62
FRANCIS J. CURRY NATIONAL TUBERCULOSIS CENTER An Introduction to Interpretation Skills for TB Control, 2nd Edition VIEWER’S GUIDE

F RA NC I S J. C U RRY
N AT I ONA L T U B E RC U LO S I S C E NT E R
Making the Connection: An Introduction to Interpretation Skillsfor TB Control, 2nd Edition
VIEWER’S GUIDE

his project was funded through the Department of Public Health and the City and County of San Francisco with funds awarded under Cooperative Agreement U52/CCU900454, Centers
for Disease Control and Prevention. Permission is granted for non-profit educational uses and library duplication and distribution. Suggested citation:
Making the Connection: An Introduction to Interpretation Skills for TB Control was filmed on location at the Tuberculosis Clinic, Ward 94, San Francisco General Hospital, San Francisco, CA, U.S.A in July 2002.
Date of original release: July 2003
Date of second edition release: December 2008
Termination Date: December 2011
Total video running time: 29 minutes
Program Manager: Lily Lam, M.A. (original release) Jeannie Fong (second edition)
This guide and video is available on the Francis J. Curry National Tuberculosis Center website: http://www.nationaltbcenter.ucsf.edu. Feedback and comments related to this product are welcome, please email: [email protected].
The faculty for this course, Elaine Quinn, R.N., M.B.A. has indicated that she has not had any financial arrangements or affiliation with commercial sponsors that have direct interest in the subject matter.
Francis J. Curry National Tuberculosis Center. Making the Connection: An Introduction to Interpretation Skills for TB Control, Second Edition. December 2008 : [inclusive page numbers].
T

Faculty Credentials Elaine Quinn, R.N., M.B.A., designs and presents training for medical and community interpreters throughout the United States. As a Director of Cross-Cultural Programs at the Texas Department of Health, she is the project lead for a statewide interpreter pool and interpreter training in social service, medical, mental health, and legal settings. Ms. Quinn designed a medical interpreter training program for the Refugee Health Screening Clinic that she opened in Austin, Texas. She is a co-founder and developer of the Medical and Community Interpreters Special Interest Group of the Austin Area Translators and Interpreters Association. She also is on the Board of Directors of the National Council for Interpreting in Health Care.
Acknowledgements The following individuals are gratefully acknowledged for this invaluable participation and guidance in this project:
Stephanie Spencer, M.A., TB Control Branch, California Department of Public Health, Richmond, California Brenda Ashkar, R.N., M.S.N., P.H.N., Nurse Consultant, Francis J. Curry National TB Center, San Francisco, California
The following individuals and organizations were instrumental in creating the original product:
Judi A. Bulmer, New York State Department of Public Health, Albany, New York
Susan K. Choi, M.S., PALS for Health, Los Angeles, California
Department of Public Health, Broward County, Florida
Department of Public Health, Orange County, Florida
Department of Public Health, Duval County, Florida
Department of Public Health, TB Control, San Francisco, California
Department of Public Health, TOPS Clinic, San Francisco, California
Mary Esther Diaz, M.Ed., Language and Learning, Buda, Texas
Heng Lam Foong, PALS for Health, Los Angeles, California
Nobuko J. Hiramine, PALS for Health, Los Angeles, California
Andy Heetderks, M.P.H., Centers for Disease Control and Prevention, Atlanta, Georgia
Wilma Jackson, M.P.H., Florida Department of Health, TB and Refugee Health, Tallahassee, Florida
Quyen Vinh La, TB Control, Department of Public Health, San Francisco, California
Deborah Sodt, R.N., P.H.N., M.P.H., Minnesota Department of Health, Minneapolis, Minnesota
Van Ta, TB Control, Department of Public Health, San Francisco, California
Julie Wallace, B.S.N., M.N., M.P.H., Harborview Medical Center, Seattle, Washington
Elba Warner, TB Control, Department of Public Health, San Francisco, California
Zamacona Productions, San Francisco, California
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition I


Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition I I I
Table of Contents
ABOUT THIS VIDEO AND VIEWER’S GUIDE . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Learning Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
I. SKILLS FOR INTERPRETERS AND HEALTHCARE PROVIDERS . . . . . . . . . . 3
A. What You Should Know About Interpreting in Healthcare Settings . . . . . . 3
B. Code of Ethics for Healthcare Interpreters . . . . . . . . . . . . . . . . . . . . . . . 6
C. Techniques for Facilitating the Interpreted Session . . . . . . . . . . . . . . . . . 8
D. Cultural Competency Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
E. Ten Tips for Providers When Working With an Untrained Interpreter. . . . . 12
II. TOOLS FOR ASSESSING INTERPRETERS AND INTERPRETER SERVICES . . . . . . 15
A. Tools to Assess Interpreter’s Skills . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
B. Interpreter Service Models: Benefits and Drawbacks . . . . . . . . . . . . . . . 29
C. Guidelines for Selecting a Telephone Interpreting Service Provider . . . . . 31
D. Guidelines for Selecting a Language Pool . . . . . . . . . . . . . . . . . . . . . . . . . 33
III. LEGAL ISSUES RELATED TO HEALTHCARE INTERPRETING . . . . . . . . . . . . . . . . . . . . 35
A. Legal Issues Related to Healthcare Interpreting . . . . . . . . . . . . . . . . . . 35
B. Title VI of the Civil Rights Act of 1964 . . . . . . . . . . . . . . . . . . . . . . . . . 36
C. Summary of Laws & Policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
IV. RESOURCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
A. Language-Appropriate Patient Materials . . . . . . . . . . . . . . . . . . . . . . . 41
B. Medical Interpretation Providers . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
V. GLOSSARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
VI. APPENDIX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
A. Discussion Topics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
B. Slides from the Video . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
C. Cultural Competency Materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46


Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 1
About This Video and Viewer’s Guide
T he population of Tuberculosis (TB) patients in the United States has become increasingly diverse. Currently, over half of TB patients are non-U.S. born. And an increasing number
speak a language other than English which can make communication a challenge for the patient, healthcare provider, and staff.
The Francis J. Curry National Tuberculosis Center is meeting this challenge by developing these training materials to help guide TB healthcare providers in working effectively with interpreters. This video and viewer’s guide will also help equip bilingual or multilingual TB staff with fundamental interpreting skills as they may be asked to interpret when a trained interpreter is not available. This viewer’s guide expands on the content covered in the 29-minute video and serves as a reference guide by providing additional information and resources. To maximize your learning experience, it is recommended that you read the viewer’s guide after watching the video.
Materials in this guide address the following topics:
I. Skills for Interpreters and Healthcare ProvidersII. Tools for Assessing Interpreters and Interpreter ServicesIII. Legal Issues Related to Healthcare Interpreting
While cultural competency is a topic beyond the scope of this video, a brief assessment instrument is also provided to obtain a thumbnail sketch of an organization’s overall cultural competency.
Slides from the video, a sample translated form, and a list of discussion topics can be found in the Appendix. If the video is shown in a group setting, a facilitator can use the topics of discussion to encourage group dialog. Although the discussion topics are not designed to be all-inclusive or defini-tive, they serve as a learning tool to share experiences, explore ideas and solutions.
Target Audience
• Bilingual or multilingual TB staff who are asked to help interpret for patients• TB healthcare providers who work with interpreters
A Word About Guidelines
Efforts have been made to ensure that this video and viewer’s guide includes applicable recom-mendations from the Centers for Disease Control and Prevention. However, the product may not address every issue of interest to all regulatory agencies. Since regulations and guidelines may vary by county and state, facilities should review local, state, and federal guidelines when applying this information to their programs.

