28
Managing Benefits from Projects Hugo Minney PhD The Social Return Company
| Date post: | 16-Apr-2017 |
| Category: |
Business |
| Upload: | association-for-project-management |
| View: | 854 times |
| Download: | 0 times |
Managing
Benefits from
Projects
Hugo Minney PhD
The Social Return
Company
Contents
1 Hour practical session to
cover:
Pick the right stakeholders
Know what makes a
difference
Measure and report to drive
change
Exercise in Stakeholder
mapping
Exercise in Benefits mapping
15 mins introduction and
explanation
20 mins stakeholder mapping
20mins benefits mapping
5 mins sum up

Who am I to talk?
1990 – PhD and Computer Salesman
2000 – Cap Gemini
2004 – NHS Modernisation Agency
Developing national policy including Emergency Care Practitioner (ECP); Regionally, locally, arms length bodies in NHS
For profit and not-for profit NHS and social care facing roles
CURRENTLY: Company Secretary of GP-led federation with 170,000 registered patients
AND: The Social Return Company lead consultant
AND Registered Project Professional, Fellow of APM

Basics of Benefits Management A benefit is a result that a stakeholder perceives to be of
value.
Benefits Management is the identification, definition, planning, tracking and realisation of business benefits
Social Return on Investment (SROI) is a framework for measuring and accounting for a broad concept of value; it seeks to reduce inequality and environmental degradation and improve wellbeing by incorporating
social, environmental and economic costs and benefits.

Benefits can be more than profit
Not-for-profit - how to measure return on investment?
• Savings on other possible costs to the public purse
• A value assigned to Quality of Life, or Happiness
• Future impact on the economy
For Profit and Commercial
• Customer satisfaction – an indicator of future business
• Staff satisfaction – R&R and productivity
• IP portfolio

Making Change Happen
Change doesn’t happen on its own – duh! (while not all changes do lead to improvement, all improvement requires change)
Change happens because people
make it happen A clear vision
A way to measure progress
A clear connection between what is done and what is achieved
Something that motivates people (The basic benefits questions
of any Change):
• Who is it all actually for?
• What do they really want out of it?
• What makes this choice better than Plan B?
Four stages when you apply Benefits
Management:
• WHY – business case, sponsor, stakeholders
• WHAT & HOW
Project planning, measurement schema
Project delivery, decisions to maximise benefits
• HANDOVER – handover capability, plus motivation
• ONGOING
Measuring and reporting
Tweaking and adjusting for even better outcomes

Define Benefits
Case for Investment
Quantify and
milestones
Decisions to
maximise
benefits
What benefits
deferred and how
to monitor them
Ben
efi
ts
Fra
mew
ork
Idea
Initiation
Define
Deliverables
Milestones
Resources
Project monitoring
Project delivery
Governance
Clo
sedow
n
Pro
ject
Man
ag
em
en
t
Handover
Benefits Management and
PRINCE2
Business
as Usual
Reporting
& tweaks
WHY WHAT &
HOW
HAND-
OVER ONGOING

