119
MANAGEMENT OF HIGH GRADE BRAIN TUMORS Dr. Abhilash G JR-2 Radiotherapy SRMSIMS
| Date post: | 07-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | abhilash-gavarraju |
| View: | 68 times |
| Download: | 4 times |

MANAGEMENT OF HIGH GRADE BRAIN TUMORS
Dr. Abhilash G JR-2 Radiotherapy SRMSIMS
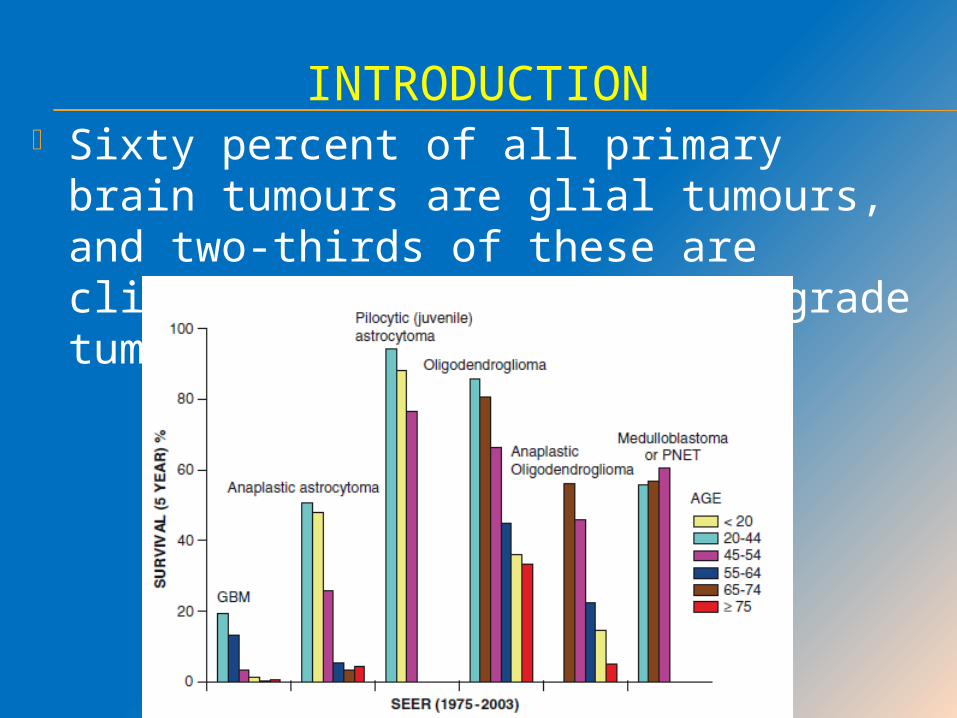
INTRODUCTION Sixty percent of all primary brain
tumours are glial tumours, and two-thirds of these are clinically aggressive, high-grade tumours.
The treatment of high-grade gliomas involves the multimodality approach of surgery, RT, and chemotherapy.
In general, for GBMs, all three modalities are used at initial diagnosis. For other high-grade gliomas, the sequencing of these modalities remains controversial.
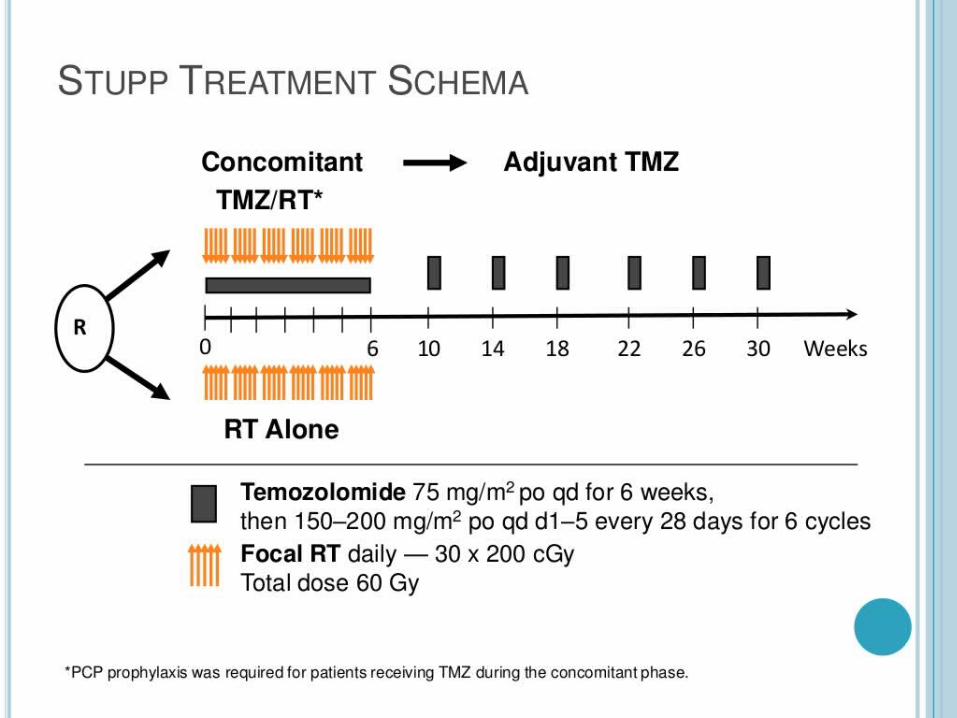
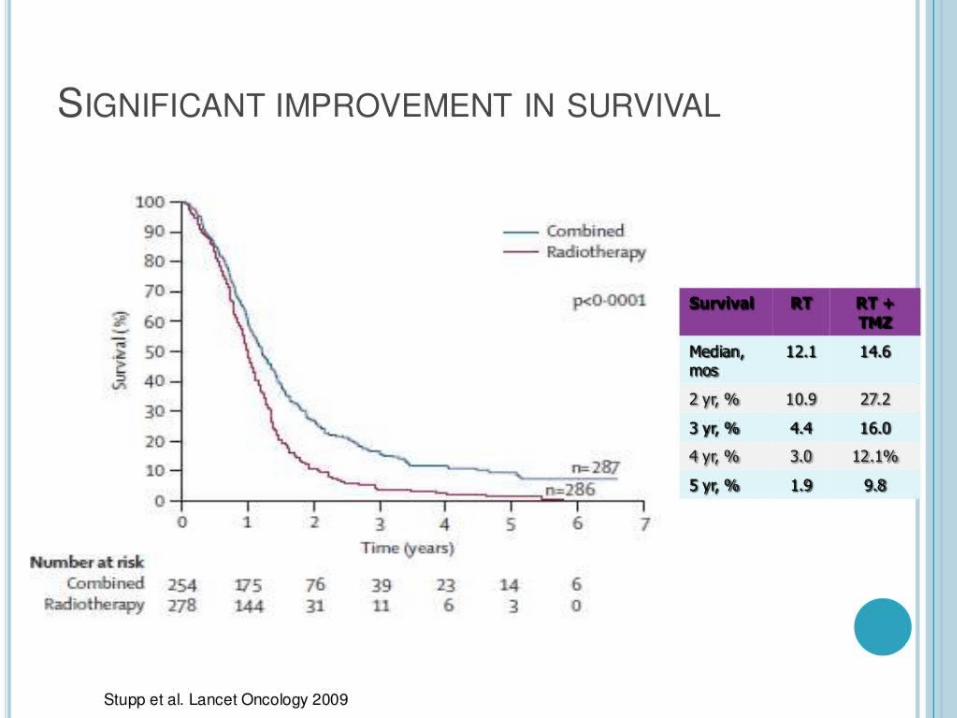
Standard treatment consists of maximal safe surgical resection followed by radiotherapy with concurrent temozolomide chemotherapy and subsequent adjuvant temozolomide chemotherapy.
GLIOBLASTOMA MULTIFORMAE
(GBM)

INDICATIONS FOR SURGERY
Biopsy for diagnosis Resection with definitive intent Palliative debulking for management of
mass Shunting to relieve symptoms caused
by increased intracranial pressure or hydrocephalus
Resection of recurrent disease in selected patients
bis-Chloronitrosourea (BCNU)-impregnated biodegradable polymer (GLIADEL wafer) may be considered for intraoperative placement if frozen section reveals high grade glioma.
INDICATIONS FOR RADIOTHERAPY
Definitive treatment (with concurrent and adjuvant chemotherapy) after resection or biopsy.
Palliative treatment to primary or metastatic foci.
RT usually started within 5 weeks of definitive resection.
RADIOTHERAPY TECHNIQUES
EBRT using Conventional RT, 3D-CRT or IMRT (WBRT or Partial Brain Irradiation)
Stereotactic radiosurgery (SRS) Fractionated Stereotactic RT (FSRT) Craniospinal Irradiation (CSI) Interstitial brachytherapy may have a
role in selected patients.
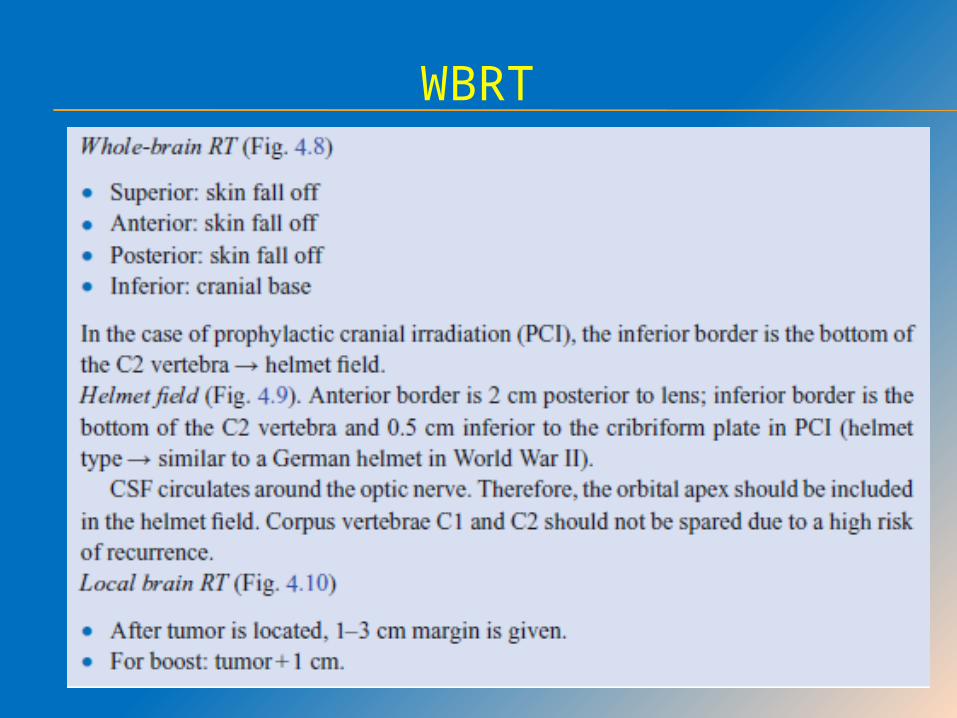
WBRT
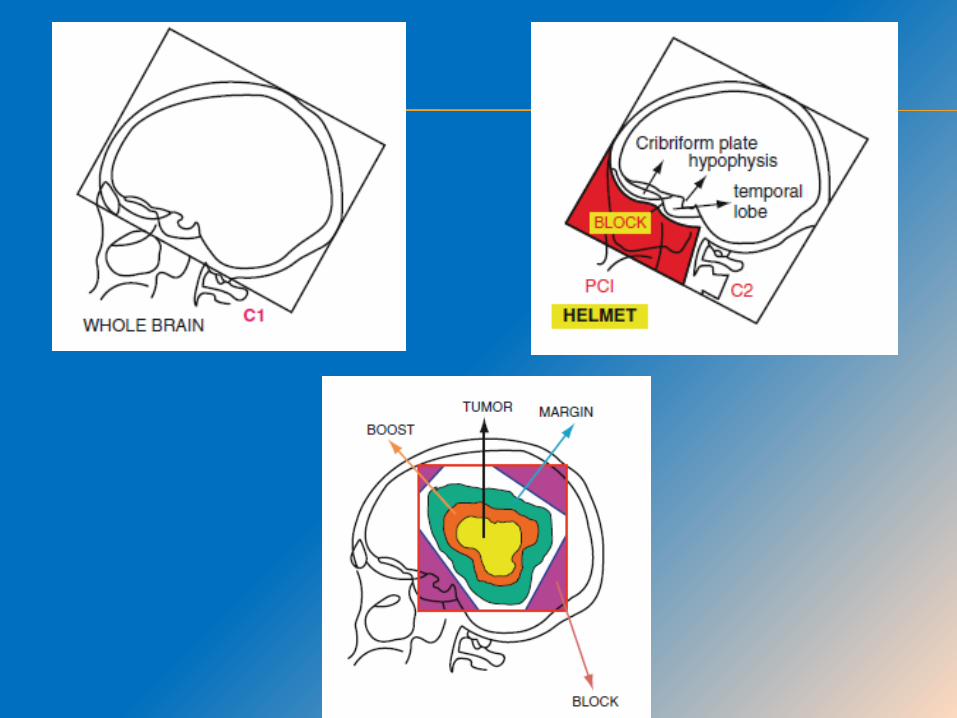
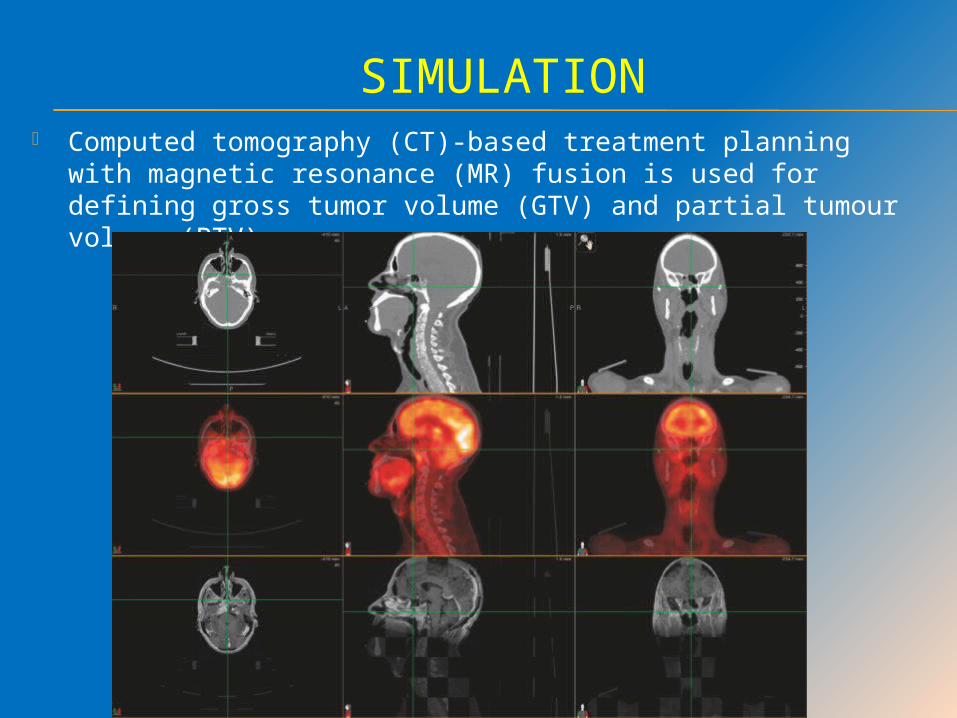
SIMULATION Computed tomography (CT)-based treatment planning with
magnetic resonance (MR) fusion is used for defining gross tumor volume (GTV) and partial tumour volume (PTV)
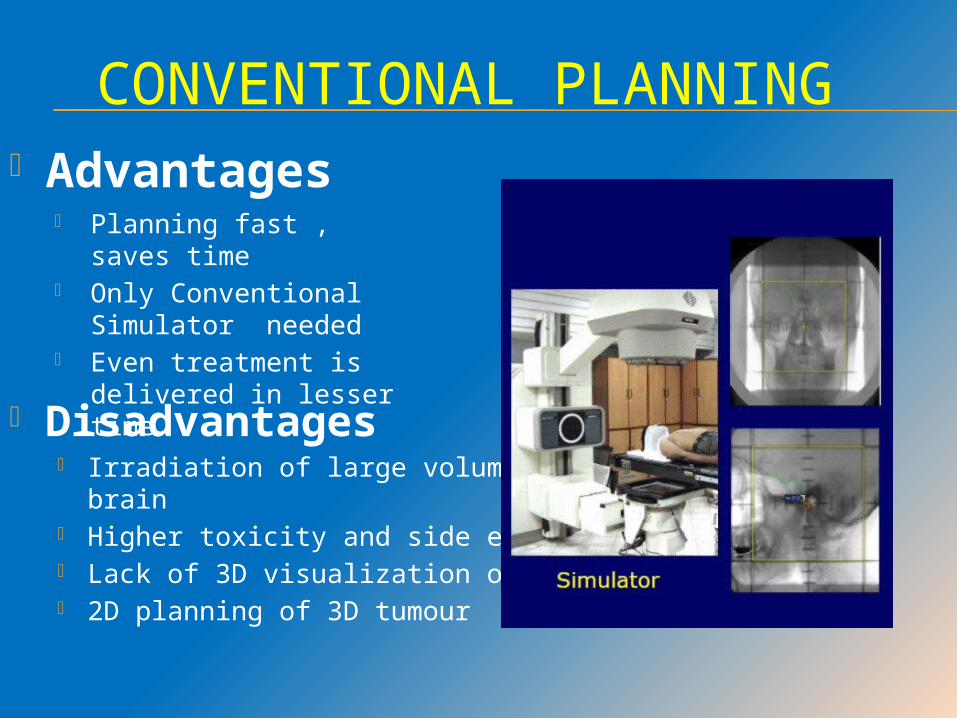
CONVENTIONAL PLANNING
Planning fast , saves time
Only Conventional Simulator needed
Even treatment is delivered in lesser time
Disadvantages Irradiation of large volumes of brain Higher toxicity and side effects Lack of 3D visualization of tumour 2D planning of 3D tumour
Advantages
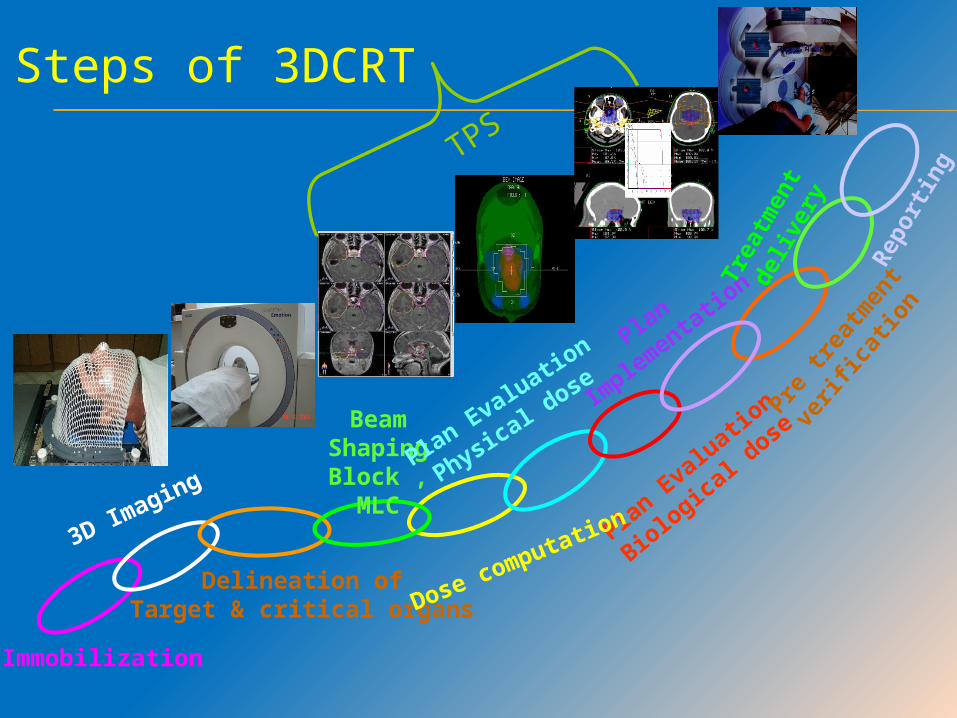
Plan Evaluation
Biological dose
Immobilization
3D Imaging
Delineation of Target & critical organs
Beam Shaping
Block , MLC
Dose computation
Plan Evaluation
Physical dose
Plan
Implementatio
n
Pre tr
eatm
ent
verif
icatio
n
Trea
tmen
t d
eliv
ery
Repo
rting
Steps of 3DCRT
TPS
