ORTHOPEDICS | Healio.com/Orthopedics n Feature Article abstract Full article available online at Healio.com/Orthopedics. Search: 20131021-12 Partial traumatic hemipelvectomy is a devastating condition. Although by definition the affected limb is not totally transected from the trunk because of retained soft tissue, the reported mortality rate is actually higher than in complete traumatic hemipelvec- tomy. Between January 2000 and December 2011, a total of 917 patients were admit- ted to the authors’ institution for pelvic fracture. Seven of these patients met the criteria for partial traumatic hemipelvectomy. All 7 patients had multiple associated injuries and met the criteria for Baskett class IV hypovolemic shock on arrival at the emergency department. The amount of bleeding was the greatest issue, and control of hemorrhage and rapid blood transfusion were the initial goals. Abdominal aorta balloon occlusion, laparotomy and packing, and pelvic external fixation were useful to control bleeding. Two patients died during the initial resuscitation phase. Angiography (digital subtrac- tion or computed tomographic) was performed in 4 patients but did not provide any treatment-altering information. Limb preservation was attempted in 2 patients; both of these patients eventually required hindquarter amputation. One patient died, and the second patient survived after a difficult postoperative course. The best results were ob- tained in 3 patients who underwent completion of the hindquarter amputation within 24 hours of trauma. All patients became wheelchair dependent, and no patient was able to return to work. Early completion of hindquarter amputation after hemorrhaging has been controlled is recommended in patients with partial traumatic hemipelvec- tomy. Angiography did not prove useful in decision making. The authors are from the Department of Orthopedics (GW, DZ, MX, JH, QL), Provincial Hospital Affiliated to Shandong University, Jinan, Shandong, China; the Po-Cheng Orthopaedic Institute (W- JS), Kaohsiung, Taiwan; and the Department of Orthopedics (GT), Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, China. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Dongsheng Zhou, MD, Department of Orthopedics, Provincial Hospital Affiliated to Shandong University, J324 Jingwu Rd, Jinan City, Shandong Province, China, 250021 ([email protected]). doi: 10.3928/01477447-20131021-12 Management of Partial Traumatic Hemipelvectomy GUODONG WANG, MD; DONGSHENG ZHOU, MD; WUN-JER SHEN, MD; MAOYUAN XIN, MD; JILIANG HE, MD; QINGHU LI, MD; GUOQING TAN, MD Figure: Anteroposterior radiograph showing an open book injury, Tile C1 pelvic fracture (A). Com- puted tomographic angiography showing complete disruption of iliac vessels (B). B A e1340
Transcript
ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
abstractFull article available online at Healio.com/Orthopedics. Search: 20131021-12
Partial traumatic hemipelvectomy is a devastating condition. Although by definition the affected limb is not totally transected from the trunk because of retained soft tissue, the reported mortality rate is actually higher than in complete traumatic hemipelvec-tomy. Between January 2000 and December 2011, a total of 917 patients were admit-ted to the authors’ institution for pelvic fracture. Seven of these patients met the criteria for partial traumatic hemipelvectomy. All 7 patients had multiple associated injuries and met the criteria for Baskett class IV hypovolemic shock on arrival at the emergency department. The amount of bleeding was the greatest issue, and control of hemorrhage and rapid blood transfusion were the initial goals. Abdominal aorta balloon occlusion, laparotomy and packing, and pelvic external fixation were useful to control bleeding. Two patients died during the initial resuscitation phase. Angiography (digital subtrac-tion or computed tomographic) was performed in 4 patients but did not provide any treatment-altering information. Limb preservation was attempted in 2 patients; both of these patients eventually required hindquarter amputation. One patient died, and the second patient survived after a difficult postoperative course. The best results were ob-tained in 3 patients who underwent completion of the hindquarter amputation within 24 hours of trauma. All patients became wheelchair dependent, and no patient was able to return to work. Early completion of hindquarter amputation after hemorrhaging has been controlled is recommended in patients with partial traumatic hemipelvec-tomy. Angiography did not prove useful in decision making.