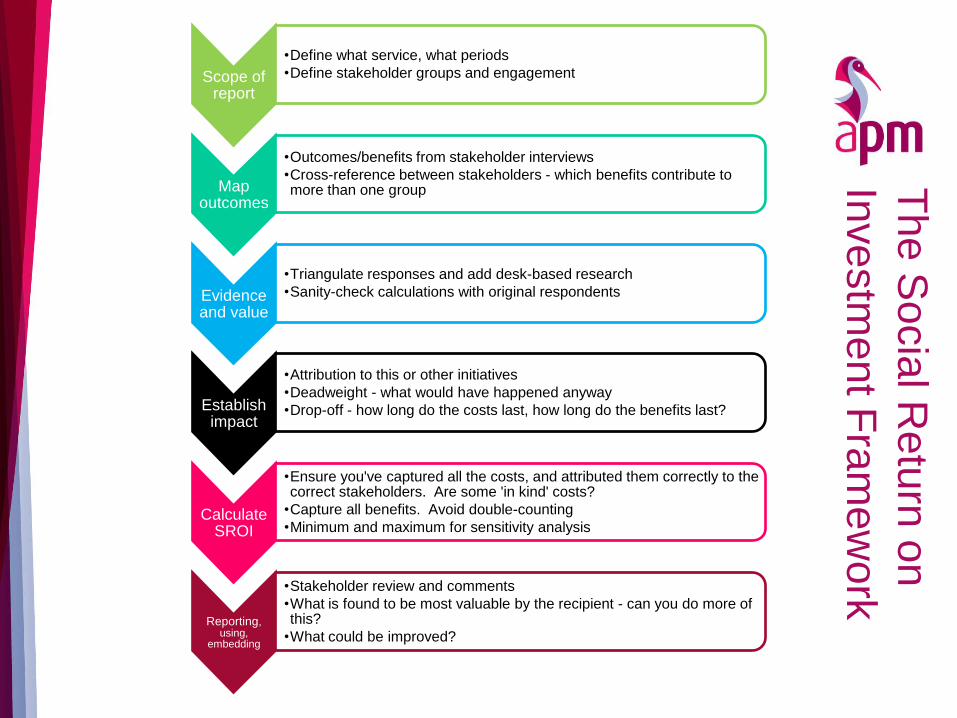
Considering Social Return on Investment
(and any other investment which plans to achieve more than PROFIT)
1. Establish Scope and identify key stakeholders (Stakeholder Mapping and
real Engagement)
2. Map outcomes (impact map/ theory of change) including 2nd and 3rd level
impacts
3. Evidence outcomes and give them a value (Value is only what is described
by stakeholder. What numbers are defendable?)
4. Establish impact (what would have happened anyway? What is attributed to
what?)
5. Calculating SROI – and if you want to do it properly, sensitivity analysis
6. Reporting, using and embedding
Th
e S
ocia
l Re
turn
on
Inve
stm
en
t Fra
me
wo
rk
Scope of report
•Define what service, what periods
•Define stakeholder groups and engagement
Map outcomes
•Outcomes/benefits from stakeholder interviews
•Cross-reference between stakeholders - which benefits contribute to more than one group
Evidence and value
•Triangulate responses and add desk-based research
•Sanity-check calculations with original respondents
Establish impact
•Attribution to this or other initiatives
•Deadweight - what would have happened anyway
•Drop-off - how long do the costs last, how long do the benefits last?
Calculate SROI
•Ensure you've captured all the costs, and attributed them correctly to the correct stakeholders. Are some 'in kind' costs?
•Capture all benefits. Avoid double-counting
•Minimum and maximum for sensitivity analysis
Reporting, using,
embedding
•Stakeholder review and comments
•What is found to be most valuable by the recipient - can you do more of this?
•What could be improved?

