Page 1
Robert O. Bonow, MD, MS
No Relationships to Disclose
Northwestern University Feinberg School of Medicine
Bluhm Cardiovascular Institute
Northwestern Memorial Hospital
Management of
Valvular Heart Disease
2016
Page 3
www.acc.org
www.americanheart.org
Evidence-based guidelines?
The majority of recommendations
are Level of Evidence C
Page 4
Stages of Valvular Heart Disease
Stage
A
B
C
D
Definition
Risk of valve disease
Mild - moderate asymptomatic disease
Severe valve disease but asymptomatic
C1: Normal LV function
C2: Depressed LV function
Severe, symptomatic valve disease
Page 5
Mitral regurgitation
Degenerative MR: primary valve disease
Functional MR: primary myocardial disease
Page 6
Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
Page 7
Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
Page 8
Chronic Mitral Regurgitation
Echo findings:
• Dilated left ventricle
• Normal LV systolic function
• Myxomatous leaflets with MVP
• Dilated left atrium
• Normal pulmonary artery pressure
• Severe mitral regurgitation
56 year old healthy man
Page 9
Chronic Mitral Regurgitation
56 year old healthy man
Issues:
• Surgery?
• Medical therapy?
• Transcatheter repair?
Page 10
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
Page 11
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
MV repair to improve survival?
What is the natural history?
?
Page 12
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
66% come to surgery in 5 years because of symptoms,
LV dysfunction, pulmonary hypertension or AF
Asymptomatic severe primary MR:
Page 13
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
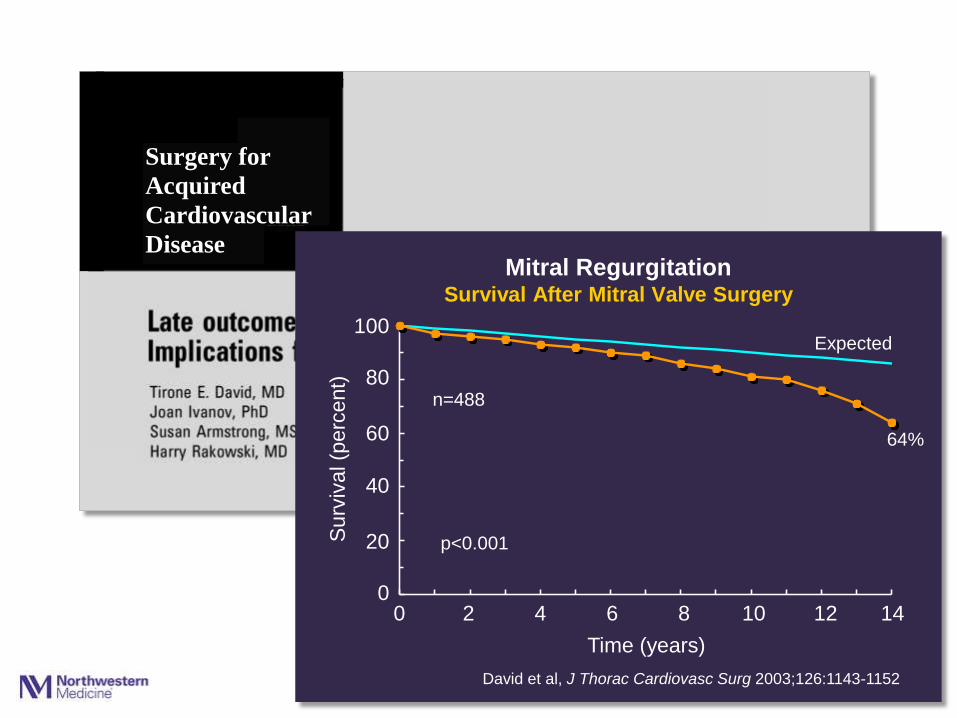
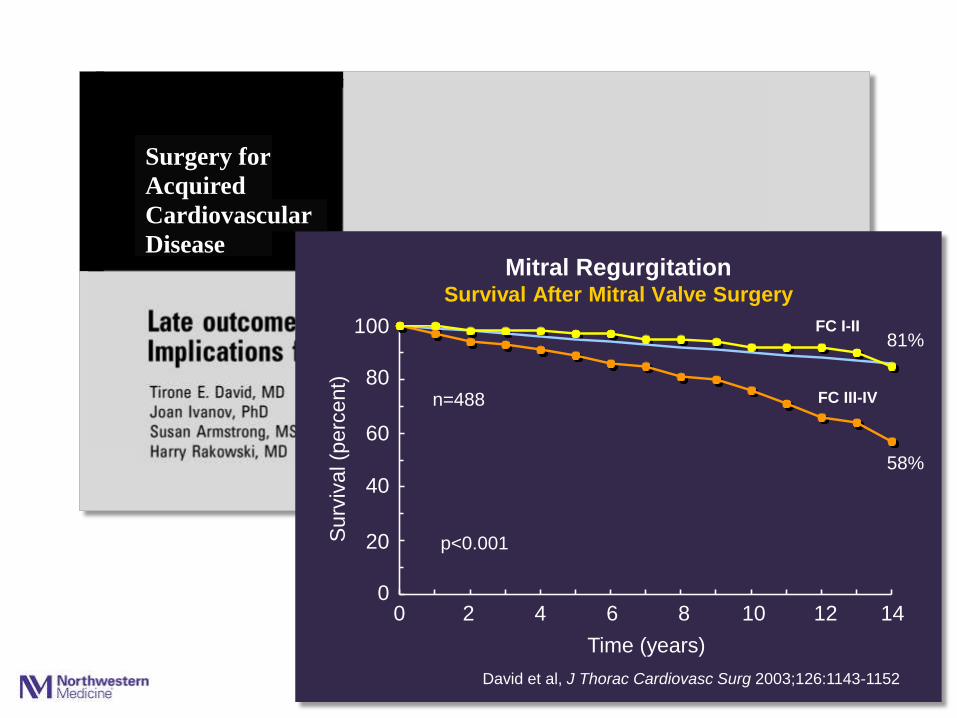
Severe primary MR:
Long-term postoperative survival is worse if surgery
is performed after patients become symptomatic
Page 14
J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
0 2 4 6 8 10 12
Time (years)
Expected
64%
n=488
p<0.001
Surgery for
Acquired
Cardiovascular
Disease
14
100
80
60
David et al, J Thorac Cardiovasc Surg 2003;126:1143-1152
Page 15
J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
0 2 4 6 8 10 14 12
Time (years)
David et al, J Thorac Cardiovasc Surg 2003;126:1143-1152
FC I-II
58%
FC III-IV
81%
n=488
p<0.001
Surgery for
Acquired
Cardiovascular
Disease
100
80
60
Page 16
J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
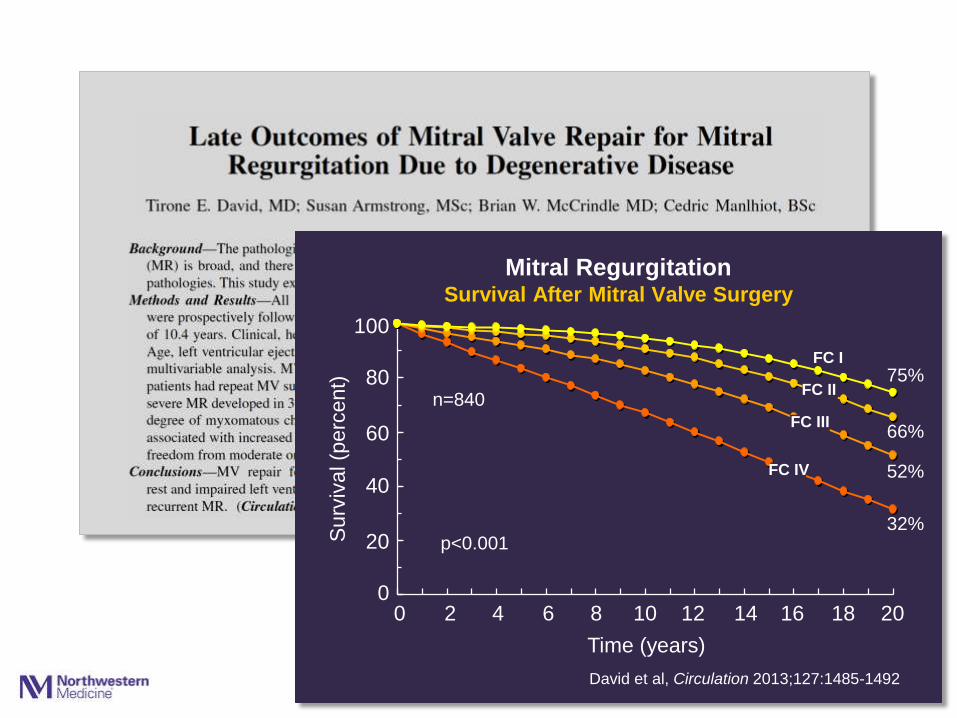
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
2 4 6 8 10 20 12
Time (years)
David et al, Circulation 2013;127:1485-1492
FC I
32%
75%
n=840
p<0.001
0 14 16 18
52%
66% 60
80
100
FC IV
FC III
FC II
Page 17
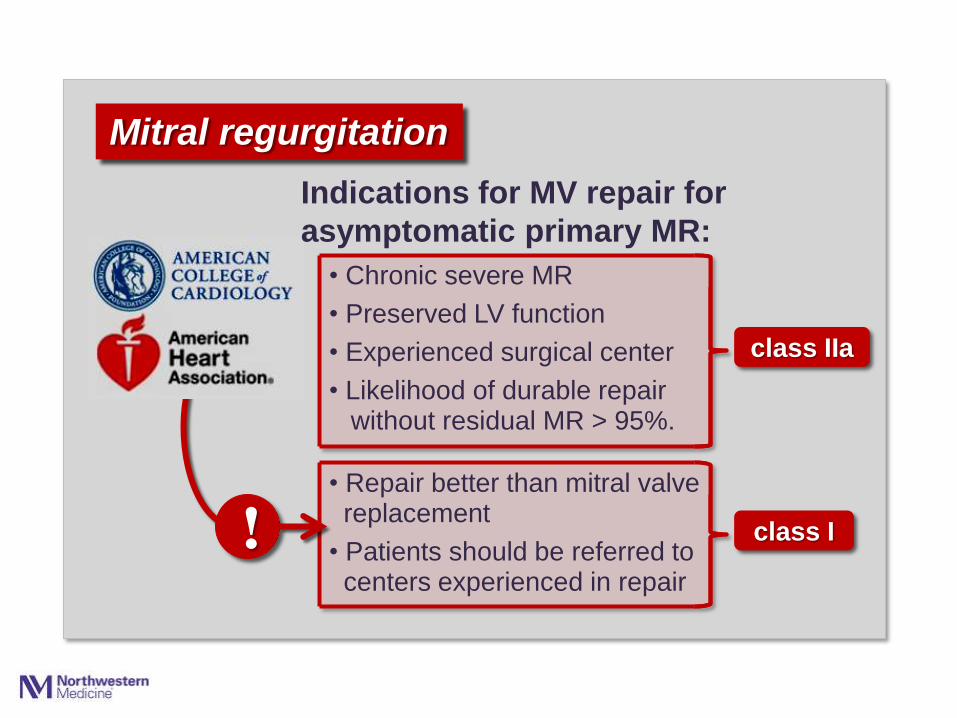
Mitral regurgitation
class IIa
class I !
