Journal of Case Reports and Images in Pathology, Vol. 6, 2020. J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com Vasudev et al. 1 CASE REPORT PEER REVIEWED | OPEN ACCESS Malignant chondroid syringoma: A case report and literature review Pooja Vasudev, Gabriela Gohla, Samih Salama, Salem Alowami ABSTRACT Introduction: Malignant mixed tumor of the skin/ malignant chondroid syringoma (MCS) is a very rare adnexal tumor that is considered as the malignant counterpart of the benign mixed tumor/benign chondroid syringoma (BSC) of the skin. It usually arises de novo in the extremities and takes an unpredictable clinical course with high incidence of local recurrence, distance metastasis, and death. We present a rare case of malignant chondroid syringoma of the forearm which metastasized to the axillary lymph node despite aggressive local treatment. Case Report: An 83-year-old male with history of numerous prior cutaneous neoplasms, presented with a forearm nodular keratotic lesion, clinically thought to be an invasive squamous cell carcinoma. Accurate histopathological examination revealed a completely excised malignant chondroid syringoma. The patient underwent wide local re-excision of the scar, followed by four weeks of local radiotherapy. Although there was no evidence of any local recurrence, he developed axillary lymph node metastasis four years after the initial diagnosis, for which he underwent axillary lymph node dissection. Pooja Vasudev 1 , Gabriela Gohla 2 , Samih Salama 3 , Salem Alowami 3 Affiliations: 1 Assistant Professor, Department of Pathol- ogy and Molecular Medicine, McMaster University, Ham- ilton, Ontario, Canada; 2 Associate Professor, Department of Pathology and Molecular Medicine, McMaster Univer- sity, Hamilton, Ontario, Canada; 3 Professor, Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada. Corresponding Author: Pooja Vasudev, Assistant Profes- sor, Department of Pathology and Molecular Medicine, St. Joseph's Healthcare, L222-5, St Luke Wing, 50 Charlton Avenue East, Hamilton, ON L8N 4A6, Canada; Email: [email protected]Received: 27 August 2020 Accepted: 27 October 2020 Published: 07 December 2020 Conclusion: Malignant chondroid syringomas are exceedingly rare tumors, but with a high incidence of recurrence, metastasis, and death. These cases need to be diagnosed with strict histopathological criteria. Current treatment of MCS comprises of complete excision with wide margins plus or minus local radiotherapy to prevent local recurrence. Close follow-up and staging are recommended to aid in early detection of recurrence or metastasis. Keywords: Chondroid syringoma, Malignant mixed tumor, Metastatic, Skin adnexal tumor How to cite this article Vasudev P, Gohla G, Salama S, Alowami S. Malignant chondroid syringoma: A case report and literature review. J Case Rep Images Pathol 2020;6:100046Z11PV2020. Article ID: 100046Z11PV2020 ********* doi: 10.5348/100046Z11PV2020CR INTRODUCTION Malignant mixed tumor of the skin/malignant chondroid syringoma (MCS) is a very rare cutaneous adnexal malignancy that is biphasic in origin, with malignant epithelial and mesenchymal components [1, 2]. Its benign counterpart, benign chondroid syringoma (BCS) is also rare, comprising <0.01% of all primary skin tumors, and mostly occurring on the head and neck region [3]. The MCS (which has only about 40 cases being reported in the literature) is most often reported in the extremities and trunk, with only a few cases reported in the head and neck region [4, 5]. Most of the time there is anaplastic changes noted from early on [2, 6], with a requirement for the diagnosis of MCS to have some semblance to its benign counterpart [7].
Transcript
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 1
CASE REPORT PEER REVIEWED | OPEN ACCESS
Malignant chondroid syringoma: A case report and literature review
Pooja Vasudev, Gabriela Gohla, Samih Salama, Salem Alowami
ABSTRACT
Introduction: Malignant mixed tumor of the skin/malignant chondroid syringoma (MCS) is a very rare adnexal tumor that is considered as the malignant counterpart of the benign mixed tumor/benign chondroid syringoma (BSC) of the skin. It usually arises de novo in the extremities and takes an unpredictable clinical course with high incidence of local recurrence, distance metastasis, and death. We present a rare case of malignant chondroid syringoma of the forearm which metastasized to the axillary lymph node despite aggressive local treatment.