The authors are from the Department of Orthopedics (GW, DZ, MX, JH, QL), Provincial Hospital Affiliated to Shandong University, Jinan, Shandong, China; the Po-Cheng Orthopaedic Institute (W-JS), Kaohsiung, Taiwan; and the Department of Orthopedics (GT), Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, China.
The authors have no relevant financial relationships to disclose.Correspondence should be addressed to: Dongsheng Zhou, MD, Department of Orthopedics,
Provincial Hospital Affiliated to Shandong University, J324 Jingwu Rd, Jinan City, Shandong Province, China, 250021 ([email protected]).
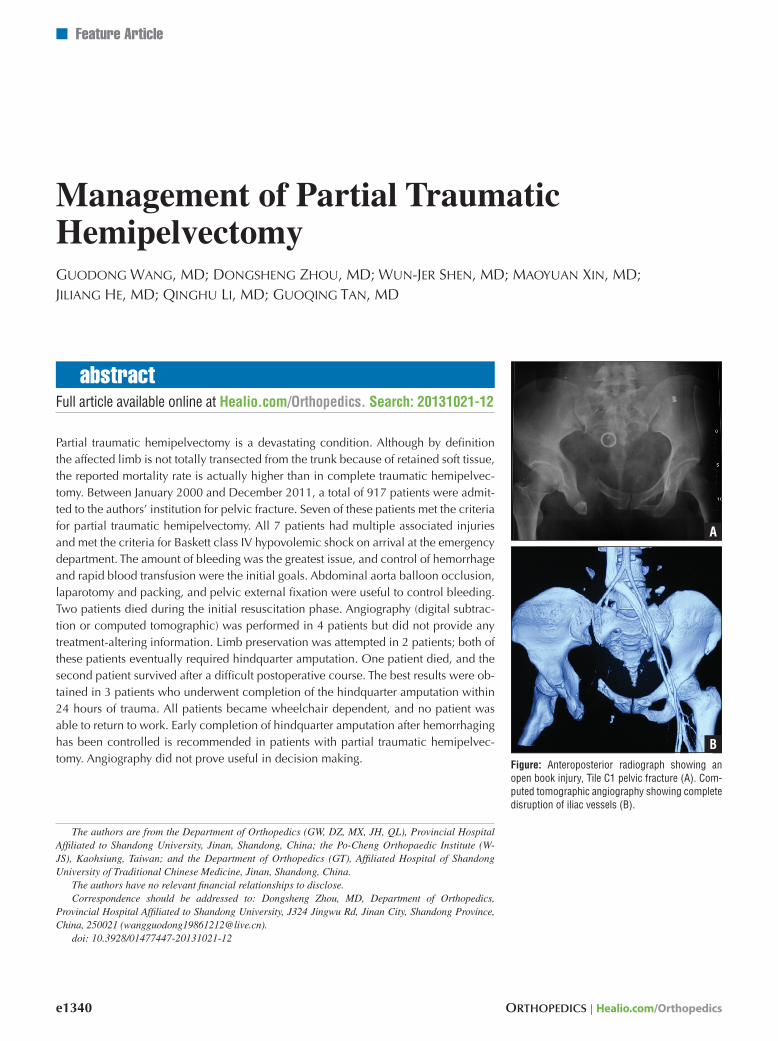
Figure: Anteroposterior radiograph showing an open book injury, Tile C1 pelvic fracture (A). Com-puted tomographic angiography showing complete disruption of iliac vessels (B).
