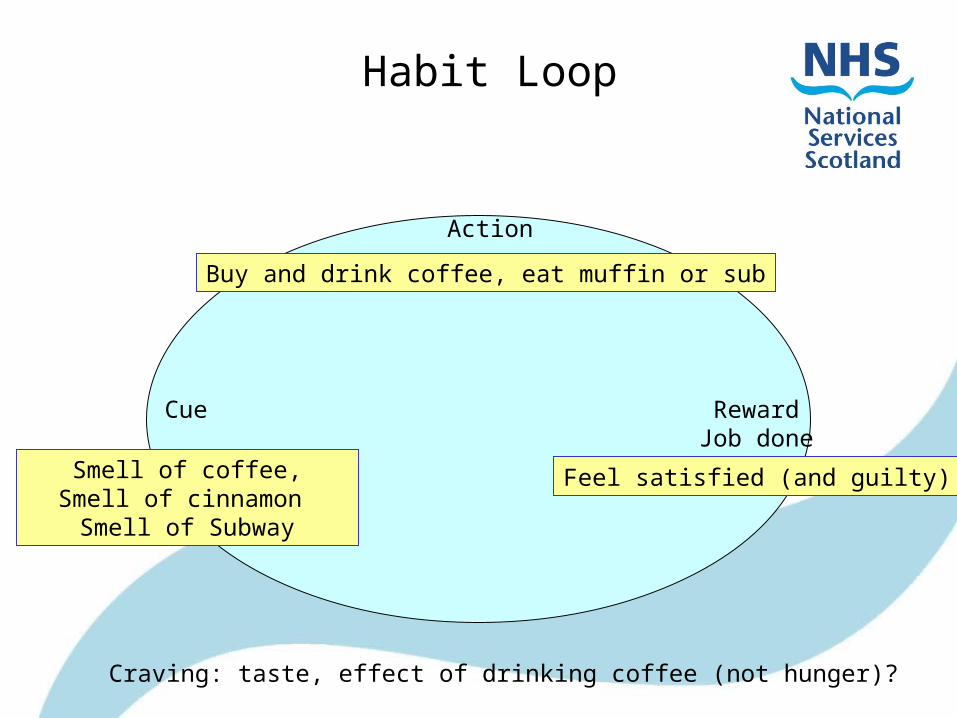
Habit Loop
Cue
Action
RewardJob done
Smell of coffee,Smell of cinnamon Smell of Subway
Buy and drink coffee, eat muffin or sub
Feel satisfied (and guilty)
Craving: taste, effect of drinking coffee (not hunger)?
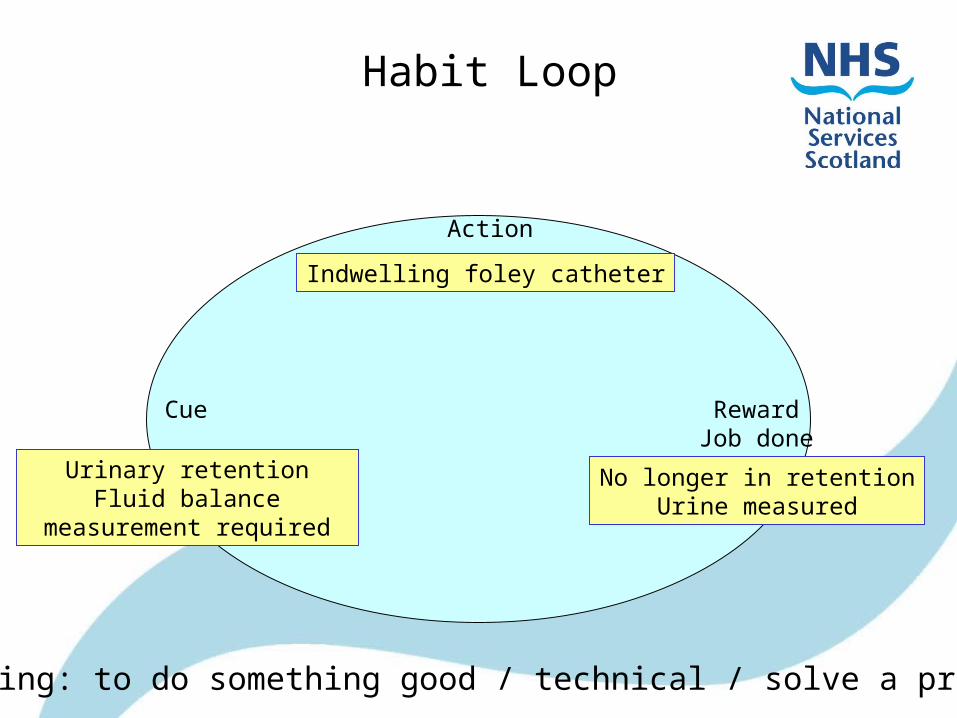
Habit Loop
Cue
Action
RewardJob done
Urinary retentionFluid balance measurement
required
Indwelling foley catheter
No longer in retentionUrine measured
Craving: to do something good / technical / solve a problem

Habit Loop• For success
– Need a new habit• Need to know and have access to alternatives
– Accurate fluid balance does not always need a catheter – scales and a bottle
– Uro-sheaths reduce infection risk– Intermittent catheters
– Need to believe that it can be achieved• Some one else has done it – group therapy • Data to show it works• Data to show it matters

