39
Management of Pulmonary Disease and Asthma Terry Flotte, M.D. University of Massachusetts Medical School
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | lesley-underwood |
| View: | 214 times |
| Download: | 0 times |

Management of Pulmonary Disease
and Asthma
Terry Flotte, M.D.
University of Massachusetts Medical School

Overview of Presentation
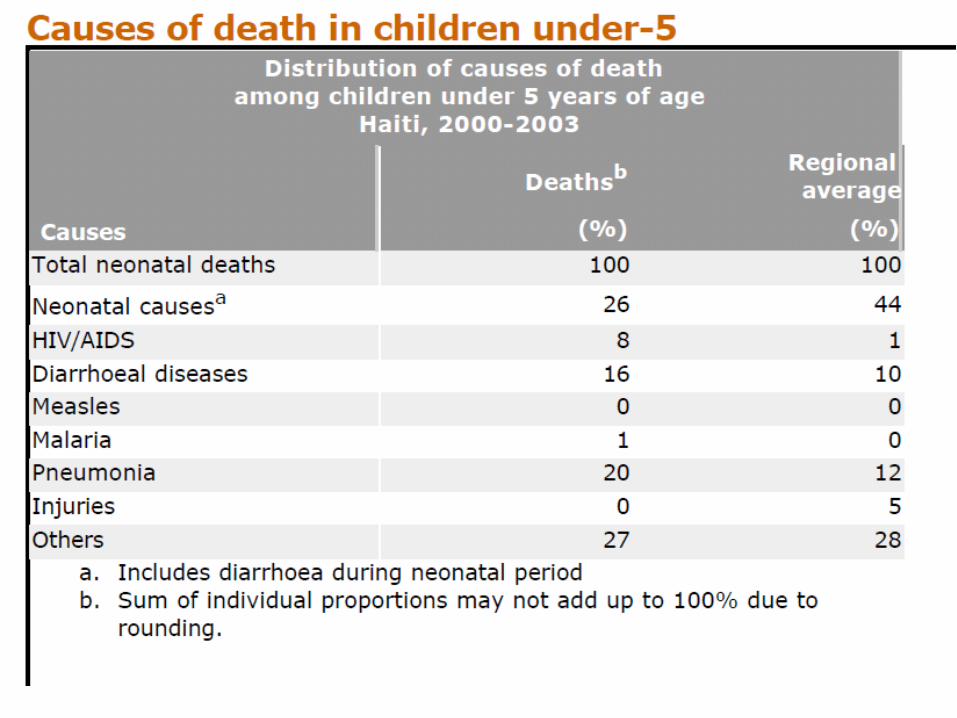
• Impact of Pulmonary Disease: Haiti and the World
• Causes of Acute and Chronic Pulmonary Syndromes
• Chronic Outpatient Management of Asthma
Risk factors for Pneumoniamorbidity and mortality (WHO-GAPP)
• Nutritional deficiency– Shortened breast-feeding time– Underweight– Zinc deficiency
• Indoor air pollution– Wood-burning– Tobacco smoke– Urban air pollution
• Immunization status (measles, pertussis, Hib, Pneumococcus)
• Case Management– Prompt detection and Antibiotic therapy
• HIV status

Management of AcuteLower Respiratory Tract Infection
• Rule-out and treat malnutrition• Evaluate for signs of sepsis or acute
decompensation– In this case, stabilize, give first dose IM and
ship to hospital• Oral therapy with TMP/sulfa or amoxicillin• Parenteral therapy with Amp/Pen and
Gentamicin or Ceftriaxone