Indications for MV repair for
asymptomatic primary MR:
• Repair better than mitral valve replacement
• Patients should be referred to centers experienced in repair
• Chronic severe MR
• Preserved LV function
• Experienced surgical center
• Likelihood of durable repair without residual MR > 95%.
Page 19
Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
• Diagnostic dilemmas
• Therapeutic dilemmas
Page 20
Imprecision in grading severity of secondary MR
What is “severe”
secondary MR?
Page 21
0
20
40
60
80
100
1 2 3 4 5 6 7 8
Surv
ival (p
erc
ent)
40
20
0
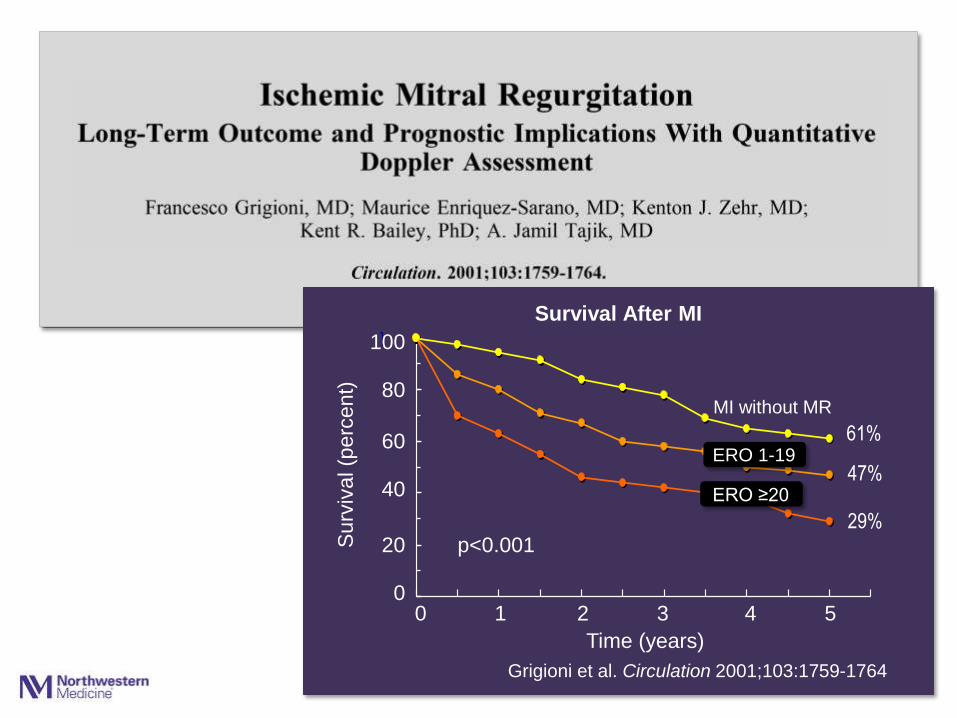
Grigioni et al. Circulation 2001;103:1759-1764
Time (years)
0 1 2 3 4 5
61%
47%
p<0.001 29%
Survival After MI
MI without MR
100
80
60 ERO 1-19
ERO ≥20
Page 22
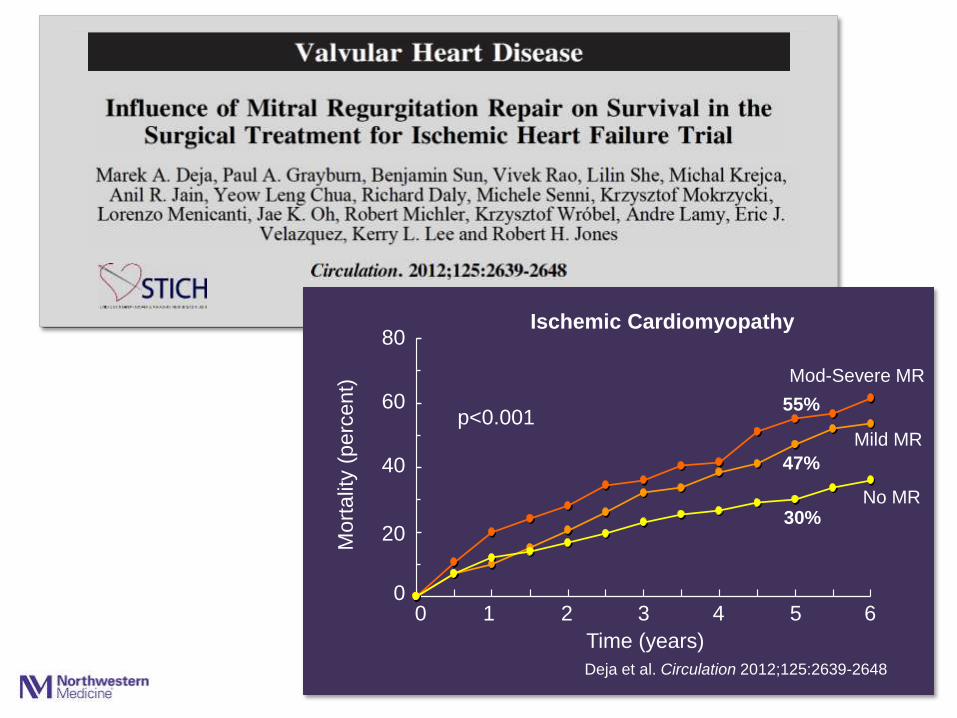
Deja et al. Circulation 2012
p<0.001
0
200
400
600
800
1 2 3 4 5 6 7 8
Ischemic Cardiomyopathy 80
0
Time (years)
0
60
40
20
Mort
alit
y (
perc
ent)
1 2 3 4 5 6
p<0.001
55%
47%
30%
Deja et al. Circulation 2012;125:2639-2648
No MR
Mild MR
Mod-Severe MR
Page 23
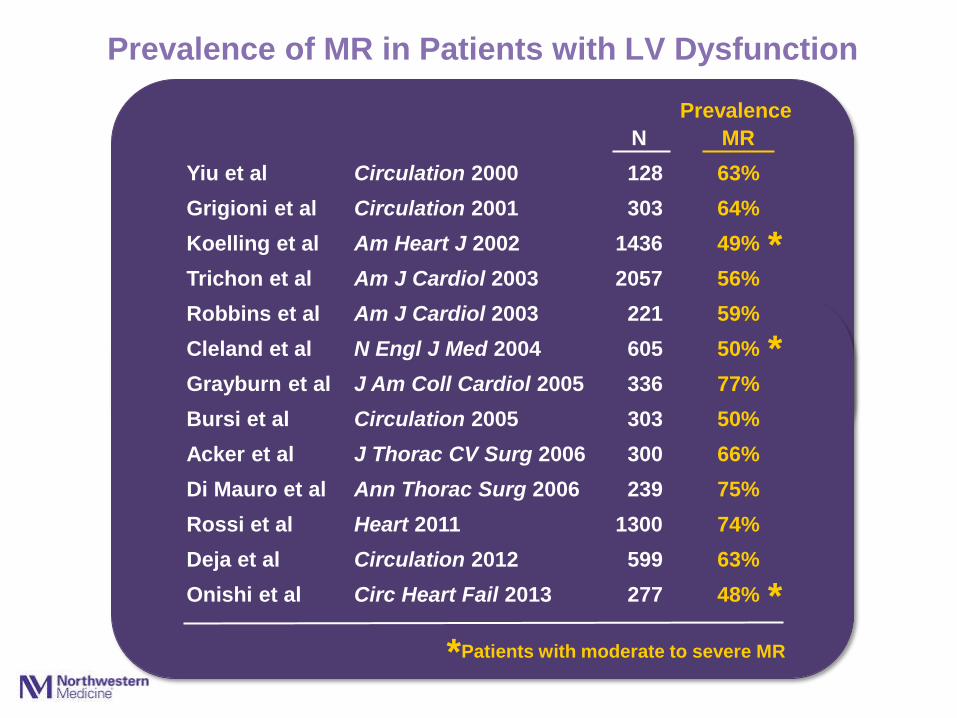
Prevalence of MR in Patients with LV Dysfunction
Prevalence
N MR
Yiu et al Circulation 2000 128 63%
Grigioni et al Circulation 2001 303 64%
Koelling et al Am Heart J 2002 1436 49%
Trichon et al Am J Cardiol 2003 2057 56%
Robbins et al Am J Cardiol 2003 221 59%
Cleland et al N Engl J Med 2004 605 50%
Grayburn et al J Am Coll Cardiol 2005 336 77%
Bursi et al Circulation 2005 303 50%
Acker et al J Thorac CV Surg 2006 300 66%
Di Mauro et al Ann Thorac Surg 2006 239 75%
Rossi et al Heart 2011 1300 74%
Deja et al Circulation 2012 599 63%
Onishi et al Circ Heart Fail 2013 277 48%
Patients with moderate to severe MR *
*
*
*
Page 24
Secondary mitral regurgitation:
…a marker of a sicker LV
- or -
…a contributor to a sicker LV?
