Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience Deirdre O’Donnell, Margaret P. Treacy, Gerard Fealy, Imogen Lyons, Amanda Phelan, Attracta Lafferty, Jonathan Drennan, Suzanne Quin, Anne O’Loughlin
Transcript
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience
Deirdre O’Donnell, Margaret P. Treacy, Gerard Fealy, Imogen Lyons, Amanda Phelan,
Attracta Lafferty, Jonathan Drennan, Suzanne Quin, Anne O’Loughlin
NCPOP Board of Programme Directors
Professor Margaret P. Treacy, Professor Gerard Fealy, Professor Denis Cusack, Professor Colm Harmon, Dr. Martin McNamara, Professor Cecily Kelleher, Ms Anne O’Loughlin, Dr. Amanda Phelan, Professor Suzanne Quin
This study was funded by the Health Service Executive as part of the work of the National Centre for the Protection of Older People (NCPOP) at University College Dublin.
This report should be cited as O’Donnell, D., Treacy, M.P., Fealy, G., Lyons, I., Phelan, A., Lafferty, A., Drennan, J., Quin, S., O’Loughlin, A. (2012) Managing Elder Abuse in Ireland: Senior case workers’ experiences, NCPOP, University College Dublin.
National Centre for the Protection of Older People (NCPOP) UCD School of Nursing, Midwifery and Heath Systems
Health Sciences Centre University College Dublin Belfield, Dublin 4, Ireland
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience
Acknowledgements
The authors are grateful to all the senior case workers who gave so generously of their time in providing the data on which this study is based. Without their engagement, the study would not have been possible.
The authors also wish to acknowledge:
• The Health Service Executive which funds the National Centre for the Protection of Older People (NCPOP) and the programme of research, of which the study is part.
• The HSE/NCPOP Management Group and the HSE/NCPOP Steering Group which advised on this study.
• The National Elder Abuse Steering Committee of the Health Service Executive, which provided important support for the study.
• Dr. Corina Naughton for her advice on aspects of the research design.
• The NCPOP International Advisory Committee, comprising Professor Simon Biggs, King’s College London; Dr. Isabel Iborra Marmolejo, Queen Sofia Centre for Studies on Violence, Valencia, Spain, and Professor Karl Pillemer, Cornell Institute for Translational Research on Aging, Cornell University.
• Ms. Judy Mathers, NCPOP Administrator for her support in the production of this report.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience
Contents
Executive Summary i
Chapter 1 1Introduction
1.1 Background 1
1.2 Report Structure 1
1.3 International Developments in Response to Elder Abuse 1
1.4 The Irish Response to Elder Abuse 3
1.4.1 HSE Dedicated Elder Abuse Structures 3
Chapter 2 5Managing Elder Abuse in Practice
2.1 Introduction 5
2.2 Aims and Method of Literature Review 5
2.3 Detection and Referral 5
2.4 Investigation and Assessment 7
2.5 Intervention Strategies and Services Provision 8
2.5.1 Case Management 8
2.5.2 Monitoring 8
2.5.3 Counselling 9
2.5.4 Support Groups 9
2.5.5 Interventions for Caregivers 10
2.5.6 Home Support Services and Respite Care 10
2.5.7 Emergency Shelters, Refuges, Safe Houses and Long Term Care 11
2.5.8 Telephone Services 12
2.5.9 Daily Money Management (DMM) 12
2.5.10 Advocacy 12
2.5.11 Mediation, Conflict Resolution and Restorative Justice 13
2.5.12 Legal Intervention 14
2.5.13 Education, Information Provision and Advice 14
2.5.14 Multi-Component Interventions 15
2.6 Outcomes and Case Closure 15
2.7 Collaboration, Multi-disciplinary and Interagency Working 16
2.8 Decision-making in Elder Abuse Cases 17
2.8.1 Ethical Dilemmas and Challenges 18
2.9 Training, Supervision and Line Management 20
2.10 Conclusions 20
Chapter 3 22Research Design
3.1 Introduction 22
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience
Contents
3.2 Aims and Objectives 22
3.3 Overview of Study Design 22
3.4 Sampling and Recruitment 22
3.5 Data Collection 23
3.5.1 Interview Guide 23
3.6 Data Analysis 23
3.7 Ethical Considerations 24
Chapter 4 25Findings Part 1: Elder Abuse, A Unique Phenomenon
4.1 Introduction 25
4.1.1 Profile of the Participants 25
4.2 The Multifaceted Nature of Elder Abuse 25
4.2.1 The Types of Elder Abuse 26
4.2.2 Balancing Self-determination and Risk 27
4.2.3 Ethical Concerns 29
4.2.4 Family Conflict 30
4.2.5 Establishing Trust and Rapport 31
4.3 Summary 31
Chapter 5 33Findings Part 2: Protecting Older People
5.1 Introduction 33
5.2 Case Management and Interventions 33
5.2.1 Responding to Referrals 33
5.2.2 Establishing Protection and Care Plans 34
5.2.3 Case Conferences and Family Meetings 35
5.2.4 Counselling and Support 36
5.2.5 Maintaining Client Relationships 37
5.2.6 Evaluating Case Outcomes 38
5.3 Interagency Working 39
5.3.1 Interagency Referrals 39
5.3.2 Interagency Communication 41
5.3.3 Negotiating Boundaries and Approaches 42
5.4 Experiencing the Role 43
5.4.1 The ‘Lone Worker’ 43
5.4.2 Managing Caseload and Time 45
5.5 Summary 46
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience
Contents
Chapter 6 48Findings Part 3: Developing Service Capacity
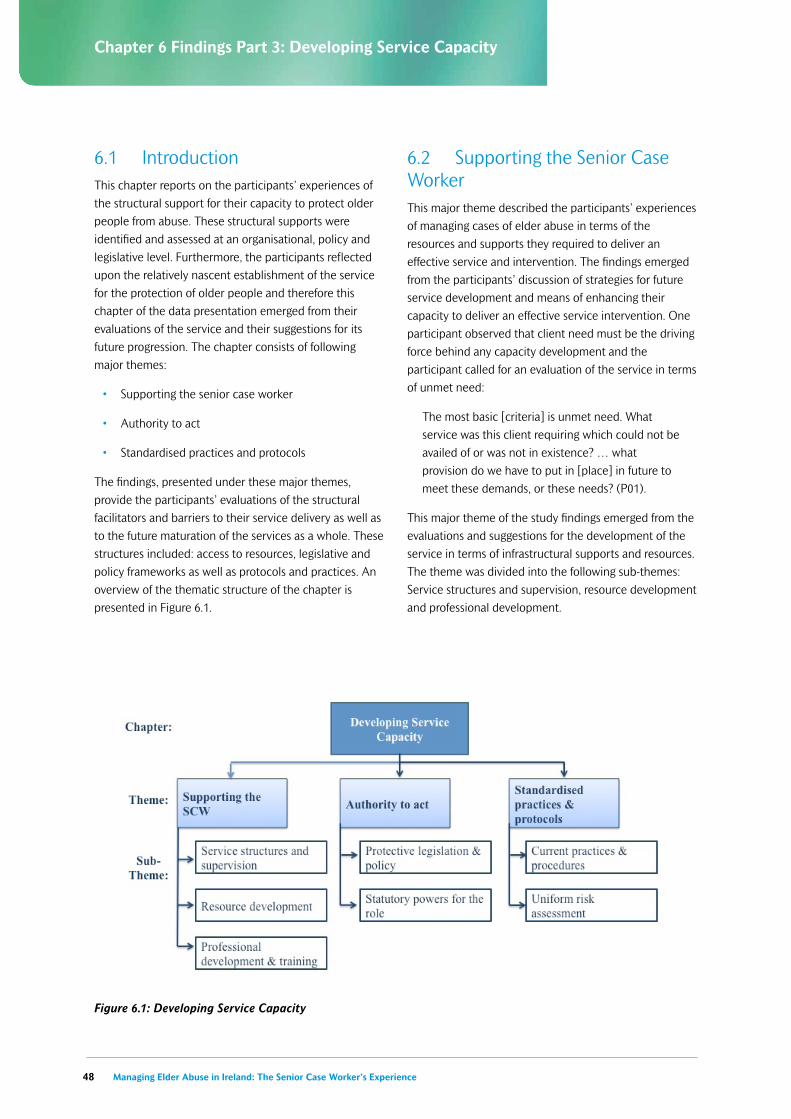
6.1 Introduction 48
6.2 Supporting the Senior Case Worker 48
6.2.1 Service Structures and Supervision 49
6.2.2 Resource Development 50
6.2.3 Professional Development and Training 52
6.3 Authority to Act 54
6.3.1 Protective Legislation and Policy 54
6.3.2 Statutory Powers for the Role 55
6.4 Standardised Practices and Protocols 56
6.4.1 Current Practice and Procedures 56
6.4.2 Uniform Risk Assessment 58
6.5 Summary 58
Chapter 7 60Discussion
7.1 Introduction 60
7.2 The Complexity of Elder Abuse in Context 61
7.2.1 Sources of Vulnerability 61
7.3 The Practice of Protecting Older People 62
7.3.1 Assessment and Intervention 63
7.3.2 Interagency Working 64
7.3.3 Client Relationship Management 65
7.4 Challenges to Managing Elder Abuse 66
7.4.1 Structural Barriers and Limitations 66
7.4.2 Effective Interagency Communication 67
7.4.3 Balancing Self-determination with Risk 68
7.5 Augmenting the Protection of Older People 69
7.5.1 Developing Resources 69
7.5.2 Standardising Practice 70
7.5.3 Legislative and Statutory Implementation 71
7.6 Limitations 71
Chapter 8 72Conclusion and Recommendations
8.1 Conclusion 72
8.2 Recommendations 72
References 75
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience i
Executive Summary
Relative to other countries, public and professional awareness of elder abuse and policy responses to elder abuse have occurred only recently in Ireland. Nevertheless, since the publication of Protecting Our Future Report in 2002, significant progress has been made in offering a national response to the problem of elder abuse. A key response was the introduction of a dedicated elder abuse service by the Health Service Executive (HSE) in 2007. This included the development of an intervention service for the management of cases of elder abuse delivered by senior case workers for the protection of older people. The senior case workers investigate allegations of elder abuse and work with older people, their families and carers to resolve alleged cases of abuse within the framework of existing policy and legislation.
A review of the literature on systems and strategies for responding to elder abuse points to a vast array of interventions but little guidance as to what might be the most effective approach to helping older people who have been abused or are being abused. Legislation, policy and models of service provision vary widely internationally, and while it is possible to compare various elements of these approaches and to explore potential benefits and limitations, research reporting the efficacy of the responses is limited and it is therefore difficult to determine the merits of certain approaches over others. Likewise the evidence base to support any specific process of intervening is sparse.
While increasing numbers of innovative interventions are being piloted and evaluated, most of the studies published thus far have methodological limitations. Efforts to assess the effectiveness of various projects and systems have also been hindered by a lack of common definitions, theoretical explanations and agreement on desired outcomes.
The literature indicates that the management of elder abuse often involves difficult cases with many ethical challenges and complex dynamics involving the older person, the perpetrator, the practitioner and the service provider. Through a qualitative descriptive research design, this study explored the complexity and challenges of the processes involved in managing cases of elder abuse from the perspective of 18 Irish senior case workers. The aim of the study was to explore the
experience of managing cases of elder abuse from the perspective of senior case workers (SCWs).
A qualitative descriptive research design was adopted using one-to-one semi-structured interviews with senior case workers with responsibility for managing cases of elder abuse. The approach was aimed at permitting a fuller understanding of their experiences in managing cases of elder abuse in the community. Interviews were semi-structured and conducted according to a prepared topic guide to ensure all areas of interest were addressed in each interview. The interview data were transcribed verbatim and subjected to a four-phase analytic process resulting in a thematic structure which reflected the combined deductive and inductive analytic approach.
The study findings highlighted the interlocking forms of abuse encountered by senior case workers and the fluid boundaries between the various forms of abuse. This meant that elder abuse was experienced as a complex phenomenon and therefore difficult to recognise, detect and manage. The senior case workers recognised the particularities of elder abuse cases, which each presented their own unique challenges, issues and dilemmas for social work practice. These particularities included the challenge of reconciling the autonomy and self-determination of their clients with issues of capacity, risk and vulnerability. Additionally, they described the necessity to manage cases of family conflict and entrenched patterns of familial behaviour. The management of this unique phenomenon was understood by the study participants to be highly demanding, in terms of assessing client capacity, making ethical judgements and using interpersonal skills.
Senior case workers provided accounts of case management, from the initial referral to the final case evaluation, showing how the multifaceted nature of elder abuse and its unique complexities and challenges determined the day-to-day practicalities and functions involved in case management and the provision of protective interventions. They spoke about the critical importance of effective interagency relationships and highlighted some of the challenges that they experienced in establishing and maintaining these relationships. The negotiation of role boundaries and responsibilities and the need to reconcile medical and social work discourses concerning best practice were described as potential sources of inter-disciplinary tension. The senior case
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experienceii
Executive Summary
workers pointed to the role of awareness-raising and training as a way to address this challenge. They provided evaluative data concerning the structural and resource contexts in which they operated, pointing to the need to balance resources and case management, which has implications for the delivery of services to those deemed to be at low risk or living in isolated rural locations.
The senior case workers offered their perspectives on the development of protective services, with reference to the capacity of the senior case worker service and the policy and legal framework in which the service is located. Many advocated a team-based approach to the protection of vulnerable adults and the management of cases of elder abuse. They perceived limited resources, inadequate training and a lack of clinical supervision as factors impacting on their service capacity. These structural limitations were described by the senior case workers as contributing to their sense of working on their own and disadvantaging older people living in isolated areas.
The senior case workers identified a need for increased protective legislation for older people and greater statutory powers for the role of the senior case worker. They also spoke of the need for better regulation of solicitors and care professionals and greater statutory authority for their own role in protecting older people from abuse. The senior case workers gave their perspectives on current practice and procedures, identifying a need for standardised procedures, greater consistency across the service regarding best-practice guidelines, procedures for case referral and documentation, and the maintenance of case statistics.
The findings of this study make an important contribution to understanding the complexity and challenges in managing cases of elder abuse in Ireland by revealing the nuanced and multifaceted experiences of 18 Irish senior case workers responsible for managing cases of elder abuse. These experiences are not unique to the Irish context and are reflected in published work on the management of elder abuse in other countries.
The senior case workers’ reports of their practice in light of the challenges and dilemmas faced by them in managing cases of elder abuse suggest a number of recommendations, which are offered within the limitations of this study. Recommendations for the practice of assessing risk and preventing elder abuse
include the need to consider targeted interventions to promote older people’s self-esteem and enhance their own psychological resources, to continue to examine the social networks of older people as part of risk assessment, and to consider efforts to secure a supportive social network for older people as part of elder abuse case management.
Among recommendations for case management approaches include the need to promote a multi-disciplinary approach and interagency working and to consider ways to formalise existing inter-professional communications and effective interagency and multi-disciplinary working. It is recommended that senior case workers’ access to and use of care services, which form part of their intervention response in managing cases of elder abuse, be monitored. It is also recommended that caution be applied in drawing on a single case management model and that flexibility in the use of models for managing cases of elder abuse should be applied, so that a chosen model is capable of addressing the complexity that inheres in individual cases of elder abuse.
Recommendations in relation to supporting senior case workers in their role include the need to evaluate current policy guidelines for the SCW role, with the aim of ensuring that the SCW role is supported by clear guidelines that give direction, but also take into account the need for flexibility and the retention of existing informal procedures that are effective in helping them in their practice. It is also recommended that resources to support SCWs’ case management be further explored along with issues of clinical supervision and peer support for SCWs in their role and that the training needs of SCWs be reviewed on a regular basis. Any increase in the statutory power and authority for the role of the senior case worker or other proposed legislative changes need to be tempered with a need to respect the older person’s right to self-determination.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 1
Chapter 1 Introduction
1.1 BackgroundSince the 1970s, elder abuse has become increasingly recognised and accepted as a global problem. As the population of older people continues to grow worldwide, many countries have begun to take measures to respond to and address this societal issue. In Ireland, public awareness and professional acknowledgment of elder abuse occurred relatively recently. However, significant progress has been made in offering a national response to the problem of elder abuse, with the introduction of a dedicated elder abuse service by the Health Service Executive (HSE) in 2007. This response included the development of an intervention service for the management of cases of elder abuse delivered by senior case workers. The senior case workers investigate allegations of elder abuse and work with older people, their families and carers to resolve alleged cases of abuse within the framework of existing policy and legislation.
Despite these developments there is still a dearth of high quality research on elder abuse both in Ireland and internationally. Elder abuse is a complex and sensitive issue, which to date lacks a sound theoretical base (Penhale 2006). A lack of agreement concerning definitions and causes makes it a challenging area to research. Accordingly, there is still little consensus on best practice in response to elder abuse. The aim of this study, therefore, was to explore the experience of managing cases of elder abuse from the perspective of senior case workers. The objectives of the study were to:
• Explore senior case workers’ experiences in managing cases of elder abuse
• Examine current practices adopted by the senior case workers
• Examine the challenges and dilemmas faced by senior case workers in managing cases of elder abuse and how these are overcome
• Identify good practice in the management of elder abuse cases, as perceived by the senior case workers
• Ascertain priorities for future service development and provision for elder abuse, as perceived by the senior case workers.
1.2 Report Structure
This report is presented in seven chapters. Chapter 1 presents the background and rationale for the study, and offers an overview of developments in response to elder abuse in Ireland and a range of other countries. This provides a global and national context for the study. Chapter 2 provides a review of the literature on the management of elder abuse cases in practice, including modes of intervention and the availability of evidence for their effectiveness. Chapter 3 provides a description of the research design and methods of participant recruitment, data collection and analysis. This study employed a qualitative research design in order to ascertain the perspective of senior case workers on managing cases of elder abuse. This ensured that the research findings were grounded in the experiential knowledge of the senior case workers. The findings which emerged from a thematic analysis of the interview data are presented in Chapters 4, 5 and 6. These chapters are structured according to the major themes which emerged from the data analysis through a combined process of deductive and inductive reasoning. This ensured that the analysis and the findings were informed by the experiences and perspectives of the senior case workers.
Existing national and international knowledge in the areas of the protection of older people and the management of elder abuse provide a context for the interpretation of the study findings, which are presented in Chapter 7. Furthermore, this discussion identifies the contribution that this study makes to existing literature in the relevant fields. Finally, the conclusion of the report indicates the key findings of this study in relation to the core study objectives. These objectives are concerned with the current practices and challenges of senior case workers in their management of elder abuse as well as identifying good practice and ascertaining priorities for future service development.
1.3 International Developments in Response to Elder Abuse Countries around the world are at varying stages in the development of national and local responses to protect older people from abuse (WHO 2002). Some countries have advanced policies, laws, and services to address the problem, while certain others have made little if any progress in acknowledging the existence of elder abuse
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience2
Chapter 1 Introduction
at all. The United States (US) has long been considered at the forefront of research and practice in elder abuse (World Health Organisation (WHO) 2002, Perel-Levin 2008). Adult Protective Services (APS) are at the core of the US response to elder abuse and play a pivotal role in investigating and responding to alleged cases of mistreatment (Bonnie and Wallace 2003).
The majority of states in the US employ dedicated adult protection workers to work with adults of any age who are considered vulnerable to abuse or neglect (Stiegel and Klem 2007). Mandatory reporting requirements are also a prominent feature of this protection-oriented service model (Bonnie and Wallace 2003, Desmarais and Reeves 2007, Brownell 2010). However, there are some exceptions to a policy of compulsory reporting; for example in New York authorities have resisted the introduction of mandatory reporting laws, based on concerns about the civil liberties of older adults. They have focused their attention on education and prevention rather than protection (Brownell 2010). Specialist multi-disciplinary elder abuse teams are also increasingly involved in the response to elder abuse in some areas, providing education, and assessment and assistance in dealing with complex cases (Dyer et al. 2005, Nerenberg 2006). Many states in the US have long standing formalised protocols for referrals and inter-disciplinary interaction. Alongside protective services, the involvement of criminal justice in the area of elder abuse has grown. Elder abuse is increasingly being criminalised in state legislation and rising numbers of cases are being prosecuted annually.
Protective service models have been introduced in Canada and in Norway; the latter country’s government funded a pilot project establishing Elder Protective Services in Oslo. This pilot project has since been adopted by other municipalities in Norway. Where elder protective services have been developed, there are specialist workers in place who act as the focal point for all cases relating to the abuse of older people. However, although services were influenced by the systems developed in the US, there are important cultural, ideological and organisational differences in their approach (Juklestad 2004). In Norway, there tends to be more emphasis on the principles of client autonomy, advocacy and rights (Johns and Juklestad 1995). There is no national policy and no specific legislation to deal with elder abuse in Norway. However, the Norwegian
government has made education and awareness-raising key priorities for the prevention of elder abuse and has funded a resource centre as well as a telephone helpline to assist victims of abuse.
The UK addresses elder abuse within the context of vulnerable adults and adult protection is usually managed within mainstream adult social care services rather than dedicated services. Elder abuse is addressed primarily through guidance, policy documents and codes of practice, emphasising appropriate procedures to follow in cases of abuse of vulnerable adults of any age. Reporting of suspected abuse is not mandatory in the UK but legislation and policies are in place to protect those who do disclose suspicions of abuse. The emphasis within the UK model is on achieving an appropriate balance between autonomy and protection. National guidelines are presented in the document No Secrets, which recommends the establishment of multi-disciplinary adult protection committees at local level to facilitate interagency collaboration and partnership working (Department of Health 2000). There has also been an emphasis on regulation and inspection within health and social care services. A number of new initiatives have been proposed by the UK Government, including putting adult protection committees on a statutory footing and increasing emphasis on the law around safeguarding adults (Department of Health 2010). However, in contrast to the US, and similar to other European countries, the UK response is focused upon providing necessary services to end abuse and restore relationships, rather than punishing perpetrators (Filinson 2006).
Australia has no national federal policy on elder abuse and most states do not have dedicated or specialist services to identify and assist victims of elder abuse (Lowndes et al. 2009). However, individual states and territories have begun to develop strategies to respond. For example, the Australia Capital Territories, South Australia and Queensland have funded specialist information and education services to provide telephone assistance and referral support in dealing with suspected cases of abuse. In Victoria, Senior Rights Victoria (SRV) was established in 2008 to safeguard the rights of, dignity and independence of older people. SRV acts as a point of contact for older people, concerned family or friends, professionals or members of the general public and provides legal services, advocacy and support, and referrals to health and social services in the community
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 3
Chapter 1 Introduction
(Victorian Government Department of Human Service 2009). In other Australian states, cases of elder abuse tend to be dealt with by existing services such as Aged Care Assessment Teams.