B
A
e1340
NOVEMBER 2013 | Volume 36 • Number 11
Partial traumatic HemiPelvectomy | Wang et al
Traumatic hemipelvectomy, also known as traumatic hindquarter am-putation, was first reported in 1915.1
It is a devastating injury, with disruption of the pelvic ring at the pubic symphysis and sacrum combined with rupture of the iliac vessels and nerves.2,3 The etiology is high-energy trauma, usually traffic accidents or industrial crush injuries.4,5 Combined with associated injuries of the head, thorax, ab-dominal organs, and other extremities,2,6 it is not surprising that most patients die be-fore arrival at the hospital.7 Survivors expe-rience the complications of devasculariza-tion, muscle necrosis, and genitourinary tract and anorectal bowel injury.8
In 1991, Klingman et al9 used the term partial traumatic hemipelvectomy to de-scribe cases in which the bony pelvis is fractured both anteriorly and posteriorly and accompanied by irreparable vascular injury, yet the affected limb is not totally transected from the trunk because of re-tained soft tissue. They noted that patients with partial hemipelvectomy had a higher mortality rate than patients with complete limb avulsion. It has been postulated that the injured vessels can retract and be closed by muscle contraction in patients with com-plete hemipelvectomy,7,9,10 whereas vessel damage may be missed in cases of partial hemipelvectomy, leading to a higher mor-tality rate.2,7
Few reports in the literature focus on partial hemipelvectomy, with most articles being case reports. This article presents the authors’ experience in the emergency as-sessment and treatment of 7 patients with partial traumatic hemipelvectomy.
Materials and MethodsBetween January 2000 and December
2011, a total of 917 patients were admit-ted to the authors’ hospital for pelvic frac-tures. Of these patients, 2 patients sustained complete traumatic hemipelvectomy and 7 met the criteria for partial traumatic hemi-pelvectomy. Permission to conduct this retrospective study was obtained from the hospital ethics committee.
Of the 7 patients with partial traumatic hemipelvectomy, 3 were men and 4 were women. Median age was 28 years (range, 21-35 years). Five patients were involved in motor vehicle accidents, 1 patient fell from a height, and 1 patient was crushed by industrial machinery. Six patients were brought directly to the hospital emergency department, and 1 patient was transferred from another hospital at 6 days postinjury for management of infection. Medical re-cords were obtained for the latter patient from the transferring hospital.
Initial treatment was damage control. All patients underwent management fol-lowing Advanced Trauma Life Support Guidelines.11 The initial diagnostic steps in-cluded obtaining thoracic and pelvic radio-graphs (Figure 1A) and performing focused assessed sonography in trauma (FAST). Visible bleeders were clamped and ligated. Laparotomy and retroperitoneal and wound packing were performed as needed (Figure 1B). Balloon occlusion of the abdominal aorta was performed in selected cases via normal limb femoral artery cutdown place-ment of a Fogarty catheter balloon. The bal-loon was placed between the renal arteries and the iliac bifurcation (Figures 1C, D). Pelvic external fixation was applied on an individual basis for temporary stabiliza-tion of the bony pelvis. Massive amounts
of blood products were required. The trans-fusion target was 1:1 volume replacement during the resuscitation period. Hindquarter amputation was performed after hemor-rhage control was achieved (Figure 1E). As soon as feasible, digital subtraction angiog-raphy or computed tomographic angiogra-phy was performed to assess pelvic vascu-lar damage before hindquarter amputation (Figure 2). This usually took 30 minutes or longer.
Depending on the associated inju-ries, treatment priorities were adjusted. Ruptured urethrae were stented with a Foley catheter, and urine was diverted via a suprapubic catheter. Intraperitoneal bladder ruptures were sutured during laparotomy.2 Ureter injuries were repaired primarily. A diverting colostomy was routinely per-formed. Vacuum-assisted closure (VAC; KCI, San Antonio, Texas) was used in sev-eral patients. For patients who survived the first few days, multiple subsequent surger-ies were undertaken, including completion of the hindquarter amputation and frequent second-look debridements. Closure of the wound was individualized and always re-quired some type of musculocutaneous flap.
resultsAll 7 patients met the criteria for Baskett
class IV hypovolemic shock on arrival at
Figure 1: Anteroposterior radiograph showing a large displaced fracture of the right sacral ala (A). Laparotomy was performed as soon as possible (B). Lateral radiograph under fluo-roscopy (C) and intraoperative pho-tograph (D) showing the descending aorta balloon occlusion procedure. Intraoperative photograph showing a complete hindquarter amputation (E).