2
LEARNING OBJECTIVES
After viewing the video and reviewing the materials in this viewer’s guide, you will be able to:
1. describe an interpreter’s responsibilities.
2. differentiate between interpretation and translation.
3. identify the three modes of interpreting.
4. describe two types of pre-sessions.
5. list at least three techniques to ensure accuracy and completeness.
6. list at least three tools to assess an interpreter’s skills.
7. list at least three techniques to facilitate an interpreted session.
8. list at least three guidelines to use when selecting interpreter services.
9. compare the benefits and drawbacks of interpreter service models.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 3
I. Skills for Interpreters and Healthcare Providers
A. WHAT YOU SHOULD KNOW ABOUT INTERPRETING IN HEALTHCARE SETTINGS • The Roles of an Interpreter • Modes of Interpreting
B. CODE OF ETHICS FOR HEALTHCARE INTERPRETERS
C. TECHNIQUES FOR FACILITATING THE INTERPRETED SESSION
D. CULTURAL COMPETENCY SELF-ASSESSMENT
E. TEN TIPS FOR PROVIDERS WHEN WORKING WITH AN UNTRAINED INTERPRETER
A. WHAT YOU SHOULD KNOW ABOUT INTERPRETINGIN HEALTHCARE SETTINGS
What does it mean to be a “healthcare interpreter?” An interpreter’s primary responsibilities include the following:
1. Facilitates the interpreted session to ensure the same quality and understanding as that of an English-speaking patient encounter.
2. Helps people communicate effectively when there are language and cutural barriers.
3. Accurately and completely interprets everything that is heard without changing the intended meaning of the message in any way.
4. Interprets with the highest standard of ethics and confidentiality.
An interpreter may be a bilingual employee, where interpretation is only one part of a larger role – including advocacy or cultural mediation. On the other hand, some view health interpreters in the same category as court or conference interpreters – where interpreters are expected to limit their role to the accurate and complete transmission of messages. These
differing views highlight the complexity of the interpreter's role. The interpreter's primary role is to facilitate clear communication.
The Roles of An InterpreterTo effectively interpret and facilitate a healthcare-related encounter, a healthcare interpreter needs to be able to function in a variety of roles that support the communications between the patient and healthcare provider.
4
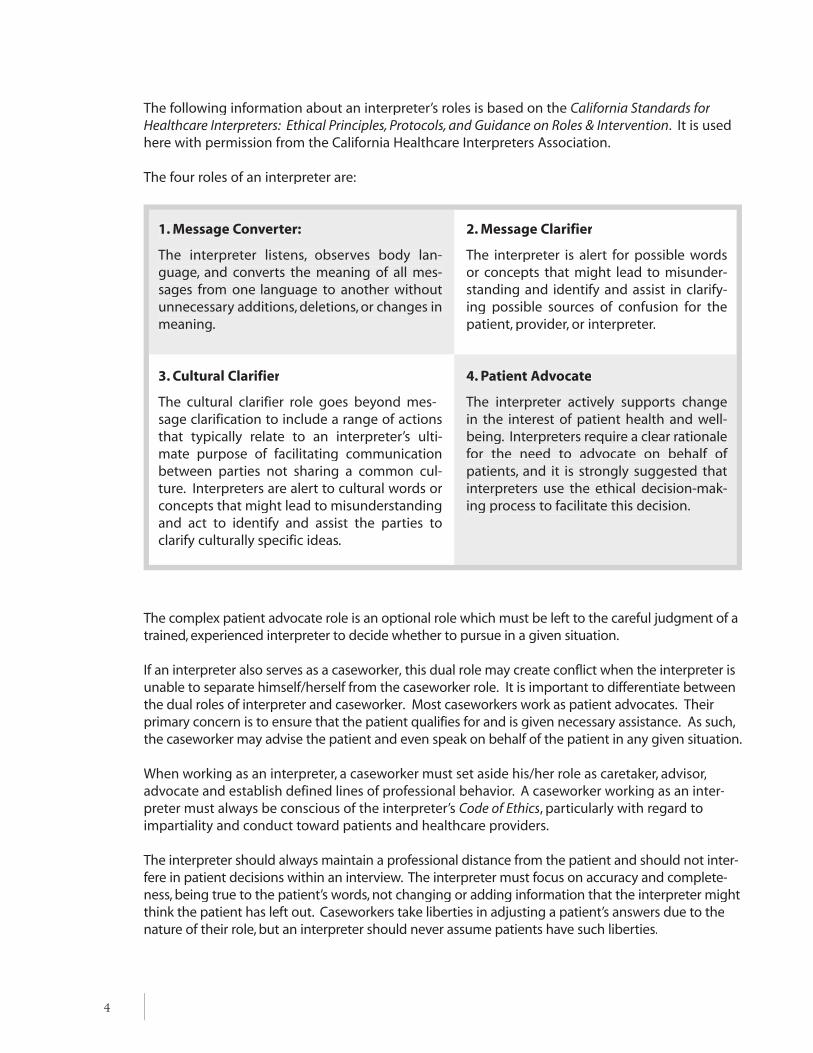
The following information about an interpreter’s roles is based on the California Standards for Healthcare Interpreters: Ethical Principles, Protocols, and Guidance on Roles & Intervention. It is used here with permission from the California Healthcare Interpreters Association.
The four roles of an interpreter are:
1. Message Converter:
The interpreter listens, observes body lan-guage, and converts the meaning of all mes-sages from one language to another without unnecessary additions, deletions, or changes in meaning.
2. Message Clarifier
The interpreter is alert for possible words or concepts that might lead to misunder-standing and identify and assist in clarify-ing possible sources of confusion for the patient, provider, or interpreter.
3. Cultural Clarifier
The cultural clarifier role goes beyond mes-sage clarification to include a range of actions that typically relate to an interpreter’s ulti-mate purpose of facilitating communication between parties not sharing a common cul-ture. Interpreters are alert to cultural words or concepts that might lead to misunderstanding and act to identify and assist the parties to clarify culturally specific ideas.
4. Patient Advocate
The interpreter actively supports change in the interest of patient health and well-being. Interpreters require a clear rationale for the need to advocate on behalf of patients, and it is strongly suggested that interpreters use the ethical decision-mak-ing process to facilitate this decision.
The complex patient advocate role is an optional role which must be left to the careful judgment of a trained, experienced interpreter to decide whether to pursue in a given situation.
If an interpreter also serves as a caseworker, this dual role may create conflict when the interpreter is unable to separate himself/herself from the caseworker role. It is important to differentiate between the dual roles of interpreter and caseworker. Most caseworkers work as patient advocates. Their primary concern is to ensure that the patient qualifies for and is given necessary assistance. As such, the caseworker may advise the patient and even speak on behalf of the patient in any given situation.
When working as an interpreter, a caseworker must set aside his/her role as caretaker, advisor, advocate and establish defined lines of professional behavior. A caseworker working as an inter-preter must always be conscious of the interpreter’s Code of Ethics, particularly with regard to impartiality and conduct toward patients and healthcare providers.
The interpreter should always maintain a professional distance from the patient and should not inter-fere in patient decisions within an interview. The interpreter must focus on accuracy and complete-ness, being true to the patient’s words, not changing or adding information that the interpreter might think the patient has left out. Caseworkers take liberties in adjusting a patient’s answers due to the nature of their role, but an interpreter should never assume patients have such liberties.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 5
An interpreter who belongs to a smaller ethnic community may experience particular strug-gles if asked to work more as a caseworker for his/her community members than as an inter-preter. In these situations, the interpreter must find a tactful and professional way to explain the interpreter role to patients. The interpreter may want to stress the importance of the patient’s exact words to the healthcare provider.
Expressing the interpreter’s role as a “transmitter of information between the patient and healthcare provider” also may ease the dilemma. The interpreter should think through how to handle such situations before taking an assignment.
Modes of Interpreting
Just as a professional interpreter uses different roles in interpreting, he/she also uses three different modes of interpreting. In each of these modes, it is important that he/she interprets accurately and completely. This means saying exactly what is said and matching the tone, vol-ume, gestures, and pauses used by the speaker.
As the interpreter listens to the message, he/she must work toward formulating the meaning of the words in the first language into a meaningful pattern into the target language. This requires the interpreter to be focused, giving full attention to all aspects of communication occurring during the interaction.
The interpreter must listen carefully in order to understand the full idea of the message. He/She must not become caught up with deciphering a single term or wrestling with per-sonal emotion or opinion over a subject. The interpreter must be cautious not to portray any of his/her own emotion in an interpretation.
The skills described above are used in the three modes of interpreting:
A. Consecutive interpretation occurs when one speaker starts to say a few sentences, then pauses for the interpreter to interpret. This process is repeated with the next speaker, pro-viding continuous interpretation until the dialogue is complete. This follows the pattern of natural speech in which only one person speaks at a time. And this is the most com-mon mode used in the healthcare setting.
B. Simultaneous interpretation occurs when the interpreter interprets at the same time as the speaker is speaking. Simultaneous interpreting is most often used when the speaker is unable to pause for the interpreter to work in consecutive mode. Other situations in which simultaneous interpreting is appropriate are when there is an emergency or in a classroom or forum setting where a person is presenting to a group of people.
Simultaneous interpreting is a skill that must be practiced and refined since it is often used with a rapid pace of speech. Unlike consecutive interpreting, there is no lag time in simultaneous interpreting. The interpreter is required to follow a dialogue at a normal rate of conversation.

6
C. Sight Translation is the oral translation of a written document into the target language. The interpreter must be proficient in reading and understanding text written in both original and target languages. The procedure for translating a document is to first read through the entire document silently to himself/herself. Since many documents are filled with technical jargon and acronyms, the interpreter needs to take the time to clarify anything that is not understood with the patient or healthcare provider before beginning the translation. Once begun, the interpreter reads the document clearly, smoothly, and at a moderate pace.
D. Telephone Interpreting is an additional mode that can be used when face-to-face interpreting is not possible and this service can be provided by a telephone interpreting company.
In this mode, the interpreter does not have the benefit of observing the body language and facial expressions of the patient and the healthcare provider. Their voices are the only means of assessing the understanding between them. Therefore, the interpreter must practice active listening and assertiveness to ensure that the interpreted session is productive.
Telephone interpretation requires total concentration to compensate for not being physically present during the interpreted session. It may actually require more energy from the inter-preter than a face-to-face interpretation.
B. CODE OF ETHICS FOR HEALTHCARE INTERPRETERS
For an interpreter to function professionally, he/she must follow a code of ethics similar to those followed by nurses and social workers. Patients must be able to have trust and confidence in
the person who communicates their personal information for them. A code of ethics protects the patient and delineates professional behavior for the interpreter.
The National Council on Interpreting Healthcare (NCIHC) has drafted a working paper entitled, “A National Code of Ethics for Interpreters in Healthcare: A Working Paper for Discussion, July 2004." It offers a set of principles generally accepted by a number of healthcare interpreting organizations in the United States.
The following information is excerpted from the above paper and is used with permission from the NCIHC. The complete text of the paper can be found at http://www.ncihc.org/http://www.ncihc.org/(click on Resouce tab and "Ethics and Standards").
The elements of an interpreters’ code of ethics include:
1. Confidentiality – All information learned in the performance of professional duties shall be held confidential. This means that interpreters will not disclose any information learned during the performance of their duties to anyone. Confidentiality is to be maintained in all situations except when states mandate a disclosure of information in specific situations such as child abuse, elder abuse, or a person threatening harm to himself/herself or others. Currently, there are no specific legal determinations on interpreter responsibilities regarding disclosure of abuse.
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 7
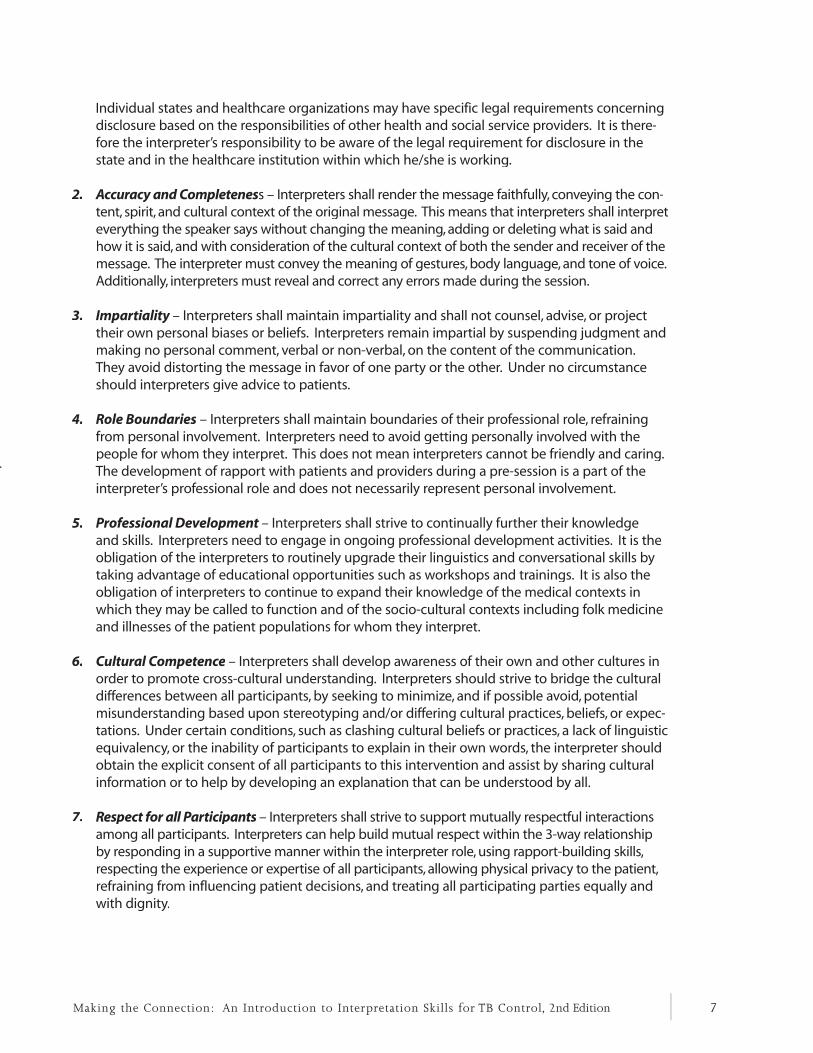
Individual states and healthcare organizations may have specific legal requirements concerning disclosure based on the responsibilities of other health and social service providers. It is there-fore the interpreter’s responsibility to be aware of the legal requirement for disclosure in the state and in the healthcare institution within which he/she is working.
2. Accuracy and Completeness – Interpreters shall render the message faithfully, conveying the con-tent, spirit, and cultural context of the original message. This means that interpreters shall interpret everything the speaker says without changing the meaning, adding or deleting what is said and how it is said, and with consideration of the cultural context of both the sender and receiver of the message. The interpreter must convey the meaning of gestures, body language, and tone of voice. Additionally, interpreters must reveal and correct any errors made during the session.
3. Impartiality – Interpreters shall maintain impartiality and shall not counsel, advise, or project their own personal biases or beliefs. Interpreters remain impartial by suspending judgment and making no personal comment, verbal or non-verbal, on the content of the communication. They avoid distorting the message in favor of one party or the other. Under no circumstance should interpreters give advice to patients.
4. Role Boundaries – Interpreters shall maintain boundaries of their professional role, refraining from personal involvement. Interpreters need to avoid getting personally involved with the people for whom they interpret. This does not mean interpreters cannot be friendly and caring. The development of rapport with patients and providers during a pre-session is a part of the interpreter’s professional role and does not necessarily represent personal involvement.
5. Professional Development – Interpreters shall strive to continually further their knowledge and skills. Interpreters need to engage in ongoing professional development activities. It is the obligation of the interpreters to routinely upgrade their linguistics and conversational skills by taking advantage of educational opportunities such as workshops and trainings. It is also the obligation of interpreters to continue to expand their knowledge of the medical contexts in which they may be called to function and of the socio-cultural contexts including folk medicine and illnesses of the patient populations for whom they interpret.
6. Cultural Competence – Interpreters shall develop awareness of their own and other cultures in order to promote cross-cultural understanding. Interpreters should strive to bridge the cultural differences between all participants, by seeking to minimize, and if possible avoid, potential misunderstanding based upon stereotyping and/or differing cultural practices, beliefs, or expec-tations. Under certain conditions, such as clashing cultural beliefs or practices, a lack of linguistic equivalency, or the inability of participants to explain in their own words, the interpreter should obtain the explicit consent of all participants to this intervention and assist by sharing cultural information or to help by developing an explanation that can be understood by all.
7. Respect for all Participants – Interpreters shall strive to support mutually respectful interactions among all participants. Interpreters can help build mutual respect within the 3-way relationship by responding in a supportive manner within the interpreter role, using rapport-building skills, respecting the experience or expertise of all participants, allowing physical privacy to the patient, refraining from influencing patient decisions, and treating all participating parties equally and with dignity.