Case Report: An 83-year-old male with history of numerous prior cutaneous neoplasms, presented with a forearm nodular keratotic lesion, clinically thought to be an invasive squamous cell carcinoma. Accurate histopathological examination revealed a completely excised malignant chondroid syringoma. The patient underwent wide local re-excision of the scar, followed by four weeks of local radiotherapy. Although there was no evidence of any local recurrence, he developed axillary lymph node metastasis four years after the initial diagnosis, for which he underwent axillary lymph node dissection.
Pooja Vasudev1, Gabriela Gohla2, Samih Salama3, Salem Alowami3
Affiliations: 1Assistant Professor, Department of Pathol-ogy and Molecular Medicine, McMaster University, Ham-ilton, Ontario, Canada; 2Associate Professor, Department of Pathology and Molecular Medicine, McMaster Univer-sity, Hamilton, Ontario, Canada; 3Professor, Department of Pathology and Molecular Medicine, McMaster University, Hamilton, Ontario, Canada.Corresponding Author: Pooja Vasudev, Assistant Profes-sor, Department of Pathology and Molecular Medicine, St. Joseph's Healthcare, L222-5, St Luke Wing, 50 Charlton Avenue East, Hamilton, ON L8N 4A6, Canada; Email: [email protected]
Received: 27 August 2020Accepted: 27 October 2020Published: 07 December 2020
Conclusion: Malignant chondroid syringomas are exceedingly rare tumors, but with a high incidence of recurrence, metastasis, and death. These cases need to be diagnosed with strict histopathological criteria. Current treatment of MCS comprises of complete excision with wide margins plus or minus local radiotherapy to prevent local recurrence. Close follow-up and staging are recommended to aid in early detection of recurrence or metastasis.
Vasudev P, Gohla G, Salama S, Alowami S. Malignant chondroid syringoma: A case report and literature review. J Case Rep Images Pathol 2020;6:100046Z11PV2020.
Article ID: 100046Z11PV2020
*********
doi: 10.5348/100046Z11PV2020CR
INTRODUCTION
Malignant mixed tumor of the skin/malignant chondroid syringoma (MCS) is a very rare cutaneous adnexal malignancy that is biphasic in origin, with malignant epithelial and mesenchymal components [1, 2]. Its benign counterpart, benign chondroid syringoma (BCS) is also rare, comprising <0.01% of all primary skin tumors, and mostly occurring on the head and neck region [3]. The MCS (which has only about 40 cases being reported in the literature) is most often reported in the extremities and trunk, with only a few cases reported in the head and neck region [4, 5]. Most of the time there is anaplastic changes noted from early on [2, 6], with a requirement for the diagnosis of MCS to have some semblance to its benign counterpart [7].
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 2
We present a case of malignant chondroid syringoma of the distal forearm in a patient with history of multiple prior cutaneous malignancies including a scalp melanoma. The MCS, which was treated with complete excision, wide re-excision of scar, and local radiotherapy; metastasized to the axillary lymph nodes, four years after the initial diagnosis. This case highlights some of the unique characteristics of this adnexal malignancy including a propensity for metastasis and probable resistance to radiotherapy. We also consider the possible utility of sentinel lymph node biopsy in the treatment of these highly malignant adnexal tumors [8].
