Making it Stick: Private Practice/Hospital/Agency Psychology Reports and the School Board Section for Psychologists in Education OPA Conference 2014 M.J. Gendron, M. Kokai, D. Lean, C. Lennox, P. Pires & K. Smolewska
Transcript
Making it Stick: Private Practice/Hospital/Agency Psychology Reports
and theSchool Board
Section for Psychologists in Education
OPA Conference 2014
M.J. Gendron, M. Kokai, D. Lean, C. Lennox, P. Pires & K. Smolewska
Challenges for psychology providers who work outside of District School Boards (DSBs)
Identification and Diagnosis Ontario Ministry of Education PPM 8 School Board Considerations
Agenda
Challenges for Psychology Providers Outside of DSBs
Dr. Paulo Pires & Dr. Kathy Smolewska
Psychological assessment (and possibly diagnosis) may be required to provide information to the Board about educational need
History of acquired brain injury (e.g., TBI, stroke) or other neurological or psychiatric condition, which is affecting their functioning at home and/or school
History of MVA involvement and require recommendations for cognitive/ psychological sequelae
Query Autism Spectrum Disorder
Private Practice Context
Complete a neuropsychological or psychological assessment (depends on referral question and client’s history)
Many clients do not clearly meet diagnostic criteria (or schools vary on what criteria they use)
Inform parents that our recommendations are not guaranteed – it is up to the school to decide whether recommendations will be implemented
Private Practice Context
Case Example – Private Practice
11-year-old female in Grade 6 – A & B student Ax requested by parents due to concerns
about her ability to retain info, learn math, understand maps, understand music, organize/plan her time, social skills
Attended Waldorf school initially & French schools – now in an English school for 1.5 yrs
Not identified and no IEP - receives resource room support for math skills during music class
Case Example Assessment Results
VCI: 100, PRI: 85, WMI: 86, PSI: 91 Single Word Reading: 100 Reading Comprehension: 116 Composite Math: 91 Composite Written Language: 80 Visual Memory < Verbal Memory Visuoperceptual/spatial skills < Language Difficulties with organization/planning BASC-II – Borderline/At Risk concerns re: Anxiety MASC2 Total Score: Very Elevated
Case Example Struggles
Informed that without a DSM-V diagnosis, the supports will be stopped & no further supports will be given
Provided diagnosis of mild Non-Verbal Learning Disability (NVLD) Learns best with verbal language skills Strong vocabulary and rote verbal memory Weak visuospatial/constructional abilities Difficulty discriminating & recognizing visual details & visual-spatial
relationships Difficulty with complex, non-linguistic perceptual tasks Academically, struggles with math [but not evident on testing] Trouble expressing herself in an organized manner through writing Difficulty with non-verbal communication , trouble making friends and
maintaining friendships Problems with anxiety - fears new situations and has trouble adjusting to change
This is not a DSM-V diagnosis – will the school accept it? There is not a large discrepancy between Ability and Achievement
scores – is this a problem?
Children with a host of developmental, neurological and mental health concerns
Treatment plans often require a school component – program modification, accommodation or alternative program
Students often struggling in school across domains although needs may not be clear School refusal Behavioural/safety intervention plans
Hospital Context
Diagnostic assessments completed Comprehensive psychological assessments as
a specialized (consultation) service in hospital programs – who may not be able to receive a psychological assessment through the school board due to eligibility, wait-lists and other factors
Treatment plans and specific recommendations for the emotional/behavioural problem
Hospital Context
Case Example – Hospital
7-year-old male in Grade 2 with social and behavioural concerns
Diagnosed before psychological with ADHD & Vocal Tics; query ASD, query cognitive/learning potential
Significant aggression at home and school Speech delay, family history of attention and
learning problems Weak motor skills, organization and planning skills,
and reactions to changes in plans/routines Not identified and no IEP - regular class with shared
solving, spelling Average: all other academic skills Variable memory (average and below) Average VMI and below average visuo-motor
precision Executive functioning deficits Mood/anxiety concerns Adaptive skills below average in many domains
Case Example Struggles
At risk for Learning Disability in the future Need to ensure continual monitoring and
future assessment Focus not just on behaviour – but the
cognitive/skill weaknesses Current average academic skills, but requires
support for both behaviour and academic (accommodations, not modifications)
Qualifies for Identification? EA support? Formal IEP development?