8
8. Professional Integrity – Interpreters shall demonstrate professionalism and personal integrity. Aspects of professionalism include the following:
a. If the interpreter believes at any time that he/she may have interpreted inaccurately or incom-pletely, he/she will make this known and, if possible, provide a corrected interpretation
b. An interpreter shall not accept an assignment, or shall withdraw from an assignment, in which he/she:
• Is not competent to interpret accurately and completely
• Perceives a conflict of interest between his/her role as an interpreter and his/her personal involvement with one of the parties in the interpretation
• Is impacted by the content to be interpreted that he/she becomes unable to interpret accurately and completely
c. The interpreter will not accept additional compensation or considerations from any participants in the interpreted sessions. The interpreter and the contracting or employing agency will agree to a fee which shall be the only remuneration that the inter-preter will accept.
C. TECHNIQUES FOR FACILITATING THE INTERPRETED SESSION
Why is facilitating the interpreted session important?
T he interpreter is responsible for facilitating the best possible communication between thepatient and the healthcare provider. The content of this section focuses on various methods
that an interpreter may use to facilitate an interpreted session. The use of appropriate facilitation skills by the interpreter can: • save time during the interpreted session • reduce confusion between patient and healthcare provider • support the primary relationship between the provider and the patient
A trained interpreter will use the following facilitation techniques without prompting by the healthcare provider.
The following information is based on an interpreter training manual entitled An Introduction to An Introduction to Community InterpretingCommunity Interpreting*. It is used here with permission by the contributing authors.
From Elaine Quinn, “Five Hats of Interpreting,” in Sharon Bush (ed.), An Introduction to Community InterpretingAn Introduction to Community InterpretingAn Introduction to Community InterpretingAn Introduction to Community InterpretingAn Introduction to Community Interpreting, unpublished training manual, Austin, Texas, 2001.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 9
1. Conducting a Pre-session – A pre-session is the interpreter’s introduction to both the provider and the patient. The pre-session is a 30 to 40 second introduction made for both the provider and the patient before the interview begins. The purpose of the pre-session is to set the parameters for how the interpreter will operate and to specify the ways that the provider and patient can help the interpreter to be effective. This helps to deal with any problems that may arise in the communication. The following are sample pre-session scripts:
The interpreter tells the patient: The interpreter tells the provider:
His/her name His/her name
His/her employer His/her employer
That he/she is a professional To speak directly to the patient
Everything said in the session will be confidential
That he/she will interpret
To speak directly to the provider To pause often
That he/she will interpret everything
“Do you have any special information that you wish for me to interpret to the patient? Please provide it to me exactly as you wish it to be said.”
To pause often Hand signal will be used if clarification is needed
2. Positioning – Positioning refers to where the interpreter sits or stands during an interpreted session.
Positioning of the patient, healthcare provider, and interpreter is important because commu-nication is affected by visual stimulus. To facilitate as much direct communication as possible between the patient and provider, the best position for the interpreter is beside and slightly behind the client. This helps the patient feel supported, yet the interpreter is not placed in the middle of the conversation. With the interpreter seated slightly behind the client, it also makes it a bit more difficult for the patient to speak directly to the interpreter.
patientpatient provider
interpreter
10
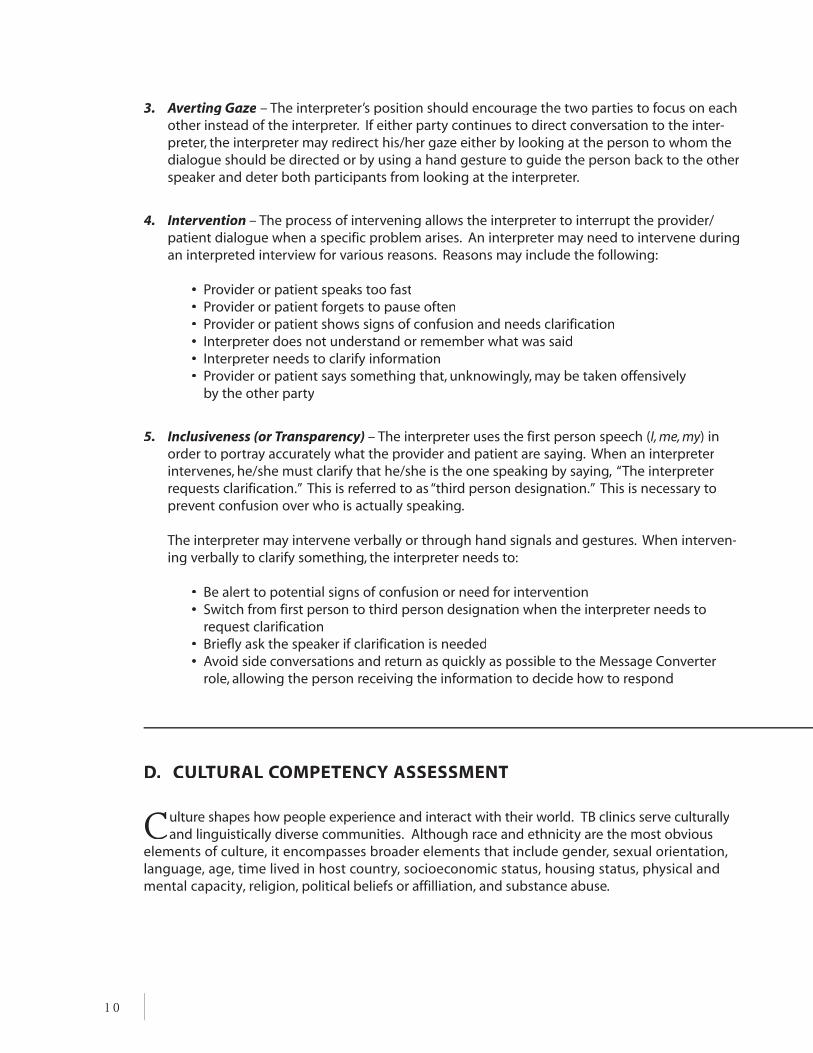
3. Averting Gaze – The interpreter’s position should encourage the two parties to focus on each other instead of the interpreter. If either party continues to direct conversation to the inter-preter, the interpreter may redirect his/her gaze either by looking at the person to whom the dialogue should be directed or by using a hand gesture to guide the person back to the other speaker and deter both participants from looking at the interpreter.
4. Intervention – The process of intervening allows the interpreter to interrupt the provider/patient dialogue when a specific problem arises. An interpreter may need to intervene during an interpreted interview for various reasons. Reasons may include the following:
• Provider or patient speaks too fast• Provider or patient forgets to pause often• Provider or patient shows signs of confusion and needs clarification• Interpreter does not understand or remember what was said• Interpreter needs to clarify information• Provider or patient says something that, unknowingly, may be taken offensively
by the other party
5. Inclusiveness (or Transparency) – The interpreter uses the first person speech (I, me, my) in order to portray accurately what the provider and patient are saying. When an interpreter intervenes, he/she must clarify that he/she is the one speaking by saying, “The interpreter requests clarification.” This is referred to as “third person designation.” This is necessary to prevent confusion over who is actually speaking.
The interpreter may intervene verbally or through hand signals and gestures. When interven-ing verbally to clarify something, the interpreter needs to:
• Be alert to potential signs of confusion or need for intervention• Switch from first person to third person designation when the interpreter needs to
request clarification• Briefly ask the speaker if clarification is needed• Avoid side conversations and return as quickly as possible to the Message Converter
role, allowing the person receiving the information to decide how to respond
D. CULTURAL COMPETENCY ASSESSMENT
Culture shapes how people experience and interact with their world. TB clinics serve culturally and linguistically diverse communities. Although race and ethnicity are the most obvious
elements of culture, it encompasses broader elements that include gender, sexual orientation, language, age, time lived in host country, socioeconomic status, housing status, physical and mental capacity, religion, political beliefs or affilliation, and substance abuse.

Organizational behaviors, policies, and attitudes throughout your agency should respect and respond to the communities served. The organization should develop systems that ensure full participation of patients with limited English proficiency and those coming from different cultures. The organization should understand that cultural competency is a journey that starts with an understanding of one’s own culture. The questions below can help to better understand and strengthen an organization’s cultural competency. Think about these seven areas within the organization. 1. Values and Attitudes
Are services delivered in a patient-centered model? Are activities regularly scheduled to promote mutual respect for differences in
the clinic population? Does the organization consider varying degrees of acculturation experienced by patients
and the effect that may have on their access and use of services? Does staff understand and accept that beliefs may influence a patient’s response to health,
illness, disease, and death?
2. Community and Consumer Participation Is active involvement of community leaders and community members in the planning for
delivery of service continuously sought after and encouraged? Are community leaders invited to speak with staff about their communities?
3. Communication Styles
Have written materials been evaluated by the community for appropriateness? Are alternatives to written communication being used in addition to documents being
written in English or the non-English language of the patient? Is language preference routinely asked of the patient? Are skilled professional interpreters ensured to be available to interpret for that
patient's appointment? Are documents that patients must read and sign routinely translated into the top five or
ten languages used in the community?
4. Policies and Procedures Does the organization’s mission statement, goals, policies, and procedures incorporate
cultural and linguistic concepts for appropriate care? Are clinical protocols incorporating cultural and linguistic concepts for appropriate care
such as the issue of self-determination and care? Does staff reflect the communities that are served? Are the hiring practices allowing equal
access for bilingual, bicultural persons? Does the organization have a quality improvement policy that has a component to assess
the communities’ satisfaction and participation? Can a patient make a “complaint” to a patient advocate and feel safe in the knowledge that
this is the expectation and that there will be no reprisals for doing so?
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 11

5. Population-based Clinical Practice Are clinicians culturally skilled enough to avoid misunderstandings due to cultural
differences and misapplication of the science of medicine? Do clinicians treat all patients as individuals and avoid stereotyping members of
cultural groups? Do clinicians understand how to initiate and practice culturally appropriate
interventions and treatments? Does the organization allow providers enough time to see patients with limited
English proficiency?
6. Physical Environment, Materials, Resources
Is the interior of the building culturally and linguistically sensitive and pleasing by design? Does the clinic have pictures, posters, artwork, magazines, brochures, audio and video, and
films that are representative of the communities that the organization serves?
7. Training and Professional Development Does the organization provide and expect participation on a regular basis in training to
understand the cultural norms for the communities that you serve? Does the organization provide and expect participation on a regular basis in training to
understand the cultural norms for the host culture? Does the organization encourage personal contact with communities from which your
patients come?
E. TEN TIPS FOR PROVIDERS WHEN WORKING WITH
AN UNTRAINED INTERPRETER
lthough a trained interpreter is always preferred, there are times when a trained interpreter may not be available. Planning is required when asking an untrained bilingual staff member or
community member to interpret. It is the provider’s responsibility to conduct a pre-session with the untrained bilingual staff member or community volunteer who is asked to interpret. It is also helpful to provide the staff member with disease specific education materials and any questions that will be asked of the patient. Request that the staff member review the materials and questions before meeting with the patient and provider. Using untrained family members as medical interpreters is strongly discouraged but don't excludethem if patient wants them to be part of the clinic visit. For more on why see "5. Ad hoc (untrained)
A
12
interpreters" on page 31.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 13
Listed below are ten tips for providers when working with an untrained interpreter, although a trained interpreter will usually follow these guidelines without prompting by the provider.
1. Make introductions among all participants and establish the grounds for confidentiality.
2. Illustrate the positioning for the interpreter by placing a chair or asking the interpreter to stand/sit in the appropriate place (page 9).
3. Establish and describe that interpreting is performed in the first person voice (e.g., I, me) when speaking for the patient or the provider. This promotes the appropriate relationship between you and your patient.
4. Explain that when the interpreter needs to speak for himself/herself, the interpreter must identify himself/herself as the person speaking and asking the question. For example, if the interpreter needs to ask a question regarding a word that is confusing, the interpreter uses the third person, “The interpreter needs clarification about…”
5. Describe and request that the interpreter use the consecutive mode of interpretation (page 5).
6. Ask the interpreter to say exactly what you and the patient say – without adding, changing, or omitting anything – even if what the patient says does not make sense.
7. Explain that the provider will speak slowly and will pause often so the interpreter can inter-pret accurately. Ask the interpreter to ask the patient to speak slowly and pause often so that he/she can interpret accurately for them. Explain that the interpreter may use a raised hand to signal for either the patient or you to stop speaking so that he/she may interpret.
8. If either the provider or patient uses a term or phrase unfamiliar to the interpreter, request that the interpreter seek clarification by using third person voice.
9. Instruct the interpreter to use a pen and paper to take notes about prescriptions, dosages, and other lists or numbers that could be confusing when repeated in the appropriate lan-guage. Also instruct the interpreter to inform the patient that any notes taken during the interpreting session will be destroyed at the end of the session and before leaving the room.
10. Ask the interpreter not to have side conversations with the patient or with the provider. The interpreter only interprets what he/she hears or asks for clarification when he/she is con-fused about a term or meaning. He/she never initiates and carries on a conversation in which one party is excluded from the conversation.