Elder abuse has been explored from many different perspectives and there is ongoing debate as to whether it is primarily an issue of human rights, domestic violence, public health, adult protection, criminal justice or empowerment. These overall paradigms can shape responses to elder abuse, and influence the types of laws enacted in a country, the policies developed and the services made available. The approaches adopted to deal with abuse are often dependent upon the discipline or theoretical background of those responsible for responding to the problem within each country. Social work practitioners and advocates, for example, tend to welcome an empowerment model. This model focuses on restoring power to the victims by encouraging them to exercise their right to self-determination, and ensuring that interventions reflect their preferences (Nerenberg 2008). However, the empowerment model is at odds with the core principles of other systems such as criminal justice which concentrate on protecting the public and holding offenders accountable rather than on the empowerment and support of the victim.
1.4 The Irish Response to Elder AbuseRecognition of elder abuse within the professional health and social care realm in Ireland began with the publication in 1990 of two case reports in Irish medical and social work journals. In 1996 a preliminary briefing on elder abuse was prepared by the National Council for the Elderly and submitted to the Minister for Health. The National Council on Ageing and Older People subsequently commissioned an exploratory study on elder abuse in an Irish context following media reports of a number of particularly distressing cases. The resulting report entitled Abuse, neglect and mistreatment of older people: An exploratory study, published in 1998, explored the issue of elder abuse in the light of Irish and international literature and the views of service providers. The report made recommendations on the mechanisms needed to effectively address the problem of elder abuse in terms of policy and infrastructure (O’Loughlin and Duggan 1998).
Out of the recommendations from this report, a Working Group on Elder Abuse (WGEA) was established to advise the Irish government on what was required to effectively and sensitively address the issue. The working group, made up of representatives from relevant agencies in the voluntary, public and private sectors, established a pilot project in two health board areas to inform future plans and policy development. The pilot programme allowed the working group to test and evaluate how draft procedures and guidelines worked in practice. The group also assessed the effectiveness of a specially designed training programme for health and social care staff. The report of the WGEA, Protecting Our Future, was published in 2002 and set out a framework for the development of policies and procedures to respond to actual or alleged cases of elder abuse. It also set out the infrastructure necessary for the implementation of the proposed policies and procedures (WGEA 2002). Recommendations were made in areas such as policy, staff structure, legislation, impaired capacity, carers, awareness, education and training, financial abuse, advocacy, research, reporting abuse, and implementation and review of the recommendations. At the time of writing, Protecting Our Future remains the seminal document on elder abuse in Ireland.
Following the publication of Protecting Our Future in 2002, the Irish government established an Elder Abuse National Implementation Group (EANIG) to oversee the implementation of the recommendations contained within the report. Established in December 2003, the group was recently disbanded. EANIG was a multi-disciplinary group made up of representatives from a wide range of agencies working with older people. The group had a key role in progressing the development of services to respond to elder abuse and in particular the establishment of the current HSE-dedicated elder abuse structures (NCAOP 2009).
1.4.1 HSE Dedicated Elder Abuse Structures
Significant progress has been made in recent years in Ireland in the development of a national response to the problem of elder abuse. This progress has been primarily driven by the health sector. This has placed considerable emphasis on research, policy development, education and awareness-raising, as well as on the provision of dedicated elder abuse services. In 2007 the HSE established a new specialist service intended to provide a coordinated and holistic approach to elder abuse, based
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience4
Chapter 1 Introduction
on a modified version of that proposed in Protecting Our Future in 2002.
A multi-disciplinary National Elder Abuse Steering Group and four Area Elder Abuse Steering Groups were established to oversee the provision of elder abuse services by the HSE as well as the implementation of the recommendations of Protecting Our Future. Four Dedicated Officers for Elder Abuse posts were created in four HSE administrative areas, namely HSE West, HSE South, HSE Dublin Mid-Leinster and HSE Dublin North East. At the time of writing, the position in HSE South was vacant. These dedicated officers have responsibility for the development, implementation and evaluation of the HSE elder abuse services. They deal with the implementation and on-going review of elder abuse policy and contribute to strategic planning, development of services, training, and collation of statistics.
In practice the service is delivered by qualified social workers, known as senior case workers (SCWs), who deal primarily with suspected cases of abuse referred to the HSE, involving people aged 65 and over. Up to 30 senior case workers (SCWs) for the protection of older people are employed in local health offices (HSC 2011). SCWs investigate allegations of elder abuse and work with older people, their families and carers to resolve alleged cases of abuse within the framework of existing policy and legislation. Senior case workers are primarily based within primary community and continuing care services, reporting to the general manager, and collaborating with Dedicated Officers for Elder Abuse, and other relevant stakeholders.
A recent report, entitled Review of the Recommendations of Protecting Our Future: Report of the Working Group on Elder Abuse, published in early 2010, examined the structures established by the HSE in relation to the management of elder abuse and found that significant progress had been made in implementing the recommendations contained within Protecting Our Future, particularly within the health sector (NCAOP 2009). However, a number of issues were highlighted relating to the response provided by this specialist service. These included regional inconsistencies in approach, a lack of interagency cooperation, in particular, a need for senior case workers to be more fully integrated into the wider services for older people and a lack of professional supervision for SCWs in some areas (NCAOP 2009).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 5
Chapter 2 Managing Elder Abuse in Practice
2.1 IntroductionThis chapter provides a detailed review of literature on the operational processes associated with the procedures and systems adopted nationally and internationally for dealing with cases of elder abuse. The review concerned with the processes of managing cases of elder abuse found an absence of research directed at evidence-based practice. Several descriptive studies were found, with a limited number of quality primary studies on which to base recommendations for practice (Kalaga et al. 2007, Ploeg et al. 2009). The literature suggests a wide variety of approaches for managing cases of elder abuse but overall responses to the problem are generally considered to be inadequate (Nerenberg 2006, Ploeg et al. 2009).
Arrangements for managing cases of elder abuse are likely to vary depending on the nature of the case, the local and national management and organisational structures, and the skills, experience and interests of individual practitioners. Cambridge and Parkes (2004b) identified a number of stages in the process of managing adult protection cases in the UK, which included initial referral or alert, preliminary investigation, planning meetings, investigation by social services or police, case conference and case closure or on-going monitoring. The authors acknowledged that adult protection cases are frequently complex and do not necessarily follow a sequential model. In many cases there may be multiple or parallel investigations and concurrent planning or case conferences as new evidence emerges.
2.2 Aims and Method of Literature ReviewA review of literature was conducted to locate the present study within the context of international published literature on the topic. The purpose of the literature review was to provide background information to inform the development of the research and to establish the current state of knowledge and evidence on the process of managing elder abuse cases in the community and the various intervention strategies employed.
A thorough search was carried out using four electronic databases: CINAHL Plus, Embase, Medline and PsychINFO. The terms “elder abuse” and “elder mistreatment” were searched in combination with
keywords such as assessment, best practice, detection, identification, intervention, management and strategy. Only literature published in the English language were searched. Additional references, including relevant articles and grey literature, were also retrieved. This retrieval was informed by the reference lists of the selected papers and from a Google search using a number of the same search terms.
Literature addressing self-neglect or abuse in institutional settings, such as nursing homes, long-term care facilities or hospitals, was considered outside the scope of this review and were excluded accordingly. These types of abuse and neglect are likely to have distinct and different causes and outcomes and are considered better addressed separately (National Research Council 2003). The majority of the literature originated in the United States, Canada and the United Kingdom. However, a small number of papers from other countries such as Australia, Ireland and Israel were also included.
2.3 Detection and Referral Detection is a critical first step in the effective management of the problem of elder abuse. Halphen et al. (2009) assert that the most beneficial intervention is reporting suspected cases of elder abuse to appropriate agencies or services. Interventions by designated authorities to manage the problem and prevent future incidents of abuse cannot occur without identification and referral. Although awareness of elder abuse has increased in recent years, there is a general consensus that detection and reporting rates continue to be low, and known cases are just the ‘tip of the iceberg’ (Baker and Heitkemper 2005, Perel-Levin 2008, Cooper et al. 2009).
Self-referral is uncommon in circumstances of elder abuse. This is attributed to a lack of physical means or mental capacity as well as feelings of shame and fear (Wolfe 2003, McGarry and Simpson 2011). An onus is therefore placed on agencies in contact with older people to be alert to any signs of mistreatment and to report concerns to appropriate authorities (Ross 2007). Research indicates that recognition of cases of elder abuse may be hindered by barriers to detection and identification. These barriers include a lack of awareness as well as difficulties distinguishing between age-associated disease and mistreatment (O’Loughlin and Duggan 1998, Penhale
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience6
Chapter 2 Managing Elder Abuse in Practice
2006). Furthermore, reporting may be complicated by a lack of knowledge about where to report suspicions (Bonnie and Wallace 2003, Halphen et al. 2009).
Screening tools have been suggested as the means of improving recognition of potential elder abuse cases (Anetzberger 2001). However, although several screening tools have been developed, none has gained widespread use (Bonnie and Wallace 2003, Fulmer et al. 2004, Anetzberger 2004, Perel-Levin 2008). Traditionally a key requirement of the screening process is a cut-off point for deciding whether a case is screened positive or negative. An assessment of the merits of this ‘cut off’ approach for managing cases of elder abuse has generated some debate. This debate has focused on the complexities of elder abuse and the necessity of employing a considerable degree of clinical judgement in the management of cases. Researchers have argued that the necessity for clinical judgement in elder abuse cases negates the use of statistical measures of risk (Bonnie and Wallace 2003). Elder abuse is a complex phenomenon with multiple causes and outcomes and there are no standard criteria for diagnosis (Fulmer et al. 2004). However, screening tools are believed to heighten professional awareness and guide users through a systematic process of observation and inquiry which ensures that potential cases of elder abuse are not missed (Anetzberger 2001, 2004). Some screening tools may therefore be useful for guiding professionals who have suspicions of abuse and thereby facilitate referral for further assessment.
Education, training, and support for professionals who may be likely to encounter elder abuse and neglect are considered a fundamental strategy for the increased detection of elder abuse (Lachs and Pillemer 2004, Perel-Levin 2008). Lack of knowledge has been shown to influence reporting rates for elder abuse amongst a range of health and social care professionals (McCreadie et al. 1998, McCreadie et al. 2000, Oswald et al. 2004). Killick and Taylor (2009) reported the results of a systematic review of professional decision-making and found that training and knowledge were shown to impact on the level of abuse identification.
Specific guidelines and protocols for identifying and responding to elder abuse are now considered essential in almost all health and social service professional organisations (Fulmer et al. 2004). Protocols may be
useful to ensure responses to suspected cases of elder abuse are consistent by highlighting key steps in the process (O’Loughlin and Duggan 1998, Lachs and Pillemer 2004, Saliga et al. 2004). These may include identifying indicators of abuse, reporting structures for suspected cases, comprehensive written documentation and procedures for referral (Anetzberger 2001, McGarry and Simpson 2011). They may be especially helpful in clarifying roles, responsibilities and accountability when there are multiple services and agencies involved in handling elder abuse cases (Anetzberger 2001). Finally, protocols may reinforce the responsibility on professionals to act when they suspect abuse has, or is likely, to take place (Wolfe 2003).
Consistency in policy and procedure is discussed in the relevant literature in terms of the benefits of standardised protocols for managing elder abuse. However, this literature also indicates concerns that structured protocols or guidelines may be overly simplistic to deal with the complexity surrounding many cases of elder abuse (O’Loughlin and Duggan 1998, Lachs and Pillemer 2004). Attempts have been made to overcome this problem. For example, The Ontario Association of Professional Social Workers outlined eight different decision trees to provide general reference points and to initiate decision-making processes. These models stress that no standard formula can deal with the complex issue of elder abuse (O’Loughlin and Duggan 1998).
In some countries, certain individuals, including health care and law enforcement professionals, are ethically and legally obliged to report suspicions of elder abuse or neglect (Cooper et al. 2009, Lowndes et al. 2009). Mandatory reporting laws typically contain definitions of abuse, specify who must report, and to whom reports should be made. Furthermore, they often incorporate penalties for failure to report concerns, including fines, or in extreme cases, loss of licensure (Fulmer et al. 2004, Nerenberg 2006). However, mandatory reporting remains a controversial issue and has never been subjected to rigorous evaluation (Bonnie and Wallace 2003, Perel-Levin 2008). According to Peri et al. (2008) research indicates that whether people report abuse, or not, has more to do with organisational, professional, cultural and ethical issues than whether there is a legal requirement to do so. The provision of legal protection for those who do disclose suspicions of abuse in good faith to an
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 7
Chapter 2 Managing Elder Abuse in Practice
appropriate authority is a widely employed strategy to encourage reporting.
There is little information in the literature on the practical process of referral and investigation into cases of elder abuse. Where mandatory reporting laws exist, there are usually specific designated recipients of reports. In the United States and Canada, this is usually the responsibility of Adult Protection Services (APS). Dayton (2005) describes the process of referral and steps in the investigation by APS in Ohio: The first contact between the person who refers the case and the APS intake officer should include discussion about the physical and mental capacity of the older individual, their ability to care for and protect themselves, and whether there are indications of abuse or neglect, based on definitions in local legislation or policy documents (Dayton 2005).
If elder abuse is suspected, one of the first steps must be to determine the urgency of the situation by assessing the risk to the older person’s safety (Cambridge and Parkes 2004b, Donovan and Regehr 2010). Cambridge and Parkes (2004b) report that the key skills considered necessary at this stage of an alleged adult protection case centred on keeping an open mind, the ability to listen and not over-react, having good communication skills, for example communicating with people with dementia, and having basic assessment abilities.
2.4 Investigation and AssessmentLocal laws or policy documents usually set out which agency or organisation is responsible for investigating suspected cases of elder abuse. In Scotland, for example, the Adult Support and Protection (Scotland) Act 2007 gives statutory responsibility to local agencies to investigate any risk of harm or abuse to older adults living in care homes or in the community and enhances powers to investigate allegations of mistreatment (Heath and Phair 2007). In the rest of the UK, guidance issued by the Department of Health and the Welsh National Assembly in 2000 under Section 7 of the Local Authority and Social Services Act 1970 gave local authorities, known as Councils with Social Services Responsibilities (CSSRs), the lead role in responding to adult protection and elder abuse. In the US, APS are usually the designated authority with responsibility to investigate and intervene in suspected elder abuse cases (Bonnie and Wallace 2003, Halphen et al. 2009). In Australia, assessments are
usually carried out by an Aged Care Assessment Team or an Aged Care Service (Kurrle 1993).
Investigations undertaken by Adult Protective Services (APS) in the US typically include a face-to-face home visit, an assessment of capacity and functional ability, and a needs assessment for medical, social, legal or financial services (Nerenberg 2006). Under Ohio State law an investigation by an APS social worker must begin within 3 days, or 24 hours in life-threatening cases (Dayton 2005). If the case is a re-referral, the case is assigned, where possible, to the social worker previously involved. A home visit is made, as a requirement of the law, and written notice is given of the purpose of the investigation, explaining that a call has been received by APS, indicating that the individual may have been abused, neglected, or exploited, or may be unable to take care of his or her own needs. The source of the referral remains confidential. The home interview is conducted in private and a critical issue is the assessment of mental status and capacity to make decisions. Investigations are likely to involve continued contact with the person who made the referral (Dayton 2005). They may also include interviews with the alleged perpetrator. Additionally, consultations with social security staff, mental health professionals, primary care physicians, home health staff, family, friends, neighbours, financial institutions and the police may be undertaken to obtain a comprehensive and accurate understanding of the situation (Dyer et al. 2005).
Fulmer et al. (2003) examined transcripts of discussions by a Neglect Assessment Team in a medical centre in New York relating to four practice cases and nineteen real cases. They found that much consideration was given to contextual information relating to the older person and their caregivers when assessing for potential neglect. This included information on the health and capacity of the older person and the caregiver, their social and economic circumstances, and the reliability of information from sources concerned. Similarly Lithwick et al. (2000) found that practitioners in community services in Canada were influenced by contextual factors such as cognitive impairment, intent, poor relationships and mutual abuse in cases where they struggled to decide whether behaviours constituted mistreatment or not.
Participants in a UK study reported by Cambridge and Parkes (2004b) advocated the necessity of a designated individual to coordinate or lead the investigation.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience8
Chapter 2 Managing Elder Abuse in Practice
According to Pratt et al. (1983) a sensitive personal approach to the older person and their family is crucial at the preliminary stage of an investigation, as it sets the tone for future interactions and may affect the way all subsequent interventions are perceived. Cambridge and Parkes (2004b) also identified communication, listening and negotiation skills as key abilities at this juncture. Accurate recording and reporting, good risk assessment capacity, ability to liaise with other agencies and services, ability to assess capacity to consent, and analytical skills were also identified as important attributes for professionals at this stage (Cambridge and Parkes 2004b). A good knowledge of policies, procedures, responsibilities and legislation, and the ability to assess the support needs of individuals are also considered critical (Cambridge and Parkes 2004b).
2.5 Intervention Strategies and Services ProvisionThe identification and reporting of elder abuse creates an imperative for the development of effective interventions and strategies to manage identified cases and prevent further mistreatment (Perel-Levin 2008). Intervention strategies for elder abuse involve the application of available services, laws and clinical procedures to treat the consequences of abuse or to prevent its occurrence or recurrence (Anetzberger et al. 2005). A wide range of practical and therapeutic interventions have been proposed, which aim to protect the welfare of individuals who have experienced abuse or are at risk of abuse. These responses to abuse are typically provided by health and social services. Interventions are delivered at a point of crisis, such as telephone help lines and emergency shelters, as well as longer-term interventions, including respite care, counselling and social support (Kalaga et al. 2007, Podnieks 2008). Intervention techniques are still in quite early stages of development and there is little evidence to support their effectiveness (Penhale 2006, Ploeg et al. 2009). Consequently, there is limited understanding about the interventions which are likely to be most effective in combating elder abuse (WHO 2011).
2.5.1 Case Management
Case management is one method of delivering a holistic response tailored to the specific needs of those involved in cases of elder abuse. This approach has been identified and recognised by many as an effective strategy to
improve quality of care and outcomes for older people (Luu and Liang 2005). Case management may be provided by public or private agencies on an on-going basis (Dayton 2005). Case managers, usually nurses or social workers, are responsible for performing comprehensive assessments as well as developing care plans and coordinating the delivery of health and social care services (Luu and Liang 2005). The goal of case management is generally to maintain the highest level of independence and autonomy possible (Nerenberg 2008). Case managers act as advocates, educators and facilitators (Luu and Liang 2005). While there are several models of case management, they generally all share a common purpose, linking clients with essential resources and services (Hepworth et al. 2010).
Some early work on elder abuse highlighted the importance of coordination of referrals to prevent older people becoming lost within a complex system of agencies and professionals (Pratt et al. 1983). Case management can prevent fragmentation in the provision of services and ensure no information is lost between disjointed services and agencies (Luu and Liang 2005, Kalaga et al. 2007). Case managers closely monitor the progress of clients, respond to problems or emergencies, and conduct routine re-assessments to evaluate the effectiveness of the care plan and detect any changes in need (Nerenberg 2006). This is especially important as the needs of older people are often dictated by functional ability which may fluctuate over time (Nerenberg 2008). The case management approach has been implemented in Ireland in recent years through the SCWs who investigate, respond to and manage suspected cases of elder abuse (HSE 2009).
2.5.2 Monitoring
Monitoring has been identified as one of the core tasks of case management and was one of the most commonly reported interventions provided to victims of elder abuse in Ireland in 2010 (HSE 2011). Shibusawa et al. (2005) described a case study illustrating the way on-going monitoring is employed as an intervention strategy by social workers in Japan where mistreatment is suspected. In this case periodic home visits were utilised to give social workers the opportunity to continue to observe the older person’s condition and circumstances, and to establish an on-going trust relationship with the client and their family and caregivers.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 9
Chapter 2 Managing Elder Abuse in Practice
2.5.3 Counselling
Counselling was the third most commonly-recorded intervention for victims of elder mistreatment in Ireland in 2010 (HSE 2011). Low self-esteem and stress can place many older people at risk of abuse or neglect and can reduce their ability to cope with abusive situations (Podnieks 2006). Many victims of elder abuse develop feelings of fear, guilt, shame, isolation and anger. Counselling may be an important and effective therapeutic intervention to help older people who have experienced abuse to alleviate traumatic stress, understand their feelings, regain a sense of independence, emotional strength and self-esteem, and to prevent recurrence of abuse or mistreatment (McKenzie 1999, Podnieks 1999, Nerenberg 2006, Kalaga et al. 2007). Counselling is considered one of the most highly valued services available to victims of elder abuse (Nerenberg 2008). In a qualitative study reported by Hightower et al. (2006), involving 64 women over 50 years of age in Canada, women spoke of the emotional abuse they suffered, including being put down and ridiculed. All of the women in the study spoke of a need for emotional support, someone trustworthy to listen to them, to believe them and keep their confidence, as well as offer practical advice.
2.5.4 Support Groups
Social support has been identified as a potentially protective factor against elder mistreatment. Research has found higher levels of social support to be independently associated with a lower risk of self-reported mistreatment (Naughton et al. 2010), while victims of abuse with less social support are thought to have higher levels of psychological distress (Fulmer et al. 2005, Dong and Simon 2008). Older adults who experience abuse may be more socially isolated and have fewer social contacts than non-abused older people (Podnieks 2006). Community-based support groups have therefore been proposed as effective interventions for both perpetrators and victims of elder abuse (Podnieks 1999, Hightower et al. 2006, Dong and Simon 2008). Pritchard (2007) describes the organisation ‘Beyond Existence’ in the UK, which, following a pilot study, had successfully secured funding to offer support groups for older people experiencing and recovering from abuse. Support groups act as a source of affirmation, information and education, creating an empowering environment (Podnieks 1999).
Support groups have been used with women who were victims of domestic violence and are purported to have many psycho-social benefits such as the development of mutual support relationships with peers, moving past guilt, enhancing self-esteem, and learning problem-solving and coping strategies (Podnieks 1999). In a qualitative study of older women’s experiences of domestic violence, Schaffer (1999) found that older women valued having peer support and other women of similar age to talk to about the abuse. The assumption behind support groups is that people who have had similar experiences are better equipped to understand and empathise with people experiencing or recovering from abuse (Nerenberg 2008). Traditionally the term ‘support group’ referred to informal gatherings of people who were experiencing similar life events and were led by lay persons. However, more recently the term is also applied to more formal circumstances where professionals introduce therapeutic and educational methods within a group setting (Nerenberg 2008).
