MANAGEMENT OF URETERIC STONE: A REVIEW OF 292 CASES1 By MILES Fox, M.D., Ch.M., F.R.C.S., L. N. PYRAH, C.B.E., DSc., Ch.M., F.R.C.S., and F. P. RAPER, F.R.C.S. Department of Urology, General Infirmary and St James’s Horpiial, Leeds THE management of stone in the ureter is frequently dependent on the combination of a number of factors which include size, position, and shape of the stone, pain, degree of obstruction and infection. In most cases the decision to carry out a certain method of treatment is not difficult, but in some a number of alternative ways of treatment is available, and in these cases con- siderable variations in the management have been recorded in the past. In the present paper a report has been made of the management of stone in the ureter in patients treated in the Department of Urology at the General Infirmary and St James’s Hospital, Leeds, over a five-year period, 1957 to 1962, and follow-up results are given. The main interest in the survey was to follow those cases in which treatment had been varied, to assess recovery of the urinary tract after different periods of obstruction and to correlate the results with the methods and timing of treatment. Case Material, Presentation, and Diagnosis.-There were 292 patients with ureteric stones in the present series ; 216 male and seventy-six female, a distribution of 2.8 to 1. Age and sex incidence according to age are shown in Figure 1. The mean age was 46 years ; the youngest patient was 15 and the oldest 71 years. The incidence was almost equal in both ureters, right 148 and left 141. Three patients had bilateral stones. Stones were most frequently arrested in the lower third of the ureter (Fig. 2) ; 61 per cent. (1 78) were in the lower third, 27 per cent. (seventy-nine) in the upper third, and 12 per cent. (thirty-five) in the middle third. Duration of symptoms varied between three hours and five years (Fig. 3) ; 80.5 per cent. of patients attended within one month of the onset of symptoms. Thirteen patients gave a history of one year or longer, which was probably attributable to the same stone. Pain was the usual presentation. Pain . 271 cases Painless hzmaturia . . 12 cases Urinary infection . . 2 cases Anuria , . 2 cases Incidental finding . . 5 cases Frank hzmaturia was reported in sixty-five patients and red cells on microscopy were seen in a further forty-two. Intravenous pyelography was performed while pain was present in 119 patients. When carried out in the acute state, pyelography yielded the most useful results, particularly if delayed films, up to twenty-four hours after injection, were taken. In most cases an outline of the affected collecting system down to the stone was eventually obtained and its position, degree of obstruction, and dilatation of the collecting system ascertained. The filled ureter often acted as a pointer to an opacity which would otherwise have been difficult to recognise as a stone (Figs. 4 and 5). Films taken after evacuation of the bladder and in the oblique position were useful (Figs. 6 and 7). Cystoscopy and passage of a ureteric catheter were carried out in ninety cases to confirm the diagnosis. Contrast medium was injected in eleven cases in which more information about the upper urinary tract was required or the presence of a radio-translucent stone was suspected. June 1965. Read at the Twenty-first Annual Meeting of the British Association of Urological Surgeons at London, 660
Transcript
MANAGEMENT OF URETERIC STONE: A REVIEW OF 292 CASES1
By MILES Fox, M.D., Ch.M., F.R.C.S., L. N. PYRAH, C.B.E., DSc., Ch.M., F.R.C.S., and F. P. RAPER, F.R.C.S.
Department of Urology, General Infirmary and St James’s Horpiial, Leeds
THE management of stone in the ureter is frequently dependent on the combination of a number of factors which include size, position, and shape of the stone, pain, degree of obstruction and infection. In most cases the decision to carry out a certain method of treatment is not difficult, but in some a number of alternative ways of treatment is available, and in these cases con- siderable variations in the management have been recorded in the past. In the present paper a report has been made of the management of stone in the ureter in patients treated in the Department of Urology at the General Infirmary and St James’s Hospital, Leeds, over a five-year period, 1957 to 1962, and follow-up results are given. The main interest in the survey was to follow those cases in which treatment had been varied, to assess recovery of the urinary tract after different periods of obstruction and to correlate the results with the methods and timing of treatment.