14

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 15
II. Tools for Assessing Interpreters and Interpreter Services
A. TOOLS TO ASSESS INTERPRETER’S SKILLS
B. INTERPRETER SERVICE MODELS: BENEFITS AND DRAWBACKS
C. GUIDELINES FOR SELECTING A TELEPHONE INTERPRETING SERVICE PROVIDER
D. GUIDELINES FOR SELECTING A LANGUAGE POOL
A. TOOLS TO ASSESS INTERPRETER’S SKILLS
The qualifications of the competent healthcare interpreter include a wide range of knowledge and skills. While it is essential that the interpreter be able to integrate his/her knowledge and
skills in the process of interpreting, it is desirable in an initial assessment to isolate specific compe-tencies using a multi-part assessment process for new hospital- and clinic-based interpreters .
The National Council for Interpreting in Healthcare (NCIHC) prepared a “Guide to Initial Assessment of Interpreter Qualifications” (2001), which is used in this document with permission. (For complete text, visit www.ncihc.orgwww.ncihc.org, Working Papers Series). This paper describes a multi-part assessment process that includes the following:
1. Credentials
2. References
3. Basic Oral Language Skills
4. Testing Resources
5. Ethics Exercise
6. Cultural Understanding Exercise
7. Interpretation Skills Role Plays (2)
8. Sight Translation Exercise
9. Oral Exam on Healthcare Terms – Parts I and II

16
The following sample assessment is based on the NCIHC paper. Each topic describes how to obtain information on a particular item and how to score or rate the findings.
1. Credentials
• Interpreter Certification from any state• Federal or State Court Interpreter Certification
• Evidence of prior education and training in interpreting
2. References – Background documentation might include:
• A letter of application• A resume• Letters of recommendation (from employers and, where appropriate, from members
of the community for whom the interpreting will be provided)
3. Basic Oral Language Skills – Any one of the following methods can be used to assess oral language skills:
a. Unstructured, oral interview between candidate and a rater who speaks both of the candidate’s working languages. Rater then describes candidate’s language skills as native, excellent, good, adequate, or poor.
b. Semi-structured interview between candidate and a rater who speaks both of thecandidate’s working languages. Rater then uses pre-established, clear criteria for scoring, such as: grammatical errors, use of false cognates, or attempts to paraphrase when the exact term is unknown.
c. Oral Proficiency Interview (OPI) or Simulated Oral Proficiency Interview (SOPI) from the American Council on the Teaching of Foreign Languages (ACTFL) [www.actfl.org]. Requires trained/certified raters. Tests available in limited number of languages. Identifies Novice, Intermediate, Advanced, Superior levels, with low, mid, and high subdivisions in each level except Superior.
4. Testing Resources – The following organizations can conduct testing.
Language Testing InternationalLanguage Testing InternationalLanguage Testing International in White Plains, NY in White Plains, NY Language Testing International in White Plains, NY Language Testing InternationalLanguage Testing International in White Plains, NY Language Testing International48 languages tested by telephone(914) 963-7110 or (800) 486-8444 http://actfltesting.org/home.cfm
Center for Applied Linguistics (CAL) in Washington, DCDirect assessment: tested by telephone or face-to-faceSemi-direct assessment: tape recorder, computer program, test booklet or some combinationof these to elicit language from test taker (202) 362-0700http://www.cal.org/topics/ta/

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 17
Educational Testing Service in Princeton, NJOnly certain locations, fixed dates(609) 771-7550http://www.ets.org/portal/site/ets/menuitem.fab2360b1645a1de9b3a0779f1751509/?vgnextoid= b5d7d898c84f4010VgnVCM10000022f95190RCRD
in Monterey, CA160 languages tested by telephone(877) 351-6636http://languageline.com/page/llu Pacific Interpreters in Portland, OR40 languages tested by telephone For more information call: (800) 626-8697http://www.pacificinterpreters.com/services/language-assessment.aspx Cyracom in Tucson, AZ20 languages tested by telephone (800) 713-4950http://cyracom.com/Default.aspx?PageId=732
5. Ethics Exercise – After sharing your institution’s adopted code of ethics with the candidate, present the following ethical scenarios to assess the interpreter’s ethical decision-making skills.
SCENARIO #1 A grateful patient brings you homemade food as a token of her appreciation and requests that you always be available to interpret for her. You accept it and agree to her request.
Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?
SCENARIO #2 Arriving home after a particularly difficult interpreted session, you are distressed about a patient’s personal situation and need to talk about it to someone. You tell your spouse about the patient and what you heard in the session.
Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?
SCENARIO #3 A young man is being treated with INH for LTBI. At his medical check-up, he says his urine is orange, and it burns his penis. The female interpreter, embarrassed to say the
Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?Is this professional behavior according to the code of ethics? Why?
SCORING SCENARIOS #1-3:
• Was the candidate able to persuasively justify his/her answer?• Was the candidate able to relate his/her answer to the code of ethics?
Test of Spoken English (TSE) from
18
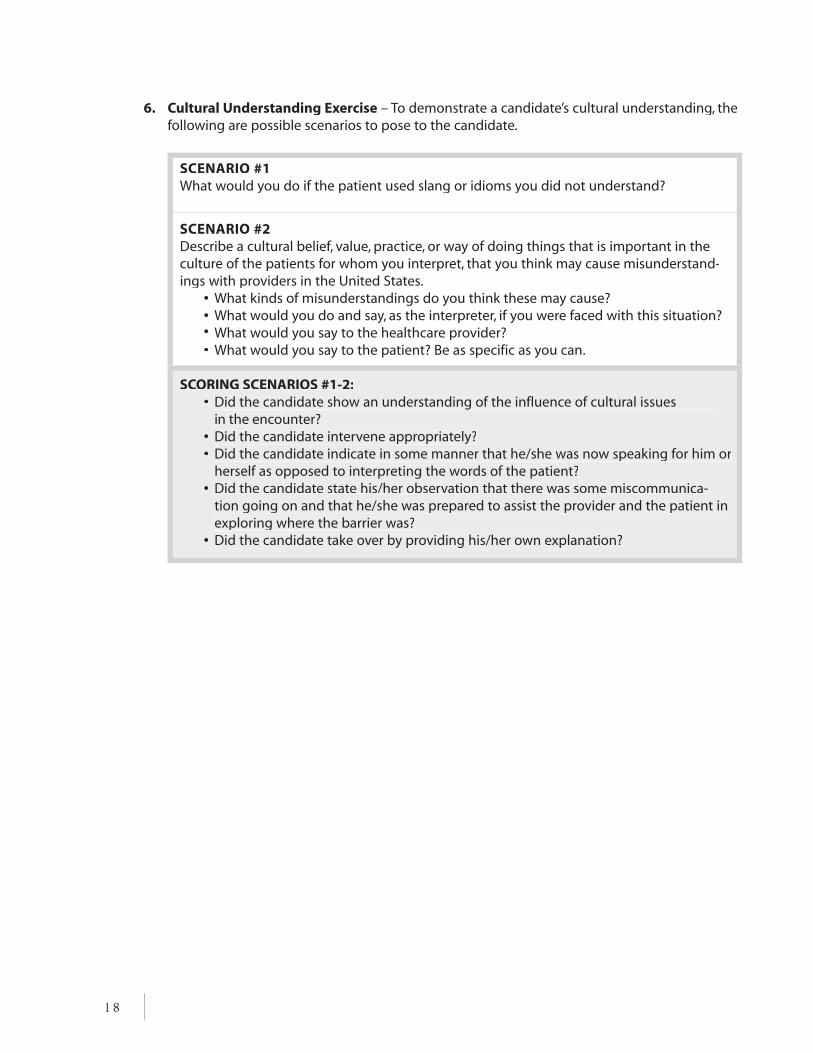
6. Cultural Understanding Exercise – To demonstrate a candidate’s cultural understanding, the following are possible scenarios to pose to the candidate.
SCENARIO #1 What would you do if the patient used slang or idioms you did not understand?
SCENARIO #2 Describe a cultural belief, value, practice, or way of doing things that is important in the culture of the patients for whom you interpret, that you think may cause misunderstand-ings with providers in the United States.
• What kinds of misunderstandings do you think these may cause? ••
What would you do and say, as the interpreter, if you were faced with this situation? What would you say to the healthcare provider?
• What would you say to the patient? Be as specific as you can.
SCORING SCENARIOS #1-2:• Did the candidate show an understanding of the influence of cultural issues
in the encounter?• Did the candidate intervene appropriately?• Did the candidate indicate in some manner that he/she was now speaking for him or
herself as opposed to interpreting the words of the patient?• Did the candidate state his/her observation that there was some miscommunica-
tion going on and that he/she was prepared to assist the provider and the patient in exploring where the barrier was?
• Did the candidate take over by providing his/her own explanation?

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 19
7. Interpretation Skills Role Playing (2) 20-minute role-play – audiotaped
The best way to evaluate an interpreter’s skills is to observe him/her interpreting in a scenario that reflects the “real world” interpreting situations found in TB clinics. Recording the role plays on audiotape can accomplish this part of the assessment and can be evaluated later.
The candidate will interpret the questions and answers posed in the scenario. In addition to the participation of the candidate, three additional roles are required for the role plays:
1. A person to read the questions (Q).2. A person who speaks the candidate’s foreign language and can sight translate the
answers (A) and read them into the different language.3. A person to listen and rate the audiotape to evaluate the accuracy and completeness of
the candidate’s interpretation.
SCORINGThe role-play should be designed to include key points to assess the interpretation. In the written copy of the script to be used for scoring, these key points should be clearly marked and numbered to match the order of those on the score sheet:
• Did the candidate interpret accurately and completely? Based on the key points in each message, the interpretation should be scored for accuracy, including mistakes, omissions, and additions.
• Accuracy refers to message conversions that are equivalent in both languages. • Mistakes are message conversions that are different in meaning from
the original. • Omissions are key points that are not interpreted. • Additions are any ideas expressed by the interpreter that were not in the
original message.
• How well did the candidate explain the role of interpreter and maintain this role throughout the role-play?
• Did the candidate use the consecutive mode of interpreting?• Did the candidate position him/herself properly?• How well did the candidate manage the flow of communication, appropriately ask
for pauses or clarifications when necessary, and use mnemonic devices (tricks to helpyou remember details)? In using these skills, did the candidate’s behavior support the patient-provider interaction or did it detract or obstruct it?
• Did the candidate handle cultural references appropriately?• When the candidate intervened, did he/she do so in such a way that it was clear
he/she was now speaking for himself/herself?