The literature reveals that endorsements for the benefits of support groups are based primarily on anecdotal evidence (Brownell and Heiser 2006). One of the few empirical evaluations produced findings that may question the efficacy of support groups as an intervention. Brownell and Heiser (2006) carried out a pilot study with 16 women, 9 of whom received a weekly 2 hour psycho-educational support group intervention for 8 weeks, while 6 were randomly assigned to a control group. The support group was facilitated by a graduate social work student and a retired professor, and covered a range of topics including: domestic violence, abuse neglect, family dynamics, self-esteem, depression, anxiety and stress, strategies for change, and services and resources available. Interviews were conducted two months before and after the intervention and no significant differences were found between or within groups on outcome measures including depression, guilt and self-esteem. However the authors noted that all but one of the participants reported that the group was helpful in increasing their self-esteem and well-being. Due to the small sample size and the limited information available about the measures employed, these results were far from conclusive (Ploeg et al. 2009). More information is still needed to determine the effectiveness of this type of intervention and how it may benefit victims of elder abuse.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience10
Chapter 2 Managing Elder Abuse in Practice
Support groups for perpetrators of elder abuse have also been proposed based on the principles of groups involving men who have committed domestic abuse, although few programmes are in place (Podnieks 1999). The group Lifespan in Rochester in New York runs one of the first groups for perpetrators of elder abuse. Entitled Stop Elder Abuse and Mistreatment (SEAM), the intervention entails a 16-week programme intended to change attitudes and behaviour, and prevent further mistreatment by raising awareness of the impact of abusive actions on victims (Nerenberg 2006). Programmes in San Francisco and Los Angeles have also experimented with small groups targeting perpetrators and using cognitive behavioural techniques to alter violent behaviour (Bonnie and Wallace 2003). No data was identified in the course of this literature review that evaluated the effectiveness of such programmes but the few methodologically-sound evaluations of programmes for abusive men in domestic violence cases are not especially encouraging. Dropout rates from programmes, even when court-mandated, are quite high and differences in repeat offending between those who attend interventions tend to be small and generally not significant (Wolfe 2003).
2.5.5 Interventions for Caregivers
Early research on elder abuse was frequently based on the premise that the stress or burden of caring for a dependent older person, or the lack of care-giving experience, knowledge and resources could lead to abuse or neglect (Reingold 2006, Nerenberg 2008). On this basis, training, education and support programmes are seen as vital aspects of prevention and management of elder abuse within a care-giving relationship (Wolfe 2003, Ross 2007). Self-assessment tools have been designed to help caregivers assess their own risk of becoming abusive (Nerenberg 2008). Caregiver support groups are intended to reduce isolation and provide emotional support and guidance in how to meet the demands of care giving and how to handle difficult behaviour which may increase tension and give rise to stress (Nerenberg 2008).
The extent to which training interventions with caregivers may reduce the risk of abuse or neglect is still a matter of debate (Nerenberg 2008). One study by Scogin et al. (1989), for example, found no statistical differences in terms of anger, self-esteem, caregiver burden or general
mental health between caregivers who received 8 weekly training sessions and those caregivers who had no such training. However, no information is provided in the study to ascertain whether there were differences between groups at baseline data collection (Ploeg et al. 2009). Other studies suggest that interventions targeted at abusive caregivers may help prevent re-offending (Nahmiash and Reis 2000, Reay and Browne 2002). Nahmiash and Reis (2000) found that strategies focused on the abuser, such as individual and family counselling, were the second most successful interventions after medical and nursing care provision. This approach to prevention and management of elder abuse is controversial. Recent research has shown correlations between abuse and higher care burden (Cooper et al. 2009). However, some researchers question the evidence linking elder abuse and caregiving stress (Lachs and Pillemer 2004). More research is needed to evaluate not only the efficacy of interventions with caregivers but also the role of care giving as a risk or causal factor as such interventions may have preventive potential in only a limited subset of cases (Pillemer et al. 2007).
2.5.6 Home Support Services and Respite Care
The most common intervention strategy employed by social workers who encounter abuse and neglect in family care giving situations in Japan is the arrangement of formal care giving services (Shibusawa et al. 2005). In Ireland in 2010 one of the most common interventions recorded by senior case workers was the provision of home support services, offered to approximately 20 percent of clients (HSE 2011). In a qualitative evaluation of 473 interventions used in 83 cases of elder mistreatment perpetrated by caregivers in Canada, a multi-disciplinary team rated general medical, nursing and rehabilitation strategies as the most successful in terms of stopping or reducing abuse or solving the identified problem (Nahmiash and Reis 2000). Professionals working with elder abuse victims have suggested that many abusive situations could be prevented if carers had more access to resources (Pritchard 2000). Services also suggested to relieve the burden of care-giving and prevent elder abuse include house-keeping, meal preparation or delivery, transportation and friendly visitors (Pillemer et al. 2007). Provision of support services can help to promote independence for those living in the community, reduce
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 11
Chapter 2 Managing Elder Abuse in Practice
social isolation and take pressure off informal caregivers (Nerenberg 2008). Service providers also note that offering support services is a credible means to establish a positive trusting relationship with clients who may be unwilling to take action against the perpetrator of abuse (Nerenberg 2008).
Respite care services can provide relief to caregivers for anything from a few hours up to extended periods. These services are delivered either through professional or volunteer carers, in the home of an older person, at day centres or in institutional settings (Nerenberg 2006). A three-year follow up study of victims of elder abuse in an area-based aged care service in Australia found that, despite the provision of community services and respite care, a significant proportion of older people remained in abusive situations. However, according to the author these community services were valued as much for personal contact as for the provision of practical assistance (Kurrle 1993).
2.5.7 Emergency Shelters, Refuges, Safe Houses and Long Term Care
Emergency shelters and refuges have been a central component in the response to domestic violence (O’Loughlin and Duggan 1998). In some circumstances older people may also require a ‘safe haven’ to remove them from an unsafe setting to avoid imminent or further abuse. Emergency refuge for older people may take the form of battered women’s shelters which have been adapted to meet the needs of older women, nursing home facilities, or shelters specifically designed for victims of elder abuse (Nerenberg 2006). However, domestic abuse services are often ill-equipped to deal with the specific and complex needs of older people, especially those who may be physically frail or lacking mental capacity (Kalaga et al. 2007). Qualitative research indicates that older women often find shelters chaotic places (Hightower et al. 2006). The literature contains few reports of specific elder abuse shelters.
The Weinberg Center in New York provides one example of a long-term shelter dedicated to victims of elder abuse (Reingold 2006). The shelter is accessed via a 24 hour free phone number, providing an initial contact point for crisis intervention. If telephone screening indicates a need for emergency shelter, triage and multi-disciplinary assessments are undertaken by staff from a medical day programme called Elder Serve. These staff members are
specially trained to address the needs of elder abuse victims. A dedicated, comfortable, safe and secure short term stay unit is available for emergency housing and support for older men and women for whom it is unsafe to return to their homes. This shelter is housed within a larger residential complex for older people, known as the Hebrew Home. This allows for the provision of a wide array of services and takes advantage of existing expertise in the care needs of vulnerable older people. Although dedicated to victims of abuse, this short stay unit also houses other short-term older residents because it is considered that integration may be beneficial for previously isolated older people by removing the stigma associated with abuse and fostering social support (Reingold 2006). Similarly, shelters for women experiencing domestic abuse are considered a means of developing support networks (O’Loughlin and Duggan 1998, Hightower et al. 2006). Victims of elder abuse may stay in the unit for approximately 30 days, after which arrangements are made either to return home, if safe, with community support services such as counselling and legal advocacy, or to transfer to either sheltered housing or admission to long-term residential care. While short-term removal from the abusive situation may be beneficial in some circumstances, interventions in elder abuse often result in long-term residential care.
The Kerby Rotary House in Calgary, Canada, was one of the first purpose-built shelters for abused older people. This service offers safe and secure shelter to men or women, alongside crisis intervention, support, advocacy and referral (Alberta Elder Abuse Awareness Network 2009). In Scotland, the Dumfriesshire and Stewartry Women’s Aid designed one of its shelter specifically for women over the age of 50. This organisation also employs a full-time project worker to provide support, counselling and advice to older women, which continues after they have been resettled (Kalaga et al. 2007). The Westgate Foundation in Cork currently offers the only emergency shelter accommodation in Ireland for older people who have suffered any type of abuse. This facility was established after examining the best international examples and consultation with social workers and health workers throughout the area (Cork Independent 2009). The shelter accepts referrals from GPs, social workers, and a wide range of other agencies.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience12
Chapter 2 Managing Elder Abuse in Practice
2.5.8 Telephone Services
Telephone helplines have been introduced in a number of countries, including France, Belgium and Israel, and have been considered an effective source of information and support for individuals who have been affected by any type of abuse or who may be at risk of abuse (Kalaga et al. 2007, Penhale 2007). These services can provide verbal counsel with the reassurance of confidentiality and anonymity (Kalaga et al. 2007). They may also be helpful for any concerned members of the public or professionals requiring additional information. Elder Abuse Response, run by the charity organisation Action on Elder Abuse, is one example of this type of service. Launched in 1997 following a successful 12-month pilot project in four areas of the UK, this is the only national helpline in the UK or Ireland dedicated to elder abuse (Action on Elder Abuse 2004). It is operated by specially trained staff and volunteers providing free confidential information and advice to members of the public (Action on Elder Abuse 2004). In Ireland, a number of telephone helplines have been introduced. The HSE offers a national information telephone helpline which provides details of HSE staff who can assist older people who are being abused. Also, a confidential senior helpline is offered by a voluntary organisation called Third Age. This service is a telephone listening service for older people and is manned by trained older volunteers.
2.5.9 Daily Money Management (DMM)
Daily money management (DMM), including assistance in paying bills, writing cheques, and making bank deposits or withdrawals is gaining popularity as a potential practical intervention to reduce the risk of financial abuse. The Jacob Reingold Institute at the Brookdale Center on Aging is considered a good example in this area. The institute undertook a survey of 200 case management and health care providers in New York City about their experiences with elder financial abuse. The study found that promoting the development and expansion of daily money management services could significantly reduce the problem of financial abuse of older people (NCPEA 2009). The Reingold Institute provides technical assistance and training materials to encourage agencies to set up money management services (Nerenberg 2006). A recent cost analysis study by the Reingold Institute reported significant cost savings when compared to alternatives such as Adult Protection Services (APS) and recommended inclusion of DMM as a
core component of case management services (Sacks et al. 2009).
2.5.10 Advocacy
Advocacy can provide older adults with an opportunity to express their concerns and experiences, and can support and enable people to make their own informed decisions (Anetzberger 2004, Kalaga et al. 2007). Empowerment is a central feature of advocacy. In practice, advocates can provide information, support and advice to older people about their rights and the range of services available to them (Kalaga et al. 2007). They may assist in setting up, facilitating or implementing plans for care or financial management (Podnieks 2008). Advocacy emphasises collaboration between older people and service providers and promotes the use of the least restrictive and intrusive interventions available (Wolfe 2003, Podnieks 2008).
Advocacy services may be provided by community-based organisations or are sometimes available through criminal justice systems, in the form of victim or witness assistance programmes (Dyer et al. 2005). For example, legal advocacy usually depends on an expert lawyer or police role focused on achieving a particular legal outcome (Cambridge and Parkes 2004b). Professional advocacy generally occurs within health or social care settings. However, this can create potential conflict between promoting the needs of the service user and the interests of the professional organisation within which the advocate works (Cambridge and Parkes 2004b). Podnieks (2008) argues that advocacy services should always be independent from formal service delivery systems. Citizen advocacy, in contrast, tends to involve unpaid advocates drawn from local communities who are independent from service agencies and often engage in longer term one-to-one relationships (Cambridge and Parkes 2004b). Peer advocacy may involve an advocate who has shared a similar experience. Finally, self-advocacy is driven by service users themselves and may involve direct action, personal empowerment and social justice.
Both formal and informal advocacy programmes are currently in operation in parts of Canada and the US (Podnieks 2008). Cripps (2001) describes the use of a rights-focused advocacy intervention to support older people to overcome situations of abuse in Australia. In this model elder abuse is seen as the denial of rights such as the right to make one’s own decisions and the right to live free from fear of violence. An advocate is seen as an
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 13
Chapter 2 Managing Elder Abuse in Practice
agent of change, assisting the older person to identify strengths in their existing and potential, formal and informal networks which may help to overcome abusive circumstances. In a retrospective analysis of 100 case records, the advocacy model was effective in enabling older people to stop the abuse in 50 percent of cases and in 34 percent of cases to allow clients to take some action towards stopping the abuse but not entirely preventing it.
The Mental Health Care and Treatment (Scotland) Act 2003 gives vulnerable adults in Scotland a legal right to advocacy services (Kalaga et al. 2007). However, the UK guidance document No Secrets called for a greater emphasis on the empowerment of vulnerable adults (Department of Health 2010).
A number of advocacy initiatives for older people have been established in Ireland in recent years, which may have a role in the prevention and management of elder abuse. The Cork Older People’s Advocacy Service was set up in 1999 to train and give on-going support and supervision to volunteer advocates to help empower older people who have difficulty in expressing their needs and concerns or accessing services (Comhairle 2003). The Finglas Volunteer Peer Advocacy Programme was began in North Dublin in 2005 with a weekly training course for volunteers taking place over 9 weeks. This programme supported by Age Action Ireland offers older people independent information and support to resolve a wide range of problems (Dooley 2007). Similarly in North Dublin, the Dementia Rights Advocacy Project, established in March 2006, advocates for anyone in the area who has or may have dementia, dealing with issues such as family conflict, access to entitlements and risk of abuse (usually financial) (Edmond 2007). The impact or effectiveness of these programmes has not been evaluated. Funded by the HSE, an Advocacy Programme for Older People in Residential Care was set up in 2007 in response to media exposure to poor care practices in a Dublin nursing home. This programme was developed under the auspices of the National Advocacy Programme Alliance (NAPA). Its main aim is to provide an independent advocacy group for older people living in residential care settings. The programme comprises three core strands: Independent volunteer advocacy programme; training programme; and information programme. An evaluation of this programme was recently undertaken and findings proposed that the programme adopts a new organisational structure and be
located outside the HSE and instead within an organisation for older people in the community and voluntary sector. Third Age now assumes responsibility for the programme.
2.5.11 Mediation, Conflict Resolution and Restorative Justice
Restorative Justice is another approach, closely linked to the advocacy model of intervention, which has recently been explored to address cases of elder abuse (Nerenberg 2008). This approach conceptualises abuse as a violation of people and relationships rather than a violation of the law (Groh 2005). The focus is therefore on resolving conflict, working towards restoring or rebuilding relationships and repairing any harm done (Groh 2005, Podnieks 2008). This may include mediation, family conferencing, and dispute resolution (Podnieks 2008). Mediation from an independent source is considered an effective method for dealing with family disputes (Kalaga et al. 2007). In England, for example, the Office of Public Guardians may act as a mediator in family disputes, especially where they may put an older person at risk of financial abuse (Kalaga et al. 2007).
The Restorative Justice Approaches to Elder Abuse Project in Kitchener, Ontario, Canada is one example of an innovative restorative justice intervention model (Groh 2005). Funded over four and a half years, this project was intended to increase the community’s ability to respond to elder abuse and decrease older adults’ fears about reporting abuse by providing a safe and fair environment to address the abuse without involving the criminal justice system. The project was a collaboration between seven community agencies including health, justice, social services, ethno-cultural and faith organisations. Referrals to the project could be made by anyone, after which a screening process was used to establish if it was safe and appropriate to use such a model in the circumstances. The restorative justice approach assigns a trained and skilled facilitator to both the victim and perpetrator of abuse. Individual counselling may be required for either or both parties before the facilitators eventually bring them together at a conference or circle where they attempt to reach consensus about how and why the abusive situation occurred and how to prevent future mistreatment. Anecdotal feedback has been positive regarding this intervention but full evaluation data was not identified (Groh 2005).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience14
Chapter 2 Managing Elder Abuse in Practice
One rationale for this collaborative approach may be supported on the basis that in many instances the perpetrator of abuse is also a caregiver or family member and may be the only source of emotional, physical and financial support for the older victim (Parra-Cardona et al. 2007). However, restorative justice approaches usually involve a time-consuming and costly process, and concerns have been raised over the potential to re-victimise the older people involved (Podnieks 2008).
2.5.12 Legal Intervention
Legal interventions in cases of elder abuse may make use of both the criminal and civil justice system (Kalaga et al. 2007). Civil law remedies can be used against actual or potential perpetrators of abuse. These may include protection or restraining orders as well as the appointment of powers of attorneys, public guardians or other surrogate decision-makers, where mental capacity is lacking. Further civil law actions include emergency removal orders or involuntary mental health placements as well as securing of assets or freezing of estates (Dyer et al. 2005, Kalaga et al. 2007). Criminal laws sanction the prosecution of individuals accused of a criminal offence (Kalaga et al. 2007).
One of the most striking changes in the field of elder abuse in the US in recent years has been the increasing numbers of prosecutions and charges filed in cases of abuse (Bonnie and Wallace 2003). This has been attributed to new legislative instruments and procedures as well as improved training for law enforcement officers and prosecutors in working with older people (Nerenberg 2006). However, legal interventions are still used in only a small minority (approximately 7 percent) of cases nationally (Dyer et al. 2005). Interventions tend to fall along a continuum with respect to safety, protection and freedom from voluntary to involuntary interventions (Nerenberg 2008). Legal interventions are considered to be amongst the most restrictive interventions available and decisions to prosecute require complex judgements balancing protection against punishment and deterrent considerations (Bonnie and Wallace 2003, Dyer et al. 2005). Legal interventions are often derived from domestic violence models but remain controversial in terms of their application to elder abuse where circumstances may be complicated by a dependency relationship between the perpetrator of abuse and the older victim (Wolfe 2003, Pillemer et al. 2007).
The efficacy of criminal and civil justice interventions is also open to debate. A study by Filinson (1993) found that the recurrence rate for abuse was 24 percent for those who received assistance, support and advocacy in the use of the criminal justice system, compared to just 17 percent in a control group. However, the incidence of recurrence of abuse was unknown in 43 percent of the control cases compared to just 12 percent of the intervention cases (Ploeg et al. 2009). Furthermore, Brownell and Wolden (2002) found no statistical differences in case solution between groups who received a legal services programme and those who received a social services programme. More cases of financial abuse were successfully resolved with the legal service programme but only a small number of cases were assessed (Ploeg et al. 2009).
Mental capacity legislation is particularly pertinent in protecting older people from abuse, especially in terms of financial exploitation. These laws are generally designed to safeguard individuals who lack the capacity to make decisions for themselves regarding either their personal welfare or financial affairs. Some jurisdictions have court investigators to consider proposed guardians or power of attorneys and investigate allegations of abuse and intervene where necessary (Nerenberg 2006). The Mental Capacity Act 2005 covering England and Wales introduced a new criminal offence of neglect that can be charged against anyone who has mistreated or wilfully neglected a person who lacks capacity. Traditionally, legal guardianship has involved the permanent removal of a person’s right to make their own decisions (Dyer et al. 2005). However, there is an increasing trend towards legislative reform to empower vulnerable adults to remain at the centre of decision-making as much as possible (Heath and Phair 2007).
2.5.13 Education, Information Provision and Advice
Qualitative research with older people who have been abused has found that they often do not know where to go for help, are unaware or unclear about their rights and entitlements, fear authorities in general and fear that services or agencies may not take them seriously (Pritchard 2000, Mowlam et al. 2007). Victims of elder abuse have identified a need for practical, accurate and reliable information on a range of issues including legal advice, income support, housing, family resources and
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 15
Chapter 2 Managing Elder Abuse in Practice
financial support (Schaffer 1999, Pritchard 2000, Lafferty et al. forthcoming). A randomised control trial carried out in New York found no significant differences in knowledge of elder abuse, awareness of services or reports of new incidents of abuse, between an intervention group who received public education via community meetings, posters in public areas and distribution of leaflets and a control group who received no education (Davis and Medina-Ariza 2001, Davis et al. 2001). However it is worth noting that only 6 percent of elderly residents at the targeted housing projects attended the educational settings (Ploeg et al. 2009).
2.5.14 Multi-Component Interventions
Many researchers and practitioners now advocate the need for different models of intervention on the basis that no one model is likely to work for all older people (Podnieks 2008). It is increasingly recognised that the distinct causal factors and myriad manifestations of elder abuse, alongside differences in geography, culture and community size and structure necessitate diverse approaches to managing cases of elder abuse (Fitzgerald 2006, Nerenberg 2008, Perel-Levin 2008, Podnieks 2008). For example, many interventions draw strongly on experiences and approaches from the fields of domestic violence and child abuse (Wolfe 2003). However, it is questionable how easily translated and how relevant these models are in the context of elder abuse (Podnieks 2008). Domestic violence approaches may not, for instance, be appropriate in circumstances of neglect (O’Loughlin and Duggan 1998). Specific interventions therefore need to be multi-layered and determined based on factors such as the type and duration of mistreatment, the willingness of the victim or abuser to accept help and the safety risk to the intervening professional (O’Loughlin and Duggan 1998, Anetzberger 2004, Kalaga et al. 2007). The service needs of both victim and perpetrator may span a broad spectrum and interventions and should therefore be context specific (Lachs and Pillemer 2004, Nerenberg 2006).
Elder abuse is frequently described as a complex phenomenon with multiple causes and a myriad of different outcomes (Nerenberg 2008). For example interventions that respond only to the older person and fail to address the needs of the family unit may result in the abuse recurring, particularly where functional dependence or a family history of abuse are factors (Pratt
et al. 1983). There is increasing support for the application of an ecological model for elder abuse. This model conceptualises abuse as the result of the complex interplay between a person’s individual characteristics, interpersonal relationships as well as the characteristics of the community in which they live and societal factors, such as policies and social norms (Perel-Levin 2008). According to such a model, a holistic, multi-component approach to intervention, addressing a range of causal factors and incorporating a variety of services, is more likely to be effective (Pillemer et al. 2007, Nerenberg 2008, Perel-Levin 2008).
2.6 Outcomes and Case ClosureStudies examining the impact of interventions employed in the management of elder abuse cases have used many different measures of outcome. These include recurrence of abuse and cessation or reduction in the level of abuse experienced by victims or perpetrated by abusers (Wilson and Micucci 2003, Ploeg et al. 2009). Some studies have also examined rates of relocation, institutionalisation or even death as an outcome. Research undertaken in Australia, for example, found that 65 percent of cases had resulted in institutionalisation three years after they were identified (Kurrle 1993). Similarly, a UK study found that the majority of victims whose abuse was reported and substantiated ended up being institutionalised or dying (Wilson 2004).
Another method of measuring outcomes in elder abuse intervention studies has been the proportion of cases classified in social service records as closed or resolved (Ploeg et al. 2009). Wolf and Pillemer (2000) found that a reduction in the severity and frequency of abuse was correlated with case resolution. Outcome measures in elder abuse cases are often difficult to ascertain and decision-making regarding case closure often relies on subjective judgements such as “safe and stable” or “a lot” resolved, or “about the same” (Wilson and Micucci 2003). According to social service workers in a study by Cambridge and Parkes (2004b), practitioners in adult protection cases must have the ability to manage sometimes “untidy endings”.
A study by Neale et al. (1997) explored the reasons given by professionals for closing a case documented in computerised records. One third of closures followed the death or relocation of the older person. A further 12.3
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience16
Chapter 2 Managing Elder Abuse in Practice
percent of cases were closed because the victim refused services and 14.2 percent because 12 months had elapsed without further incidents of abuse. In 34.5 percent of closed cases a professional had reassessed the case and deemed the individual to be at a low risk of further abuse. As these findings illustrate, it is not always possible to achieve a satisfactory outcome. In some cases complex relationships and ill-health hinder successful case resolution (Killick and Taylor 2009). In cases where a client refuses services, social workers may struggle with the awareness that in spite of the case being closed the abuse is likely to recur (Dayton 2005). Donovan and Regehr (2010) suggest that follow up or monitoring may be necessary in many cases. This difficulty will be discussed in more detail in section 2.8 in terms of the ethical dilemmas often faced by case workers in their
decision-making and their case management.
