Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment— An Update EDWARD T. RYAN EPIDEMIOLOGY Overview An estimated 300 million cases of malaria occur each year, annually accounting for 1.5 to 2.7 million deaths (1). Most of these deaths are due to infection with Plasmodium falci- parum and occur among children and pregnant women in the developing world, especially sub-Saharan Africa. Unfortunately, mortality during severe or complicated malaria still exceeds 10% to 30% (2). Due to increasing resistance among malaria parasites to chemotherapeutic agents, dissolution of malaria control programs, and increasing inter- national travel, the incidence of malaria is increasing worldwide. Large scale multinational efforts have been initiated to “roll back malaria,” including major commitments of finan- cial, clinical, and research resources (3,4). Malaria in Travelers Although the overwhelming majority of morbidity and mortality associated with malaria occurs in the developing world, this disease also affects travelers. Without chemoprophy- laxis, a traveler’s risk of acquiring malaria is highest in areas of Oceania (more than 20% per month in regions of New Guinea) and in sub-Saharan Africa (approximately 2% per month); the risk is intermediate in South Asia (0.1% to 0.01% per month); and lowest in the Americas and Southeast Asia (less than 0.01% per month) (5–7). Each year, approxi- mately 30,000 individuals who travel from industrialized nations to the developing world contract malaria, and more than 1000 cases of malaria are reported to the Centers for Disease Control and Prevention (CDC) in the United States (8,9). Although malaria can occur after travel to any malarious area, most cases of malaria reported in the United States occur after travel to Africa (40% to 50% of reported malaria cases), the South Asia-Indian subcontinent region (approximately 25% of cases), and Central America and the Caribbean (15% to 20% of cases) (9,10). Malaria can present months or even years after travel (Table 4.1). Of the cases reported in the United States, approximately 40% to 50% involve infection with P. vivax, 35% to 45% are due to P. falciparum, 4% are caused by P. malariae, 2% to 3% are due to P. ovale, approximately 5% involve unknown species, and less than 1% are due to multiple species (9). Malaria in travelers is largely preventable: most occurrences are due to inadequate or incorrect pre-travel advice or lack of compliance with a recommended chemopro- 83
Transcript
Malaria: Epidemiology, Pathogenesis,Diagnosis, Prevention, and Treatment—An Update
EDWARD T. RYAN
EPIDEMIOLOGY
Overview
An estimated 300 million cases of malaria occur each year, annually accounting for 1.5 to2.7 million deaths (1). Most of these deaths are due to infection with Plasmodium falci-parum and occur among children and pregnant women in the developing world, especiallysub-Saharan Africa. Unfortunately, mortality during severe or complicated malaria stillexceeds 10% to 30% (2). Due to increasing resistance among malaria parasites tochemotherapeutic agents, dissolution of malaria control programs, and increasing inter-national travel, the incidence of malaria is increasing worldwide. Large scale multinationalefforts have been initiated to “roll back malaria,” including major commitments of finan-cial, clinical, and research resources (3,4).
Malaria in Travelers
Although the overwhelming majority of morbidity and mortality associated with malariaoccurs in the developing world, this disease also affects travelers. Without chemoprophy-laxis, a traveler’s risk of acquiring malaria is highest in areas of Oceania (more than 20%per month in regions of New Guinea) and in sub-Saharan Africa (approximately 2% permonth); the risk is intermediate in South Asia (0.1% to 0.01% per month); and lowest inthe Americas and Southeast Asia (less than 0.01% per month) (5–7). Each year, approxi-mately 30,000 individuals who travel from industrialized nations to the developing worldcontract malaria, and more than 1000 cases of malaria are reported to the Centers forDisease Control and Prevention (CDC) in the United States (8,9).
Although malaria can occur after travel to any malarious area, most cases of malariareported in the United States occur after travel to Africa (40% to 50% of reported malariacases), the South Asia-Indian subcontinent region (approximately 25% of cases), andCentral America and the Caribbean (15% to 20% of cases) (9,10).
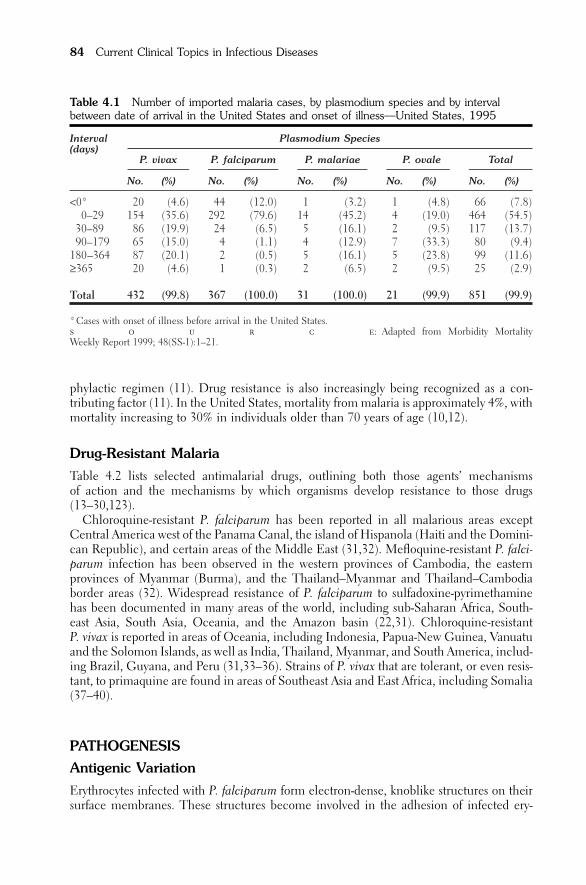
Malaria can present months or even years after travel (Table 4.1). Of the cases reportedin the United States, approximately 40% to 50% involve infection with P. vivax, 35% to45% are due to P. falciparum, 4% are caused by P. malariae, 2% to 3% are due to P. ovale,approximately 5% involve unknown species, and less than 1% are due to multiple species(9).
Malaria in travelers is largely preventable: most occurrences are due to inadequate or incorrect pre-travel advice or lack of compliance with a recommended chemopro-
83
phylactic regimen (11). Drug resistance is also increasingly being recognized as a con-tributing factor (11). In the United States, mortality from malaria is approximately 4%, withmortality increasing to 30% in individuals older than 70 years of age (10,12).
Drug-Resistant Malaria
Table 4.2 lists selected antimalarial drugs, outlining both those agents’ mechanisms of action and the mechanisms by which organisms develop resistance to those drugs(13–30,123).
Chloroquine-resistant P. falciparum has been reported in all malarious areas exceptCentral America west of the Panama Canal, the island of Hispanola (Haiti and the Domini-can Republic), and certain areas of the Middle East (31,32). Mefloquine-resistant P. falci-parum infection has been observed in the western provinces of Cambodia, the easternprovinces of Myanmar (Burma), and the Thailand–Myanmar and Thailand–Cambodiaborder areas (32). Widespread resistance of P. falciparum to sulfadoxine-pyrimethaminehas been documented in many areas of the world, including sub-Saharan Africa, South-east Asia, South Asia, Oceania, and the Amazon basin (22,31). Chloroquine-resistant P. vivax is reported in areas of Oceania, including Indonesia, Papua-New Guinea, Vanuatuand the Solomon Islands, as well as India, Thailand, Myanmar, and South America, includ-ing Brazil, Guyana, and Peru (31,33–36). Strains of P. vivax that are tolerant, or even resis-tant, to primaquine are found in areas of Southeast Asia and East Africa, including Somalia(37–40).
PATHOGENESIS
Antigenic Variation
Erythrocytes infected with P. falciparum form electron-dense, knoblike structures on theirsurface membranes. These structures become involved in the adhesion of infected ery-
84 Current Clinical Topics in Infectious Diseases
Table 4.1 Number of imported malaria cases, by plasmodium species and by intervalbetween date of arrival in the United States and onset of illness—United States, 1995
* Cases with onset of illness before arrival in the United States.s o u r c e: Adapted from Morbidity MortalityWeekly Report 1999; 48(SS-1):1–21.
throcytes to vascular endothelium, and they may be possibly involved in erythrocyte roset-ting (41). The knobs are composed of both host and parasite proteins, including the para-site proteins KAHRP (knob-associated histidine-rich protein) and PfEMP-1 (P. falciparumerythrocyte membrane protein-1) (41). The large (250 to 320kDa) PfEMP-1 proteins areencoded by the var (“variety”) family of genes (42–46). Approximately 150 var genes havebeen identified to date, although the number that are functional is not currently known(45,47). A number of var genes may be transcribed within a specific P. falciparum parasite,
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 85
Table 4.2 Selected antimalarial drugs: mechanisms of action and resistance
Drug Mechanism of Action Mechanism of Resistance
Chloroquine Inhibition of heme metabolism Decreased intraparasite accumulation of by the parasite (13,14) chloroquine. Probably predominantly
mediated by mutations in PfCRT, atransmembrane protein in the parasitephagolysosome, resulting in increasedefflux of chloroquine from the lysosome (14,15). Mutations in multidrug resistance (MDR) P-glycoprotein pumps (Pgh) encoded by Pfmdr1 and Pfmdr2 may also contribute (14–21)
Mefloquine, Probably inhibition of heme Mefloquine and halofantrine resistancehalofantrine, metabolism may be related to amplification ofquinine Pfmdr1, increased expression of Pgh1,
mutations in pfcrt, and increased efflux of drug (22,23). The details of quinine resistance have not been established, although quinine and mefloquine resistance often correlate (24).
Cycloguanil, Block folate synthesis via Resistance mediated through pointchlorcycloguanil, inhibition of dihydrofolate mutations in dhfr and dhps genes, pyrimethamine reductase (DHFR) although more efficient use of available Sulfonamides and Block folate synthesis via folate may also contribute (24–29).sulfones inhibition of dihydropteroate (sulfadoxine, synthase (DHPS)dapsone)
Atovaquone Inhibition of mitochondrial Point mutations in mitochondriallyelectron transport in encoded cytochrome b gene (123).cytochrome bc1 complex,resulting in collapse of mitochondrial membrane potential
Artemisinin Damage of intraparasitic Stable resistance not yet identified inderivatives organelles and alkylation of clinical isolates.
parasite proteins via intraparasite heme-catalyzed production of carbon-centered free radicals (24,30)
but only one var gene is dominantly expressed on the surface of an infected erythrocyte atany given time (48,49).
PfEMP-1 proteins are involved in cytoadhesion of P. falciparum-infected erythrocytes to thrombospondin (TSP) and several endothelial cell receptors, including CD36, inter-cellular adhesion molecule 1 (ICAM-1), vascular adhesion molecule (VCAM), andendothelial leukocyte adhesion molecule (ELAM) (Figure 4.1) (45,50–54). Infected erythrocytes expressing a PfEMP-1 protein that binds ICAM-1 have been associated withcerebral malaria (55,56). In addition, PfEMP-1 proteins have been identified that mediatebinding of infected erythrocytes to chondroitin sulfate A and hyaluronic acid—both mol-ecules that are expressed in large amounts in placental tissue; this relationship may partlyexplain the placental sequestration of infected erythrocytes during pregnancy (52). Aftertargeted cytoadhesion, local tissue hypoxia and nitric oxide production ensue, contribut-ing to the malarial pathophysiology (57). Specific binding of P. falciparum-infected erythrocytes to endothelial cells of placental tissue is also mediated by non-PfEMP-1 pro-teins (58).
In addition to var genes, a number of other multigene families have been identified in P. falciparum, including stevor, rif, and Pf60 gene families (59,60). Proteins encoded bystevor and rif are variable surface antigens of unknown function (although rif products areinvolved in rosette formation of infected erythrocytes) (4,60). Proteins encoded by Pf60remain in the nucleus and have an unknown function (59).
86 Current Clinical Topics in Infectious Diseases
Figure 4.1. Schematic of a P. falciparum-infected erythrocyte expressing aPfEMP-1 with anti-CD36 binding capacity. Other endothelial surface moleculesrepresented are intercellular adhesion molecule-1 (ICAM-1), vascular adhesionmolecule (VCAM), and endothelial leukocyte adhesion molecule (ELAM).
Immunity
Immunity to malaria develops over several years of almost continuous exposure and infec-tion. It is characterized by a gradual decrease in the frequency and severity of clinicaldisease. Repetitive waves of antigenic variation may account for this gradual onset of immu-nity (61–64). Recent work has also elucidated more about the nature of immunity:
• Erythrocytes infected with P. falciparum also adhere to dendritic cells, inhibiting their maturationand reducing their capacity to stimulate T cells (65).
• Cohabitating strains of malaria (strains of the same species of plasmodium simultaneously presentwithin a host) influence each other’s survival by downregulating cellular immune responsesthrough altered peptide ligand antagonism of naturally occurring variant cytotoxic T-cell epitopes(66,67).
• Cross-species interactions of malaria parasites result in nonindependent, sequential episodes ofinfection with different species of plasmodia (68).
Immunization with a malaria vaccine containing certain T-cell epitopes could, therefore,impede the ability to control infection with a strain expressing a related but distinct T-cellepitope (68). In addition, a malaria vaccine that proves successful against one species ofmalaria might possibly increase the incidence of disease due to another strain (68).
DIAGNOSIS
Worldwide, microscopy remains the tool of choice for diagnosing malaria. In comparisonto analysis of blood by polymerase chain reaction (PCR), microscopy is 85% to 95% sensitive and 95% to 100% specific (69,70). Microscopic examination of peripheral bloodstained with Giemsa, Wright’s and Field’s stains permits detection of 10 to 100 parasitesper microliter of blood, and microscopy permits species identification. Microscopy is,however, time-consuming and requires sufficient operator expertise.
Fluorescent microscopy has also been used to identify malaria parasites (69). One suchassay is the QBC Malaria Test system (Becton Dickinson, Sparks, Maryland). In this assay,a sample of blood is mixed in a capillary tube with acridine orange, microcentrifuged, andanalyzed under fluorescent microscopy. Although it gives results more quickly than tradi-tional microscopy (preparing, spinning, and reading the sample requires 10 minutes),species identification can be more problematic with this assay (71–73). Moreover, in com-parison to thin- and thick-smear analysis, the QBC system is 70% to 100% sensitive and85% to 95% specific, with its sensitivity falling to 40% to 70% when fewer than 100 para-sites are present per microliter of blood (69,71,72,74–78). Although the QBC system isuseful, the requirement for a fluorescent microscope and tabletop centrifuge has limitedits use in much of the developing world.
More recently, a number of rapid diagnostic tests have been developed that detect par-asite proteins in peripheral blood. Some of these tests detect malaria histidine rich proteinII (HRPII), such as the ParaSight F-test (Becton Dickinson), the ICT Malaria P.f.test/MalaQuick (ICT Diagnostic, Sydney, Australia), the PATH P. falciparum malaria ICstrip (Program for Appropriate Technology in Health, Seattle, Washington), and the Deter-mine Malaria Pf test (Abbot Laboratories, Japan) (79–81). Early versions of these assaysdetected only HRPII of P. falciparum; newer-generation assays, however, detect antigens ofboth P. falciparum and P. vivax (such as the ICT Malaria P.f./P.v. test) (82). In addition,assays that detect all four malaria species are under development (69).
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 87
Another group of assays have been developed that detect plasmodial lactate dehydroge-nase (pLDH) via immunochromatographic detection (OptiMAL kit; Flow, Inc., Portland,Oregon), or via enzymatic reaction (ICpLDH; Flow, Inc.) (83). The pLDH assays are ableto detect antigens of both P. falciparum and P. vivax (84).
The diagnostic abilities of the various HRP and pLDH rapid assays are comparable. Incomparison to thin- and thick-blood-smear analysis, these assays are approximately 90% to95% sensitive and 85% to 95% specific, although sensitivity of the rapid assays is muchlower (30% to 60%) in the presence of low parasitemia (fewer than 50 to 100 parasites permicroliter of blood) and even occasionally in the presence of very high parasitemia(69,83,85–88).