20
SCENARIO #1: MEDICAL HISTORYStart with Pre-Session (introductions and instructions)
Q. Good afternoon, Ms. Romo. I’m going to ask you a few questions about your medi-cal history before the doctor examines you, all right?
A. Yes, ma’am. That’s fine.
Q. First of all, what is the reason for your visit today?A. Well, I have been coughing a lot, and I feel very tired. My family suggested that I see a
doctor to be examined.
Q. When did these symptoms start?A. About 3 weeks ago.
Q. Had you ever had this problem before?A. Yes. I had this about 4 years ago and the doctor said I had TB. I’m afraid I might
have it again.
Q. Were you treated at that time?A. Yes, I was treated for about 6 months, and then I just took some teas and herbs that my
sister-in-law’s grandmother gave me.
Q. Did you complete the treatment?A. Yes.
Q. When was the last time you had a chest x-ray?A. Right after I finished my treatment. The clinic should have that information.
Q. Have you lost any weight recently?A. Yes, about 15 pounds in the past 3 months. At first I was glad, but then I started to worry.
Q. Have you traveled outside the country recently or have you had any contact with people from across the border?
A. Yes. My family visits me or I visit them in Monterey about once a month.
Q. Has anyone else in your family had TB?A. No. Not that I know of.
Q. Have you or your family had any medical problems?A. No, except for my grandmother; she had heart trouble.
Q. Have you ever had any other infectious disease such as typhoid, cholera, or diphtheria?A. No, not that I know of.
Q. Have you ever had any operations?A. Yes. In ’85 I had my tonsils removed.
Q. I take it you were hospitalized for this operation?A. Yes. I was hospitalized a couple of days for my tonsils.
Q. Okay, that’s all the questions I have. Just slip on a gown and get up on the examining table. The doctor will be right with you.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 21
SCENARIO #2: MONITORING
Q. Good morning Ms. Romo. I’m glad to see you today. It looks like you missed yourlast two appointments.
A. Yes. I’ve been feeling better, so I didn’t see any point in coming in.
Q. Have you been taking your medicine?A. Yes. I’m just about finished with it.
Q. Have you had any trouble with it?A. No. I just want to finish it before my cousin’s wedding that’s coming up in a couple
of weeks. She’s going to have a big wedding with lots of dancing and drinking, and my boyfriend and I want to go and have a good time.
Q. You understand how important it is to finish your treatment, right?A. Yes. The first time I had this, I only took some of the pills and then I got sick again.
Q. TB is a very serious illness. If you don’t take your medication, you could end up in the hospital or even quarantined.
A. What do you mean by "quarantined"?
Q. It means that you would have to be kept away from other people to avoid infect-ing them – including your boyfriend.
A. Well, I certainly don’t want that!
Q. Then just be sure to finish all of your medication and not to mix it with alcohol.A. Okay. I’ll try.

22
8. Sight Translation Exercise
In clinic and hospital settings, interpreters are frequently given forms in English to read to patients in their language. This is called sight translation. A good interpreter will be able to do this as smoothly as if he/she were reading in the patient’s language.
The following text can be used to test this skill. The candidate may be asked to sight translate a portion of this fact sheet from the American Lung Association of Texas (reprinted here with permission). The sight translation will need to be recorded on audiotape for evaluation.
The candidate will demonstrate sight translation of a designated portion of the following text.
TUBERCULOSIS FACT SHEET*
Tuberculosis (TB) is an airborne infection caused by the bacterium Mycobacterium tuberculosis. Although TB primarily affects the lungs, other organs and tissues may be affected as well.
TB is spread by an airborne germ. Therefore, someone with TB can spread the germs by cough-ing, sneezing, laughing, or even singing. However, repeated exposure to someone with the TB disease is generally necessary for a person to become infected. TB germs cannot be spread by touch or the sharing of utensils used by an infected person. Sexual contact by itself cannot spread the germs, unless extrapulmonary TB of the genital organs is involved.
It is important to understand that there is a difference between being infected with TB and hav-ing TB disease. Someone who is infected with TB has the TB germs, or bacteria, in his/her body. The body’s defenses are protecting them from the germs, and they are not sick. Someone with TB disease is sick and, if not properly treated, can spread the disease to other people. A person with symptoms of TB disease or evidence of infection needs to be seen by a physician.
Several symptoms are associated with TB, including prolonged coughing (including cough-ing up blood), repeated night sweats, unexplained weight loss, loss of appetite, fever, chills, and general lethargy. Because these signs may be indicative of other diseases as well, a person must consult a physician to determine the cause of these symptoms.
The simplest way to find out if you have a TB infection is to get a TB skin test (or TST), which is widely available at clinics or at a doctor’s office (some health departments use IGRAs or blood tests to identify TB infection). For a TST, a small amount of testing material is injected under the very top layers of skin on the forearm. In 48 to 72 hours the reaction is read by a trained person, usually a nurse or doctor. If the test is positive, then you probably have TB infectionand the doctor will run more tests, such as a chest x-ray, to determine whether you have TB disease. In some groups, such as the elderly or those with impaired immunity, a simple skin test (or IGRA) may not be enough to determine whether they have TB infection. Furtherevaluation may be necessary for these individuals if they have symptoms of signs of TB.
* From American Lung Association of Texas Fact Sheet.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 23
Most TB can be cured. There are drugs that can kill the germs that cause TB, but a person must continually take the prescribed medication, usually for 6 months. Some patients require a year or more for successful treatment.
If a person stops taking the medicine before completing treatment, the germs may come back more resilient than before. Surviving bacteria may become resistant to the drugs used to treat TB, causing multidrug-resistant TB (MDR-TB).
Anyone can get TB. It strikes people of all races, ages, and income levels. Certain groups are at higher risk. These include:
• People who associate with others who have active TB disease• Poor and medically underserved• Homeless people• Those who come from countries with high TB incidence rates• People in congregate settings, such as nursing homes or prisons• Alcoholics and intravenous drug users• People with medical conditions that impair their immunity, such as HIV or AIDS, or
who are undergoing treatments likely to impair their immune systems• The elderly• Healthcare workers and others who come in contact with high-risk populations,
e.g., prison guards
SCORING:
• Did the candidate translate exactly what was written? Was the meaning of the message translated accurately, without adding, deleting, or changing anything?
• Did the candidate successfully deal with the style and contextual assumptions of the original document?
• How did the candidate negotiate ambiguous terms?
• Did the candidate ask for clarification of any words or concepts that he/she did not understand?
• Was the candidate’s speech well-paced, clear, and understandable?
• Does the candidate work with a language that lacks equivalents of Western medical terms, or with a community that is less likely to understand Western medical practices and technology? If so, how well did the interpreter convey the intended meaning of the source text?

9. Oral Exam on Healthcare Terms – Part I of II
Terms like the following should be very familiar to the interpreter in both English and the target language. Terms should cover a variety of body systems, as TB patients’ medical history rarely includes only respiratory disease. To assess a candidate’s knowledge of medical terms, the interviewer can read each word to the candidate in English and have him/her repeat it into the target language. Responses can be audiotaped for someone to listen, rate, and evaluate the accuracy of responses.
From English Into Target Language ankle
appendectomy
aspirin
biopsy
bladder
bronchoscopy
cardiologist
chemotherapy
chills
coughing up blood
diabetes
directly observed therapy (DOT)
distended abdomen
elevated levels
extrapulmonary TB
eye drops
fever
gall bladder
gastrointestinal
glucose test
gynecologist
high blood pressure
inpatient
insulin
intensive care unit
intramuscular
intravenously
kidney
laparoscopy
latent TB infection (LTBI)
laterally
laxative
lethargy
24

From English Into Target Language leukemia
liver function tests (LFTs)
loss of appetite
lungs
medication
multidrug-resistant TB (MDR-TB)
night sweats
nocturnal
normally
outpatient
oxygen
pediatrician
periodically
physical therapy
primary care
primary symptoms
progression from infection to disease
prolonged coughing
pulmonologist
radiology
regularly
shortness of breath
sputum specimens
sterilizer
surgery
tuberculosis (TB)
TB skin test (TST)
thigh
throbbing headaches
to become infected
to draw blood
to elevate
to examine
to intubate
tumor
ultrasound
unexplained weight loss
wheelchair
x-ray
Scoring Candidate should be able to interpret 70% of above terms, accurately, into the target language.
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 25

26
Oral Exam on Healthcare Terms – Part II of II Additional healthcare terms related to TB
Terms like the following should be very familiar to the interpreter in both English and the target language. Terms should cover a variety of body systems, as TB patients’ medical history rarely includes only respiratory disease.
To assess a candidate’s knowledge of medical terms, the interviewer can read each word to the candidate in English and have him/her repeat it into the target language. Responses can be audiotaped for someone to listen, rate, and evaluate the accuracy of responses.
From English Into Target LanguageAnatomical terms:alveoli (air sacs)
bronchi
bronchioles
larynx
lungs
nose
nasal passages
pharynx
pleura
Procedures:arterial blood gases (ABG)
biopsy
bronchoscopy
glucose test
intravenously
laparoscopy
laxative
liver function test (LFT)
lobectomy
physical therapy
pulmonary function studies
pneumonectomy
spirogram
sputum culture
TB skin test (TST)
to draw blood
to elevate
to examine
to intubate

From English Into Target Language tracheostomy tracheotomy ultrasound x-ray
Symptoms: barrel chest chills coughing up blood cyanosis cystic fibrosis distended abdomen dyspnea fatigue fever hemoptysis lethargy loss of appetite malnutrition night sweats nocturnal orthopnea shortness of breath throbbing headaches unexplained weight loss paroxysmal nocturnal dyspnea primary symptoms prolonged coughing rales
Specialties and departments: cardiologist gynecologist inpatient intensive care unit outpatient pediatrician pulmonologist radiology
Therapies: chemotherapy directly observed therapy (DOT) INH therapy
(table continues on next page)
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 27

From English Into Target Language insulin medication oxygen treatment of latent TB infection (preventive therapy)
Diagnoses: asthma atelectasis bronchitis bronchiectasis chronic obstructive airway disease (COAD) chronic obstructive lung disease (COLD) chronic obstructive pulmonary disease (COPD) emphysema extrapulmonary TB high blood pressure interstitial fibrosis laryngitis miliary TB multidrug-resistant TB (MDR-TB) mycobacterial infection mycotic infection pneumoconiosis pneumonia pneumonitis pulmonary embolism pulmonary fibrosis pulmonary hypertension pulmonary infarction pulmonary thrombosis tuberculosis (TB) tumor
Public Health/Community TB Control Terms: case management contact investigation exposure face mask infectious period transmission Scoring
Candidate should be able to interpret 70% of above terms, accurately, into the target language.
28
ConclusionAn assessment of the interpreter’s skills alone is not sufficient to ensure the quality of the inter-preter’s performance. On-the-job training and supervision are necessary in order for interpreters to hone their skills and enhance their understanding of the interpreter role.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 29
B. INTERPRETER SERVICE MODELS: BENEFITS AND DRAWBACKS
The interpreter can help to establish a better rapport with the patient, which should result in better outcomes in the areas of compliance, utilization, and satisfactory completion of TB
treatment. In selecting an interpreter, one or more of the following sources can be utilized:
1. Hospital- or clinic-based interpreters – Due to frequent needs for healthcare interpreters, an organizaion can employ hospital- or clinic-based interpreters. These interpreters must be trained in the skills, concepts, and ethics of interpreting.
Benefits:• Meets the needs of the institution and many needs of the patients. Issues of organiza-
tional efficiency and liability may be addressed, and patients may have a higher level of satisfaction and compliance with their treatment
• Interpreters are employed for their skills as opposed to holding a dual position as out-reach caseworker and interpreter
Drawbacks:• May be cost prohibitive to many public health clinics. The language spoken by the inter-
preter must be encountered frequently enough to keep a full or part-time interpreter
• Interpreter may perceive conflict between his/her neutral role as a language services pro-vider and his/her loyalty to the employer
2. Language pools and agencies for on-site interpretation – Interpreters are not limited to a particular institution or service area. They typically provide broader access to social service, health, educational, and legal services.
Benefits:• Often this approach is more efficient as services can be provided in a greater number of
languages, and many of the training components would be similar for a number of ser-vice areas
• Interpreters are centrally coordinated, and the coordinating body usually provides train-ing and supervision. Many community “language banks” also are based on this model
• Interpreters can remain neutral. Cost to the organization is less than keeping a staff person dedicated to interpreting. The organization can access the numerous languages that can be supported by a dedicated interpreter organization
Drawbacks:• Interpreters may not be available for walk-ins and urgent cases. When the interpreter is
requested from an external agency, finding an available interpreter and allowing travel time to the patient’s location can take longer than the patient and provider can wait
• Interpreters may not have had training or experience in medical vocabulary and healthcare settings