1A
1D
1B 1C
1E
e1341
ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
the emergency department.12 Time from trauma to arrival was less than 2 hours in 4 patients and between 2 and 3 hours in the remaining 3 patients. Mean Injury Severity Score was 5468 points (range, 42-67 points) for the 6 patients directly admitted to the hospital.13
All 7 patients sustained unilateral par-tial traumatic hemipelvectomy. Patient de-mographics are summarized in the Table. By the Tile classification,14 5 cases were C1 type and 2 were C2 type. The fracture line in the posterior pelvic ring was in the Denis zone II of the sacrum in 1 patient and passed through the sacroiliac joint in 6 patients. Anteriorly, superior and inferior pubic ramus fractures occurred in 5 patients (3 were bilateral and 2 were unilateral), and pubic symphysis diastasis occurred in 2 pa-tients.
Bleeding was the major problem. Abdominal aorta balloon occlusion was needed in 5 patients; mean occlusion time was 51 minutes (range, 34-62 minutes). For patients who survived, mean units of packed red blood cells and fresh-frozen plasma transfused per patient within the first 24 hours was 2668 and 1764 units, respectively. The volume replacement ratio of transfusion was 1:1 during resuscita-tion. Pelvic external fixation was used as a method to stabilize the pelvis and decrease the pelvic cavity volume prior to hindquar-ter amputation.15 Laparotomy and packing of the abdominal or retroperitoneal cavity also were performed in all 7 patients. Two patients died in the emergency department during the resuscitation phase.
Six patients had genitourinary tract inju-ries, all 7 patients had anorectal or colon in-juries, 5 patients had perineum tears, and 4 patients had Morel-Lavallée lesions. Three patients sustained thoracic injuries, 3 had head injuries, 5 had abdominal injuries, and 6 had additional extremity injuries (Table).
Urgent digital subtraction or computed tomographic angiography was performed for the 4 surviving patients who were ad-mitted directly to the hospital. Blood flow blockage at the iliac artery level was ob-
served in all 4 patients, with contrast agent diffusion around the iliac vessel noted in 1 patient. Severe vessel damage, rupture, and thrombosis were diagnosed.
Surgical completion of the hindquarter amputation was performed on the first day of admission in 3 patients and on the fifth day in 1 patient. In the latter patient, am-putation was delayed in an attempt to save the limb; however, the patient developed massive infection and died from sepsis on the 10th day of hospitalization. The 3 pa-tients who received immediate amputation required multiple additional second-look exploration and debridement, but all 3 of these patients survived.
The patient who was transferred from another hospital on postinjury day 6 had undergone a hip disarticulation (instead of a hindquarter amputation) in an effort to preserve the hemipelvis. However, tissue necrosis and uncontrolled infection devel-oped in this patient (Figures 3A, B). A for-mal hindquarter amputation was performed in this patient, and the infection eventually was controlled after 21 visits to the operat-ing room (Figures 3C, D).
A rectus abdominis flap was used to close the wound in 3 patients, a composite island flap was used in 2 patients, and split-thickness skin grafting was used in 4 pa-tients (more than 1 modality was needed per patient). Large wounds with excessive exu-date are, in theory, good candidates for vac-
uum-assisted closure. In 2 of our patients, vacuum-assisted closure was attempted, but the sheer size of the wounds and the need for frequent surgical debridements made vacuum-assisted closure impractical.