Although the rapid diagnostic assays offer a number of attributes that make them attrac-tive for use in the developing world (minimally trained personnel find them easy to use,no equipment is required, and samples can be read with the naked eye), they also have anumber of disadvantages that limit their utility:
• The assays are unable to quantify the level of parasitemia (except for the ICpLDH assay) (83).
• They are currently unable to detect all malarial species.
• They are unreliable in the presence of low-level (and occasionally even very-high-level) para-sitemia (88).
• They remain positive for 7 to 14 days after treatment (complicating discernment of relapsing,recrudescent, or cured malaria at follow-up visits) (86,89).
• They may give false-positive reactions in individuals with positive rheumatoid factor (especiallyHRP-detecting assays) (69,90,91).
Recent studies have also shown that these rapid diagnostic assays are dangerous whenused by travelers to self-diagnose malaria (80). In this setting, false-negative interpretationsare frequent in the presence of low-level parasitemia (and even with high-level parasitemiawith some of the assays) (80). The assays are, however, useful when performed by trainedlaboratory personnel and probably will have their greatest utility in areas of the world withextremely limited resources or with limited expertise in microscopic diagnosis of malaria(92,93). The assays are also more sensitive than microscopic analysis of peripheral bloodin identifying women with placental malaria (94).
PREVENTION OF MALARIA
Malaria can be prevented through interventions that minimize the number of mosquitobites, including the appropriate use of N,N diethylmethyltoluamide (DEET)-containinginsect repellents and permethrin-impregnated bednets and clothing (1,95–99). The diseasecan also be prevented through the judicious use of effective chemotherapeutic agents(Table 4.3). Unfortunately, the use of chemotherapeutic agents remains impractical inmuch of the developing world, although targeted use during pregnancy can be beneficial(100–102). In such areas, both chloroquine prophylaxis and intermittent presumptive treat-ment with sulfadoxine-pyrimethamine during pregnancy are safe and may be effective(100–102). Although prophylactic use of mefloquine in pregnant women is also safe andmore effective than chloroquine in preventing malaria, mefloquine’s expense has limitedits use (103–105).
The decision to use a chemoprophylactic agent to prevent malaria in a traveler should
88 Current Clinical Topics in Infectious Diseases
weigh that individual’s risk of acquiring malaria against the possibility that the person will develop an adverse reaction to the selected agent. The selection of an agent (or thechoice to use no agent at all) should reflect the traveler’s medical condition and medica-tions taken, the time of year of travel, the individual’s destination, the susceptibility ofmalaria parasites to various agents in that destination, and the person’s overall risk of acquir-ing malaria. Resources giving standard recommendations on the prevention of malariashould be consulted when advising travelers (32,106,107). Note that travelers to certaindestinations, including most urban areas and tourist destinations in Latin America andSoutheast Asia, often require no chemoprophylaxis, although they should practice behav-ioral modification to limit their risk of insect-borne diseases, including the use of insectrepellents.
Chloroquine
Chloroquine is the drug of choice for prophylaxis of individuals at high risk of acquiringmalaria who are traveling to areas of the world in which chloroquine-resistant malaria hasnot been reported (32,107). The most common side effect associated with this agent is pru-ritus, which is usually most severe in individuals of African descent. Chloroquine can exac-erbate psoriasis or porphyria. When extremely high dosages of chloroquine are ingestedover prolonged periods, retinopathy may develop (108). In addition, this drug can causecardiac arrhythmias, especially in individuals with underlying arrhythmic disorders of theheart, including prolonged QT syndrome (108).
Chloroquine’s bitter taste usually requires that it be mixed with a sweet agent for con-sumption by young children (109). Nursing children should be given an individual doseof chloroquine because insufficient quantities are expressed in breast milk.
Concomitant use of chloroquine and intradermal administration of human diploid cellrabies vaccine (HDCV) can result in lower immune responses to the vaccine (32,109).Intradermal administration of HDCV should be completed seven days before beginningchloroquine prophylaxis; alternatively, HDCV can be given intramuscularly or anotherrabies vaccine can be administered without concern for interaction.
Amodiaquine is an aminoquinoline related to chloroquine that is used in some areas ofthe world. Its association with rare, but idiosyncratic toxic hepatitis and agranulocytosis haslimited its use (110).
Mefloquine
Mefloquine is a 4-quinoline methanol with a half-life of 7 to 30 days. In the United States,this drug is a chemoprophylactic agent of choice for individuals at high risk of acquiringchloroquine-resistant malaria (32). When used as a prophylactic agent, mefloquine isextremely effective, with efficacy rates exceeding 90% to 95% (5,7,111). It is usuallyextremely well tolerated by most individuals. Severe neuropsychiatric reactions, includingseizures and psychosis, occur in approximately 1 in 10,000 to 1 in 13,000 users of pro-phylactic mefloquine, however. Fewer than 5% of individuals who use prophylactic mefloquine report milder neuropsychological adverse events, including sleep disturbances,insomnia, nightmares, cognitive changes, anxiety, or depression that are disabling enoughto result in drug discontinuation(1,112–116). Long-term use of mefloquine has not beenassociated with additional adverse effects (111).
Mefloquine should not be used in individuals with underlying cardiac arrhythmias orconduction disturbances, individuals with a history of psychiatric illnesses such as psychosis
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 89
Tabl
e 4.3
Pro
phyl
axis
for
mal
aria
*†
Med
icat
ion
Adult
Dose
Ped
iatr
ic D
ose
Chl
oroq
uine
-sens
itive
are
as‡
Chl
oroq
uine
pho
spha
te30
0m
g ba
se (
500
mg
salt)
onc
e pe
r w
eek,
beg
inni
ng 1
to 2
wee
ks
5m
g/kg
bas
e (8
.3m
g/kg
sal
t), u
p to
adu
lt do
se,
befo
re e
nter
ing
and
cont
inui
ng u
ntil
4 w
eeks
afte
r le
avin
g on
ce p
er w
eek,
as
for
adul
tsm
alar
ious
are
a
Chl
oroq
uine
-resi
stan
t ar
eas‡
Mefl
oqui
ne§
228
mg
base
(25
0m
g sa
lt) in
Uni
ted
Stat
es (
250
mg
base
out
side
<15
kg: 5
mg/
kg (
salt)
; 15–
19kg
: 1 / 4ta
blet
;U
nite
d St
ates
) on
ce p
er w
eek,
beg
inni
ng 1
to 2
wee
ks b
efor
e 20
–30
kg: 1 / 2
tabl
et; 3
1–45
kg: 3 / 4
tabl
et;
ente
ring
and
cont
inui
ng u
ntil
4 w
eeks
afte
r le
avin
g m
alar
ious
>45
kg: 1
tabl
et, o
nce
per
wee
k, a
s fo
r ad
ults§
area
§
OR
Dox
ycyc
line¶
100
mg
once
per
day
, beg
inni
ng 1
to 2
day
s be
fore
ent
erin
g an
d 2
mg/
kg/d
ay, u
p to
adu
lt do
se, a
s fo
r ad
ults¶
cont
inui
ng u
ntil
4 w
eeks
afte
r le
avin
g m
alar
ious
are
a
OR
Atov
aquo
ne/p
rogu
anil||
One
250
mg/
100
mg
tabl
et o
nce
per
day,
beg
inni
ng 1
to 2
day
s 11
–20
kg: 6
2.5
mg/
25m
g; 2
1–30
kg:
befo
re e
nter
ing
and
cont
inui
ng u
ntil
7 da
ys a
fter
leav
ing
125
mg/
50m
g; 3
1–40
kg: 1
87.5
mg/
75m
g;m
alar
ious
are
a>4
0kg
: 250
mg/
100
mg,
dai
ly, a
s fo
r ad
ults
90
Alte
rnat
ives
Prim
aqui
ne**
30m
g ba
se o
nce
per
day,
beg
inni
ng 1
to 2
day
s be
fore
ent
erin
g 0.
5m
g/kg
bas
e da
ily, u
p to
adu
lt do
se, a
s fo
ran
d co
ntin
uing
unt
il 7
days
afte
r le
avin
g m
alar
ious
are
aad
ults
OR
Chl
oroq
uine
pho
spha
teSe
e ab
ove
See
abov
e
PL
US
prog
uani
l††20
0m
g on
ce p
er d
ay, b
egin
ning
1 to
2 d
ays
befo
re e
nter
ing
and
<2 y
ears
: 50
mg;
2–6
yea
rs: 1
00m
g; 7
–10
cont
inui
ng u
ntil
4 w
eeks
afte
r le
avin
g m
alar
ious
are
aye
ars:
150
mg;
>10
yea
rs: 2
00m
g, d
aily
, as
for
adul
ts
Mefl
oqui
ne-re
sist
ant
area
s‡
Dox
ycyl
ine¶
See
abov
eSe
e ab
ove
Atov
aquo
ne/p
rogu
anil‡‡
See
abov
eSe
e ab
ove
*If
an in
divi
dual
is a
t hig
h ris
k of
con
tract
ing
mal
aria
and
is ta
king
che
mop
roph
ylax
is, c
onsid
er p
rimaq
uine
pho
spha
te 1
5m
g ba
se (
child
ren
0.3
mg/
kg b
ase,
up
to a
dult
dose
)da
ily fo
r la
st tw
o w
eeks
of c
hem
opro
phyl
axis
to d
ecre
ase
likel
ihoo
d of
late
-ons
et m
alar
ia d
ue to
P. v
ivax
and
P. o
vale
. Do
not g
ive
if th
e pa
tient
is g
luco
se 6
-pho
spha
te d
ehy-
drog
enas
e de
ficie
nt o
r pr
egna
nt. N
ot r
equi
red
if th
e ch
emop
roph
ylax
is us
ed d
urin
g ex
posu
re is
prim
aqui
ne.
†Pr
esum
ptiv
e se
lf-tre
atm
ent o
f mal
aria
is n
ot r
outin
ely
reco
mm
ende
d; in
divi
dial
s w
ith fe
ver
at r
isk fo
r m
alar
ia s
houl
d se
ek m
edic
al a
ttent
ion.
Exp
ert a
dvic
e m
ay b
e be
nefic
ial
for
trave
lers
who
will
be
unab
le to
obt
ain
timel
y m
edic
al c
are
and
for
trave
lers
who
can
not t
ake
the
optim
al p
roph
ylax
is.‡C
hlor
oqui
ne-re
sista
nt P
. fal
cipa
rum
has b
een
repo
rted
in a
ll m
alar
ious
are
as e
xcep
t Mex
ico,
Cen
tral A
mer
ica
wes
t of t
he P
anam
a C
anal
, Hai
ti, th
e D
omin
ican
Rep
ublic
, and
scat
tere
d ar
eas
of th
e M
iddl
e E
ast.
Mefl
oqui
ne-re
sista
nt P
. fal
cipa
rum
has
been
rep
orte
d in
Wes
tern
pro
vinc
es o
f Cam
bodi
a, E
aste
rn p
rovi
nces
of M
yanm
ar (
Bur
ma)
, and
the
bord
er r
egio
ns b
etw
een
Tha
iland
and
Mya
nmar
and
bet
wee
n T
haila
nd a
nd C
ambo
dia.
§M
efloq
uine
may
be
adm
inist
ered
wee
kly
for
thre
e w
eeks
bef
ore
ente
ring
a m
alar
ious
are
a, o
r it
may
be
front
-load
ed w
ith d
aily
dos
ing
for
thre
e co
nsec
utiv
e da
ys (
of n
orm
alw
eekl
y do
se),
then
wee
kly
until
fou
r w
eeks
afte
r le
avin
g th
e m
alar
ious
are
a. M
efloq
uine
sho
uld
not
be u
sed
by i
ndiv
idua
ls w
ith a
hist
ory
of p
sych
iatri
c ill
ness
, sei
zure
s, or
card
iac
cond
uctio
n ab
norm
aliti
es. I
t is
not a
ppro
ved
for
use
durin
g pr
egna
ncy,
alth
ough
its
use
at p
roph
ylac
tic d
osag
es is
pro
babl
y sa
fe, e
spec
ially
dur
ing
the
seco
nd a
nd th
irdtri
mes
ters
. Lim
ited
data
sug
gest
that
it is
saf
e du
ring
the
first
trim
este
r. T
he p
edia
tric
dosa
ge is
not
app
rove
d by
the
U.S
. Foo
d an
d D
rug
Adm
inist
ratio
n (F
DA)
, but
is r
ecom
-m
ende
d by
the
Cen
ters
for
Dise
ase
Con
trol a
nd P
reve
ntio
n.¶D
o no
t use
in p
regn
ant w
omen
and
chi
ldre
n yo
unge
r th
an 8
yea
rs o
f age
. Dox
ycyc
line
can
caus
e ph
otos
ensit
ivity
and
vag
inal
mon
ilias
is, a
nd it
can
dec
reas
e th
e ef
ficac
y of
horm
onal
con
trace
ptiv
e ag
ents.
Tak
e w
ith fo
od; d
o no
t sim
ulta
neou
sly u
se a
ntac
ids
or b
ismut
h-co
ntai
ning
pro
duct
s an
d do
xycy
clin
e.||Fi
xed
com
bina
tion
tabl
ets
cont
aini
ng 2
50m
g at
ovaq
uone
/100
mg
prog
uani
l an
d 62
.5m
g at
ovaq
uone
/25
mg
prog
uani
l ar
e av
aila
ble
in t
he U
nite
d St
ates
(M
alar
one;
Gla
xoW
ellc
ome)
. Tak
e w
ithin
45
min
utes
afte
r ea
ting.
Mal
aron
e is
U.S
. FD
A ap
prov
ed fo
r pr
ophy
laxi
s (a
nd tr
eatm
ent)
of P
. fal
cipa
rum
only
. Effi
cacy
as
prop
hyla
xis
agai
nst o
ther
spec
ies
is le
ss w
ell d
efine
d at
pre
sent
, and
may
be
low
er th
an th
at a
gain
st P.
falc
ipar
um.
**Ta
ke w
ith fo
od. D
o no
t use
in p
regn
ant w
omen
and
indi
vidu
als
defic
ient
in g
luco
se 6
-pho
spha
te d
ehyd
roge
nase
. Taf
enoq
uine
, a r
elat
ed a
gent
, is
curr
ently
bei
ng e
valu
ated
.††
Not
ava
ilabl
e in
the
Uni
ted
Stat
es. C
hlor
oqui
ne–p
rogu
anil
has
decr
ease
d ef
ficac
y ag
ains
t m
alar
ia c
ompa
red
with
mefl
oqui
ne a
nd d
oxyc
yclin
e in
are
as w
here
it
has
been
studi
ed. C
hlor
oqui
ne–p
rogu
anil
has
been
use
d sa
fely
in p
regn
ancy
.‡‡
Prel
imin
ary
data
sug
gest
atov
aquo
ne/p
rogu
anil
is ef
fect
ive
in th
e pr
even
tion
of m
alar
ia c
ause
d by
mul
ti-dr
ug r
esist
ant P
. fal
cipa
rum
. Effi
cacy
aga
inst
othe
r sp
ecie
s of
mal
aria
may
be
low
er.
so
urc
e:
Adap
ted
from
dat
a pu
blish
ed in
Rya
n E
T, K
ain
KC
. Hea
lth a
dvic
e an
d im
mun
izat
ions
for
trave
lers
. N E
ngl J
Med
200
0;34
2:17
16–1
725.
91
and anxiety disorders, and individuals with a history of seizures. The drug is commonlyused in children who are at high risk of acquiring chloroquine-resistant malaria (32).Although specific pediatric dosages have not been approved by the U.S. Food and DrugAdministration, they are recommended by the CDC (32).