Case Material, Presentation, and Diagnosis.-There were 292 patients with ureteric stones in the present series ; 216 male and seventy-six female, a distribution of 2.8 to 1. Age and sex incidence according to age are shown in Figure 1. The mean age was 46 years ; the youngest patient was 15 and the oldest 71 years. The incidence was almost equal in both ureters, right 148 and left 141. Three patients had bilateral stones.
Stones were most frequently arrested in the lower third of the ureter (Fig. 2) ; 61 per cent. (1 78) were in the lower third, 27 per cent. (seventy-nine) in the upper third, and 12 per cent. (thirty-five) in the middle third. Duration of symptoms varied between three hours and five years (Fig. 3) ; 80.5 per cent. of patients attended within one month of the onset of symptoms. Thirteen patients gave a history of one year or longer, which was probably attributable to the same stone. Pain was the usual presentation.
Frank hzmaturia was reported in sixty-five patients and red cells on microscopy were seen in a further forty-two.
Intravenous pyelography was performed while pain was present in 119 patients. When carried out in the acute state, pyelography yielded the most useful results, particularly if delayed films, up to twenty-four hours after injection, were taken. In most cases an outline of the affected collecting system down to the stone was eventually obtained and its position, degree of obstruction, and dilatation of the collecting system ascertained. The filled ureter often acted as a pointer to an opacity which would otherwise have been difficult to recognise as a stone (Figs. 4 and 5). Films taken after evacuation of the bladder and in the oblique position were useful (Figs. 6 and 7). Cystoscopy and passage of a ureteric catheter were carried out in ninety cases to confirm the diagnosis. Contrast medium was injected in eleven cases in which more information about the upper urinary tract was required or the presence of a radio-translucent stone was suspected.
June 1965. Read at the Twenty-first Annual Meeting of the British Association of Urological Surgeons at London,
660
M A N A G E M E N T OF U R E T E R I C S T O N E
NUMBER OF PATIENTS
I50 -
100-
50-
0-
661
AGE INCIDENCE OF URETERIC STONE NUMBER OF
PATIENTS
0 MALES S FEMALES
510 10-19 20-29 30-39 40-49 50-59 60-69 70-79 YEARS
FIG. 1
POSITION OF URETERIC STONES
DURATION OF SYMPTOMS IN 292 PATIENTS WITH
STONES
NUMBER OF 40 PATIENTS
so I
FIG. 2
FIG. 3
662 B R I T I S H J O U R N A L O F UROLOGY
FtG. 4 FIG. 5
Fig. 4.-Plain X-ray. Small opacity right side of pelvis. Fig. 5.-Intravenous pyelogram, post-evacuation film, 11. hours after injection of contrast medium.
FIG. 6 FIG. I Fig. 6.--Jntravenous pyelogram. Three-hour film. Two opacities in line of ureter. Fig. 7.--lntravenous pyelogram. Three-hour film, oblique. The larger opacity is extra-ureteric.
M A N A G E M E N T O F U R E T E R I C S T O N E 663
MANAGEMENT
The methods of management are shown in Figure 8.
Spontaneous Passage.-In eighty-nine patients (30.5 per cent. of all cases) the ureteric stones were passed spontaneously (forty-seven from the left and forty-two from the right ureter). Adequate information was not available in nine cases.
Duration of’ Passage and Degree of Obstruction.-The time interval between onset of pain
FIG. 8 Management of ureteric stones. Ureteric catheter inserted in 30 per cent. for diagnostic and for therapeutic purposes. 18.6 per cent. stones subsequently passed.
NUMBER OF PATIENTS
FIG. 9
and passage of the stone is shown in Figure 9. It varied from two days to twelve months. The degree of initial urinary tract obstruction is also shown. The dark lines indicate cases (sixty-four) in which no radiological evidence of obstruction or only ureteric hold-up or mild hydronephrosis was present. The light spaces represent patients (sixteen) who had severe ureteric obstruction at the time of admission, marked by long delay in excretion, nephrogram effect, or considerable dilatation of the collecting system. All the patients with marked obstruction managed to pass their stones within one month. Severe obstruction in itself, therefore, did not appear to be a contra-indication to spontaneous passage.