2.7 Collaboration, Multi-disciplinary and Interagency Working By far the most widely agreed aspect of best practice in the management of elder abuse is the development of multi-disciplinary teams and collaborative interagency working. While individual efforts are important, it is unlikely that any single profession, specialism or agency holds sufficient expertise and resources to deal with the diverse and complex circumstances in which elder abuse occurs (Baker and Heitkemper 2005, Nerenberg 2006, Penhale 2008). An integrated multi-agency approach involving inter-disciplinary teams is now considered imperative to successfully develop and implement effective multi-component and multi-phase strategies (Perel-Levin 2008). However, similar to other approaches little empirical evidence supports this assumption and few in-depth studies have been carried out to identify how interagency and multi-disciplinary collaborations function and impact on the problem of elder abuse (Teaster et al. 2005).
Multi-disciplinary teams (MDTs) are generally composed of a broad range of professionals and practitioners from various fields and different organisations. These teams often include the health and social care sector, volunteer services and faith communities, crime reduction or law enforcement agencies as well as legal and financial services. Many communities have established MDTs to provide a forum for professionals from diverse fields to
discuss difficult cases, learn what services, approaches and resources are available and share information and expertise (Nerenberg 2006). In a study of 31 MDTs in the US, Teaster et al. (2005) identified the two most frequently-cited functions of this approach: providing expert consultation to service providers and identifying service gaps and systems problems. The majority of teams also update members about services, programmes and legislation, advocate for change, plan and carry out training events and conduct coordinated investigations or care planning (Teaster et al. 2005).
Teaster et al. (2005) found that several multi-disciplinary teams focus on particularly problematic cases. Five teams in Teaster et al.’s (2005) study identified themselves as Financial Abuse Specialist Teams (FASTs), a model developed in Los Angeles in the early 1990s and since replicated elsewhere. However, there are wide variations among FASTs; for example, one FAST reported meeting every two weeks and including only representatives from public agencies. It emphasised rapid response to deter abuse and preserve assets. By contrast, another FAST which participated in the study reported meeting quarterly with over 50 members, including representatives from private and non-profit agencies (Teaster et al. 2005).
One of the strengths of a multi-disciplinary approach is acknowledgment of the limitations of individual disciplines while accepting different points of view (Perel-Levin 2008). Specialist input from different disciplines is likely to be valuable throughout the process to provide a more holistic approach to assessment and investigation, intervention, monitoring and reviewing elder abuse cases (Anetzberger et al. 2005, Penhale 2008). According to Lai (2008), a collaborative multi-disciplinary approach to combat elder abuse helps to enhance autonomy and choice for the older person and improves access to community services and supports. This approach facilitates a coordinated community response with professionals working together to assess overall needs in a holistic manner. In this way, the team may devise and implement more appropriate, comprehensive and integrated individual care plans (Wolfe 2003, Podnieks 2008). Multi-disciplinary teams may also have a role in identifying systemic problems or making recommendations to improve responses (Bonnie and Wallace 2003, Teaster et al. 2005, Nerenberg 2006). However, in order to be effective, MDTs require strong
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 17
Chapter 2 Managing Elder Abuse in Practice
leadership, awareness and understanding as well as clear communication skills in dealing with professionals from across a range of different disciplines (Penhale 2008). Teaster et al. (2005) identified the main challenge facing MDTs as a lack of participation and engagement by certain disciplines, most notably law enforcement, alongside others such as medical professionals, clergy, prosecutors, attorneys, financial institutions, pharmacists, regulatory agencies and mental health workers.
While the emphasis on multi-disciplinary and interagency collaboration is common to most existing national policies on elder abuse, the level of cooperation and the model for implementation varies between regions. Specialist multi-disciplinary teams are growing in popularity in the US, while in the UK the emphasis is on developing formal interagency arrangements between existing agencies. However, a UK study by Pritchard (2000) identified problems liaising with other agencies as a key issue for social service professionals engaged with interagency working. The police were one of the main targets for criticism and were considered by the social service professionals to be unhelpful in dealing with elder abuse referrals. Agencies working from within hospitals as well as general medical practitioners were also identified as lacking in awareness of the nature of elder abuse. Confidentiality was also a concern for cases dealt with by multiple practitioners and/or organizations (Pritchard 2000, Beaulieu and Leclerc 2006). By contrast, in their study Teaster et al. (2005) found that breaches in confidentiality were not identified as a challenge for the majority of MDTs surveyed. They argued that some MDTs have taken precautions to ensure confidentiality through the use of confidentiality agreements and the use of pseudonyms when discussing cases.
In Ireland interagency collaboration is similarly considered a key policy aim. A recent review of existing arrangements found that in some areas, the elder abuse service works in isolation from other services for older people (NCAOP 2009). The review identified a lack of access to other health and social care services and suggested that the role of senior case workers needs to be more fully integrated with other existing services for older people.
2.8 Decision-making in Elder Abuse CasesElder abuse often involves complex dynamics between the individual at the centre of the case and the perpetrator as well as environmental factors (O’Keeffe et al. 2007, Killick and Taylor 2009). Two systematic reviews reported insufficient evidence for the efficacy of any singular intervention relating to elder abuse, whether targeted at older victims, perpetrators, or health and social care professionals (Wilson and Micucci 2003, Ploeg et al. 2009). The absence of clear guidance may increase the burden on individual professionals to make crucial decisions in isolation of clear procedure or protocol. In undertaking these decisions, professionals must account for clinical, legal and ethical considerations in order to come to a satisfactory and responsible resolution for their client (Donovan and Regehr 2010). Factors that impact on decision-making relate to the individual affected, the specifics of the case, the practitioners themselves, as well as features of the agency, organisation and system within which they work.
The literature suggests that practitioners should take into account factors specific to the individual older person such as their level of risk and vulnerability. Furthermore, the gender, age and health status of the older person is considered (Killick and Taylor 2009, Donovan and Regehr 2010). However, Pratt et al. (1983) reported that the age of the victim did not significantly impact on what intervention professionals would select (Pratt et al. 1983).
Other factors related to the specific case include the type and severity of abuse. Different types of abuse occur in different circumstances and for different reasons and therefore may require different forms of intervention (Kurrle 1993, Killick and Taylor 2009). Daly and Jogerst (2005) conducted a Delphi survey of adult protection workers to identify indicators they used when making decisions. They found that although some indicators were common to all types of abuse, others were specific to the form of abuse. Pratt et al. (1983) found that the severity of abuse was significantly related to the interventions chosen by social service providers and physicians using hypothetical elder abuse vignettes. This study found that as abuse became more severe, referrals, particularly to the police and safe housing, significantly increased and personal interventions or recommendations for counselling decreased. However, Killick and Taylor (2009)
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience18
Chapter 2 Managing Elder Abuse in Practice
found that the frequency and severity of abuse received surprisingly little attention in the literature in a systematic review on decision-making in this area.
Research indicates that practitioner and agency factors are also significant in decision-making around elder abuse (Killick and Taylor 2009). These may include, for example, the attitudes and values of professionals working with elder abuse cases as well as their practical experience in this area. Professionals’ perceptions of older people have been identified as a factor in decision-making and therefore when planning interventions practitioners should consider how their own preconceptions and personal values may impact on their clinical judgement (Killick and Taylor 2009, Donovan and Regehr 2010). This may be one explanation for the substantial variance in decisions and reasoning provided by different participants as reported in a study by Wilson (2004). Bergeron (1999) also noted the importance of professionals’ emotions such as a fear and frustration, and ‘gut feeling’ when making decisions in elder abuse cases. However, Cambridge and Parkes (2004b) reported that participants identified impartiality as an important feature in effective decision-making and that “another pair of eyes” on the case was required to provide objectivity and capacity to distance oneself from emotions and issues, or conflicts of interest that may arise.
Killick and Taylor (2009) reported that adult protection workers’ opinions about the potential effectiveness of their intervention are also a factor in deciding to respond to alleged abuse. Attitudes towards interventions appear to vary. Jogerst et al. (2001) surveyed 1409 APS workers throughout the US and found that all but one felt that interventions had positive results “most or some of the time”. In contrast, participants in a small qualitative study reported by Wilson (2004) indicated that intervention often had a negative impact on the victim and as a result some practitioners worked towards management aims rather than ethical practice. Although it is likely that professionals develop these attitudes over time Pratt et al. (1983) found that professionals’ actual experience with abuse was not significantly related to the intervention recommended.
The availability of resources and the size of the practitioners’ caseload have also been highlighted as potential organisational or agency factors influencing decision making. Jogerst et al. (2001) suggest that a lack
of available resources might produce a more negative outcome and such negative outcomes may influence a professionals’ future decision making. Cambridge and Parkes (2004b) identified accountability and responsibility for decision-making within an organisation as having an impact on the decision-making of professionals. Furthermore, conflicting demands and considerations between professionals, teams and managers was also a factor for decision-making in this study (Cambridge and Parkes 2004b).
A flexible and collaborative approach, taking into account local organisational and resource circumstances, legal considerations, the wishes of the older person and an awareness of the advantages and risks of each intervention, is considered the key to realistic and effective decision-making in elder abuse cases (Bergeron 1999, Anetzberger et al. 1997, Cambridge and Parkes 2004b). In a study in one local authority in the UK, case conferences were seen as the ideal model of decision-making in adult protection (Cambridge and Parkes 2004b). Donovan and Regehr (2010) suggest that it is important that workers describe the options available to older clients so that they, together with the professional, can choose which interventions best suit their beliefs, culture, community and philosophy of life. A study by Pritchard (2000) supports this approach by finding significant differences in the needs identified by victims and those identified by professionals. Pritchard reports that victims were more specific and found it easier to describe and explain their precise needs, whereas workers gave more general responses often using general social work terms. Professionals gave little attention to the importance of leisure activities, interests and hobbies; concerns highlighted by victims of elder abuse (Pritchard 2000).
2.8.1 Ethical Dilemmas and Challenges
As the previous section illustrates, practitioners in the field of elder abuse are often faced with complex problems, ethical dilemmas and difficult decisions to make that challenge the limits of their professional knowledge and training (Donovan and Regehr 2010). Research indicates that professionals often struggle with some the complexities or ethical dilemmas in their cases (Cambridge and Parkes 2004b). Specific examples of these challenges include: victims not recognising behaviours as abusive, victims wanting to remain in an
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 19
Chapter 2 Managing Elder Abuse in Practice
abusive situation, lack of time and resources and issues around capacity. In a study aiming to explore the needs of victims of elder abuse, Pritchard (2000) found that in focus groups with staff, discussions quickly moved towards the difficulties and frustrations felt by staff in working with elder abuse rather than the needs of victims.
Professional codes of ethics such as the National Association of Social Workers Code of Ethics (2008) and the Canadian Association of Social Workers Code of Ethics (2005) specify values and principles which act as a guide for the professional conduct of practitioners (Woodcock 2011). However, ethical positions may vary in accordance with professions and services and this may be a concern particularly within multi-disciplinary teams and interagency work (Beaulieu and Leclerc 2006). Furthermore, these ethical codes typically stipulate that the social worker has a professional duty to uphold the best interests of the clients as a priority and to safeguard their rights. In practice, this stipulation may involve the social worker trying to balance a concern for individual rights with professionals’ views of the best interests of their clients (Donovan and Regehr 2010).
One area of concern related to this is the rights of older people to autonomy and confidentiality. Moves towards mandatory reporting and intervention in some jurisdictions have created controversy regarding the rights of older people to self-determination (Donovan and Regehr 2010). Social work is committed to the doctrine of self-determination, whereby the client has the right to wholly participate in the decisions made with respect to them (Regehr and Antle 1997). The American College of Physicians, for example, has also published clinical policy that supports a competent older person’s right to decide for him or herself to have a case reported. This can create a difficult ethical dilemma for doctors in jurisdictions where mandatory reporting exists (Geroff and Olshaker 2006).
The challenge in elder abuse work is to balance a duty to protect the safety of vulnerable older people with the client’s right to self-determination (Donovan and Regehr 2010). There is an ethical imperative to support self-determination which extends to an obligation to inform clients of their right to refuse or cease services. However, professionals entrusted with a duty to protect clients from harm may experience difficulty in reconciling this duty
with an older person’s right to refuse services and remain in an abusive situation (Donovan and Regehr 2010).
Research by Spencer (2005) examined 128 cases of elder abuse in Canada and found 58 percent of victims declined help from community services. In some instance practitioners may encounter the situation where a victim denies abuse due to the fear of repercussions from reporting (Anetzberger et al. 2005, Podnieks 2008). This may result in a conflict of values, whereby respecting someone’s autonomy may not be in their best interest (Beaulieu and Leclerc 2006). In a study of primary care physicians and mandatory reporting, Rodriguez et al. (2006) found that most physicians used a cost-benefit evaluation for each patient to determine the potential impact of mandatory reporting on the quality of life of the older person. Most were guided by the ethical principle of beneficence, to act in a manner which was believed to be in the best interests of the patient. In contrast, Pritchard (2000) found that the majority of workers wanted to ‘rescue’ victims from the abusive situation.
The National Association of Social Workers (NASW) code of ethics attempts to address this situation by stating ‘‘social workers may limit clients’ right to self-determination when, in the social workers’ professional judgment, clients’ actions or potential actions pose a serious, foreseeable, and imminent risk to themselves or others’’ (NASW 2008, p. 2). However, the critical issue in these circumstances is the capacity of the older person to fully understand the risks and consequences of their decision. Beaulieu and Leclerc (2006) found that practitioners tend to be comfortable ceasing intervention when the older person is autonomous and has the necessary cognitive capacity to make an informed choice. However, practitioners may feel uneasiness over closing a case when there are doubts about the older person’s capacity to make decisions and protect themselves from harm (Beaulieu and Leclerc 2006, Donovan and Regehr 2010). Appropriate skills for assessing and determining cognitive capacity or access to expert advice are therefore crucial in this field of work (Donovan and Regehr 2010).
Maintaining objectivity and impartiality is another ethical imperative which has been identified as a challenge for workers dealing with cases of elder abuse when faced with complex family and contextual factors (Killick and Taylor 2009). Donovan and Regehr (2010) point to the
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience20
Chapter 2 Managing Elder Abuse in Practice
importance of social workers being aware of both their own preconceptions and how their own personal values can influence clinical judgement. They must strive to refrain from impressing personal values or preferences on clients (CASW 2005). Social workers need to be sensitive to the cultural beliefs and values of the victim and their families as a failure to do so may lead to a poor response plan, inappropriate interventions and thus unsuccessful outcomes (Moon 2000, Podnieks 2008). Douglass (2005) emphasises the importance of sensitivity when introducing interventions.
Professionals in the area of elder abuse also report challenges in providing effective practice in the absence of appropriate resources (Bergeron 1999). Workers in the study by Pritchard (2000) described pressure to get things done quickly, which resulted in rushed investigations, and emphasis on administrative elements of the job rather than the client’s needs and client interaction. Even when particular needs have been identified there are often insufficient, inappropriate or inflexible resources to draw upon. There is often pressure on social workers to have up-to-date expertise on a wide range of issues from basic human rights to well-being, health, legal and financial matters (Schwiebert et al. 2000). Inadequate collaboration with other services, training in these areas and supervision can create a sense of isolation for individual workers. Financial abuse, in particular, has been highlighted by some professionals as an area where there is a need for specialist advice (Pritchard 2000).
These challenges and ethical dilemmas in casework may have significant consequences for professionals responsible for managing elder abuse cases. In focus groups with social service workers, Pritchard (2000) found predominantly negative attitudes towards this area of work, with many believing that little can be done in circumstances of elder abuse. Bergeron (1999) also described feelings of frustration and Wilson (2004) found that social workers sometimes use ‘avoidance’ as a professional strategy to deal with these challenges.
2.9 Training, Supervision and Line Management
The challenges facing professionals in resolving elder abuse cases highlights the necessity for more intensive and more regular inter-disciplinary training and discussion. This was particularly pertinent for coping with the ethical dimensions of the work and for improving
services and interventions for older people who have been abused (Pritchard 2000, Donovan and Regehr 2010). Research indicates that a lack of knowledge among social work professionals managing elder abuse cases results in lack of confidence in their ability to successfully resolve complex cases (Pritchard 2000). A number of core competencies for effective decision-making in adult protection emerged out of Cambridge and Parkes’ (2004b) training intervention. These included: an ability to stay calm in spite of serious or critical disclosures, good operational knowledge of policies and procedures to inform practice, effective and active listening skills, communication skills, ability to record information accurately, a good knowledge of relevant individuals and agencies to liaise with, an ability to assess risk and prioritise, and a capacity to manage confidentiality in disclosure and information management. Pritchard (2000) also identified particular training needs relating to: Definitions of abuse, signs and symptoms; investigation skills; interviewing skills; understanding why abuse happens; and understanding abusers. In some areas there is also an emphasis on training in broader areas of violence and abuse, such as domestic violence (Dayton 2005).
In addition to training, good supervision and support from line managers, peer support and collaboration with other professional colleagues as well as access to additional specialist advice have been identified by social service staff as basic needs (Cambridge and Parkes 2004b). Supervisors and other experts may be instrumental in the decision-making process of difficult elder abuse cases, offering both insight and support to practitioners (Bergeron 1999). However, while managers must have sufficient knowledge and experience in this area to be able to advise and adequately support the worker, research indicates that this is not always the case (Pritchard 2000).
2.10 Conclusions
A review of the literature on systems and strategies for responding to elder abuse points to a vast array of interventions but little guidance on what might be the most effective approach to helping older people who have been or are being abused. Legislation, policy and models of service provision vary widely internationally, and while it is possible to compare various elements of these approaches and to explore potential benefits and
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 21
Chapter 2 Managing Elder Abuse in Practice
limitations, research reporting the efficacy of the responses is limited and it is therefore difficult to determine the merits of certain approaches over others. Likewise the evidence base to support any specific process of intervening is sparse.
While increasing numbers of innovative interventions are being piloted and evaluated, most of the studies published thus far have methodological limitations. Efforts to assess the effectiveness of various projects and systems have also been hindered by a lack of common definitions, theoretical explanations and agreement on desired outcomes. Further research is therefore needed to build consensus on definitions and theories associated with elder abuse, to ensure interventions and services are beneficial and accessible to older people, and to establish consistent guidelines and international best practices for responding to elder abuse in the community.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience22
Chapter 3 Research Design
3.1 IntroductionThis chapter describes the research design used to realise the aim and objectives of this study. A qualitative design was adopted to ensure the prioritisation of the experiential knowledge of the participants and to facilitate the emergence of rich and nuanced data. Thematic analysis was undertaken which was grounded in the voices and perspectives of the research participants. This chapter provides an overview of study design, including the sampling procedures, methods of data collection and analysis and the ethical aspects of the study.
3.2 Aims and ObjectivesThe overall aim of this study was to explore the experience of managing cases of elder abuse from the perspective of senior case workers.
The objectives of the study were to:
1. Explore senior case workers’ experiences in managing cases of elder abuse.
2. Examine current practices adopted by the senior case workers.
3. Examine the challenges and dilemmas faced by senior case workers in managing cases of elder abuse and how these are overcome.
4. Identify good practice in the management of elder abuse cases, as perceived by the senior case workers.
5. Ascertain priorities for future service development and provision for elder abuse, as perceived by the senior case workers.
3.3 Overview of Study DesignA qualitative descriptive research design was adopted using one-to-one semi-structured interviews with the senior case workers for elder abuse. The design of the study reflects the objectives of the research and was informed by the relevant literature.
As the literature review outlined, there is limited research available on the management of elder abuse in practice. HSE statistics published annually offer some quantitative
data on the management of elder abuse through the HSE dedicated elder abuse service in Ireland (HSE 2011). This includes information on the number of cases referred to the service, general demographic information on older people who have been abused, general categories of intervention and limited information on case outcomes. However, these statistics do not provide details on the process by which investigations, assessments and interventions are determined. A qualitative approach permitted a fuller understanding of the experiences of senior case workers in managing cases of elder abuse in the community.
A qualitative design captures study participants’ individual experiences, perceptions, motivations and intentions (McGivern 2006, Bryman 2008). As the literature has highlighted, the management of elder abuse often involves difficult cases with many ethical challenges and complex dynamics involving the older person, the perpetrator, the practitioner and the service provider. Qualitative research may provide insight into the understandings and reasons that influence the way that people act, which facilitates an appreciation of how
decisions are made in cases of elder abuse.
3.4 Sampling and RecruitmentThere are currently approximately 30 senior case workers (SCWs) based in local health offices around Ireland and employed by the HSE to manage cases of elder abuse (HSE 2011). SCWs are responsible for investigating, assessing and managing cases of suspected elder abuse referred to the HSE. They therefore regularly encounter older people who have been victims of abuse. SCWs possess a wealth of knowledge and insight into the management of elder abuse cases and so are considered one of the key stakeholder groups in the provision of abuse services for older people in Ireland. As they are a prime source of information on current practices employed in addressing and responding to elder abuse, their knowledge and experiences are considered invaluable to this study which seeks to examine current practices and management of elder abuse cases in Ireland.
A purposive sample of the SCWs was recruited for this study. Each SCW was invited to participate in the study. Their participation was entirely voluntary. Purposive sampling techniques were used to recruit the participants
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 23
Chapter 3 Research Design
for this study. Although contact information for the SCWs is in the public domain, permission was sought from the HSE National Elder Abuse Steering Committee, which oversees elder abuse services, to approach the SCWs. The Steering Committee agreed to support this study and encourage SCWs to participate.
All SCWs currently in post received a letter and an information sheet about the study, inviting them to participate in the study. Follow-up telephone calls and emails were used to arrange interviews. Eighteen SCWs volunteered to participate in the study. At least four SCWs from each HSE area took part.
3.5 Data CollectionData were collected through face-to-face interviews. Interviews were arranged for a convenient time and place that best suited the participant, usually in their own office or a meeting room in their place of work. At the beginning of the interview the SCWs had an opportunity to ask questions and were then asked to sign a consent form. At the end of the interview they were asked to complete a short anonymous demographic sheet. Interviews lasted between approximately one hour and two hours 30 minutes. All interviews, apart from one, were audio recorded with participant permission. The recorded interviews were transcribed verbatim and any identifying information was removed. Field notes were recorded for any interviews where consent for digital recording was withheld.
3.5.1 Interview Guide
The interviews were semi-structured and conducted according to a prepared topic guide to ensure all areas of interest were addressed in each interview. Semi-structured interviews allowed the researcher to vary the sequence of the questions, probe for understanding and explore responses in more depth while maintaining the focus on the research objectives. The key areas included in the interview topic guide emerged from the study aims and objectives and the relevant literature in the field. The guide was finalised through an in-depth developmental process which involved input from an inter-disciplinary team of experts in the field of elder abuse. The interview guide covered a number of key areas, examining:
• Professional background and role of the SCWs
• Current practices used in assessing and managing elder abuse cases
• Dilemmas and challenges faced by the SCWs
• Collaboration and interagency working
• Supervision, line-management and training
• Future of elder abuse services in Ireland.