Translating information from a context primarily operating from a medical model, to an educational model
How is diagnostic and treatment planning information translated to potential identification and formal educational planning?
Who should child psychologists in the community/hospital setting communicate with at the school/Board?.... School Psychology Staff
Struggles
Understanding differences in services, models of special education support
Understanding exceptionalities – and nuances in how a particular Board has defined the exceptionality (specific criteria)
Understanding what the Board requires to address the needs of students (because identification is not the only route to getting support)
Accessing relevant school board providers Detail in reports (sensitive family/psychiatric
information)
Common Challenges for Providers Outside of DSBs
What language is most effective to use in reports?
How do we ensure the right people have access to the information?
How does the Board view Learning Disorders (DSM) diagnoses?
Concern about stigma of mental health – ensuring understanding
Specific Challenges
Sensitive to “not telling the school” what to do
Try not to put the school system behind the eight ball – balance children needs with school resources
Communicate to the parent that recommendations are not “guaranteed”
Recommending IEP and/or Identification Inviting yourself to be part of school
consultation/intervention planning
As a Provider outside the DSB…
Identification and Diagnosis
Dr. Maria Kokai
Identification
History and background Categories of Exceptionalities Placement options
1980: Bill 82 all children with disabilities have
access to publically funded education; school boards must establish special
education programs and services for exceptional pupils
5 principles: Universal access Education at public expense Appeal process Ongoing identification and continuous
assessment and review (IPRC) Appropriate program
History of Special Education
Identification in Special Education
Mechanism for identification of special education needs:
Identification, Placement and Review Committee (IPRC)
Identification, Placement, and Review Committee (IPRC)
School board committees - decide whether or not students should be identified as exceptional
Identify the student’s exceptionality Decide appropriate placement Review identification and placement at
least once each year.
Identification in Special Education
Who is identified as an exceptional pupil?
“a pupil whose behavioural, communicational, intellectual, physical or multiple exceptionalities are such that he or she is considered to need placement in a special education program....” Students are identified according to the categories and definitions of exceptionalities provided by the Ministry of Education.http://www.edu.gov.on.ca/eng/general/elemsec/speced/hilites.html
Caution: DSB may have differing interpretations and additional identification criteria!
5 PLACEMENT OPTIONS: Regular class with indirect support Regular class with resource assistance Regular class with withdrawal assistance Special education class with partial integration Full time special education class
“Communicating to the individual or his or her personal representative a diagnosis identifying a disease or disorder as the cause of symptoms of an individual in circumstances in which it is reasonably foreseeable that the individual or his or her personal representative will rely on the diagnosis.”
“In the course of engaging in the practice of psychology, a member is authorized, subject to the terms, conditions and limitations imposed on his or her certificate of registration, to communicate a diagnosis identifying, as the cause of a person’s symptoms, a neuropsychological disorder or a psychologically based psychotic, neurotic or personality disorder.”
Psychology Act, 1991
What is a diagnosis
Learning Disability (40% of all students identified with special education needs)
Autism ADHD ID ODD CD GAD Etc….
Frequently occurring diagnoses in education
Psychological Assessments in Education
Input from psychological assessment is critical:
IPRC relies on psychological assessments IEPs rely on psychological assessments
The changing role of Psychological Assessments in Education
Old “gatekeeper” model: assessment to determine identification for IPRC
Current model: assessment to help understand learning profile, assist in programming (IEP); incorporated in a multi-tiered support
Target audience for reports: regular class and SE teachers
Caution: students do not have to be identified to get special education support!