CASE REPORT
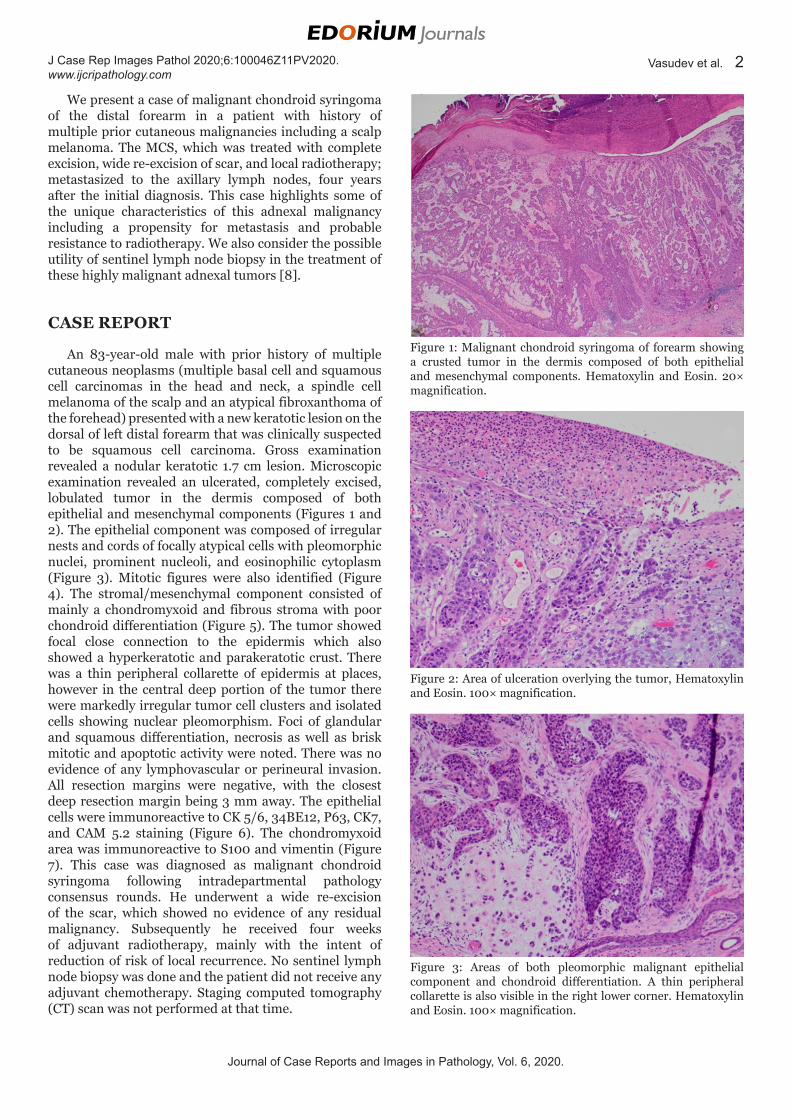
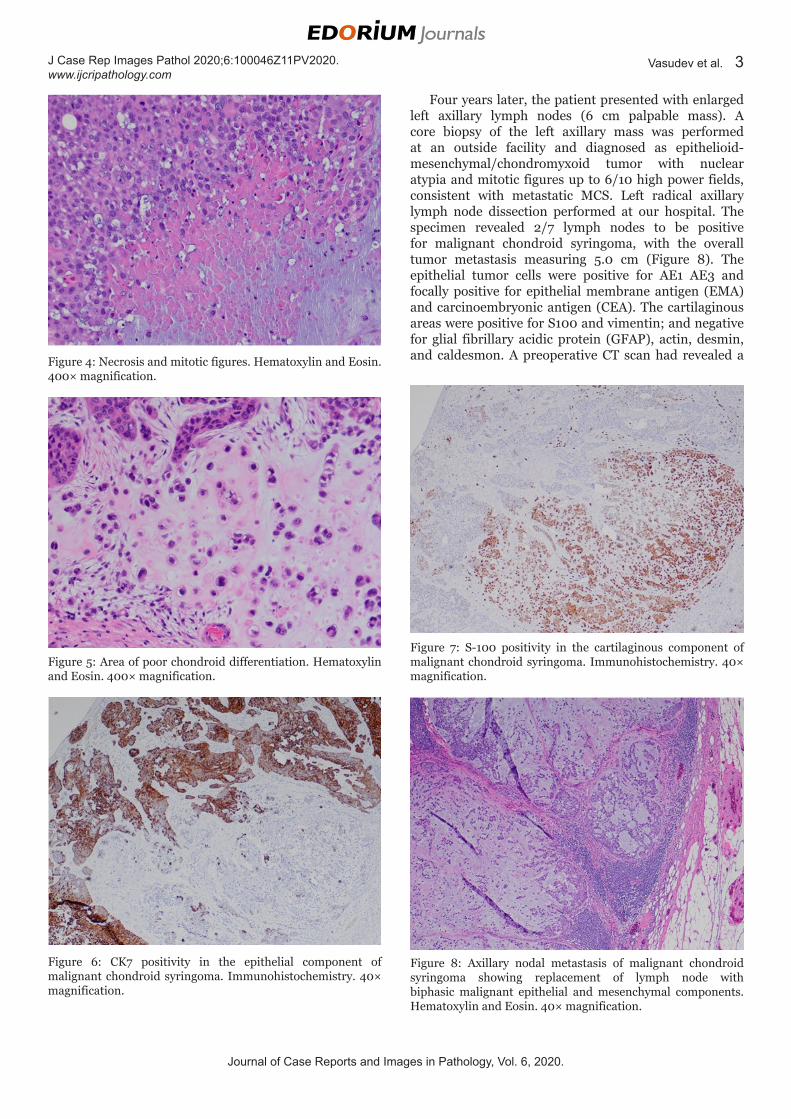
An 83-year-old male with prior history of multiple cutaneous neoplasms (multiple basal cell and squamous cell carcinomas in the head and neck, a spindle cell melanoma of the scalp and an atypical fibroxanthoma of the forehead) presented with a new keratotic lesion on the dorsal of left distal forearm that was clinically suspected to be squamous cell carcinoma. Gross examination revealed a nodular keratotic 1.7 cm lesion. Microscopic examination revealed an ulcerated, completely excised, lobulated tumor in the dermis composed of both epithelial and mesenchymal components (Figures 1 and 2). The epithelial component was composed of irregular nests and cords of focally atypical cells with pleomorphic nuclei, prominent nucleoli, and eosinophilic cytoplasm (Figure 3). Mitotic figures were also identified (Figure 4). The stromal/mesenchymal component consisted of mainly a chondromyxoid and fibrous stroma with poor chondroid differentiation (Figure 5). The tumor showed focal close connection to the epidermis which also showed a hyperkeratotic and parakeratotic crust. There was a thin peripheral collarette of epidermis at places, however in the central deep portion of the tumor there were markedly irregular tumor cell clusters and isolated cells showing nuclear pleomorphism. Foci of glandular and squamous