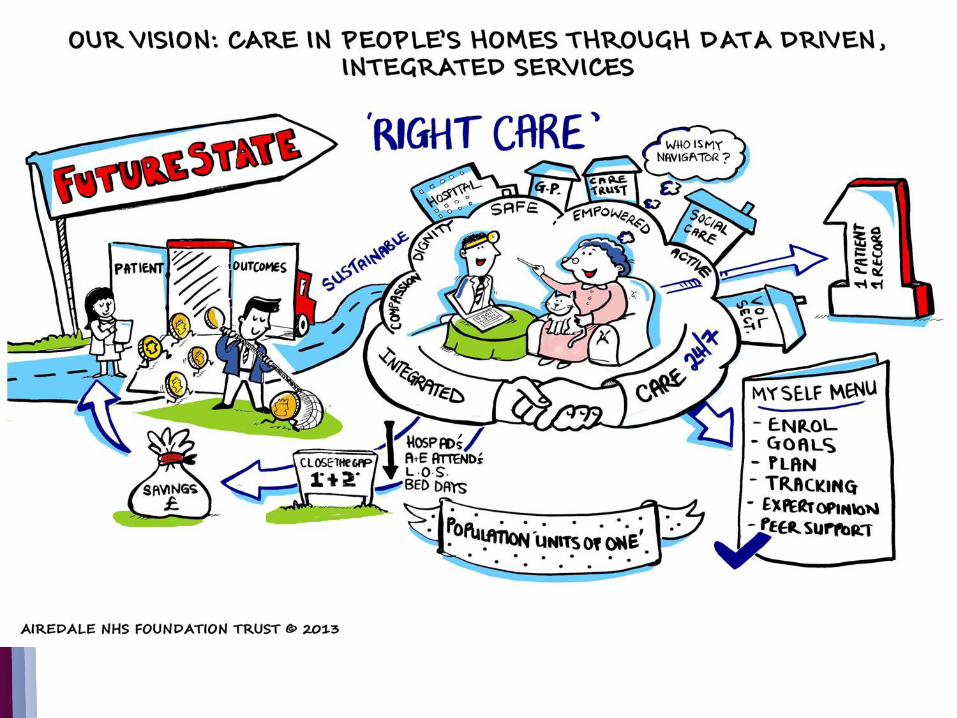
Engaging Stakeholders
Introduction to Airedale Integrated Care
project
“1 Patient 1 Record”
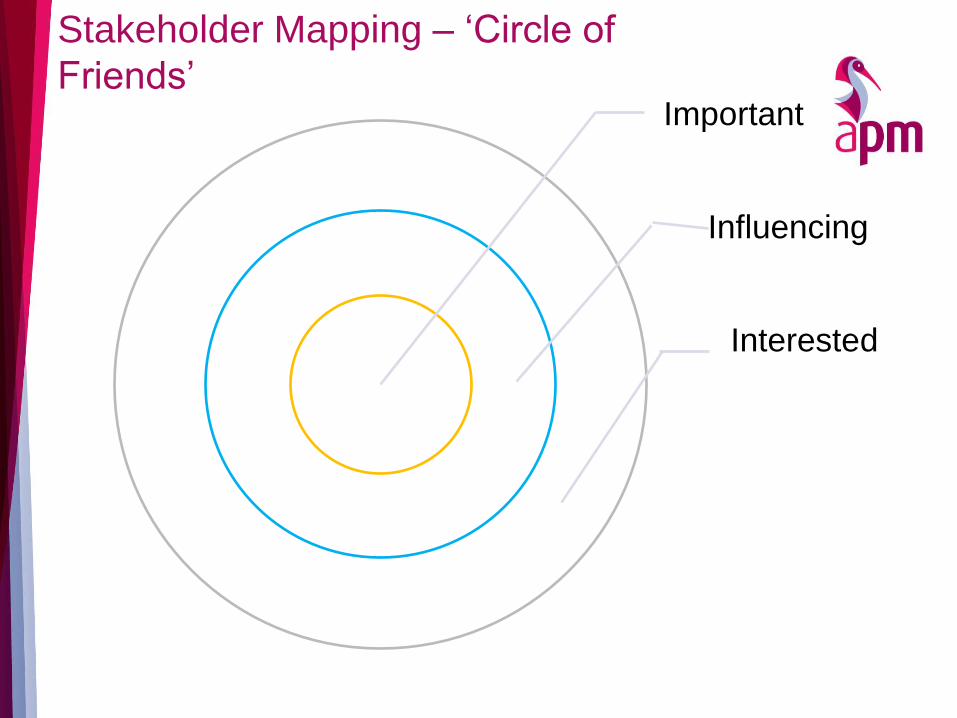
Stakeholder Mapping – ‘Circle of
Friends’ Important
Influencing
Interested
WIIFM
Take one of the stakeholders from the
centre and list the non-financial benefits
they want to see
A benefit is a result that a stakeholder perceives to be of
value.