Psychological Assessments in Education
Not all identifications require a diagnosis
Not all diagnoses lead to identification
Caution: with requests to identify a specific exceptionality!
to support parents to support teachers to support students
Ontario Ministry of EducationPolicy and Programme Memorandum
8
Dr. Carolyn Lennox
... one of a number of neurodevelopmental disorders that persistently and significantly has an impact on the ability to learn and use academic and other skills and that: results in (a) academic underachievement that is inconsistent with
the intellectual abilities of the student (which are at least in the average range) and/or (b) academic achievement that can be maintained by the student only with extremely high levels of effort and/or with additional support;
affects the ability to perceive or process verbal or non-verbal information in an effective and accurate manner in students who have assessed intellectual abilities that are at least in the average range;
results in difficulties in the development and use of skills in one or more of the following areas: reading, writing, mathematics, and work habits and learning skills;
Ministry of EducationDefinition of Learning Disability
may typically be associated with difficulties in one or more cognitive processes, such as phonological processing; memory and attention; processing speed; perceptual-motor processing; visual-spatial processing; executive functions (e.g., self-regulation of behaviour and emotions, planning, organizing of thoughts and activities, prioritizing, decision making);
may be associated with difficulties in social interaction (e.g., difficulty in understanding social norms or the point of view of others); with various other conditions or disorders, diagnosed or undiagnosed; or with other exceptionalities;
is not the result of a lack of acuity in hearing and/or vision that has not been corrected; intellectual disabilities; socio-economic factors; cultural differences; lack of proficiency in the language of instruction; lack of motivation or effort; gaps in school attendance or inadequate opportunity to benefit from instruction.
Ministry of EducationDefinition of Learning Disability
Cognitive abilities
“At least in the average range”: Some issues for us as experts are:
What is salient depends on test, student, subtest scatter, entire profile – clinical judgment based on evidence-based practice
Grey and discussion! How is average determined in diagnosis of learning
disability? Not a cut-off score but common understanding of
interpretation and functional information for board
of behaviour and emotions, planning, organizing of thoughts and activities, priorizing, decision making.
Academic underachievement
Processing difficulties results in difficulties in the development and use of skills in one or more of the following areas: reading, writing, mathematics, and work habits and learning skills;
Inconsistent with intellectual abilities and/or Academic achievement that can be maintained by
the student only with extremely high levels of effort and/or with additional
Notion of disability/need?
Assessment guidelines
Measures should be based on Canadian norms; culturally sensitive; use accessible format (e.g., sign language, Braille, large print). Assessment results conveyed using standard scores instead of grade levels or age and/or grade-level equivalencies.
All psycho-educational and psychological assessments must be performed by or under the supervision of a qualified member of the College of Psychologists of Ontario, with informed consent from the parent(s).
The results of the assessments must inform the development of the student’s Individual Education Plan (IEP) (whether or not the student has been identified).
Associated and exclusionary factors
may be associated with difficulties in social interaction (e.g., difficulty in understanding social norms or the point of view of others); with various other conditions or disorders, diagnosed or undiagnosed; or with other exceptionalities;
is not the result of a lack of acuity in hearing and/or vision that has not been corrected; intellectual disabilities; socio-economic factors; cultural differences; lack of proficiency in the language of instruction; lack of motivation or effort; gaps in school attendance or inadequate opportunity to benefit from instruction.
Prior to Psychological Assessment
School boards are required to implement procedures for early and ongoing identification of the learning abilities and needs of student. See clause 8(3)(a) of the Education Act
If assessment and instruction, including early intervention strategies, have been tailored over a period of time to a student’s strengths and needs; if the student’s progress has been closely monitored and assessed; and if the student persistently demonstrates key characteristics of potential learning disabilities, the student should be considered for more in-depth assessments.