differentiation, necrosis as well as brisk mitotic and apoptotic activity were noted. There was no evidence of any lymphovascular or perineural invasion. All resection margins were negative, with the closest deep resection margin being 3 mm away. The epithelial cells were immunoreactive to CK 5/6, 34BE12, P63, CK7, and CAM 5.2 staining (Figure 6). The chondromyxoid area was immunoreactive to S100 and vimentin (Figure 7). This case was diagnosed as malignant chondroid syringoma following intradepartmental pathology consensus rounds. He underwent a wide re-excision of the scar, which showed no evidence of any residual malignancy. Subsequently he received four weeks of adjuvant radiotherapy, mainly with the intent of reduction of risk of local recurrence. No sentinel lymph node biopsy was done and the patient did not receive any adjuvant chemotherapy. Staging computed tomography (CT) scan was not performed at that time.
Figure 1: Malignant chondroid syringoma of forearm showing a crusted tumor in the dermis composed of both epithelial and mesenchymal components. Hematoxylin and Eosin. 20× magnification.
Figure 2: Area of ulceration overlying the tumor, Hematoxylin and Eosin. 100× magnification.
Figure 3: Areas of both pleomorphic malignant epithelial component and chondroid differentiation. A thin peripheral collarette is also visible in the right lower corner. Hematoxylin and Eosin. 100× magnification.