Because it takes six to nine weeks to achieve therapeutic blood levels of mefloquine withstandard weekly dosing (117), some authorities recommend that individuals begin meflo-quine prophylaxis two to three weeks before they enter a malarious area. Alternatively,mefloquine may be taken as a once-daily dose (of the weekly dose) consecutively for threedays, one to two weeks before entering a malarious area (109,117,118). Such “front-loading” achieves therapeutic blood levels in approximately four days (109,117,118) andpermits early identification of individuals who are intolerant of mefloquine (109,119).Approximately 2% of “front-loaded” individuals will discontinue mefloquine prophylaxis,usually because of dizziness or gastrointestinal upset (109,119).
Doxycycline
Doxycycline may be used by individuals at risk of chloroquine-resistant malaria who cannottake mefloquine; it is also a drug of choice for all individuals at risk of malaria traveling toareas of the world reporting mefloquine-resistant malaria (7,32,109,120). When used as aprophylactic agent, doxycycline has a protective efficacy equivalent to that of mefloquine—that is, greater than 90% (1,7). The apparent lower efficacy of doxycycline relative tomefloquine is attributable to poor compliance with daily dosing (121).
Doxycycline should not be administered to children younger than 8 years of age, nor should it be used by pregnant or lactating women. Its adverse effects include the following:
• Photosensitivity—including sensitivity to both ultraviolet A and ultraviolet B light.
• Vaginal moniliasis—especially in women who have a history of recurrent yeast infections.
• Decreased efficacy of hormonal contraceptive agents—women using such agents should use abackup mechanism of contraception for at least two cycles after stopping doxycycline.
• Gastrointestinal upset—doxycycline should be taken with a meal.
• Esophageal erosions—especially in individuals with gastroesophageal reflux or if the medicine istaken immediately before reclining; doxycycline should, therefore, be taken with an 8-oz glass ofwater and should not be taken at bedtime.
• Decreased absorption when ingested with heavy metals such as bismuth and those in antacids—doxycycline should not be taken simultaneously with these agents (109).
Atovaquone and Proguanil
Atovaquone is a hydroxynaphthoquinone that inhibits mitochondrial electron transport(122,123). Resistance to atovaquone develops rapidly when this agent is used alone(123,124). Proguanil hydrochloride is a prodrug that is metabolized in vivo to cycloguanil.This agent is both a blood and tissue schizonticide, inhibiting the growth of both bloodand the pre-erythrocytic liver stage of the parasite. It is not effective against the latent hypnozoite intrahepatic forms of P. vivax and P. ovale, however (125). Resistance toproguanil develops rapidly when the agent is used alone.
The combination of atovaquone and proguanil acts synergistically against plasmodia
92 Current Clinical Topics in Infectious Diseases
in vitro and in vivo (124,126). Interestingly, when proguanil is used with atovaquone, it appears to act as the parent molecule (proguanil), rather than as the metabolite(cycloguanil); that is, proguanil does not act as a dihydrofolate reductase inhibitor whenused with atovaquone (24). The synergy with atovaquone appears to result from a lower-ing of the effective concentration at which atovaquone collapses mitochondrial membranepotential in malaria parasites (126).
Because of its unique mechanism of action, atovaquone has similar activity against bothchloroquine-sensitive and chloroquine-resistant strains of P. falciparum. Both atovaquoneand proguanil have causal prophylactic activity against the liver stages of P. falciparum(127). The combination therapy is not effective against the latent hypnozoite forms of P. vivax and P. ovale, however (128).
Three placebo-based clinical trials have examined prophylactic use of the atovaquone–proguanil combination in African adults and children with uncomplicated P.falciparum malaria. In those studies, compared to placebo, daily atovaquone–proguanil wasfound to be safe, well tolerated, and 95% to 100% effective against P. falciparum parasitemia(129–131). A number of completed or ongoing studies have evaluated (or are addressing)the prophylactic use of atovaquone-proguanil in nonimmune adults (132,133). In thesestudies, atovaquone-proguanil has been shown to be well tolerated and highly efficaciousin preventing malaria caused by P. falciparum (95%). The efficacy of atovaquone andproguanil as a prophylactic combination regimen against P. vivax, P. ovale, and P. malar-iae has been less well studied, although preliminary data would suggest that the drug combination is less effective against P. vivax (70–90%) than against P. falciparum (95%)(124,134,135).
An atovaquone–proguanil combination (Malarone; GlaxoWellcome Inc., Research Tri-angle Park, NC) has recently become available in the United States for use as a prophy-lactic regimen against P. falciparum malaria, including the prevention of chloroquineresistant P. falciparum. The combination is well tolerated; infrequently reported adverseevents include mild nausea, vomiting, abdominal pain and diarrhea, and transient asymp-tomatic elevations in serum hepatic transaminase and amylase values (1).
Primaquine
Primaquine is an 8-aminoquinoline antimalarial agent with causal prophylactic activity. Itdestroys pre-erythrocytic hepatic stages of the parasite.
Primaquine has historically been used as a terminal prophylactic agent to eradicatehepatic hypnozoite stages of P. vivax and P. ovale (the latent hepatic forms can result in relapses months or even years after primary infection). When used as a terminal prophylactic agent, this drug should be taken daily for two weeks after the person leaves amalarious area.
Daily primaquine (at 0.5mg/kg of base per day [up to 30mg]) may also be used as a primary causal prophylactic agent (136–139). When taken as a causal prophylactic,the drug should be taken one to two days before the person enters a malarious area and continued daily until two to seven days after the individual leaves the malarious area.
Primaquine may cause methemoglobinemia and oxidant-induced hemolytic anemia,especially in individuals with glucose-6 phosphate dehydrogenase deficiency (118). Thisagent should not be used in pregnant women. Even after one year of daily use, primaquineis well tolerated; the most frequently reported side effect is gastrointestinal upset, whichcan be ameliorated by taking the medication with food (108,118,136).
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 93
Tafenoquine
Tafenoquine (WR238605) is an 8-aminoquinoline agent related to primaquine(108,140,141). It has potent activity against both liver and blood asexual stages and sexual(gametocyte) stages of the malaria parasite. Tafenoquine appears to be better tolerated thanprimaquine (140). Whereas primaquine requires daily dosing, tafenoquine may be effec-tive when taken as a single loading dose before a short trip or when taken weekly duringtravel. Its role in the prevention and therapy of malaria is currently being evaluated. As isthe case with primaquine, its use is contraindicated in individuals with glucose 6-phosphatedehydrogenase deficiency and in pregnant women.
Chloroquine and Proguanil
The combination of daily proguanil with weekly chloroquine is more effective at prevent-ing malaria in sub-Saharan Africa than is weekly chloroquine alone. Unfortunately, theprotective efficacy of the chloroquine–proguanil combination is poor: it is 50% to 70%effective as compared with doxycycline or mefloquine (1,5,111,118,142). The combina-tion of daily and weekly medications can also result in increased confusion and decreasedcompliance.
Proguanil is usually well tolerated, although oral ulcerations, pancytopenia, thrombocy-topenia, and granulocytopenia have been associated with its use. This drug is not availableas a single agent in the United States.
Azithromycin
Azithromycin is a macrolide antibiotic related to erythromycin. It shows some activityagainst plasmodia species, but its protective efficacy against P. falciparum infection is low(approximately 70% to 83%, even among partially immune adults). In addition, dailyadministration is required, and the agent is not causally prophylactic (1,143). No field trialhas as yet examined the efficacy of azithromycin in preventing malaria in nonimmuneadults. Although it is well tolerated, azithromycin is much more expensive than other, moreeffective agents. It should not be used as an agent to prevent malaria (135).
Prevention of Malaria in Pregnant Women and Children
Pregnant women and children are at increased risk of suffering severe adverse events frommalaria. As a consequence, steps should be taken to prevent malaria in these individuals,including the appropriate use of DEET-containing insect repellents and permethrin-impregnated bednets and clothing (1,95–99).
Chloroquine can be safely administered to all pregnant women (that is, during alltrimesters of pregnancy) and children. Doxycyline, primaquine, and tafenoquine shouldnever be used during pregnancy, and doxycycline should not be used in children youngerthan 8 years of age. Proguanil has been employed safely during pregnancy and in smallchildren. Note, however, that the combination of chloroquine and proguanil is not as effective as mefloquine. Atovaquone’s (and therefore atovaquone-proguanil’s) safety in pregnancy has not been established. Atovaquone-proguanil is, however, approved for usein children weighing more than 10kg, and a pedatric tablet is available.
The CDC has recommended the use of mefloquine in children of all ages and allweights who are deemed at high risk of acquiring chloroquine-resistant P. falciparum infec-
94 Current Clinical Topics in Infectious Diseases
tion (32). (Atovaquone-proguanil may also be used in children weighing more than 10kg.)No human study has linked prophylactic use of mefloquine during pregnancy with teratogenicity or congenital malformations in newborns (105,144–147). When mefloquineis administered as a prophylactic agent during the second and third trimesters of pregnancy,its use has not been associated with any significant adverse events in either the mother orthe fetus (106,110,147). Some studies, however, have found an increased rate of mis-carriage when mefloquine is used during the first trimester (145). Other studies have found no increased risk compared to background rates and compared to rates in womentaking chloroquine, chloroquine–proguanil, or sulfadoxine-pyrimethamine (110,144,148).Prophylactic use of mefloquine during pregnancy is, therefore, probably safe, especiallyduring the second and third trimesters. Limited data also suggest that it is safe when usedfor prophylaxis during the first trimester (32).
At present, no safe and effective chemophophylactic agent is available for childrenyounger than 8 years of age and pregnant women traveling to mefloquine-resistant areas ofthe world (109). The combination of atovaquone and proguanil may be used in such indi-viduals, but the safety of this combination in young children and pregnant women remainsto be established.
TREATMENT
Table 4.4 lists the currently available options for treatment of malaria. In many areas of theworld, individuals with malaria are treated as outpatients, often with an antipyretic agentand an inexpensive antimalarial agent such as chloroquine or sulfadoxine-pyrimethamine.Hospitalization and parenteral administration of antimalarial agents are usually reservedfor individuals with severe or complicated malaria—that is, malaria associated withimpaired consciousness, coma, seizures, renal failure, pulmonary edema, shock, severe acidosis, severe jaundice, hypoglycemia, and/or parasitemia levels greater than 5% to 15%(2,149,150) In industrialized countries, individuals with malaria, especially those with P. falciparum malaria, are usually treated as inpatients.
In North America, the most common errors in the management of individuals withmalaria relate to the following:
• Failure to consider the diagnosis.
• Inappropriate choice of drug or route of administration.
• Misjudgment of the severity of infection.
• Failure to recognize and treat the complications of severe malaria (including severe hypoglycemia).
• Inappropriate management of fluid and electrolyte status.
• Failure to monitor clearance of parasitemia (11).
Treatment of Chloroquine-Sensitive Malaria
Chloroquine Oral chloroquine phosphate is the therapeutic agent of choice for individ-uals with uncomplicated infection with P. ovale, P. malariae, chloroquine-sensitive P. vivax,or chloroquine-sensitive P. falciparum. If chloroquine is not available, hydroxychloro-quine sulfate may be used. Blood smears and clinical parameters should be followed, and
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 95
Tabl
e 4.4
Trea
tmen
t of
mal
aria
*
Med
icat
ion
Adult
Dose
Ped
iatr
ic D
ose
OR
AL
TH
ER
AP
Y†
Chl
oroq
uine
-sens
itive
plas
mod
ia‡
Chl
oroq
uine
pho
spha
te§
600
mg
base
(1
g sa
lt), t
hen
300
mg
base
(50
0m
g sa
lt) 6
h 10
mg
base
/kg
(up
to a
dult
dose
), th
en
late
r, th
en 3
00m
g ba
se (
500
mg
salt)
at 2
4 an
d 48
h5
mg
base
/kg
6h
late
r, th
en5
mg
base
/kg
at 2
4 an
d 48
h
Chl
oroq
uine
-resi
stan
tP. f
alci
paru
m‡¶
Atov
aquo
ne-p
rogu
anil
(Mal
aron
e)||
4 ta
blet
s (2
50m
g-at
ovaq
uone
/100
mg-
prog
uani
l) 11
–20
kg =
250
mg/
100
mg
daily
¥3
day
21–3
0kg
=50
0m
g/20
0m
g31
–40
kg =
750
mg/
300
mg
>40
kg =
1g/
400
mg,
daily
¥3
day
OR
Qui
nine
sul
fate
650
mg
q8h
¥3–
7 da
y**
25m
g/kg
/day
(up
to d
aily
adu
lt do
se)
in 3
do
ses
¥3–
7 da
y**
PL
US
Dox
ycyc
line††
100
mg
bid
¥7
day
2m
g/kg
/day
(up
to d
aily
adu
lt do
se)
¥7
day
OR
PL
US
tetra
cycl
ine††
250
mg
qid
¥7
day
6.25
mg/
kg (
up to
adu
lt do
se)
qid
¥7
day
OR
PL
US
Sulfa
doxi
ne-p
yrim
etha
min
e‡‡3
tabl
ets
at o
nce
on la
st da
y of
qui
nine
<1yr
: 1 / 4ta
blet
(Fan
sidar
)1–
3yr
: 1 / 2ta
blet
4–8
yr: 1
tab
let
9–14
yr: 2
tab
lets
≥15
yr: 3
tab
lets,
as
for
adul
ts
OR
PL
US
clin
dam
ycin
§§90
0m
g tid
¥5
day
20–4
0m
g/kg
/day
(up
to d
aily
adu
lt do
se)
in
3 do
ses
¥5
day
96
Alte
rnat
ives
Mefl
oqui
ne¶¶
750
mg
once
follo
wed
by
500
mg
12h
late
r15
mg/
kg o
nce
follo
wed
by
10m
g/kg
8–1
2h
late
r (£
45kg
)H
alof
antri
ne**
*||||
500
mg
q6h
¥3
dose
s; re
peat
in 1
wee
k†††
8m
g/kg
(up
to a
dult
dose
) q6
h ¥
3 do
ses
(<40
kg);
repe
at in
1 w
eek††
†
Atov
aquo
ne‡‡
‡50
0m
g bi
d ¥
3 da
y11
–20
kg: 1
25m
g bi
d ¥
3 da
y21
–30
kg: 2
50m
g bi
d ¥
3 da
y31
–40
kg: 3
75m
g bi
d ¥
3 da
y≥4
1kg
: adu
lt do
se
PL
US
prog
uani
l***
‡‡‡
200
mg
bid
¥3
day
11–2
0kg
: 50
mg
bid
¥3
day
21–3
0kg
: 100
mg
bid
¥3
day
31–4
0kg
: 150
mg
bid
¥3
day
≥41
kg: a
dult
dose
OR
PL
US
doxy
cycl
ine††
100
mg
bid
¥3
day
2m
g/kg
/d (
up to
dai
ly a
dult
dose
) ¥
3 da
y
Arte
suna
te**
*4
mg/
kg/d
¥3
day
PL
US
mefl
oqui
ne¶¶
750
mg
once
follo
wed
by
500
mg
12h
late
r15
mg/
kg o
nce
follo
wed
by
10m
g/kg
8–1
2h
late
r (£
45kg
)
Chl
oroq
uine
-resi
stan
tP. v
ivax
‡§§§
Qui
nine
sul
fate
650
mg
q8h
¥3–
7 da
y**
25m
g/kg
/day
(up
to d
aily
adu
lt do
se)
in 3
do
ses
¥3–
7 da
y**
PL
US
doxy
cycl
ine††
100
mg
bid
¥7
day
2m
g/kg
/day
(up
to d
aily
adu
lt do
se) ¥
7 da
y
OR
PL
US
Sulfa
doxi
ne-p
yrim
etha
min
e‡‡3
tabl
ets
at o
nce
on la
st da
y of
qui
nine
<1yr
: 1 / 4ta
blet
(Fan
sidar
)1–
3yr
: 1 / 2ta
blet
4–8
yr: 1
tab
let
9–14
yr: 2
tab
lets
≥15
yr: 3
tab
lets,
as
for
adul
tsM
efloq
uine
¶¶75
0m
g on
ce fo
llow
ed b
y 50
0m
g 12
h la
ter
15m
g/kg
onc
e fo
llow
ed b
y 10
mg/
kg 8
–12
hla
ter
(£45
kg)
97
Tabl
e 4.4
Con
tinu
ed
Med
icat
ion
Adult
Dose
Ped
iatr
ic D
ose
Alte
rnat
ives
Hal
ofan
trine
***||
||50
0m
g q6
h ¥
3 do
ses
8m
g/kg
(up
to a
dult
dose
) q6
h ¥
3 do
ses
Chl
oroq
uine
25m
g ba
se/k
g in
3 d
oses
ove
r 48
h
PL
US
prim
aqui
ne¶¶
¶2.