IPRC
Multisource Information presented to IPRC typically should include the following: information provided by the parent(s), the student, and the
educator(s) (e.g., the language spoken at home, developmental history, observations in the classroom)
educational history medical information (e.g., information on vision, hearing,
and physical condition) educational assessments and/or other professional
assessments (e.g., psycho-educational and/or psychological assessments, other assessments by health professionals)
Program Planning
students who have been identified as exceptional by an IPRC
AND any other students who demonstrate
difficulties in learning and who would benefit from special education programs and/or services that are appropriate for students with learning disabilities
Program Planning
The determining factor for the provision of special education programs or services is not any specific diagnosed or undiagnosed medical condition, but rather the needs of individual students based on the individual assessment of strengths and needs (professional assessment not needed, could be classroom assessment).
Assessment (my words: classroom or professional) results should inform the description of a student’s strengths and needs and be used to determine special education programs and/or services for the student. The school principal may decide to develop an IEP for a student who demonstrates difficulties in learning and who would be likely to benefit from a special education program and/or services appropriate for students with learning disabilities.
IEP
Principals should ensure that parents, students (where appropriate), and relevant school personnel are invited to participate in the development of the IEP of students with learning disabilities
Transition planning must be considered as part of the IEP development process
Transitions are entry to school; between grades; from one programme area or subject to another; moving from school to school or agency to school; elementary to secondary; secondary to post-secondary or work
IEP Strategies
The IEP of students with learning disabilities may include the following strategies,: • Instructional, environmental, and assessment accommodations so that the student is able to access grade-level curriculum expectations and to demonstrate learning. • Modification of learning expectations may include the use of expectations at a different grade level and/or an increase or decrease in the number and/or complexity of expectations • Alternative expectations and/or courses that are not derived from an Ontario curriculum policy document (e.g., expectations focused on social skills, self-advocacy, transition planning, study skills) will be developed as needed
