46
Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine

Management of
Neuroendocrine Tumors
James R. Howe, M.D.
Director, Surgical Oncology
and Endocrine Surgery
University of Iowa College of Medicine

Stage at Diagnosis
Localized Regional Distant
Yao et al. J. Clin. Oncology 26:3063, 2008
85%
nodes
77%
liver
51%
nodes
37%
liver
SEER vs. University of Iowa

Small Bowel Neuroendocrine
Tumors (SBNETs)

SBNETs
Most common GI site
Incidence 12 per million
50% multicentric
Well-differentiated
Indolent but present late
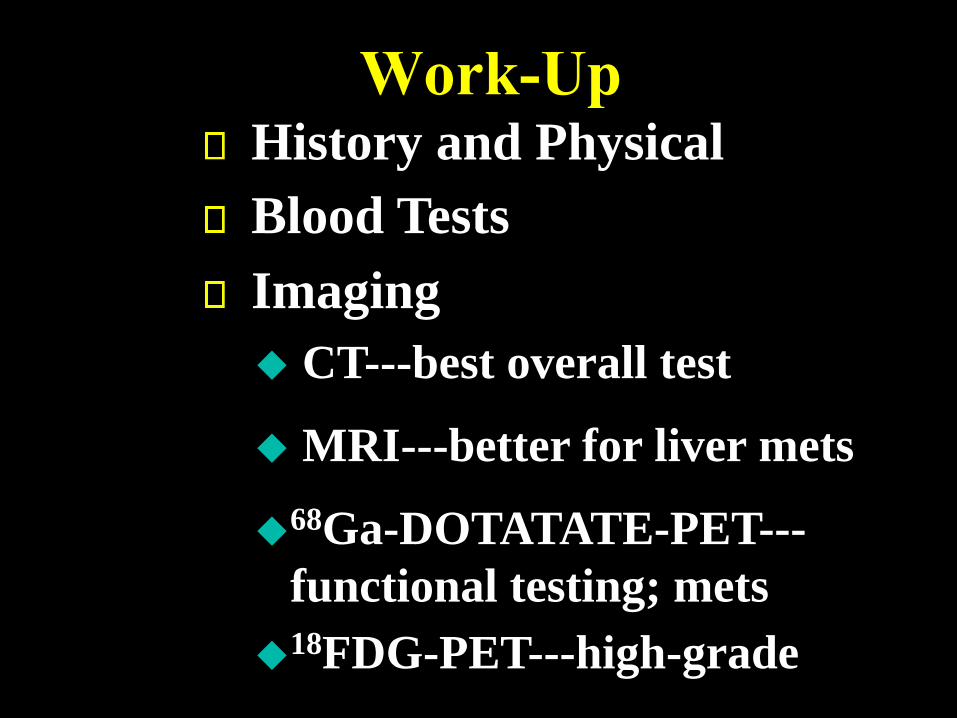
Work-UpHistory and Physical
Imaging
CT---best overall test
MRI---better for liver mets
68Ga-DOTATATE-PET---
functional testing; mets
18FDG-PET---high-grade
Blood Tests

Typical SBNET Patient

Exploration
Howe, J.R. in Atlas of Endocrine and Neuroendocrine Surgery
(Howe, J.R. ed.) Springer-Verlag (2017)