5m
g ba
se/k
g in
3 d
oses
ove
r 48
h
PAR
EN
TE
RA
L T
HE
RA
PY:
AL
L P
LA
SMO
DIA
†
Qui
nidi
ne g
luco
nate
||||
||10
mg/
kg lo
adin
g do
se (
max
. 600
mg)
IV
in n
orm
al s
alin
e Sa
me
as a
dult
dose
slow
ly o
ver
1 to
2h,
follo
wed
by
cont
inuo
us in
fusio
n of
0.02
mg/
kg/m
in u
ntil
oral
ther
apy
can
be s
tarte
d
OR
Qui
nine
dih
ydro
chlo
ride||
||||
20m
g/kg
load
ing
dose
IV
in 5
% d
extro
se o
ver
4h,
Sa
me
as a
dult
dose
follo
wed
by
10m
g/kg
ove
r 2–
4h
q8h
(max
. 180
0m
g/da
y)un
til o
ral t
hera
py c
an b
e st
arte
d
Alte
rnat
ives
Arte
met
her*
**3.
2m
g/kg
IM
, the
n 1.
6m
g/kg
IM
dai
ly ¥
5–7
day
Sam
e as
adu
lt do
se
PR
EV
EN
TIO
N O
F R
EL
AP
SES
(P. V
IVA
XA
ND
P.
OVA
LE
ON
LY)
Prim
aqui
ne p
hosp
hate
****
¶¶¶
15m
g ba
se (
26.3
mg
salt)
onc
e/da
y ¥
14 d
ay o
r 45
mg
0.3
mg
base
/kg
(up
to a
dult
dose
) on
ce/d
ay
base
(79
mg
salt)
onc
e/w
k ¥
8w
k¥
14 d
ay
*Pr
esum
ptiv
e se
lf-tre
atm
ent o
f mal
aria
is n
ot r
outin
ely
reco
mm
ende
d; in
divi
dual
s w
ith fe
ver
at r
isk o
f mal
aria
sho
uld
seek
med
ical
atte
ntio
n.†Pa
rent
eral
the
rapy
sho
uld
be u
sed
to t
reat
ind
ivid
uals
who
are
una
ble
to t
ake
oral
med
icat
ions
and
tho
se w
ith s
ever
e or
com
plic
ated
mal
aria
(i.e
., m
alar
ia a
ssoc
iate
d w
ithim
paire
d co
nsci
ousn
ess,
com
a, se
izur
es, r
enal
failu
re, p
ulm
onar
y ed
ema,
shoc
k, se
vere
aci
dosis
, sev
ere
jaun
dice
, hyp
ogly
cem
ia, a
nd/o
r par
asite
mia
leve
ls gr
eate
r tha
n 5–
15%
).E
xcha
nge
trans
fusio
n ha
s be
en h
elpf
ul fo
r so
me
patie
nts
with
hig
h-de
nsity
(>1
0%)
para
sitem
ia, a
ltere
d m
enta
l sta
tus,
pulm
onar
y ed
ema,
or
rena
l com
plic
atio
ns.
‡C
hlor
oqui
ne-re
sista
nt P
. fal
cipa
rum
has b
een
repo
rted
in a
ll m
alar
ious
are
as e
xcep
t Mex
ico,
Cen
tral A
mer
ica
wes
t of t
he P
anam
a C
anal
, Hai
ti, th
e D
omin
ican
Rep
ublic
, and
scat
tere
d ar
eas
of th
e M
iddl
e E
ast.
Chl
oroq
uine
-resis
tant
P. v
ivax
has
been
rep
orte
d in
are
as o
f Oce
ania
incl
udin
g In
done
sia, P
apua
–New
Gui
nea,
Van
uatu
, and
the
Solo
mon
Isla
nds,
as w
ell a
s In
dia,
Tha
iland
, Mya
nmar
, and
are
as in
Sou
th A
mer
ica,
incl
udin
g B
razi
l, G
uyan
a, a
nd P
eru.
§If
chlo
roqu
ine
phos
phat
e is
not
avai
labl
e, h
ydro
xych
loro
quin
e su
lfate
is
equa
lly e
ffect
ive;
400
mg
of h
ydro
xych
loro
quin
e su
lfate
sal
t is
equi
vale
nt t
o 50
0m
g of
chl
oroq
uine
phos
phat
e sa
lt.¶Ad
ditio
nal a
ltern
ativ
es b
eing
act
ivel
y stu
died
for
treat
men
t of i
ndiv
idua
ls w
ith u
ncom
plic
ated
mal
aria
cau
sed
by c
hlor
oqui
ne-re
sista
nt P
. fal
cipa
rum
incl
ude
arte
met
her
plus
benfl
umet
ol (l
umef
antri
ne) (
a co
mbi
natio
n is
avai
labl
e as
CG
P 56
697:
co-
arte
met
her)
, pyr
onar
idin
e, c
hlor
prog
uani
l plu
s dap
sone
, and
chl
oroq
uine
plu
s chl
orph
enira
nine
(see
text
). M
ultid
rug-
resis
tant
P. f
alci
paru
m(in
clud
ing
resis
tanc
e to
mefl
oqui
ne a
nd h
alof
antri
ne) h
as b
een
repo
rted
in S
outh
east
Asia
, esp
ecia
lly T
haila
nd. A
7-d
ay c
ours
e of
qui
nine
98
and
tetra
cycl
ine
or d
oxyc
yclin
e ca
n be
use
d to
tre
at i
ndiv
idua
ls w
ith P
. fal
cipa
rum
acqu
ired
in t
hese
are
as. A
tova
quon
e pl
us p
rogu
anil
also
app
ears
to
be p
rom
ising
in
early
trial
s. Ar
tesu
nate
plu
s m
efloq
uine
, ar
tem
ethe
r pl
us m
efloq
uine
, an
d m
efloq
uine
plu
s te
tracy
clin
e or
dox
ycyc
line,
hav
e al
so b
een
used
to
treat
ind
ivid
uals
infe
cted
with
m
ultid
rug-
resis
tant
P. f
alci
paru
m.
||Fi
xed
com
bina
tion
tabl
ets
of 2
50m
g at
ovaq
uone
/100
mg
prog
uani
l an
d 62
.5m
g at
ovaq
uone
/25
mg
prog
uani
l ar
e av
aila
ble
in t
he U
nite
d St
ates
. T
he c
ombi
natio
n sh
ould
be
use
d on
ly i
n th
e tre
atm
ent
of i
ndiv
idua
ls w
ith a
cute
non
-seve
re u
ncom
plic
ated
mal
aria
cau
sed
by P
. fa
lcip
arum
. D
ue t
o hi
gh e
ffica
cy a
nd a
low
er s
ide
effe
ct p
rofil
e,
atov
aquo
ne/p
rogu
anil
may
hav
e ce
rtai
n ad
vant
ages
ove
r tra
ditio
nal
quin
ine-
base
d th
erap
y in
the
tre
atm
ent
of s
uch
indi
vidu
als.
At p
rese
nt, a
tova
quon
e/pr
ogua
nil
shou
ld n
ot
be u
sed
in th
e tre
atm
ent o
f ind
ivid
uals
with
sev
ere
or c
ompl
icat
ed m
alar
ia c
ause
d by
P. f
alci
paru
m(m
alar
ia a
ssoc
iate
d w
th im
paire
d co
nsci
ousn
ess,
com
a, s
eizu
res,
rena
l fai
l-ur
e, p
ulm
onar
y ed
ema,
sho
ck, s
ever
e ac
idos
is, s
ever
e ja
undi
ce, h
ypog
lyce
mia
, and
/or
para
sitem
ia le
vels
grea
ter
than
5–1
5%).
Atov
aquo
ne-p
rogu
anil
shou
ld a
lso n
ot b
e us
ed
in th
e tre
atm
ent o
f pre
gnan
t wom
en w
ith m
alar
ia u
nles
s ot
her
agen
ts ar
e un
avai
labl
e. A
tova
quon
e-pr
ogua
nil s
houl
d be
tak
en w
ith fo
od. T
he m
ost c
omm
on s
ide
effe
cts
are
naus
ea, v
omiti
ng, a
nd a
bdom
inal
disc
omfo
rt. A
lthou
gh a
ppro
ved
for
once
dai
ly d
osin
g, to
dec
reas
e na
usea
and
vom
iting
, the
dos
e m
ay b
e di
vide
d in
two
afte
r th
e fir
st da
y of
ther
apy.
**D
ue to
incr
easin
g to
lera
nce
to q
uini
ne in
Sou
thea
st As
ia, i
ndiv
idua
ls w
ith m
alar
ia a
cqui
red
in th
is ar
ea s
houl
d be
trea
ted
for
7 da
ys if
qui
nine
is u
sed.
Qui
nine
is u
sual
lypo
orly
tole
rate
d. I
ts us
e is
asso
ciat
ed w
ith d
izzi
ness
, tin
nitu
s, de
afne
ss, a
nd n
ause
a. I
t may
cau
se h
ypog
lyce
mia
and
car
diac
arr
ythm
ias.
††D
o no
t use
in p
regn
ant w
omen
and
chi
ldre
n yo
unge
r th
an 8
yea
rs o
f age
.‡‡
Fixe
d co
mbi
natio
nFa
nsid
ar t
able
ts co
ntai
n 50
0m
g of
sul
fado
xine
and
25
mg
of p
yrim
etha
min
e. S
ulfa
doxi
ne-p
yrim
etha
min
e re
sista
nce
has
been
rep
orte
d in
Oce
ania
, sub
-Sa
hara
n Af
rica,
Sou
th a
nd S
outh
east
Asia
, and
the
Amaz
on b
asin
.§§
Safe
to u
se in
pre
gnan
t wom
en a
nd c
hild
ren.
¶¶At
this
dosa
ge, a
dver
se e
ffect
s, in
clud
ing
naus
ea, v
omiti
ng, d
iarr
hea,
diz
zine
ss, d
istur
bed
sens
e of
bal
ance
, tox
ic p
sych
osis,
and
sei
zure
s, ca
n oc
cur.
Cur
rent
ly, m
efloq
uine
isno
t rec
omm
ende
d fo
r us
e as
a tr
eatm
ent f
or p
regn
ant w
omen
with
mal
aria
. It s
houl
d no
t be
give
n to
geth
er w
ith q
uini
ne, q
uini
dine
, or
halo
fant
rine,
and
cau
tion
is re
quire
din
usin
g qu
inin
e, q
uini
dine
, or
halo
fant
rine
to tr
eat p
atie
nts
with
mal
aria
who
hav
e ta
ken
mefl
oqui
ne fo
r pr
ophy
laxi
s. T
he p
edia
tric
dosa
ge h
as n
ot b
een
appr
oved
by
the
U.S
.Fo
od a
nd D
rug
Adm
inist
ratio
n. R
esist
ance
to
mefl
oqui
ne h
as b
een
repo
rted
in s
ome
area
s, su
ch a
s th
e w
este
rn p
rovi
nces
of
Cam
bodi
a, t
he e
aste
rn p
rovi
nces
of
Mya
nmar
(Bur
ma)
, and
the
Tha
iland
–Mya
nmar
and
Tha
iland
–Cam
bodi
a bo
rder
s an
d in
the
Amaz
on b
asin
. Whe
n tre
atin
g in
divi
dual
s w
ith m
alar
ia a
cqui
red
in th
ese
area
s, 25
mg/
kgsh
ould
be
used
. In
the
Uni
ted
Stat
es, a
250
-mg
tabl
et o
f mefl
oqui
ne c
onta
ins
228
mg
mefl
oqui
ne b
ase.
Out
side
the
Uni
ted
Stat
es, e
ach
275-
mg
tabl
et c
onta
ins
250
mg
base
.||
||M
ay b
e ef
fect
ive
in tr
eatin
g in
divi
dual
s with
mul
tidru
g-re
sista
nt P
. fal
cipa
rum
mal
aria
. Tre
atm
ent f
ailu
res a
nd re
sista
nce
have
bee
n re
porte
d, h
owev
er, a
nd th
e dr
ug h
as c
ause
dle
ngth
enin
g of
the
PR a
nd Q
Tc
inte
rval
s an
d fa
tal c
ardi
ac a
rrhy
thm
ias.
It sh
ould
not
be
used
for
patie
nts
with
car
diac
con
duct
ion
defe
cts
or in
con
junc
tion
with
oth
er d
rugs
that
may
affe
ct th
e Q
T in
terv
al, s
uch
as q
uini
ne, q
uini
dine
, and
mefl
oqui
ne. C
ardi
ac m
onito
ring
is re
com
men
ded.
Var
iabi
lity
in a
bsor
ptio
n is
a pr
oble
m; h
alof
antri
ne s
houl
dno
t be
take
n on
e ho
ur b
efor
e to
two
hour
s af
ter
mea
ls, b
ecau
se fo
od in
crea
ses
its a
bsor
ptio
n. I
t sho
uld
not b
e us
ed in
pre
gnan
cy.
***
Not
com
mer
cial
ly a
vaila
ble
in th
e U
nite
d St
ates
.††
†A
singl
e 25
0-m
g do
se (
<40
kg: 8
mg/
kg; u
p to
250
mg)
can
be
used
for
repe
at tr
eatm
ent i
n m
ild to
mod
erat
e in
fect
ion.
‡‡‡Fi
xed
com
bina
tion
tabl
ets
of 2
50m
g at
ovaq
uone
/100
mg
prog
uani
l and
62.
5m
g at
ovaq
uone
/25
mg
prog
uani
l are
ava
ilabl
e in
the
Uni
ted
Stat
es. (
See
abov
e.)
The
com
bina
-tio
n sh
ould
be
used
onl
y fo
r ac
ute
unco
mpl
icat
ed m
alar
ia c
ause
d by
P. f
alci
paru
m. T
ake
with
mea
ls.§§
§At
ovaq
uone
/pro
guan
il m
ay b
e ef
fect
ive
in c
lear
ing
the
eryt
hroc
ytic
pha
se o
f ch
loro
quin
e-re
sista
nt P
. viv
ax; h
owev
er, r
ecru
desc
ence
s ar
e co
mm
on a
nd t
erm
inal
tre
atm
ent
with
prim
aqui
ne is
req
uire
d (s
ee b
elow
).¶¶
¶Ta
ke w
ith fo
od. D
o no
t use
in p
regn
ant w
omen
and
indi
vidu
als
defic
ient
in g
luco
se 6
-pho
spha
te d
ehyd
roge
nase
.||
||||C
ontin
uous
ele
ctro
card
iogr
aphi
c, b
lood
pre
ssur
e, a
nd g
luco
se m
onito
ring
are
reco
mm
ende
d, e
spec
ially
in p
regn
ant w
omen
and
you
ng c
hild
ren.
Qui
nidi
ne m
ay h
ave
grea
ter
antim
alar
ial a
ctiv
ity th
an q
uini
ne. T
he lo
adin
g do
se s
houl
d be
dec
reas
ed o
r om
itted
in th
ose
patie
nts
who
hav
e re
ceiv
ed q
uini
ne o
r m
efloq
uine
. If m
ore
than
48
hour
s of
par
-en
tera
l tre
atm
ent i
s re
quire
d, th
e qu
inin
e or
qui
nidi
ne d
ose
shou
ld b
e re
duce
d by
one
-third
to o
ne-h
alf.