Measuring the SRoI
Care Commissioners want to see empowered patients (on the assumption that empowered patients take more care of themselves and so make less demand on resources)
Empowerment:
• Understand their condition and what they can do about it (scale?)
• Take action to self-manage (scale?)
• Impact on other resource use

Benefits Mapping
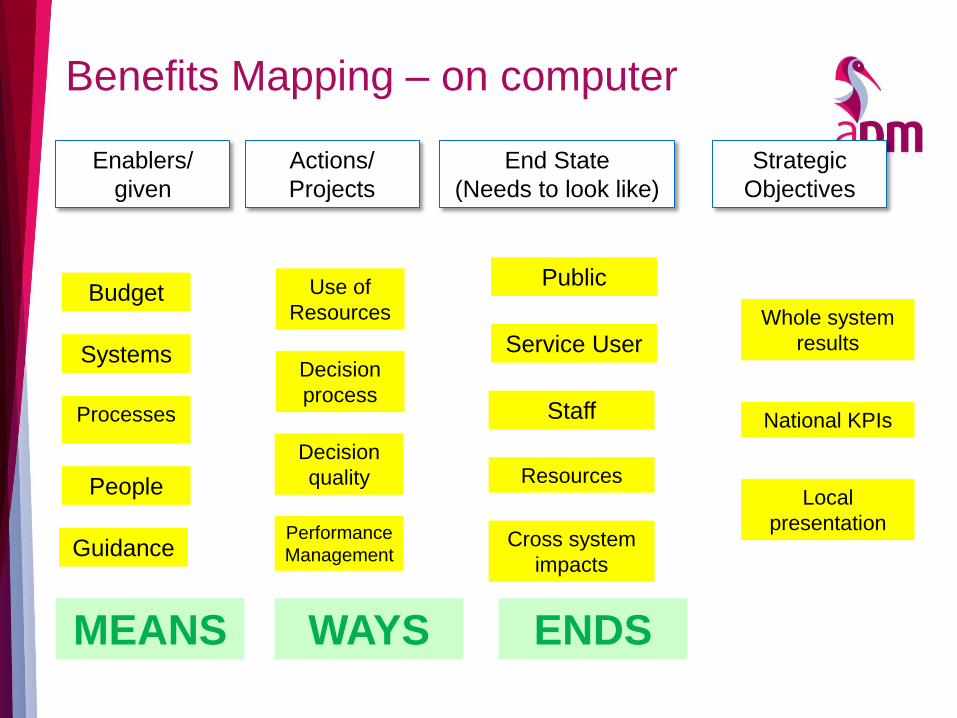
Benefits Mapping – on computer
Enablers/
given
Actions/
Projects
End State
(Needs to look like)
Strategic
Objectives
Use of
Resources
Decision
process
Decision
quality
Performance
Management
Budget
Systems
Processes
People
Guidance
Whole system
results
National KPIs
Local
presentation
Public
Service User
Staff
Cross system
impacts
Resources
MEANS WAYS ENDS