Size of’Stone.--ln all but five cases the ureteric stone had one diameter smaller than 8 cm. No stone was passed with a diameter greater than 4 cm. ; 70 per cent. were in the lower third when first seen, 2 per cent. in the middle, and 28 per cent. in the upper third of the ureter. All
6 64 B R I T I S H J O U R N A L O F U R O L O G Y
the stones which passed within one week of the start of symptoms were situated in the lower third of the ureter. Thereafter there was no obvious relation between the position in which the stone was found and the length of time it took to pass.
Mild hydronephrosis was noted on only one occasion in a patient who had passed a stone two weeks previously and who also had a stone in one of the lower renal calyces. No relation was found between the degree of initial upper urinary tract dilatation, duration of passage, and return of the collecting system to normal, provided the stone passed spontaneously. Infection was not present in any of these cases.
Follow-up pyelography was performed in forty-six cases.
Ureteric Catheterisation.-In eighty-nine patients a ureteric catheter was passed usually as a diagnostic procedure, and withdrawn one to two hours later after X-rays had been taken. On twenty-four occasions a catheter was inserted beyond the stone and in two it was left in place for one and two days. There was no convincing evidence that this procedure speeded up the process of spontaneous passage. None of the stones passed ( 1 8.6 per cent.) was larger than cm. at its narrowest diameter.
Ureteric Basket.-In twenty patients an attempt was made to remove a low-lying stone with a ureteric basket. On sixteen occasions the attempt failed, usualiy as a result of inability to insert the basket past the stone. In twelve of these cases, however, the stone passed within one week afterwards. Extraction was successful on three occasions. The stones which were removed or subsequently passed were again all less than 4 cm. in diameter. The Council1 basket was used mainly in the first part of the survey, while later the Dormia basket was employed. In one case the Dormia basket, with the engaged stone, became impacted and finally broke when attempts were made to free it. Ureterolithotomy was required in the remaining case.
Ureteric Orifice Meatotomy.-Ureteric orifice meatotomy was performed on nineteen occasions. In all cases the stone was in the lowermost part of the ureter and the orifice was Edematous, or the stone was just visible at the ureteric orifice. In eighteen patients, the stone was passed within the succeeding seven days. Ureterolithotomy was required in the remaining case.
Uretero1ithotomy.-Ureterolithotomy was carried out in 109 patients. Distribution was almost equal on both sides (fifty-five on the right and fifty-one on the left). In three cases the stones were bilateral in the lower parts of the ureter. They were removed by a transperitoneal approach at one operation.
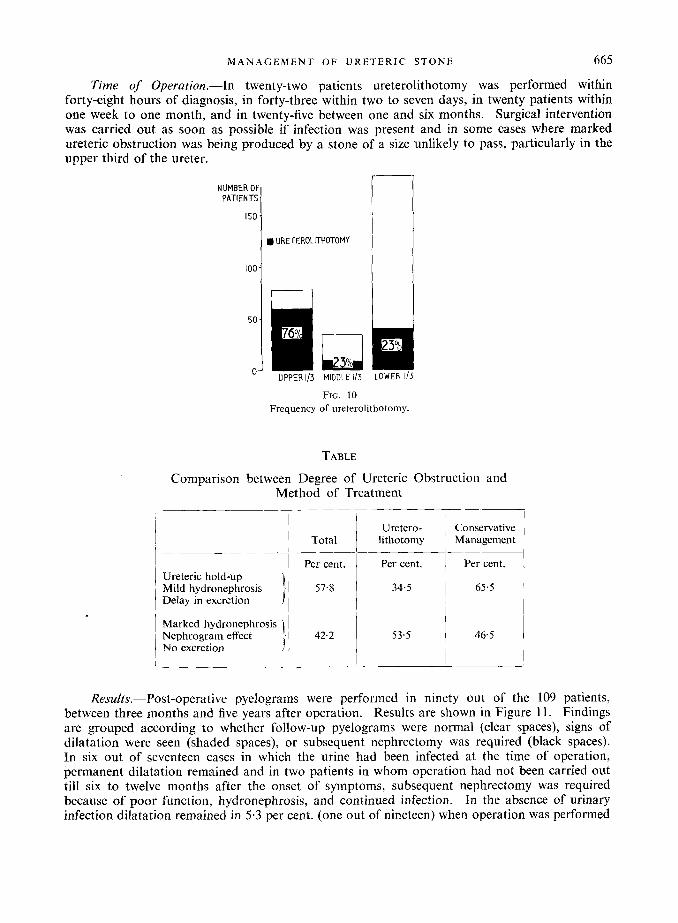
Position.-Figure 10 shows the distribution of all stones in this series among the three parts of the Ureter, and the proportion of cases in which open operation was performed. Operative removal was carried out most frequently when the stone was arrested in the upper third of the ureter-76 per cent., 23 per cent. in the middle third, and 23 per cent. in the lower third. Out of the whole series only 9 per cent. of stones which were cm. or smaller in diameter were operated on. Ureterolithotomy was required in 77 per cent. of cases when the stone was 4 cm. or larger. All stones with a diameter of cm. or more were removed by operation when arrested in the upper third of the ureter.