****
Rel
apse
s hav
e be
en re
porte
d w
ith th
is re
gim
en, a
nd su
ch c
ases
shou
ld b
e tre
ated
with
a se
cond
14-
day
cour
se o
f 30
mg
base
/day
(in
child
ren,
0.5
mg
base
/kg/
day)
. Rep
eat
cour
ses
may
be
nece
ssar
y. S
train
s of
P. v
ivax
“tol
eran
t” o
r “r
esist
ant”
to p
rimaq
uine
hav
e be
en r
epor
ted
in a
reas
of S
outh
east
Asia
and
Eas
t Afri
ca, i
nclu
ding
Som
alia
. Ind
ivid
-ua
ls w
ith P
. viv
axin
fect
ion
acqu
ired
in th
ese
area
s m
ay b
e tre
ated
for
14 d
ays
with
30
mg
base
/day
(in
chi
ldre
n, 0
.5m
g ba
se/k
g/da
y).
so
urc
e:
Adap
ted
in p
art f
rom
dat
a pu
blish
ed in
Dru
gs fo
r Pa
rasit
ic I
nfec
tions
. Han
dboo
k of
Ant
i-mic
robi
al T
hera
py. N
ew R
oche
lle, N
Y: T
he M
edic
al L
ette
r, 20
00:1
04–1
26.
ww
w.m
edle
tter.c
om.
99
clearance of infection should be documented to exclude recrudescence of chloroquine-resistant organisms, especially chloroquine-resistant P. falciparum or P. vivax (31).
Treatment of Chloroquine-Resistant Malaria
Quinine Sulfate and a Second Agent Quinine sulfate has historically been the agent ofchoice for treating individuals with uncomplicated malaria caused by chloroquine-resistantP. falciparum or chloroquine-resistant P. vivax (31). This drug is, unfortunately, usuallypoorly tolerated, with patients reporting dizziness, tinnitus, deafness, and nausea. Quininesulfate should be administered with a second agent, such as doxycycline or tetracycline in a nonpregnant adult, or clindamycin in pregnant women and children younger than 8 years of age (31,151–155). In some areas of the world, quinine sulfate is used with a one-time dose of sulfadoxine-pyrimethamine, although resistance to sulfadoxine-pyrimethamine limits the utility of this regimen (31). Increasing resistance to quinine hasbeen reported in many areas, including Southeast Asia, South America, and Africa(24,106,156,157).
Atovaquone and Proguanil The combination of atovaquone and proguanil is highlyeffective in the treatment of individuals with uncomplicated P. falciparum infection(158–163). In many areas of the world, combination atovaquone-proguanil is replacingquinine plus a second agent as the treatment of choice for individuals with uncomplicatedmalaria caused by P. falciparum (including chloroquine-resistant and multi-drug resistantstrains). At therapeutic dosages, both agents are very well tolerated; the most frequentlyreported adverse events include mild abdominal discomfort with nausea, vomiting, diar-rhea, and mild elevations in hepatic transaminases (160). Although the atovaquone–proguanil combination has not been extensively studied as a treatment for individuals withmalaria caused by species other than P. falciparum, it has been uniformly effective in thesmall number of patients with P. ovale, P. vivax, and P. malariae infections in whom it hasbeen used (134). When used to treat individuals with P. vivax or P. ovale infection, a sub-sequent course of primaquine must be administered to prevent late relapse (124,158).
Atovaquone and Doxycycline A three-day course of oral atovaquone and doxycycline isalso safe and effective in the treatment of individuals with uncomplicated malaria causedby chloroquine-resistant P. falciparum (122,164). This combination should not be used inpregnant women and children younger than 8 years of age.
Mefloquine Mefloquine became a drug of choice for the treatment of uncomplicatedmultidrug-resistant P. falciparum malaria in Southeast Asia in the 1980s (165). No par-enteral formulation is available. Unfortunately, resistance has since appeared in SoutheastAsia, especially in the border areas between Thailand and Cambodia and between Thai-land and Myanmar (24,32). If mefloquine is used to treat individuals with malaria acquiredin these areas, it should be used in combination with a second agent, usually an artemisininderivative, tetracycline, or doxycycline (166,167). The drug should not be given withquinine, quinidine, or halofantrine (31). When mefloquine is used to treat individuals withmalaria caused by chloroquine-resistant P. falciparum acquired along the border areas ofThailand or in the Amazon basin, a dosage of 25mg/kg body weight should be used (24,31).When used in therapeutic dosages, this agent can precipitate anxiety attacks and other
100 Current Clinical Topics in Infectious Diseases
neuropsychiatric adverse advents, including acute psychosis in as many as 1 in 250 to 1 in1700 individuals (24,108).
Halofantrine Halofantrine is a phenanthrene methanol compound that is metabolizedto its active form, desbutylhalofantrine, in vivo. This agent’s major use is in the treatmentof individuals with multidrug-resistant P. falciparum infection. No parenteral formulationis available (108). Intestinal absorption can be variable and increases when the patient takeshalofantrine with a fatty meal; because of its unpredictable absorption and toxicity, thisdrug should not be taken with food (31).
Halofantrine can prolong the PR and the corrected QT (QTc) intervals, resulting in ven-tricular arrhythmias (168). Due to a high incidence of cardiotoxicity, three-day regimensof this agent should not be employed. Even one-day regimens should not be administeredto individuals with cardiac conduction abnormalities, and halofantrine should not be usedto treat individuals taking other agents that affect the QT interval (such as mefloquine,quinidine, and quinine) (31).
Artemisinin Derivatives A number of artemisinin derivatives are in common use as anti-malarial agents worldwide, including artemether, artesunate, and dihydroartemisinin.Artemisinin derivatives are the most rapidly acting of all malaria therapies (149). Prepara-tions are available for oral, rectal (suppository), and parenteral administration. Unfortu-nately, all artemisinin derivatives can produce brain-stem damage in laboratory animals.The doses prescribed for humans are much lower than those causing toxicity in animals,however, and neuronal damage has not been observed in humans treated with these agents(108,169–172).
Artemisinin derivatives are most widely used for treating individuals infected with multidrug-resistant P. falciparum (173,174). Although clinical resistance to these drugs hasnot yet been described, reappearance of P. falciparum within 28 days of short (four- to five-day) courses of artemisinin derivatives limit the usefulness of these agents when used asmonotherapy (175). As a consequence, they are often administered with a longer-actingagent, such as mefloquine or benflumetol (lumefantrine) (108,175–180).
Co-artemether Co-artemether (CGP 56697) is a 1 :6 combination of short-actingartemether and long-acting benflumetol (lumefantrine). Lumefantrine is an arylaminoalcohol schizonticide that bears certain structural similarities to quinine, mefloquine, andhalofantrine; it appears to be less cardiotoxic than the latter agents (108,181,182).
Co-artemether is available in an oral preparation that is well tolerated (183). Absorptionis variable, but increases with fatty foods (184,185). Co-artemether is effective in the treat-ment of individuals with uncomplicated chloroquine-resistant P. falciparum infection,although recrudescences occur when short-course therapy is used. To overcome thisproblem, a six-dose regimen (doses at 0, 8, 24, 48, 72, and 96 hours) is recommended(175,181,186,187).
Pyronaridine Pyronaridine is a benzonaphthyridine derivative that has been used inChina for more than 20 years to treat individuals with malaria caused by P. falciparum orP. vivax. It is also being evaluated in the treatment of individuals infected with P. ovaleor P. malariae (188). Pyronaridine is available in oral and parenteral formulations, is welltolerated, and is more effective than chloroquine in the treatment of partially immune individuals with uncomplicated malaria (189–191). Unfortunately, recrudescence rates as
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 101
high as 12% have been seen with pyronaridine monotherapy, especially in areas of South-east Asia. In addition, increasing resistance is being recognized in areas of the world wherethis agent has been widely used (192). A combination therapy consisting of pyronaridineand sulfadoxine-pyrimethamine is now being evaluated (193).
Chlorproguanil and Dapsone Chlorproguanil is converted in vivo to chlorcycloguanil,and the combination of chlorproguanil–dapsone potently inhibits folate synthesis (108).This combination therapy is just as effective as treatment for individuals with uncompli-cated P. falciparum infection as is sulfadoxine-pyrimethamine, and it is more effective thanchloroquine in areas characterized by chloroquine-resistant malaria (194–197). Somestrains of P. falciparum that are resistant to sulfadoxine-pyrimethamine are nevertheless susceptible to chlorproguanil–dapsone (108,198). Unfortunately, strains that are resistantto both chlorproguanil–dapsone and sulfadoxine-pyrimethamine have been identified inSoutheast Asia and are expected to spread (108).
The chlorproguanil–dapsone combination is administered orally and is well tolerated.At present, it is primarily used as an inexpensive agent for the treatment of uncomplicatedP. falciparum infection in areas of Africa where sulfadoxine-pyrimethamine is no longereffective.
Chloroquine and Chlorpheniramine Chlorpheniramine is a histamine H1 receptorantagonist. Simultaneous administration of chlorpheniramine and chloroquine increaseswhole-blood chloroquine concentrations in vivo (through an unclear mechanism), result-ing in a limited “reversal” of chloroquine resistance (108,199). In field studies in WestAfrica, the chloroquine–chlorpheniramine combination appeared to be more effective thaneither chloroquine alone or sulfadoxine-pyrimethamine in treating individuals with uncom-plicated P. falciparum malaria, but less effective than mefloquine (the protective efficacyof chloroquine–chlorpheniramine in this setting is 65% to 100%) (199–203). Whether thecombination offers similar effectiveness outside of West Africa remains unknown. The drugcombination is, however, well tolerated (202,203).
Treatment of Multidrug-Resistant P. falciparum
The optimal treatment for uncomplicated, multidrug-resistant P. falciparum infection(including resistance to chloroquine, mefloquine, sulfadoxine-pyrimethamine, and tolerance to quinine) has not yet been established. Atovaquone-proguanil combinationtherapy shows promise. Other currently used regimens include seven-day courses ofquinine with tetracycline or doxycycline; mefloquine–artesunate combination therapy;mefloquine–artemether combination therapy; and combination therapy with mefloquineand either tetracycline or doxycycline (31,163,166).
Treatment of Chloroquine-Resistant P. vivax
Although formal efficacy studies have not been performed, current therapy for chloroquine-resistant P. vivax infection resembles that for chloroquine-resistant P. falciparum infection.Quinine sulfate with a second agent such as doxycycline or sulfadoxine-pyrimethaminemay be administered (31). Individuals with chloroquine-resistant P. vivax have also beensuccessfully treated with therapeutic doses of mefloquine or halofantrine as well as com-bination therapy with chloroquine and primaquine (137). If combination atovaquone-proguanil is used, terminal treatment with primaquine is required.
102 Current Clinical Topics in Infectious Diseases
Parenteral Therapy for Severe/Complicated Malaria
Parenteral therapy should be used to treat individuals with severe or complicated malaria—that is, malaria associated with impaired consciousness, coma, seizures, renal failure, pul-monary edema, shock, severe acidosis, severe jaundice, hypoglycemia, and/or parasitemialevels greater than 5% to 15% (2,149,150). In addition, it is recommended for individualswith malaria who cannot take oral medications.
Quinidine Gluconate and Quinine Dihydrochloride In many areas of the world,quinine dihydrochloride is the parenteral agent of choice for treating individuals with severemalaria. In the United States, parenteral quinine is not available; quinidine gluconate isused instead. The latter agent is more active than quinine against malaria, but it is alsomore expensive and more cardiotoxic (204–207).
Quinine dihydrochloride may be administered intravenously or intramuscularly. Quini-dine gluconate, a class IA antiarrhythmic agent, should be administered intravenously. Bothintravenous quinidine and quinine should be delivered by continuous infusion; when theyare administered by rapid or bolus injection, they can induce fatal hypotension (31,149).
Individuals receiving parenteral quinidine should be monitored electrocardiographically.If the QTc interval increases more than 25% above the baseline reading, then the infusionrate should be reduced.
Intravenous therapy with quinine or quinidine should continue until the patient is ableto take oral medications. If parenteral therapy extends over more than two or three days, theintravenous dose should be reduced by 30% to 50% after 48 to 72 hours to avoid accumula-tion of drugs and increased toxicity (31,149). The intravenous administration of quinine orquinidine can induce hypoglycemia, which usually occurs 24 hours after treatment is initi-ated and most frequently affects pregnant women and small children (31,149,208).
Artemisinin Derivatives Parenteral artemether has also been used in the treatment ofindividuals with severe malaria. Clinicians originally hoped that the ability of these drugsto rapidly clear parasitemia would decrease mortality associated with severe malaria. Unfor-tunately, artemisinin derivatives do not appear to be more effective than quinine in thisrespect, although they do offer equivalent performance (149,209–211). Artemisinin deriv-atives can be given via rectal suppository if parenteral therapy is unavailable (212).
Prevention of Relapses
The liver hypnozoite stages of P. vivax and P. ovale can lead to relapses months or evenyears after the individual originally became infected. To prevent late relapses, patients withP. vivax or P. ovale infection should receive primaquine. This drug should not be used inpregnant women and in individuals deficient in glucose 6-phosphate dehydrogenase.Strains of P. vivax that are tolerant (or even resistant) to primaquine have been reported inareas of Southeast Asia and East Africa (including Somalia); larger doses of primaquineshould be used to treat individuals with such strains (213–215).
Treatment of Malaria During Pregnancy
Malaria during pregnancy represents a life-threatening infection for both mother and fetus.Therapy should therefore be directed toward eradicating infection. The susceptibility tomalaria is highest during the second and third trimesters of pregnancy and the early post-partum period (up to 60 days after delivery) (216).
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 103
Chloroquine is safe for use in this patient population. When appropriately administered,quinine or quinidine with clindamycin is also safe, although hypoglycemia and hypoten-sion can complicate the administration of parenteral quinine and quinidine during preg-nancy. Doxycycline, primaquine, and tafenoquine should not be used. Treatment withmefloquine of pregnant women with malaria may increase the risk of stillbirth; until furtherevaluations are performed, treatment-dose mefloquine should not be administered duringpregnancy unless other agents prove insufficient or are unavailable (217). Halofantrine istoxic to embryos in animal studies and should not be used during pregnancy (109).Although sulfadoxine-pyrimethamine is considered safe during all trimesters of pregnancy,sulfadoxine may cause kernicterus if given during the third trimester. Although artemisininderivatives have been used with apparent safety in the second and third trimesters of preg-nancy, they can cause resorption of embryos in animal studies; consequently, these agentsshould not be used during the first trimester (110,218). As yet, insufficient data have beengathered to prove or disprove the safety during pregnancy of artemether–benflumetol(lumefantrine), pyronaridine, chlorproguanil–dapsone, chloroquine–chlorpheniramine,and combination atovaquone-proguanil.
Ancillary Treatment
Few ancillary therapies have been shown to be effective in the treatment of individuals withmalaria (2,150). Antipyretics can lower fever, and intravenous administration of glucose-containing solution may lessen the incidence of hypoglycemia (149). Exchange trans-fusions can benefit individuals with severe or complicated malaria with parasitemia levelsexceeding 5% to 15% (219,220).
Steroids, heparin, and cyclosporin do not offer benefits in the treatment of individualswith malaria (149). Likewise, the administration of iron chelators (such as deferoxamine),antitumor necrosis factor agents (such as pentoxifylline), and agents that lower intracranialpressure (such as mannitol) has not been shown to help individuals with malaria (221–224).
Although prophylactic use of antiseizure medications such as phenobarbital does preventseizures in individuals with cerebral malaria, administration of such agents also doublesthe mortality rate due to respiratory arrests in such individuals. Consequently, individualswith malaria receiving prophylactic phenobarbital should be carefully monitored (225).