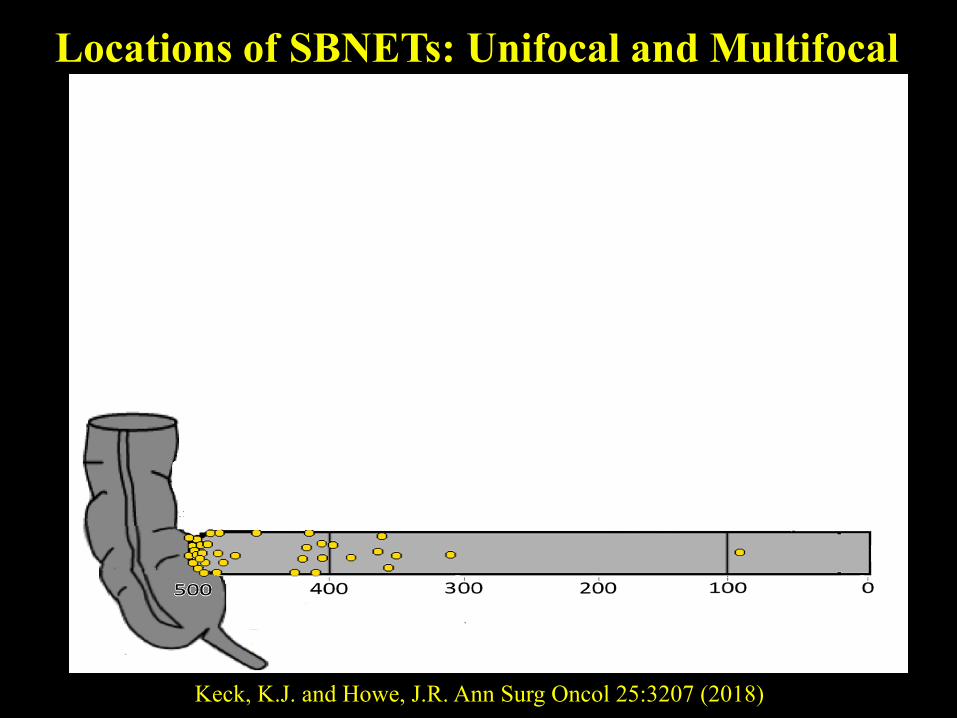
Locations of SBNETs: Unifocal and Multifocal
Keck, K.J. and Howe, J.R. Ann Surg Oncol 25:3207 (2018)

Locoregional Spread
www.lilienthenthalusa.com

Nodal Dissection
Howe, J.R. in Atlas of Endocrine and Neuroendocrine Surgery
(Howe, J.R. ed.) Springer-Verlag (2017)

Lymphadenopathy
SMV
SMA
Nodes

Open Approach with Small
Incision
Enlarged
Node

Cholecystectomy at Exploration
Somatostatin analogues lead
to gallstones
Hepatic embolization can result
in GB necrosis

Pancreatic Neuroendocrine
Tumors (PNETs)
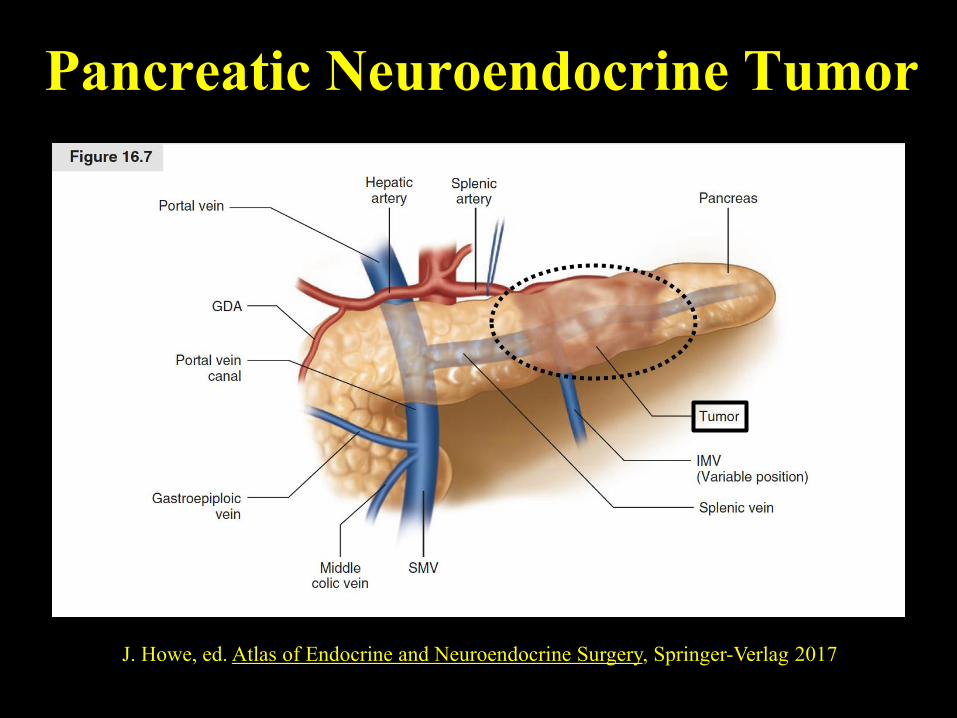
Pancreatic Neuroendocrine Tumor
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017

