35
Managing DAA treatment failure and Drug Resistance in Clinical Practice Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain

Managing DAA treatment failure and Drug Resistance in Clinical Practice
Vicente Soriano Infectious Diseases Unit
La Paz University Hospital Madrid, Spain
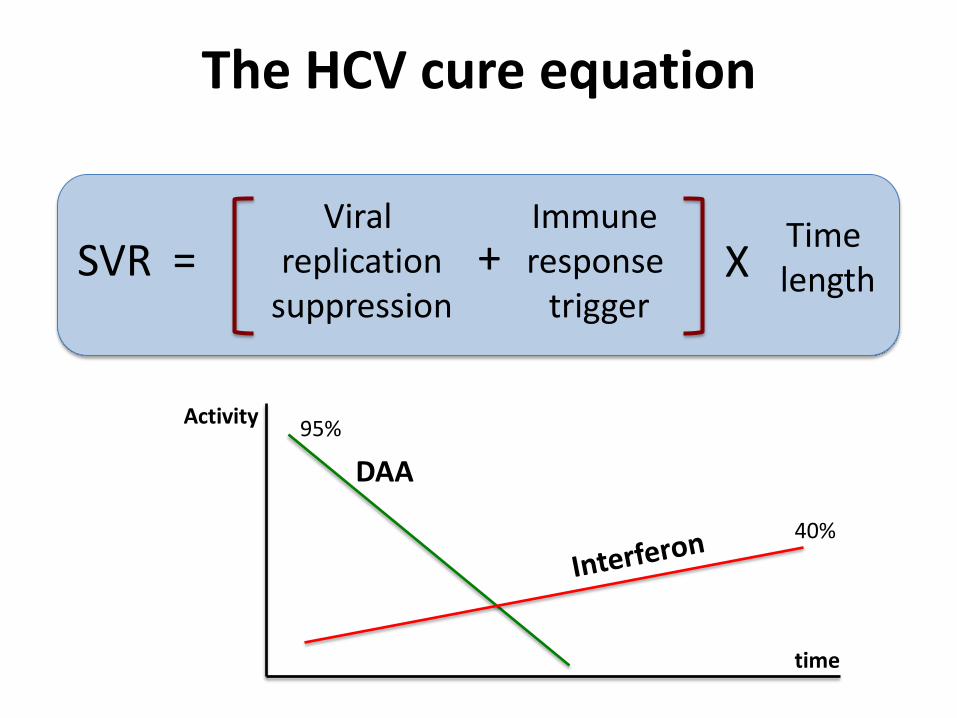
The HCV cure equation
SVR Viral
replication suppression
Time length
Immune response
trigger = + X
DAA
Activity
time
40%
95%

HCV
Hepatocyte
RNA
Pro Cytosol
Pol
CD4+
T-lymphocyte
HIV
RNA
RT
Nucleus
Integration
Provirus Pro
Differences in the replication life cycle of HIV and HCV

Classification of recommended DAA (2016)
NS3 protease inhibitors
NS5A inhibitors
Nucleos(t)ide polymerase inhibitors
Non-nucleoside polymerase inhibitors
Simeprevir Asunaprevir Paritaprevir Grazoprevir
Ledipasvir Daclatasvir Ombitasvir Elbasvir Velpatasvir
Sofosbuvir Beclabuvir Dasabuvir
Squares record co-formulations or co-packaged medications. Velpatasvir will soon replace ledipasvir.