ACKNOWLEDGMENTS
Helpful information was provided by Dr. Kevin C. Kain. This work was supported by anInternational Collaborations in Infectious Disease Research Award from the National Institute of Child Health and Human Development (HD39165) as part of the Interna-tional Centers for Tropical Disease Research Network, National Institute of Allergy andInfectious Diseases, and by a grant from the National Institute of Allergy and InfectiousDiseases (AI/K081332).
REFERENCES
104 Current Clinical Topics in Infectious Diseases
1 Kain KC, Keystone JS. Malaria in travelers. Epi-demiology, disease, and prevention. Infect DisClin North Am 1998;12:267–284.
2 Warrell DA. Management of severe malaria.Parassitologia 1999;41:287–294.
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 105
3 Sina B. The multilateral initiative on malaria: anaction plan [news]. Parasitol Today 2000;16:139–140.
4 Adams JH, Wu Y, Fairfield A. Malaria Researchand Reference Reagent Resource Center [news].Parasitol Today 2000;16:89.
5 Steffen R, Fuchs E, Schildknecht J, et al.Mefloquine compared with other malariachemoprophylactic regimens in tourists visitingEast Africa [see comments]. Lancet 1993;341:1299–1303.
6 Hill DR, Behrens RH, Bradley DJ. The risk ofmalaria in travellers to Thailand. Trans R SocTrop Med Hyg 1996;90:680–681.
7 Ohrt C, Richie TL, Widjaja H, et al. Meflo-quine compared with doxycycline for the pro-phylaxis of malaria in Indonesian soldiers. Arandomized, double-blind, placebo-controlledtrial. Ann Intern Med 1997;126:963–972.
8 Handszuh H, Waters SR. Travel and tourismtrends. In: DuPont HL, Steffen R, eds. Textbookof travel medicine and health. Hamilton,Ontario: B.C. Decker, 1997:20–26.
9 Williams HA, Roberts J, Kachur SP, et al.Malaria surveillance—United States, 1995. MorMortal Wkly Rep CDC Surveill Summ 1999;48:1–23.
12 Greenberg AE, Lobel HO. Mortality from Plas-modium falciparum malaria in travelers from theUnited States, 1959 to 1987. Ann Intern Med1990;113:326–327.
13 Ridley RG. Planting the seeds of new antimalar-ial drugs [comment]. Science 1999;285:1502–1503.
14 Warhurst DC. A molecular marker for chloro-quine-resistant falciparum malaria. N Engl J Med2001;344:299–301.
15 Djimde A, Doumbo OK, Cortese JF, et al. Amolecular marker for chloroquine-resistant falci-parum malaria. N Engl Med 2001;344:257–263.
16 Gomez-Saladin E, Fryauff DJ, Taylor WR, et al.Plasmodium falciparum mdr1 mutations and invivo chloroquine resistance in Indonesia. Am JTrop Med Hyg 1999;61:240–244.
17 Wellems TE, Walker-Jonah A, Panton LJ.Genetic mapping of the chloroquine-resistancelocus on Plasmodium falciparum chromosome 7.Proc Natl Acad Sci USA 1991;88:3382–3386.
18 Basco LK, Ringwald P. Chloroquine resistancein Plasmodium falciparum and polymorphism of the cg2 gene. J Infect Dis 1999;180:1979–1986.
19 Durand R, Gabbett E, Di PJ, et al. Analysis ofkappa and omega repeats of the cg2 gene andchloroquine susceptibility in isolates of Plasmod-ium falciparum from sub-Saharan Africa. MolBiochem Parasitol 1999;101:185–197.
20 Basco LK, Ringwald P. Molecular epidemiologyof malaria in Yaounde, Cameroon. V. Analysis ofthe omega repetitive region of the Plasmodiumfalciparum cg2 gene and chloroquine resistance.Am J Trop Med Hyg 1999;61:807–813.
21 Adagu IS, Warhurst DC. Association of cg2 andpfmdr1 genotype with chloroquine resistance infield samples of Plasmodium falciparum fromNigeria. Parasitology 1999;119:343–348.
22 Milhous WK, Kyle DE. Introduction to themodes of action of and mechanisms of resis-tance to antimalarials. In: Sherman IW, ed.Malaria: parasite biology, pathogenesis, and pro-tection. Washington, DC: ASM Press, 1998:303–316.
23 Wilson CM, Serrano AE, Wasley A, et al.Amplification of a gene related to mammalianmdr genes in drug-resistant Plasmodium falci-parum. Science 1989;244:1184–1186.
24 White NJ. Drug resistance in malaria. Br MedBull 1998;54:703–715.
25 Urdaneta L, Plowe C, Goldman I, Lal AA. Pointmutations in dihydrofolate reductase and dihy-dropteroate synthase genes of Plasmodium falci-parum isolates from Venezuela. Am J Trop MedHyg 1999;61:457–462.
26 Diourte Y, Djimde A, Doumbo OK, et al.Pyrimethamine-sulfadoxine efficacy and selec-tion for mutations in Plasmodium falciparumdihydrofolate reductase and dihydropteroate synthase in Mali. Am J Trop Med Hyg 1999;60:475–478.
27 Wang P, Brobey RK, Horii T, et al. Utilizationof exogenous folate in the human malaria para-site Plasmodium falciparum and its critical role inantifolate drug synergy. Mol Microbiol 1999;32:1254–1262.
28 Durand R, Di PJ, Longuet C, et al. Increasedincidence of cycloguanil resistance in malariacases entering France from Africa, determined aspoint mutations in the parasites’ dihydrofolate-reductase genes. Ann Trop Med Parasitol 1999;93:25–30.
29 Wang P, Read M, Sims PF, Hyde JE. Sulfadox-ine resistance in the human malaria parasite Plas-modium falciparum is determined by mutationsin dihydropteroate synthetase and an additionalfactor associated with folate utilization. MolMicrobiol 1997;23:979–986.
30 Kamchonwongpaisan S, Meshnick SR. Themode of action of the antimalarial artemisininand its derivatives. Gen Pharmacol 1996;27:587–592.
31 Anonymous. Drugs for parasitic infections. In:Anonymous, ed. Handbook of antimicrobial
106 Current Clinical Topics in Infectious Diseases
therapy. New Rochelle, NY: The Medical Letter,2000:104–126. www.medletter.com.
32 Centers for Disease Control and Prevention.Health information for international travel1999–2000. Atlanta, GA: Department of Healthand Human Services, 1999.
33 Garg M, Gopinathan N, Bodhe P, KshirsagarNA. Vivax malaria resistant to chloroquine: casereports from Bombay. Trans R Soc Trop Med Hyg1995;89:656–657.
34 Fryauff DJ, Tuti S, Mardi A, et al. Chloroquine-resistant Plasmodium vivax in transmigration settlements of West Kalimantan, Indonesia. Am J Trop Med Hyg 1998;59:513–518.
35 Marlar T, Myat PK, Aye YS, et al. Developmentof resistance to chloroquine by Plasmodium vivaxin Myanmar. Trans R Soc Trop Med Hyg 1995;89:307–308.
36 Baird JK, Leksana B, Masbar S, et al. Diagno-sis of resistance to chloroquine by Plasmodiumvivax: timing of recurrence and whole bloodchloroquine levels. Am J Trop Med Hyg 1997;56:621–626.
37 Petruccelli BP, Murphy GS, Sanchez JL, et al. Treatment of traveler’s diarrhea withciprofloxacin and loperamide. J Infect Dis1992;165:557–560.
38 Whitby M. Drug resistant Plasmodium vivaxmalaria. J Antimicrob Chemother 1997;40:749–752.
39 Smoak BL, DeFraites RF, Magill AJ, et al. Plas-modium vivax infections in U.S. Army troops:failure of primaquine to prevent relapse in studiesfrom Somalia. Am J Trop Med Hyg 1997;56:231–234.
40 Collins WE, Jeffery GM. Primaquine resistancein Plasmodium vivax. Am J Trop Med Hyg1996;55:243–249.
41 Waller KL, Cooke BM, Nunomura W, et al.Mapping the binding domains involved in theinteraction between the Plasmodium falciparumknob-associated histidine-rich protein (KAHRP)and the cytoadherence ligand P. falciparum ery-throcyte membrane protein 1 (PfEMP1). J BiolChem 1999;274:23808–23813.
42 Wahlgren M, Barragan A, Chen Q, et al. Roset-ting of malaria-infected erythrocytes: ligands,host receptors, and the involvement of serum proteins. In: Sherman IW, ed. Malaria: parasitebiology, pathogenesis, and protection. Washing-ton, DC: ASM Press, 1998:387–398.
43 Howard RJ, Barnwell JW, Kao V. Antigenic variation of Plasmodium knowlesi malaria: identi-fication of the variant antigen on infected ery-throcytes. Proc Natl Acad Sci USA 1983;80:4129–4133.
44 Leech JH, Barnwell JW, Miller LH, Howard RJ.Identification of a strain-specific malarial antigenexposed on the surface of Plasmodium falci-parum-infected erythrocytes. J Exp Med 1984;159:1567–1575.
45 Su XZ, Heatwole VM, Wertheimer SP, et al.The large diverse gene family var encodes pro-teins involved in cytoadherence and antigenicvariation of Plasmodium falciparum-infected erythrocytes [see comments]. Cell 1995;82:89–100.
46 Baruch DI, Pasloske BL, Singh HB, et al.Cloning the P. falciparum gene encodingPfEMP1, a malarial variant antigen and adher-ence receptor on the surface of parasitizedhuman erythrocytes [see comments]. Cell 1995;82:77–87.
47 Borst P, Bitter W, McCulloch R, et al. Antigenicvariation in malaria [comment]. Cell 1995;82:1–4.
48 Moormann AM, Sullivan AD, Rochford RA, et al. Malaria and pregnancy: placental cytokineexpression and its relationship to intrauterinegrowth retardation. J Infect Dis 1999;180:1987–1993.
49 Chen Q, Fernandez V, Sundstrom A, et al.Developmental selection of var gene expressionin Plasmodium falciparum. Nature 1998;394:392–395.
50 Baruch DI, Gormely JA, Ma C, et al. Plas-modium falciparum erythrocyte membraneprotein 1 is a parasitized erythrocyte receptor foradherence to CD36, thrombospondin, and inter-cellular adhesion molecule 1. Proc Natl Acad SciUSA 1996;93:3497–3502.
51 Bull PC, Lowe BS, Kortok M, et al. Parasiteantigens on the infected red cell surface aretargets for naturally acquired immunity tomalaria. Nat Med 1998;4:358–360.
52 Reeder JC, Cowman AF, Davern KM, et al. Theadhesion of Plasmodium falciparum-infected ery-throcytes to chondroitin sulfate A is mediated byP. falciparum erythrocyte membrane protein 1.Proc Natl Acad Sci USA 1999;96:5198–5202.
53 Fried M, Duffy PE. Maternal malaria and para-site adhesion. J Mol Med 1998;76:162–171.
54 Baruch DI, Ma XC, Singh HB, et al. Identifi-cation of a region of PfEMP1 that mediatesadherence of Plasmodium falciparum infectederythrocytes to CD36: conserved function withvariant sequence. Blood 1997;90:3766–3775.
55 Newbold CI, Craig AG, Kyes S, et al. PfEMP1,polymorphism and pathogenesis. Ann Trop MedParasitol 1997;91:551–557.
56 Newbold C, Warn P, Black G, et al. Receptor-specific adhesion and clinical disease in Plas-modium falciparum [see comments]. Am J TropMed Hyg 1997;57:389–398.
57 Clark IA, Cowden WB. Why is the pathology of falciparum worse than that of vivax malaria?Parasitol Today 1999;15:458–461.
58 Pouvelle B, Buffet PA, Lepolard C, et al.Cytoadhesion of plasmodium falciparum ring-stage-infected erythrocytes. Nat Med 2000;6(11):1264–1268.
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 107
59 Bischoff E, Guillotte M, Mercereau-PuijalonO, Bonnefoy S. A member of the Plasmodiumfalciparum Pf60 multigene family codes for anuclear protein expressed by readthrough of aninternal stop codon. Mol Microbiol 2000;35:1005–1016.
60 Cheng Q, Cloonan N, Fischer K, et al. stevorand rif are Plasmodium falciparum multicopygene families which potentially encode variantantigens. Mol Biochem Parasitol 1998;97:161–176.
61 Wahlgren M, Fernandez V, Chen Q, et al.Waves of malarial variations. Cell 1999;96:603–606.
62 Barragan A, Kremsner PG, Weiss W, et al. Age-related buildup of humoral immunity against epi-topes for rosette formation and agglutination in African areas of malaria endemicity. InfectImmun 1998;66:4783–4787.
63 Bull PC, Lowe BS, Kortok M, Marsh K. Anti-body recognition of Plasmodium falciparum ery-throcyte surface antigens in Kenya: evidence for rare and prevalent variants. Infect Immun1999;67:733–739.
64 Giha HA, Staalsoe T, Dodoo D, et al. Nine-yearlongitudinal study of antibodies to variant anti-gens on the surface of Plasmodium falciparum-infected erythrocytes. Infect Immun 1999;67:4092–4098.
65 Urban BC, Ferguson DJ, Pain A, et al.Plasmodium falciparum-infected erythrocytesmodulate the maturation of dendritic cells [seecomments]. Nature 1999;400:73–77.
66 Gilbert SC, Plebanski M, Gupta S, et al. Asso-ciation of malaria parasite population structure,HLA, and immunological antagonism [see com-ments]. Science 1998;279:1173–1177.
67 Plebanski M, Lee EA, Hannan CM, et al.Altered peptide ligands narrow the repertoire of cellular immune responses by interfering withT-cell priming. Nat Med 1999;5:565–571.
68 Bruce MC, Donnelly CA, Alpers MP, et al.Cross-species interactions between malaria para-sites in humans. Science 2000;287:845–848.
69 Hanscheid T. Diagnosis of malaria: a review ofalternatives to conventional microscopy. ClinLab Haematol 1999;21:235–245.
70 Humar A, Ohrt C, Harrington MA, et al.ParaSight F test compared with the polymerasechain reaction and microscopy for the diagnosisof Plasmodium falciparum malaria in travelers.Am J Trop Med Hyg 1997;56:44–48.
71 Rickman LS, Long GW, Oberst R, et al. Rapiddiagnosis of malaria by acridine orange stainingof centrifuged parasites. Lancet 1989;1:68–71.
72 Rickman LS, Long GW, Hoffman SL. Rapiddiagnosis of malaria [letter]. Lancet 1989;1:1271.
73 Tanpradist S, Tharavanij S, Yamokgul P, et al.Comparison between microscopic examination,ELISA and quantitative buffy coat analysis in the
diagnosis of falciparum malaria in an endemicpopulation. Southeast Asian J Trop Med PublicHealth 1995;26:38–45.
74 Baird JK, Purnomo, Jones TR. Diagnosis ofmalaria in the field by fluorescence microscopyof QBC capillary tubes [see comments]. Trans RSoc Trop Med Hyg 1992;86:3–5.
75 Wang X, Zhu S, Liu Q, et al. Field evaluationof the QBC technique for rapid diagnosis of vivaxmalaria. Bull World Health Organ 1996;74:599–603.
76 Anthony RL, Bangs MJ, Anthony JM,Purnomo. On-site diagnosis of Plasmodium falci-parum, P. vivax, and P. malariae by using theQuantitative Buffy Coat system. J Parasitol1992;78:994–998.
77 Benito A, Roche J, Molina R, et al. Applicationand evaluation of QBC malaria diagnosis in aholoendemic area. Appl Parasitol 1994;35:266–272.
78 Lowe BS, Jeffa NK, New L, et al. Acridineorange fluorescence techniques as alternatives totraditional Giemsa staining for the diagnosis ofmalaria in developing countries [publishederratum appears in Trans R Soc Trop Med Hyg1996;90:102]. Trans R Soc Trop Med Hyg1996;90:34–36.