Page 25
Secondary mitral regurgitation:
…a marker of a sicker LV
- or -
…a therapeutic target?
Therapies that produce beneficial
reverse remodeling also reduce
severity of functional MR
Page 26
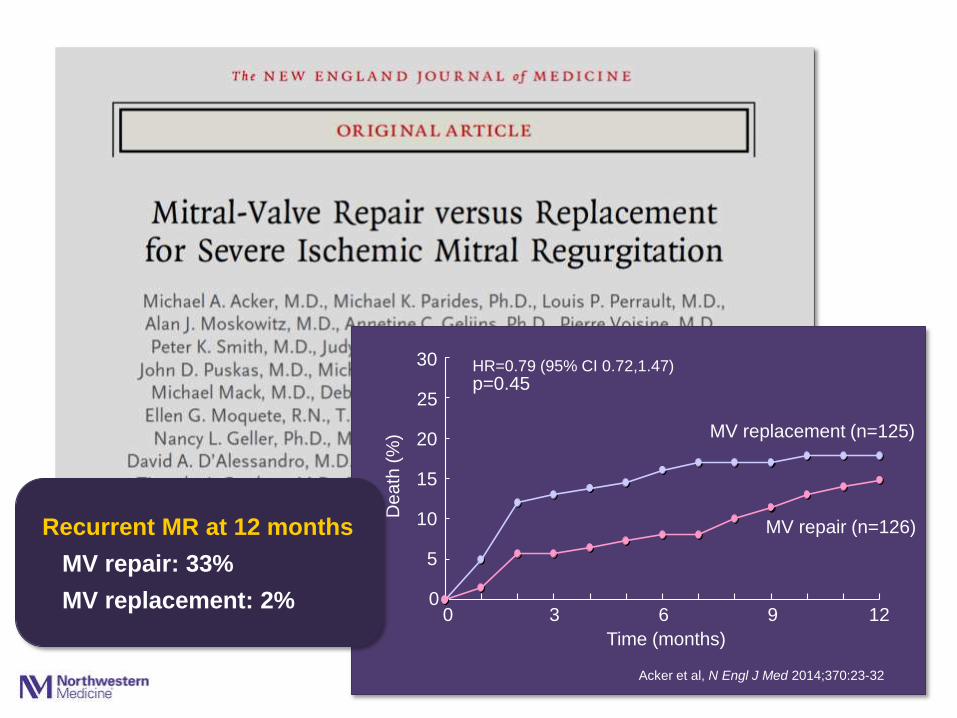
Secondary mitral regurgitation
can be repaired.
But should it be repaired?
… or replaced?
Unlike repair of myxomatous MR,
repair of secondary MR
is often not durable
Page 27
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8
30
20
15
10
5
0
De
ath
(%
)
Recurrent MR at 12 months
MV repair: 33%
MV replacement: 2% 0 3 6 9 12
Time (months)
Acker et al, N Engl J Med 2014;370:23-32
MV replacement (n=125)
MV repair (n=126)
p=0.45 HR=0.79 (95% CI 0.72,1.47)
25
Page 28
0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100100
80
60
40
20
0 LV
En
d-S
ysto
lic V
olu
me In
de
x (
mL
/m2)
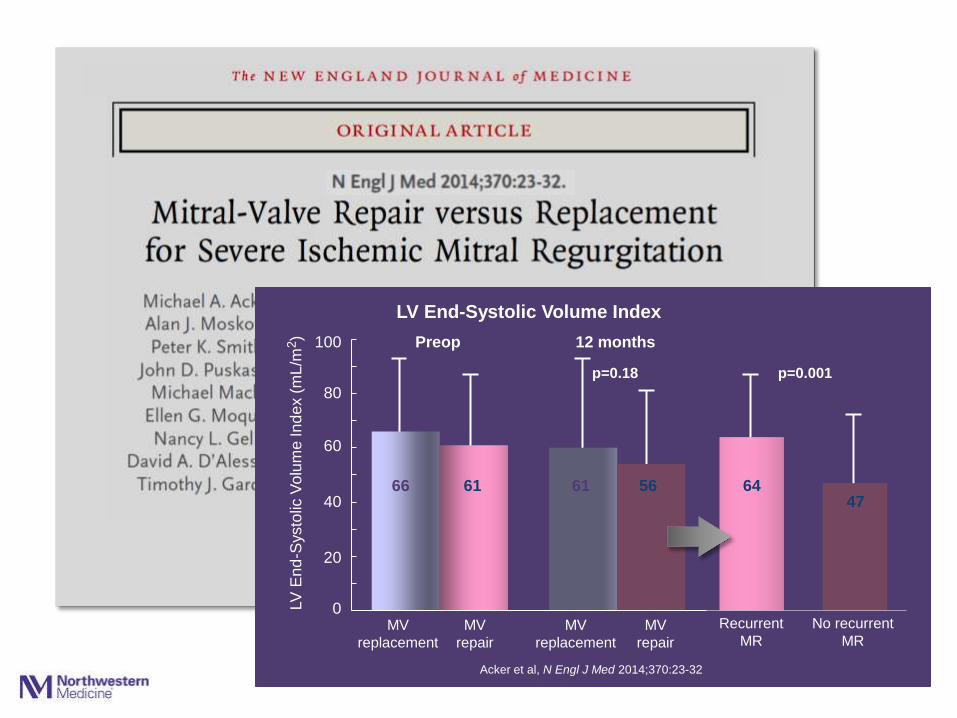
LV End-Systolic Volume Index
MV
replacement
MV
repair
MV
repair
MV
replacement
Preop 12 months
Recurrent
MR
No recurrent
MR
p=0.18 p=0.001
Acker et al, N Engl J Med 2014;370:23-32
66 61 61 56 64 47
Page 29
0
10
20
30
40
1 2 3 4 5 8 Time (months)
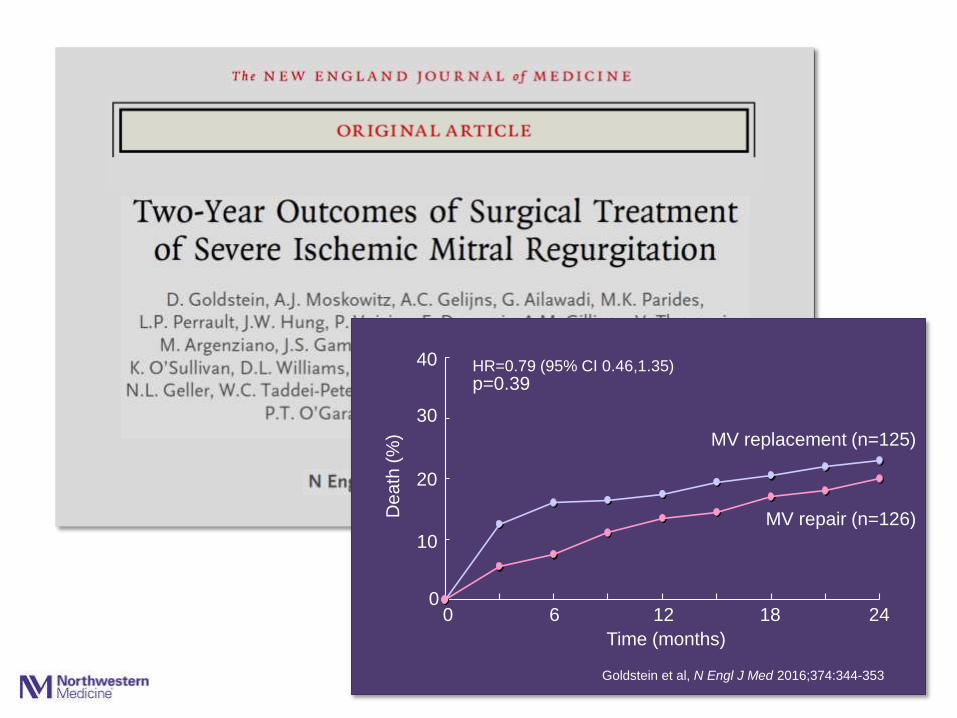
Goldstein et al, N Engl J Med 2016;374:344-353
40
30
20
10
0
De
ath
(%
)
0 6 12 18 24
MV replacement (n=125)
MV repair (n=126)
HR=0.79 (95% CI 0.46,1.35) p=0.39
Page 30
0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
70
60
50
40
30
20
10
0
Pe
rce
nt o
f P
atie
nts
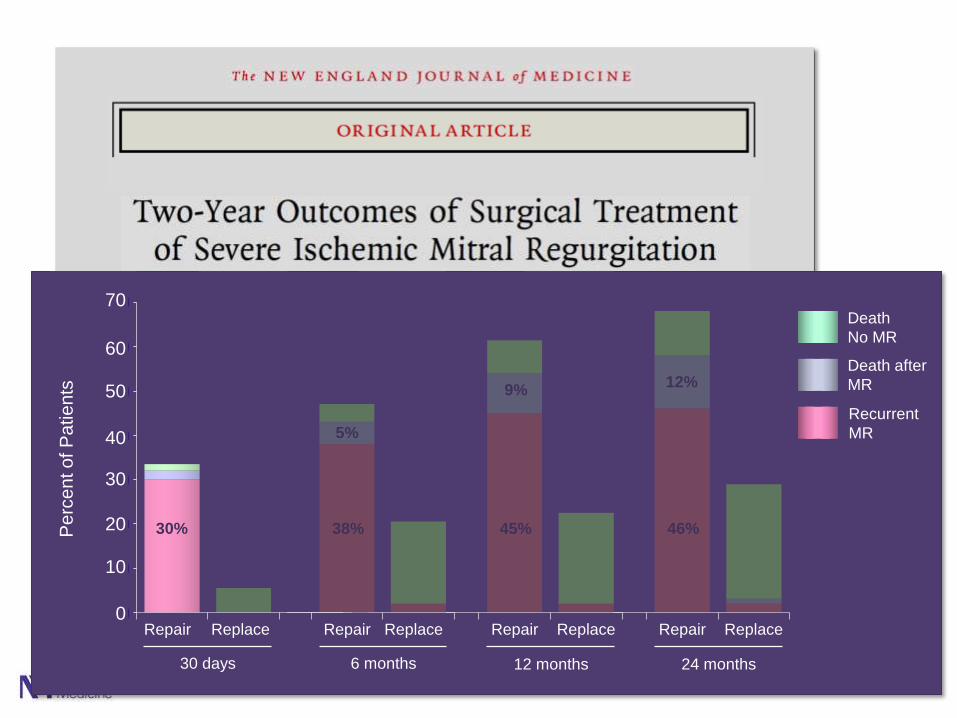
Recurrent
MR
Death
No MR
Repair Repair Repair Repair Replace Replace Replace Replace
30 days 6 months 12 months 24 months
30% 38% 45% 46%
5%
9% 12%
Death after
MR
Page 32
Indications for mitral valve surgery:
• Severe MR, persistent symptoms despite optimal medical therapy, including CRT
