29
MANAGEMENT OF LEUKOPLAKIA Shashank Trivedi (110301192)
| Date post: | 14-Aug-2015 |
| Category: |
Healthcare |
| Upload: | shashank-trivedi |
| View: | 44 times |
| Download: | 7 times |

MANAGEMENT OF LEUKOPLAKIA
Shashank Trivedi
(110301192)

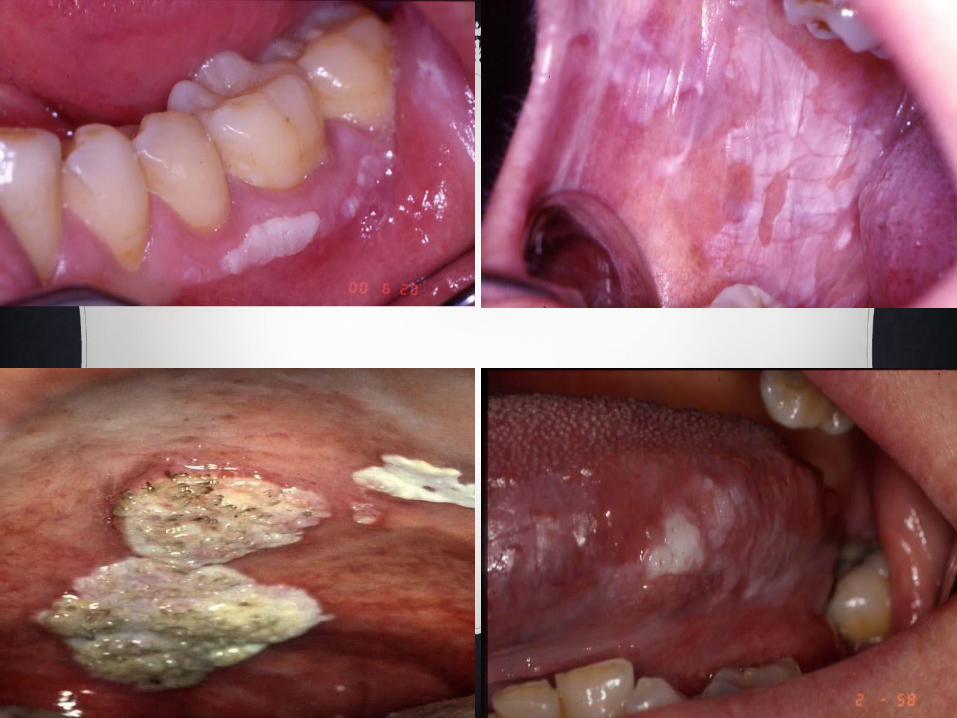
WHAT IS LEUKOPLAKIA
Leukoplakia is defined as “A
predominantly white lesion of the oral
mucosa that cannot be characterized as any
other definable lesion”.
It is the most common pre-malignant
lesion of the oral mucosa with a malignant
potential of 15.6 to 39.2%.
Extrinsic:
-Smoking
-Tobacco
-Spirit
-Sepsis(HPV/Candidiasis)
-Sunlight
-Sharp Teeth
-Spices
ETIOLOGICAL FACTORS
Intrinsic:
-Genetics
-Old Age(>45 years)
-Nutrition
-
Immunosuppression

CLINICAL PRESENTATION
Leukoplakia can be either solitary or
multiple.
Leukoplakia may appear on any site of the
oral cavity, the most common sites being:
buccal mucosa, alveolar mucosa, floor of the
mouth, tongue, lips and palate.
Classically two clinical types of
leukoplakia are recognised: homogeneous
and non-homogeneous, which can co-exist.

INVESTIGATIONS
TOLUIDINE BLUE STAINING
Toluidine blue clinically stains malignant lesions,but not
normal mucosa.The dye is taken up by the nuclei of
malignant cells manifesting increased DNA sysnthesis.
It serves as a guide to biopsy by localizing tumor cells
within the area of the lesion.
It uses 1% aq.solution of the dye that is decolorized with 1%
acetic acid
The dye binds to dysplastic and malignant epithelial cells
with a high degree of accuracy.