PNET
Normal
Pancreas
Stomach
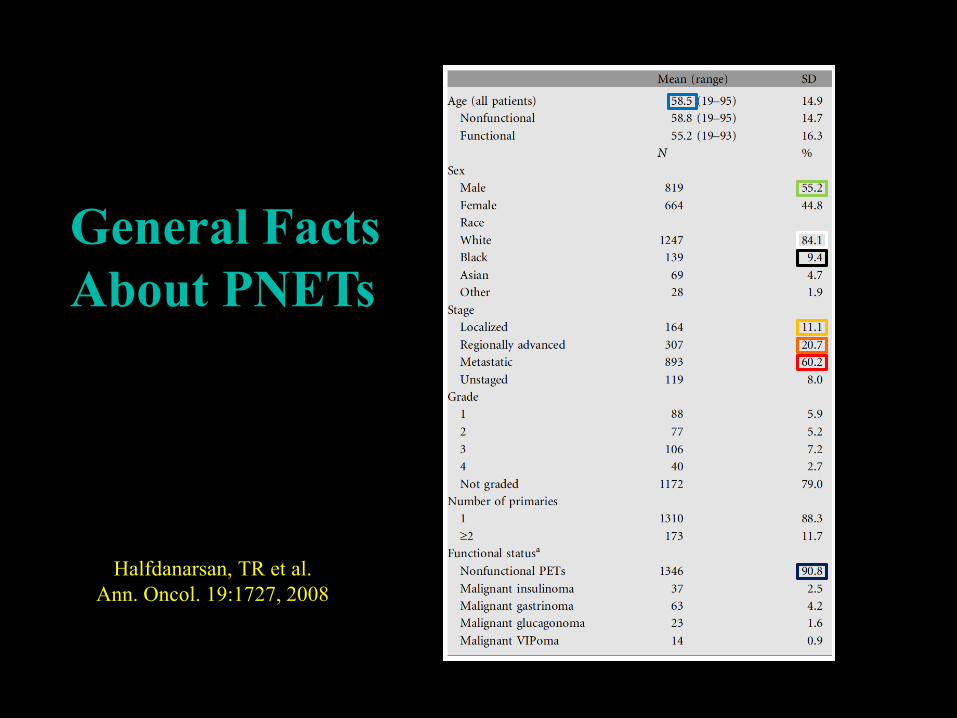
Halfdanarsan, TR et al.
Ann. Oncol. 19:1727, 2008
General Facts
About PNETs

Familial PNETs
A. Pea et al. Expert Rev Gastroenterol Hepatol 9:1407, 2015
Pancreatic Neuroendocrine Tumors
Non-functional
Insulinoma
Gastrinoma
VIPoma
Glucagonoma
Somatostatinoma
Pancreatic Polypeptide?