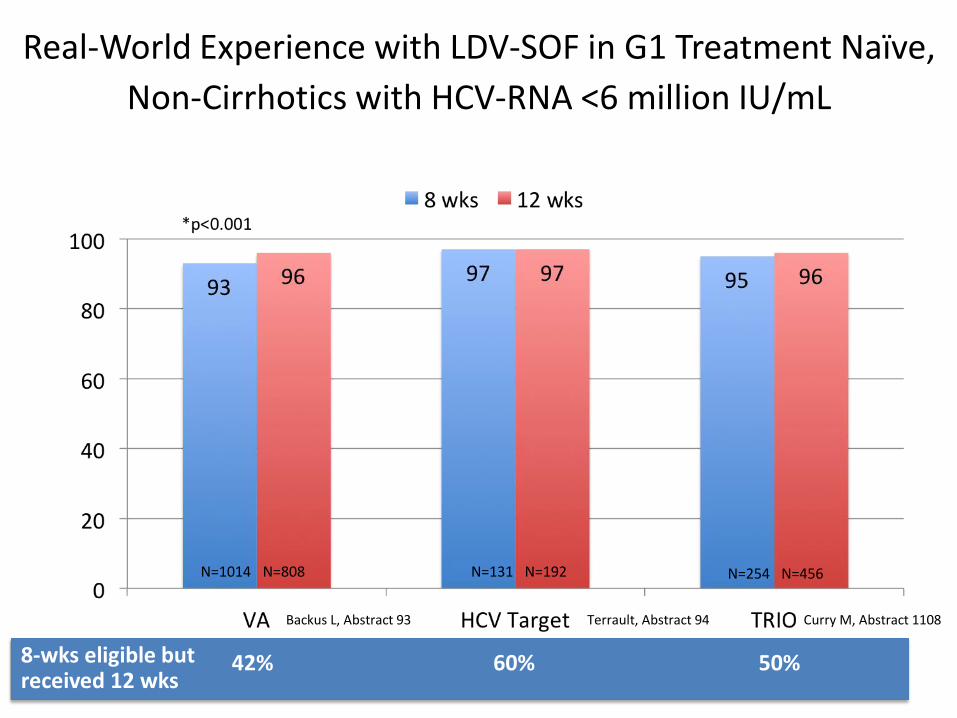
Real-World Experience with LDV-SOF in G1 Treatment Naïve,
Non-Cirrhotics with HCV-RNA <6 million IU/mL
N=131 N=192 N=254 N=456
42% 60% 50% 8-wks eligible but received 12 wks
N=1014 N=808
Curry M, Abstract 1108 Backus L, Abstract 93 Terrault, Abstract 94

DAA real world experience
TRIO (n=1685)
Spain (n=363)
Male 58% 75%
Advanced liver fibrosis 30% (cirrhosis) 48%
Elevated ALT ? 83%
Baseline HCV-RNA > 6 log 21% (>6 million) 59%
HCV genotype 4 0 (67% G1a ) 15%
HIV coinfection 7% 31%
Ribavirin added 5% 38%
Prior interferon failure ? 49%
SOF+LDV 88% 80%
SVR 96% 97%*
Afdhal et al. AASLD 2015 Arias et al. AVT (in press) *Analysis per protocol (no ITT)

Sustained virological response (n=352)
Treatment failure (n=11)
p
Male gender, n (%) 255 (73.1) 9 (81.8) 0.7
Elevated ALT, n (%) 311 (81.2) 10 (90.9) 0.8
IL28B-CC, n (%) 97 (27.1) 2 (18.2) 0.9
Advanced liver fibrosis, n (%) 146 (42.8) 10 (90.9) 0.003
Baseline HCV-RNA >6 log IU/mL, n (%) 225 (62.4) 6 (54.5) 0.7
Prior interferon exposure, n (%) 164 (47.2) 6 (54.5) 0.7
HIV coinfection, n (%) 91 (27.2) 7 (63.6) 0.04
HCV genotype 4, n (%) 46 (13.1) 4 (36.4) 0.05
Ribavirin added, n (%) 120 (34) 5 (45.4) 0.4
Main characteristics of the study population according to treatment outcome.
Arias et al. AVT (in press) *Analysis per protocol (no ITT)