How do we change habits• Need to learn new habits that overpower
the current habit behaviours• Find new routines and rewards from cues• Works for (some but not all) alcoholics• The ingredient that made a reworked habit
into a permanent behaviour – Belief
• What is our (habit) reaction to:“we are going to introduce a new initiative
to……. “
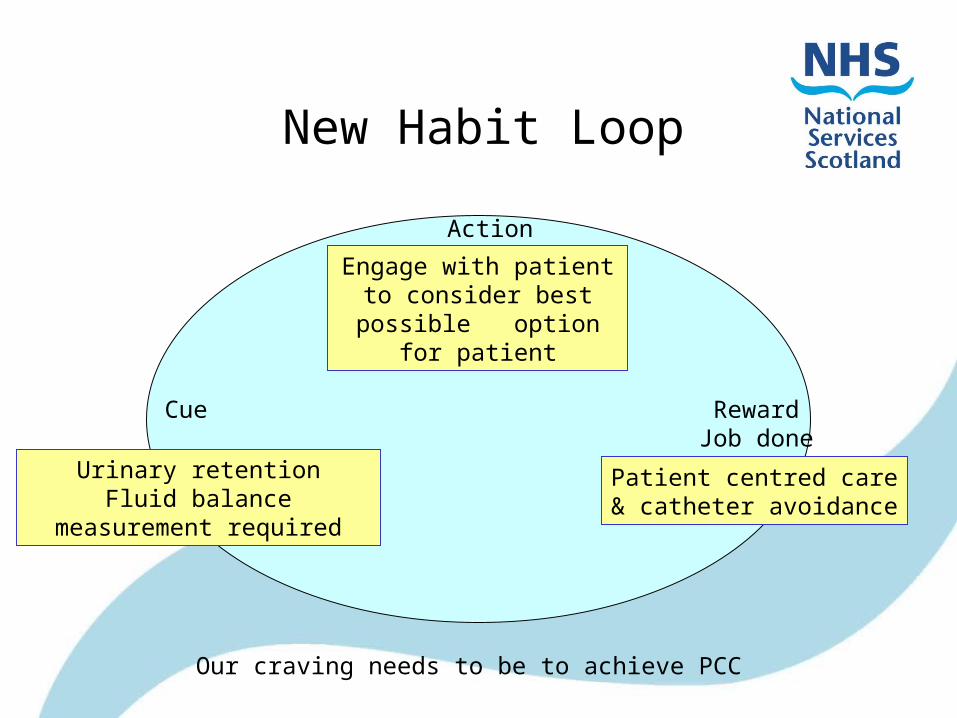
New Habit Loop
Patient centred care& catheter avoidance
Urinary retentionFluid balance measurement
required
Engage with patient to consider best possible
option for patient
RewardJob done
Cue
Action
Our craving needs to be to achieve PCC

Social Marketing
• A process that applies marketing principles and techniques to create, communicate, and deliver value in order to influence target audiences behaviours that benefit society (public health, safety, the environment and communities)
Kolter et al (2006)

If not social marketing what else?
• Education & Data feedback– Use of rational facts to persuade people
to adopt a different behaviour
• Coercion– Forces people to adopt a behaviour
under threat of penalty for not doing so
Is • A social behaviour change strategy• Most effective when it activates people• Targeted towards those who have a reason to care • Strategic and requires efficient use of resources• Integrated and works on a plan
Social marketing
Social marketing in healthcare, Radha Aras
4ps of Social Marketing• Product: Desired behaviours
– Reduction in urinary catheter usage with an increase in safer alternatives
– Increase in patient involvement in decision making– Optimisation of clinical decision making
• Price: Cost associated with the behaviour changes– Price of CA-UTI (physical and psychological)– Effort – resource required
• Place: Make it convenient – to translate the motivation into action. Intervene at the point of decision making
• Promotion: Make the new habit acceptable, easy, and desirable to the audiences
Social marketing in healthcare, Radha Aras

Lets now look at a plan to join our habit knowledge with our social
marketing knowledge
To modify a habit you need to answer these questions
• Location: where are people when the cue happens / decisions are made / first acts?
• Time: does it happen at a particular time?• Emotional state: what state are people in
when the cue arises? • Other people: who else is around to help
with decision making?• Immediate preceding action: what happens
just before the decision?
Before you start• Identify and prioritise barriers
– Don’t have easy access to alternatives– Don’t know what to use when– Don’t consider remove ASACI
• What will over come barriers– Get help from continence support– From whoever has the budget– Alternatives and placement of alternatives– Training
• Pilot• (We still need education and data)

Clear message catheters are dangerous


S T O P
Before you catheterise….

Reason to believe: Limiting urinary catheters is doable
and better for patients• 7mth pre period; 4 mth intervention period • Limit criteria set: urinary tract obstruction, hourly
output measurement, etc.• Measured
– CAUTI – Urinary catheter– Nursing experience
• UC usage decreased by 42%,CAUTI by 57% nursing satisfaction improved
Rothfeld et al AJIC 2010 38 568-71

What we do in nursing• Are learned behaviours• Habits run by – cue, action, reward• To bring about safer action
– Need different habits (that involve patients more)
– Need education on safest alternatives for patients to optimise clinical decision making
– Need easy access to the safest alternatives
– Need data that shows we provide optimal care

Habit and social marketing
• Social marketing can help deliver the message– Alternatives to catheterisation are
suitable and safer in many cases– Here are the alternatives to
catheterisation• This messaging will make the case for new
habits (create the belief) and make it easier for new habits to become established
Need to find out – what are the attitudes to the process to be
changed
• Is it a settled way of thinking or feeling, typically reflected in our behaviour?
• Or are we ready to break a habit?

Very likely Likely Low likelihood UndetectableReduce harm / risksImprove pt experienceReduce costsFaesible
Potential benefits assessment
Lets do one together
• The problem?• How big is it?• What is driving the problem?• What is achievable?• Benefit Assessment?

