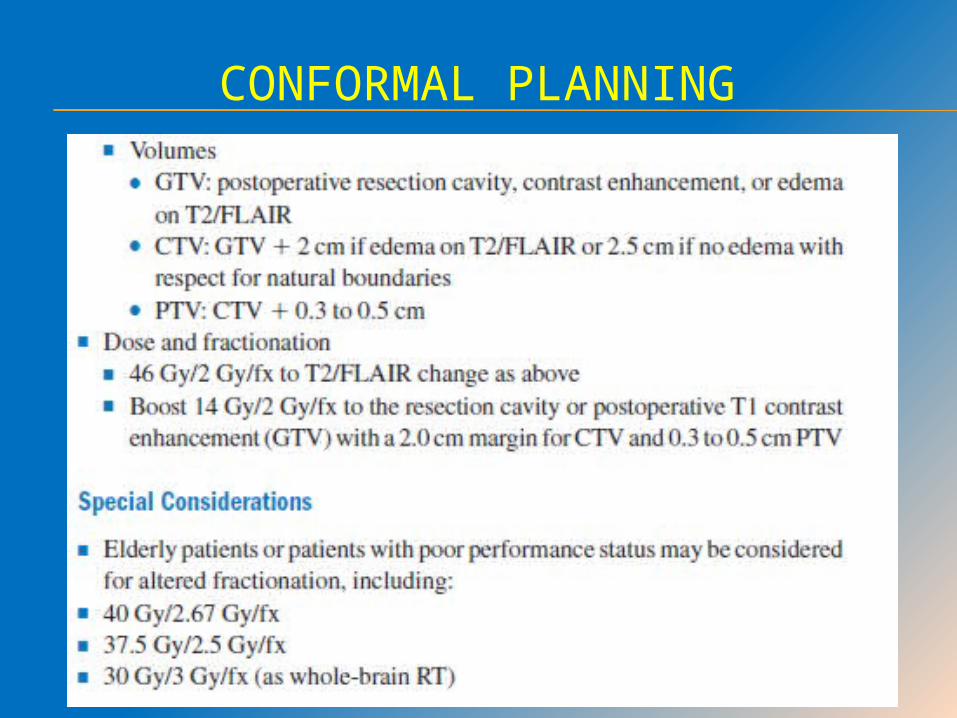
CONFORMAL PLANNING
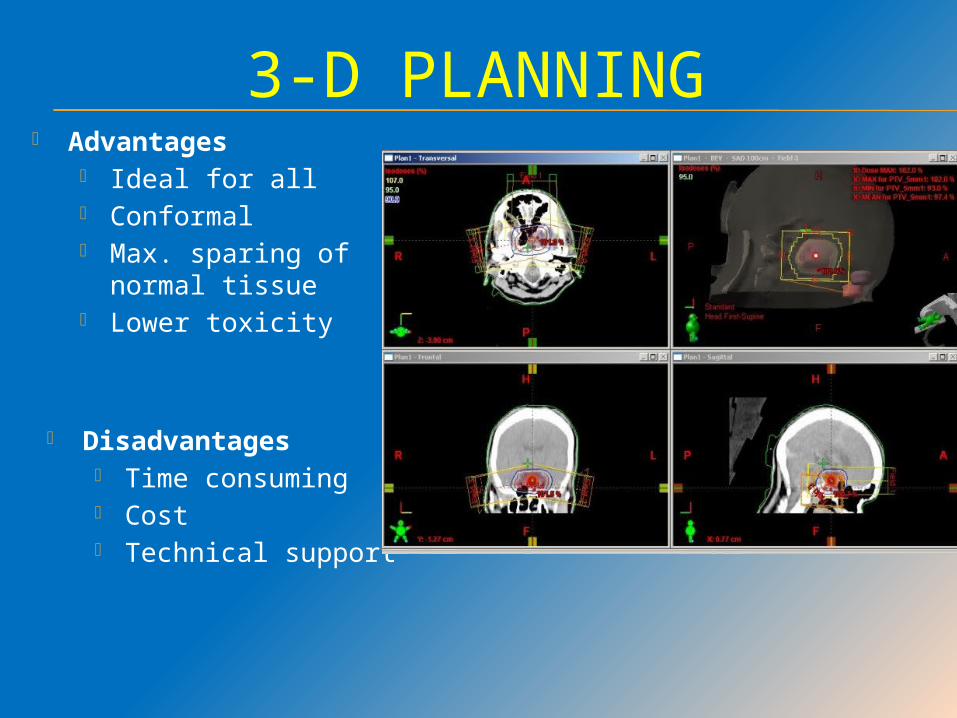
3-D PLANNING Advantages
Ideal for all Conformal Max. sparing of normal
tissue Lower toxicity
Disadvantages Time consuming Cost Technical support
FIELD ARRANGEMENTS
Treatment should be delivered with multiple fields in an attempt to achieve homogeneity throughout the volume and to spare dose to uninvolved brain.
In general, parallel opposed portals are not used; however, in cases where tumour is infiltrating across midline through corpus callosum, this may be a very reasonable field arrangement.
On-board imaging techniques with kV images or cone-beam CT can be used for daily treatment verification and setup adjustment.

NORMAL TISSUE TOLERANCE
Organs at risk (OAR) in RT of gliomas include eyes, optic nerves, optic chiasm, brainstem, cochlea, spinal cord, and perhaps the pituitary/hypothalamus.
STEREOTACTIC RADIOSURGERY (SRS)
In LINAC radiosurgery circular or oval collimators ranging from 4 to 40 mm are used to collimate the treatment beam into a circular pencil beam
Treatment is delivered using multiple noncoplanar arcs that intersect at a single point to treat an approximately spherical target of <4 cm in diameter.
Newer miniaturized multileaf collimators allow beam shaping

Radiation Therapy Oncology Group (RTOG) study 90-05
Maximum tolerated dose of single faction SRS
≤20 mm - 24 Gy 21 to 30 mm - 18 Gy 31 to 40 mm - 15Gy
FRACTIONATED STEREOTACTIC RADIOTHERAPY
For lesions larger than 4 cm and/or located in critical regions, the delivery of a single large-fraction treatment as in SRS is not desirable because of a high risk of CNS toxicity.
Reported accuracy of 1 to 3 mm.
HEAVY CHARGED PARTICLES
A small number of European and Japanese centers are treating CNS tumors with carbon ions, which putatively have higher LET and presumed superior RBE, but no substantial clinical data are available to back these claims.
Neutron-beam irradiation, with or without co administration of boronated agents to increase the cross-sectional area of interaction, continues to be used in some U.S. centers.
BRACHYTHERAPY AND RADIOCOLLOID SOLUTIONS
Selection criteria for brachytherapy include
- Tumour confined to one hemisphere, - No transcallosal or subependymal
spread, - Small size (<5 to 6 cm) - Well circumscribed on CT or MRI - Accessible location for the implant.
A balloon-based system, GliaSite placed into the cavity at the time of surgery has been employed in the treatment of recurrent malignant gliomas whose largest spatial dimension is <4 cm and are roughly spherical.
After treatment planning the balloon is filled with a liquid that contains organically bound iodine-125 (125I), and treatment is completed within 3 to 7 days.
DIRECT DELIVERY OF AGENTS
CED involves the use of intracerebrally implanted catheters to deliver a drug into the brain parenchyma or tumor at a slow but continuous rate of flow.