class IIb
• Patients with severe MR undergoing CABG or AVR
class IIa
Secondary mitral regurgitation
class I
• Patients with moderate MR undergoing CABG or AVR
class IIb
Guideline-directed medical
therapy for heart failure,
including CRT
Page 33
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999
684 hospitals
142,488 AVRs
Medicare data
0
2
4
6
8
10
12
14
16
86 87 88 90Age Group (years)
16
0
Pre
vale
nce (
perc
ent)
20-34
10
8
45-54 55-64 65-79 35-44 ≥80
4
Men
Women
6
2
14
12
Prevalence of Heart Failure
United States
Source: NHANES, CDC, and American Heart Association
Page 34
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999
684 hospitals
142,488 AVRs
Medicare data
0
2
4
6
8
10
12
86 87 88 90Age Group (years)
12
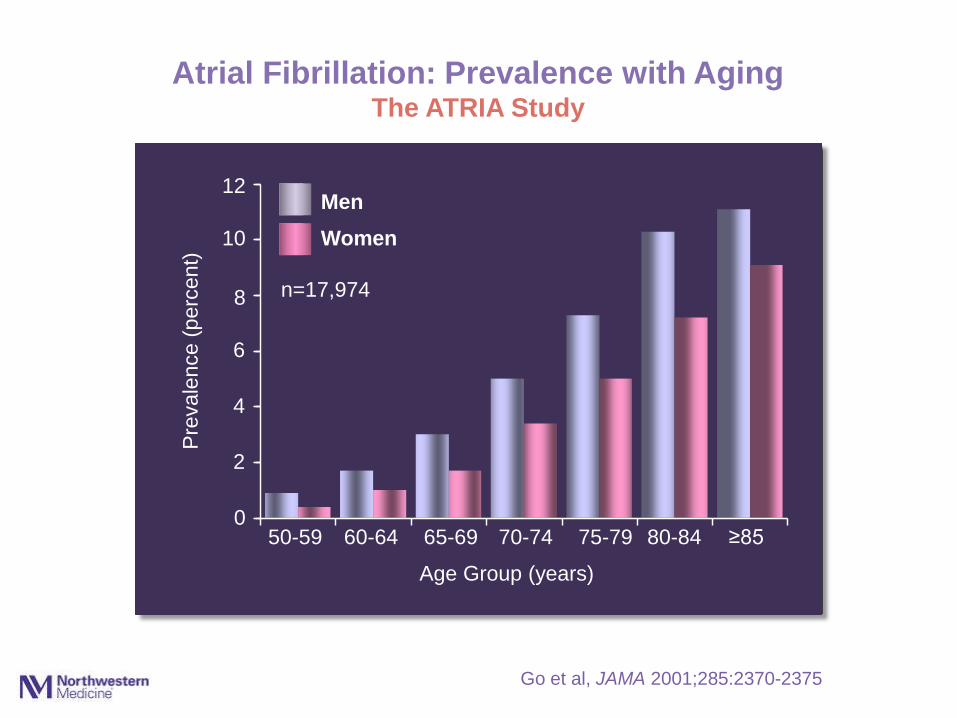
0 50-59
Atrial Fibrillation: Prevalence with Aging
The ATRIA Study
10
8
Go et al, JAMA 2001;285:2370-2375
65-69 75-79 80-84 60-64 70-74 ≥85
4
Men
Women
6
2
n=17,974
Pre
vale
nce (
perc
ent)
Page 35
0
10
20
30
40
50
60
70
80
90
100
86 87
0
10
20
30
40
50
60
70
80
90
100
86 87
100
80
60
40
20
0
Pe
rce
nt o
f P
atie
nts
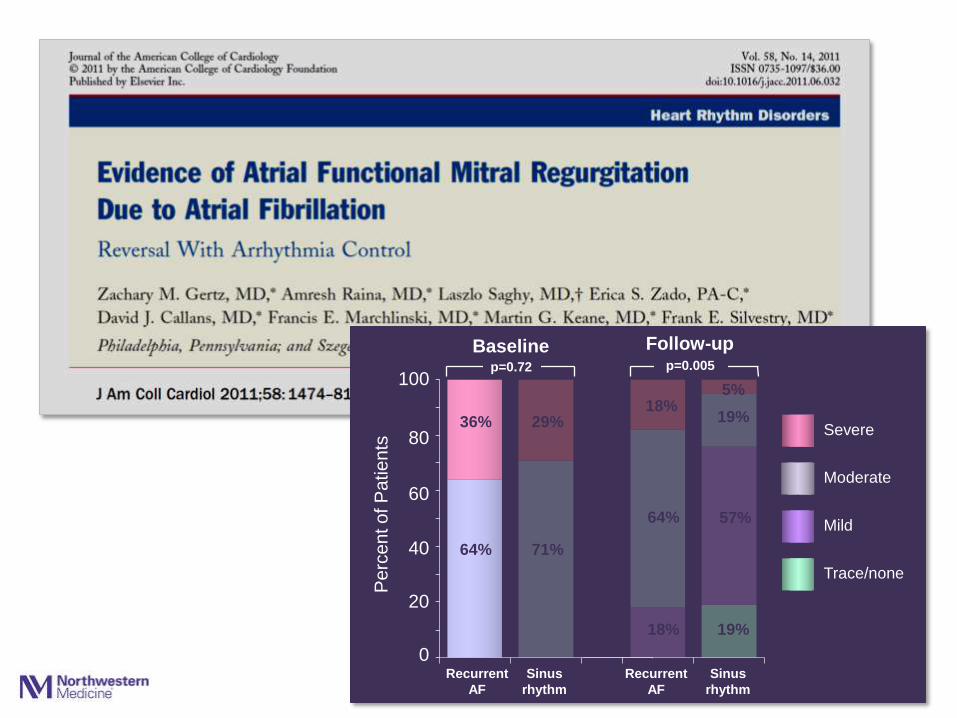
Recurrent
AF
Recurrent
AF
Sinus
rhythm
Sinus
rhythm
Baseline Follow-up p=0.005 p=0.72
Severe 36% 29%
71% 64%
Moderate
Mild
18%
18%
64%
19%
19%
57%
5%
Trace/none
Page 36
Lancet 2006;368:1005-1011
0
1
2
3
4
5
6
7
8
9
10
1 2 3
Perc
ent
Nkomo et al, Lancet 2006;368:1005-1011
7.3
9.6
2
4
8
10
0
Olmstead County (n=16,501)
<45 45-54 55-64 65-74 ≥75
Age
ARIC, CHS, CARDIA (n=11,911)
28,412 subjects
6
Moderate-Severe Mitral Valve Disease
Page 37
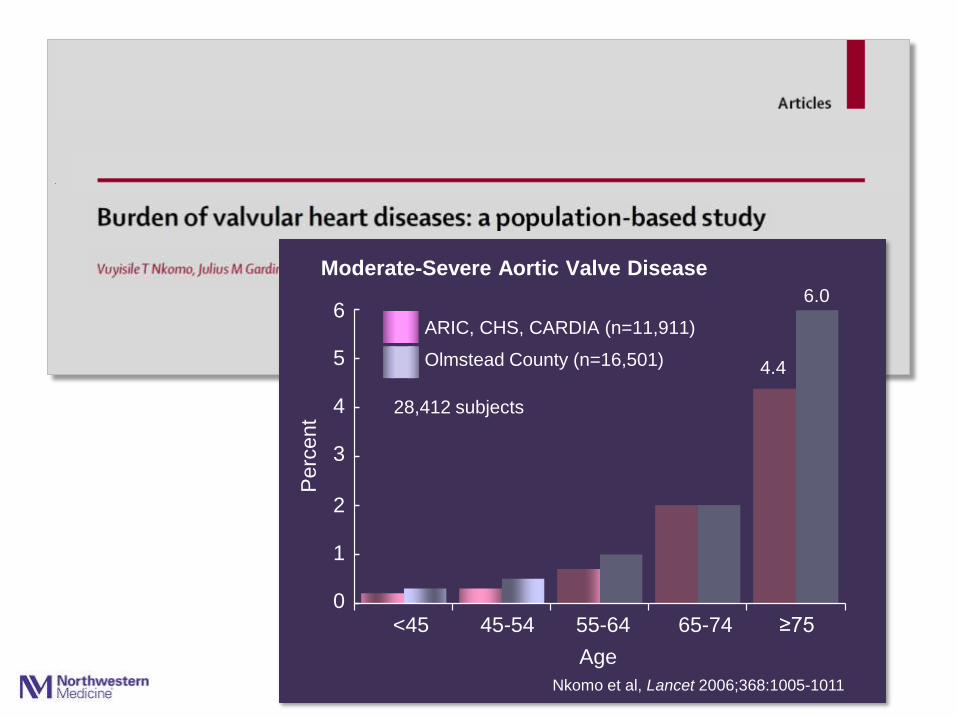
Lancet 2006;368:1005-1011
0
1
2
3
4
5
6
1 2 3
Nkomo et al, Lancet 2006;368:1005-1011
6.0
4.4
4
6
0