79 Bustos DG, Olveda RM, Negishi M, KurimuraT. Evaluation of a new rapid diagnostic test“Determine Malaria PF” against standard bloodfilm, ICT Malaria P.F and ParaSight F. Jpn JTrop Med Hyg 1999;27:417–425.
80 Funk M, Schlagenhauf P, Tschopp A, SteffenR. MalaQuick versus ParaSight F as a diagnosticaid in travellers’ malaria. Trans R Soc Trop MedHyg 1999;93:268–272.
81 Gaye O, Diouf M, Diallo S. A comparison ofthick smears, QBC malaria, PCR and PATH falciparum malaria test trip in Plasmodium falciparum diagnosis. Parasite 1999;6:273–275.
82 Tjitra E, Suprianto S, Dyer M, et al. Field eval-uation of the ICT malaria P.f/P.v immunochro-matographic test for detection of Plasmodiumfalciparum and Plasmodium vivax in patients witha presumptive clinical diagnosis of malaria ineastern Indonesia. J Clin Microbiol 1999;37:2412–2417.
83 Piper R, Lebras J, Wentworth L, et al. Immuno-capture diagnostic assays for malaria using Plas-modium lactate dehydrogenase (pLDH). Am JTrop Med Hyg 1999;60:109–118.
84 Palmer CJ, Lindo JF, Klaskala WI, et al. Evalu-ation of the OptiMAL test for rapid diagnosis ofPlasmodium vivax and Plasmodium falciparummalaria. J Clin Microbiol 1998;36:203–206.
85 Mills CD, Burgess DC, Taylor HJ, Kain KC.Evaluation of a rapid and inexpensive dipstickassay for the diagnosis of Plasmodium falciparummalaria. Bull World Health Organ 1999;77:553–559.
108 Current Clinical Topics in Infectious Diseases
86 Murahwa FC, Mharakurwa S, Mutambu SL, et al. Diagnostic performance of two antigencapture tests for the diagnosis of Plasmodium fal-ciparum malaria in Zimbabwe. Cent Afr J Med1999;45:97–100.
87 Jelinek T, Grobusch MP, Schwenke S, et al.Sensitivity and specificity of dipstick tests for rapiddiagnosis of malaria in nonimmune travelers. J Clin Microbiol 1999;37:721–723.
88 Iqbal J, Sher A, Hira PR, Al-Owaish R. Com-parison of the OptiMAL test with PCR for diag-nosis of malaria in immigrants. J Clin Microbiol1999;37:3644–3646.
89 Mharakurwa S, Shiff CJ. Post treatment sensi-tivity studies with the ParaSight-F test for malariadiagnosis in Zimbabwe. Acta Trop 1997;66:61–67.
90 Laferi H, Kandel K, Pichler H. False positivedipstick test for malaria [letter] [see comments].N Engl J Med 1997;337:1635–1636.
91 Iqbal J, Sher A, Rab A. Plasmodium falciparumhistidine-rich protein 2-based immunocapturediagnostic assay for malaria: cross-reactivity withrheumatoid factors. J Clin Microbiol 2000;38:1184–1186.
92 Banchongaksorn T, Prajakwong S, Rooney W,Vickers P. Operational trial of ParaSight-F (dip-stick) in the diagnosis of falciparum malaria at theprimary health care level. Southeast Asian J TropMed Public Health 1997;28:243–246.
93 Uguen C, Rabodonirina M, De PJ, et al.ParaSight-F rapid manual diagnostic test of Plas-modium falciparum infection. Bull World HealthOrgan 1995;73:643–649.
94 Leke RF, Djokam RR, Mbu R, et al. Detectionof the Plasmodium falciparum antigen histidine-rich protein 2 in blood of pregnant women:implications for diagnosing placental malaria. JClin Microbiol 1999:2992–2996.
95 Fradin MS. Mosquitoes and mosquito repellents:a clinician’s guide. Ann Intern Med 1998;128:931–940.
96 Nevill CG, Some ES, Mung’ala VO, et al.Insecticide-treated bednets reduce mortality andsevere morbidity from malaria among childrenon the Kenyan coast [see comments]. Trop MedInt Health 1996;1:139–146.
97 Binka FN, Mensah OA, Mills A. The cost-effectiveness of permethrin impregnated bednetsin preventing child mortality in Kassena-Nankana district of Northern Ghana. HealthPolicy 1997;41:229–239.
98 Kere NK, Arabola A, Bakote’e B, et al. Perme-thrin-impregnated bednets are more effectivethan DDT house-spraying to control malaria inSolomon Islands. Med Vet Entomol 1996;10:145–148.
99 Rowland M, Durrani N, Hewitt S, et al. Per-methrin-treated chaddars and top-sheets: appro-priate technology for protection against malaria
in Afghanistan and other complex emergencies.Trans R Soc Trop Med Hyg 1999;93:465–472.
100 Parise ME, Ayisi JG, Nahlen BL, et al. Efficacyof sulfadoxine-pyrimethamine for prevention ofplacental malaria in an area of Kenya with a highprevalence of malaria and human immunodefi-ciency virus infection. Am J Trop Med Hyg1998;59:813–822.
101 Shulman CE, Dorman EK, Cutts F, et al. Inter-mittent sulphadoxine-pyrimethamine to preventsevere anaemia secondary to malaria in preg-nancy: a randomised placebo-controlled trial.Lancet 1999;353:632–636.
102 Cot M, Le HJ, Miailhes P, et al. Effect ofchloroquine prophylaxis during pregnancy onmaternal haematocrit. Ann Trop Med Parasitol1998;92:37–43.
103 Steketee RW, Wirima JJ, Slutsker L, et al.Malaria parasite infection during pregnancy andat delivery in mother, placenta, and newborn:efficacy of chloroquine and mefloquine in ruralMalawi. Am J Trop Med Hyg 1996;55(suppl1):24–32.
104 Steketee RW, Wirima JJ, Hightower AW, et al.The effect of malaria and malaria prevention inpregnancy on offspring birthweight, prematurity,and intrauterine growth retardation in ruralMalawi. Am J Trop Med Hyg 1996;55(suppl 1):33–41.
105 Nosten F, ter Kuile F, Maelankiri L, et al.Mefloquine prophylaxis prevents malaria duringpregnancy: a double-blind, placebo-controlledstudy [see comments]. J Infect Dis 1994;169:595–603.
106 World Health Organization. International travel and health. Vaccination requirements andhealth advice. Geneva, Switzerland: WHO,1999.
107 Ryan ET, Kain KC. Health advice and immu-nizations for travelers. N Engl J Med 2000;342:1716–1725.
108 Winstanley PA. Chemotherapy for falciparummalaria: the armoury, the problems and theprospects. Parasitol Today 2000;16:146–153.
109 Kain KC. Prophylactic drugs for malaria: why dowe need another one? J Travel Med 1999;6(suppl1):S2–S7.
110 Alecrim WD, Espinosa FE, Alecrim MG. Plas-modium falciparum infection in the pregnantpatient. Infect Dis Clin North Am 2000;14:83–95.
111 Lobel HO, Miani M, Eng T, et al. Long-termmalaria prophylaxis with weekly mefloquine.Lancet 1993;341:848–851.
112 Lobel HO, Kozarsky PE. Update on preventionof malaria for travelers [see comments]. JAMA1997;278:1767–1771.
113 Croft A, Garner P. Mefloquine to preventmalaria: a systematic review of trials [see com-ments]. BMJ 1997;315:1412–1416.
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 109
114 Weinke T, Trautmann M, Held T, et al. Neu-ropsychiatric side effects after the use of meflo-quine. Am J Trop Med Hyg 1991;45:86–91.
115 Barrett PJ, Emmins PD, Clarke PD, BradleyDJ. Comparison of adverse events associated withuse of mefloquine and combination of chloro-quine and proguanil as antimalarial prophylaxis:postal and telephone survey of travellers [seecomments]. BMJ 1996;313:525–528.
116 Schlagenhauf P. Mefloquine, methodologies,and the media. J Travel Med 1996;3:197–199.
117 Boudreau E, Schuster B, Sanchez J, et al. Tol-erability of prophylactic Lariam regimens. TropMed Parasitol 1993;44:257–265.
118 Baird JK, Hoffman SL. Prevention of malaria intravelers. Med Clin North Am 1999;83:923–44,vi.
119 Bradley DJ, Warhurst DC. Guidelines for theprevention of malaria in travellers from theUnited Kingdom. PHLS Malaria Reference Laboratory, London School of Hygiene and Tropical Medicine. Commun Dis Rep CDR Rev 1997;7:R137–R152.
120 Pang LW, Limsomwong N, Boudreau EF, Sing-haraj P. Doxycycline prophylaxis for falciparummalaria. Lancet 1987;1:1161–1164.
121 Wallace MR, Sharp TW, Smoak B, et al.Malaria among United States troops in Somalia.Am J Med 1996;100:49–55.
122 Hudson AT, Dickins M, Ginger CD, et al.566C80: a potent broad spectrum anti-infectiveagent with activity against malaria and oppor-tunistic infections in AIDS patients. Drugs ExpClin Res 1991;17:427–435.
123 Srivastava IK, Morrisey JM, Darrouzet E, et al.Resistance mutations reveal the atovaquone-binding domain of cytochrome b in malaria par-asites. Mol Microbiol 1999;33:704–711.
124 Looareesuwan S, Viravan C, Webster HK, et al.Clinical studies of atovaquone, alone or in combination with other antimalarial drugs, fortreatment of acute uncomplicated malaria inThailand. Am J Trop Med Hyg 1996;54:62–66.
125 Warhurst DC. Antimalarial drugs. An update.Drugs 1987;33:50–65.
126 Srivastava IK, Vaidya AB. A mechanism for thesynergistic antimalarial action of atovaquone andproguanil. Antimicrob Agents Chemother 1999;43:1334–1339.
127 Shapiro TA, Ranasinha CD, Kumar N,Barditch-Crovo P. Prophylactic activity of atovaquone against Plasmodium falciparum inhumans. Am J Trop Med Hyg 1999;60:831–836.
128 Chulay JD. Challenges in the development ofantimalarial drugs with causal prophylactic activ-ity. Trans R Soc Trop Med Hyg 1998;92:577–579.
129 Shanks GD, Gordon DM, Klotz FW, et al. Effi-cacy and safety of atovaquone/proguanil as sup-pressive prophylaxis for Plasmodium falciparummalaria. Clin Infect Dis 1998;27:494–499.
130 Sukwa TY, Mulenga M, Chisdaka N, et al. Arandomized, double-blind, placebo-controlledfield trial to determine the efficacy and safety ofMalarone (atovaquone/proguanil) for the pro-phylaxis of malaria in Zambia. Am J Trop MedHyg 1999;60:521–525.
131 Lell B, Luckner D, Ndjave M, et al. Ran-domised placebo-controlled study of atovaquoneplus proguanil for malaria prophylaxis in chil-dren. Lancet 1998;351:709–713.
132 van der Berg JD, Duvenage CS, Roskell NS,Scott TR. Safety and efficacy of atovaquone andproguanil hydrochloride for the prophylaxis ofPlasmodium falciparum malaria in South Africa.Clin Ther 1999;21:741–749.
133 Hogh B, Clarke PD, Camus D, et al. Ato-vaquone-proguanil versus chloroquine-proguanilfor malaria prophylaxis in non-immune travelers:a randomized, double-blind study. MalaroneInternational Study Team. Lancet 2000;356(9245):1888–1894.
134 Radloff PD, Philipps J, Hutchinson D, Krem-sner PG. Atovaquone plus proguanil is an effec-tive treatment for Plasmodium ovale and P.malariae malaria. Trans R Soc Trop Med Hyg1996;90:682.
135 Shanks GD, Kremsner PG, Sukwa TY, et al.Atovaquone and proguanil hydrochloride for pro-phylaxis of malaria. J Travel Med 1999;6(suppl1):S21–S27.
136 Fryauff DJ, Baird JK, Basri H, et al. Randomisedplacebo-controlled trial of primaquine for pro-phylaxis of falciparum and vivax malaria. Lancet1995;346:1190–1193.
137 Baird JK, Basri H, Subianto B, et al. Treatmentof chloroquine-resistant Plasmodium vivax withchloroquine and primaquine or halofantrine. J Infect Dis 1995;171:1678–1682.
138 Weiss WR, Oloo AJ, Johnson A, et al. Daily primaquine is effective for prophylaxis against falciparum malaria in Kenya: comparison withmefloquine, doxycycline, and chloroquine plusproguanil [see comments]. J Infect Dis 1995;171:1569–1575.
139 Soto J, Toledo J, Rodriquez M, et al. Pri-maquine prophylaxis against malaria in nonim-mune Colombian soldiers: efficacy and toxicity.A randomized, double-blind, placebo-controlledtrial [see comments]. Ann Intern Med 1998;129:241–244.
140 Brueckner RP, Lasseter KC, Lin ET, SchusterBG. First-time-in-humans safety and pharmaco-kinetics of WR 238605, a new antimalarial. AmJ Trop Med Hyg 1998;58:645–649.
141 Walsh DS, Looareesuwan S, Wilairatana P, et al. Randomized dose-ranging study of thesafety and efficacy of WR 238605 (tafenoquine)in the prevention of relapse of Plasmodium vivax malaria in Thailand. J Infect Dis 1999;180:1282–1287.
110 Current Clinical Topics in Infectious Diseases
142 Peragallo MS, Sabatinelli G, Majori G, et al.Prevention and morbidity of malaria in non-immune subjects; a case-control study amongItalian troops in Somalia and Mozambique,1992–1994. Trans R Soc Trop Med Hyg 1997;91:343–346.
143 Anderson SL, Berman J, Kuschner R, et al.Prophylaxis of Plasmodium falciparum malariawith azithromycin administered to volunteers.Ann Intern Med 1995;123:771–773.
144 Phillips-Howard PA, Wood D. The safety of anti-malarial drugs in pregnancy. Drug Saf1996;14:131–145.
145 Smoak BL, Writer JV, Keep LW, et al. Theeffects of inadvertent exposure of mefloquinechemoprophylaxis on pregnancy outcomes andinfants of US Army servicewomen. J Infect Dis1997;176:831–833.
146 Vanhauwere B, Maradit H, Kerr L. Post-marketing surveillance of prophylactic meflo-quine (Lariam) use in pregnancy. Am J Trop MedHyg 1998;58:17–21.
147 Nosten F, Karbwang J, White NJ, et al. Meflo-quine antimalarial prophylaxis in pregnancy:dose finding and pharmacokinetic study. Br JClin Pharmacol 1990;30:79–85.
148 Phillips-Howard PA, Steffen R, Kerr L, et al.Safety of mefloquine and other antimalarialagents in the first trimester of pregnancy. J TravelMed 1998;5:121–126.
149 White NJ. The treatment of malaria [see com-ments]. N Engl J Med 1996;335:800–806.
150 World Health Organization (2000). Severe falciparum malaria. Transactions of the RoyalSociety of Tropical Medicine and Hygiene, 94,supplement 1.
151 Looareesuwan S, Wilairatana P, Vanijanonta S,et al. Efficacy of quinine–tetracycline for acuteuncomplicated falciparum malaria in Thailand[letter]. Lancet 1992;339:369.
152 Watt G, Loesuttivibool L, Shanks GD, et al.Quinine with tetracycline for the treatment ofdrug-resistant falciparum malaria in Thailand.Am J Trop Med Hyg 1992;47:108–111.
153 Meek SR, Doberstyn EB, Gauzere BA, et al.Treatment of falciparum malaria with quinineand tetracycline or combined mefloquine/sulfadoxine/pyrimethamine on the Thai–Kampuchean border. Am J Trop Med Hyg1986;35:246–250.