Examples of agents used in CED studies include viruses, paclitaxel, topotecan, and a variety of engineered, targeted protein toxins
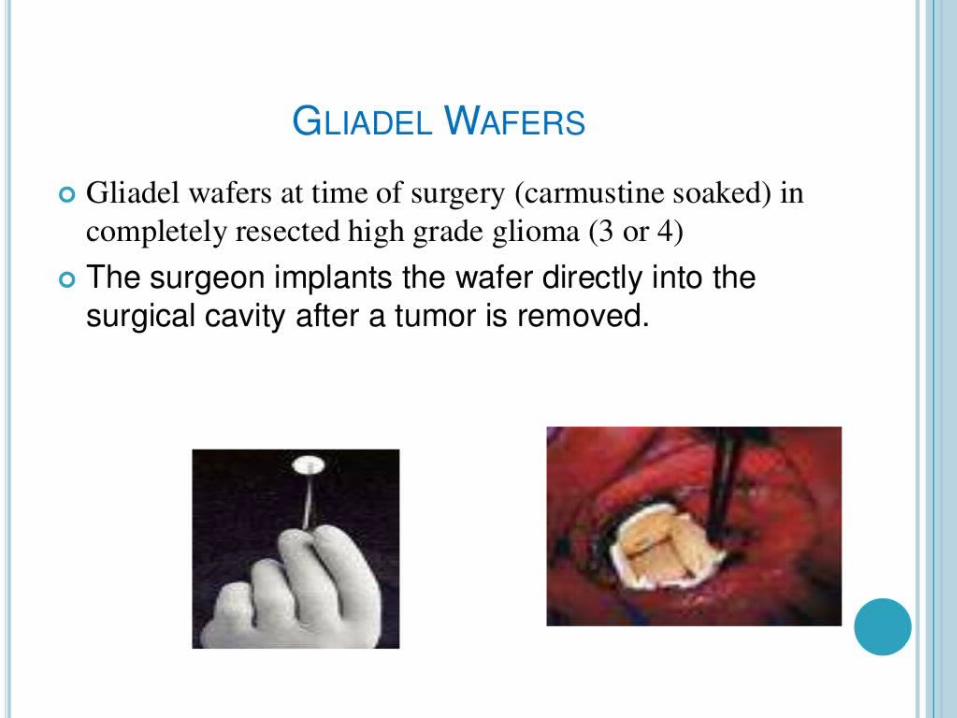
BCNU impregnated in a polymer and made into a wafer has been used for local delivery, placed on the walls of the resection cavity at the time of surgery. The wafer slowly undergoes biodegradation, releasing the active drug.
This local delivery system has the advantages of minimal systemic toxicity, no limitation posed by the BBB, and delivery of very high local concentrations of chemotherapy
RADIOTHEAPY DOSE SUMMARY Standard therapy is a total dose of 60Gy in
30-33 # A benefit for dose > 60Gy has not been
demonstrated. Dose intensification using 3D CRT or IMRT
has not shown to improve clinical outcome.
RTOG 83-02 – Hyperfractionated regimens showed no difference in medial survival.
RTOG 0023 – FSRT Dose escalation showed no survival advantage.
CHEMOTHERAPY Indications for chemotherapy - Concomitant treatment with RT - Adjuvant treatment after RT - Mainstay treatment for salvage palliative
therapy
Temozolomide, an oral alkylator that crosses the BBB, is the chemotherapy of choice in glioma, and it significantly improves treatment outcome in patients with GBM.
FDA approved carmustine and lomustine for the treatment of brain tumors in the 1970s.
The only chemotherapeutic agent that has demonstrated efficacy in a randomized, controlled clinical trials is temozolomide, an oral imidazotetrazine derivative of dacarbazine that is metabolized in vivo to an active agent.
Approval for the treatment of recurrent anaplastic astrocytoma was obtained from the FDA in 1999


Methylation of MGMT promoter improves survival following adjuvant radiotherapy plus temozolomide
MGMT methylation occurs in approximately 1/3 of patients[1]
Median survival[2]
Methylation: 22 mo No methylation: 15 mo
2-year survival[2]
Methylation: 46% No methylation: 25%
1. Rosell R, et al. Future Oncol. 2008;4:219-228. 2. Hegi M, et al. N Engl J Med. 2005;352:997-1003.
Unmethylated
Analysis of 206 GBM patients in a Phase III Study[2]
Pro
bab
ilit
y o
f O
S (
%)
100
80
60
40
20
06 12 18 24 30 36 42
Methylated114 100 59 16 7 4 192 84 64 46 24 7 1
0
No. at Risk Months
MethylatedMGMT promoter
UnmethylatedMGMT promoter
P < .00110
50
30
70
90
MGMT Methylation and OS in GBM
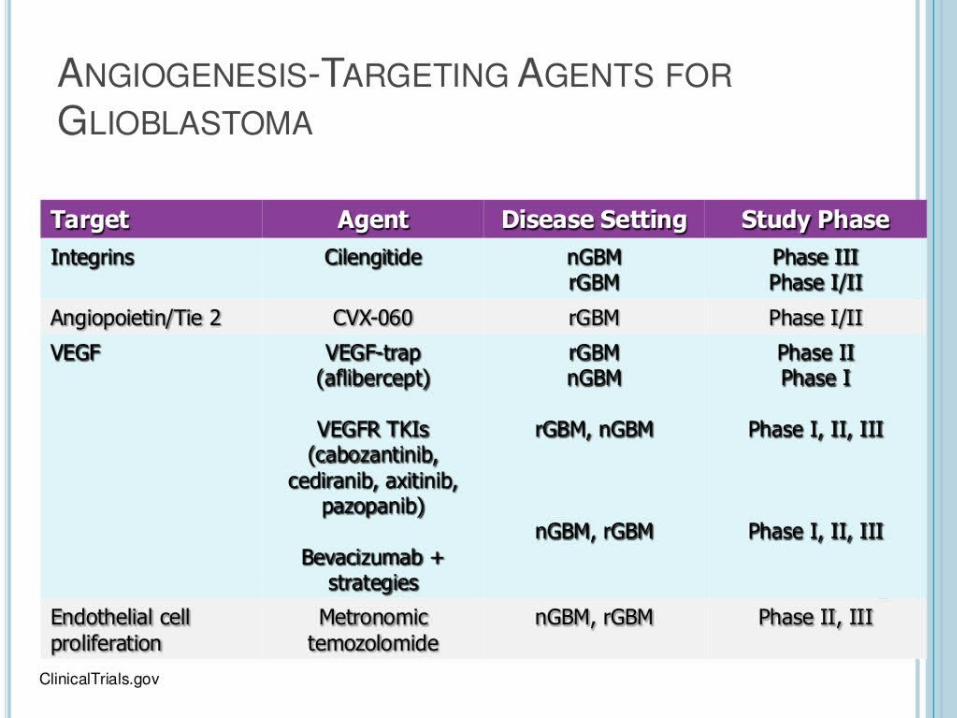
TARGETED THERAPY TKI’s - Geftinib, Nimotuzumab, Cetuximab, Lapatinib Farnesyl Protein Transferase Inhibitors - Tipifarnib, Lonafarnib mTOR Inhibitors - Everolimus, Tacrolimus Anti-angiogenesis drugs - Bevacizumab, Cediranib, Enzastaurin Peptide Vaccines - Rindopepimut (CDX-110), PEPvIII
BIOMAb EGFR as a therapy option for GBM
STUDY TITLE
An Open Label, Prospective, Multicentric Study to Evaluate the Safety and Efficacy of BIOMAb EGFR (Nimotuzumab) as Induction and Maintenance Therapy in Combination with Radiotherapy Plus Temozolomide (Concomitant & Adjuvant) in Indian Patients with Glioblastoma Multiforme
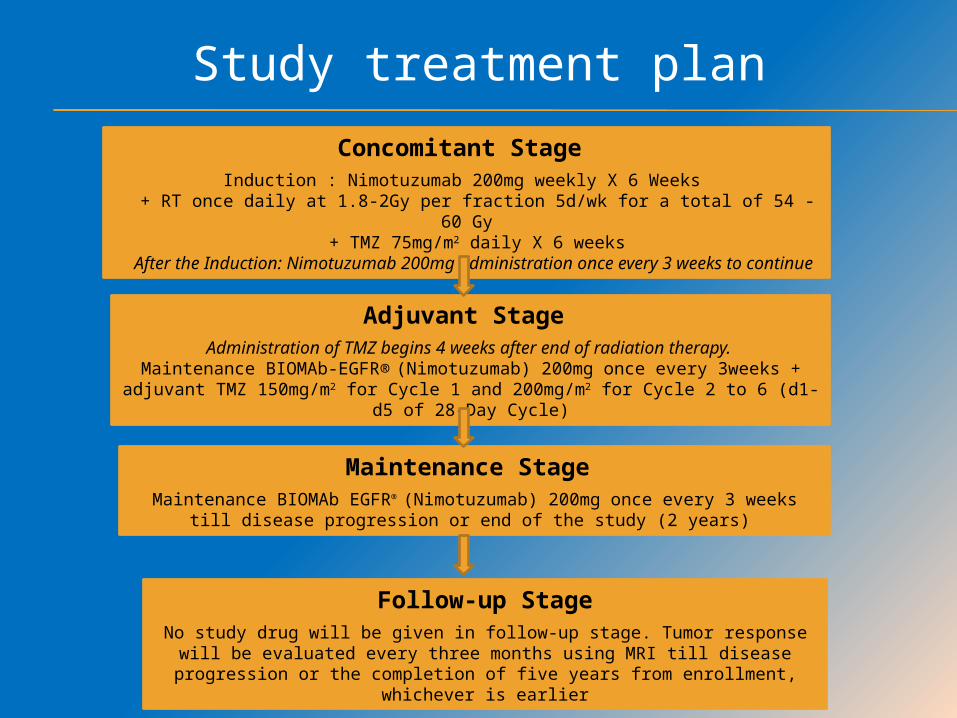
Concomitant Stage Induction : Nimotuzumab 200mg weekly X 6 Weeks
+ RT once daily at 1.8-2Gy per fraction 5d/wk for a total of 54 - 60 Gy + TMZ 75mg/m2 daily X 6 weeks
After the Induction: Nimotuzumab 200mg administration once every 3 weeks to continue
Adjuvant Stage Administration of TMZ begins 4 weeks after end of radiation therapy.
Maintenance BIOMAb-EGFR® (Nimotuzumab) 200mg once every 3weeks + adjuvant TMZ 150mg/m2 for Cycle 1 and 200mg/m2 for Cycle 2 to 6 (d1-d5 of 28-
Day Cycle)
Maintenance Stage Maintenance BIOMAb EGFR® (Nimotuzumab) 200mg once every 3 weeks till
disease progression or end of the study (2 years)
Follow-up StageNo study drug will be given in follow-up stage. Tumor response will be evaluated every three months using MRI till disease progression or the
completion of five years from enrollment, whichever is earlier
Study treatment plan
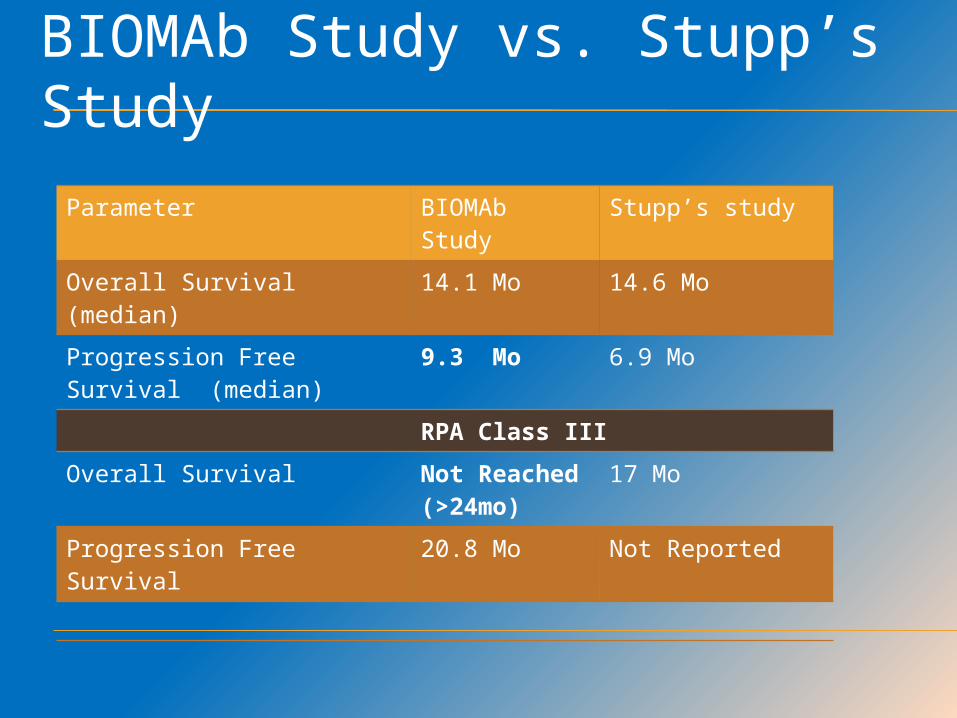
BIOMAb Study vs. Stupp’s Study
Parameter BIOMAb Study
Stupp’s study
Overall Survival (median)
14.1 Mo 14.6 Mo
Progression Free Survival (median)
9.3 Mo 6.9 Mo
RPA Class III
Overall Survival Not Reached (>24mo)
17 Mo
Progression Free Survival 20.8 Mo Not Reported
CONCLUSION
At median follow-up period of 27.1 months, Nimotuzumab in combination with TMZ and radiotherapy reported:
mOS of 14.1 months mOS observed in RPA class III and Class V were better than median
OS observed in Stupp et al., (2009) study showing a possible median survival benefit in these two RPA sub-classes III and V by the addition of Nimotuzumab
mPFS of 9.3 months, whereas it was 6.2 months in the Stupp et al., (2009) study on TMZ with radiotherapy
Nimotuzumab in combination with standard of care was well tolerated with a good safety profile
Addition of BIOMAb EGFR (Nimotuzumab) to the temozolomide based
chemoradiotherapy has an apparent progression free survival benefit and a possible overall survival benefit in RPA class III and V
without major safety concerns
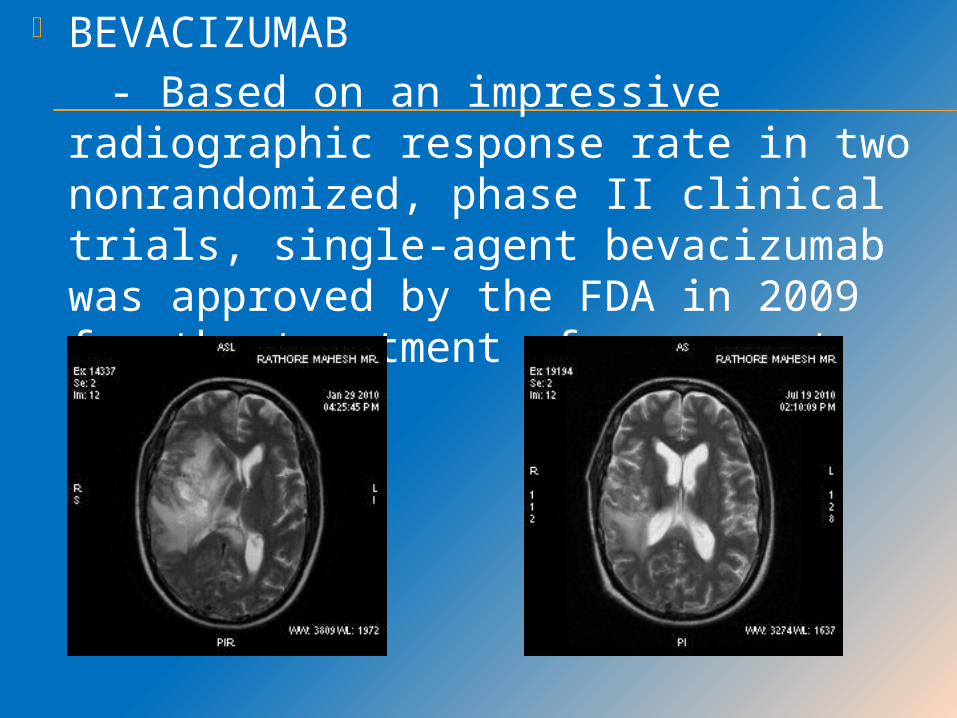
BEVACIZUMAB - Based on an impressive radiographic
response rate in two nonrandomized, phase II clinical trials, single-agent bevacizumab was approved by the FDA in 2009 for the treatment of recurrent glioblastoma
RESULTS The results of the phase III AVAglio trial were presented at the 49th
ASCO in the Central Nervous System Tumours Session by Professor Wolfgang Wick, M.D., Professor of Neurology, Chairman of the Division of Neuro-oncology at the Neurology Centre.