Diagnosis of PNETs
Symptoms
Imaging Tests
Biochemical testing
Biopsy: Endoscopic US or CT

When to Resect PNETs
Functional lesions
>2 cm
Not < 1 cm
Controversy in 1-2 cm1-3
>3 cm in VHL5
>2 cm in MEN14
1. L.C. Lee et al. Surgery 152:965, 2012
2. E.J. Kuo et al. Ann. Surg. Onc. 20:2815, 2013
3. S.M. Sharpe et al. J. Gastrointest. Surg 19:117, 2015
5. S.K. Libutti et al. Surgery 124:1153, 1998
4. F. Triponez et al. Ann. Surg. 243:265, 2006
Surgical Treatment Options
Enucleation
Distal Pancreatectomy
Pancreaticoduodenectomy (Whipple)
Laparoscopic distal pancreatectomy

Enucleation
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017

Enucleation
Hepatic
Artery
Splenic
Artery
SMV Splenic
Vein
Tumor
Pancreatic
Neck/Body
Surgical Treatment of Pancreatic
Body/Tail Lesions

CT: Pancreatic Body/Tail Mass
Tumor

Spleen
Tail of
PancreasTumor
Splenic
Artery

Distal Pancreatectomy/Splenectomy
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017

Pathology Specimen: Distal Pancreas and Spleen
SpleenTumor
Pancreatic
Margin
>1 cm
Surgical Treatment of Pancreatic
Head Lesions
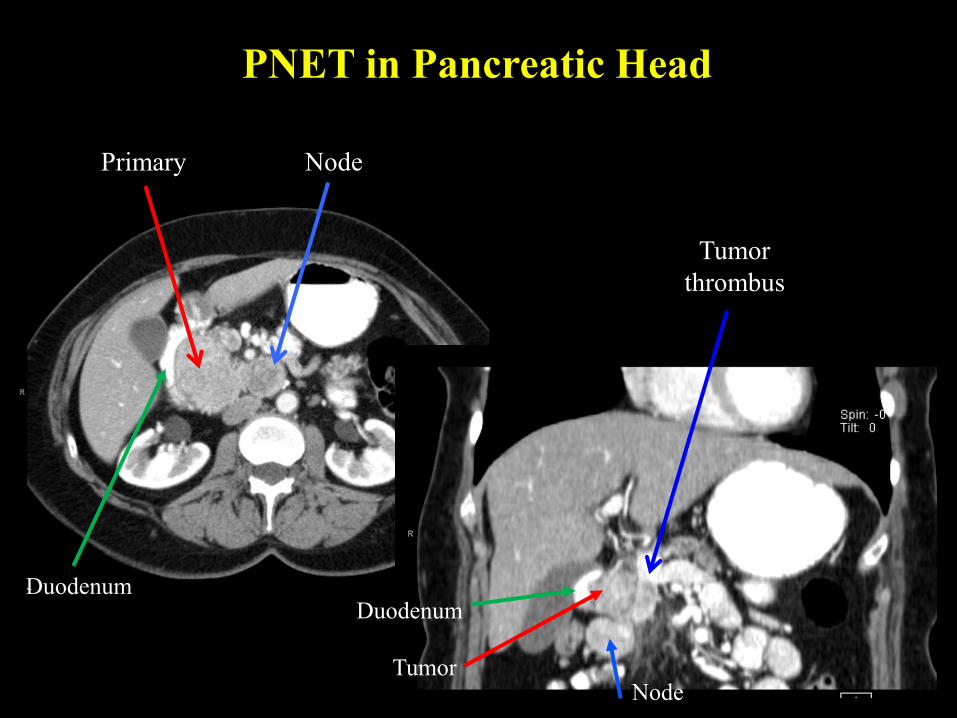
PNET in Pancreatic Head
Primary Node
Tumor
thrombus
DuodenumDuodenum
TumorNode