Degree of Obstruction.-The table shows a comparison between the severity of ureteric obstruction and frequency of operative and conservative management. The figures show that the degree of obstruction was not in itself the determining factor in the management.
Size of Stone.-No relation was found between the size of the stones and site of impaction in the ureter, except that only the very large calculi (over 2 cm.) were stopped in the middle portion. Stones impacted in the upper third of the ureter produced severe obstruction to urine flow twice as often as stones in the lower two-thirds.
M A N A G E M E N T OF U R E T E R I C S T O N E 665
Time of Operation.-Ln twenty-two patients ureterolithotomy was performed within forty-eight hours of diagnosis, in forty-three within two to seven days, in twenty patients within one week to one month, and in twenty-five between one and six months. Surgical intervention was carried out as soon as possible if infection was present and in some cases where marked ureteric obstruction was being produced by a stone of a size unlikely to pass, particularly in the upper third of the ureter.
100-
50.
0-
PATIENTS
I Total Conservative Uretero-
lithotomy Management
r l URETEROLITHOTOMY
GPER 113 MIDDLE ID LOWER 1/3
FIG. 10 Frequency of ureterolithotomy.
TABLE
Comparison between Degree of Ureteric Obstruction and Method of Treatment
1 1
I J
] Ureteric hold-up Mild hydronephrosis 1 Delay in excretion 1
I Marked hydronephrosis Nephrogram effect No excretion
Per cent.
57.8
42.2
Per cent. I 34.5
1 53.5
1 Per cent.
1 65.5
1 I 1 46.5
Results.-Post-operative pyelograms were performed in ninety out of the 109 patients, between three months and five years after operation. Results are shown in Figure 11. Findings are grouped according to whether follow-up pyelograms were normal (clear spaces), signs of dilatation were seen (shaded spaces), or subsequent nephrectomy was required (black spaces). In six out of seventeen cases in which the urine had been infected at the time of operation, permanent dilatation remained and in two patients in whom operation had not been carried out till six to twelve months after the onset of symptoms, subsequent nephrectomy was required because of poor function, hydronephrosis, and continued infection. In the absence of urinary infection dilatation remained in 5.3 per cent. (one out of nineteen) when operation was performed
666 B R I T I S H J O U R N A L O F U R O L O G Y
within one week of the onset of symptoms. In the group operated on after one and under four weeks, 11-1 per cent. (two out of eighteen) showed mild residual dilatation, 16.7 per cent. (three out of eighteen) between one and six months, and 33-3 per cent. (six out of eighteen) between six and twelve months. One patient in the last group finally required nephrectomy.
Stricture of the ureter occurred in two patients, mild in one, complete in another, necessitating re-implantation of the ureter into the bladder after three months (without residual dilatation). In another patient the lower third of the ureter became detached while being mobilised. It was re-implanted into the bladder at the same operation. After six months there was no obvious function and nephrectomy was carried out. In one patient a second stone became arrested at the site of the operation two months after ureterolithotomy, and surgical removal was again required.