Evaluation of children with recurrent pneumonia in Haiti
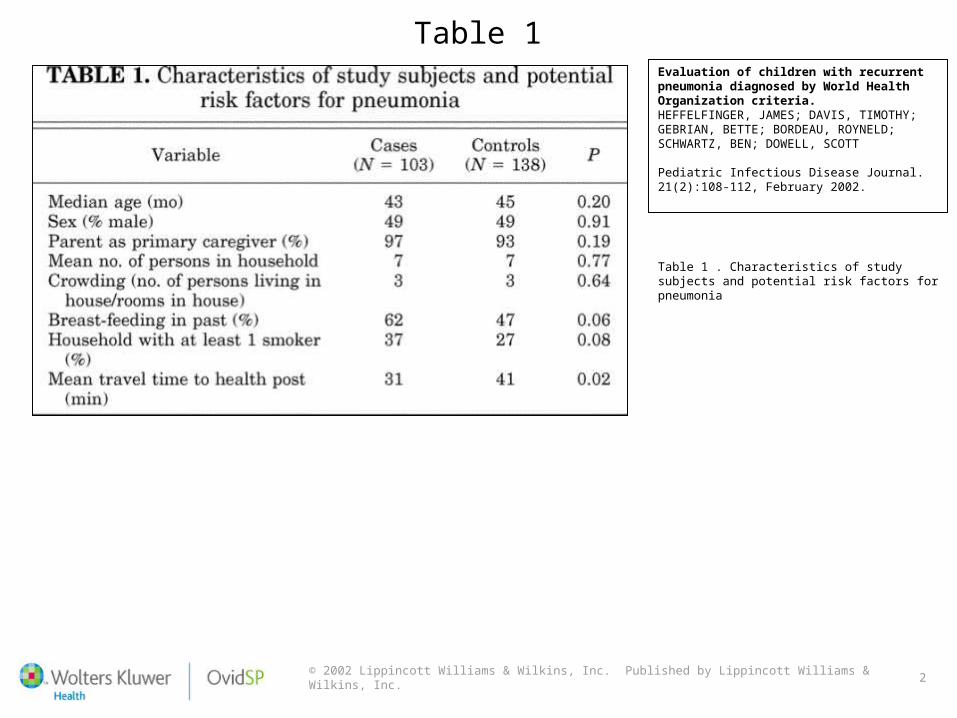
• Heffelfinger, et al., Peds Inf Dis Journal 2002– Screened for TB, immune deficiency, HIV– Most were sporadic– Only association was with Asthma
© 2002 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
Table 1Evaluation of children with recurrent pneumonia diagnosed by World Health Organization criteria.HEFFELFINGER, JAMES; DAVIS, TIMOTHY; GEBRIAN, BETTE; BORDEAU, ROYNELD; SCHWARTZ, BEN; DOWELL, SCOTT
Pediatric Infectious Disease Journal. 21(2):108-112, February 2002.
Table 1 . Characteristics of study subjects and potential risk factors for pneumonia

© 2002 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 4
Table 3Evaluation of children with recurrent pneumonia diagnosed by World Health Organization criteria.HEFFELFINGER, JAMES; DAVIS, TIMOTHY; GEBRIAN, BETTE; BORDEAU, ROYNELD; SCHWARTZ, BEN; DOWELL, SCOTT
Pediatric Infectious Disease Journal. 21(2):108-112, February 2002.
Table 3 . History of wheezing, matching for community health worker and adjusting for age
The Other Side • Adding simple markers like history of
previous respiratory distress and response to brochodilator therapy to the existing WHO guidelines it is possible to reliably differentiate pneumonia from acute exacerbation of asthma…. Bringing the overuse of antibiotics from 78.9% to 26.3% (p <0.001)
Redefining the WHO algorithm for DX of PNA w/Simple Additional MarkersSavitha MR. Khanagavi JB.
Indian Journal of Pediatrics. 75(6):561-5, 2008 Jun.

Diagnosis of Asthma
• Episodic symptoms of airflow obstruction or airway hyperresponsiveness are present– Cough– Wheeze– Difficulty breathing/chest tightness
• Airflow obstruction is at least partially reversible (low FEV1, low FVC, low flows)
• Alternative Diagnoses are excluded


“All that wheezes (or coughs) is not asthma”
• Allergic rhinitis• Foreign body• Vocal cord dysfunction• Vascular rings or
laryngeal webs• Laryngotracheomalacia• External compression by
lymph nodes or tumor
• Viral bronchiolitis• Obliterative bronchiolitis• Cystic fibrosis• Bronchopulmonary
dysplasia• Heart disease• Gastroesophageal reflux
with or without aspiration





Classification of Asthma
• Severity: The intrinsic intensity of the disease process– Intermittent– Persistent: Mild, Moderate, Severe
• Control: The degree to which manifestations are controlled
• Responsiveness: the ease with which control is achieved by therapy