3.6 Data AnalysisThe interview data were subjected to a four phase analytic process resulting in a thematic structure which reflected the combined deductive and inductive analytic approach. Thematic analysis provided a flexible method for identifying, analysing and reporting patterns or themes within data (Braun and Clarke 2006).
Phase one of the analysis involved focused reading of the interview transcripts which allowed for a general overview of the participants’ accounts and facilitated the emergence of common trends, patterns and themes in the data. During this phase any identifiers were removed from the transcripts (e.g. names and places). Furthermore, the transcripts were imported into NVivo software to assist with data management and coding.
Phase two of the data analysis involved ‘open coding’ of the transcripts into NVivo nodes. ‘Open coding’ represented an inductive approach to data analysis whereby themes were identified from the raw data. During this phase, conceptual themes were tentatively named and identified with the aim of creating a descriptive and multi-dimensional thematic framework for analysis. Words, phrases and events that appeared to be similar were grouped into the same node. These nodes were subject to continual modification and re-conceptualisation throughout this phase of the analysis. An ‘audit-trail’ was created which facilitated the tracking of each data extract. This ensured the integrity of the data findings which were grounded in the voice of the participants and their experiential knowledge.
The next phase of the analysis involved ‘axial-coding’ or re-examination of the conceptual themes through collaborative in-depth team discussions. During these discussions the themes identified during the open coding
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience24
Chapter 3 Research Design
were compared, linked and combined into a thematic structure which allowed for the emergence of a conceptual model of the data. Finally, during the fourth phase of the analysis the conceptual model was translated into an agreed structure for the presentation of the themes and sub-themes. This resulted in a tightly woven account of the data findings representing the complexities and nuances of the data collected for the study.
3.7 Ethical ConsiderationsThis study involved interviews conducted with professionals, who were unlikely to experience any significant risk of harm as a consequence of participating. Accordingly, it was approved for exemption from a full ethical review by the Human Research Ethics Committee at University College Dublin.
The protocol for ethical approval required that all participants gave written informed consent prior to taking part in the interview. Prior to the interview, each participant received an information sheet and was offered an opportunity to ask questions and clarify any aspect of the study. Participants had the option of withdrawing from the study at any stage. Participants were assured that information provided for the purposes of the study would remain confidential, that digital and written files would be stored securely, coded and password protected and that any findings would be reported anonymously and in a way that ensured that individuals could not be recognised.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 25
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
4.1 IntroductionAnalysis of the interview transcripts gave rise to a number of major themes and subthemes. For the purpose of this report, the findings are presented in three distinct chapters, as follows:
• Elder abuse: a unique phenomenon
• Protecting older people
• Developing service capacity
Each chapter is presented with reference to themes and sub-themes, which are described in each respective chapter. The themes and sub-themes constitute a complex conceptual model, which emerged from the four-stage thematic analysis of the data, into a structured account of the participants’ experiential knowledge. This model is presented in Figure 4.1 and provides the overarching thematic structure for presenting the study findings.
4.1.1 Profile of the Participants1
A total of six male and twelve female senior case workers were interviewed for the study. The age range of the sample was 30 to 59 years. A majority of the participants had obtained a post-graduate qualification and had over ten years of social work experience since qualification. The majority of the participants had been working in the
role of senior case worker for more than two years and had over six years’ experience of working in the general area of abuse or violence. The participants were approximately evenly split between those who had between two and five years’ experience of working with older people and those with greater than ten years’ experience.
This chapter of the findings focuses upon the participants’ understanding of the phenomenon of elder abuse from their experience of managing cases. In their accounts the participants provided an insight into this phenomenon from the perspective of protective social services. They revealed the complexities, nuances and challenges of the phenomenon of elder abuse and they identified it as unique in terms of social work practice.
4.2 The Multifaceted Nature of Elder AbuseThis chapter is composed of a single major theme, ‘The multifaceted nature of elder abuse’. This theme encapsulated the participants’ accounts of the complex phenomenon of elder abuse and reflected the nuances and complexities of working for the protection of older people. An overview of the theme is presented in Figure 4.2.
Figure 4.1: The Thematic Structure for the Presentation of Findings
1 An ad hoc coding system was applied to the interview data whereby a number was randomly assigned to participants.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience26
This major theme of the data analysis was concerned with the unique nature of elder abuse and the experiential knowledge which was identified as necessary to meet the complex challenges presented by this work. In particular, the theme highlighted the degree of clinical judgement required by the participants in their handling of elder abuse cases as well as the necessity of recognising the influence of the life course on their clients’ interpretation of their situations and their willingness for change. As one participant noted there is often a legacy effect with elder abuse cases whereby the clients present with a history of long term abuse and patterns of familial and spousal behaviour that are entrenched over a long period of time:
Because often these cases, they are over 65 but often the abusive situations are there for a long, long time before this service ever gets involved (P18).
4.2.1 The Types of Elder Abuse
This sub-theme described the many sources of vulnerability for older people and the participants’ perspectives on the multi-dimensional nature of elder abuse. In their accounts they spoke about the fluid boundaries between the types of abuse which may be experienced by older people. One participant acknowledged that psychological abuse is common to most cases of elder abuse and coincides with the other forms of more direct abuse:
I suppose the referrals again are very broad ranging. Some specifically fit into the categories of elder abuse, nearly all of them fit into psychological abuse. Others or the next one would be financial and the next one would be self-neglect (P11).
During the interviews the participants described the many types of abuse that they encountered in their practice. The most commonly encountered forms of direct abuse were financial, neglect and physical abuse as well as self-neglect cases. In the cases of financial abuse that were described by the participants, the abuser was most often a relative who was a primary care provider for the older person. This added an extra layer of complexity to these cases and the participants spoke about the need to balance the older person’s dependency on the perpetrator for their care with the risk of abuse. As one participant noted, in these cases the client often makes a choice to tolerate a degree of loss of autonomy over their finances in order to safeguard their existing care relationships:
The older person willingly allows the person to manage their pension but maybe isn’t really given a lot of money for their own needs but at the same time is saying, ‘well if I actually didn’t have him or her managing my pension, I wouldn’t be able to pay the bills, I wouldn’t be able to pay the rent, I couldn’t get a taxi down to the hospital appointment. I kind of rely on them but I would love to get my hair cut every so often or what not’ (P10).
The management of the older person’s care emerged as an important aspect of the senior case workers’ description of their role. This was related to the types of abuse or vulnerabilities that the client experiences. Neglect was a common form of abuse which emerged from the data analysis and as a participant noted cases of neglect often involve a complex negotiation of care and a management of the expectation for care provision:
There is no onus or obligation on them to be providing care but if the relationship is such that there is an expectation maybe that you should have been providing care … If someone was out drinking every night and there was an expectation there, you know that they would be doing things … there would have been neglect, definitely neglect, no doubt about it (P12).
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Figure 4.2: The Multifaceted Nature of Elder Abuse
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 27
Another type of abuse that emerged from the interview analysis was physical abuse. This abuse occurred both between spouses as well as within families. The participants recognised that very often, in cases of spousal abuse, the domestic violence was an historical abuse that had occurred throughout the marriage. These cases were often particularly challenging for the participants and difficult to resolve as they involved complex negotiations of power and control over the lifetime of a marriage. These factors make this type of physical abuse difficult to manage under the remit of elder abuse rather than domestic violence:
Very few of them are domestic violence that happened in old age, they are actually historical domestic violence … I said, ‘when did your husband first abuse you?’ ‘On our honeymoon’ … so you are talking about 40 years of domestic violence. But very few of those people are actually going to, of their own volition, choose to leave that situation (P07).
Physical abuse also emerged from the participants’ accounts as occurring between an older person and their adult children or indeed grandchildren. Similar to other forms of abuse, many of the participants noted the difficulty they often encountered in managing these cases where the older person chose to continue to live in a situation of familial abuse for cultural and personal reasons. As one participant explained, there are often cultural reasons as well as a sense of familial loyalty and shame which keep the older person in situations of abuse:
Twenty-seven stitches, where her daughter and her granddaughter threw her down the stairs and they kicked her; they were incredibly abusive to her … went with her to several sheltered housing complexes and in the end she said, ‘… I appreciate your help and I’m sorry for wasting your time, but I’m going to go home’, and I said, ‘ok, could the same thing happen again?’, ‘oh god yes’, I said ‘and you’d prefer to go home to that’, ‘oh yes’, the shame of it, so that was very hard for me to let her make up her own mind, but I also know that it’s her choice (P02).
Psychological and emotional abuse were common to many of the cases of elder abuse that the participants described and they spoke about their role in providing
emotional support to their clients. This support focused on empowering the older person to make choices to end their abuse or to alleviate the impact of the abuse on them:
Well I suppose it’s back to social work basic principles about trying to believe the person, to make them feel supported, listened to and to try and understand the impact it’s having on them and try to see, explore ways, how are we going to reduce this impact on you, em so it’s about that approach really (P01).
While self-neglect cases are not elder abuse they fall under the remit of the case workers in their role in protecting older people. A common outline of a typical self-neglect case was found across the participants’ accounts:
The person is resistant to any support … and it is not until something has happened or something is about to happen that you get involved or they give permission and then you are involved a lot in restoration or refurbishment of a house, and then they withdraw again. And you might find the same client comes up two years later when there is an issue that they have fallen again or a member of the public says, ‘you are not doing anything to support this person’ (P11).
This sub-theme described the many types of abuse that the participants encountered during their practice and it highlighted the fluid nature of elder abuse as it traverses the boundaries of its multiple dimensions. Some of the complex aspects of elder abuse, which emerged from this sub-theme, included the necessity to manage an older person’s caring relationships as well as the legacy effects of historical abuse which may have been endured over the lifetime of a marriage. Furthermore, the theme highlighted the necessity for the participants to empower older people to make decisions to end their abuse. This work coincides with respect for the cultural and social forces which may influence an older person’s decisions as well as the right of an older person to self-determination.
4.2.2 Balancing Self-determination and Risk
This sub-theme was concerned with the participants’ experiences of balancing the self-determination of their client with their assessment of the client’s exposure to
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience28
risk or vulnerabilities. The participants’ accounts of their cases, particularly those concerned with self-neglect, emphasised the guiding principle of social work practice in the area of adult services. This principle placed the autonomy of the client at the centre of practice and recognised the right to self-determination. This concern for client self-determination was at the core of the particularity of elder abuse described by the participants. They recognised the importance of respecting a client’s right to choose their own living situations and they described the difficulties they often encountered in balancing this right with their assessments of a client’s risk:
And this is a part of my work that can be difficult at times, that while we might feel that something is good for the person, in the best interests of the person … they obviously have rights to make a decision and it’s rights versus risks (P04).
Another participant spoke about providing support to the older person and thereby facilitating the client to make choices and decisions concerning their own lives:
So you can only work with people for as far as they want to work and then you’ve got to respect that, and I always say to people whatever decision you make I will respect, right, no matter what, I might not agree with you but I will support you in whatever you decide (P01).
A common element of handling elder abuse cases, which emerged from the findings, was the role of the participant in managing the relationship of their client with the perpetrator of abuse. This was a feature of the participants’ accounts of elder abuse which distinguishes it from other cases of abuse or protection that they may have encountered in their prior professional experience. One participant observed that the necessity of respecting the relationship between the perpetrator and the victim of elder abuse can often mean facilitating a client’s desire to maintain that relationship, despite the risk to their safety or autonomy which may be incurred as a result:
She has been a mother to her children for 40 or 50 years, it may be incredibly hard, even though they may be useless good for nothings, for her to accept that and to do something about it. And she may not want to. And I think at some stage you have to respect as long as she is still able to think straight
and she is making an informed decision, as long as you know you have given her options (P07).
Similarly, another participant noted the need for senior case workers to respect the boundary between their desire to address their perception of the degree of risk to their client and the rights and autonomy of the older person. In particular, a participant commented upon the importance of respecting the capabilities of an individual to manage difficult familial situations; capabilities which have developed over a lifetime:
A lot of older people have been managing very difficult situations all of their lives and while we are all sitting around going, ‘oh gosh this is awful’, this has actually been their life, managing a young person with a mental health problem or a husband who has an alcohol problem and is violent (P10).
The difficulty often encountered by the participants in balancing self-determination with risk was related to a further debate concerned with issues of capacity. The participants explained that their management of cases which required a balance between self-determination and risk was guided and informed by the capacity of their clients. In this way, an individual who is deemed to have full capacity has the right to autonomy in relation to decision-making concerning their situations of abuse. The participants conditioned their responses to the abuse cases according to the direction of their clients, who were considered to have capacity. This respect for self-determination occurred despite concerns over the level of risk or vulnerability to the older person:
And I think those cases are the worst ones to deal with where you know people are at risk, you know they are very vulnerable, you know they are needing help but they are refusing help and because they have capacity we can’t do anything else. They are the tough ones (P13).
Access to capacity assessment emerged from the participants’ accounts as a particular challenge for them related to the particular phenomenon of elder abuse and the necessity to balance risk and client self-determination. A guiding principle of social work practice in the protection of older people, described by the participants, was the importance of client direction informing the case management and outcomes. This practice was contingent upon the assumption of client
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 29
capacity and the participants spoke about the complexities involved in assessing an older person’s capacity to make decisions about their lives. This issue was central to the phenomenon of elder abuse described by the participants. As one participant acknowledged, determining capacity and its relationship to decision-making was neither straight forward nor transparent:
I suppose I’m running on the assumption that everybody has got capacity until such time as they’ve been deemed as not having capacity. I think the method of assessment of someone having capacity is very antiquated … ‘oh they’ve only got 15 out of 30’. That means nothing to me … because if a person’s able to indicate that they want to live at home that means they want to live at home ... even if they don’t know what day of the week it is, I don’t care (P01).
A further issue related to capacity, which was raised by the participants, was their reliance upon other services for capacity assessments and the difficulties they encountered in accessing these services. This barrier to capacity assessment had the result that the participants were often obliged to follow client direction despite on-going concerns regarding their client’s capacity to give that direction:
And mental health will not assess someone unless they are referred by the GP … So then you are caught in a catch 22 situation, you know someone is self-neglecting, you know that their capacity mightn’t be great, you know their mental health mightn’t be great, but you have to presume that they have full capacity (P11).
As noted by another participant, the barrier to capacity assessment resulted in a dilemma whereby they had to reconcile best social work practice with their concerns for their clients’ safety:
They only do assessments for capacity if a solicitor requests it … So there’s a huge dilemma around does a person have capacity or not … I suppose for ourselves we have to assume capacity until proven otherwise but how do we get it proven otherwise if we’re not able to get capacity assessments (P03).
This sub-theme addressed the challenges experienced by the participants in balancing their perception of a client’s
risk or vulnerability with their right to self-determination and autonomy. This concern for client autonomy and self-determination emerged from the findings as a distinguishing feature of elder abuse and a contributing factor to the complexity of dealing with this phenomenon. The participants’ management of these challenges was contingent upon their understanding and assessment of a client’s capacity to make decisions and determine their living situations. The reliance of the participants upon other services for capacity assessment was identified in this sub-theme as a challenge to the participants’ effective case management.
4.2.3 Ethical Concerns
This sub-theme described the participants’ reflections upon the ethical dimensions of their work. The participants spoke about experiencing ethical dilemmas and they considered the influence of morals and values on their practice. A concern for the ethics of choice and how this related to the participants’ understanding of elder abuse emerged from their accounts of managing the self-determination and capacity of their clients:
Self-neglect is a choice but what is that choice based on? I find that really difficult and if you neglect yourself that much, is it because you have no self-value and self-worth? Is it because you’ve been beaten into that place? Well then it’s no longer self-neglect, it’s abuse. So I have huge dilemmas around that (P02).
Another participant reflected upon the difficulty in resolving the ethical dilemma of choice which often involved a consideration of morals and resulted in unanswered challenging questions:
A married couple and one only has capacity and carers think they shouldn’t have a sexual relationship anymore. You know, who can make that decision? … if you have been married for 50 years, you know, because you no longer have capacity do you no longer want a relationship with your husband? I don’t know what the answer to that one is (P13).
The ethical concerns raised by the participants in their consideration of the nature of elder abuse had implications for their decision-making and judgement as to their practice. One participant related an experience
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience30
of dealing with a case of self-neglect and the dilemma this raised for the participant in terms of procedure:
I certainly would have liked to offer him more in the house, some way of giving him a bit of comfort. But then again you would have been encouraging him to stay there … You have the dilemma then of supporting somebody in an unsafe house (P12).
Similarly, another participant spoke about the difficulty of balancing issues of care with risk of abuse and vulnerability under the remit of protecting an older person:
And I can hear the ethical question for [public health nurses], like they genuinely see the older person is being cared for but there is financial abuse and if I go in and stop that abuse it will mean that person leaving the house. But I can’t condone abuse under any circumstance (P15).
In their discussion of their role in protecting older people the participants acknowledged the necessity for them to decide the best interests of their clients who have diminished capacity. This necessity raised ethical concerns for the participants in relation to their power to make decisions which determine life outcomes for an individual:
I just realised the powerlessness of certain people when they become older and they have dementia; that all your decisions are sort of made for you (P18).
The ethical concerns experienced by the participants when they attempted to represent the best interest of their clients were discussed in relation to their advocacy role. The participants spoke about their inability to provide independent advocacy while also being employed within a particular organisation; subject to particular policies and procedures. Furthermore, the participants described the challenge of advocating for the best interests of their client, as assessed by the relevant agencies involved in the case, while at the same time advocating for the sometimes conflicting wishes of their client:
And while I have been an advocate in allowing her to object, which is her right to do … I feel at this stage now I wouldn’t be advocating on her behalf to continue … I am still working in her best interest but I am no longer going to support her on getting
more medical reports … It is in her best interest to apply for the ward of court, I genuinely feel that, but I kind of wanted to be an advocate and support her as well (P15).
This sub-theme highlighted the particular ethical challenges experienced by the participants in their role managing cases of elder abuse. These challenges were directly related to the participants’ understanding of the unique phenomenon of elder abuse and their desire to deliver a client-directed protective intervention. Ethical challenges were one of the many facets of their practice. This facet was associated with the necessity to respect the individual choices, to determine capacity and to represent the best interests of their clients.
4.2.4 Family Conflict
This sub-theme was concerned with the participants’ descriptions of their frequent encounters with situations of family conflict. These descriptions generated a discussion of their remit as senior case workers for the protection of older people and their understanding of elder abuse. One participant, for example, reflected upon being deliberately drawn into conflict situations and thus being manipulated by the family:
There are so many families where there is so much conflict and sometimes they use the services to try and resolve the conflict without them getting involved … We can’t solve 20 years of sibling rivalry (P13).
While the participants recognised that resolving historical family abuse was not within their remit as senior case workers for the protection of older people, it was often difficult for the participants to make that distinction in their practice. As one participant explained, the level of distress, caused to the older person by situations of conflict, often presents as abuse. Furthermore, the nature of family conflict, described in the accounts, was such that it tended to have an historical legacy and be grounded in entrenched patterns of behaviour which made these situations extremely complex and difficult to resolve:
The man wasn’t being neglected, the abuse was more that he was being used as a pawn in people’s games … and a lot of family disputes are like that and when you … get the referral in the first place you don’t know that and in fact sometimes you are
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 31
embroiled with cases for years and it is only suddenly then that you realise actually exactly what is going on in a situation (P07).
Similarly, another participant noted the complexity of family dispute which may result in the increased vulnerability of the older person. This made it very difficult for the participant to distinguish between situations of abuse and family conflict:
So there can be a lot of family disharmony, a lot of issues over money, over land, over who is providing the care, how they are providing the care … and sometimes you get involved in cases that you wonder, are they elder abuse or are they just long standing issues of abuse that have gone on in this family for generations? (P11).
As the participants are concerned with the establishment and realisation of a care plan for the older person they often have to take on the role of family mediator in an attempt to end situations of dispute. This added a further element to the phenomenon of managing elder abuse cases and the participants remarked on the experience, skills and knowledge that were necessary for them to effectively realise their objectives in relation to the older person:
… sometimes these rows are so engrained that you can see that the brother or sister is so fixed in their position that it would be very difficult to shift them or move them or see the other person’s perspective. So you have to be a bit wise about which family meetings are going to work and which ones are not going to yield positive results (P18).
The recognition of the necessity of managing family relationships and negotiating family dynamics emerged from the findings presented in this sub-theme. While the participants acknowledged that this was a core aspect of their practice they emphasised the importance of focussing upon the needs and wishes of their clients. As a result, the participants spoke about developing a relationship with the older person to gain their trust and to build a rapport. This was central to their effective protection of older people and it added another layer of complexity to the phenomenon of elder abuse.
4.2.5 Establishing Trust and Rapport
This sub-theme presented the participants’ reflections upon the work that they do to establish a relationship and a rapport with the older person. They explained that this was a necessity of the phenomenon of elder abuse which was often characterised by the social isolation of the client. As one participant explained, the importance of rapport building distinguished elder abuse from other areas of social protection:
It’s much easier in child protection in a sense that you’ve got an hour, and it’s an hour of assessment, but with older people they need to know your history, and they need to put you into a place, and it takes much longer, much slower, and they have, you know, a visitor, for a lot of the older people that are isolated (P02).
Similarly, another participant commented upon the necessity of establishing trust with older people through the development of a good relationship and rapport:
Build that relationship with them and establish that rapport with them that they are going to tell you things that they maybe never told anybody in their life … how much worse can it get than trying to tell a stranger about your son or your daughter abusing you (P09).
The participants’ accounts emphasised time cost that was incurred as a result of the relationship building with the client and this had implications for case management. This was necessitated however by the unique nature of elder abuse and the participants recognised the importance of this aspect of their work.
4.3 SummaryThis chapter reported a single major theme; ‘The multifaceted nature of elder abuse’. This major theme was composed of five sub-themes which explored the unique phenomenon of elder abuse from the perspective of the participants and highlighted its complex and multifaceted nature. In particular, the causes, characteristics and outcomes of elder abuse were understood to be multi-dimensional. This complexity was manifested in the interlocking forms of abuse and the fluid boundaries between the types of abuse. This complexity was reported to make elder abuse difficult to recognise, detect and manage. In particular, the challenge
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience32
Chapter 4 Findings Part 1: Elder Abuse, A Unique Phenomenon
of reconciling the autonomy and self-determination of their clients with issues of capacity, risk and vulnerability emerged from the accounts as a facet of elder abuse which presented ethical dilemmas for the participants. Furthermore, the necessity of handling cases of family conflict and of establishing trust and rapport with a client were explored from the perspective of the participants. A key finding, emerging from this chapter, was the participants’ recognition of the particularities of elder abuse cases which present their own unique challenges, issues and dilemmas to social work practice. These particularities distinguished elder abuse from other areas of social protection that the participants may have encountered in their prior professional experience. The management of this unique phenomenon was understood by the participants to be highly demanding in terms of assessing capacity, ethical judgements and inter-personal skills.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 33
Chapter 5 Findings Part 2: Protecting Older People
5.1 IntroductionThis chapter of the data findings is concerned with the participants’ perspectives on the experiences of managing cases of elder abuse. The chapter is composed of the following three major themes:
• Case management and interventions
• Interagency working
• Experiencing the role
These themes highlighted the various aspects of the participants’ role in protecting older people and their reflection upon their everyday practice. Furthermore, the themes emphasised the skills required to manage cases of elder abuse. An overview of the themes is presented in Figure 5.1
5.2 Case Management and InterventionsCase management and interventions emerged as a major theme of the research findings and it was concerned with the participants’ accounts of their case management from the initial referral through to their final evaluation of a case outcome. The participants reported that they
typically deal with an average of 43 cases at any one time. One participant described the standard procedure for the management of a case of elder abuse as involving three stages: an evaluation of the presenting concerns through information gathering and assessment, ascertaining the wishes of the client, family members and relevant professionals, and finally the establishment of a care plan and interventions. This theme of ‘Case management and interventions’ was composed of the following sub-themes: responding to referrals, establishing care plans, case conferences and family meetings, counselling and support, maintaining client relationships, balancing rapport with risk of dependency and evaluating case outcomes.