People who received Avastin plus radiotherapy and temozolomide chemotherapy did not have a statistically significant improvement in OS (the other co-primary endpoint), compared to those who received radiotherapy and temozolomide chemotherapy plus placebo (HR=0.88; [95% CI 0.76, 1.02], p=0.0987). Median survival was similar in both arms (16.8 months versus 16.7 months, respectively) but significant improvement in PFS (mPFS 10.6 months vs 6.2 months). Study experienced 39% reduction in the risk of disease worsening or death. Currently, AVASTIN is approved in 60 countries worldwide for treatment of progressive GBM following prior therapy. No new safety findings were observed in the AVAglio study and adverse events were consistent with those seen in previous trials.
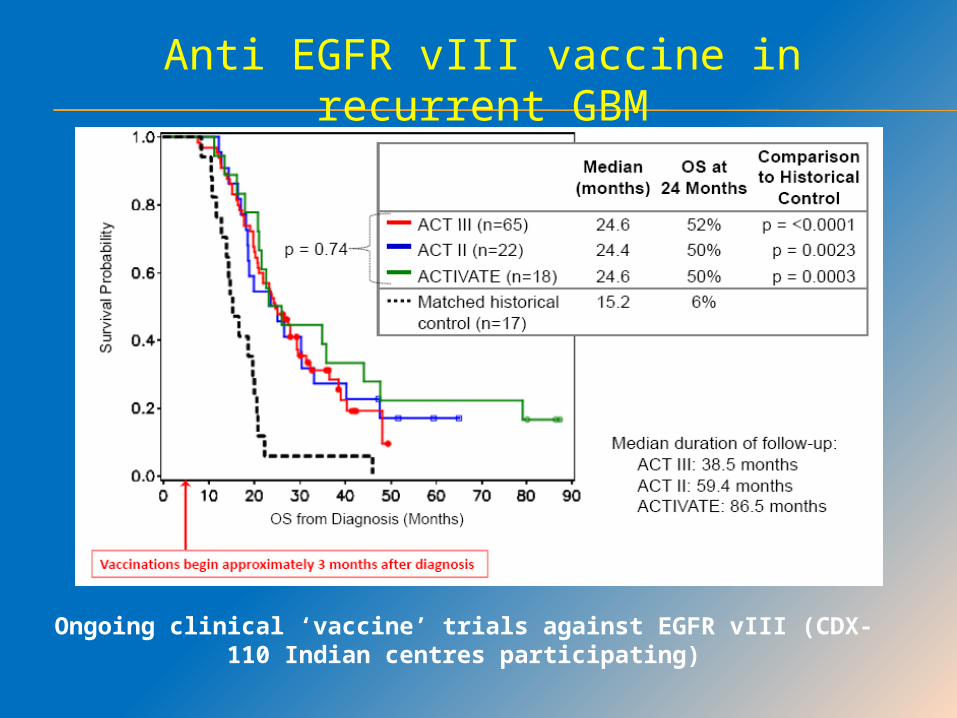
Anti EGFR vIII vaccine in recurrent GBM
Ongoing clinical ‘vaccine’ trials against EGFR vIII (CDX-110 Indian centres participating)
CLINICAL PROGNOSTIC FACTORS
Age at diagnosis (>50 yrs poor prognosis)
KPS Extent of resection Duration of symptoms Neurological status
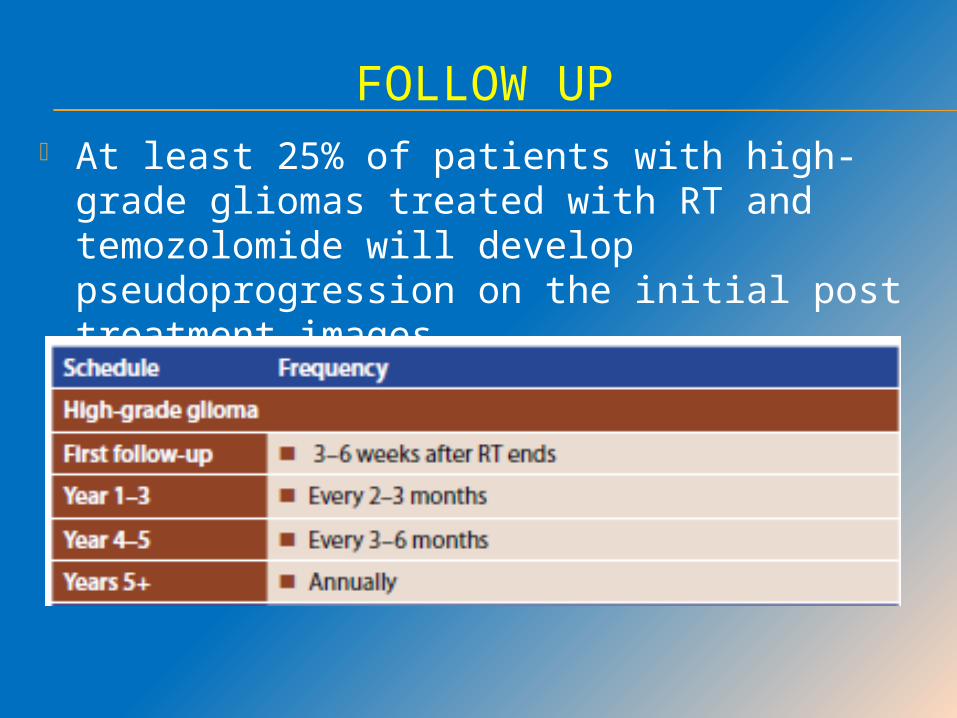
FOLLOW UP At least 25% of patients with high-grade
gliomas treated with RT and temozolomide will develop pseudoprogression on the initial post treatment images.
THE CURRENT STANDARD OF CARE FOR PATIENTS WITH ANAPLASTIC GLIOMAS IS MAXIMAL SURGICAL RESECTION FOLLOWED BY POSTOPERATIVE RADIOTHERAPY. THE RADIOTHERAPY TARGET VOLUME AND DOSE ARE THE SAME AS FOR GBM.
ANAPLASTIC GLIOMA
INTRODUCTION
WHO grade III gliomas: Anaplastic Astrocytoma Anaplastic Oligoastrocytoma Anaplastic Oligodendroglioma 25% of high-grade gliomas in adults Young to middle adulthood Without necrosis or neovascularisation
MOLECULAR GENETICS
Allelic loss of 1p and 19q is believed to be an early genetic alteration in the transformation and progression of oligodendrogliomas.
Deletions in 1p and 19p have been associated with longer PFS and chemosensitivity and radiosensitivity.
The prognosis for patients with anaplastic glioma is heavily influenced by a number of molecular genetic factors.
RTOG 94-02 – PCV f/b RT Vs RT alone - RTOG reported survival benefit from
the addition of PCV chemotherapy in the 1p19q codeleted subset with longer median survival time (8.7 vs 2.7 years)
EORTC 26951 – RT f/b PCV Vs RT alone - Patients with codeletions of 1p and 19q
had significantly longer OS irrespective of treatment, and similar to the RTOG trial
1p19q codeletion is both a prognostic and predictive marker.
MGMT PROMOTER METHYLATION MGMT promoter methylation has
demonstrated prognostic significance for anaplastic oligodendroglial tumours.
MGMT promoter methylation has not shown similar predictive significance for outcome to PCV chemotherapy in anaplastic oligodendroglial tumours.

IDH 1 MUTATION IDH1 mutations have been observed in 55%
to 80% of grade II and III gliomas. IDH1 mutations are frequently present in
secondary grade IV gliomas that develop from lower-grade tumours.
EORTC 26951 observed IDH1 mutations in 46% of patients and demonstrated prognostic significance, independent of 1p/19q codeletion, in both arms of the trial for both PFS and OS.
German Phase III trial - IDH1 mutations to be a stronger prognostic factor than 1p19q codeletion or MGMT promoter hypermethylation.
CHEMOTHERAPY Significant toxicity and only marginal
survival benefit. Use of chemotherapy - not universally
adopted Phase 3 studies are currently enrolling
patients to more clearly define the role of chemotherapy for patients with anaplastic astrocytoma, or non-codeleted anaplastic gliomas.
For codeleted subset of anaplastic gliomas, chemotherapy is now considered “standard of care.”
ADJUVANT CHEMOTHERAPY OPTIONS
Temozolomide 150-200 mg/sq.m P.O D1-5 q4w
Carmustine 150-200 mg/sq.m i.v D1 q6w
PCV q6-8 wks x 6 cycles Procarbazine – 60mg/sq.m P.O qd D8-21 Lomustine – 110 mg/sq.m P.O D1 Vincristine – 1.4-2 mg/sq.m i.v D8,29
ADULT BRAINSTEM GLIOMA
INTRODUCTION
Brainstem gliomas account for 15% of all paediatric brain tumours but are rare in adults.
DIPG – High grade astrocytomas or GBM
Focal, Dorsally exophytic or cervicomedullary – Low grade
DIPG - Most challenging Rapidly developing neurologic findings of multiple cranial
nerve palsies (most commonly VI and VII), hemiparesis, and ataxia, in combination with MRI finding of diffuse enlargement and poorly marginated T2 signal involving >50% of the pons. Most diffuse intrinsic pontine gliomas are nonenhancing
TREATMENT
Corticosteroids may be necessary to manage neurologic symptoms until treatment is instituted.
Surgery is the treatment of choice for operable lesions.
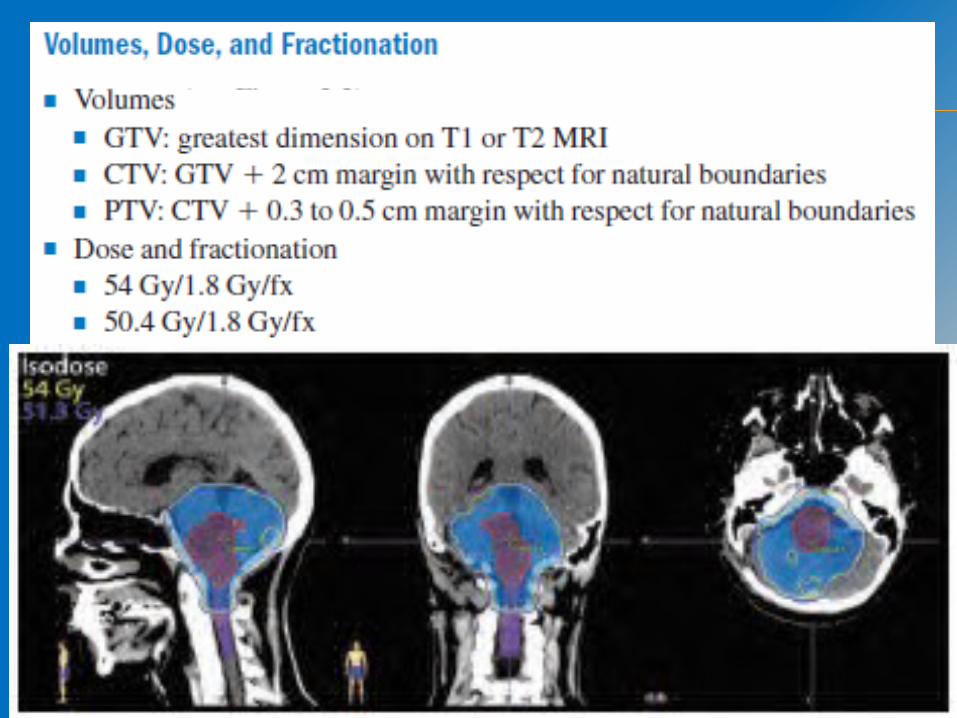
Involved field radiotherapy is the primary treatment for infiltrating pontine gliomas
55.8 to 60 Gy using daily fractions of 1.8 to 2.0 Gy per day.