Important Environmental Factors in Asthma control
• Tobacco Smoke exposure• Other irritants: auto exhaust, dust,
chemicals• Allergens
– Dust mites– Molds– Cockroach– Animal fur/dander (cat, dog, other)– Outdoor aeroallergens

Co-morbid Conditions
• GE reflux• Obstructive Sleep apnea• Rhinitis or Sinusitis• Stress and depression• Obesity• Allergic Bronchopulmonary Aspergillosis


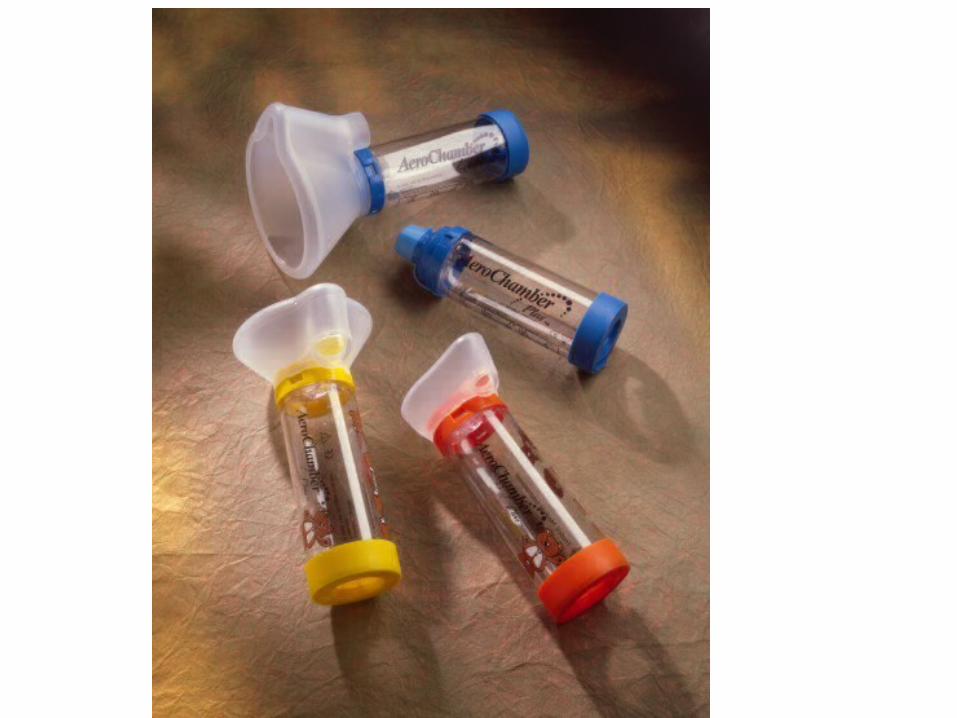
Short-acting Beta Agonist (SABA)
• Albuterol/Salbutamol in various forms– MDI can be used in all ages all severities– Nebulizer acceptable alternative
• Levalbuterol• SQ epi may still have a role

Inhaled Corticosteroids (ICS)
• Fluticasone• Budesonide• Others

Combination Inhalers (ICS + LABA)
• Advair– Fluticasone + Salmeterol
• Symbicort– Budesonide + Formoterol

Leukotriene inhibitors and others
• Montelukast• Cromolyn• Nedocromil

Sequential therapy
• Daily Controller Med– ICS, montelukast, etc based on steps
• SABA – up to every 6 hours as needed only
• Oral Prednisone, prednisolone, or methylpredniosolone short course: – 1 to 2 mg/kg/day x 5 days




Management of Acute Asthma Exacerbations
• Assessment• Oxygenation• Bronchodilators• Systemic Steroids• Adjunctive therapies


…and now Dr. Tina Slusher….

A 10-year old known asthmatic presents with 3 day history of cough, wheeze with exertion and mild dyspnea. Has not been user controller medicine. Feels better after albuterol inhaler use.

FEV1 = 60% predictedFVC = 100% predictedFEV1/FVC ratio = 60% predictedFEF 25-75 = 45% predictedPeak flow = 100%
A 7-year old with known asthma presents with an acute exacerbation and is tachyneic, with a respiratory rate of 60 bpm. You obtain an ABG:
pH/pCO2/pO2/bic
7.42/42/51/22
What is the most likely cause of hypoxemia?
How can CO2 and O2 be so disparately affected?
What level of monitoring is appropriate for this patient?


