Speckled leukoplakia after Toluidine Blue staining

CYTOBRUSH TECHNIQUE
This technique is more accurate than any
other cytologic technique used in the oral
cavity.
This technique uses a brush with firm
bristles that obtains individual cells from the
full thickness of the epithelium.

BIOPSY
When the suspicious lesion is
identified,an incisional biopsy using a
scalpel or a biopsy forceps is
recommended.
When the lesion is very small,Excisional
biopsy is performed as an investigative
procedure and as a treatment modality.

Incisional Biopsy
Histological appearance:
Hyperkeratosis and basal cell hyperplasia

TREATMENT


GENERAL CONSIDERATIONS
All possible agents leading to white keratotic lesions should
be eliminated(such as sharp teeth/Candidal infection) so as to
rule out other definable lesions.
In persisting lesions/absence of possible causative factor:
Biopsy should be taken to exclude histologically the presence
of a definable lesion and to establish the degree of epithelial
dysplasia.
Up to 60% of leukoplakias regress or totally disappear if
tobacco use is stopped.
MEDICAL MANAGEMENT( C H E M O P R E V E N T I O N )
Carotenoid and Retinoid:Eg:β-Carotene
Vitamin E
Selenium
Canthaxanthin
Astaxanthin
phytoene

1. Vitamin A75000-300000 IU/day for 3-18 months
2. 13-cis retinoic acid1.5mg/Kg per day for 3 months Followed by0.5mg/Kg per day for 9 months
3. β Carotene30mg daily for 3-6 months

4. Fenretinide -Synthetic retinoid -200mg/day -Reduces the relapse and appearance of new leukoplakias
5. Vitamin E 800 IU/day

PHOTODYNAMIC THERAPY(PDT)
PDT involves using specific wavelength of laser
light to activate a photosensitizing drug which is
administered systemically and is retained selectively
in the lesion.
This triggers a cold photochemical reaction
resulting in the generation of reactive products such
as singlet oxygen that damages tissue

Advantages:Inactivation of clinically subtle/undetectable alteration.Sparing of normal tissue.Minimal morbidity.
Disadvantage:Cutaneous photosensitivity which can persist for several months after administration of the photosensitizer which can be a major problem in the Indian Subcontinent,where oral cancer is most common.
TOPICAL CHEMOTHERAPY
Involves the use of Podophyllin solution or
Bleomycin.
According to the studies conducted by
Kovacs et al,1962 and Hammersley el
al,1985:These drugs have induced some
regression or even total resolution of
dysplasia and of clinical lesions.


OTHER ALTERNATIVE MODALITIES OF
TREATMENT
Green Tea
It has an anti-inflammatory action,antioxidant
action and Anticancer action.
Oral Lycopene
in the dose of 8 mg/day is beneficial in the
treatment of oral leukoplakia.

SURGICAL LINE OF TREATMENT
If the lesion is very small,it should be excised as a
part of investigation and as a treatment option.
Complete surgical removal (leaving free-lesion
borders) is recommended in cases with epithelial
dysplasia.
Even if the lesion is completely removed, long term
review is still usually indicated since leukoplakia can
recur.

CONCLUSIONThere is no known therapy to prevent development of oral
leukoplakia and there is no known therapy to prevent oral
squamous cell carcinoma developing from oral leukoplakia.
It has been demonstrated that a healthy life style and the
abstinence of tobacco are the best way to prevent both. Fresh
fruits and vegetables may have a protective effect in the primary
prevention of oral cancer and precancer.
Early diagnosis and treatment of leukoplakia, can reduce the
high rates of oral cancer morbidity and mortality in many
countries.

BIBLIOGRAPHY
Textbook of Oral Medicine and Radiology- Dr.Ravikiran Ongole
Textbook of Oral Medicine- Burkitt
Textbook of Oral Pathology- Shafer’s

Thank You

