Olmstead County (n=16,501)
<45 45-54 55-64 65-74 ≥75
Age
ARIC, CHS, CARDIA (n=11,911)
28,412 subjects
Perc
ent
5
3
1
2
Moderate-Severe Aortic Valve Disease
Page 38
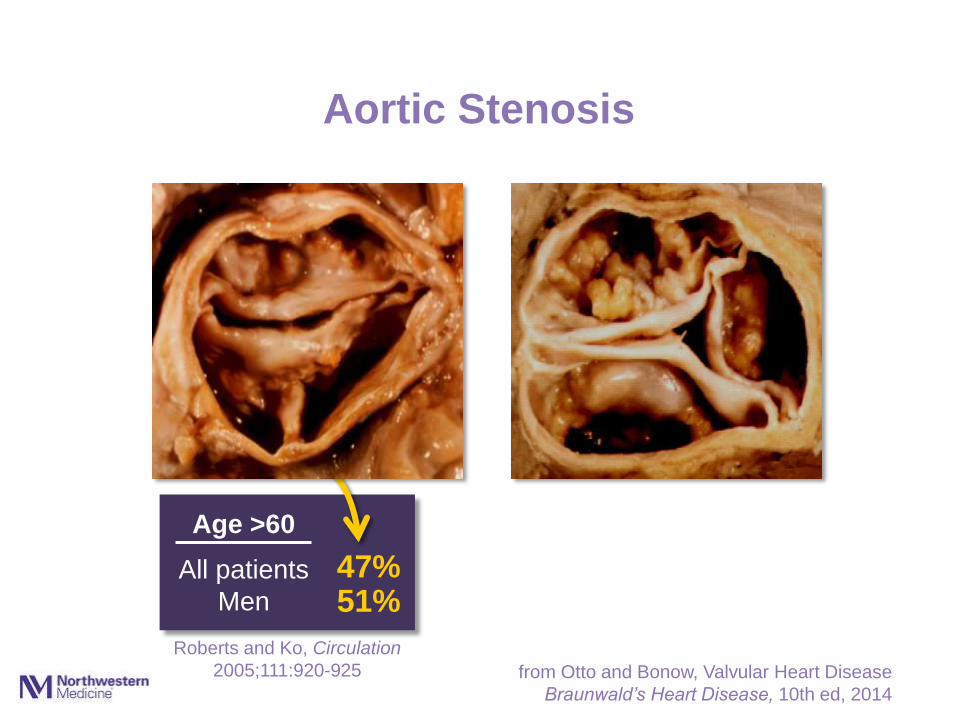
Aortic Stenosis
Age >60
All patients
Men
Roberts and Ko, Circulation
2005;111:920-925
47% 51%
from Otto and Bonow, Valvular Heart Disease
Braunwald’s Heart Disease, 10th ed, 2014
Page 39
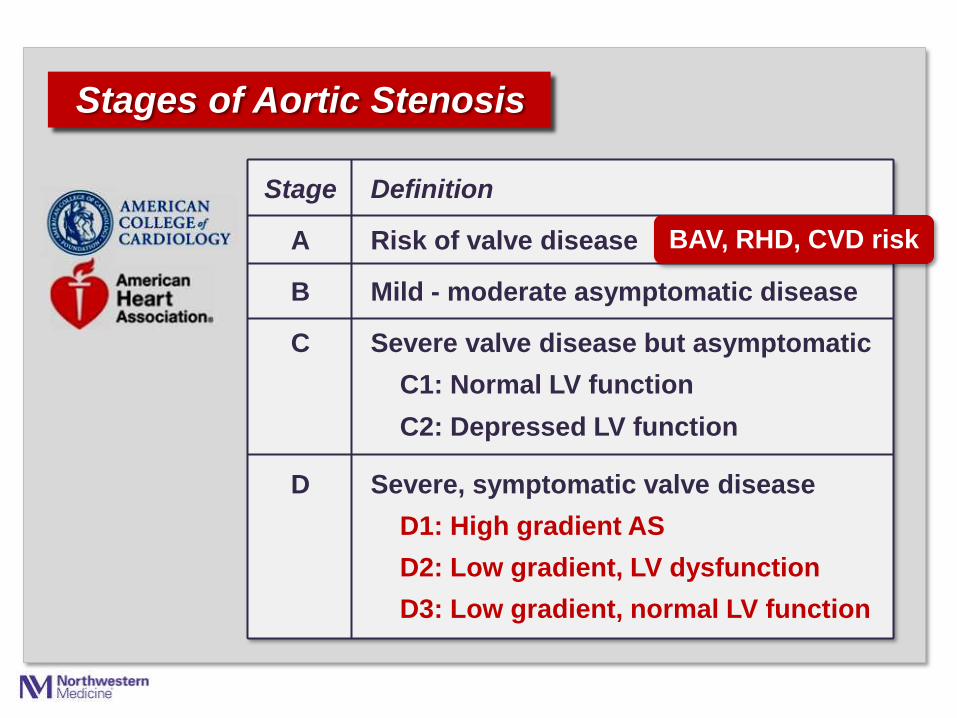
Stages of Aortic Stenosis
Stage Definition
A Risk of valve disease
B Mild - moderate asymptomatic disease
C Severe valve disease but asymptomatic
C1: Normal LV function
C2: Depressed LV function
D Severe, symptomatic valve disease
D1: High gradient AS
D2: Low gradient, LV dysfunction
D3: Low gradient, normal LV function
BAV, RHD, CVD risk
Page 41
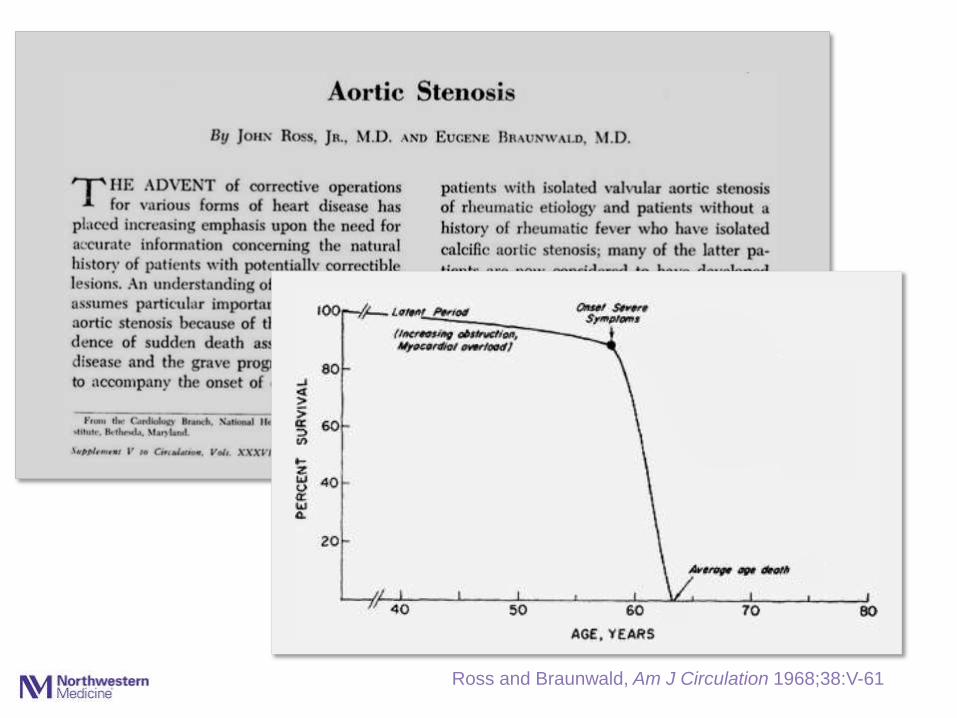
… the grave prognosis that appears to
accompany the onset of certain symptoms
Ross and Braunwald, Am J Circulation 1968;38:V-61
Page 42
Ross and Braunwald, Am J Circulation 1968;38:V-61
Page 43
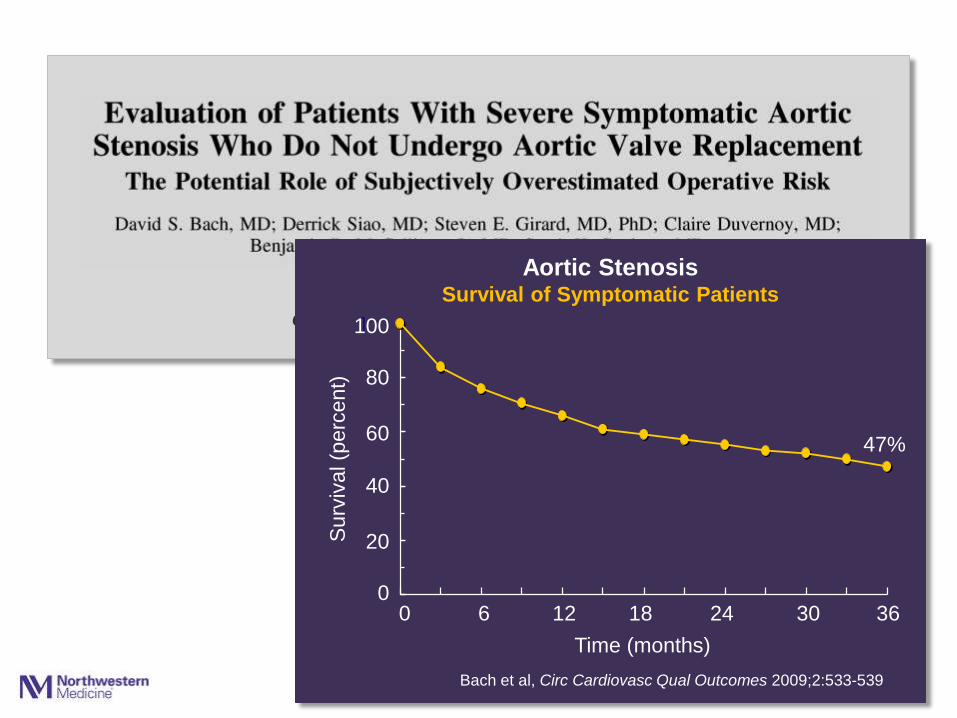
Circ Cardiovasc Qual Outcomes 2009;2:533-539
0
20
40
60
80
100
0 1 2 3 4
Surv
ival (p
erc
ent)
40
20
0
Bach et al, Circ Cardiovasc Qual Outcomes 2009;2:533-539
0 6 12 18 24 30 36
47%
Time (months)
Aortic Stenosis Survival of Symptomatic Patients
60
80
100
Page 44
Indications for AVR
• Symptomatic patients with severe AS
Aortic Stenosis
class I
Page 45
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Aortic Stenosis
Page 46
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Aortic Stenosis
Page 47
Aortic stenosis
Indications for valve replacement
Exercise test results:
• Symptoms
• Hypotension
class I
class IIa
Should asymptomatic patients
with severe AS undergo AVR?