Chemotherapy has no established role
MEDULLOBLASTOMA
INTRODUCTION The majority arise in the 20- to 40-year age group.
More frequently located laterally than those in childhood (50% vs. 10%), and are more frequently desmoplastic.
Homer Wright rosettes (clustered cells surrounding a central eosinophilic core) are characteristic.
CSF dissemination may manifest as positive cytology.
Systemic spread is seen in approximately 5% of patients, mostly to bone and bone marrow.

TREATMENT Complete resection if feasible.
Postoperative radiotherapy should begin within 28 to 30 days following surgical resection.
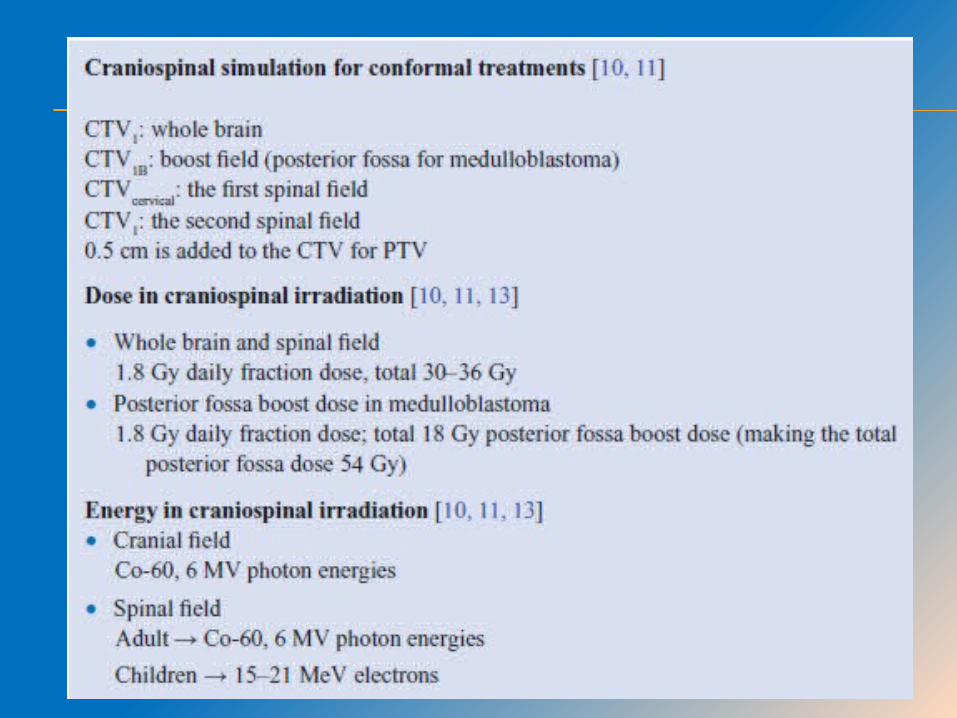
Radiotherapy is delivered to the entire craniospinal axis. This is followed by a boost to the entire posterior fossa using parallel-opposed portals or, more commonly, posterior oblique fields or other multifield techniques to spare the cochlea.
Adults treated for medulloblastoma with a mean dose to the whole brain of 35 Gy have been shown to have long-term cognitive deficits.
The total dose to the posterior fossa should be 54 to 55.8 Gy.
Immobilization & positioning of a large target area
Large & irregular shape of the clinical target volume (CTV)
Multiplicity of fields Inhomogeneity at the junctions between the
brain and spinal fields Large number of critical normal structures
having direct bearing on the late effects in these pediatric long term survivors.
CHALLENGES IN PLANNING CSI
POSITIONING
PRONE: It provides direct visualization of the
field junctions on the patient. Good alignment of the spine.SUPINE
Comfortable.Useful in anesthesia(in < 7yr age
gp)
IMMOBILIZATION Prone position of patient Arms by the side on a CSI board CSI
board(shoulders in low position if possible) Lucite base plate with a sliding
semicircular Lucite structure for head-rest & chin-rest.
Slots from A to E to allow various degrees of extension of neck
Alignment of the thoracic & lumbar spine parallel to the couch (to confirm under fluoroscopy)

RADIOTHERAPY PLANNING
Phase I Two lateral cranial fields 1 or 2 spinal fields
Phase II: Posterior fossa boost Two lateral cranial fields Conformal technique in low
risk cases.
CRITICAL ISSUES IN CSI FIELDS
• Concern 1
Divergence of the upper border of the spinal field in case of single spinal field(and interdivergence of spinal fields in case of 2 spinal fields)
• Concern 2
Divergence of both cranial fields
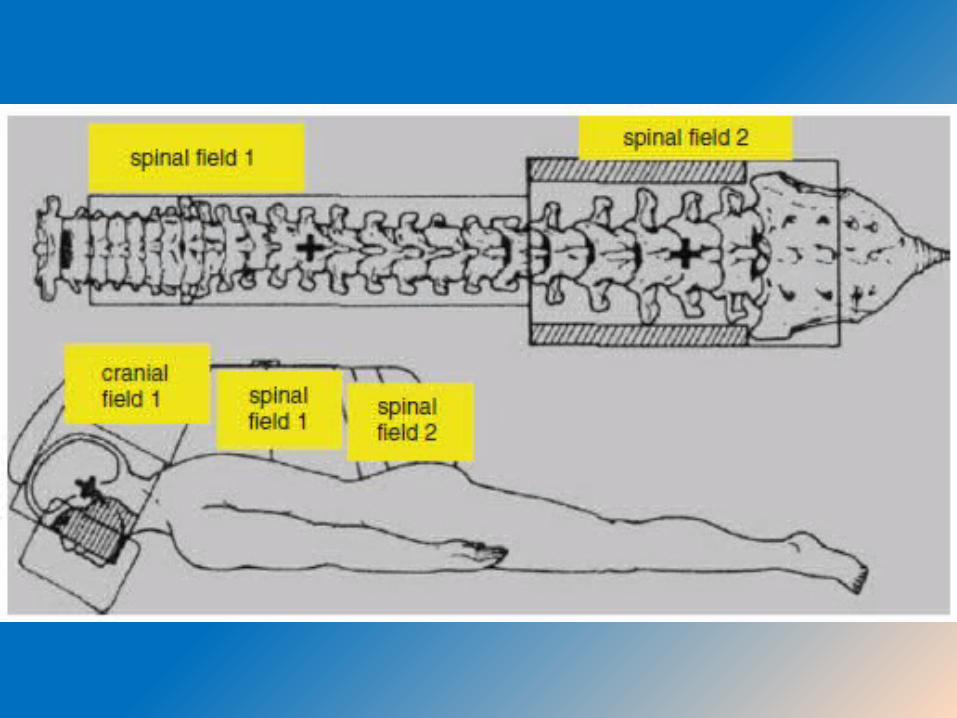
Spinal field simulated first (get to know the divergence of the spinal field)
SSD technique 2 spinal fields if the length is > 36 cm Upper border at low neck Lower border at termination of thecal sac
or S2 whichever is lower In case of 2 spinal fields , junction at
L2/L3
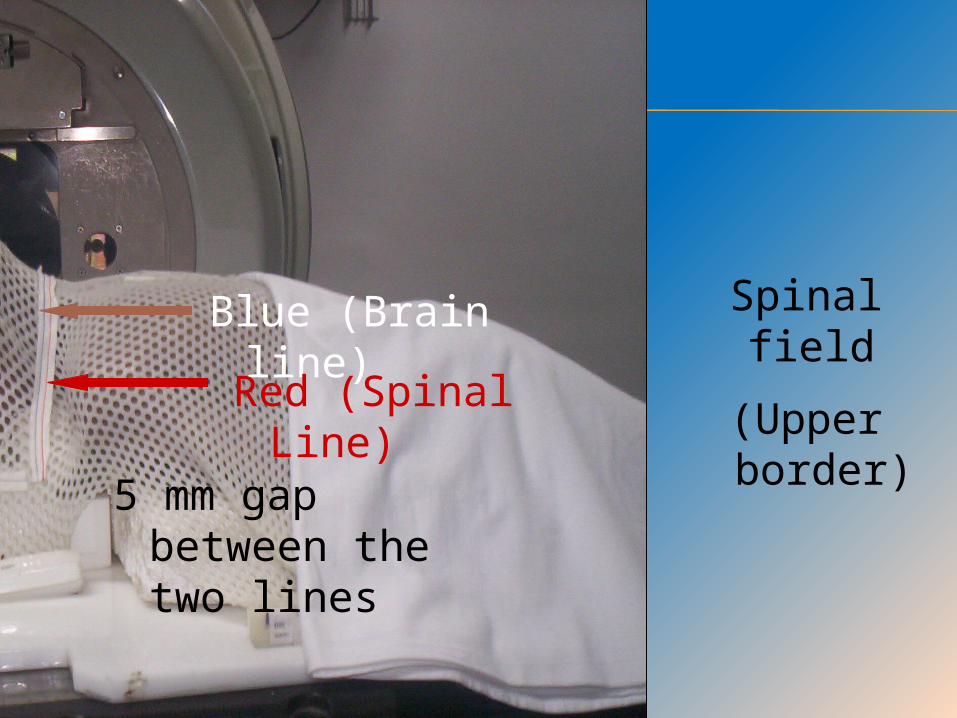
Spinal field
(Upper border)Blue (Brain line)
Red (Spinal Line)
5 mm gap between the two lines

FIXED OR CALCULATED GAPSPINAL FIELDS
Use of fixed gap ranging from < 5 mm to 10mm between fields OR
Customized gap for each patient
depending on the field length & depth of prescription, may be more appropriate
Spinal fields are simulated after gap calculation.
Width - vertebral body + 1 cm to include the intervertebral foramina, usually 5 to 7 cm.
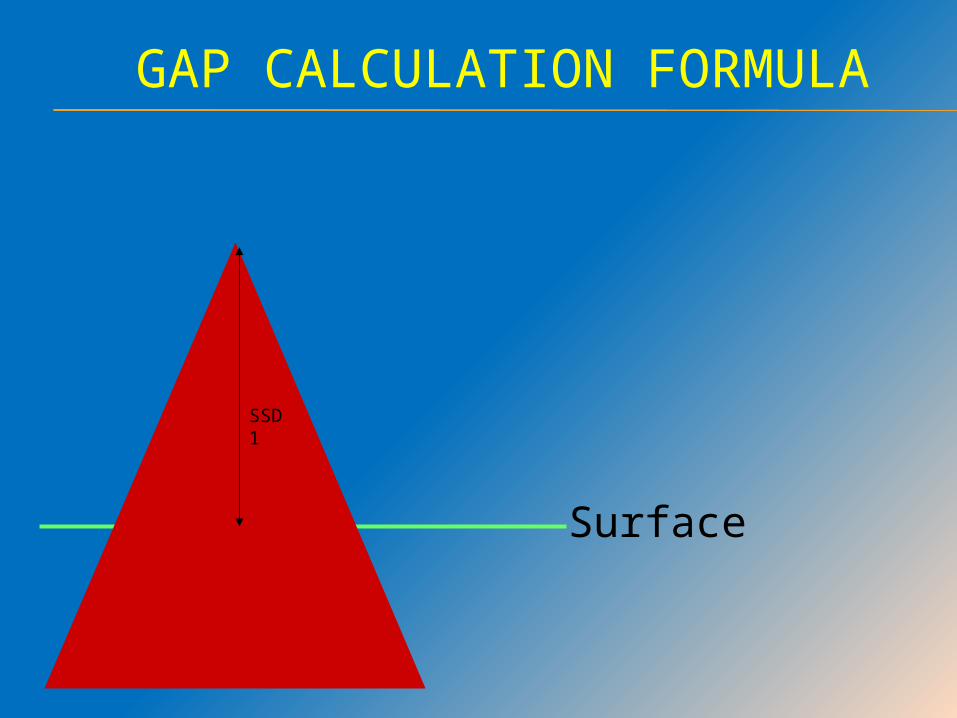
SSD 1
GAP CALCULATION FORMULA
Surface
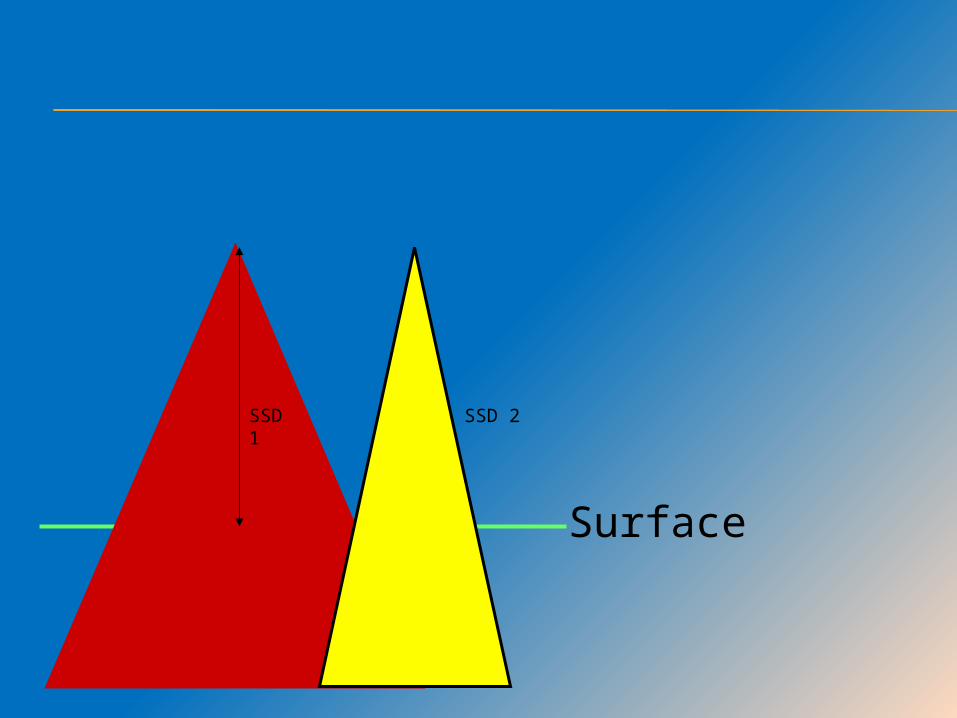
SSD 1
SSD 2
Surface
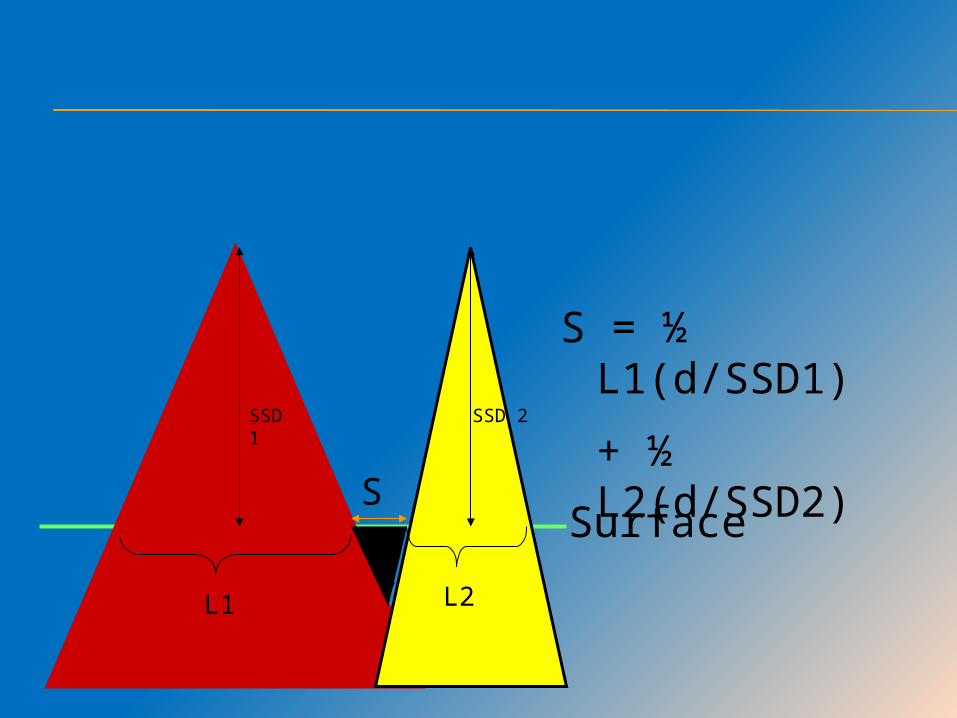
SSD 1
SSD 2
L1 L2d
S
S = ½ L1(d/SSD1)
+ ½ L2(d/SSD2)
Surface

SIMULATION-CRANIAL FIELD
Whole brain field is simulated & lower border is matched with the superior border of spinal field.
