AET Symposium Management of Refractory Status Epilepticus December 1, 2012 Aristea S. Galanopoulou, MD PhD Albert Einstein College of Medicine, Bronx NY USA American Epilepsy Society | Annual Meeting
Transcript
AET Symposium Management of Refractory Status
Epilepticus December 1, 2012
Aristea S. Galanopoulou, MD PhD
Albert Einstein College of Medicine, Bronx NY USA
American Epilepsy Society | Annual Meeting
Disclosure
Novartis
Morgan & Claypool Publishers,
John Libbey Eurotext Limited,
Elsevier
NINDS NS078333, NS020253
Autism Speaks
American Epilepsy Society | Annual Meeting 2012
Speaker’s honorarium
Royalties for publications
Research Grants
Overall Learning Objectives
Recognize and initiate appropriate treatment algorithms for RSE for adults and pediatric patient populations.
Learn current theories on the basic mechanisms of RSE and apply this information in patient care.
Recognize when autoimmune and inflammatory pathogenic processes may underlie RSE and implement etiology-specific treatment protocols in patient care.
Recognize when emerging treatments for RSE may be helpful in the management of RSE patients.
American Epilepsy Society | Annual Meeting 2012
Case 1 30 year old man (70kg) with no prior history of illness or seizures:
- 6 pm: noted to have generalized tonic clonic seizure (GTC) activity, EMS was called
- 6:10 pm: EMS arrival: afebrile, normal BP, unresponsive with continuous seizure activity 4 mg lorazepam IV given no effect
- 6:25pm: arrival to the ER, continuous seizure activity repeat 4 mg lorazepam IV given no effect
- 6:30 pm: fosphenytoin 20 mg PE/kg IV infusion started
- 6:50 pm: still unresponsive, normal BP, with persisting seizure activity
American Epilepsy Society | Annual Meeting 2012
Management of refractory status epilepticus (RSE)
•Introduction Aristea S. Galanopoulou, MD PhD •Management of RSE in adults Andrea Rossetti, MD •Management of RSE in the pediatric population Tobias Loddenkemper, MD •Pathophysiology and treatment of RSE: lessons from animal models Claude Wasterlain, MD American Epilepsy Society | Annual Meeting 2012
Case 2 12 year old girl:
2 weeks prior to admission: fever, headache and upper respiratory symptoms
1 week later: progressive anxiety, insomnia, delusions and paranoia, and episodes of catatonia
On admission: temperature of 390C, oro-lingual-facial dyskinesias and right hand twitching were noted
EEG: continuous seizure activity maximal at the left hemisphere
CSF: lymphocytic pleocytosis, mildly increased protein, and negative bacterial cultures
Benzodiazepines and phenytoin load did not have any effect on abnormal movements and seizures
American Epilepsy Society | Annual Meeting 2012
Management of refractory status epilepticus (RSE)
•Paraneoplastic and autooimmune encephalitis resulting in RSE Josep Dalmau, MD PhD •The role of immune system in RSE: preclinical perspectives Annamaria Vezzani PhD •Future perspectives in the management of RSE Eugen Trinka, MD MSc •Conclusions Angus A. Wilfong, MD
American Epilepsy Society | Annual Meeting 2012
Management of Refractory
Status Epilepticus in Adults December 1st 2012
Andrea O. Rossetti, MD
Service de Neurologie, CHUV
Lausanne, Switzerland
American Epilepsy Society | Annual Meeting
8
Disclosure
Pfizer, UCB, Astra-Zeneca,
Eisai, Sandoz, GSK
American Epilepsy Society | Annual Meeting 2012
Research support
Several medications discussed in this presentation
are not FDA approved for status epilepticus
9
Learning Objectives
• To understand definition, frequency and prognosis of
refractory SE
•To tailor pharmacological treatment according to the
clinical situation
American Epilepsy Society | Annual Meeting 2012 10
Background
Prognosis
Treatment
Conclusion
Summary
11
Background
Prognosis
Treatment
Conclusion
Summary
12
Refractory SE: definition
SE resistant to 1st + 2nd line AED Holtkamp Lancet Neurol 2007
23%-43% of SE Mayer Arch Neur 2002, Novy Epilepsia 2010, Kellinghaus Epil Behav 2012
Most (17/29) RSE patients not in the ICU! Novy Epilepsia 2010
13
RSE etiologies
Novy Epilepsia 2010
• Up to 50% without previous seizures
14
Background
Prognosis
Treatment
Conclusion
Summary
15
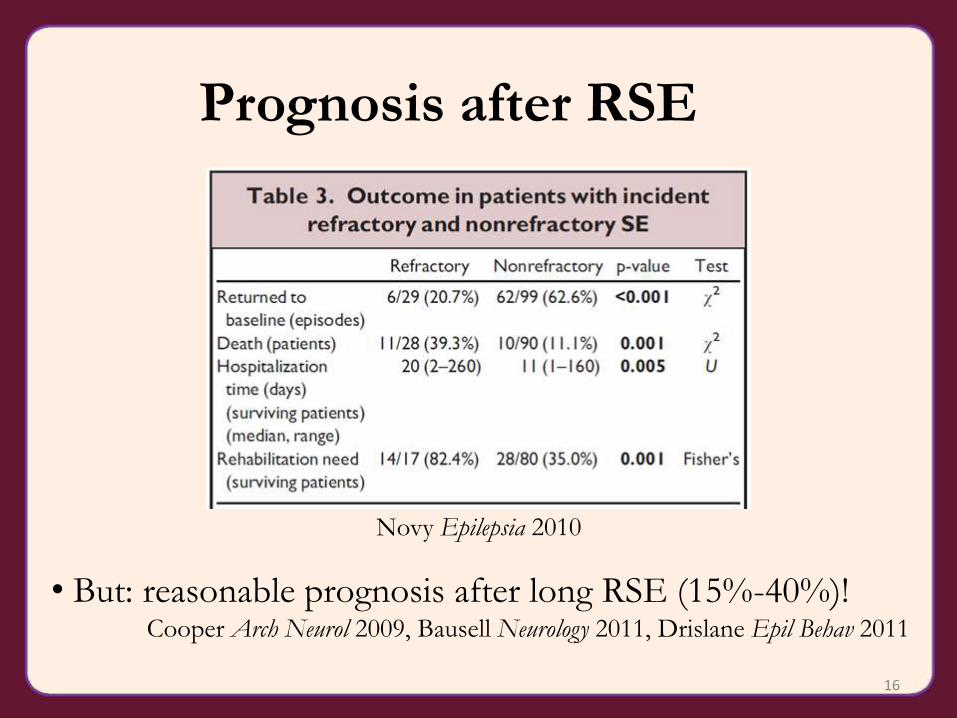
Prognosis after RSE
Novy Epilepsia 2010
• But: reasonable prognosis after long RSE (15%-40%)! Cooper Arch Neurol 2009, Bausell Neurology 2011, Drislane Epil Behav 2011