5.2.1 Responding to Referrals
This sub-theme described the reported first stage of a case of elder abuse; responding to a referral. The participants observed that a referral was typically received from the relevant agencies, such as public health nurses, as well as family members or, in some cases, the general public. The participants explained that a written referral was the standard process for receiving a notice to investigate a suspected case of abuse. However, as one participant acknowledged in a lot of cases the referrer
Figure 5.1: Protecting Older People
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience34
Chapter 5 Findings Part 2: Protecting Older People
will make initial contact via a phone call and this will be followed by the written referral if appropriate:
Most referrals would probably be the person ringing up first of all to say, ‘can I have a chat about this case, I’m not sure if it’s appropriate or not?’, usually it would be appropriate, but we talk about it (P02).
Following the receipt of a referral, the participants spoke about the next stage of the case as involving gathering relevant information from the stakeholders and agencies in contact with the older person at the centre of the referral. This information was obtained from the referral process as well as through telephone requests for background information. The participants spoke about the importance of this information gathering to their initial management of a suspected case of abuse. In particular, GPs, Gardaí and the initial referrer were frequently mentioned by the participants as being key information sources at this stage of the case management. According to the participants’ accounts, this information gathering was undertaken prior to the initial contact with the older person at the centre of the referral. The participants explained that the information gathered informed how they would approach a case and make that initial contact with the older person. This practice of putting the particular circumstances and concerns of the older person at the centre of their case management ensured that the participants delivered a client directed intervention. One participant, for example, spoke about the benefit of ensuring, where possible, that the older person was aware that a referral had been made and they were happy to speak to a senior case worker about their situation:
So what I have learned … is asking the referrer to go back, either themselves or somebody the older person trusts, to have that conversation with the older person about what their concerns are and then to establish if the older person is happy to speak to a social worker (P10).
Similarly, another participant described the client-centred approach to social work case management and the importance of following the direction and wishes of the older person. This participant noted the practice of encouraging the older person to find a solution and empowering them to overcome their situation themselves:
You try and work at their own pace and their own comfort, you don’t highlight the problem but you let them try and tell you if there is a problem ... so you have to measure it up … is there a criminal action being carried out? … Is the person’s capacity an issue? … You try to find out what solutions they might offer to improve the situation (P12).
The participants’ accounts revealed the necessity of ensuring that the appropriate and necessary information was obtained in the early stages of the case management and intervention. They spoke about the importance of supporting the client to lead the direction of the intervention and empower them to take control of their situation. These aspects of case management, described by the participants, were noted as providing the foundation for the establishment and implementation of a suitable and effective protection plan.
5.2.2 Establishing Protection and Care Plans
This sub-theme was concerned with the accounts of establishing a protection plan. A protection plan emerged from the analysis of the participants’ accounts as being the primary aim in any case intervention. As one participant explained, these accounts take into account the particular circumstances and wishes of the older person:
You gather as much information as you possibly can. You identify the risks to the older person, you identify the wishes of the older person and based on the risks and the wishes of the older person you formulate a management or a protection plan. So that is the basic sort of intervention process that happens (P09).
One of the predominant features of the protection plans, outlined by the participants, was the management of the care situation of the older person. The participants spoke about interagency working and service referral as the mechanism by which they established a plan for the older person. In particular, the participants frequently mentioned employing the services of home help, public health nurses, respite facilities, day care facilities as well as private care options. As one participant noted, care interventions required a team-based approach to the delivery of services:
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 35
Chapter 5 Findings Part 2: Protecting Older People
So you are looking at continued respite, you are looking at an increase in home help, an increase in private care, attendance at the day centre. You are looking at all the options and again you are team working in that approach (P11).
The participants spoke about the importance of care interventions in protecting older people from abuse and in managing cases of suspected abuse. According to their accounts, the majority of their case interventions involved some form of care support. As one participant acknowledged, implementing care support for a participant increased their interpersonal contact either with home care professionals and/or with day care facilities. The participant pointed out that increased interpersonal contact was associated with increased protection through minimising the older person’s risk of social isolation:
The research would show that abuse thrives when a person is isolated so if you increase the older person’s contacts and get them involved in as many things as they want to become involved in, it’s good (P10).
Connecting an older person with a day care facility emerged from the analysis of the participants’ accounts as providing a common type of case intervention. The participants spoke about the day care facilities as not only addressing the needs of an older person in terms of nutrition and, in some cases, personal care, but also providing them with an outlet for social community-based connectivity. One participant, for example, spoke about the role of day care facilities in providing respite care for an older person; day care is often the most common type of intervention:
[day care centre] often gives the perpetrator space which is sometimes what is needed, it is a safe environment. And it also gives an outlet to the victim as well. So generally if it is available and it can be used, it would be the one that I would go for often, more so than anything else (P06).
A further aspect of care interventions which was reported to be connected to the protection of older people was the use of care plans as a means of monitoring a case following direct intervention. The participants spoke about the role of care providers and services in communicating with the participants; keeping them
informed as to the on-going situation of the older person. As one participant explained, care plans are a useful way for the participants to evaluate the efficacy of their intervention and to provide a connection between the client and the participant:
For me that is a way of knowing whether [an intervention] is working or not. Is this woman coping? Is she refusing services? … so the care plan is the safety net … It is a way of monitoring it as well. The monitoring is in there plus the feedback, there is capacity for feedback (P15).
The findings, presented in this sub-theme, emphasised the importance of establishing care plans and interventions for the protection of an older person. These care plans were used by the participants to increase the interpersonal contact of their client and thereby reduce social isolation; identified as a risk factor for elder abuse. Furthermore, respite services were employed as part of a protection plan not only to provide for the needs of their client but also to reduce carer burden. In this way, care interventions were also employed as a preventative measure by the participants. The participants’ discussion of the role of care interventions for their protection plans emphasised the interagency aspect of the participants’ case management and their reliance upon services for the on-going monitoring and prevention of abuse.
5.2.3 Case Conferences and Family Meetings
This sub-theme focussed upon the participants’ accounts of working with the family of an older person when devising a protection plan and intervening in situations of suspected or confirmed abuse. This family engagement involved both informal family meetings as well as more formal case conferences which included all the professionals involved in a case as well as family members. One participant, for example, spoke about the importance of family engagement in a case where possible:
I try and get family involvement wherever I can … in the main, families are often very supportive. And families can get a lot done within families that you can’t do as a professional … so family involvement would also be core as well (P10).
The participants acknowledged that case conferences, involving the older person, their family and professionals,
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience36
Chapter 5 Findings Part 2: Protecting Older People
are likely to be necessary in more complex cases or in situations which have reached a crises point. The participants pointed out the usefulness of case conferences in terms of creating a team-based approach and in garnering the support of the relevant agencies involved in a case. In particular, the participants spoke about sharing out the responsibility of a case through inter-disciplinary agreement as to the intervention and approach. One participant, for example, argued that case conferences were important in terms of governance and interagency working:
Case conferences are essential really especially in terms of governance … if something has gone wrong I think it is very important that you have given people the opportunity to voice their concerns and voice their opinions as to what may work or whatever (P12).
In the participants’ accounts of setting up case conferences, they spoke about the usefulness of having a professionals’ meeting prior to the conference in order to ensure the efficacy of the conference. The participants pointed out that case conferences are more effective when there is a consensus among the professionals as to a course of action which can then be discussed with the older person and their families. As one participant noted, a case conference which is badly managed can cause distress to a family particularly if there is no agreed plan of action among the relevant professionals:
I think going into a case conference if we don’t know what we’re saying it’s very upsetting for family members … let’s have a professionals’ meeting and then let’s have a case conference because at least then we have an agenda, we know what we’re saying and we know what we’re going to do (P02).
The findings, presented in this sub-theme, identified family engagement as a core aspect of the participants’ role in protecting an older person. Interaction with families occurred primarily through the medium of family meetings or case conferences, which included professionals. The participants noted that good interagency communication was a key ingredient of successful case conferences and they pointed out the value of having an agreed strategy among the professionals which may be presented to the family. This sub-theme emphasised the importance of communication and engagement with family members
for the realisation of an effective care or protective intervention.
5.2.4 Counselling and Support
This sub-theme was concerned with the participants’ descriptions of the work they do with an older person in terms of ascertaining their wishes and empowering them to control their situation. While engagement with professionals and with family members were noted as key aspects of their case management, the participants spoke about the older person at the centre of a case as their primary focus. They spoke about their case management practice as being client-centred and they depicted themselves as following the direction, wishes and pace of the older person. Furthermore, in situations where the client’s capacity was impaired, the participants explained that their role was to establish the best interests of the older person and to advocate on their behalf. As one participant acknowledged, this type of work involved one-to-one conversation with the client in order to establish the direction that the older person wanted to take:
So my intervention is around talking with the older person, talking to them or explaining options to them, offering them support and following up on what they need me to do (P14).
Similarly, another participant described this counselling aspect of the role and spoke about the time that is invested in establishing this relationship:
And, I worked with her for several months, talking roundabout it … and so we managed to get her in a position where she turned around to say ‘I’m not giving you any more money, you need to manage your own affairs’ … and she is now feeling in a much more better place … able to feel comfortable saying no, without feeling guilty (P01).
The participants’ accounts contained references to different forms of direct therapeutic intervention which included: motivational interviewing, task-centred work, brief solutions therapy and crises intervention. One participant described these forms of intervention as ‘client-centred approach therapy’ and commented upon the necessary counselling skills obtained in social work training:
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 37
Chapter 5 Findings Part 2: Protecting Older People
I suppose there is crisis intervention, there is client-focused, there is brief solution … I would look back on kind of my training … so very much client-centred approach therapy would be what I would like (P04).
While the participants recognised the importance of establishing a rapport with their clients which would facilitate their role in supporting the older person, they also spoke about the necessity of balancing this rapport with a risk of dependency. One participant, for example, described a case where an older person understood her relationship with the participant to be that of friendship rather than professional. This was a challenge for the participant in terms of managing the clients social and care relationships:
Up until she went into hospital she refused to let anybody inside the door except myself. She didn’t think of me as a social worker, she thought of me as her friend … never clicked with her that I am actually employed to come and see [her] (P07).
Another participant spoke about this relationship with clients as being a result of the unique phenomenon of elder abuse which may concern vulnerable adults who are often socially isolated. This participant spoke about taking precautions to minimise any risk of the client becoming dependent upon the participant for social contact:
You’re welcome into people’s houses, they love to see you … and I also try not to make my visits to older people very long because I don’t want them to depend upon me for their community with society or their community (P01).
This sub-theme described the work of the participants in establishing rapport and trust with their clients using counselling techniques which empowered the older person to make changes. This work was reported to involve direct one-to-one conversation with the older person and the provision of support. The participants recognised the need to increase their clients’ social engagement and autonomy in their relationships as a means of reducing their vulnerability to isolation and dependency. The sub-theme emphasised the client direction of the service for the protection of older people and it reported the need for the participants to empower their clients to direct their protective intervention.
5.2.5 Maintaining Client Relationships
Another sub-theme, which emerged from the accounts of case management and interventions, concerned the role of the participant in safeguarding the existing relationships of their clients with family members and the wider community. The participants spoke about working with families and carers to ensure that they contributed to the case management and protection plan. They reported that this desire to maintain client relationships meant that they were sometimes safeguarding relationships that were concerning in terms of the care or treatment of the older person. However, the participants explained they continued to protect those relationships by working with the family to address causes for concern and to implement a protection plan. In this way, the participants minimised the risk of the older persons’ isolation. As one participant reported, the desire to protect family relationships, despite concerns over the dynamics of those relationships, was driven by an awareness of the older person’s potential dependency upon these relations for their care and social contact:
Usually you would try and include the family if at all possible … even if there was a concern over them … we would be conscious not to damage some of those relationships because … if the person becomes ill or dependent and that is [the] person they are going to go back to for support. So we have to tread carefully (P12).
Similarly, another participant described a case which involved managing an on-going relationship between a client and a perpetrator of financial abuse in order to safeguard the caring dynamics of the relationship:
I know from seeing the older man in respite, that he actually is the appropriate weight, he is in great physical condition, always well dressed, quite content in himself … But I suspect that his son is probably siphoning off his pension for his own needs ... what I am trying to do there is to keep the links with the older person and the probable perpetrator of abuse and try and keep the older person linked to services, try and keep a monitor on the situation to make sure the older person is being looked after (P10).
The participants spoke about keeping the older person linked into services as being an important element of
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience38
Chapter 5 Findings Part 2: Protecting Older People
their care plans and a mechanism for monitoring the clients’ on-going relationships. Furthermore, the participants revealed that very often their protection plans for an older person involved interventions to assist their client’s primary carer and thereby reduce stress or carer burden. As one participant noted, interventions which relieve the stress of carers can address the risk of abuse of the older person at the centre of a case:
And there is only so much a carer can cope with. So quite often the intervention is about relieving the carer and opening doors for them and options (P09).
While relieving carer burden or stress was a common feature in the participants’ accounts of their case management, they reported that they often work with perpetrators of abuse in terms of service referrals. They spoke about referring perpetrators to addiction services, counselling and social welfare or housing services. As one participant explained, this work with perpetrators was connected to decreasing the risk of abuse and was often a feature of a protection plan for an older person:
So a lot of my work I would actually work indirectly with the person causing concern and try to refer them on to relevant services, thus decreasing the abuse that the older person is involved in (P04).
The findings presented in this sub-theme provided insight into a particular source of the complexity of managing elder abuse cases; the management of client relationships. The participants spoke about the management of an older person’s care as well as their relationships with family and the wider community as an important element of their case management and interventions. The sub-theme highlighted the connection between care plans and protective interventions through the participants’ descriptions of linking their clients with community and home care services. These services minimised the risk to the older person by decreasing their social isolation, the provision of physical and social care needs as well as relieving potential carer burden. This element of the participants’ work frequently involved them in delivering interventions and support to a perpetrator of abuse in order to reduce the vulnerability or risk of an older person. The sub-theme emphasised that contact with perpetrators and the management of client social, care and family relationships was a
significant feature of the protection plans and interventions established by the elder abuse services.
5.2.6 Evaluating Case Outcomes
This sub-theme focused upon the criteria and standards by which the participants evaluated the outcomes of a case. The participants’ accounts of the various aspects of their case management and interventions revealed the complexity of elder abuse cases. The participants explained that this level of complexity must be accounted for when evaluating the outcomes of a case. In particular, they reported that their client-centred approach to case management determined that they evaluated the outcomes of a case in relation to the older person’s expectations and wishes. One participant explained that this necessity to take direction for case management from the older person imposed limitations upon expectations for a case. This participant argued that evaluation of outcomes must be realistic in terms of the limitations imposed by the older person:
They sometimes want the behaviour to change without addressing it openly with the alleged perpetrator. They sometimes just want to tell you about it and that is enough without having to address any changes in the person’s behaviour … Are you looking for a miracle or are you looking for something amazing to happen? Or are you being realistic that you are working within the older person’s expectations and limitations? (P11).
In their accounts, the participants recognised the challenge, presented by the right to self-determination, to realising a positive outcome to an elder abuse case. However, they spoke about the importance of continuing to respect this right despite the case outcome. One participant, for example, reflected upon a negative case outcome which resulted from lack of careful attention to the direction of the client:
But that was one that didn’t turn out well and really made me take a step back and realise that all the time you have to go at the pace of your client … if you throw solutions at them or try to drag them along with the solution the outcome won’t be great (P18).
In their evaluation of case management and outcomes, the participants highlighted some of the key aspects of a successful case. These aspects included: the increased
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 39
Chapter 5 Findings Part 2: Protecting Older People
safety of the participant, the establishment and continual review of a protection plan, a client-centred approach and also effective interagency working which incorporated all relevant service providers, family members and the older person. One participant, for example, identified effective interagency working as key to a successful case outcome:
I suppose why that worked was because everybody was on board … including the person causing concern I suppose that was why that case worked like. I suppose it was very much bringing everybody around the table and then [we] put a review into place (P03).
The participants’ accounts of their decision-making with regards to closing a case were also reflective of the complexity of the phenomenon of elder abuse. Many of the participants spoke about finding this aspect of their case management quite challenging. The source of this difficulty was their desire for a positive resolution to the situation of abuse and the recognition of the limitations of their practice with regards to client choice and self-determination. The participants spoke about creating ‘life-lines’ for their clients, which were understood as routes back into the social work service for those older people that have refused intervention or have decided to remain at risk of abuse. The maintenance of these life-lines required a form of distance monitoring whereby the participants would establish links with care providers and they would supply the older person with the appropriate information to engage the protection services in the future. One participant, for example, described this form of distance monitoring as providing a safety net for the older person through effective interagency links:
And we had to close the case because she didn’t wish for me to work with her anymore … So what I did was really just try to create a safety net … The home helps continued to be allowed in, the lady was attending day centre and if any major issue came or she made another disclosure to refer it onto us and we would deal with it (P15).
This sub-theme highlighted that expectations for case outcomes were modified by the recognition of the multifaceted and complex nature of elder abuse. In particular, the findings indicated that the client-centred direction of the protection services necessitated evaluating case outcomes in relation to the older person’s
expectations and wishes. A key finding emerging from this sub-theme was the role of interagency working in the establishment of life-lines for a client and the on-going monitoring of a situation. These interagency links were important for the participant to manage the dilemma of having to close a case despite the on-going abuse or vulnerability of the older person. This challenge was reflective of the unique phenomenon of elder abuse particularly in relation to balancing a client’s autonomy with risk.
5.3 Interagency WorkingThe complexities and practical challenges of interagency working was a further theme emerging from the participants’ accounts of their case management. This major theme highlighted the necessity and challenge of interacting on a daily basis with other agencies that come into contact with an older person from the health and community care sectors. While the participants spoke about the benefits of interagency work in terms of offsetting some of the negative effects of working single-handedly they also remarked upon the challenges inherent in this type of work and the particular skill set it demanded:
It is very definitely a multi-agency/multi-disciplinary intervention so you have to relate to a lot of different groups of people and individuals … that takes a lot of skill in itself, to get people to share cases with you, share the responsibility with you and attend meetings (P09).
The presentation of findings under this theme of interagency working was divided according to the following sub-themes: Interagency referrals, interagency communication and negotiating boundaries and approaches. These sub-themes explored the various encounters the participants had with other agencies in the course of their work and provided the participants’ perspective upon this aspect of their role in protecting older people from abuse.
5.3.1 Interagency Referrals
One of the primary ways that the participants encountered other agencies was through referrals of suspected elder abuse cases from organisations working with older people as well as service referrals made by the participants when implementing a care plan for their
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience40
Chapter 5 Findings Part 2: Protecting Older People
client. This sub-theme of the findings was concerned with the accounts of this referral relationship and the specific challenges and opportunities it presented to the delivery of a successful intervention. The most common agency sources of referrals, noted by the participants, were public health nurses followed by GPs, family and members of the public. Some of the participants remarked that interagency referrals may occasion a source of tension particularly in relation to the appropriateness of the referrals. As one participant described, inappropriate referrals can come from an agency due to a lack of understanding of the participants’ role in relation to elder abuse rather than adult services:
There are public health nurse and GPs that will refer anything because I’m a dumping ground, so I just take those with a pinch of salt, and say you know, ‘forget it like, this doesn’t seem even to be abuse’, so I’ll send it back (P02).
Another aspect of the referral relationship between the participants and other agencies was the necessity for the participants to establish a care plan for their client which involved service referral. One participant, for example, spoke about the various services that were involved in establishing a care plan:
I think a lot of what I use is actually referral to services, referring the older person to ... the likes of day centres, inpatient respite, increasing home care packages, referring them to [voluntary service] who have a home visitation service (P10).
While overall the participants recognised their effective interagency working in terms of service referral some of the participants spoke about difficulties in accessing particular agencies including psychological and geriatric medical assessment, financial and legal advice. Accessing legal advice emerged from the participants’ accounts as important for supporting their role in protecting older people from abuse. One participant, for example, commented upon the role legal services can play in deciding upon the best intervention for a case:
They would have been present at various professional meetings to say is there any way that we can best protect this lady or is there any other legal framework that we can use? (P04)
Many of the participants spoke about the budgetary restrictions imposed upon their access to legal advice which might have implications for their referral to this service. However, as one participant acknowledged, if they could establish a need for legal advice based upon the particular requirements of a case, access to this service was usually forthcoming:
If legal advice was really necessary, I was never refused legal advice but I would only use in very few cases and it has to be specific, specific reason for it (P05).
A further aspect of interagency working and service referral which emerged from the participants’ accounts was the perceived need for greater input from both the legal and the banking sectors, particularly in relation to protecting older people from financial abuse. As one participant remarked, these institutions were implicated in the role of protecting older people, however the participant found it difficult to get banks and the legal profession on board:
In relation to say legal profession and in relation to banks and things like that … I think we need them on board to take more of a role in terms of protecting older people. I think we need them on board and I think it’s hard to get them on board (P07).
The findings presented under this sub-theme focussed upon the referral relationship between the participants and other relevant agencies. These findings revealed the necessity of this relationship in terms of establishing effective case interventions through interagency service referral. The participants spoke about relying upon agencies for referrals to the protective services as well as for establishing interventions and protection plans. The findings presented under this sub-theme highlighted the necessity for greater understanding among the agencies of the role of the participant in protecting older people. In particular, the appropriateness of referrals was revealed to be a source of tension in this interagency referral relationship. Furthermore, it was reported that there was need for the agencies to recognise their responsibility to support the protection plans implemented by the participant and to work to reduce the vulnerability of older people. The findings highlighted legal services, as well as financial institutions and geriatric medical services, as being particularly relevant to this discussion
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 41
Chapter 5 Findings Part 2: Protecting Older People
of the need for greater awareness of elder abuse issues and responsibility towards vulnerable older people.