Cameron JL Atlas of Surgery BC Decker, Inc. 1990
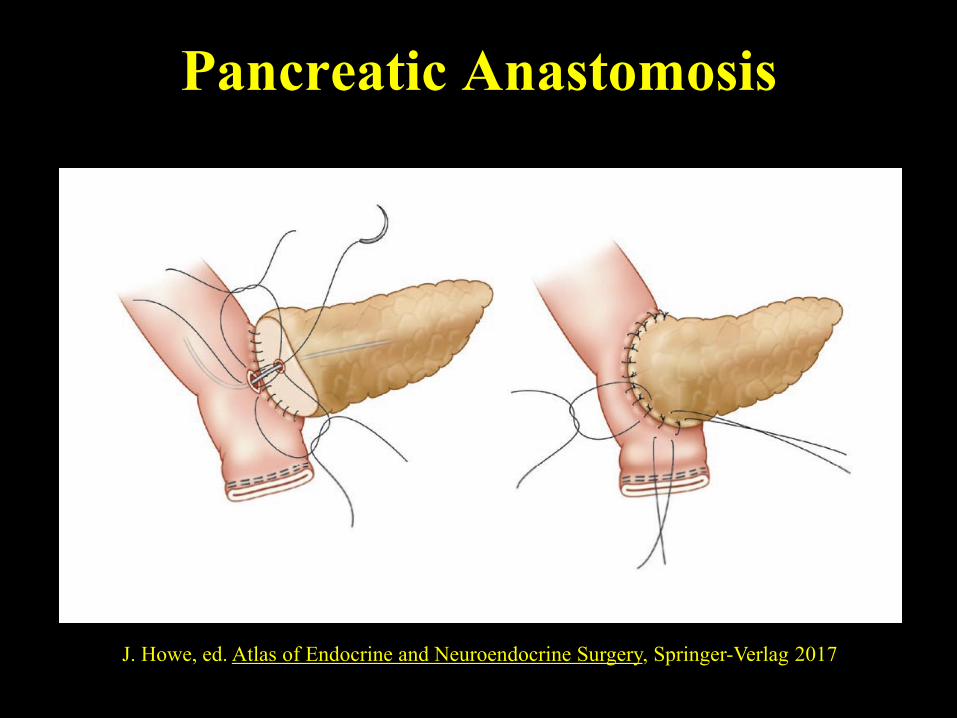
Pancreatic Anastomosis
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017

Bile Duct Anastomosis
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017
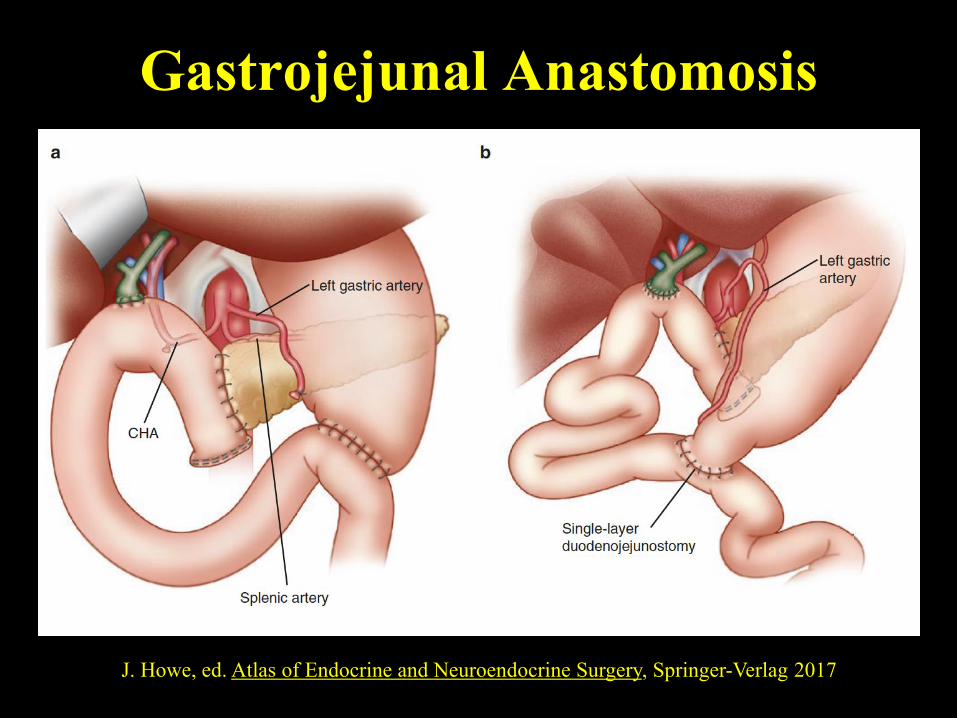
Gastrojejunal Anastomosis
J. Howe, ed. Atlas of Endocrine and Neuroendocrine Surgery, Springer-Verlag 2017