AP width & superior border include the entire skull with 2 cm clearance.
Techniques for matching craniospinal fields. Collimator/couch rotation Half beam block Asymmetric jaws Penumbra generators Wedge Tissue compensator
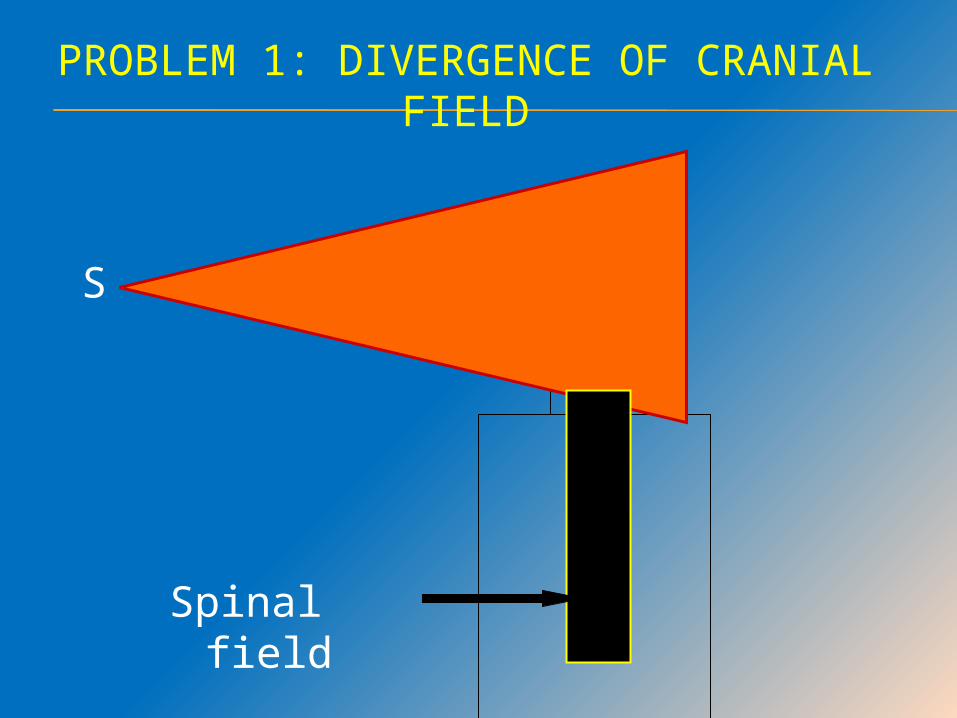
PROBLEM 1: DIVERGENCE OF CRANIAL FIELD
S
Spinal field
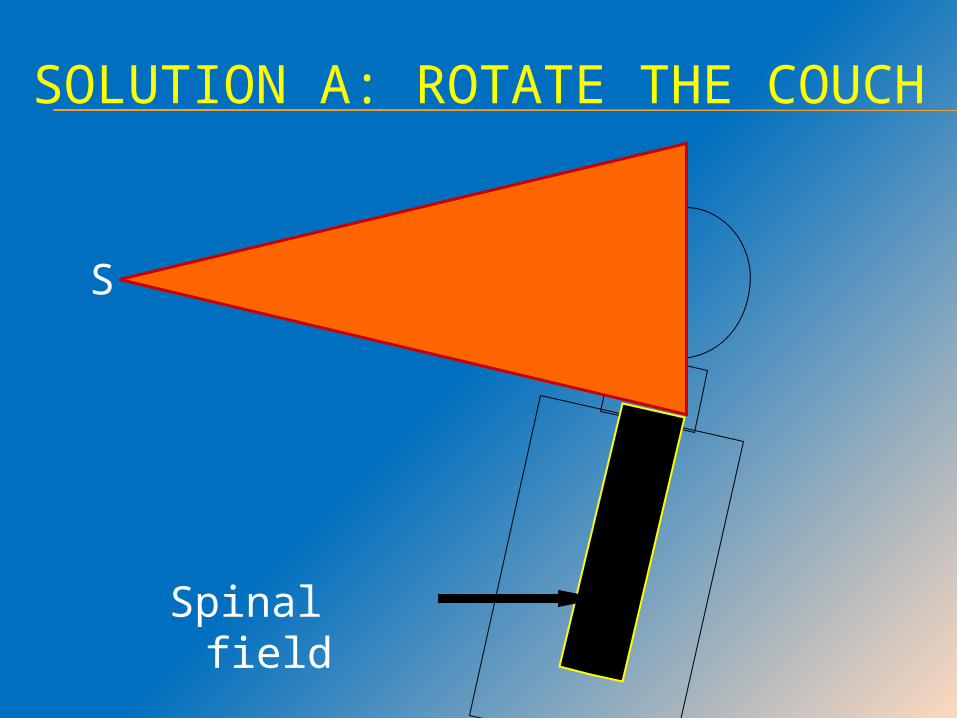
SOLUTION A: ROTATE THE COUCH
S
Spinal field
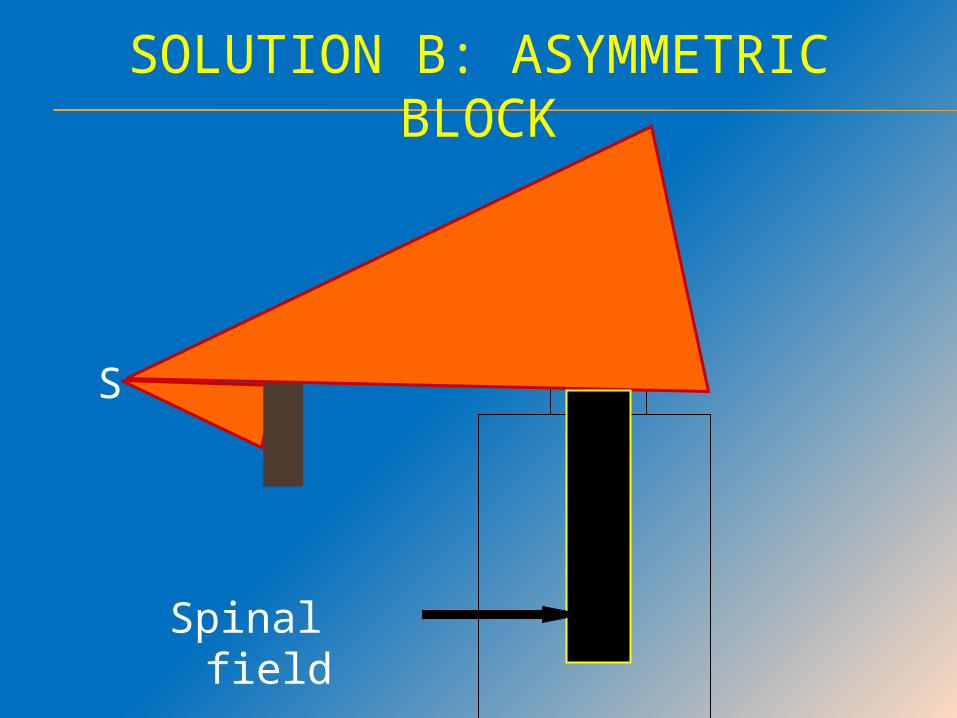
S
SOLUTION B: ASYMMETRIC BLOCK
Spinal field
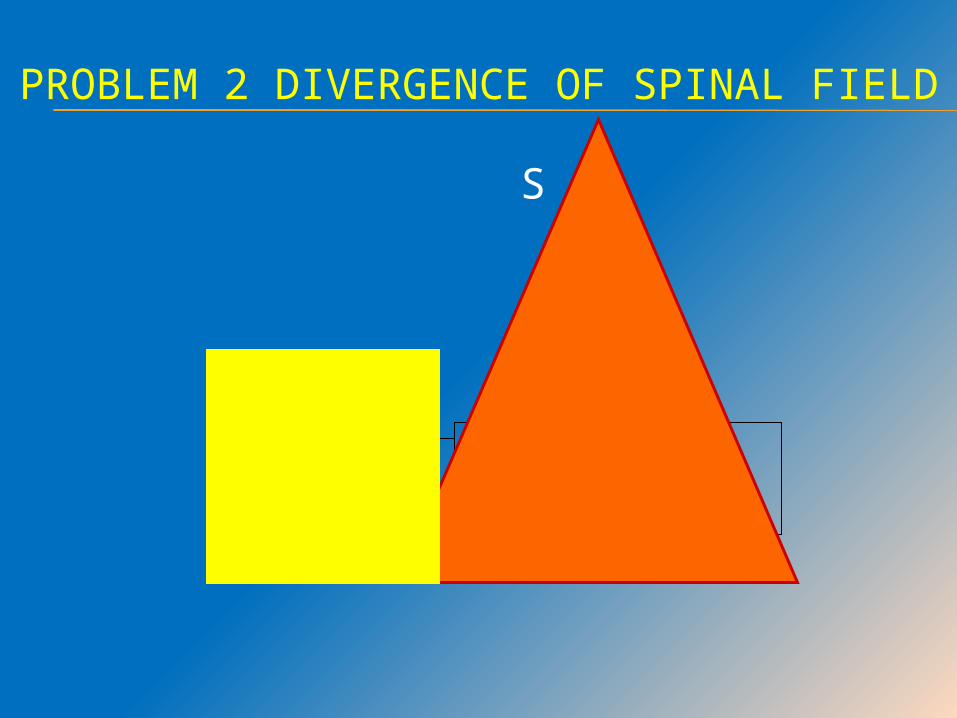
PROBLEM 2 DIVERGENCE OF SPINAL FIELD
S
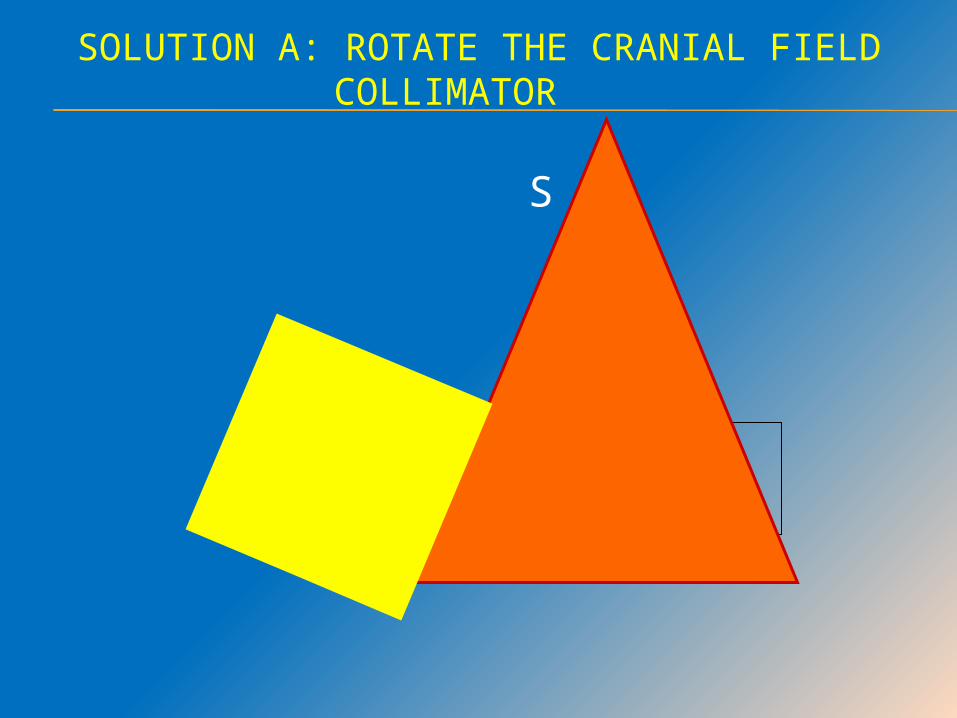
SOLUTION A: ROTATE THE CRANIAL FIELD COLLIMATOR
S

S
SOLUTION B: USE ASYMMETRIC SPINAL BLOCK
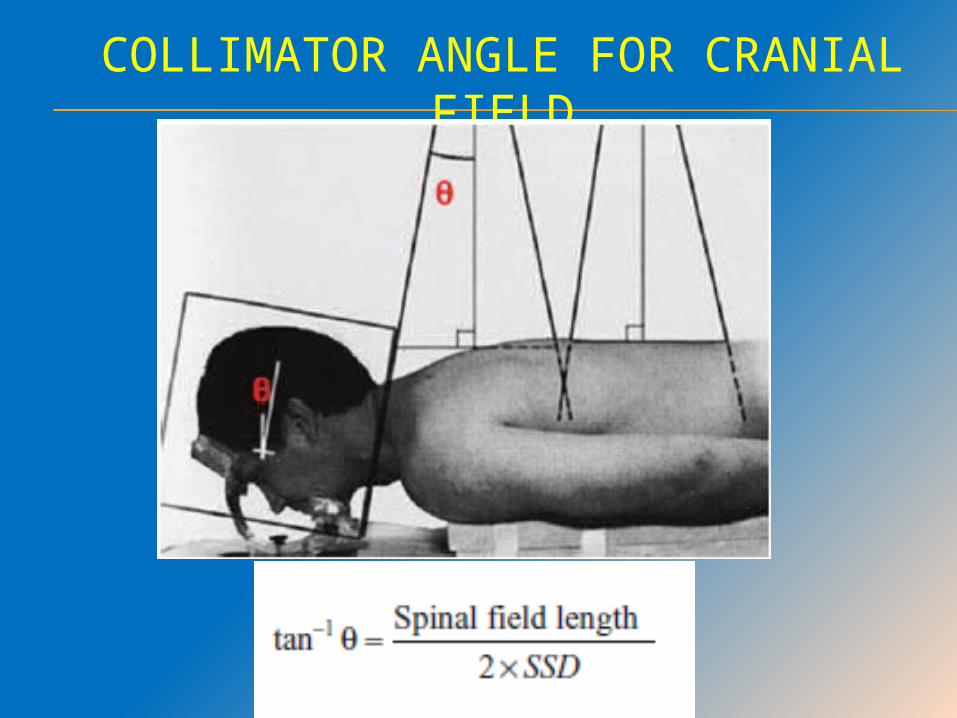
COLLIMATOR ANGLE FOR CRANIAL FIELD
SHIELDING
More important is what not to shield !