…when they are really asymptomatic?
Page 48
Aortic Stenosis
84 year old man with severe AS
• Watchful waiting?
• More data (more testing)?
• Aortic valve replacement?
Page 49
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
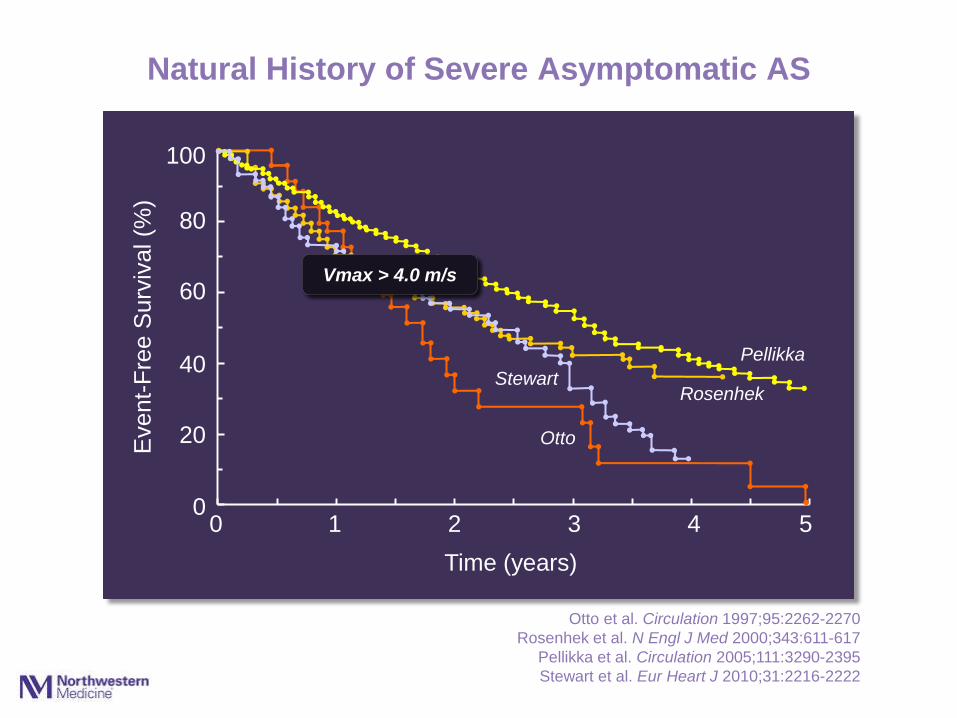
Natural History of Severe Asymptomatic AS
Time (years)
Otto et al. Circulation 1997;95:2262-2270
Rosenhek et al. N Engl J Med 2000;343:611-617
Pellikka et al. Circulation 2005;111:3290-2395
Stewart et al. Eur Heart J 2010;31:2216-2222
Pellikka
Otto
Stewart Rosenhek
Vmax > 4.0 m/s
Page 50
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
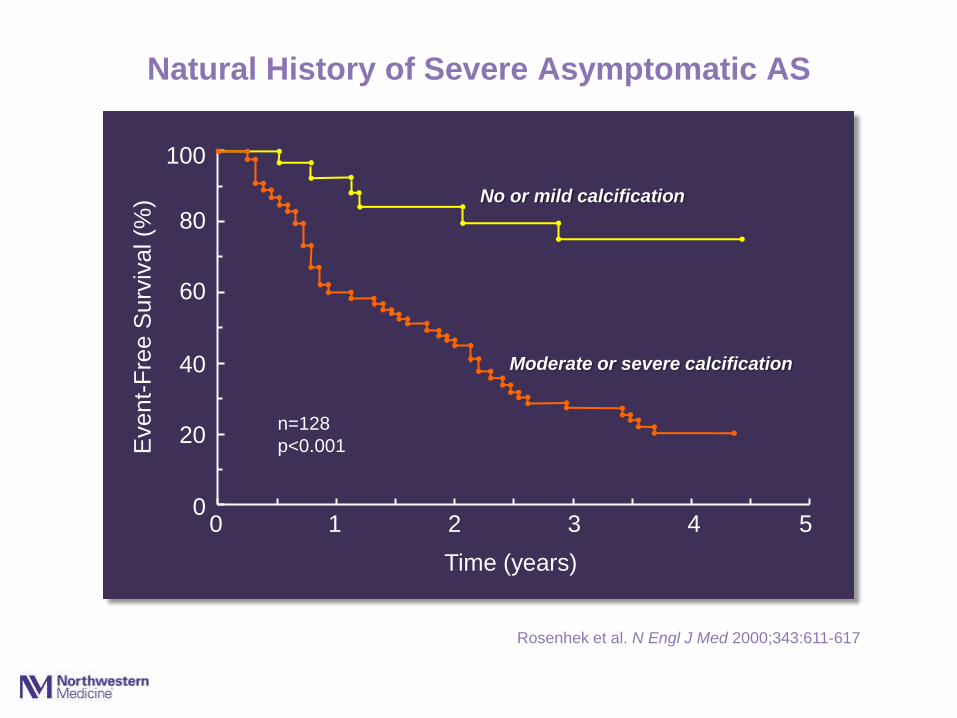
Natural History of Severe Asymptomatic AS
Time (years)
Rosenhek et al. N Engl J Med 2000;343:611-617
Moderate or severe calcification
No or mild calcification
n=128
p<0.001
Page 51
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Natural History of Severe Asymptomatic AS
Time (years)
Vmax 5.0 – 5.5 m/s
Vmax >5.5 m/s
Vmax 4.0 – 5.0 m/s
Rosenhek et al. Circulation 2010;121:151-156
n=198
p<0.001
Page 52
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
What is the risk of death while
waiting for symptoms to trigger AVR?
Aortic Stenosis
Page 53
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Surv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
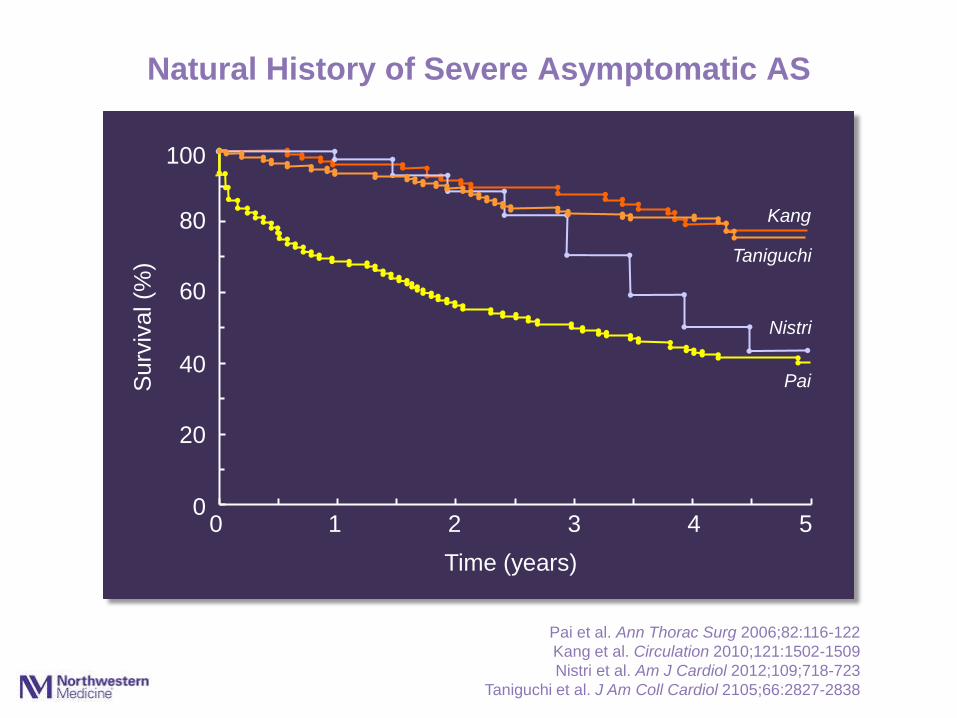
Natural History of Severe Asymptomatic AS
Time (years)
Pai et al. Ann Thorac Surg 2006;82:116-122
Kang et al. Circulation 2010;121:1502-1509
Nistri et al. Am J Cardiol 2012;109;718-723
Taniguchi et al. J Am Coll Cardiol 2105;66:2827-2838
Pai
Kang
Nistri
Taniguchi
Page 54
Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Surv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Time (years)
Conservative (n=291)
AVR (n=291)
Taniguchi et al. J Am Coll Cardiol 2105;66:2827-2838
85%
74% Taniguchi
31% of patients who developed
symptoms did not have AVR
17 deaths
Natural History of Severe Asymptomatic AS
Page 55
class IIb
class IIa
Aortic stenosis
Indications for valve replacement
in asymptomatic patients:
• Very severe AS:
Vmax ≥5 m/s
• Rapid progression and low
surgical risk
Page 56
Aortic stenosis
The ACC/AHA guidelines have
lowered the threshold for surgery
in asymptomatic patients with AS
• Severity of AS
• Severity of calcification
• Left ventricular function
• Exercise response
• BNP?