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 3
Four years later, the patient presented with enlarged left axillary lymph nodes (6 cm palpable mass). A core biopsy of the left axillary mass was performed at an outside facility and diagnosed as epithelioid-mesenchymal/chondromyxoid tumor with nuclear atypia and mitotic figures up to 6/10 high power fields, consistent with metastatic MCS. Left radical axillary lymph node dissection performed at our hospital. The specimen revealed 2/7 lymph nodes to be positive for malignant chondroid syringoma, with the overall tumor metastasis measuring 5.0 cm (Figure 8). The epithelial tumor cells were positive for AE1 AE3 and focally positive for epithelial membrane antigen (EMA) and carcinoembryonic antigen (CEA). The cartilaginous areas were positive for S100 and vimentin; and negative for glial fibrillary acidic protein (GFAP), actin, desmin, and caldesmon. A preoperative CT scan had revealed a Figure 4: Necrosis and mitotic figures. Hematoxylin and Eosin.
400× magnification.
Figure 5: Area of poor chondroid differentiation. Hematoxylin and Eosin. 400× magnification.
Figure 6: CK7 positivity in the epithelial component of malignant chondroid syringoma. Immunohistochemistry. 40× magnification.
Figure 7: S-100 positivity in the cartilaginous component of malignant chondroid syringoma. Immunohistochemistry. 40× magnification.
Figure 8: Axillary nodal metastasis of malignant chondroid syringoma showing replacement of lymph node with biphasic malignant epithelial and mesenchymal components. Hematoxylin and Eosin. 40× magnification.
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 4
suspicious left lower lobe lung nodule, 1.8 cm in largest dimension; the patient underwent a CT guided biopsy of the same with a diagnosis of metastatic melanoma.
The patient’s past clinical history was significant for chronic renal failure, anemia, hypertension, dyslipidemia, chronic atrial fibrillation, benign prostatic hyperplasia, a possible past transient ischemic attack affecting left hand, a recent right hip fracture treated with open reduction and internal fixation and a recently identified left frontal meningioma. After the radical axillary lymph node dissection, the patient was discharged home with no additional medical management, beyond the drugs he was already on for control/treatment of his existing medical conditions.
DISCUSSION
Malignant chondroid syringomas are extraordinarily rare tumors which are considered to be the malignant counterpart of BCS; biphasic tumors of eccrine cutaneous glands origin comprising of epithelial and mesenchymal components, similar conceptually to the pleomorphic tumor of salivary glands [1]. Malignant chondroid syringomas usually arise de novo or can rarely develop in a BSC [2, 9].
There is no clear age predisposition for these tumors; the mean age of the patients at the time of diagnosis was 48.3 years (range 13–86 years) [1, 6]. Malignant chondroid syringoma has an apparent female predisposition (female: male ratio of 3:2), and occurs most commonly in the extremities [10]. Other reported sites include the trunk such as the sacral region, and the head and neck area [6]. While BCSs are usually small well-defined lesions, MCSs may have a more infiltrative appearance and have a median size of 4 cm (range 1.4–10 cm) [4]. Clinical diagnosis is often challenging, due to the lack of defining clinical characteristics and rarity of this condition [2]. These lesions have been clinically thought to be a variety of other entities such as a sebaceous cyst or neurofibroma [3]. In our case, the small size, keratotic nodular appearance, and prior history of multiple prior sun exposure-related cutaneous neoplasms in an elderly male lead to the clinical impression of invasive squamous cell carcinoma.
The final diagnosis rests of accurate histopathological examination of hematoxylin and eosin (H&E) stained slides of the excision specimen [4]. The epithelial component has both epithelial and myoepithelial cells with either eccrine or apocrine differentiation. The malignant epithelial component usually shows increased cellularity, isolated cells, small clusters, glands, solid sheets, infiltrative growth, necrosis (including comedonecrosis), nuclear pleomorphism, tumor giant cells, increased mitotic activity, atypical mitoses, and perineural and/or lymphovascular invasion [1, 4, 10]. We found similar features, as well as increased apoptotic activity and both glandular and squamous differentiation.
The mesenchymal components can be mucinous, cartilaginous, or osteoid in differentiation [3]. Aggressive behavior is associated with a large amount of mucoid matrix and poor chondroid differentiation of the tumor, the latter of which appears to be consistent with the findings and presentation in our case [11]. Dermal satellite nodules and osseous metaplasia have also been reported [6, 11]. Involvement of subcutaneous/deep structures and a local recurrence of a lesion also raises the possibility of malignancy [2, 3]. Due to the extreme rarity of MCS, no formal grading system has been suggested. In a single institute study of 50 cases of malignant adnexal tumors, less than half of the cases were assigned histological grade, and grade was not found to be predictive of overall survival rate [8].