School Board Considerations
Dr. Marie-Josee Gendron
Diagnosis vs. Identification
Diagnosis refers to the DSM V or other diagnostic criteria by a professional
Identification is a ministerial requirement that defines exceptional students “whose behavioural, communicational, intellectual, physical or multiple exceptionalities” are such that they require placement in a special education program.
Identification, Placement, and Review Committee (IPRC)
School board committees that decide whether or not students should be identified as exceptional
Identify the areas of the student’s exceptionality
Decide appropriate placement for student
Review identification and placement at least once each year
Categories of exceptionalities
Behaviour: o Behaviour
Communication: o Autismo Deaf and hard-of-hearingo Language impairmento Speech impairmento Learning disability
Categories of exceptionalities (cont’d)
Intellectual: o Giftednesso Mild Intellectual Disabilityo Developmental Disability
Physical: o Physical disabilityo Blind and Low vision
Multiple Exceptionalities
Individual Educational Plan (IEP)
IEPs are developed for students who:
are identified as exceptional by an IPRC
are receiving special education programs and services but are not identified exceptional by an IPRC
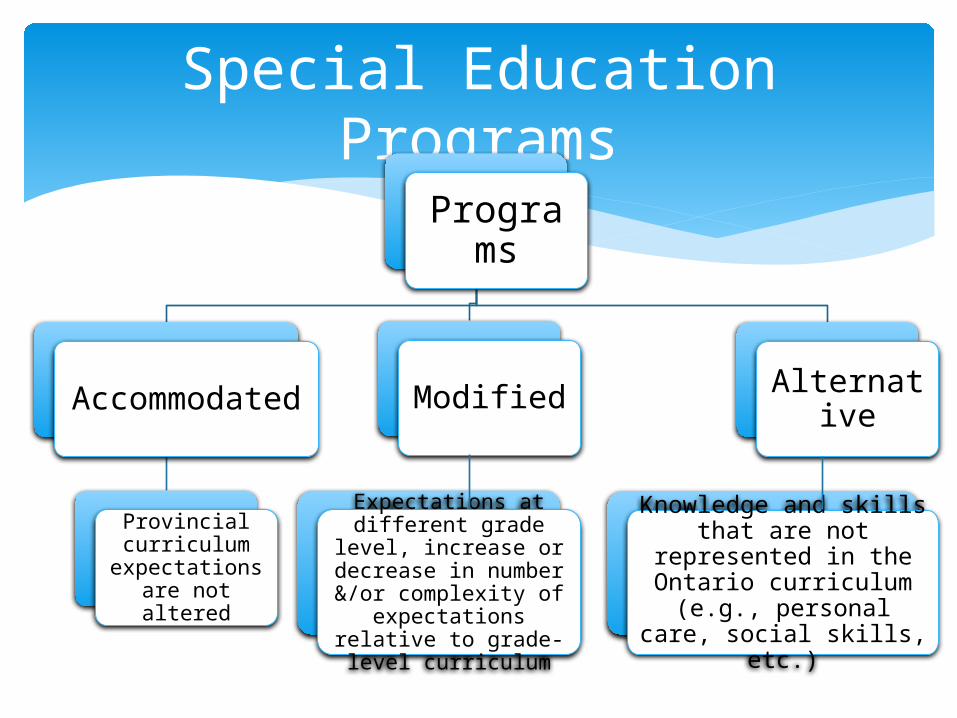
Special Education Programs
Programs
Accommodated
Provincial curriculum
expectations are not altered
Modified
Expectations at different grade level, increase or decrease
in number &/or complexity of
expectations relative to grade-level
curriculum
Knowledge and skills that are not
represented in the Ontario curriculum
(e.g., personal care, social skills, etc.)
Alternative
Placements
Options for placement:
Regular classroom with indirect support Regular classroom with resource
assistance Regular classroom with withdrawal
assistance Special education class with partial
integration Special education class full time
Types of Accommodations
Instructional: changes in teaching strategies that allow the student to access the curriculum
Environmental: changes that are required to the classroom and/or school environment
Assessment: changes in procedures that are required in order for the student to demonstrate learning
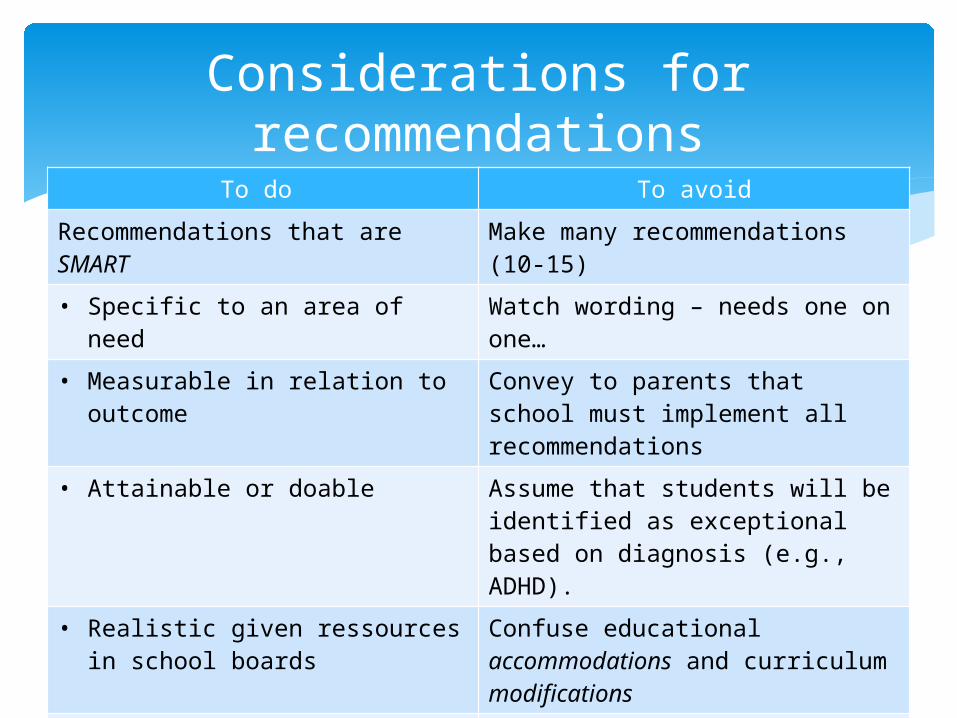
Considerations for recommendations
To do To avoid
Recommendations that are SMART
Make many recommendations (10-15)
• Specific to an area of need Watch wording – needs one on one…
• Measurable in relation to outcome
Convey to parents that school must implement all recommendations
• Attainable or doable Assume that students will be identified as exceptional based on diagnosis (e.g., ADHD).