5.3.2 Interagency Communication
Good communication skills were highlighted by the participants as being integral to the efficacy of their interagency working. This sub-theme explored the findings related to the participants’ evaluation of their interagency communication and networking. There was widespread acknowledgement among the participants for the importance of effective communication with other relevant agencies:
And I suppose one of the things you have to be is to be very open with people and to be transparent so that they know what the service is about, that they know that they can just pick up the phone to you at any stage, or maybe if they just want to talk to you about a case. And being visible as well has helped (P14).
Furthermore, establishing a good working relationship with key personnel within the relevant agencies was reported by the participants as being critical to effective service delivery for their client. As one participant pointed out, the establishment of a working relationship was built up over time and was grounded upon trust and respect for each other’s role:
If the service provider for whom you are looking for a service from knows you … and knows you are a professional, knows that the information you give is reliable, that you follow through on work you say you will do … It generally leads to better interagency working definitely … if you know someone or you have a contact in an agency you can get things done quicker (P10).
Many of the participants spoke about the importance of interagency work not only for the establishment of care plans but also as a means of monitoring a client’s situation through communication with agencies delivering services to the older person. As one participant explained, integration with the agencies provided on-going support to the participants in their role in protecting older people from abuse:
Tell those services, ‘if you notice a change in the other person’s behaviour, if they tell you something about things deteriorating at a home, come back to
me, let me know.’ And often with those cases I am so reliant on that information, for them to link back in (P14).
Another participant highlighted the need for agencies to feedback into the protection services in order to maintain this monitoring relationship:
Other professionals don’t feel they need to link back with you so you make the referral or you make a contact with them and they are involved but they don’t think it is necessary to get back to us. [There is] huge frustration among us (P13).
The participants recognised that the development of good communication and trusting relationships with the relevant agencies often occurred on an informal basis. As one participant explained, bureaucratic communication procedures or protocols may act as an impediment to existing affective informal communication:
But I would know some of the community guards here … And often, off the record you would have conversations with them … I wouldn’t go to the station because then you lose the confidentiality aspect of things then, if it goes into a book, there is going to be a report … often I would ask them to keep an eye on a house, just to see if you are passing by if there is anything (P06).
This sub-theme highlighted the communication and networking skills which were integral to the role of protecting older people and the delivery of effective protection plans. The findings indicated that these interagency relationships involved the establishment of trust and rapport between the participant and the relevant agency personnel and they were constructed over time. A key finding of the sub-theme was the role of effective interagency communication in the monitoring of clients and the continual review of protection plans. In particular, the participants emphasised the necessity for this communication to be two-way and they spoke about their reliance upon the feedback from the agencies in relation to the on-going monitoring of a client. A further key finding, which emerged from this sub-theme, was the caution regarding the formalising of existing interagency relationships. The participants argued that imposing mandatory reporting and bureaucratic regulation of these relationships may damage existing informal lines of communication established by the participants over time.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience42
Chapter 5 Findings Part 2: Protecting Older People
5.3.3 Negotiating Boundaries and Approaches
This sub-theme emerged from the participants’ accounts of the challenges of balancing the different disciplinary approaches to elder abuse and negotiating the specific responsibilities of the different agencies involved. One participant, for example, described the challenge of trying to establish a shared team-based approach to a case rather than agencies working independently of each other:
But if they take on a case it is usually like they take on the whole case and want to manage it … this kind of thinking within certain organisations that just want to stay very, independent maybe and they don’t want interference (P05).
Another participant spoke about the danger of agencies abandoning cases into the hands of the participant and therefore not recognising their on-going role in the case. This participant described the potential for agencies to wrongly claim ‘that’s [SCW’s] area, not ours’ (P16). Another participant provided a different perspective on this complex issue of role boundaries. This participant described an experience whereby a public health nurse had overstepped their role and thereby created difficulties for the participant in managing the case:
[public health nurse] … decided upon themselves to go and investigate themselves, screwed it up because they told the son who made the referral so the family were now divided and at loggerheads … and I was absolutely furious because the person they should contact is me immediately. They don’t go out and try and sort it out themselves because it’s not their role, it’s my role and they made a mess of it (P01).
The necessity to manage different disciplinary approaches emerged from the accounts as a challenge for effective interagency working. This was particularly evident from the participants’ discussions of balancing client self-determination with risk of abuse. One participant, for example, remarked that the greatest challenge of the role was balancing what the older person wanted with what other people thought was best for the client. A participant explained that the principles of social work practice ensure a client-directed approach to case management and intervention and this was often
difficult for family members as well as other professionals to accept. This conflict between the disciplinary approaches was particularly evident in cases where the participants had to weigh up a client’s wishes against risk. As one participant reflected, decisions in these cases were often difficult for professionals from differing disciplinary perspectives to accept:
You might be under a fair bit of pressure from your colleagues, like maybe a public health nurse, a home help or a GP … that famous phrase, ‘something must be done’ … And you go along and talk to him but he might still say, ‘no I don’t want anything’. And I suppose if he does, you have to respect that as well if he is able to make that decision (P08).
Another challenging aspect of negotiating disciplinary approaches, which emerged from the participants’ accounts, was concerned with the different attitudes towards a client’s rights in relation to the provision of information to family members. One participant commented upon the HSE and HIQA nursing home policies which make it compulsory to inform family members of incidences of abuse of an older person in their charge. The participant claimed that these policies were implemented even in cases where the older person had capacity and has expressed a wish for the families not to be informed (P16). Similarly, another participant commented on the challenge that this mandatory reporting of abuse to family members presented to an individual’s rights:
Sometimes you might find actually that the way that person is treated has actually been very ageist … they haven’t sought the person’s consent to contact a family member or to contact a professional … and that worries me because in that process the older person is lost, they have lost sight of the older person’s rights (P17).
A further source of interagency tension, related by the participants, was concerned with the differing procedural approaches taken by different disciplines. Mental health was identified by some of the participants as presenting a particular challenge in relation to accessing assessments. One participant described the difficulty they experienced in persuading clients to attend the service and to remain engaged. This difficulty was compounded for the participant by the inflexibility of the service:
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 43
Chapter 5 Findings Part 2: Protecting Older People
If I have a client that I’m working with, with mental health problems, but if they don’t keep their appointments they are written off the psych’s books … but because their mental health problem dictates who they see and who they, how they behave … they could miss three appointments at a time, then they don’t have a problem anymore and to me it’s just crazy (P02).
The participants identified the need to reconcile a social work and a medical model as a source for the challenge of negotiating different disciplinary approaches to the protection of older people. They recognised that the balance between the two approaches represented the best practice for the client in terms of service delivery and implementation of a care plan or intervention. However, many of them also noted the difficulties of working within a medical discourse particularly in terms of their authority to access services for their clients:
There is a lack of a clinical pathway for people who are in these sort of social circumstances, social vulnerabilities. Maybe not having had the opportunity to have a medical [diagnostic code for a mental disorder] on their situation and the gate keepers to services are medicalised, it is dominant a medical discourse. And I think in these situations it often needs a balance between the social and the medical (P17).
Awareness-raising and effective interagency communication were identified by the participants as key to overcoming the challenges posed by the negotiation of role boundaries and disciplinary approaches. The participants spoke about using the medium of the training sessions to heighten an understanding among the different relevant agencies about elder abuse from the social work perspective. One participant, for example, made the connection between awareness-raising and improved interagency understanding of client self-determination and the role of the case worker:
And I suppose the more I do awareness-raising and training, the more people understand. And I am talking to them and saying … ‘they have the right to choice, the right to self-determination.’ And sometimes the choices that they choose are not ones that you or me may feel are the right choice or that, but you have to respect that they have made that choice (P14).
This sub-theme was concerned with the participants’ reflections upon establishing role boundaries and negotiating inter-disciplinary approaches as a key challenge for their successful interagency working. The findings, presented in this sub-theme, related the difficulties and successes of the participants in establishing a team-based approach to the protection of older people. This involved emphasising the different responsibilities of relevant agencies and safeguarding role boundaries. A key finding emerging from this sub-theme was the participants’ experiences of conflict between disciplinary approaches. This conflict was particularly manifested in the practice of establishing a client-directed service and respecting an older person’s right to self-determination. Furthermore, the findings revealed the challenge for the participants of combining a medical and social work model in their approach to protecting older people. They reflected upon the frustration they felt when confronted with inflexible disciplinary procedures; this was particularly relevant to their discussion of the mental health services. Finally, the sub-theme presented the participants understanding of the role of awareness-raising, communication and training in addressing these challenges. They commented upon the successes they had experienced in establishing good interagency practice through the forum of awareness-raising and training.
5.4 Experiencing the RoleThis third major theme of the findings emerged from the participants’ overall perspectives on their role and their evaluation of the experience of protecting older people from abuse. In the findings presented under this theme, the participants took an overview of their day-to-day practice and reflected upon their general experiences of managing cases within particular structural contexts. This major theme, ‘Experiencing the role’ was divided into the following sub-themes: The ‘lone worker’ and managing caseload and time.
5.4.1 The ‘Lone worker’
The participants reported working within the structure of a dedicated health service for the protection of older people and they noted that they had sole responsibility for the delivery of this service within their geographical boundaries. This sub-theme of the findings presentation emerged from the participants’ discussion of this
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience44
Chapter 5 Findings Part 2: Protecting Older People
structural context. In particular, they reflected upon feeling isolated in terms of the extensive workload and responsibility of the post. The challenge of working without administrative support was a particularly strong feature emerging from the participants’ accounts. They noted the cost of administrative demands in terms of time spent with the older person:
We need some kind of a secretarial service, it is madness here, you are doing your own typing, printing, photocopying, dealing with issues on the phone. We are being paid a social worker team leader salary and I would rather be using my time to deal with older people than sitting here at the desk (P15).
A related issue, which emerged from the participants’ discussion of the administrative aspects of their role, was an increasing fear of litigation that led to an emphasis on report writing and record keeping. This compounded the challenge of working alone for the participants particularly in relation to the amount of time taken up with their administrative duties:
I think people are very concerned about litigation and a lot of time is being spent now on making sure you have recorded this and you have minuted that … taking time away from clients (P10).
In their accounts, the participants connected the challenges and demands of their administrative duties with their sense of working in isolation. Many of the participants noted the lack of a social work duty system or a team-based approach to the protection of older people. As one participant remarked, the lack of a team approach was often the most challenging aspect of the role:
I find the difficult part of the work, and the most challenging part of the work I suppose is that it’s a single-handed post. I’m not a member of, there’s not an established team (P03).
Similarly, another participant compared prior professional experience of a social work duty system with current experience of a single-handed post:
I worked on the duty system so there was 5 social workers who were very much part of a team based in the same office and knew all the same cases and really were very cohesive. So this took a while to
get used to because you are kind of an individual (P18).
The participants related this individual-based approach to their role with a sense of isolation and a feeling that they are carrying the responsibility for often complex and distressing cases on their own. As one participant noted:
When it is appropriate you will be liaising with other professionals but there are some cases that come to us … and there isn’t need for other services to be involved so you won’t be liaising with them. So you are dealing with the complexities of the case by yourself (P14).
Another participant commented on the burden this sense of isolation can place on personal well-being:
There wouldn’t be a whole lot of laughter and fun in work because there is sadness with elder abuse cases. And because, when you are single handed, you are not really rubbing shoulders a whole lot of the time with people (P17).
A further implication of the single-handed nature of the post that emerged from the participants’ accounts was their concern for their own personal safety. As one participant acknowledged the role often incurs risks to personal safety:
It’s not the safest of jobs, and we go to places that are in the middle of nowhere, and we’re going to houses that nobody has been in for years … it’s a very unsafe job (P02).
Similarly, another participant connected the single-handed nature of the post with an increased risk to personal safety:
We are very much lone workers … what kind of a situation are we putting ourselves into as well like? … because sometimes we don’t know (P03).
This sub-theme emerged from the participants’ reflections upon the lack of structural work supports for their role. In their accounts, they identified a sense of having to take on the responsibility of a demanding and pressurising role on their own. A key finding arising from this sub-theme was the challenge of working without administrative support and the demands this placed upon the participant in relation to time. The participants acknowledged that the post of protecting older people
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 45
Chapter 5 Findings Part 2: Protecting Older People
was unique in terms of their prior professional experience of a duty or team-based approach to protective services. This presented a challenge to the personal safety and well-being of the participants. They noted a sense of isolation and spoke about having to cope with the impacts of distressing and complex cases on their own. This challenge of working alone was compounded by the nature of elder abuse which was often complex and multi-dimensional as well as an increasing case-load.
5.4.2 Managing Caseload and Time
This sub-theme concerned the participants’ reflections upon managing a demanding caseload with limited resources in terms of time. Time management was a predominant concern raised by the participants in their discussions of the various aspects of their role. They noted the demands placed on their time by their different duties and the necessity for them to prioritise the older person at the centre of an abuse case. The delivery of training and raising awareness was an aspect of their role which emerged from the participants’ accounts as carrying a heavy burden in terms of their time management:
Last year I did training with home helps and public health nurses and older people themselves and I’d have ran I would say something in the region of maybe 40 or 50 sessions last year, that’s very time consuming (P07).
While the participants recognised the implications of training and awareness-raising on their time they also acknowledged the efficacy of these duties in terms of their increased profile among relevant agencies. One participant, for example, commented upon the increase in appropriate referrals as a result of training sessions with relevant agencies:
Since I started doing [training sessions] I get more appropriate referrals … it makes life busier but they are more appropriate and people are more able to identify possible abuse and to refer it on (P15).
The participants connected the awareness-raising duties of their role with an increasing number of referrals. They commented upon the implications of this for their caseload and time management. The sometimes overwhelming caseload was described in their accounts and they spoke about the implications of this for their
management of time. One participant, for example, described the constant struggle to respond to referrals and to manage a demanding caseload:
I have 100 open cases at the moment … and I have about 30 unallocated cases … I’ve done the preliminary assessment but they are not high up on the priority list and I have maybe 7 that I haven’t even done the preliminary assessment on because they have only come in this week … then I have 8 or 9 from that one nursing home, which I’m trying to work my way through today and I’m getting nowhere fast (P02).
Similarly, another participant described the implications of taking an annual leave day in the context of a demanding caseload and the lack of any administrative support:
I had 28 messages on my landline and 19 messages on my mobile on Monday after the weekend. I had been out of the office on Friday. It is crazy, how do you even prioritise? (P15).
Furthermore, another participant identified the size of the geographical area under the remit of a senior case worker as well as a demanding caseload as having an impact upon case management:
But actually trying to get to see everybody and do a proper assessment and do what you should be doing as a professional is hugely difficult because of the numbers and because of the geographical area that we’re covering (P04).
A predominant aspect of the participants’ accounts was their necessity to prioritise their duties in the face of overwhelming caseload and time demands. Many of the participants identified risk as the primary concern for prioritising cases and they spoke about evaluating the risk to an older person’s safety posed by the abuse:
It depends on the risk, if it’s an immediate risk, if it’s severe or substantial risk then obviously that takes priority over everything else so every case is prioritised (P06).
In recognising the importance of risk for prioritising cases, the participants acknowledged the implications of this policy for cases of abuse which have been evaluated as low priority:
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience46
Chapter 5 Findings Part 2: Protecting Older People
I suppose my priority would be I give some cases more time, more attention. I suppose we could make a mistake and not give enough attention to one case that you didn’t think was serious maybe (P12).
Self-neglect cases were frequently mentioned by the participants as being vulnerable to de-prioritisation under circumstances of a demanding caseload and the necessity to evaluate risk. One participant explained, when faced with a large number of acute high risk cases, self-neglect cases are often moved down the list of priority because of the chronic and on-going nature of self-neglect:
You go through I think periods of time where there would be a whole lot of crisis cases and for a period there I had to actually stop taking cases because the caseload was so big and self-neglect became very low on the priority because it is a situation that is on-going and it is a situation that is not likely to change (P11).
The logistics of geographical boundaries were also a factor that emerged from the participants’ accounts of managing a demanding caseload. They spoke about planning their case visits according to travel and time restrictions and they noted the phenomenon of ‘geographical visits’. As one participant explained, when travelling to a particular location to manage a high-priority case they would organise to visit any other clients who may be resident in that area:
Sometimes it’s kind of a practical matter as well, let’s say if you are going to visit a certain area and you have two or three cases there, you kind of tend to maybe deal with them first because you know you can actually go and visit the person (P05).
As many of the participants noted, the practicalities of ‘geographical visits’ allowed for effective case management within budgetary restrictions on travel, however, these restrictions can have a discriminating effect for those clients in very isolated areas. The practicalities of single-handedly managing a demanding caseload in the face of budget and travel restrictions emerged from the participants’ accounts as a necessity of their everyday practice. The findings presented in this sub-theme described the requirement to balance the concerns for client risk with the realities of an overwhelming caseload. The participants noted the
implications of juggling caseload, risk and practicalities for the service delivery. In particular, they acknowledged the repercussions of these practicalities for those cases which are pushed down the priority list as well as those in isolated geographical areas.
5.5 SummaryThis chapter was composed of three major themes which emerged from the data analysis: Case management and interventions, interagency working and experiencing the role. The first of these major themes ‘Case management and interventions’ included six sub-themes which provided a step-by-step description of the accounts of managing a case from the initial referral to the final case evaluation. The participants’ emphasised case management as being the most important aspect of their role. In particular, they spoke about the interventions they put in place on behalf of, or with, their clients which reduced the risk and impact of abuse. This often involved working with perpetrators of abuse as well as establishing rapport and contact with other professionals and family members. Furthermore, the findings presented according to this major theme, connected the establishment of care plans with the protection of older people, by highlighting the role of care plans in reducing vulnerability and potential carer burden. These thematic findings revealed how the multifaceted nature of elder abuse; its unique complexities and challenges, determined the day-to-day practicalities and functions involved in case management and the provision of protective interventions.
The second major theme presented in this chapter was ‘Interagency working’. This major theme was composed of three sub-themes which emphasised the necessity and practical challenges associated with establishing effective interagency relationships. Crucial to these working relationships, were open lines of communication and the establishment of trust and rapport with agency personnel. The participants emphasised the time they invested into establishing effective communication and they noted that these relationships were often formed on an informal basis. They reflected upon the importance of safeguarding these relationships as critical to the delivery of a holistic protective service. A key finding emerging from this major theme was the necessity of the participants to negotiate role boundaries and responsibilities. This finding indicated that this complex negotiation was often a source of interagency tension.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 47
Chapter 5 Findings Part 2: Protecting Older People
The participants commented upon meeting this challenge through on-going awareness-raising and communication. Also emerging from this major theme was a reflection upon the participants’ experiences of reconciling medical and social models in their approaches. They described the tensions and frustrations they experienced in negotiating differing disciplinary procedures and discourses concerning elder abuse and access to services. These tensions represented a significant challenge to the participants in their service delivery and they noted the role of interagency awareness-raising and training to address this challenge.
‘Experiencing the role’ was the final major theme presented in this chapter. This major theme was composed of two sub-themes which provided the participants’ overall perspectives on their day-to-day practice in relation to the structural contexts in which they operated. A key finding emerging from this major theme was the lack of structural supports for the role in terms of administration or a team-based approach with participants reporting that they worked very much on their own. This had implications for the personal safety and well-being of the participants and was particularly relevant to the challenge of managing a demanding and increasing caseload. The limited resource of time was found to present a significant challenge to case management and the participants described feeling overwhelmed at times by the caseload demands. Prioritisation was a common feature of the accounts and it was revealed to be a key strategy employed to reconcile the challenges of working alone with limited resources. However, a key finding emerging from this major theme was the recognition that the necessity to balance resources and case management had implications for the delivery of services to those deemed low risk or who were living in an isolated rural location.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience48
Chapter 6 Findings Part 3: Developing Service Capacity
6.1 IntroductionThis chapter reports on the participants’ experiences of the structural support for their capacity to protect older people from abuse. These structural supports were identified and assessed at an organisational, policy and legislative level. Furthermore, the participants reflected upon the relatively nascent establishment of the service for the protection of older people and therefore this chapter of the data presentation emerged from their evaluations of the service and their suggestions for its future progression. The chapter consists of following major themes:
• Supporting the senior case worker
• Authority to act
• Standardised practices and protocols
The findings, presented under these major themes, provide the participants’ evaluations of the structural facilitators and barriers to their service delivery as well as to the future maturation of the services as a whole. These structures included: access to resources, legislative and policy frameworks as well as protocols and practices. An overview of the thematic structure of the chapter is presented in Figure 6.1.
6.2 Supporting the Senior Case WorkerThis major theme described the participants’ experiences of managing cases of elder abuse in terms of the resources and supports they required to deliver an effective service and intervention. The findings emerged from the participants’ discussion of strategies for future service development and means of enhancing their capacity to deliver an effective service intervention. One participant observed that client need must be the driving force behind any capacity development and the participant called for an evaluation of the service in terms of unmet need:
The most basic [criteria] is unmet need. What service was this client requiring which could not be availed of or was not in existence? … what provision do we have to put in [place] in future to meet these demands, or these needs? (P01).
This major theme of the study findings emerged from the evaluations and suggestions for the development of the service in terms of infrastructural supports and resources. The theme was divided into the following sub-themes: Service structures and supervision, resource development and professional development.
Figure 6.1: Developing Service Capacity
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 49
Chapter 6 Findings Part 3: Developing Service Capacity
6.2.1 Service Structures and Supervision
This sub-theme was concerned with the participants’ reflections upon the service structures in which they operate and their evaluation of the service efficacy in terms of these structures. A participant, for example, questioned whether the existing structures in which the service is placed are appropriate. This participant argued for evaluating service need and subsequently to put in place the necessary structures to address this need and realise effective service delivery:
I think we need to decide really where elder abuse is going to be, where it is going to fit in … we should look at the actual service as such, the need for the service and then decide where we go rather than trying to fit into the existing service structures … if it means that we need to create new structures then I think we should try and do that (P05).
In their assessment of service need, the participants spoke about the difficulty they experienced in delivering their service to older people vulnerable to abuse in isolation of any generic social service for adults. Many of the participants spoke about being diverted into cases which are outside their remit because of an absence of any alternative social care options. The participants spoke about not wanting ‘to turn their back on’ people who needed a service despite the fact that they did not fit under the remit of elder abuse. One participant, for example, explained that the elder abuse service was often used to fill an existing gap in terms of social service delivery to adults:
I suppose more welfare type concerns, maybe to do with housing or whatever like. They might not necessarily come under my remit … I have to because … they are looking for help as well. In some of the cases they have no support either or don’t know where to go with these cases like (P03).
The participants spoke about the challenge of balancing a demanding caseload with a perceived service gap in terms of primary social care for vulnerable adults in the community. Many of the participants argued for the enhancement of the service structures to support the delivery of a generic service for adults. The participants spoke about these enhanced structures as providing greater support to them in terms of meeting their increasing caseload as well as ensuring the effective
delivery of services to meet existing need. A participant, for example, expressed a desire to utilise existing primary care to meet the increasing demand for the elder abuse service. This participant explained that those cases which have been assessed as low priority or as involving minor cases of abuse could be handled by a primary care team social worker, thereby freeing the participant to focus on the more complex cases. Similarly, another participant expressed a desire for a duty system for elder abuse which would create a team-based approach to service delivery for vulnerable adults:
So like a duty system for elder abuse or even some kind of duty system that will cover mental health adults service, vulnerable adults duty system, I know it is funding and that but the ideal would be to have a duty system (P15).