Adequate records of the length and extent of post-operative urinary leakage through the
WSTOPERATWE IYP RESULTS COMPARED W i l H T M
BETWEEN ONSET OF NMPTONS AN) URETERCUTHOmm
0 NORMAL wEIM;RAM El DILATATION
SUBSEQUENT MPHRECTM
URINE mLE
IWEEK I-4WEEKS b6MOKMs M2"MS ~~ .
URNE NFECTED
OI 5
FIG. I I
incision are not available. If leakage did not subside spontaneously in about three weeks, it did so fairly promptly following insertion of a ureteric catheter which was [left in place for two to three days.
There was no mortality.
Nephrectomy.-Nephrectomy and ureterectomy was carried out in one patient as a primary procedure because of a large stone in the middle third of the ureter which had probably been there for a number of years. The kidney was hydronephrotic and infected. Nephrectomy was performed in two cases after ureterolit hotomy because of continuing infection.
Partial nephrectomy, because of stone in the lower pole of the kidney, was carried out in one patient at the same time as removal of a calculus from the upper third of the ureter. The kidney was edematous but this did not appreciably add to the difficulty of the operation and convalescence was uneventful.
Calculous Anuria.-Two patients were admitted with anuria because of a stone obstructing the ureter from a solitary kidney. A ureteric catheter could not be inserted past the stone in either case. Ureterolithotomy was carried out on the day of admission in one patient. The other had a blood urea of 380 mg. per cent. Hzmodialysis was performed the day he was admitted and the stone was removed two days later.
M A N A G E M E N T O F U R E T E R I C S T O N E 667
DISCUSSION
In 1935 Hinman stated that about 10 per cent. of ureteric stones were missed on urography. Besides non-opaque stones small calculi can easily be overlooked, especially in the middle and lower thirds of the ureter, and about 3 to 5 per cent. are invisible (Herman, 1938). Although in most cases the history is clear, in some it is atypical and the pain may closely mimic abdominal emergencies. Vague abdominal discomfort or only right iliac fossa pain with vomiting may occur, and in a percentage of cases there is no pain at all. A diagnosis of acute appendicitis with subsequent appendicectomy is a mistake which has been made fairly frequently. In 1930 Bumpus and Thompson reported mistaken appendicectomy in 26.8 per cent. of 1,001 patients, while as recently as 1945 Dourmashkin recorded 11.8 per cent. in 910 cases.
Accurate and prompt diagnosis is most important in the management of ureteric stone. It is achieved by the intravenous pyelogram carried out in the acute stage (Hellmer, 1935) and the use of delayed films (Pyrah, 1951). By establishing the site, size, shape, and degree of obstruction produced by the stone, it is possible to make an early decision whether conservative, manipulative, or operative treatment should be carried out, and to institute treatment without delay and thus avoid the danger of permanent damage to the urinary tract.
The following factors have to be considered in deciding on a course of management :- 1. Duratiori and Severity of Symptoms.-In a series of 5 IS cases reported by Sandegard (1956),
76 per cent. of the stones were passed spontaneously. Proportions of over 50 per cent. have been recorded by many other observers including Boeminghaus (1940), Arnesen (1940), Busch (1943), and Prentiss et al. (1952), while a considerably lower percentage (17.1) was reported by Higgins and Straffon (1963). Figures between 24 and 36 per cent. have been given in other, including recent large series (Chwalla, 1929 ; Hellstrom, 1935 ; Prince and Scardino, 1960 ; Fetter el al., 1963). In many cases one of the major deciding factors appears to be the waiting period deemed safe and practicable before endoscopic or operative measures are undertaken. In the present series 30.5 per cent. of stones were passed spontaneously and of these, one-third were passed between one month and one year after the onset of symptoms. A further 18.6 per cent. passed following insertion of a ureteric catheter, but it is not possible to determine whether this procedure had any significant influence on the passage of the stones.