Although there are no immunohistochemical stains specific to MCS, the use of some stains may help confirm the biphasic/mixed differentiation of these lesions and to rule out metastasis [1, 6]. The epithelial component stains positive for cytokeratins including CK5/6, EMA, CEA (glandular differentiation), and p63 (myoepithelial or squamous differentiation) [6]. Our case demonstrated positivity for both high molecular weight (CK5/6, 34BE12) and low molecular weight (CK7, CAM5.2) cytokeratins as well as p63. The mesenchymal chondroid differentiation areas show S-100 and vimentin positivity as expected to occur in chondroid differentiation of other malignancies such as metaplastic carcinoma of breast [12]. Other site specific immunostains can be performed to rule out metastasis as has been widely discussed in reviews of utility of immunohistochemistry in unknown primary, although there may be some overlap with immunophenotype of salivary gland and mammary tumors [13].
Histological differential diagnosis includes primary cutaneous carcinosarcoma, a term which encompasses any biphasic malignant tumors arising within the context of other adnexal neoplasms, such as eccrine porocarcinoma, malignant cylindroma, malignant spiradenoma, and pilomatrical carcinosarcoma [6]. The current World Health Organization (WHO) classification emphasized the need of some benign chondroid syringoma like areas to confirm the diagnosis of MCS and to avoid using overlapping terms like cutaneous carcinosarcoma, when distinctive benign adnexal tumor is seen in the background [7]. Other differential diagnosis includes a BCS, a direct extension and/or metastasis of another malignant biphasic lesion such as malignant pleomorphic adenoma or metaplastic carcinoma of the breast. Careful histopathological examination in the view of clinical history can usually help in reaching a definitive diagnosis, although this may be difficult on small/partial biopsies [3].
The clinical course of MCS has been considered unpredictable, although based on the current literature it appears to be quite an aggressive malignancy. About 50% show local recurrence, up to 62% show nodal and distant metastasis and about 27% patients die of advanced
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 5
metastatic disease [2, 4]. The most common site for distal metastasis is lung, followed by the bone and brain [4]. Local bone invasion has also been reported [14]. Death occurred as early as 9 weeks following surgery to about 12 years after diagnosis [11, 15].
Surgical excision is the mainstay of treatment for MCS. Although tissue conservation surgical technique such as Moh’s micrographic surgery has been recently proposed to be adequate treatment of this lesion on the face, most authors seem to be of the opinion that wide local surgical excision, or staged margin-controlled excision be preferred in these highly malignant lesions [1, 4]. Various chemotherapy protocols with or without radiotherapy have been administered to patients without significant response. Close follow-up is mandatory for early detection of local recurrence or metastasis [4]. A sentinel lymph node biopsy may also be offered to the patients with MCS, especially with the presence of high-risk features such as large amount of mucoid matrix, malignant chondroid differentiation, or extensive lymphovascular invasion [8]. Further accumulating literature may help to delineate better prognostic characterization and treatment guidelines.
CONCLUSION
Malignant chondroid syringomas are exceedingly rare tumors, but with a high incidence of recurrence, metastasis, and death. These cases need to be diagnosed with strict histopathological criteria and with attention paid to the amount of mucoid matrix, poor chondroid differentiation, and margin status. A wide local excision is so far the mainstay of treatment, although sentinel lymph node biopsy may be considered as part of a comprehensive surgical management of these highly malignant tumors. Adjuvant radiotherapy and chemotherapy have not proven to be useful in preventing metastasis.
REFERENCES
1. Lal K, Morrell TJ, Cunningham M, O’Donnell P, Levin NA, Cornejo KM. A case of a malignant cutaneous mixed tumor (chondroid syringoma) of the scapula treated with staged margin-controlled excision. Am J Dermatopathol 2018;40(9):679–81.