30
3. Telephone interpreters – The most common form of telephone interpretation is remote tele-phone interpretation services or “language lines” which are used frequently in the United States.
Benefits:• These services can be invaluable in emergency situations (e.g. , Emergency Medical
Technicians at an accident scene) as they are available in many languages on a 24-hour basis
Drawbacks:• While these are expensive on a per-minute basis, these services can be cost-effective if
there is only occasional demand for a certain language or when the appointment might be less than a 15-minute encounter, for example, in directly observed therapy (DOT)
While considered superior in quality to ad hoc interpretation, telephone interpreters may not have the specific medical training required.
4. Medical and non-medical bilingual staff – Another way to address language barriers is to rely on non-medical bilingual staff employed in other positions within the healthcare organization.
Benefits:• In some situations these interpreters may have medical training, while others will have
no medical experience
Drawbacks:• Because these staff members, in general, might not have received training in interpretation
skills, concepts or ethics, you cannot assume that the quality of interpretation that they deliv-er is any better than that provided by family members or community volunteers
• Caution should be used when asking bilingual staff to interpret. While it is often assumed that hospital staff trained as medical professionals in their own countries would be ideal interpreters, this is not always the case
• A related concern is the inefficiency of removing staff from their regular duties. Resentment often arises when additional duties are placed on bilingual staff without recognition or compensation. Monolingual colleagues who are required to “pick up the slack” also may experience this resentment while the bilingual staff member provides interpretation services
• There may be significant class or political differences between the participant and the “interpreter” which may create the potential for role conflict for intervening as a health professional
Note: Note: The Policy Guidance Memorandum from the Health and Human Services’ Office for Civil Rights states that individuals used as interpreters should be trained in the skills, con-cepts, and ethics of interpreting.
Bilingual providersIt would be ideal for the organization to hire healthcare providers to communicate directly with a patient in his/her own language, but this is not often possible. While this form of com-munication is not interpreting, such providers should demonstrate fluency in both English and the target language.
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 31
5. Ad hoc (untrained) interpreters – The individual functioning as the interpreter is not trained and may be an adult family member or child of the patient. Sometimes volunteers from com-munity agencies, church groups, etc. are used as interpreters.
Benefits:• This method may seem appealing because of the low or no cost to the provider or
provider agency
Drawbacks:• PROVIDER, BEWARE. The use of untrained family members and community volunteers
can result in word omissions, substitution, and semantic errors that can distort symp-toms and instructions
• Patient confidentiality may be breached and it creates barriers to the provider-patient relationship
• It can upset familial relationships and hierarchies that are deeply rooted in culture. For these reasons, children under 16 years of age should never be used as interpreters
• It can be more harmful than helpful when the word substitutions, errors, and patient unwillingness to fully disclose information are taken into account.
C. GUIDELINES FOR SELECTING A TELEPHONE INTERPRETING
SERVICE PROVIDER
A telephone interpreting provider offers immediate language services by phone. The hospital or clinic may subscribe to this service for a fee. When considering to contract with a telephone
interpreting company, some guidelines for selecting a provider are as follows:
1. Access 24/7/365 – There should never be a concern about accessing the appropriate interpreter. Service should be available 24 hours a day, 7 days a week, 365 days a year.
2. Quick connect time to the appropriate interpreter – When time is paid for by the minute or, more importantly, in a life or death situation, a quick connect time to an interpreter is of utmost consequence. The company should be able to measure their connect time and share this information. A connect time should average no longer than 45 seconds from the moment the caller is greeted until the interpreter comes on the line.
3. Diversity means a 100 language minimum – As many as 250 languages are spoken in some communities. Therefore, a company offering a diversity of languages is preferable. Choose a service with access to the specific languages commonly spoken.
4. Interpreter training and development – To ensure that companies use interpreters trained in the field of medical interpreting, request the name or components of their medical training and refer back to the company’s training manual as a guide for accepted norms in the medical interpreting field. Other important training and development would include an assessment of the interpreter’s language skills in English and the target language, phone etiquette, customer service, and continuing education opportunities.

32
5. Emergency preparedness – The telephone service provider must be able to satisfy a request even during a “disaster.” Make sure that a back-up system is in place and that the company can remain operational.
6. Competitiveness – Be cautious! Sometimes interpreting companies charge more than the “basic” rate they quote for languages that are less frequently requested and for requests during their night hours or on weekends. The ideal fee structure is one flat (per-minute) rate for any language, at any time, with no service set-up fee.
7. High tech call center – Since “connect” time is an established standard of comparison for telephone interpreting, a technical system capable of supporting connect time, as well as the multiple calls that may come in, is crucial. Ask about what type of equipment is needed and the number of customer service agents available to connect customers when they call.
8. Customer reports for quality improvement and business management – Ask the telephone interpreting company what reports they can routinely offer their clients. Monitor usage by:• Department• Budget category• Language used• Quality improvement efforts
Good reports also will help financial staff reconcile specific budgets and appropriate charges
9. A satisfied current customer base – A good language pool will expect that potential clients will ask for references from their current customers. Three types of references to select are: • A small organization• A local organization, if available• A very large organization
Ask the references about their satisfaction with the service and performance from the tele-phone interpreting company.
10. After-sales support – Check that the company has assigned a specific service representative. It is better to have a dedicated service representative contact rather than trust the luck of the draw of customer service during a call. Ask them about other services they might offer.
For example, if an organization needs assistance with retrofitting phones suitable for tele-phone interpreting, their current hardware may not be suitable. They will want to use a ser-vice that is willing to provide this technical support and advice.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 33
D. GUIDELINES FOR SELECTING A LANGUAGE POOL
A language pool may offer interpreting services by phone, in person, or by appointment for a moderate fee. Language pools are often run by nonprofit organizations in the local com-
munity. When thinking about contracting with a language pool, here are some guidelines for selecting one. These are very similar to the guidelines for selecting a telephone interpreting ser-vice, with the exception of #2 and #7 below.
1. Access 24/7/ 365 – There should never be a concern about accessing the appropriate interpreter. Service should be available 24 hours a day, 7 days a week, 365 days a year. Sometimes smaller community pools do not have the resources to operate for 24 hours a day. For example, they may only work from 6 a.m. to 10 p.m. However, their ability to assist with small language groups outweighs the inconvenience of securing them and an alternate telephone service for times they are unavailable.
2. Ability to provide an on-site interpreter upon 24 hour notice – On-site interpretation will seldom be as responsive as telephone interpreting. However, satisfying a request that is made 24 hours prior to the scheduled appointment time is a realistic expectation.
3. Diversity means a 100 language minimum – As many as 250 languages are spoken in some communities. Therefore, a company offering a diversity of languages is preferable. Choose a service with access to the specific languages commonly spoken.
4. Interpreter training and development – To ensure that companies use interpreters trained in the field of medical interpreting, request the name or components of the medical training and refer back to the company’s training manual as a guide for accepted norms in the medical interpreting field. Other important training and development would include an assessment of the interpreter’s language skills in English and the target language, ethics, and continuing education opportunities.
5. Emergency preparedness – The telephone service provider must be able to satisfy a request even during a “disaster.” Make sure that a back-up system is in place and that the company can remain operational.
6. Competitiveness – Be cautious! Sometimes interpreting companies charge more than the “basic” rate they quote for languages that are less frequently requested and for requests dur-ing their night hours or on a weekend. The ideal fee structure is one flat rate for any language at any time.
7. Responsive call center – The language pool should have a schedule of who is available during business hours. The system for scheduling a patient’s interpreter should be straightforward and reliable.

34
8. Customer reports for quality improvement and business management – Ask the telephone interpreting company what reports they can routinely offer their clients. Monitor usage by:• Department• Budget category• Language used• Quality improvement efforts
Good reports also will help financial staff reconcile specific budgets and appropriate charges.
9. A satisfied current customer base – A good language pool will expect that potential clients will ask for references from their current customers. Three types of references to select are: • A small organization• A local organization, if available• A very large organization
Ask the references about their satisfaction with the service and performance from the telephone interpreting company.
10. After-sales support – Check that the company has assigned a specific service representative. It is better to have a dedicated service representative contact rather than trust the luck of the draw of customer service during a call. Ask them about other services they might offer.
For example, an organization may need assistance with translating their consent forms. They may want to use a service that is willing to provide this technical support and advice.

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 35
III. Legal Issues Related To Healthcare Interpreting
A. LEGAL ISSUES RELATED TO HEALTHCARE INTERPRETING B. TITLE VI OF THE CIVIL RIGHTS ACT OF 1964
C. SUMMARY OF LAWS AND POLICIES
A. LEGAL ISSUES RELATED TO HEALTHCARE INTERPRETING
Medical interpreting is an emerging discipline. There are few recognized experts in the field; one of these is Cynthia Roat with the National Council on Interpreting in
Healthcare (NCIHC). She provides the following introduction to this topic of laws related to medical interpreting.
“Around the U.S., hospitals and clinics are becoming more aware of their legal respon-sibility to provide linguistic access to their services for patients who speak limited English. For example, the Americans with Disabilities Act clearly supports the provi-sion of interpreters as well as other methods to guarantee clear communication with patients who are deaf or hard of hearing. Also, Title VI of the Civil Rights Act of 1964 states that no organization receiving federal funds may run its programs in such a way as to create discrimination on the basis of race, color, or country of national origin. This means that any institution receiving Medicaid or Medicare, for example—essentially every major medical center in the country—must provide language access to those who need it. The institution cannot charge the patient for this service, and the use of family and friends is generally not acceptable. Some clinics provide language access by hiring bilingual providers, but in most cases, the answer is an interpreter.”
A summary of the Title VI of the Civil Rights Act of 1964 can be found on the next page followed by a brief list of key laws and policy guidance concerning provision of services to people with limited English proficiency (LEP).

36
B. TITLE VI OF THE CIVIL RIGHTS ACT OF 1964*
T itle VI of the Civil Rights Act of 1964 is a national law that protects persons from discrimination based on their race, color, or national origin in programs and activities that receive Federal
financial assistance. If you are eligible for Medicaid, other healthcare, or human services, you cannot be denied assistance because of your race, color, or national origin. The Office for Civil Rights (OCR) in the U. S. Department of Health and Human Services (DHHS) enforces Title VI as well as other civil rights laws.
Some of the institutions or programs that may be covered by Title VI are:
• Extended care facilities • Public assistance programs • Nursing homes • Adoption agencies • Hospitals • Day care centers • Mental health centers • Senior citizen centers • Medicaid and Medicare • Family health centers and clinics • Alcohol and drug treatment centers
Prohibited Actions – There are many forms of illegal discrimination based on race, color, or national origin that frequently limits the opportunities of minorities to gain equal access to ser-vices. A recipient of Federal financial assistance may not, based on race, color, or national origin:
• Deny services, financial aid, or other benefits provided as a part of health or human Deny services, financial aid, or other benefits provided as a part of health or human Deny services,service programs
• Provide a different service, financial aid, or other benefit, or provide them in a different manner from those provided to others under the program
• Segregate or separately treat individuals in any matter related to the receipt of any service, financial aid, or other benefit
More common discriminatory practices are identified in the DHHS Title VI regulation found at 45 CFR Part 80, www.hhs.gov/ocr/part80rg.htmlwww.hhs.gov/ocr/part80rg.htmlwww.hhs.gov/ocr/part80rg.html
For information on how to file a complaint of discrimination, or to obtain information of a civil rights nature, please contact the Office for Civil Rights, Department of Health and Human Services. Employees will make every effort to provide prompt service.
Hotlines: 1-800-368-1019 1-800-368-1019 (Voice) 1-800-537-7697 1-800-537-7697 (TDD)
E-Mail: [email protected] Website: http://www.hhs.gov/ocr/title6.htmlhttp://www.hhs.gov/ocr/title6.htmlhttp://www.hhs.gov/ocr/title6.htmlhttp://www.hhs.gov/ocr/title6.htmlhttp://www.hhs.gov/ocr/title6.html
* From Title VI Fact SheetTitle VI Fact Sheet by the U.S. Department of Health and Human Services Office for Civil Rights. by the U.S. Department of Health and Human Services Office for Civil Rights.Title VI Fact Sheet by the U.S. Department of Health and Human Services Office for Civil Rights.Title VI Fact SheetTitle VI Fact Sheet by the U.S. Department of Health and Human Services Office for Civil Rights.Title VI Fact Sheet