I t is well known (Higgins, 1954) that the longer a stone stays in the ureter the less are its chances of spontaneous passage. A significant number, however, do pass after one month. Sandegard ( 1956) reported that 1 I per cent. of stones passed only one to eighteen months after diagnosis. In the present series it was shown that a stone could stay in the ureter for up to one year without producing residual damage, provided it was eventually passed spontaneously. Delay in operative treatment, however, if required, did lead to significant irrecoverable damage, even if no infection was present, when the waiting period was longer than one week from the onset of symptoms. A decision should therefore be made within about one week which stone is likely to pass spontaneously and which will not, so as to avoid the risk of permanent damage.
2. Size of’ Calculus.-Most observers agree that prognosis is influenced by the size of the stone (Sandegard, 1956), but there is marked divergence of opinion as to the actual dimensions. Joly (1929) advised medical treatment for patients who passed gravel or in whom the X-ray shadow was not larger than 5 to 10 mm. in diameter. Stevens and Collings (1930), Engel (19391, Brosig ( I 948), Davidson (1952), and Nation ( I 953) believed that spontaneous passage was probable if the stone was not larger than 1 cm. Others (Hellstrom, 1932 ; Foley, 1935 ; Priestley, 1954 ; Winsbury-White, 1954) have claimed that stones were unlikely to pass if larger than 4 cm., while Braasch (1917) advised against manipulative treatment if the stone was larger than 2 cm. Perlmann (1950) even stated that the size of the stone had no influence on the prospects of passage. However, in many reports it is not clear whether the measurement given refers to the length or width of the stone, and its shape and type of surface are given but rarely.
668 B R I T I S H J O U R N A L OF U R O L O G Y
In the present series 91 per cent. of stones f cm. or smaller at their narrowest diameter passed either spontaneously or with the help of endoscopic procedures. Ureterolithotomy was required in 77 per cent. of cases when the stone was 8 cm. in diameter or larger.
3. Position.-A large proportion of stones in the upper third of the ureter require removal by open operation. Foley (1935) and Priestley (1954) advised open operation for high stones with a diameter of B cm. or more, while Sargent (1954) suggested open operation for all high stones independent of size, unless they soon passed down the ureter. Sandegard (1956, 1958) found that about 50 per cent. of upper stones with a diameter between 4 and 6 mm. passed down the ureter, but when larger than 6 mm. they rarely moved. Similar findings were reported by Fetter et al. (1963).
In the present cases no stones 4 cm. or larger in diameter were passed when found in the upper part of the ureter. Some might have done so if left longer, but as obstructive symptoms were present more often and were usually more marked in the upper part of the ureter than elsewhere, early intervention appeared the safer course to follow. Smaller stones were carefully watched and if obstruction was present and the stone did not move soon, open operation was usually advised.
More conservative measures were adopted when the stone was in the lower parts of the ureter. If it was producing obstruction, not moving, and over 4 cm. in diameter, early open operation appeared the safest course to follow. From the results obtained it appeared that in these cases the period of waiting should not be longer than one week from the beginning of symptoms.
There has been a marked difference in the literature in the proportion of stones removed by endoscopic procedures. Figures as high as 93.3 per cent. have been recorded by Dourmashkin (1945) in 1,550 cases. He used metallic dilators for stones in the lower third of the ureter and aimed to dilate the ureter a t or below the level of the calculus, to or just above the size of the stone. Alyea (1938) removed 72 per cent. of 377 ureteric stones, some larger than 2 mm. at their narrowest diameter. Squires (1930) extracted 87-15 per cent. of stones in a series of 606 patients and Dodson et al. (1957) in a collected series of 4,947 found the proportion to be 68.2 per cent. More recently, considerably lower figures have been given by Fetter et a/. (1963), 48.1 per cent., while in Prince and Scardino’s 1960 series of 816 cases, endoscopic manipulation was attempted in only 31 per cent. and extraction was successful in 65.4 per cent. of these cases. It was noted, however, that in the unsuccessful cases 63 per cent. of the stones were passed subsequently.