The Role of Laparoscopy for PNETs
Especially good for small, distal lesions
Can also enucleate
Well-suited for distal
pancreatectomy/splenectomy
J. Howe, ed. Atlas of Endocrine
and Neuroendocrine Surgery,
Springer-Verlag (in press)
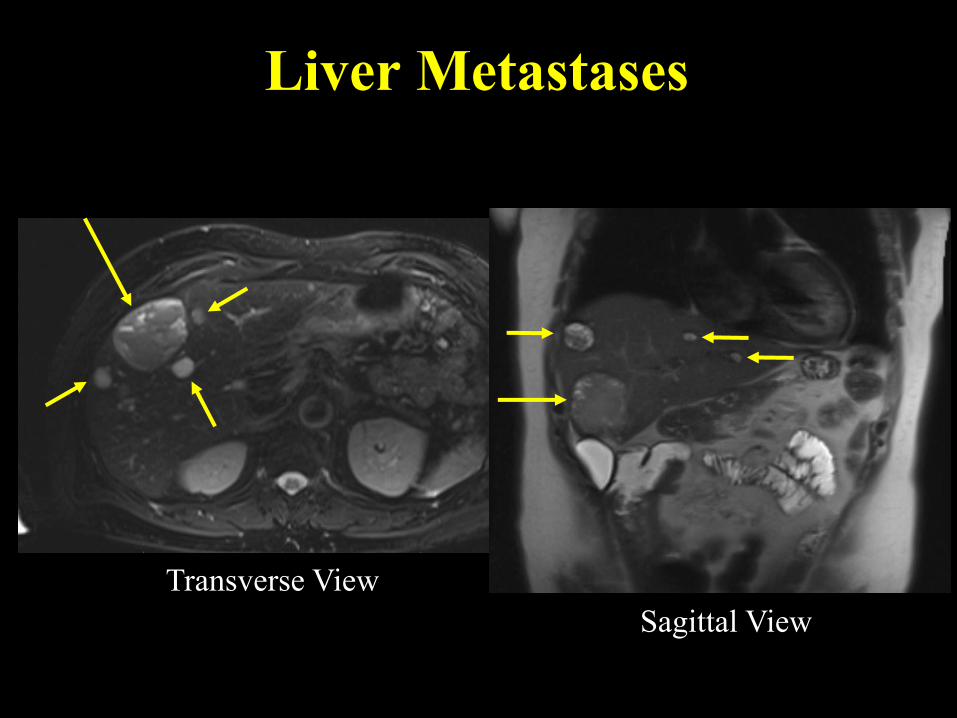
Liver Metastases
Transverse View
Sagittal View
Options for Liver Metastases
Embolization
Radioembolization