• Realistic given ressources in school boards
Confuse educational accommodations and curriculum modifications
• Temporally-defined (elementary vs. secondary school)
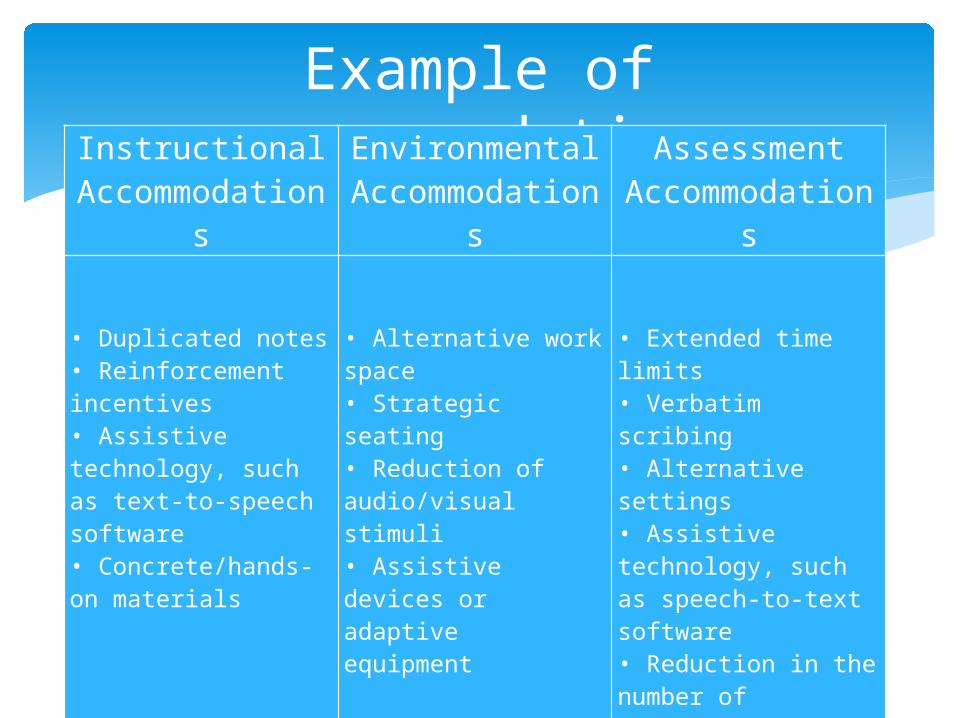
Example of recommendationsInstructional
Accommodations
Environmental Accommodation
s
Assessment Accommodation
s
• Duplicated notes• Reinforcement incentives• Assistive technology, such as text-to-speech software• Concrete/hands-on materials
• Alternative work space• Strategic seating• Reduction of audio/visual stimuli• Assistive devices or adaptiveequipment
• Extended time limits• Verbatim scribing• Alternative settings• Assistive technology, such as speech-to-text software• Reduction in the number oftasks used to assess a concept or skill
Resources
Ontario Ministry of Education: edu.gov.on.ca/eng/general/elemsec/speced/hilites.html
Ontario Ministry of Education: edu.gov.on.ca/eng/teachers/buildingfutures/teachPres/SupportingStudentsSpecialEducationNeeds.pdf