Follow-up in the 4 patients who survived ranged from 17 to 41 months. A hindquarter amputation prosthesis was fabricated for 1 of the patients but proved to be awkward and was soon discarded by the patient. All 4 pa-tients are wheelchair dependent, and none of the patients have been able to return to work.
discussionTraumatic hemipelvectomy is the most
severe type of pelvic fracture.1-5,16 In the current study, the incidence was 0.98% (9 of 917) for all pelvic injuries, which is con-sistent with the incidence of 0.6% to 1.8% reported in the literature.2,11 The true mor-tality rate is unknown because many, if not most, of these patients die before reaching the hospital.5,12,13,16 For those who reach the emergency department, the statistics are better; in 104 documented cases, 71 pa-tients survived.1,2,11-13,16
The etiology is high-energy trauma, usually motor vehicle accidents or indus-trial crush injuries. In motor vehicle acci-dents, the force vector is believed to pass from an abducted and external rotated lower limb to the pelvis.5 In a fall from a height, the mechanism is probably an ip-silateral knee-contact ground strike with
Figure 2: Anteroposterior radiograph showing an open book injury, Tile C1 pelvic fracture (A). Computed tomographic angiography showing complete disruption of iliac vessels (B).
2B2A
e1342
NOVEMBER 2013 | Volume 36 • Number 11
Partial traumatic HemiPelvectomy | Wang et al
the hip and knee flexed. Previous studies have shown that the fracture line usually crosses the pubic symphysis and sacroiliac joint.17 In the current 7 patients, only 2 had symphysis separation; the remaining 5 had pubic ramus fractures.
Severe soft tissue damage involving the pelvic vessels, nerves, genitourinary tract, anorectal bowel, and muscles,2,5,10,18,19 along with the fracture, results in massive bleeding and subsequent hypovolemic
shock.9 Despite the large amount of blood transfused, 2 patients in the current series died during resuscitation. Laparotomy and packing of the abdominal and ret-roperitoneal cavity were necessary to control hemorrhage. During laparotomy, clamping of the abdominal aorta is usual-ly necessary for hemostasis.16,20 The cur-rent authors also have found intra-aortic balloon occlusion helpful for hemostasis during emergency resuscitation.21-23
The role of urgent angiography (digi-tal subtraction or computed tomographic) after initial resuscitation is debated.24,25 Although these studies may provide ad-ditional information regarding the status of the pelvic vessels, obtaining the studies require time when time is of the essence. Proponents believe angiography aids in identifying bleeding points and may help to decide which patients have a real chance at limb salvage. Detractors believe that the
Table
Patient Demographics
Patient No./Sex/Age, y ISS
Mechanism of Injury
Rectal & Colon Genit Assoc Injuries Open Wound Complications Outcome
extra time spent waiting for the study re-sults can be better used, and in cases of true traumatic hemipelvectomy, comple-tion of amputation is inevitable and angi-ography serves no purpose. In the current series, angiography was performed in 4 patients, and all showed irreparable vessel damage. The procedure takes longer than 30 minutes and hinders other resuscitation efforts. The authors originally believed angiography could provide information to help decide which limbs could be pre-served, but unfortunately, it confirmed that amputation was necessary. Angiography is no longer part of their treatment protocol. Schoderbek et al24 proposed angiographic embolization to achieve emergency hemo-stasis; however, the current authors have no experience with that procedure.
Because a hemipelvectomy is at stake, the differential diagnosis between partial traumatic hemipelvectomy and open Tile C pelvic injury is of utmost importance. The use of digital subtraction or computed tomographic angiography to determine the severity of vascular injury in this situation is controversial. Williams et al25 advocated angiography before completing a partial hemipelvectomy to confirm the diagnosis; however, this recommendation was made based on their experience with only 2 pa-tients. Labler et al2 reviewed 96 cases and found that angiography did not increase the rate of lower limb salvage. They fur-ther stated that hemipelvectomy should be completed as a life-saving interven-tion when bleeding is difficult to control. Schoderbek et al24 published their experi-ence in using angiographic embolization to achieve emergency hemostasis, but they also ultimately decided to remove it from their treatment protocol. It was found that early completion of hemipelvectomy resulted in a lower complication rate and smoother hospital course than initial man-agement with angiography and attempted reconstruction.