Benefits Mapping
Map the links from “1 Patient, 1 Record” to
More Empowered Patients
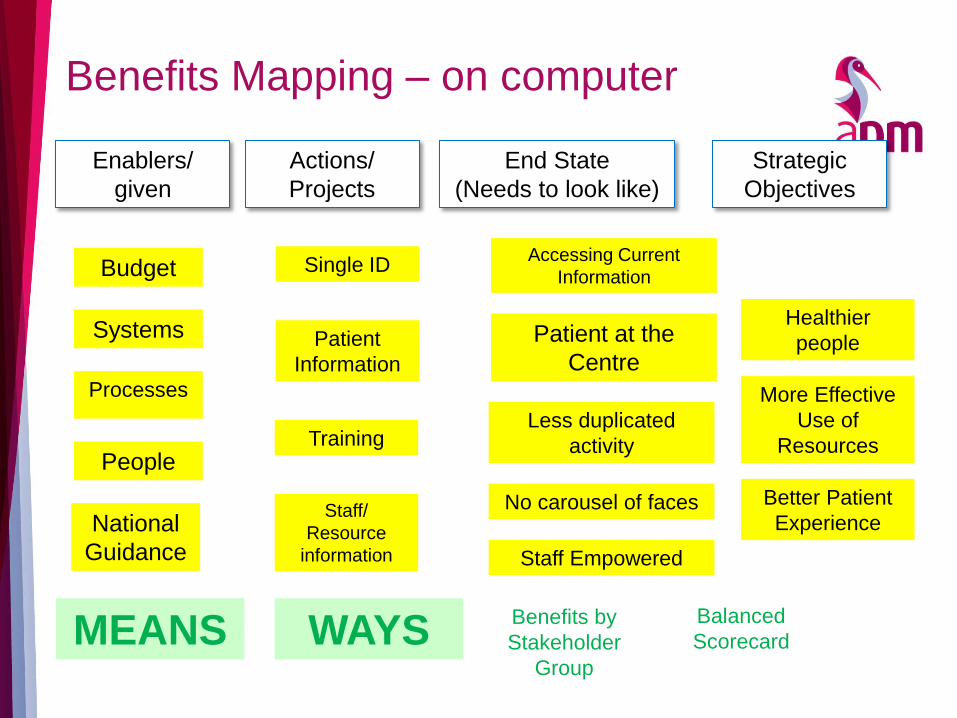
Benefits Mapping – on computer
Enablers/
given
Actions/
Projects
End State
(Needs to look like)
Strategic
Objectives
Single ID
Patient
Information
Training
Staff/
Resource
information
Budget
Systems
Processes
People
National
Guidance
Healthier
people
More Effective
Use of
Resources
Better Patient
Experience
Accessing Current
Information
Patient at the
Centre
Less duplicated
activity
Staff Empowered
No carousel of faces
MEANS WAYS Benefits by
Stakeholder
Group
Balanced
Scorecard

Staff Motivation
“I can tell my grandchildren ‘I did a good job this week’ “
Lower Sickness/ Absence
Easier Recruitment/ Retention
Getting much more done
Engaged with corporate objectives – even to MAKE MONEY
The calculations for Empowered
patients How many people are more empowered?
How much are they more empowered (may need to segment into types of empowerment)?
What difference does it make:
• Quality of Life (and what’s our value assigned? Who for?)
• Happiness (value assigned)
• Use of resources (over next 12 months, next 36 months, next 5 years?) – predicted based on experience/ research
What would have happened anyway?
What’s the normal progression of disease/
decrepitude? (without empowerment)
• When do they need residential care?
• When do they need hospital care?
• What’s changed in society’s attitudes?
How much would this normally cost?
The price of happiness
Votes
Sickness (loneliness and heart disease.
Demotivation and obesity)
What I would want for myself – an how much
of someone else’s money will I assign to it?
How much would I spend for myself?
What gets you up in the morning?
Nobody comes in to work to do a bad job (well, almost nobody)
We all want to make a difference – make the world a better place
Very few people work just for the money*
• Osterloh & Frey 2007 Does pay for performance really motivate employees?
• PwC NextGen 2013: Millennial workers want …
“I can tell my grandchildren ‘I did a good job this week’ “
Driving improvement
We (the people who talk to the client/ do the work) see the need/problem first!
We know what to do about it (have the most experience)
We can inspire*
We won’t resist our own design for change
(a new problem – managing configuration)
Malcolm Gladwell – Tipping Point

When the best leader’s work is
done, the people will say:
“We did it ourselves”
Lao Tzu
Hugo Minney
PhD, Acc Prac SROI, F APM, PRINCE2,
RPP
07786 961837

