Page 57
Aortic stenosis
…but there needs to be
renewed emphasis on the
class I indications for
surgery in symptomatic
patients with severe AS
The ACC/AHA guidelines have
lowered the threshold for surgery
in asymptomatic patients with AS
Page 58
Aortic stenosis
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Page 59
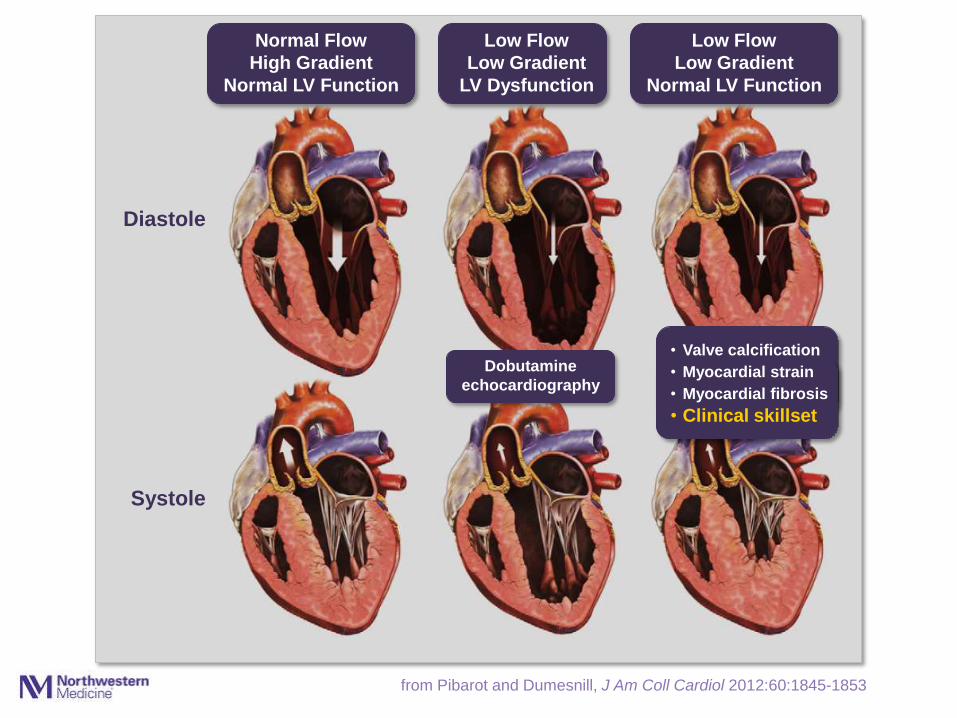
from Pibarot and Dumesnill, J Am Coll Cardiol 2012:60:1845-1853
Diastole
Systole
Normal Flow
High Gradient
Normal LV Function
Low Flow
Low Gradient
LV Dysfunction
Low Flow
Low Gradient
Normal LV Function
Dobutamine
echocardiography
• Valve calcification
• Myocardial strain
• Myocardial fibrosis
• Clinical skillset
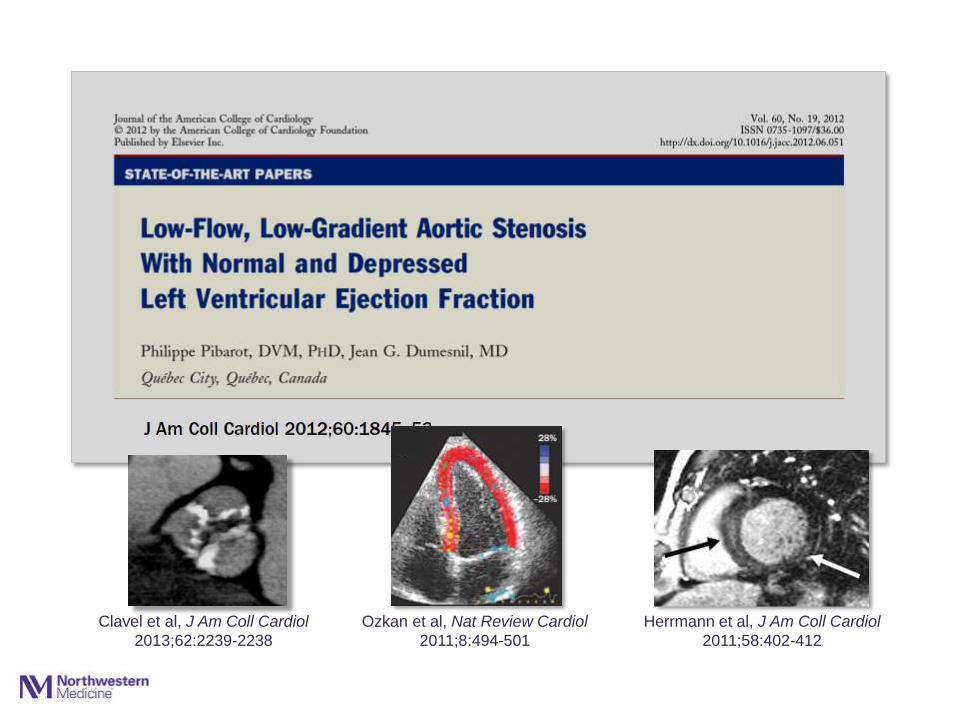
Page 61
Clavel et al, J Am Coll Cardiol
2013;62:2239-2238
Ozkan et al, Nat Review Cardiol
2011;8:494-501
Herrmann et al, J Am Coll Cardiol
2011;58:402-412
Page 62
class IIa
Low Flow, Low Gradient Aortic Stenosis
Indications for valve replacement:
• Normal EF, if clinical,
hemodynamic and anatomic
data support severe AS
Page 63
Aortic stenosis
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Page 64
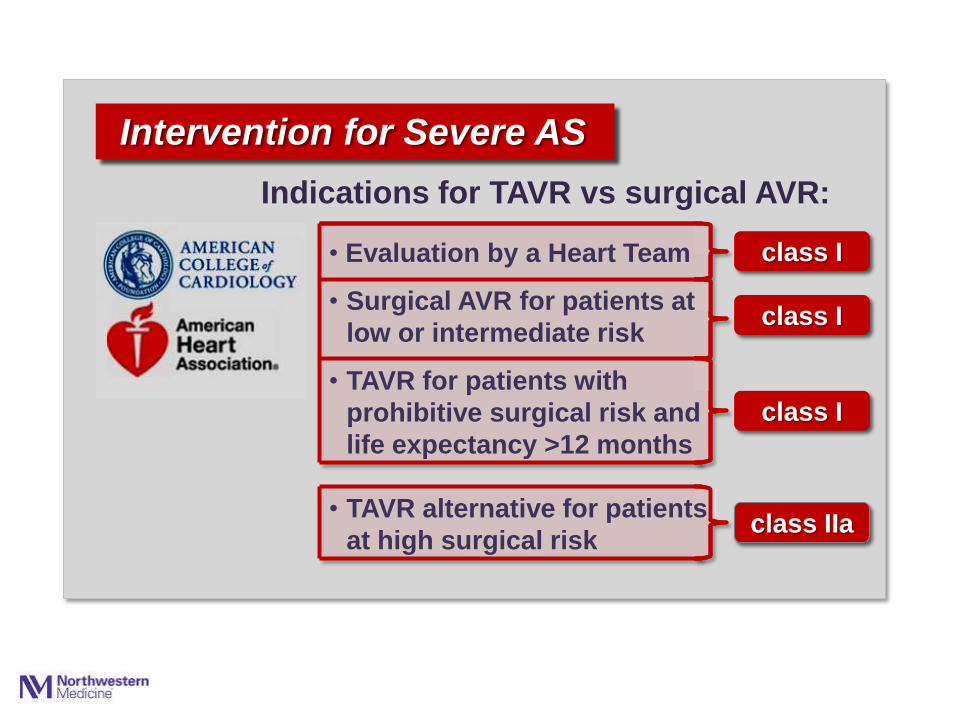
Indications for TAVR vs surgical AVR:
class I
class IIa
Intervention for Severe AS
• Evaluation by a Heart Team
• Surgical AVR for patients at
low or intermediate risk
• TAVR for patients with
prohibitive surgical risk and
life expectancy >12 months
class I
class I
• TAVR alternative for patients
at high surgical risk
Page 65
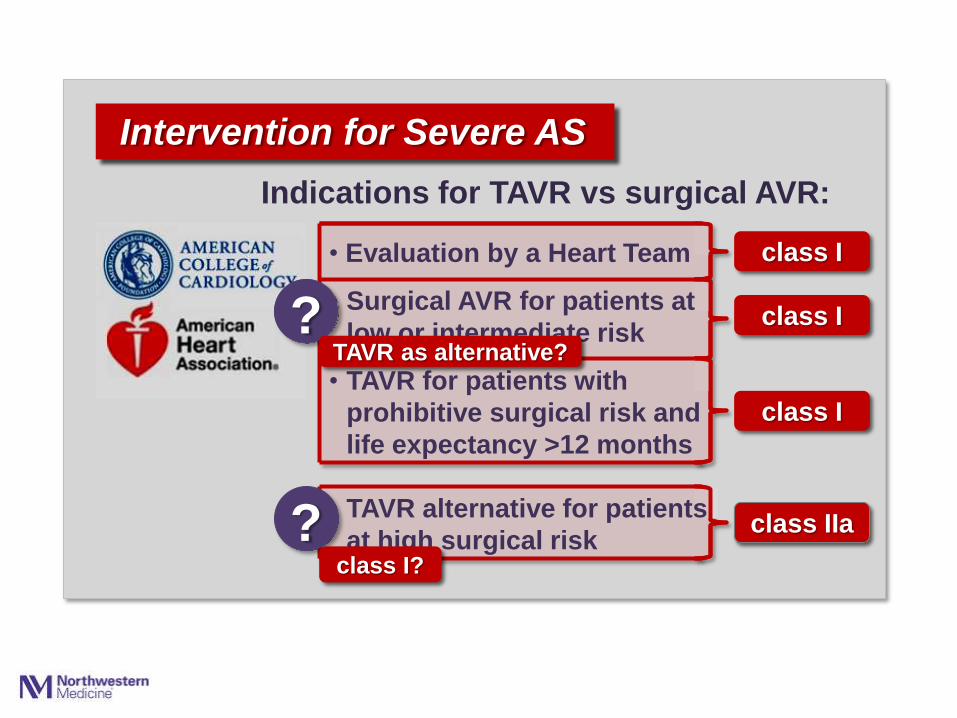
Indications for TAVR vs surgical AVR:
class I
class IIa
Intervention for Severe AS
• Evaluation by a Heart Team
• Surgical AVR for patients at
low or intermediate risk
• TAVR for patients with
prohibitive surgical risk and
life expectancy >12 months
class I
class I
• TAVR alternative for patients
at high surgical risk
?