Genitourinary tract injury and anorectal or colon injury is to be expected in trau-matic hemipelvectomy, occurring in all of
the patients in the current series and in more than 80% of patients reported by Rieger and Dietl.17 A diverting colostomy is recom-mended to prevent further fecal contamina-tion.26,27 Placement of the colostomy stoma should take into consideration the condition of the abdominal wall and the location of the fracture, especially when the hemipel-vectomy is on the left side.
Surgeons are trained to save life and limb, and every extra joint preserved im-proves quality of life. Unfortunately, evi-dence suggests that attempts to preserve the limb, or even just to try to preserve the fractured hemipelvis and buttocks (ie, hip disarticulation instead of hemipelvectomy), leads to necrosis and infection.2 In the cur-rent study, the best results were obtained in the 3 patients who underwent completion of hindquarter amputation within 24 hours after trauma. The patient who underwent delayed amputation died days later from sepsis, and the patient who initially under-
went hip disarticulation eventually required conversion to hindquarter amputation. The authors now recommend early completion of the hindquarter amputation.
Because of its traumatic nature, it is im-possible to plan wound closure as one would for elective hemipelvectomy in cases of tu-mor. Due to ongoing tissue necrosis and in-fection, aggressive second-look exploration and debridement should be performed after hindquarter amputation surgery.5 Closure of the amputation wound must be tailored individually. Musculocutaneous flaps are usually necessary to cover the wound.9,16 Many variations have been described, in-cluding the gluteus, thoracoabdominal, rec-tus abdominis, latissimus dorsi, and com-posite island flaps.28-30 Skin grafting may be sufficient if patients have viable muscular coverage.5,10,31 The current authors prefer the rectus abdominis flap. Vacuum-assisted closure is a well-established technique, but during the acute phase of treatment, it
3A
Figure 3: Anteroposterior radiograph (A) and photograph (B) showing tissue necrosis and uncontrolled infection in a patient who underwent hip disarticulation in an attempt to preserve the hemipelvis. Antero-posterior radiograph (C) and photograph (D) at 18-month follow-up showing the infection resolved after complete hindquarter amputation in our hospital.
3B
3D3C
e1344
NOVEMBER 2013 | Volume 36 • Number 11
Partial traumatic HemiPelvectomy | Wang et al
proved technically difficult to use due to the presence of massive amounts of necrotic tissue and fluid exudate, and it also was a hindrance during the frequent debride-ments.
Even when performed electively, hemi-pelvectomy is a mutilating procedure. Prosthetic fitting is difficult. Several de-signs are available, but all are cumbersome, heavy, and impractical for daily use. The literature indicates that almost all patients prefer to use a wheelchair,2,32,33 and the cur-rent authors’ experience confirms this. Severe depression is common, and few, if any, patients are able to return to work.
2. Labler L, Trentz O, Keel M. Traumatic hemi-pelvectomy. Eur J Trauma. 2005; 31:543-550.
3. Osti M, Mittler C, Putzke M, Benedetto K. Traumatic hemipelvectomy: a report of successful reimplantation. Injury. 2006; 37(10):1015-1018.
4. Klasen H, ten Duis H. Traumatic hemipelvec-tomy. J Bone Joint Surg Br. 1989; 71(2):291-295.
5. Beal S, Blaisdell F. Traumatic hemipelvec-tomy: a catastrophic injury. J Trauma. 1989; 29(10):1346-1351.
6. Pohlemann T, Paul C, Gänsslen A, Regel G, Tscherne H. Traumatic hemipelvectomy: ex-periences with 11 cases. Unfallchirurg. 1996; 99(4):304-312.
7. Lasurt S, Combalia-Aleu A. Complete trau-matic hemipelvectomy: report of a case after 19 years of follow-up. Injury. 2010; 41(8):874-882.
8. Kauvar D, Baskin T, Hayda R, Martin R. Complete traumatic hemipelvectomy re-sulting from roadside guardrail penetra-tion of a motor vehicle. Injury Extra. 2005; 36(10):454-457.