DO NOT SHIELD
Frontal (cribriform plate) Temporal region


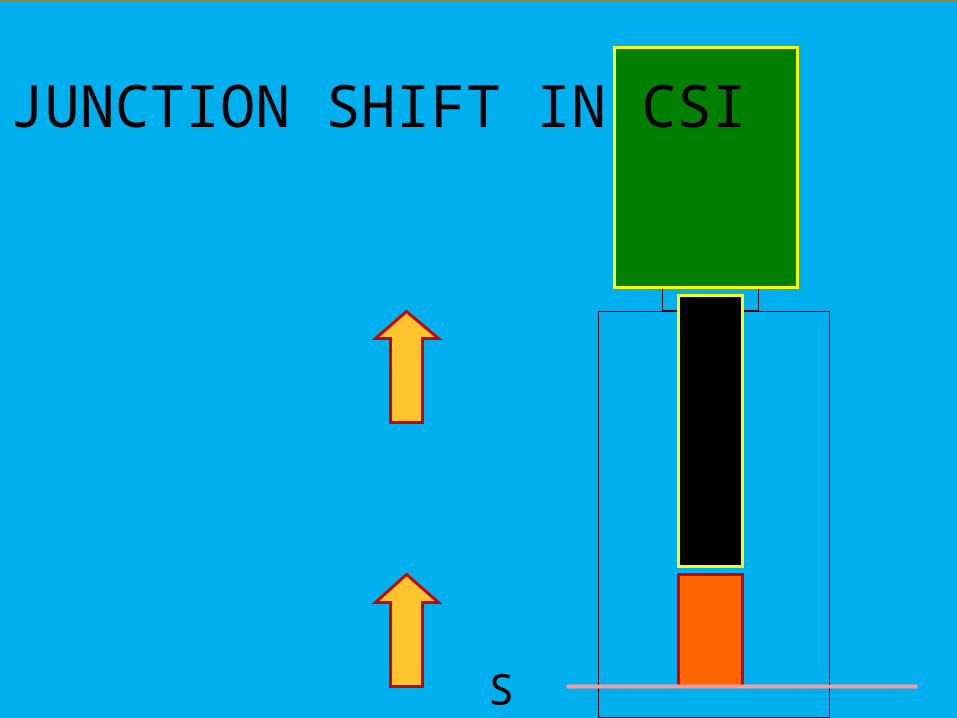
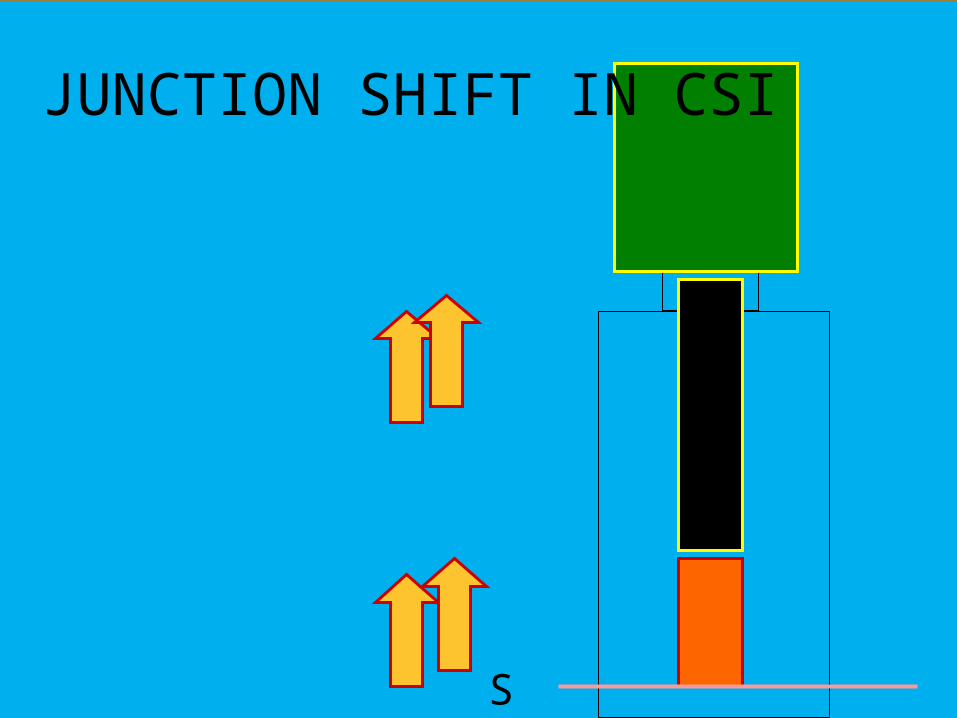
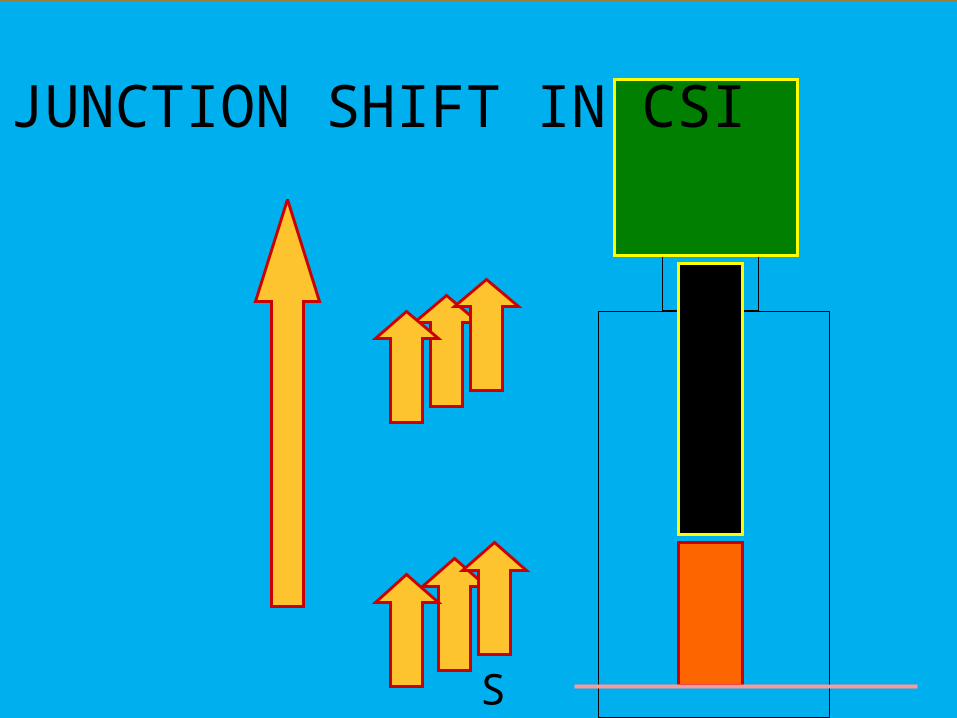
MOVING JUNCTION IN CSI 5mm overlap at 4mv photons 30 to 40%
overdose(14Gy for 36Gy prescribed dose) which may exceed cord tolerance
(Hopulka, 1993, IJROBP).
Systematic error during radiotherapy delivery could further lead to an overlap or gap.
Feathering after every 5 to 7 fraction smoothens out any overdose or underdose over a longer segment of cord.
S 2
JUNCTION SHIFT IN CSI
JUNCTION SHIFT IN CSI
S 2
S 2
JUNCTION SHIFT IN CSI
POSTERIOR FOSSA BOOSTBorders
Anterior: Posterior clinoid process. Posterior: Internal occipital protuberance. Inferior: C2-C3 interspace. Superior: Midpoint of foramen magnum &
vertex or 1 cm above the tentorium (as seen on MRI).
Field arrangement Two lateral opposing fields. 3DCRT boost to the preop tumor bed with
appropriate margins
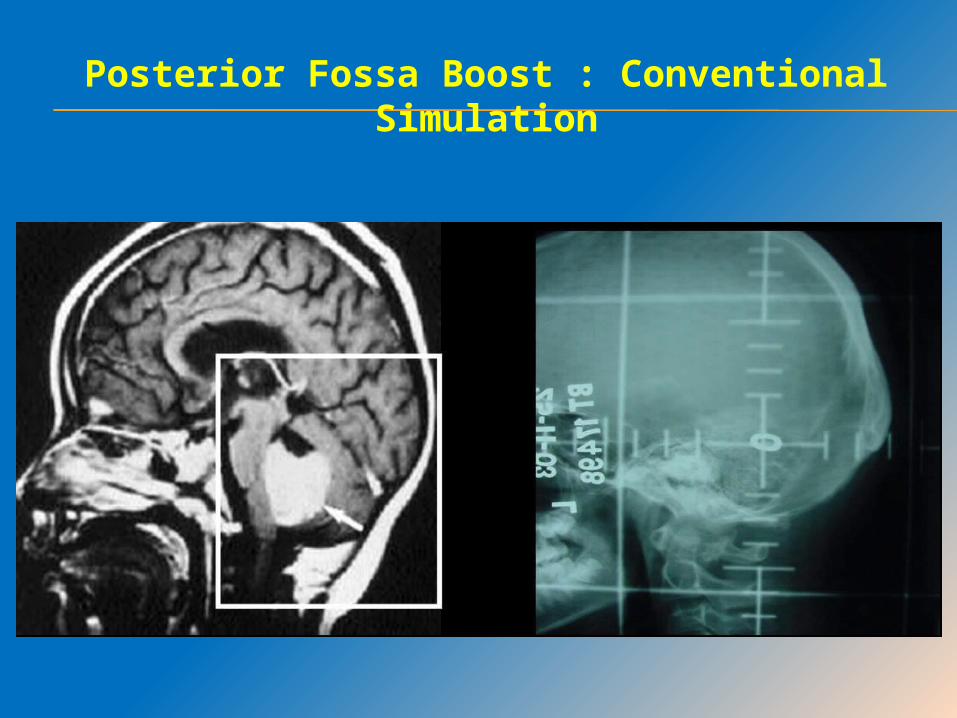
Posterior Fossa Boost : Conventional Simulation
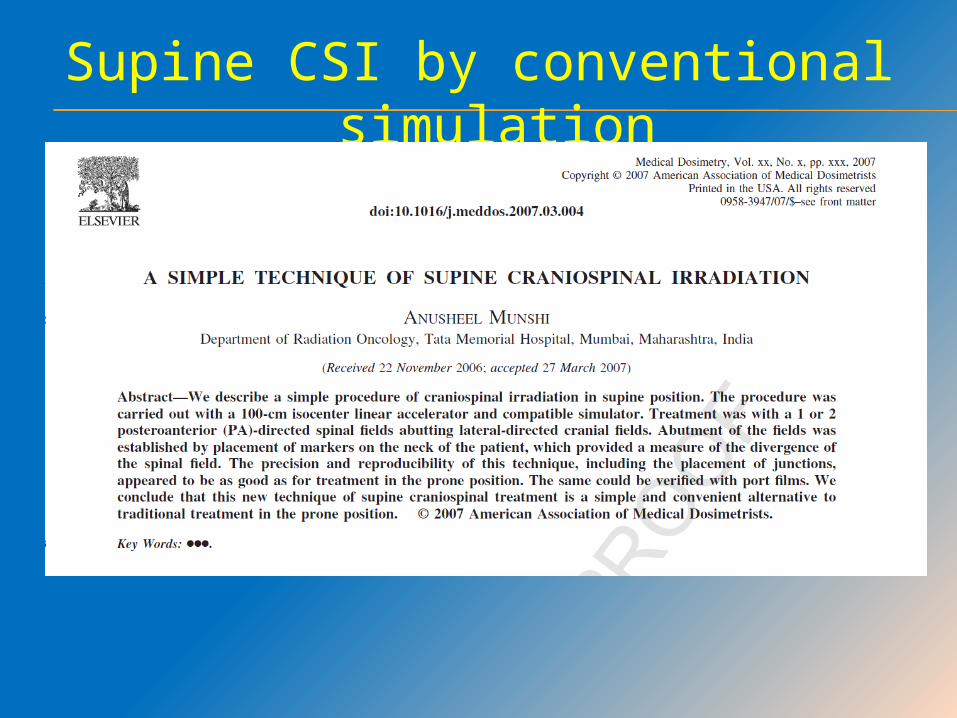
Supine CSI by conventional simulation

SUPINE CSI PLANNING - CONVENTIONAL
Positioning: Supine with arms by the side of body. Check spinal column alignment on
fluoroscopy. Neck in near neutral position but
slightly extended. Immobilization:
Thermoplastic mold for immobilization of face & neck.