? class I?
TAVR as alternative?
Page 66
0
20
40
60
80
100
120
140
160
0
20
40
60
80
100
120
140
160
0
20
40
60
80
100
120
140
160
16
14
12
10
8
6
4
2
0
30-D
ay M
ort
alit
y (
pe
rce
nt)
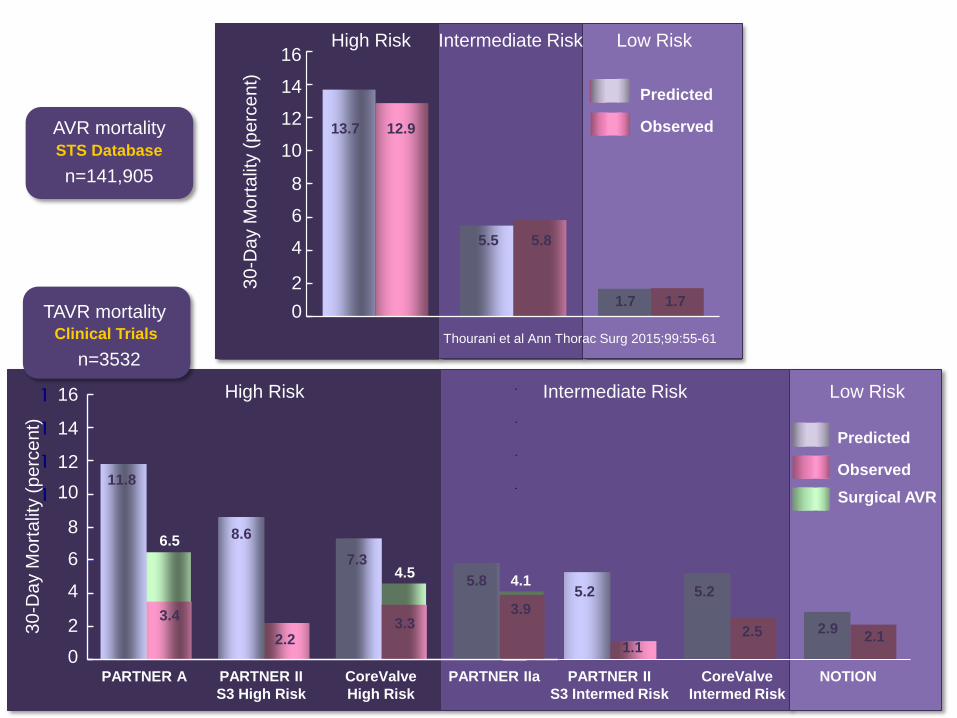
High Risk Intermediate Risk Low Risk
Thourani et al Ann Thorac Surg 2015;99:55-61
1.7
Observed
Predicted
AVR mortality STS Database
n=141,905
Low Risk
TAVR mortality Clinical Trials
Predicted
Observed
5.3
2.5
NOTION
n=3532
Surgical AVR
1.7
12.9
0
20
40
60
80
100
120
140
160
11.8
3.4
8.6
2.2
7.3
3.3
5.2
2.9 2.1
6.5
4.5
30-D
ay M
ort
alit
y (
pe
rce
nt)
16
10
12
8
6
4
0
13.7
5.5 5.8
14
2
PARTNER A PARTNER II
S3 High Risk
CoreValve
High Risk
PARTNER II
S3 Intermed Risk
CoreValve
Intermed Risk
High Risk Intermediate Risk
PARTNER IIa
5.2
1.1
5.8
3.9
4.1
Page 67
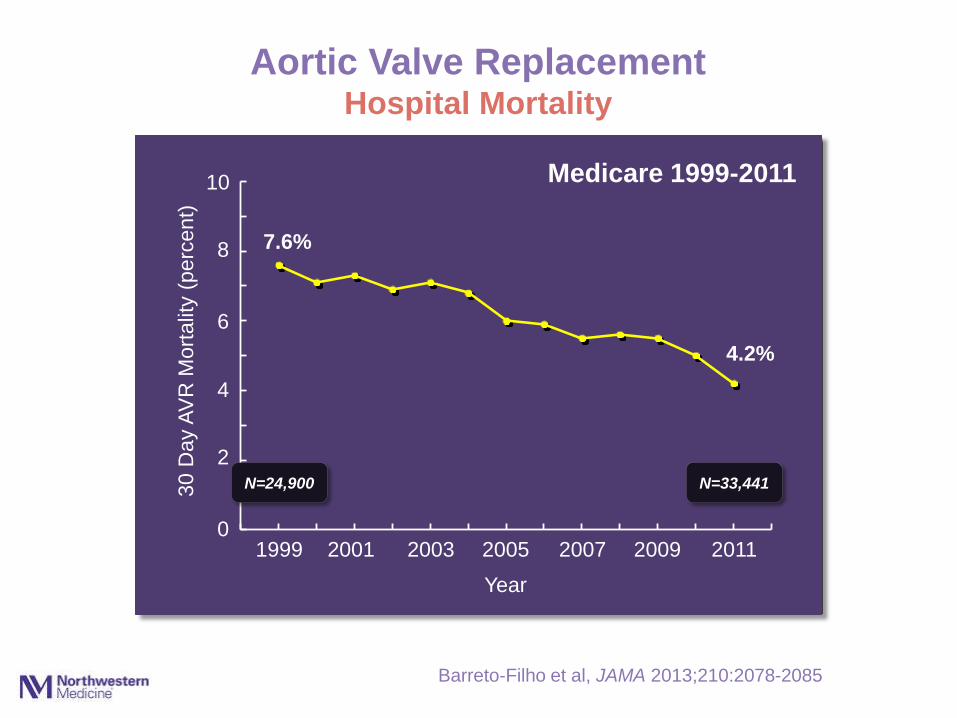
Barreto-Filho et al, JAMA 2013;210:2078-2085
Aortic Valve Replacement Hospital Mortality
Medicare 1999-2011
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5
30
Da
y A
VR
Mort
alit
y (
perc
en
t)
8
10
6
4
2
0 1999 2001 2003 2005 2007 2009 2011
7.6%
4.2%
Year
Medicare 1999-2011
N=24,900 N=33,441
Page 68
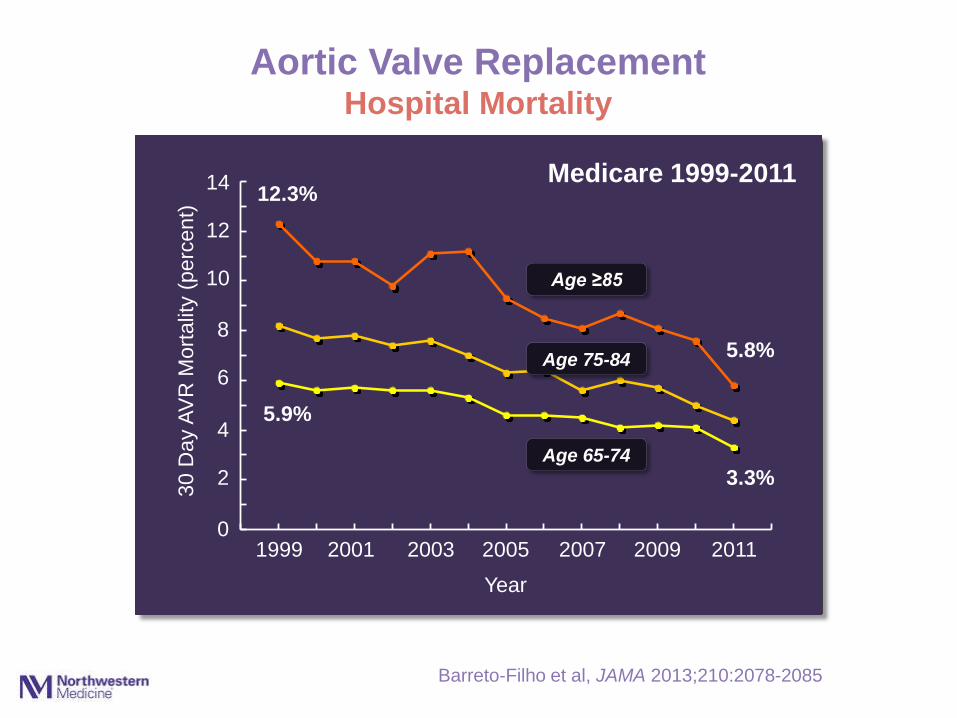
Barreto-Filho et al, JAMA 2013;210:2078-2085
Aortic Valve Replacement Hospital Mortality
Medicare 1999-2011
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 1 2 3 4 5
30
Da
y A
VR
Mort
alit
y (
perc
en
t)
8
14
6
4
2
0 1999 2001 2003 2005 2007 2009 2011
5.9%
12.3%
Year
5.8%
3.3%
12
10
Age 65-74
Age 75-84
Age ≥85
Medicare 1999-2011
Page 69
TAVR Now
• TAVR has been truly transformative
• Surgical AVR remains the standard with proven
durability and safety for most patients
• TAVR provides treatment options for patients
who previously had no options other than a
predictably very poor short term outcome
• TAVR is an alternative to SAVR in patients at
high surgical risk
• The threshold for TAVR is declining in clinical
trials, registries and clinical practice
• All patients want this
Page 70
TAVR in the Future
• Judgment of the Heart Team remains essential
in patient selection for TAVR
• Appropriate use criteria and performance
measures are needed to define quality
• Guidelines will need to adapt to the rapidly
evolving TAVR evidence base
TAVR in intermediate and low risk surgical patients
• Availability of TAVR is likely to inform new
indications for valve replacement
Moderate AS in primary cardiomyopathy
Asymptomatic severe AS?
• •
Page 71
Aortic stenosis is a simple mechanical fault
which, if severe enough, imposes a heavy
burden on the left ventricle and sooner or
later overcomes it.
Wood P, Am J Cardiol 1958;1:553-571