9. Klingman R, Smith P, Stromberg B, Valen-tine J, Goebel M. Traumatic hemipelvecto-my. Ann Plast Surg. 1991; 27(2):156-163.
10. Timmers T, Tiren D, Hulstaert P, Schellekens P, Leenen L. Traumatic hemipelvectomy: improvements in the last decennia illustrated by 2 case reports. Int J Surg Case Rep. 2012; 3(7):246-252.
11. Collicott P, Hughes I. Training in ad-vanced trauma life support. JAMA. 1980; 243(11):1156-1159.
12. Baskett PJ. ABC of major trauma: manage-ment of hypovolaemic shock. BMJ. 1990; 300(6737):1453-1457.
13. Baker S, O’Neill B, Haddon W Jr, Long W. The injury severity score: a method for de-scribing patients with multiple injuries and evaluating emergency care. J Trauma. 1974; 14(3):187-196.
14. Tile M. Pelvic ring fractures: should they be fixed? J Bone Joint Surg Br. 1988; 70(1):1-12.
15. Heini P, Ganz J. The pelvic C-clamp for the emergency treatment of unstable pelvic ring injuries: a report on clinical experience of 30 cases. Injury. 1996; 27(suppl 1):38-45.
16. Moore W, Brown J, Haynes J, Viamontes L. Traumatic hemipelvectomy. J Trauma. 1987; 27(5):570-572.
17. Rieger H, Dietl K. Traumatic hemipelvec-tomy: an update. J Trauma. 1998; 45(2):422-426.
18. Lipkowitz G, Phillips T, Coren C, Spero C, Glassberg K, Tolete-Velcek F. Hemipelvec-tomy, a lifesaving operation in severe open pelvic injury in childhood. J Trauma. 1985; 25(9):823-827.
19. Cho K, Kang Y, Ahn J, Yoo T. Traumatic hemipelvectomy before body image has de-veloped. Yonsei Med J. 1999; 40(1):80-83.
20. Siemens R, Flint LJ. Traumatic hemipel-vectomy: a case report. J Trauma. 1977; 17(3):245-247.
21. Martinelli T, Thony F, Decléty P, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma. 2010; 68(4):942-948.
22. Li L, Zhou D, Wang L, Wang B, Mu W, Wang F. Treatment of massive bleeding after pelvic fracture with temporary occlusion of abdom-inal aorta. Chinese Journal of Orthopedics. 2011; 31(5):487-490.
23. Morrison J, Percival T, Markov N, et al. Aor-tic balloon occlusion is effective in control-ling pelvic hemorrhage. J Surg Res. 2012; 177(2):341-347.
24. Schoderbek R, Battaglia T, Dorf E, Kahler D. Traumatic hemipelvectomy: case report and literature review. Arch Orthop Trauma Surg. 2005; 125:358-362.
25. Williams D, Masood U, Norton MR. A case of traumatic hemipelvectomy. Injury Extra. 2009; 40:99-100.
27. Rodriguez-Morales G, Phillips T, Conn A, Cox EF. Traumatic hemipelvectomy: report of two survivors and review. J Trauma. 1983; 23(7):615-620.
28. Cooper M, Waterhouse N. Reconstruction of the pelvis using a composite island flap salvaged from the remaining leg. Ann Plast Surg. 1987; 19(3):276-283.
29. Raftos J, Ethell A, Bye W, Giles J, Cameron-Strange A. Traumatic hemipelvectomy asso-ciated with contralateral hip dislocation: case report. J Trauma. 1994; 36(4):583-588.
30. Nichter L, Bolton L, Rink D. Bony and soft tissue reconstruction and rehabilitation fol-lowing traumatic hemipelvectomy, exsan-guination and cardiac arrest. Ann Plast Surg. 1988; 20(4):326-330.
31. Evans RJ, Foss F. Traumatic hemipelvec-tomy in combination with traumatic amputa-tion of an upper extremity. J Trauma. 1984; 24(4):342-345.