154 Kremsner PG, Winkler S, Brandts C, et al.Curing of chloroquine-resistant malaria with clin-damycin. Am J Trop Med Hyg 1993;49:650–654.
155 Kremsner PG, Zotter GM, Feldmeier H, et al.Clindamycin treatment of falciparum malaria in Brazil. J Antimicrob Chemother 1989;23:275–281.
156 Zalis MG, Pang L, Silveira MS, et al. Charac-terization of Plasmodium falciparum isolatedfrom the Amazon region of Brazil: evidence for
quinine resistance. Am J Trop Med Hyg 1998;58:630–637.
157 Adagu IS, Warhurst DC, Ogala WN, et al. Anti-malarial drug response of Plasmodium falciparumfrom Zaria, Nigeria. Trans R Soc Trop Med Hyg1995;89:422–425.
158 Kremsner PG, Looareesuwan S, Chulay JD.Atovaquone and proguanil hydrochloride fortreatment of malaria. J Travel Med 1999;6(suppl1):S18–S20.
159 Looareesuwan S, Wilairatana P, ChalermarutK, et al. Efficacy and safety of atovaquone/proguanil compared with mefloquine for treat-ment of acute Plasmodium falciparum malaria inThailand. Am J Trop Med Hyg 1999;60:526–532.
160 Looareesuwan S, Chulay JD, Canfield CJ,Hutchinson DB. Malarone (atovaquone andproguanil hydrochloride): a review of its clinicaldevelopment for treatment of malaria. MalaroneClinical Trials Study Group. Am J Trop Med Hyg1999;60:533–541.
161 Mulenga M, Sukwa TY, Canfield CJ, Hutchin-son DB. Atovaquone and proguanil versuspyrimethamine/sulfadoxine for the treatment ofacute falciparum malaria in Zambia. Clin Ther1999;21:841–852.
162 Bustos DG, Canfield CJ, Canete-Miguel E,Hutchinson DB. Atovaquone–proguanil com-pared with chloroquine and chloroquine–sulfadoxine-pyrimethamine for treatment ofacute Plasmodium falciparum malaria in thePhilippines [see comments]. J Infect Dis1999;179:1587–1590.
163 Sabchareon A, Attanath P, Phanuaksook P, etal. Efficacy and pharmacokinetics of atovaquoneand proguanil in children with multidrug-resistant Plasmodium falciparum malaria. TransR Soc Trop Med Hyg 1998;92:201–206.
164 Yeo AE, Edstein MD, Shanks GD, RieckmannKH. Potentiation of the antimalarial activity ofatovaquone by doxycycline against Plasmodiumfalciparum in vitro. Parasitol Res 1997;83:489–491.
165 Harinasuta T, Bunnag D, Lasserre R, et al.Trials of mefloquine in vivax and of mefloquineplus “fansidar” in falciparum malaria. Lancet1985;1:885–888.
166 Looareesuwan S, Wilairatana P, Chokejin-dachai W, et al. Research on new antimalarialdrugs and the use of drugs in combination at theBangkok Hospital for Tropical Diseases. South-east Asian J Trop Med Public Health 1998;29:344–354.
167 Price R, Luxemburger C, Van Vugt M, et al.Artesunate and mefloquine in the treatment ofuncomplicated multidrug-resistant hyperpara-sitaemic falciparum malaria. Trans R Soc TropMed Hyg 1998;92:207–211.
168 Monlun E, Leenhardt A, Pillet O, et al. Ven-tricular arrhythmia and halofantrine intake.
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 111
169 van Vugt M, Angus BJ, Price RN, et al. A case-control auditory evaluation of patients treatedwith artemisinin derivatives for multidrug-resistant Plasmodium falciparum malaria. Am JTrop Med Hyg 2000;62:65–69.
170 McIntosh HM, Olliaro P. Treatment of severemalaria with artemisinin derivatives. A systematicreview of randomised controlled trials. Med Trop(Mars) 1998;58(suppl 3):61–62.
171 Ribeiro IR, Olliaro P. Safety of artemisinin andits derivatives. A review of published and unpub-lished clinical trials. Med Trop (Mars) 1998;58(suppl 3):50–53.
172 Dayan AD. Neurotoxicity and artemisinin com-pounds: do the observations in animals justifylimitation of clinical use? Med Trop (Mars)1998;58(suppl 3):32–37.
173 Looareesuwan S, Viravan C, Vanijanonta S, et al. Randomised trial of artesunate and meflo-quine alone and in sequence for acute uncom-plicated falciparum malaria. Lancet 1992;339:821–824.
174 Nosten F, Luxemburger C, ter Kuile FO, et al.Treatment of multidrug-resistant Plasmodium falciparum malaria with 3-day artesunate–mefloquine combination [published erratumappears in J Infect Dis 1995;171:519]. J Infect Dis 1994;170:971–977.
175 von Seidlein L, Jaffar S, Pinder M, et al. Treat-ment of African children with uncomplicated fal-ciparum malaria with a new antimalarial drug,CGP 56697. J Infect Dis 1997;176:1113–1116.
176 McIntosh HM, Olliaro P. Treatment of uncom-plicated malaria with artemisinin derivatives. Asystematic review of randomised controlled trials.Med Trop (Mars) 1998;58:57–58.
177 Price R, Simpson JA, Teja-Isavatharm P, et al.Pharmacokinetics of mefloquine combined withartesunate in children with acute falciparummalaria. Antimicrob Agents Chemother 1999;43:341–346.
178 Price R, van Vugt M, Phaipun L, et al. Adverseeffects in patients with acute falciparum malariatreated with artemisinin derivatives. Am J TropMed Hyg 1999;60:547–555.
179 de Vries PJ, Bich NN, Van Thien H, et al.Combinations of artemisinin and quinine foruncomplicated falciparum malaria: efficacy and pharmacodynamics. Antimicrob AgentsChemother 2000;44:1302–1308.
180 Doherty JF, Sadiq AD, Bayo L, et al. A ran-domized safety and tolerability trial of artesunateplus sulfadoxine-pyrimethamine versus sulfadox-ine-pyrimethamine alone for the treatment ofuncomplicated malaria in Gambian children.Trans R Soc Trop Med Hyg 1999;93:543–546.
181 Anonymous. The comparative efficacy and tolerability of CGP 56697 (artemether + lume-
fantrine) versus halofantrine in the treatment ofuncomplicated falciparum malaria in travellersreturning from the tropics to the Netherlands and France. Int J Antimicrob Agents 1999;12:159–169.
182 van Vugt M, Ezzet F, Nosten F, et al. No evi-dence of cardiotoxicity during antimalarial treat-ment with artemether–lumefantrine. Am J TropMed Hyg 1999;61:964–967.
183 Skelton-Stroud P, Mull R. Positioning, labelling,and medical information control of co-artemether tablets (CPG 56697): a fixed novelcombination of artemether and benflumetol.Novartis Co-Artemether International Develop-ment Team. Med Trop (Mars) 1998;58(suppl3):77–81.
184 White NJ, van Vugt M, Ezzet F. Clinical pharmacokinetics and pharmacodynamics ofartemether–lumefantrine. Clin Pharmacokinet1999;37:105–125.
185 Ezzet F, van Vugt M, Nosten F, et al. Pharma-cokinetics and pharmacodynamics of lume-fantrine (benflumetol) in acute falciparummalaria. Antimicrob Agents Chemother 2000;44:697–704.
186 Tanariya P, Tippawangkoso P, Karbwang J, et al.In vitro sensitivity of Plasmodium falciparum andclinical response to lumefantrine (benflumetol)and artemether. Br J Clin Pharmacol 2000;49:437–444.
187 van Vugt MV, Wilairatana P, Gemperli B, et al.Efficacy of six doses of artemether–lumefantrine(benflumetol) in multidrug-resistant Plasmodiumfalciparum malaria. Am J Trop Med Hyg1999;60:936–942.
188 Ringwald P, Bickii J, Same-Ekobo A, Basco LK.Pyronaridine for treatment of Plasmodium ovaleand Plasmodium malariae infections. AntimicrobAgents Chemother 1997;41:2317–2319.
189 Ringwald P, Bickii J, Basco LK. Efficacy of oralpyronaridine for the treatment of acute uncom-plicated falciparum malaria in African children.Clin Infect Dis 1998;26:946–953.
190 Ringwald P, Bickii J, Basco L. Randomised trialof pyronaridine versus chloroquine for acuteuncomplicated falciparum malaria in Africa [seecomments]. Lancet 1996;347:24–28.
191 Chang C, Lin-Hua T, Jantanavivat C. Studieson a new antimalarial compound: pyronaridine.Trans R Soc Trop Med Hyg 1992;86:7–10.
192 Looareesuwan S, Kyle DE, Viravan C, et al.Clinical study of pyronaridine for the treatmentof acute uncomplicated falciparum malaria inThailand. Am J Trop Med Hyg 1996;54:205–209.
193 Chen C, Zheng X. Development of the new anti-malarial drug pyronaridine: a review. BiomedEnviron Sci 1992;5:149–160.
194 Watkins WM, Brandling-Bennett AD, NevillCG, et al. Chlorproguanil/dapsone for the treat-ment of non-severe Plasmodium falciparum
112 Current Clinical Topics in Infectious Diseases
malaria in Kenya: a pilot study. Trans R Soc TropMed Hyg 1988;82:398–403.
195 Keuter M, van Eijk A, Hoogstrate M, et al.Comparison of chloroquine, pyrimethamine andsulfadoxine, and chlorproguanil and dapsone astreatment for falciparum malaria in pregnant and non-pregnant women, Kakamega District,Kenya. BMJ 1990;301:466–470.
197 Ortelli F, Maxwell CA, Curtis J, Watkins WM.Studies on anti-folate antimalarials in East Africa.Parassitologia 1999;41:313–314.
198 Nzila-Mounda A, Mberu EK, Sibley CH, et al.Kenyan Plasmodium falciparum field isolates:correlation between pyrimethamine and chlorcy-cloguanil activity in vitro and point mutations inthe dihydrofolate reductase domain. AntimicrobAgents Chemother 1998;42:164–169.
199 Okonkwo CA, Coker HA, Agomo PU, et al.Effect of chlorpheniramine on the pharmacoki-netics of and response to chloroquine of Niger-ian children with falciparum malaria. Trans RSoc Trop Med Hyg 1999;93:306–311.
200 Sowunmi A, Oduola AM, Ogundahunsi OA, etal. Enhanced efficacy of chloroquine–chlor-pheniramine combination in acute uncom-plicated falciparum malaria in children [seecomments]. Trans R Soc Trop Med Hyg 1997;91:63–67.
201 Sowunmi A, Oduola AM. Comparative efficacyof chloroquine/chlorpheniramine combinationand mefloquine for the treatment of chloroquine-resistant Plasmodium falciparum malaria inNigerian children. Trans R Soc Trop Med Hyg1997;91:689–693.
202 Sowunmi A, Oduola AM, Ogundahunsi OA,Salako LA. Comparative efficacy of chloroquineplus chlorpheniramine and pyrimethamine/sulfadoxine in acute uncomplicated falciparummalaria in Nigerian children. Trans R Soc TropMed Hyg 1998;92:77–81.
203 Sowunmi A, Fehintola FA, Ogundahunsi OA,et al. Comparative cardiac effects of halofantrineand chloroquine plus chlorpheniramine in chil-dren with acute uncomplicated falciparummalaria. Trans R Soc Trop Med Hyg 1999;93:78–83.
204 Phillips RE, Warrell DA, White NJ, et al. Intra-venous quinidine for the treatment of severe fal-ciparum malaria. Clinical and pharmacokineticstudies. N Engl J Med 1985;312:1273–1278.
205 Sabchareon A, Chongsuphajaisiddhi T, Sin-hasivanon V, et al. In vivo and in vitro responsesto quinine and quinidine of Plasmodium falci-parum. Bull World Health Organ 1988;66:347–352.
206 Anonymous. Treatment of severe Plasmodiumfalciparum malaria with quinidine gluconate: dis-
continuation of parenteral quinine from CDCdrug service. MMWR 1991;40:240.
207 Anonymous. Treatment with quinidine glu-conate of persons with severe Plasmodium falci-parum infection: discontinuation of parenteralquinine from CDC Drug Service. MMWR1991;40:21–23.
208 Phillips RE, Looareesuwan S, White NJ, et al.Hypoglycaemia and antimalarial drugs: quini-dine and release of insulin. Br Med J (Clin ResEd) 1986;292:1319–1321.
209 van Hensbroek MB, Onyiorah E, Jaffar S, et al.A trial of artemether or quinine in children withcerebral malaria [see comments]. N Engl J Med1996;335:69–75.
210 Tran TH, Day NP, Nguyen HP, et al. A con-trolled trial of artemether or quinine in Viet-namese adults with severe falciparum malaria[see comments]. N Engl J Med 1996;335:76–83.
211 Pittler MH, Ernst E. Artemether for severemalaria: a meta-analysis of randomized clinicaltrials. Clin Infect Dis 1999;28:597–601.
212 Birku Y, Makonnen E, Bjorkman A. Compari-son of rectal artemisinin with intravenousquinine in the treatment of severe malaria inEthiopia. East Afr Med J 1999;76:154–159.
213 Luzzi GA, Warrell DA, Barnes AJ, Dunbar EM.Treatment of primaquine-resistant Plasmodiumvivax malaria [letter]. Lancet 1992;340:310.
214 Bunnag D, Karbwang J, Thanavibul A, et al.High dose of primaquine in primaquine resistantvivax malaria [published erratum appears inTrans R Soc Trop Med Hyg 1994;88:584]. TransR Soc Trop Med Hyg 1994;88:218–219.
215 Wilairatana P, Silachamroon U, Krudsood S, et al. Efficacy of primaquine regimens for primaquine-resistant Plasmodium vivax malaria inThailand. Am J Trop Med Hyg 1999;61:973–977.
216 Diagne N, Rogier C, Sokhna CS, et al.Increased susceptibility to malaria during theearly postpartum period. N Engl J Med 2000;343(9):598–603.
217 Nosten F, Vincenti M, Simpson J, et al. Theeffects of mefloquine treatment in pregnancy.Clin Infect Dis 1999;28:808–815.
218 McGready R, Cho T, Cho JJ, et al. Artemisininderivatives in the treatment of falciparum malariain pregnancy. Trans R Soc Trop Med Hyg1998;92:430–433.
219 Looareesuwan S, Phillips RE, Karbwang J, et al.Plasmodium falciparum hyperparasitaemia: useof exchange transfusion in seven patients and a review of the literature. Q J Med 1990;75:471–481.
220 van den Ende, Moorkens G, van Gompel A, etal. Twelve patients with severe malaria treatedwith partial exchange transfusion. Comparisonbetween mathematically predicted and observedeffect on parasitaemia. Trop Geogr Med 1994;46:340–345.
Malaria: Epidemiology, Pathogenesis, Diagnosis, Prevention, and Treatment 113
221 Thuma PE, Mabeza GF, Biemba G, et al.Effect of iron chelation therapy on mortality inZambian children with cerebral malaria. Trans RSoc Trop Med Hyg 1998;92:214–218.
222 Hemmer CJ, Hort G, Chiwakata CB, et al.Supportive pentoxifylline in falciparum malaria:no effect on tumor necrosis factor alpha levels or clinical outcome: a prospective, randomized,placebo-controlled study. Am J Trop Med Hyg1997;56:397–403.
223 Looareesuwan S, Wilairatana P, Vannaphan S,et al. Pentoxifylline as an ancillary treatment forsevere falciparum malaria in Thailand. Am J TropMed Hyg 1998;58:348–353.
224 Newton CR, Crawley J, Sowumni A, et al.Intracranial hypertension in Africans with cere-bral malaria. Arch Dis Child 1997;76:219–226.
225 White NJ, Looareesuwan S, Phillips RE, et al.Single dose phenobarbitone prevents convul-sions in cerebral malaria. Lancet 1988;2:64–66.