2. Tural D, Selçukbiricik F, Günver F, Karışmaz A,Serdengecti S. Facial localization of malignant chondroid syringoma: A rare case report. Case Rep Oncol Med 2013;2013;907980.
3. Nguyen CM, Cassarino DS. Local recurrence of cutaneous mixed tumor (chondroid syringoma) as malignant mixed tumor of the thumb 20 years after initial diagnosis. J Cutan Pathol 2017;44(3):292–5.
4. Sánchez Herreros C, Belmar Flores P, De Eusebio Murillo E, Díez Recio E, Cuevas J. A case of cutaneous malignant mixed tumor treated with mohs micrographic surgery. Dermatol Surg 2011;37(2):267–70.
5. Malik R, Saxena A, Kamath N. A rare case of malignant chondroid syringoma of scalp. Indian Dermatol Online J 2013;4(3):236–8.
6. Nel CE, van der Byl D, Grayson W. Malignant chondroid syringoma: A report of two cases with a sarcomatous mesenchymal component. Dermatopathology (Basel) 2019;6(2):77–84.
7. Kazakov DV, Argenyi ZB, Brenn T, et al. Malignant mixed tumour. In: Elder DE, Massi D, Scolyer RA, Willemze R, editors. World Health Organization Classification of Tumours. WHO Classification of Skin Tumours. 4ed. Lyon: IARC Press; 2018. p. 163.
8. Oyasiji T, Tan W, Kane J 3rd, et al. Malignant adnexal tumors of the skin: A single institution experience. World J Surg Oncol 2018;16(1):99.
9. Mathiasen RA, Rasgon BM, Rumore G. Malignant chondroid syringoma of the face: A first reported case. Otolaryngol Head Neck Surg 2005;133(2):305–7.
10. Krishnamurthy A, Aggarwal N, Deen S, Majhi U, Ramshankar V. Malignant chondroid syringoma of the pinna. Indian J Nucl Med 2015;30(4):334–7.
11. Barnett MD, Wallack MK, Zuretti A, Mesia L, Emery RS, Berson AM. Recurrent malignant chondroid syringoma of the foot: A case report and review of the literature. Am J Clin Oncol 2000;23(3):227–32.
12. Bhosale SJ, Kshirsagar AY, Sulhyan SR, Sulhyan SR, Jagtap SV. Matrix-producing metaplastic breast carcinoma – a rare malignancy. Am J Case Rep 2013;14:213–5.
13. Kandalaft PL, Gown AM. Practical applications in immunohistochemistry: Carcinomas of unknown primary site. Arch Pathol Lab Med 2016;140(6):508–23.
14. Menéndez RH, Erice SG, Bas CA, Casas G, Dillon HS. Spinal cord compression secondary to metastasis of malignant chondroid syringoma: Case report. J Neurosurg Spine 2015;22(3):310–3.
15. Watarai A, Amoh Y, Aki R, Takasu H, Katsuoka K. Malignant chondroid syringoma: Report of a case with lymph node metastasis 12 years after local excision. Dermatol Online J 2011;17(9):5.
*********
Author ContributionsPooja Vasudev – Conception of the work, Design of the work, Acquisition of data, Analysis of data, Interpretation of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Gabriela Gohla – Conception of the work, Design of the work, Acquisition of data, Analysis of data, Interpretation of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Journal of Case Reports and Images in Pathology, Vol. 6, 2020.
J Case Rep Images Pathol 2020;6:100046Z11PV2020. www.ijcripathology.com
Vasudev et al. 6
Samih Salama – Conception of the work, Design of the work, Acquisition of data, Analysis of data, Interpretation of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Salem Alowami – Conception of the work, Design of the work, Acquisition of data, Analysis of data, Interpretation of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone.
Consent StatementThis case does not use any specific patient identifiers, and the pictures are of microscopic histology and immunohistochemistry that cannot be used for patient identification purposes. In the department of pathology, we do not directly interact with patients, but all efforts have been made in great detail to anonymize the case as much as possible.
Conflict of InterestAuthors declare no conflict of interest.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.