Close fit at the nasion. Any constraint for the jaw is removed
to facilitate anaesthetic maneuvers.
Step 1: Two lead markers by the side of the neck at the same laser level
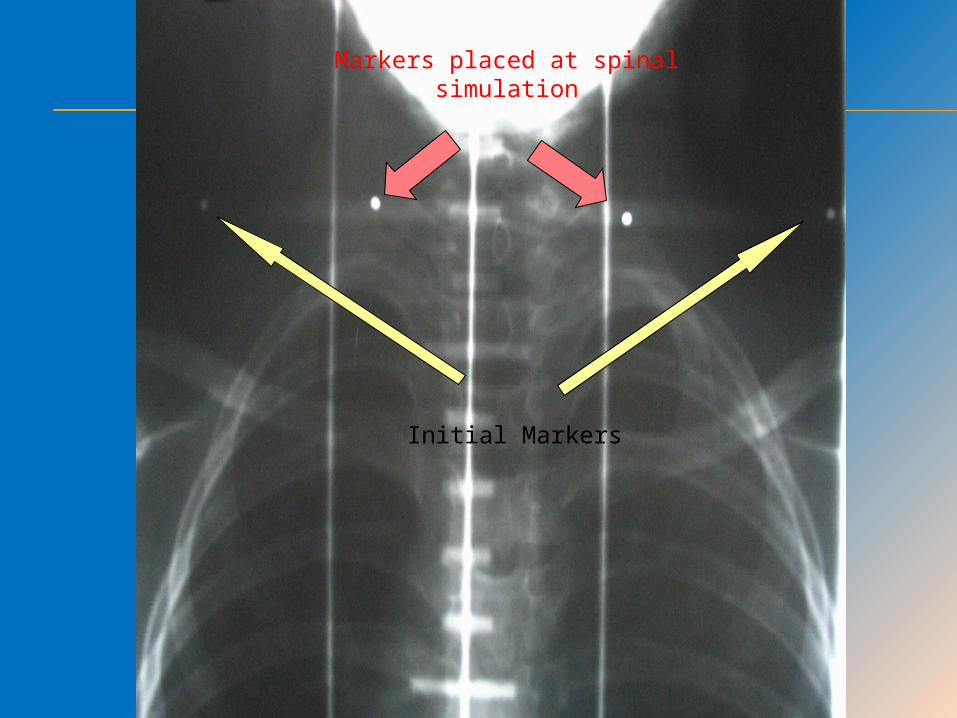
Initial Markers
Markers placed at spinal simulation
Step A : Gantry taken through table and the upper border of spinal field matched with the markers.
Step B: Two additional markers placed in the line of upper border
Step C: Collimation of the cranial field adjusted according to the line joining the two markers on one side of the neck(which is the divergence of the spinal
field)
CT basedCSI planning
(supine/prone)
STEPS IN CT SIMULATION Patient positioned using all ancillary devices and the
spinal columns aligned with the sagittal external laser.
Topogram taken to confirm spinal alignment Three-point reference marks drawn on the mask in a
transverse plane at the center of the head with the aid of the external lasers.
Two or three reference marks were placed on the posterior skin surface along the spinal column(if prone)
Spiral CT images of 3-5 mm thickness are acquired. A total of 130–170 images are reconstructed
depending on the patient’s height.
OPTIONS AFTER CT CUTS HAVE BEEN TAKEN
Virtual simulation 3 D CRT planning IMRT techniques
Dynamic IMRT Tomotherapy Volumetric Modulated arc therapy/
rotational therapies
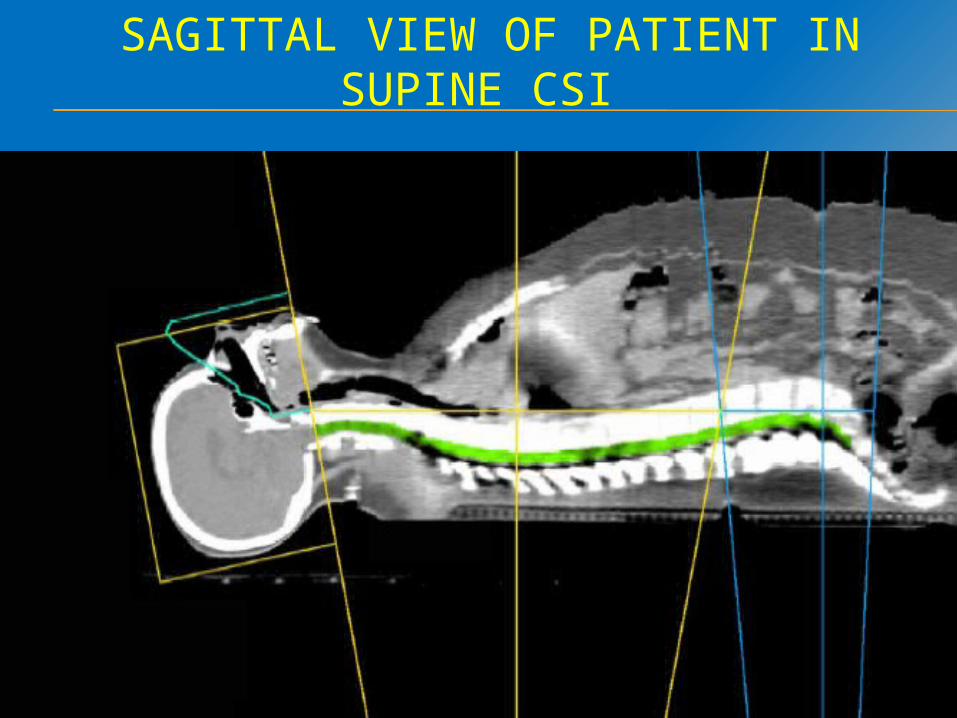
SAGITTAL VIEW OF PATIENT IN SUPINE CSI
SUMMARY
Multiple options and techniques available for treating brain tumors.
Need to use the optimum technique
Decision to be based on need of patient and available technique
CSI demands intensive planning and meticulous delivery
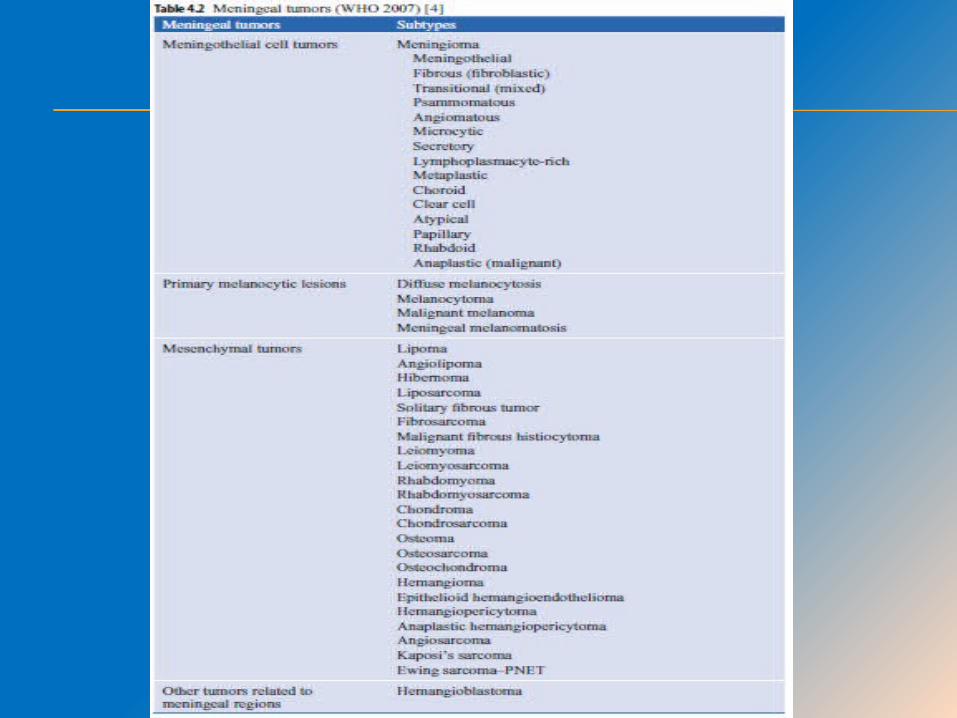
MENINGIOMA
INTRODUCTION Meningiomas account for approximately 30%
of primary intracranial neoplasms and are the most common benign intracranial tumour in adults.
The peak age of incidence is in the sixth and seventh decades. They are more common in women.
Malignant varieties with invasive growth and aggressive behaviour occasionally occur.

2007 WHO GRADING CRITERIA
Benign (78-80%) – Grade I Atypical (20%) – Grade II Anaplastic /Malignant (3-5%) – Grade III
Meningiomas are known to be induced by ionizing radiation, with an average interval to diagnosis of 19 to 35 years, depending on the dose of radiation.
They may be multiple in patients with NF2 and in non-NF2 families with a hereditary predisposition to meningioma.
The most common cytogenetic alteration in meningiomas involves a deletion of chromosome 22.
Allelic losses of chromosomal arms 6q, 9p, 10q, and 14q are seen in both atypical and anaplastic meningiomas.
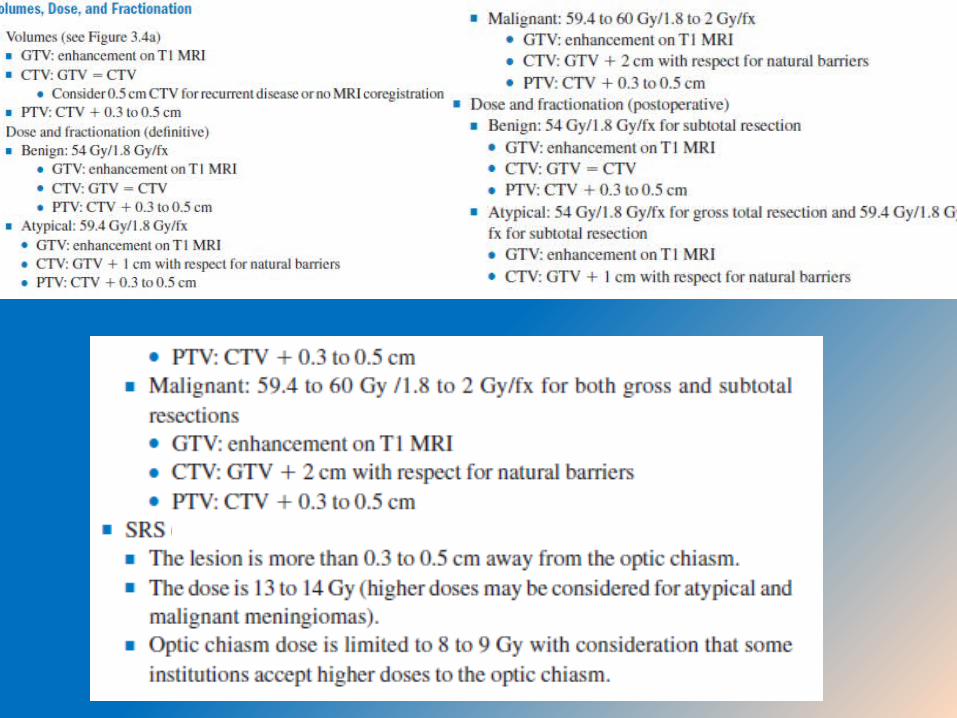
TREATMENT
GRADE III MENINGIOMAS
For atypical or malignant meningiomas, the recurrence rate after surgery alone is high (41% to 100% at 5 years), even after complete surgical resection, and postoperative irradiation after maximal resection is recommended for all patients.
Systemic therapy has no defined role. Combined chemotherapy with vincristine, Adriamycin, and cyclophosphamide has shown some efficacy in patients with malignant meningiomas.
UNRESECTABLE OR RECURRENT MENINGIOMA
In patients in whom aggressive surgery is not an option, radiotherapy may relieve symptoms and decrease the rate of tumour progression.
Various chemotherapy regimes combined doxorubicin and dacarbazine or ifosfamide and mesna.
Long-term, low-dose daily hydroxyurea may have some activity
HORMONAL MANIPULATION
Hormonal manipulation, including tamoxifen and the antiprogesterone drug RU486, showed some activity in a SWOG phase II evaluation of tamoxifen in unresectable or refractory meningiomas.
However, a subsequent SWOG phase III study of mifepristone for unresectable meningioma was negative.
EPENDYMOMA
INTRODUCTION
Ependymoma accounts for only 1.8% of all adult brain tumors.
Rosette formation is a hallmark of ependymoma on pathologic specimens.
75% of ependymomas in the adult population arise in the spinal canal and present with sensory deficits.
Occasionally disseminate through the CSF.
TREATMENT Maximal surgical resection, including second
surgery if necessary, is the initial treatment for ependymoma.
54 to 59.4 Gy are typically prescribed.
Patients with neuraxis spread (positive MRI or positive CSF cytology) should receive craniospinal irradiation (40 to 45 Gy), with boosts to the areas of gross disease and to the primary tumor to total doses of 50 to 54 Gy.
THANK YOU

