Peptide Receptor Radiotherapy (PRRT)
Somatostatin analogues
Systemic therapy
Resection, enucleation, ablation
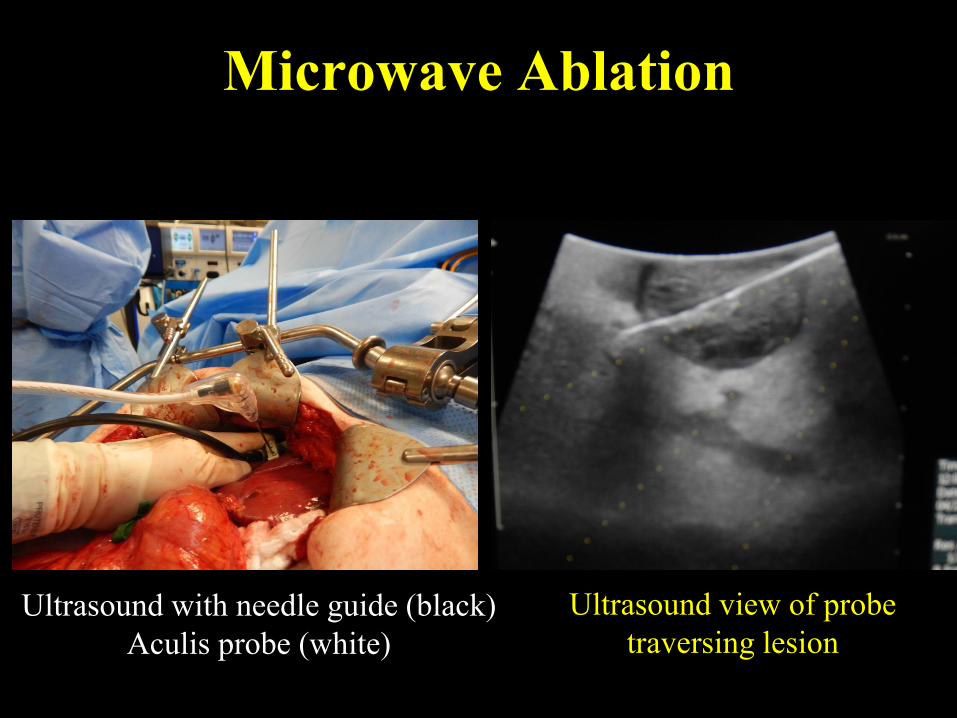
Microwave Ablation
Ultrasound with needle guide (black)
Aculis probe (white)
Ultrasound view of probe
traversing lesion
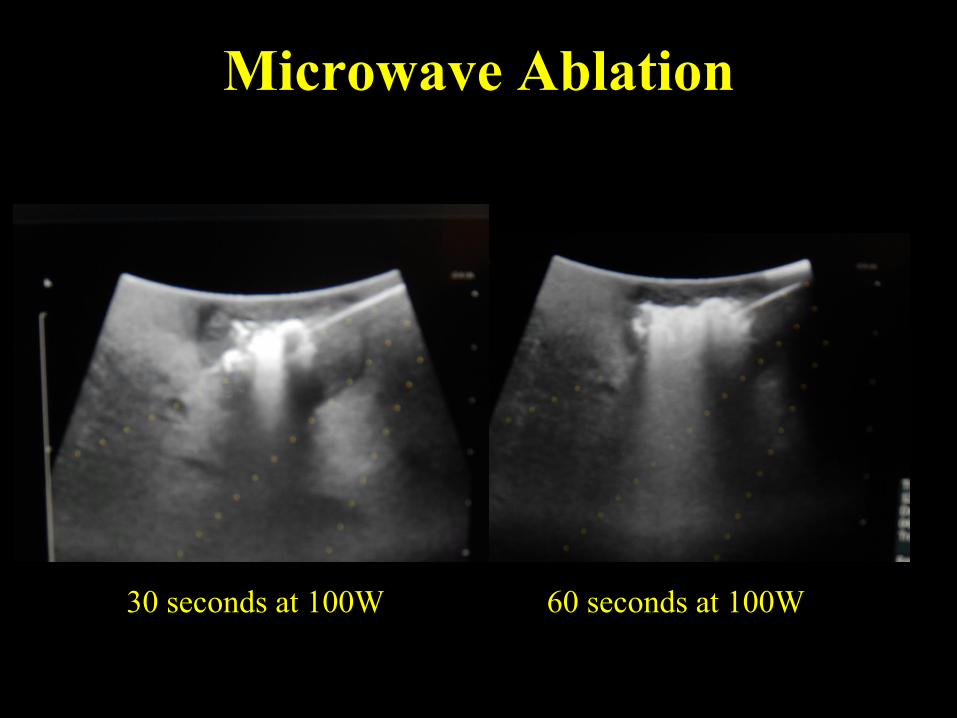
Microwave Ablation
30 seconds at 100W 60 seconds at 100W