Main baseline characteristics of chronic hepatitis C patients that experienced DAA treatment failure.
1 2 3 4 5 6 7 8 9 10 11
Age (years) 52 55 78 54 50 50 57 49 49 45 52
Gender male male male male male male male
female male
male female
ALT (IU/L) 39 87 53 64 45 30 73 70 55 69 83
Serum HCV-RNA (log IU/mL)
6.5 5.8 6.3 6.5 5.8 6.9 5.8 6.7 4.8 7.1 4.6
HCV genotype 1a 4 1b 1a 4 1a 1b 4 3 4 1b
Liver fibrosis stage (Metavir)
F4 F4 F4 F1 F4 F3 F4 F4 F4 F3 F3
IL28B polymorphisms CC CT CT CT CT CT CC CT CT TT CT
Prior interferon exposure
no no no no yes yes yes no yes yes yes
HIV coinfection yes yes no yes yes no yes yes no no yes
DAA regimen SOF/LDV/R
BV
SOF/LDV/RBV
SOF/LDV/RBV
SOF/LDV
SOF/LDV/RBV
SOF/LDV
SOF/SMV
SOF/SMV
SOF/RBV
SOF/LDV
SOF/LDV
Arias et al. AVT (in press)

Predictors of DAA treatment failure in the study population. Multivariate analysis.
Male gender (73%)
HIV coinfection (27%)
Advanced liver fibrosis (F3-F4) (43%)
Serum HCV-RNA >106 IU/mL (63%)
Interferon experience (47%)
HCV genotype 4 (13%)
treatment failure sustained virological response
Ribavirin added (34%)
p=0.04
p=0.01
1.7
2.1
odds ratio
Arias et al. AVT (In press)

Predictors of DAA failure
Baseline On-treatment
• Cirrhosis • Genotype 3 • RAVs • Prior interferon failure • Elevated serum HCV-RNA • IFNL4 unfavorable • AA ethnicity
• Drug adherence • Side effects • Drug interactions

Anecdotal SAEs with DAA
• Bradyarrithmias (and syncope) • Pulmonary arterial hypertension • Lung toxicity • Hepatotoxicity • Photosensitivity • Hyperbilirrubinemia • Hypoglycemia in diabetics on insulin • Hepatitis B reactivation
Fontaine et al. NEJM 2015; 373: 1886-8. Ahmad et al. Hepatology 2015; 62: 409-16. Dyson et al. J Hepatol 2016; 64: 234-8. Soriano et al. Hepatology (in press) Stine et al. Dig Dis Sci 2015; 60: 1031-5.
Shibata et al. Hepatology (in press) Marchan et al. J Hepatol (in press) Helmers et al. Mayo Clin Proc 2015; 90: 1294-7. Renard et al. Chest 2016; 149: e69-73. Soriano et al. Antivir Ther (in press)
Rapid HCV drop


HBV reactivation during DAA for hep C
Collins et al. Clin Infect Dis 2016 Ende et al. J Med Case Rep 2015 Takayama et al. Hepatol Res 2016 *De Monte J Clin Virol 2016
*

Difficult-to-cure HCV populations
• End-stage renal disease • Decompensated cirrhosis • Prior DAA failures • Potential drug interactions:
– HIV, psychiatric, elder, etc
• Difficult drug adherence: – homeless, illegal immigrants, jail, active IDU,
psychiatric
• Insufficient data: – Alcoholics, NASH-obese-diabetics, HBsAg+

Considerations for HCV re-treatment
• Virologic challenges: – Presence of RAVs (prior DAA failure)
– Exclude HCV genotype shift (misinterpretation)
– Exclude HCV re-infection (risk behaviors)
• Strategic management: – Adding ribavirin
– Extent the length of therapy
• Maximize drug benefit: – Avoid drug interactions (co-morbidities)
– Prevent and manage side effects
– Ensure drug adherence
How urgent is it ? Any chance to wait for better DAA?

Principles guiding selection of HCV regimens for re-treatment of prior DAA failures
NS3 protease inhibitors
Telaprevir Boceprevir Simeprevir
NS5A inhibitors
Ledipasvir Daclatasvir
NS3 protease inhibitors plus NS5A inhibitors
Paritaprevir + Ombitasvir Grazoprevir + Elbasvir
Prior DAA failure Re-treatment options
NS5A inhibitors
Ledipasvir Daclatasvir
NS3 protease inhibitors
Simeprevir
PegIFN+RBV o
Sofosbuvir + Sofosbuvir +
+ Sofosbuvir Sofosbuvir +
+ Sofosbuvir ?