In the present series endoscopic extraction, using either a Councill or a Dormia basket, was performed relatively infrequently (6.8 per cent.). In most cases the attempt was unsuccessful, but in many the stone when 4 cm. or smaller passed soon afterwards. Manipulation or dilatation of the ureter below the level of the stone probably accelerated its passage. The method has its dangers as pointed out by Rushe and Bacon (1940), Wishard (1943), Councill (1945), and Dodson et al. (1957). I t should not be used to try to remove stones from the upper or middle thirds of the ureter. When larger stones are present, ureterolithotomy offers a more certain, safer, and frequently more expeditious method of treatment.
4. Degree of Obstruction.-Some reports have indicated that obstruction of the ureter for even a short period may give rise to permanent renal damage (Kerr, 1954; Width, 1958), while case histories of patients with complete recovery of renal function after prolonged total obstruction have been recorded (Badenoch, 1963). Prince and Scardino (1960) believed that when a stone completely obstructs the ureter, immediate action should be taken to reinstate drainage by endoscopic or surgical measures.
The present results show that the chances of spontaneous passage are not necessarily related to the degree of obstruction. The smaller stones sometimes produce complete obstruction and they are subsequently passed spontaneously, without leaving residual damage. The size and position of the stone appear to be more important in determining management. However, if
MANAGEMENT O F URETERIC STONE 669
repeated X-rays reveal little or no progress in the descent of the stone and a progressively enlarging hydronephrosis, the obstruction should be relieved.
5. Infection.-In the presence of infection prompt relief of obstruction is required. Pyo- nephrosis with destruction of renal tissue soon occurs and the prognosis of the affected kidney rapidly deteriorates. Nephrectomy, together with removal of the dilated ureter, should be considered as a primary procedure if infection has been long-standing, and if marked dilatation and destruction of renal tissue are present.
6. Renal Function.-When a stone becomes impacted in the ureter from a solitary functioning kidney, operative intervention is required as a matter of emergency. If it is not possible to bypass the obstruction with a ureteric catheter when the blood urea is high, hzmo- dialysis will allow an elective operation to be carried out one to two days later.
7. Associated Renal Stone.-A stone may be washed from the kidney by the increased flow of urine after the relief of ureteric obstruction and may be arrested at the site of the uretero- lithotomy. Removal of the renal stone and partial nephrectomy if necessary, at the same time as ureterolithotomy will avoid this complication.
SUMMARY
The management of 292 patients with stone in the ureter treated jn the Department of Urology in Leeds between I957 and 1962 is described. Indications for conservative and operative procedures are discussed in the light of follow-up results.
REFERENCES
ALYEA, E. P. (1938). J . Urol., 40, 83. ARNESEN, A. (1940). Z . urol. Chir., 45, 94. BADENOCH, A. W. (1963). Brit. J . Urol., 35, 385. BOEMINGHAUS, H. (1940). “ Konservative und chirurgische Behandlung des Harnleitersteins.” (Leipzig :
BRAASCH, W. F. (1917). Surg. Gynec. Obstet., 24, 8. BROSIG, W. (1918). Beitv. klin. Chir., 177, 121. BUMPUS, H. C., and THOMPSON, G. J. (1930). Surg. Gynec. Obstet., 50, 106. BUSCH, F. (1943). Zbl. Chir., 70, 172. CHWALLA, R. (1929). Z . Urol. Chir., 26, 157. COUNCILL, W. A. (1945). J. Urol., 53, 534. DAVIDSON, G. R. (1952). Med. J. Ausst., 1, 840. DODSON, A. I., SIPE, W. R., and LORD, K. H. (1957). J. Urol., 78, 575. DOURMASHKIN, R. L. (1945). J . Urol., 54, 245. - ENGEL, W. J. (1939). Surg. Clin. N . Amer., 19, 1275. FETTER, T. R., ZIMSKIND, D. P., GRAHAM, R. H., and BRODIE, D. E. (1963). J. Amer. med. Ass., 186,21. FOLEY, F. E. B. (1935). J. Amer. med. Ass., 104, 1314. HELLMER, H. (1935). Acta radio1 (Stockh.), 16, 51. HELLSTROM, J. (1932). Hygiea (Stockh.), 94, 337.