● Not Just for Symptoms
● Improves Survival
● Parenchymal Sparing reasonable
● <10 lesions do better
● Cytoreduction target: >70-90%
Hepatic Cytoreduction
● <25% replacement do better
High Recurrence Rates in the liver---94% at 5 yrs.

Summary: Optimal Surgical
Approach to NETs
Remove the primary
Resect regional nodes
*when other options not feasible or at progression
Cytoreduce liver metastases
Use Somatostatin analogues
Use systemic therapy*
Cholecystectomy
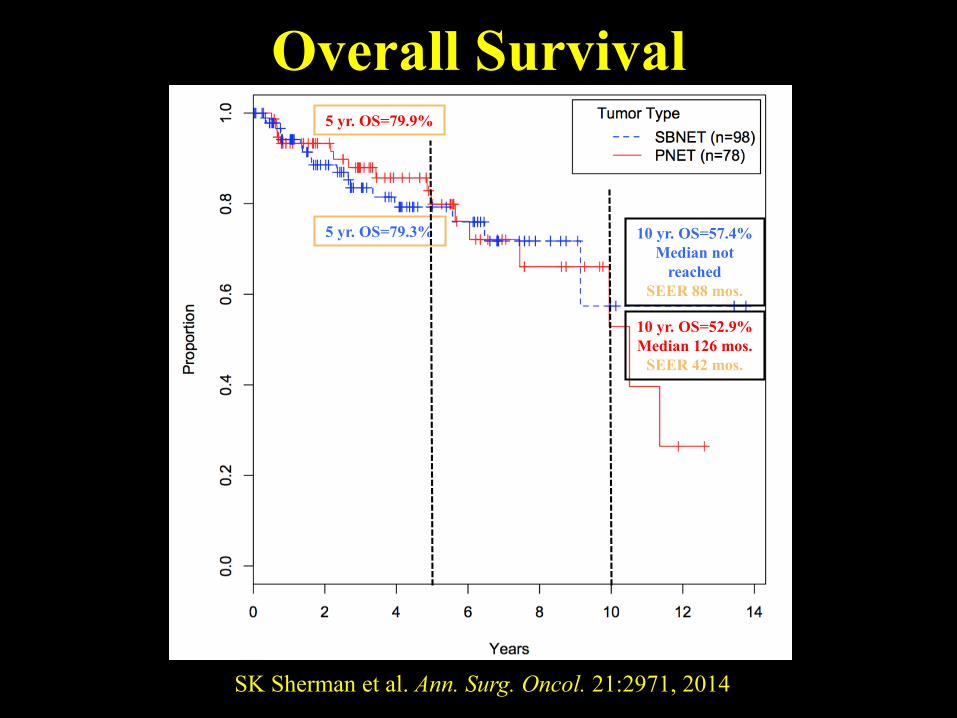
Overall Survival
5 yr. OS=79.3% 10 yr. OS=57.4%
Median not
reached
SEER 88 mos.
10 yr. OS=52.9%
Median 126 mos.
SEER 42 mos.
5 yr. OS=79.9%
SK Sherman et al. Ann. Surg. Oncol. 21:2971, 2014

University of Iowa
NeuroEndocrine Cancer Clinic
Thomas O’Dorisio-Endocrinology
James Howe-Surgical Oncology
Sue O’Dorisio-Pediatric Oncology
Yusuf Menda, Dave Bushnell-Nuc. Med.
C. Chandrasekharan-Medical Oncology
Andrew Bellizzi-Pathology
Jackie Sexton, Kim Miller-Nursing
Joseph Dillon-Endocrinology
NIH SPORE P50 CA174521-01

Kinnick Stadium
Thanks from Iowa!!
Old Capitol
Undergraduate Campus
University Hospital
Medical School
Press Box at Kinnick

