HCV Drug Resistance (RAVs)
• Prevalence vary by geno/subtype and geographic region.
• Baseline RAVs may reduce SVR in some patients: – NS3 – Q80K – reduced SVR in G1a cirrhotics
– NS5A – reduced SVR in cirrhotics with prior IFN failure
• Extending the length of DAA therapy may overcome the harmful impact of baseline RAVs
• Not all RAVs are equal, “some are more equal than others” – NS3 protease – D168X
– NS5A – Y93H
– NS5B – S282T


GT 1 NS5A RAV Prevalence by Region
Using a 15% cut-off, the prevalence of NS5A RAVs was 14% in North America, 15% in Europe, 20% in Asia Pacific, and 17% in Oceania
21
Europe 25% (235/933)
USA
Canada
Puerto Rico
Belgium
Switzerland
Czech Republic
Germany
Spain
France
United Kingdom
Italy
Netherlands
Poland
China
India
Japan
Korea
Russia
Taiwan
Australia
New Zealand
Asia Pacific 26% (154/597)
Oceania 27% (115/427)
North America 25% (870/3440)
* Based on 1% cut-off
Zeuzem S, AASLD 2015. Abstract 91

LDV-SOF in Patients with and without Baseline NS5A RAVs
22
SVR
12
(%
)
Naïve & VL<6M Naive Experienced
Zeuzem S, AASLD 2015. Abstract 91
No cirrhosis

23
26/27 65/68
12 weeks 24 weeks
SVR
12 (
%)
10/10 8/9 27/27 19/19
Treatment Naive Treatment Experience
12 weeks 24 weeks
LDV-SOF in Patients with and without Baseline NS5A RAVs
With cirrhosis
Zeuzem S, AASLD 2015. Abstract 91
7/7





Estimated clearance time for RAVs selected upon treatment failure
days months years
10%
RAVs (%)
Benitez et al. Exp Op Pharmacother (in press)



Drug Resistance Tests
• Commercially available methods not available in most countries.
• Population sequencing (Sanger) of the NS3 protease, NS5A domain I and NS5B by homemade methods. Sensitivity for RAVs: 20%
• Potential interest of NGS, but thresholds for
clinical significance should be set up at 10%.

HCV resistance testing
• At baseline – Q80K in G1a if simeprevir to be used • At failure – RAVs selected to most agents on board but sofosbuvir • At re-treatment – persistence of RAVs mostly for NS5A inhibitors and NS5B non-nuc inhibitors and less frequently for NS3 protease inhibitors

Prospects for HCV resistance testing
Interesting academically to learn mechanisms of failure and potential cross-resistance. Avoid short lengths and close monitoring in cirrhotics However, the pace of development of better treatments and broader options would overcome the need to require individual resistance information for most re-treatments. Reminds what has happened in HIV.

Summary
• Failure to current DAA combinations occurs in 5-15% of chronic hepatitis C patients outside clinical trials.
• Most failures to oral DAA combinations are relapses instead of viral breakthroughs on therapy.
• Failures occur more frequently in treatment-experienced patients, those with advanced cirrhosis and infection with HCV genotypes 3 or 1a.
• In non-cirrhotics patients, DAA failure is rare and generally seen only when therapy is given for less than 12 weeks.
• Virologic breakthrough during DAA therapy generally reflects poor drug adherence.
• DAA failure is frequently associated with emergence of RAVs but to sofosbuvir.
• HCV drug resistance testing should be recommended for choosing the most convenient salvage DAA regimen as re-treatment for prior DAA failures.




![DAA MID2 [UandiStar.org]](https://static.documents.pub/doc/80x56/545a7372af7959755d8b5b4b/daa-mid2-uandistarorg.jpg)