~ (1935). Njur-och uretarsten. Nord. Kirurg. For. Furhandl. Kupenhafn. HERMAN, L. (1938). “ The Practice of Urology.” (Philadelphia : W. B. Saunders Co.) HIGGINS, C. C. (1954). In “ Urology.” Ed. by M. F. Campbell. (Philadelphia: W. B. Saunders Co.) HIGGINS, C. C., and STRAFFON, R. A. (1963). In “ Urology,” p. 746. Ed. by M. F. Campbell. (Philadelphia:
HINMAN, F. (1935). “ Principles and Practice of Urology.” (Philadelphia : W. B. Saunders Co.) JOLY, J. S. (1929). “ Stone and Calculous Disease of the Urinary Organs.” (London : Wm. Heinemann.) KERR, W. S. (1954). J. appl. Physiol., 6 , 762. NATION, E. F. (1953). J . Urol., 70, 373. PERLMANN, S. (1950). Z. Urol., 24, 303. PRENTISS, R. J., MULLENIX, R. B., and WHISENAND, J. M. (1952). Calif. Med., 7, 77. PRIESTLEY, J . T. (1954). Urol. Surv., 4, 49. PRINCE, C. L., and SCARDINO, P. L. (1960). J. Urol., 83, 561.
Georg Thieme Verlag).
W. B. Saunders Co.)
670 BRITISH J O U R N A L OF UROLOGY
PYRAH, L. N. (1951). Proc. Roy. Sac. Med., 44, 933. RUSHE, C. F., and BACON, S. F. (1940). J. Urol., 44, 177. SANDEGARD, E. (1956). Actu chit-. scand., Suppl. 219. __ (1958). Acra chir. xawd., 116,44. SARGENT, J. C. (1954). Postgrad. Med., 15, 238. SQUIRES, C. B. (1930). J. Urol., 24, 461. STEVENS, A. R., and COLLINGS, C. W. (1930). Amev. J. Suvg., 9, 484. WIDBN, T. (1958). Acta vadiol. (Stockh.), Suppl. 162. WINSBURY-WHITE, H. P. (1954). " Stone in the Urinary Tract." (London : Butterworth & Co. Ltd.) WISHARD, W. N. (1943). J. Urol., 50, 775.
DISCUSSION
Mr Turner Warwick (London) : Most of us would wish to endorse the value of the emergency intravenous pyelogram in confirming the diagnosis of ureteric colic. Unfortunately many radiodiagnostic departments are overworked and find difficulty in fitting in unhooked intravenous pyelograms without warning ; none, however, should find the " Casualty Officer's *' modified I.V.P. too burdensome. A straight X-ray alone is of little value in cases of suspected ureteric colic because it may or may not show an opacity which may or may not be in the ureter; while the pain is still present at least one I.V.P. film should be taken in addition. N o compression is used and fluid restriction is not essential. In most cases a thirty-minute film demonstrates the ureter distended down to an obstructing calculus which may not itself be visible. If a nephrogram only is defined on the side of the colic, a second post-voiding film is taken after two hours; if this also fails to demonstrate the site of the ureteric obstruction, a second injection of contrast is given and a further post-voiding film taken after six to eight hours (timing of additional films according to indications). An additional oblique film is occasionally indicated if, after voiding, a residual bladder shadow obscures a suspected calculus at the lower end of the ureter. The presence of some small opaque and non-opaque ureteric stones can best, and sometimes only, be diagnosed by intravenous pyelography during an attack of colic ; per contra, absence of ureteric obstruction at such a time excludes a diagnosis of ureteric colic. The single thirty-minute pyelo- gram usually provides all the information that is urgently required ; it is, however. not an alter- native to a full pyelogram which, if indicated, may be better postponed until the technique is not compromised by colic.
Conservative management of ureteric calculi of critical size is most usefully controlled by a series of single-film post-voiding thirty-minute pyelograms, repeated at suitable intervals of days or weeks. Other things being equal a stone which is not causing obstruction between attacks of colic can be treated conservatively for longer than one which is obstructing ; this fact cannot be determined from a straight X-ray and is considerably more important then the actual position of the calculus. The single-film pyelogram is also useful for checking the state of the upper tract before the patient leaves hospital after a urinary tract reconstruction.