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 37
C. SUMMARY OF LAWS & POLICIES
The following is a summary of key federal and national laws and policies concerning provision of service to people with limited English proficiency (LEP). Failure to review the complete text of
these laws and policy guidance may result in misinterpretation and misapplication. Individual state's laws may have similar or more stringent requirements.
Law & Policy Summary For More Information
Title VI of Civil Rights Act of 1964From Title VI Fact Sheet by the U.S. Department of Health and Human Services Office for Civil Rights.
Title VI of the Civil Rights Act of 1964 is a national law that protects per-sons from discrimination based on their race, color, or national origin in programs and activities that receive Federal financial assistance. The Office for Civil Rights (OCR) in the U. S. Department of Health and Human Services (DHHS) enforces Title VI as well as other civil rights laws.
More common discriminatory practices are identified in the U. S. Department of Health and Human Services (DHHS) Title VI regulation found at 45 CFR Part 80. www.hhs.gov/ocr/part80rg.htmlFor more information on how to file a complaint of discrimination, or to obtain information of a civil rights nature, please contact:Office of Civil Rights, DHHSHotlines: 1-800-368-1019 (Voice) 1-800-537-7697 1-800-537-7697 (TDD)Email: Web: http://hhs.gov/ocr/title6.htmlhttp://hhs.gov/ocr/title6.html
United States Department of Health and Human Services Policy Guidance on the Prohibition Against National Origin Discrimination as it Affects Persons with Limited English Proficiency
Policy guidance clarifies responsibili-ties of providers of health and social services who receive federal financial assistance from the U. S. Department of Health and Human Services (DHHS).
For a complete text of this policy guidance, please refer to:www.hhs.gov/ocr/lep/guide.htmlwww.hhs.gov/ocr/lep/guide.html
National Standards for Culturally and Linguistically Appropriate Services in Healthcare (2001)
These national standards issued by the U.S. Department of Health and Human Services (HHS) and Office of Minority Health (OMH) respond to the need to ensure that all people entering the healthcare system receive equitable and effective treatment in a culturally and linguistically appropriate manner.
For the complete text of these stan-dards, please refer to:www.omhrc.gov/assests/pdf/ checked/finalreport.pdf

38
Law & Policy Summary For More Information
Executive Order 13166 Issued by President Clinton on August 11, 2000. Contains two major initiatives. The first is designed to better enforce and implement an existing obligation: Title VI of the Civil Rights Act of 1964 and the sec-ond initiative indicates that federal agencies should ensure that feder-ally-funded entities in their area of responsibility know the general standards for LEP access and apply the agency’s plan to the activities they are conducting on behalf of the agency.
For the complete text of this Executive Order, please refer to
Disadvantaged Minority Health Improvement Act
The Act specifically states that feder-ally supported community health centers are required to provide pri-mary healthcare services in the lan-guage of the intended recipient.
From 42 USC Section 3000-6(b)7
Hill-Burton Act An additional legal source for stipu-lating healthcare providers’ obliga-tion to serve the LEP population is the Hill-Burton Act. Otherwise known as the Hospital Survey and Construction Act of 1946, the Hill-Burton Act provided funds for the construction and improvement of numerous public and nonprofit com-munity hospitals, health centers and nursing homes.
http://www.hhs.gov/ocr/hbcsreg.htmlhttp://www.hhs.gov/ocr/hbcsreg.htmlhttp://www.hhs.gov/ocr/hbcsreg.htmlhttp://www.hhs.gov/ocr/hbcsreg.htmlhttp://www.hhs.gov/ocr/hbcsreg.html
Violations of LEP Policies and Guidelines
To better understand the implica-tions of LEP policies and guidelines, it may be useful to review examples and actual cases involving com-plaints filed with the Office for Civil Rights related to access to services for LEP persons.
http://www.usdoj.gov/crt/legalinfo/http://www.usdoj.gov/crt/legalinfo/http://www.usdoj.gov/crt/legalinfo/http://www.usdoj.gov/crt/legalinfo/http://www.usdoj.gov/crt/legalinfo/
Criminal Violations of Civil Rights, Federally Assisted Programs.
tual cases, see: http://www.hhs.gov/ocr/selectacts/http://www.hhs.gov/ocr/selectacts/http://www.hhs.gov/ocr/selectacts/http://www.hhs.gov/ocr/selectacts/http://www.hhs.gov/ocr/selectacts/

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 39
Law & Policy Summary For More Information
Ensuring Linguistic Access: Rights and Responsibilities (197 pages) produced by National HealthLaw Program
An excellent summary of legal requirements to provide language services.
Can be ordered by calling the Henry J. Kaiser Family Foundation at 800-656-4533 800-656-4533 or through their website at www.kff.orgwww.kff.org

42

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 41
IV. Resources
A. LANGUAGE-APPROPRIATE PATIENT MATERIALS
B. B.
B. MEDICAL INTERPRETATION PROVIDERS
Please note: These listings of materials and providers does not constitute an endorsement from the Francis J. Curry National Tuberculosis Center. This information is for reference only.
A. LANGUAGE-APPROPRIATE PATIENT MATERIALS
Association of Asian Pacific Community Health Organizations (AAPCHO)“Stop TB” poster is available in Chinese, Ilocano, Korean, Tagalog, and Vietnamese.300 Frank H. Ogawa Plaza, Suite 620
Phone: (510) 272-9536 Fax: (510) 272-0817
Centers for Disease Control and Prevention (CDC) Answers to frequently asked questions and TB: http://www.cdc.gov/tb/faqs/defalut.htm TB Education and Training Resources website: http://www.findtbresources.org/scripts/index.cfm�� - This website is inteded for use by TB and other healthcare professionals, patients, and the general- public. Some TB educational materials are offered in different languages.- Language website directory: http://www.cdc.gov/Other/languages - This site includes materials in Chinese, French, German, Italian, Korean, Russian, Spanish,Tagalog, - and Vietnamese
Ethnomed
Cultural profiles and translated patient education materials available in Amharic, Cambodian, Oromo, Somali, Spanish, Tigrinya, and Vietnamese.
http://www.ethnomed.org/ Florida Department of Health This site contains educational materials in Arabic, Bosnian, English, Farsi, Korean, Spanish, Haitian, Creole, Serbian, Russian, and Vietnamese, including “Get The Facts about TB” and “Breathe Easier." http://www.doh.state.fl.us/Disease_Ctrl/tb/Educational-materials/edmat.html
Oakland, CA 94612
http://www.aapcho.org/site/aapcho/content.php?type=6&id=55
HHS Healthfinder EspañolDesigned to provide Spanish speaking consumers with easy access to reliable health information. Offers a Spanish text search and a list of topics in Spanish that can be browsed. This site makes it easy for users of the site to switch between Spanish and English versions of the same information. English speaking family members or health professionals can use this feature to search in English for information to share with Spanish speaking relatives or patients.http://www.healthfinder.gov/espanol
C. CULTURAL COMPETENCY MATERIALS

42
Portland, OR 97201Phone: (503) 641-9393 or (503) 241-9393
Minnesota Department of HealthBrochure and fact sheets for patients are available in Amharic, Arabic, Bosnian, Croatian, English,Hmong, Karen, Khmar , Laotian, Oromo, Russian, Somali, Spanish, Tibetan, and Vietnamese.http://www.health.state.mn.us/divs/idepc/diseases/tb/factsheets/translations.html
National Center for Farmworker Health (NCFH)NCFH provides a wide range of services dedicated to improving the health of the workers who harvest America’s crops. The site includes resources such as low literacy, bilingual (English/Spanish) patient educational materials, videos, and other healthcare provider resources. Materials are downloadable or available at cost to non-profit entities.http://www.ncfh.
NSW Multicultural Health Communication ServiceBased in Australia, Multicultural Health Communication Service aims to facilitate the communi-cation of quality information about health issues and health services to people of non-English speaking backgrounds. This site contains multilingual health information in 42 languages including: Arabic, Bosnian, Chinese, Croatian, English, Farsi, French, German, Khmer/Cambodian, Korean, Lao, Russian, Spanish, Thai, and Vietnamese.http://mhcs.health.nsw.gov.au/
Patient Education Resources for Clinicians, Oregon Health and Science University LibrariesThis site provides web resources for patient education materials. It includes a list of Spanish sites,low literacy handouts in Spanish, and other non-English language of sites of interest.http://www.ohsu.edu/library/patiented/links.shtml
Refugee Assistance Project“Skin Test for Tuberculosis” available in LaotianP.O. Box 355, Building #501725 W 17th StreetSanta Ana, CA 92702Phone: (714) 834-2379
Indochinese Language Resource Center “Positive Skin Test? So What” and “INH, a Pill Between You and TB” available in Laotian. 3030 SW 2nd Avenue
Medical Leadership Council on Cultural Proficiency (MLC) MLC Language Access Database provides links to downloadable patient education materials in languages other than English. http://www.medicalleadership.org/educational_patient.shtml
New York University School of Medicine, Centers for Immigrant Health TB brochures are available in Bengali, Chinese, Creole, English, French, Korean, Russian, Spanish, Tibetan, and Urdu.
http://www.med.nyu.edu/cih/tb/brochures.html
Selected Patient Information Resources in Asian Languages (SPIRAL)Provides access to patient information materials that were created by non-profit health agencies and organizations. This site contains educational materials in English, Cambodian, Chinese, Hmong,Japanese, Korean, Laotian, Thai, and Vietnamese.http://spiral.tufts.edu/

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 43
Utah Department of Health (UDOH), Center for Multicultural Health (CMH)The CMH provides health education materials in many languages to assist health professionals incommunicating with people who don’t speak English or have a low English proficiency.http://www.health.utah.gov/cmh/multilinguallibrary.htm
B. MEDICAL INTERPRETATION PROVIDERS
This list provides resources in the following categories:• Face-to-face Interpreting Services• Telephone Interpreting Services• Medical Interpreter Training Organizations• Medical Encyclopedias/Dictionaries• Helpful Websites
1. FACE-TO-FACE INTERPRETING SERVICES
American Translators Association-Interpreters Division (ATA)This division provides support for interpreters through networking and information sharing. This site contains articles on all types of interpreting, including medical interpreting. This site is also a good place to find out the latest developments in interpreter certification across the country and includes a nationwide directory of interpreters.http://www.atanet.org/index.php
Austin Area Translators and Interpreters Association (AATIA)AATIA serves members through education, networking, and promotion of the translation and interpretation professions through meetings, conferences, workshops, The AATIA Letter The AATIA Letter, and a , and a The AATIA Letter, and a The AATIA Letter The AATIA Letter, and a The AATIA Letterwebsite. Its Medical and Community Interpreters Special Interest Group focuses on the needs of interpreters in medical and social service settings. This organization includes interpreters of all specialties, including medical, community, court, and conference interpreting throughout Texas. Paper or online directory at http://www.aatia.org/
California Healthcare Interpreting Association (CHIA)This organization includes healthcare interpreters throughout California. CHIA offers continu-ing education seminars, healthcare interpreter conferences, referral resources for interpreters, newsletters, and a website.http://chiaonline.org/ International Medical Interpreters Association (IMIA)The IMIA is committed to the advancement of professional medical interpreters as the best practiceto equitable language access to healthcare for linguistically diverse patients. http://www.imiaweb.org/default.asp
Interpreters IndexSan Diego, CaliforniaThis index lists interpreters in all specialties throughout the country.www.interpretersindex.comwww.interpretersindex.com or Fax
Texas Refugee Interpreters Coalition (TRIC)Austin and San Antonio: 800-975-9772800-975-9772 Dallas/Fort Worth: Houston: 713-776-4700713-776-4700 Amarillo: 806-345-7907 This organization includes healthcare interpreters throughout Texas.

44
2. TELEPHONE INTERPRETING SERVICES
Albors & Associates, IncWinter Park, FloridaFace-to-face, telephone interpreting, and translation services for medical, legal, insurance, rehabilitation, engineering, advertising, and government agencies, 215 languages.https://www.altrausa.com 1-800-785-8634 CyraCom International, Inc.Tucson, ArizonaTelephone interpreting services in medical, business, and legal fields.150 languages, 24 hours a day, 7 days a week.http://www.cyracom.net 1-800-713-4950 Interpreter.com 170 languages, 24 hours a day, 7 days a week. http://www.interpreter.com 1-800-497-5038 Interpreters Unlimited San Diego, CA Interpretation by telephone is available in more than 130 languages. http://www.interpretersunlimited.com/ 1-800-566-7492
Language Line ServicesMonterey, CaliforniaTelephone interpreting services in medical, business, and government fields.170 languages, 24 hours a day, 7 days a week, 365 days a year.http://www.languageline.com 1-800-752-6096
Language Translation, Inc. San Diego, CaliforniaTelephone interpreting services in medical, legal, business, and government fields.150 languages, 24 hours a day, 7 days a week, 365 days a year.http://www.languagetranslation.com 1-800-655-3397
Languatek, Inc.East Aurora, New York150 languages, 24 hours a day, 7 days a week, 365 days a year.http://www.languatek.com 716-652-9887 Lionbridge Technologies, Inc.Waltham, MassachusettsFace-to-face, telephone interpreting services for business, legal, healthcare, and governmental agencies.250 languages. http://www.lionbridge.com/lionbridge/en-US/services/interpretation/medical.htm 1-800-423-6756 x4045 Network Omni Multilingual CommunicationsWestlake Village, CaliforniaFace-to-face, telephone interpreting in medical, business, and legal fields. 150 lanuguages, 24 hours a day, 7 days a week. http:www.networkomni.com/ 1-800-543-4244 or 818-706-7890

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 45
Pacific InterpretersPortland, OregonTelephone interpreting services in medical, business, and legal fields.180 languages, 24 hours a day, 7 days a week.
http://pacificinterpreters.com 1-800-311-1232
3. MEDICAL INTERPRETER TRAINING ORGANIZATIONS
ACEBOSpreckels, CaliforniaInterpreter training materials: The interpreter’s RX self-paced training manual and audio CDs for medical interpreters. The Interpreter’s Companion- glossary of medical and legal terminologyhttp://www.acebo.com 831-455-1507 or fax 831-455-1541
Bridging the Gap; A Basic Training for Medical InterpretersCross Cultural Health Care ProgramSeattle, Washingtonhttp://www.xculture.org/BTGwelcome.php 1-800-691-9441
Verbatim SolutionsSalt Lake City, UtahTelephone interpreting services in medical and legal fields. 120 languages, 24 hours a day, 7 days a week.
http://www.verbatimsolutions.com 1-800-573-5702
International Medical Interpreters Association (IMIA) MassHealth Access Program (MAP) Boston, Massachusetts http://www.imiaweb.org/default.asp 508-856-4849
NYC School of Medicine, Center for Immigrant Health Working with Medical Interprters Training New York City, New York http://www.med.nyu.edu/cih/language/interpretation.html 212-263-8783
Dr. Koop’s Health Encyclopedia Excellent information on medical tests and hundreds of diseases in lay terms. http://www.drkoop.com/ency/93/diseidxa.html
4. DICTIONARY RESOURCES
Medline Plus Multilingual DirectoryMedline is the National Library of Medicine’s online database that contains 11 million references to journal articles in the health sciences. To access hundreds of topics in different languages, click on multiple languages by health topic.http://medlineplus.gov/ Your Dictionary.ComMassive portal for dictionaries and languages services on the web. It contains over 1,500 dictionaries.http://www.yourdictionary.com/language/index.html

46
5. HELPFUL WEBSITES
Cross Cultural Health Care Program (CCHCP)Through a combination of cultural competency trainings, interpreter trainings, research projects, community coalition building and other services, the CCHCP serves as a bridge between communitiesand healthcare institutions to ensure full access to quality healthcare that is culturally and linguistically appropriate. This site lists books, resources, news on an access to care issues, and links to other sites. http://www.xculture.org
Kaiser Family FoundationThis site includes a section on minority health that contains state-by-state data by race/ethnicity for population demographics, insurance coverage, and health status.http://www.statehealthfacts.kff.org
Limited English Proficiency (LEP) - A Federal Interagency WebsiteProvides information and guidance on language access for federal agencies, recipients of federal funds, and community based organizations and individuals.http://www.lep.gov
CBS News: Health Watch - MedscapeSite created to meet the needs of non-MD’s and consumers. Blending Medscape's longstandingreputation for trusted, health information with innovative, interactive management tools to helpsupport personal health and wellness.http://www.cbsnews.com/sections/health/main204.shtml
National Council on Interpreting in HealthcareNCIHC is a multidisciplinary organization whose mission is to promote culturally competent profe- ssionalhealthcare interpreting as a means to support equal access to health services for individuals with limitedEnglish proficiency.http://ncihc.org/mc/page.do
Healthfinder.Gov - U.S. Department of Health and Human ServicesProvides resources on a wide range of reliable health information and the latest news from over1,600 government and non-profit organizations. http://www.healthfinder.gov
C. CULTURAL COMPETENCY MATERIALS
Cross Cultural Health Care Program (CCHCP) Through a combination of cultural competency trainings, interpreter trainings, research projects, community coalition building and other services, the CCHCP serves as a bridge between com- munities and healthcare institutions to ensure full access to quality healthcare that is culturally and linguistically appropriate. This site lists books, resources, news on an access to care issues, and links to other helpful sites. http://www.xculture.org
Ethnomed
Cultural profiles and translated patient education materials available in Amharic, Cambodian, Oromo, Somali, Spanish, Tigrinya, and Vietnamese.
http://www.ethnomed.org/

Kaiser Family FoundationThis site includes a section on minority health that contains state-by-state data by race/ethnicity for population demographics, insurance coverage, and health status.http://www.statehealthfacts.kff.org
National Council on Interpreting in HealthcareNCIHC is a multidisciplinary organization whose mission is to promote culturally competent professional healthcare interpreting as a means to support equal access to health services for individuals with limited English proficiency.http://ncihc.org/mc/page.do
New Jersey Medical School Global Tuberculosis Institute
Southeastern National Tuberculosis Center (SNTC)SNTC is one of four Regional Training and Medical Consultation Centers (RTMCC) in the U.S. This site contains several products named that provide background information, epidemiology, common misperceptions and beliefs about TB and HIV/AIDS, general practices and cultural courtesies from various countries (Dominican Republic,Ecuador, Honduras, India, Mexico, Philippines, Somalia, Vietnam). This site also contains PSAs and posters in Spanish.http://sntc.medicine.ufl.edu/Products.aspx
This website offers an audio file "An Introduction to Cultural Competency in TB Prevention and Control" which provides a basic foundation for understanding cultural differences in health attitudes, beliefs, behaviors, and language, which can help individuals function moreeffectively in cross-cultural patient encounters. This site also contains "TB and CulturalCompetency: Notes from the Field Newsletters." http://www.umdnj.edu/globaltb/audioarchives/culturalcompetency.htmhttp://www.umdnj.edu/globaltb/products/newsletter.htm (Newsletter)
Berkeley Media, LLC"A World of Differences: Understanding Cross-Cultural Communication" This video examines 14 different facets of both verbal and nonverbal cross-cultural
misunderstandings. http://www.berkeleymedia.com/search/
Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 47

36

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 49
V. Glossary
GLOSSARY
1st person voice Interpreter uses “I/me/my” statements during interpretation
3rd person voice When interpreter intervenes for a transparent clarification, interpreter refers to himself/herself in 3rd person voice by using “he/him/his” or “she/her/hers” statements
Accuracy Interpreter interprets everything the speaker says without changing the meaning and conveying what is said, and how it is said without additions, deletions, or alterations, but with due consideration of the cultural context of both the sender and the receiver of the message
Completeness Interpreter conveys the meaning of gestures, body language, and tone of voice of the speaker
Cultural competence A set of practiced skills, knowledge, and attitudes, that mustencompass 5 elements: awareness and acceptance of difference;awareness of own cultural values; understanding the dynamics of
difference; development of cultural knowledge; ability to adapt
Hand signal Interpreter raises hand to patient or provider to request a pause to interpret accurately or for clarification
Interpretation Involves conversion of SPOKEN words from one language to another and requires the use of an interpreter
Intervention The process of intervening allows the interpreter to break into the provider/patient dialogue when a specific problem arises
LEP “Limited English Proficient” is a term used by the Office of Civil Rights to describe patients/clients who have limited English proficiency
Consecutive interpretation When one speaker starts to say a few sentences, then pauses for the interpreter to interpret. This process is repeated with the next speaker, providing continuous interpretation until the dialogue is complete
practice skills to fit the cultural content of the client or patient
Face-to-face Interpretation Interpreter is present with both, or at least one of the personswhom interpreting is provided
5
Pre-session A introduction made to both the provider and patient before theappointment begins. Sets the parameters for how the interpreter will operate and specifies ways that the provider and patient can help the interpreter to be effective. May also be used to alertprovider to cultual issues
Proper positioning
To facilitate as much direct communication as possible between patient and provider, the interpreter sits/stands beside and slightly behind the patient during interpreted session
Sight translation Oral translation of a written document into the target language
Simultaneous interpretation Occurs when the interpreter interprets at the same time as the speaker is speaking
Transparent clarification Occurs when the interpreter needs to intervene and stop the conversation with a hand signal, then switches to third person voice, and refers to interpreter as “the interpreter”
Telephone interpreting Interpreting carried out remotely, with the interpreter connectedby telephone to doctor and patient
Translation Involves conversion of WRITTEN text from one language to another and requires the services of a translator
Note-taking Interpreter can take notes on things that can be easily trans-posed such as numbers, dosages and times. This helps to keep the interpretation accurate
Post-session An opportunity to learn from interpreter about cultural topicsor behavior that can assist in effective interaction between patient and provider
50

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 51
VI. Appendix
A. DISCUSSION TOPICS
B. B. B. SLIDES FROM THE VIDEO
A. DISCUSSION TOPICS
I f the video is shown in a group setting, the following questions may be used during the video or at the end of the video to stimulate discussion. Although these discussion topics are not
designed to be all-inclusive or definitive, they serve as a learning tool to share experiences, explore ideas and solutions.
Topic A: Considerations when working with limited English proficient TB patients
1. What challenges do you face while working with limited English proficient TB patients?2. What challenges do limited English proficient TB patients face while working with
healthcare providers?
Topic B: Deciding what type of interpretation service to use
How do you address language issues with limited English proficient TB patients?
Topic C: Working with untrained interpreters
How do you currently work with nonprofessional or untrained healthcare interpreters?

52
DISCUSSION TOPICS: ANSWER KEY
Although answers will vary, listed below are some possible responses.
Topic A: Considerations when working with limited English proficient TB patients
1. What challenges do you face in working with limited English proficient TB patients?
Sample response(s):Sample response(s):• Understanding language and cultural differences
2. What challenges do limited English proficient TB patients face in working with healthcare providers?
Sample response(s):Sample response(s):• Patient has to see and learn to trust the clinic as a non-immigration and naturalization
service related agency that is truly concerned with helping them to get better• Language and cultural differences
Topic B: Deciding what type of interpretation service to use
How do you address language issues with limited English proficient TB patients?
Sample response(s):Sample response(s):As much as possible, recruit and assign bilingual workers
• If there is no one available among the staff, ask for help from someone in the patient’s community who can be trusted with patient confidentiality
• Telephone interpreters (language lines)
Topic C: Working with untrained interpreters
How do you currently work with nonprofessional or untrained healthcare interpreters?
SaSample response(s):mple response(s):Spanish-speaking co-workers are used as interpreters

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 53
B. SLIDES FROM THE VIDEO

54

Making the Connection: An Introduction to Interpretation Skills for TB Control, 2nd Edition 55

56

