The existing structures for the delivery of child protection services were frequently cited by the participants as representing a potential model for the development of services for the protection of older people. One participant, for example, spoke about this model as providing the potential for enhanced service delivery in terms of greater family support and the provision of long term protective interventions:
There is a need to look at the child protection service as a model and cherry pick from it in terms of having family support workers maybe or social care workers that can actually do the longer term piece work with a family (P17).
A further, frequently cited, benefit of the development of team-based approach to the protection of older people was the potential to garner greater support for the role from these structures. The participants’ accounts frequently referenced a sense of working in isolation and a feeling of sole responsibility for service delivery. For this reason, the participants argued that a team-based approach would enhance the service and provide them with greater structural support. As one participant explained, the availability of a team with the relevant management structures would allow for the responsibility of a demanding caseload to be shared and thus provide a more effective delivery of service:
That you have basic grade social workers, you have social work team leaders and you have a principal … It doesn’t just have to be for the older person …
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience50
Chapter 6 Findings Part 3: Developing Service Capacity
If you have structure and you know where you can go back and talk to somebody, if issues arise, you’re more likely to work in a more effective way (P04).
The participants’ desire for a team-based approach to the protection of older people was related to their evaluation of their managerial structures and support and in particular the challenges associated with working single-handedly. All of the participants were receiving some degree of managerial supervision. This supervision pertained to their professional development and often to the management of complex cases. The participants spoke about obtaining supervision for cases which involved complex legal concerns, determining capacity and balancing concerns of risk as well as decision-making regarding case closure. However, in their discussion of their day-to-day case management the participants frequently spoke about a sense of working on their own and the resulting feeling of personal responsibility in relation to their case management and decisions. This acknowledgement of their sense of isolation typically resulted in a call for greater clinical supervision and support by the participants. The participants spoke about requiring more clinical supervision in their case management which would provide them with greater confidence and thereby increase the efficacy of their service. One participant, for example, spoke about the necessity of social work supervisory skills:
Sometimes you are so immersed in the case, you are getting stories from every side; you need somebody who is removed with social work supervisory skills (P15).
While some participants reported having limited access to clinical supervision others testified that they did not receive any such supervision and had to rely on general line management or support from their colleagues. One participant, for example, spoke about garnering peer support to compensate for the lack of clinical supervision and thereby prevent stress associated with working alone:
I would love to have regular supervision but I don’t so what I do is I look to my peers to make sure within cases that I am working well so if I am working better I know that I am not going to be as stressed (P04).
Similarly, another participant explained the benefit of having peer contact in terms of discussing a case and evaluating the direction for the service delivery:
I suppose if you have any complicated cases, you’d talk about them and I suppose you just try to thrash them through … and then we’d have a discussion about it, how to actually move it forward … it’s a sounding board to just try and thrash it out (P03).
In the findings presented within this sub-theme, the participants argued for a needs-based analysis and approach to decision-making concerning the progression of the elder abuse service. The sub-theme highlighted the need for generic services for the protection of all vulnerable adults as well as increased personnel to facilitate the management of a demanding caseload. This structural concern was related to the participants’ evaluation of their supervision and management supports and their sense of working single-handedly. Emerging from this sub-theme was a concern for a team-based approach to the protection of vulnerable adults and the management of elder abuse cases.
6.2.2 Resource Development
This sub-theme was concerned with the participants’ views of the resources available to them to support their role in protecting older people from abuse. The lack of administrative support emerged from the participants’ accounts as a barrier to their effective case management. This resource deficit contributed to the participants’ sense of working on their own and it resulted in a challenge for the participants to meet the demands of an increasing caseload. As one participant explained, the lack of any administrative support presented a challenge to case management because administrative duties encroached upon the time allocated for service delivery:
There is no secretarial services, no screening, it is just me here and you never know what is at the other end of the line … it keeps getting pushed back, keeps getting pushed back and keeps building up, it is a huge amount of calls on that phone on a day to day basis and emails and that (P15).
In their discussion of their administrative duties, the participants spoke about their sense of mounting pressure and frustration. They noted the difficulty this resource deficit presented to them in relation to
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 51
Chapter 6 Findings Part 3: Developing Service Capacity
structuring their case management and delivering an effective intervention. One participant, for example, argued strongly that administrative duties were an ineffective allocation of time in terms of service delivery. The participant conveyed a strong sense of the frustration which was common to many of the accounts:
I am the best paid secretary in [county] ... That is the most frustrating part. I spend probably 40 percent of my time on administrative duties, a downright disgrace (P09).
Travel allowance and budgetary travel restrictions also emerged from the accounts as structural barriers associated with limited resources. The participants frequently commented upon the impact this restriction had upon their capacity to manage a demanding caseload across a wide geographical boundary. As one participant explained, budgetary travel restrictions presented a challenge to effective management of cases of elder abuse across large geographical boundaries:
One of the difficulties we have here now as well is that our travel allowance is cut back to 300 miles a month and we cover 2 counties here, we cover as far as [town], which is about, almost 50 miles from here. So that is 100 if you go out and do your business there that would be a third of your budget gone in one day (P12).
The participants observed that the travel restrictions did not account for the practicalities of an elder abuse case intervention which necessitated a degree of face-to-face contact in order to establish the rapport required for risk assessment. A participant made the point that the vulnerability of those older people who lived in very rural or isolated areas of a county was increased through the implementation of the travel restrictions:
If somebody lives in town and I get a call about them, the chances are I will hop in the car and I will call around. And I might call to somebody who lives in town 50 times and the chances are if they live out on the border of [county], if I go out there once they will be lucky to see me … you have got a limit on your travel, so you are not going to be able to go out there two or three times a week (P07).
Limited resources also impacted the participants’ case interventions in terms of their access to community
based care and support services. Emergency respite care featured strongly in this discussion and the participants explained that they had very limited access to this service intervention. In crises situations, which required the removal of an older person from a situation of abuse, the participants described having to fall back on women’s refuge centres and general hospital accident and emergency admissions. They agreed that accident and emergency hospital admissions and women’s refuges were not appropriate for older people and the preference would be for more dedicated emergency respite services. As one participant recognised, limited access to this resource impacted upon efficacy of the service intervention and the participant identified respite as an unmet client need:
It would be good to be able to remove somebody from a situation until it dies down and allow them back in and often they want that, it is not that I would be taking them out. So I suppose something like that would be very good, access to an emergency bed (P15).
Also included in the participants’ accounts of the limited intervention resources available to them was their recognition of the need for greater community-based care services in the form of home help and day-care facilities. Many of the participants commented upon the decreasing availability of these community-based services and as one participant explained, this impacted upon their capacity to protect an older person from abuse:
I suppose even getting home help twice a week for a person is really difficult and you know if you have that, that at least that is somebody else going into the house (P14).
The role of these services in the delivery of an effective case intervention was universally noted by the participants. They described using these services in their protection plans for the on-going support and monitoring of a client. As one participant pointed out, the limited access to these resources presented an obstacle to the service capacity and restricted the participant in terms of intervention planning:
And I think at the minute the resource issue, you can’t get any home help or home care packages really in this area at the minute so we haven’t got that to offer (P18).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience52
Chapter 6 Findings Part 3: Developing Service Capacity
Another feature of the participants’ accounts of limited resources impacting upon service capacity was recognition of the need for greater community-based counselling and advocacy services. This was particularly relevant to the participants’ discussion of the need for longer term protective interventions which would support the participants’ emergency protection plans. One participant, for example, observed a deficit of counselling support for carers and family members suffering stress which had long term implications for the prevention of elder abuse:
So if more help was available to families who are under stress and strain. Through the Carer’s Association, if they had access to free counselling. There is a counselling centre here in [town] but there is a 3 month waiting list for that. If that was more available I think it would be an excellent source of support (P11).
This sub-theme described the particular resource areas which provided challenges to the participants in terms of the realisation of an effective service intervention. These resource areas included; a lack of administrative support, budgetary restrictions and travel allowance. Further areas of resource deficit highlighted by the participants included access to community-based care services, most notably respite services, home-help, day care facilities, advocacy and counselling services. These resource limitations were perceived as structural barriers impacting upon the capacity of the participant and the efficacy of the service. They contributed to the participants’ sense of working on their own without support and they disadvantaged older people living in rural and isolated areas. These structural barriers and limitations impacted negatively upon the participants’ protection planning and the availability of necessary care interventions which would protect an older person from abuse.
6.2.3 Professional Development and Training
This sub-theme explored the participants’ accounts of their professional development and their access to training. The participants’ experiences of the training they had received since they began their role in protecting older people were varying. There were some participants that were satisfied with the type and level of training that they had undertaken. For example, one participant spoke about receiving training on cognition
and dementia and spoke about annual training as being beneficial to practice:
Well the training every year now, I do benefit from that, giving me more insight on dementia and cognitive impairments … yes I think it is very important to have training (P17).
There were, however, other participants who gave a poor account of the training received in terms of its relevance to their practice and their professional development. These participants spoke about wanting training to reflect their needs and they pointed out the particularity of their needs in terms of the individual working to prevent elder abuse and protect older people. As one participant argued, training should arise from need and it should reflect the complexity of elder abuse and the practice of protecting older people:
They should ask us what we want, and they should listen to us … we can perfectly well do case … they had us up in Dublin doing case scenarios. I mean for Christ sake, we’re well out of college, it’s a nonsense, we need something more in-depth (P01).
The participants identified particular training needs which arose from a reflection upon their experience of managing elder abuse cases and their day-to-day practice. Handling cases involving family conflict, which required mediation and counselling skills, emerged from the accounts as an aspect of their work which would benefit from training. Many of the participants recognised that training in ‘family dynamics’ and in direct family interventions such as brief solution therapy would facilitate their management of these demanding cases. As one participant noted, family conflict frequently arose in cases of elder abuse and these cases were particularly demanding in terms of their complexity and the time cost associated with managing family conflict:
A huge amount of our work comes up around conflict within the family … Because those cases … are cases that are extremely complex, take up a huge amount of time and there can be a lot of anger and upset within those cases by the family, by the older person themselves (P14).
A concern with the legalities of their practice and the need for clearer guidelines and legal protection also arose from the participants accounts of their training and
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 53
Chapter 6 Findings Part 3: Developing Service Capacity
professional development needs. Report writing skills were frequently mentioned particularly as they related to the legal implications of the role of protecting older people from financial abuse. The participants conveyed a sense of anxiety associated with the complexity of cases of financial abuse and their uncertainty as to the limitations of their role in these cases. These participants argued for training which would clarify their role in relation to handling cases of financial abuse and which would provide consistency among their colleagues in terms of best practice for these cases. One participant described feeling legally vulnerable when managing cases of financial abuse and identified training in report writing and legalities as necessary to address this sense of vulnerability. Furthermore, the participant acknowledged the need for consistency in practice in relation to the handling of financial abuse cases:
I have looked for legal training on report writing, I have looked for legal training giving evidence … I sometimes feel the vulnerability, particularly managing financial abuse cases where I might actually stick my neck out a little bit further than might be expected in my role ... I suppose there is that kind of sense of what level of protection is there for us as case workers and if there was a fitness to practice enquiry then they are obviously going to look at what my colleagues would do in that case (P17).
A clearer understanding of the legislation that impacts upon the lives of older people also arose from the participants’ accounts as an area for future training. The impending Mental Capacity Bill was mentioned by the participants as an area which would require training as was a greater understanding of the Fair Deal scheme. As one participant explained the practicalities of protecting older people often involves managing clients’ legal or administrative decisions such as Fair Deal applications. This participant pointed out that this aspect of managing cases requires training which would provide the participant with the necessary competencies:
We’re being asked to go out and assist people to fill in the Fair Deal application forms as part, maybe as cases that we are involved in and I necessarily wouldn’t know enough about the Fair Deal myself actually (P03).
Another training area and knowledge deficit which emerged from the participants’ experiences of managing cases of elder abuse concerned the particular health conditions associated with ageing. They spoke about frequently encountering cases which involved clients with dementia or other cognitive and motor functional impairments associated with ageing. The participants recognised their need to understand these impairments better in order to deliver an effective protective intervention. According to the participants’ accounts, these cases had both a legal and a care aspect to them whereby it was necessary for the participant to be aware of guardianship and decision-making capacity issues as well as the care requirements associated with particular conditions. One participant, for example, spoke about the requirement to understand medical terms and conditions which are associated with a new referral and necessary for the subsequent case management:
I would like to understand more about when I get a referral in, hypertension, COPD, like I don’t know what they are … I would really something like that around older people’s conditions and what they mean and just have a little bit of knowledge
This sub-theme highlighted the specific areas that the participants identified as their training requirements as well as their experiences of their professional development and training so far. The areas identified for future training included: The health needs and conditions of older people, training in ‘family dynamics’ and in direct family interventions, report-writing skills and training related to the legal implications of their role. Training in best professional and legal practice in managing cases of financial abuse also emerged from this major theme as an area requiring training. Furthermore, the participants argued for more training in relation to legislation which impacts older people’s lives and the practice of protecting older people from abuse. The findings reported here underpinned the importance of delivering training on the basis of client and participant need. This needs-based training would reflect the multifaceted nature of elder abuse cases which often involve complex family dynamics and have legal and medical implications for the participants’ case management.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience54
Chapter 6 Findings Part 3: Developing Service Capacity
6.3 Authority to ActThis major theme of the findings was concerned with the participants’ views of the existing legislation and policy which informed their practice. Findings highlighted the ‘legal void’ in which the participants work to protect vulnerable older people. This void concerned the legislative protection of older people as well as the legal authority of the participant to act effectively to protect older people from abuse. This major theme was divided into the following two sub-themes: Protective legislation and policy as well as statutory powers for the role.
6.3.1 Protective Legislation and Policy
This sub-theme of the findings concerned the participants’ accounts of the legislation in place for older people and its impact on their role in managing cases of elder abuse. The deficit of protective legislation for older people vulnerable to abuse was identified across the accounts. One participant, for example, described this deficit as a ‘void’:
I mean the legal situation for us is there is only two pieces of legislation, that’s the Domestic Violence Act 1991 and the Lunacy Regulation Act of 1871 and apart from that we have nothing so I mean we’re left in sort of a big void legally (P01).
The participants’ discussion of the deficit of protective legislation or policy extended to the legal instruments available to older people in situations of family abuse. As one participant argued, court proceedings including barring orders were not appropriate for many cases of elder abuse by a son or daughter, particularly if the perpetrator was also the older person’s primary carer:
It is a very blunt instrument, a barring order. Because then once the older person gets the barring order, if the person comes back into the house again they are obliged to contact the Guards and they find it very hard to do that (P08).
The participants spoke about the increased vulnerability of older people with diminished capacity which resulted from a deficit of adequate protective legislation. One participant, for example, described a case which involved the financial abuse of an older person who had diminished capacity. The participant argued that the client’s capacity status precluded the Gardaí from taking the required victim statement and thereby prevented
them from pursuing the case further. This participant pointed to existing legislation in other jurisdictions whereby in cases where the victim has diminished capacity, an impact statement or testimony can be obtained from other parties, for example a social worker or a general practitioner.
Many of the participants spoke about the role of solicitors in cases of financial abuse and the need for stringent legislatively sanctioned codes of practice for the legal profession which would safeguard the best interests of an older person. This was particularly pertinent in the participants’ descriptions of the vulnerability of older people with diminished capacity, to financial abuse. The participants spoke about the discrepancy between medical and legal tests of capacity and questioned some solicitors’ judgements as to a person’s capacity to make instructions in relation to their will and other major financial decisions. The participants spoke about the vulnerability of older people in these situations and how perpetrators can use the inadequate protective legislation to carry out financial abuse. One participant provided a comprehensive account of the process by which older people are made vulnerable to abuse by a perpetrator using the inadequate legal frameworks and legislation:
A solicitor can arrive with a benefactor, and does sometimes, to an old person and makes a will. And the older person may, in the eyes of a number of people, not have capacity, but if they pass the legal test, whatever it is, and I am not too sure what it is, then the transaction will go ahead. That is frustrating because on occasions it certainly wouldn’t have been my opinion that they would have capacity. There is the whole issue then about whether the solicitor is acting for the benefactor or acting for the donor, and that is a big issue. And that is not enshrined in the new guidelines for will-making, for which I think it should be (P09).
A further aspect of the vulnerability of older people caused by inadequate protective legislation emerged from the participants’ accounts of the guidelines concerning home care workers. One participant raised a concern regarding the lack of a central body to monitor care workers and called for the implementation of legislation which would protect older people from abuse by care workers. In particular, the participant noted the
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 55
Chapter 6 Findings Part 3: Developing Service Capacity
need for greater accountability and monitoring for care workers in terms of their fitness to practice. The impact of the legislative void on the participants’ case management was noted in the accounts. They commented upon the increased complexity of dealing with cases of abuse under these conditions and they argued for the urgent need to implement new protective legislation. As one participant explained proper protective legislation would reduce some of the challenges associated with protecting older people including the time cost involved in cases which involved issues of capacity and wardship:
And the mental capacity bill, I think there has to be the resources for that quite quickly, you know, when that is passed. And the wardship act, I think that would help take the complexity and the challenges and the time that it takes to put those particular measures in place I think that will resolve a lot of those challenges (P17).
The findings presented under this sub-theme have highlighted the legislative void in which the participants work to protect older people. This void was shown to be particularly pertinent to cases where the older person’s capacity status increases their vulnerability to financial abuse and exploitation. Furthermore, the participants’ accounts described the role of the legal profession, particularly solicitors, in this process. They highlighted the need for better regulation of both solicitors as well as care professionals which would assist them in their role in protecting older people from abuse.
6.3.2 Statutory Powers for the Role
This sub-theme of the findings emerged from the participants’ discussion of the legal authority and powers associated with the role of protecting older people from abuse. Many of the participants agreed that the role required greater legislative authority in order to realise effective protective interventions. As one participant acknowledged, the general expectation for the role was high in terms of service delivery however, this high expectation was not matched with authority to act:
Senior case workers for the protection of older people have lots of responsibility but very little authority or legislative framework to back that up. So they are in a double whammy. The expectation is high and the resources or the authority is very, very low (P09).
The participants explained that they do not have any statutory right to access a person’s home and undertake a risk assessment and this emerged from their accounts as a source of frustration which was undermining the authority of their role. Many of the participants called for their rights to access and assessment to be given a statutory basis and thereby increase their power to protect a vulnerable older person. One participant described this statutory act as giving footing to the workload of protecting older people and argued that the lack of legislative authority for the role was hindering the delivery of the service:
I think the service probably cannot advance significantly and won’t unless there is some legislation in place to give some footing to the workload … You need access to an older person, we don’t have that at present. If somebody doesn’t want to let you in their house they don’t have to (P06).
The discussion of the statutory basis for the role of protecting older people also pertained to the participants’ desire for stronger legislation which would support their right to recommend protective services. Some participants compared the service to child protection where compulsory supervision orders can be put in place and they argued that similar legislation would increase their powers in relation to implementing protection plans. The participants referred to ‘legislation to back me up’ and spoke about having to develop protection plans without the authority to enforce them, instead they had to take an advisory or advocacy role. The discussion of this issue of greater power for the role of protecting older people included recognition of the need to balance an older person’s civil rights, in particular their right to self-determination, with the authority of the participant to act upon their concerns for an individual’s safety. One participant acknowledged the challenge of working to protect older people in the context of limited authority however, the need to safeguard the rights of the older person was also noted:
I suppose the short coming with working with older people is that if legislation could be brought in regarding a supervision order which gives you right to access and right to recommend services. But then again you are facing the whole civil rights issue (P12).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience56
Chapter 6 Findings Part 3: Developing Service Capacity
Another area in which the participants perceived a need for greater statutory powers for their role was in relation to their ability to access protective services including community care facilities and emergency respite. One participant identified a discrepancy between the policy and the powers associated with the role which can limit access to resources:
Well to me the biggest challenge is that we have a policy which suggests that we have more powers than we actually have … when it comes to actually resource management you don’t necessarily get all that much more influence in terms of getting those resources (P07).
Many of the participants described public health nurses as acting as gatekeepers today and home care services. This had the effect of limiting the participants’ direct access to these care services which were a vital aspect of their protection plans for vulnerable older people. While most participants agreed that they were able to overcome this barrier to services through good interagency relationships they also acknowledged that disciplinary focus can diverge between the health and social criteria for gaining access to care services. Many participants expressed a frustration at the lack of authority for their role which could present as a barrier to services and to successful interagency working. One participant recognised the need to balance statutory authority with the rights of an older person. However, this participant argued for the need for increased authority for the role when dealing with other agencies particularly in terms of realising the protective recommendations:
There is something about not having a statutory base makes sense because we are dealing with an adult population. But there is something about the power structures and the power dynamics and the people in positions of power who will have, it seems to me sometimes, a total disregard for the recommendations made by this service (P17).
The findings presented in this sub-theme concerned the participants’ perception of the need for greater statutory powers for their role in order to increase their authority to act. The sub-theme highlighted the complexity of the issue particularly in terms of the need to safeguard an individual’s right to self-determination. Furthermore, emerging from the participants’ arguments for increased
statutory powers was the importance they placed on having direct access to key protective services in the community for older people. This was related to the need for increased powers which would provide the participants with a stronger statutory footing in their interagency working, particularly in overseeing the recommendations of their protection plans.
6.4 Standardised Practices and ProtocolsThis major theme of the findings was concerned with the participants’ reflections on the procedures and protocols which guide their practice. The participants spoke about standardising best practice through the solidification of existing practice and the establishment of recognisable procedures and protocols. This major theme of the research findings included the following sub-themes; national standards and practices as well as risk assessment.
6.4.1 Current Practice and Procedures
This sub-theme of the data findings emerged from the participants’ consideration of their current practice and the need to establish consistency across the elder abuse service in relation to best practice. In comparing the service with child protection, one participant explained that while the procedures in child protection are clearly established much of the practices associated with the protection of older people have yet to be solidified into a general agreed understanding of best practice:
If I walked into any office in child protection I could probably pick up and take over cases, whereas if somebody came in here, any of my colleagues even, they’d say, ‘what is that about?’ … we need to able to have national standards … so, I think we need criteria … I think we need guidelines for just about everything, you know? (P02).
The relative youth of the service compared with other social protection services was attributable to the lack of clearly established guidelines for managing a typical case of elder abuse. The participants described the service as ‘very much your opinion and my opinion’ and ‘based on your experience’ rather than grounded in clearly identifiable standards. While this was understood in the context of a young service it was generally agreed that there was a need for the implementation of guidelines to
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 57
Chapter 6 Findings Part 3: Developing Service Capacity
create a sense of consistency in practice. As one participant commented, this consistency was required in terms of guiding the practice of the social worker but also in the structural supports for the role, including consistency in the management and supervision of the service:
Just to have consistency right across in terms of all the services and ourselves … other senior case workers have faced problems where they have a different management structure and just the inconsistency in the service (P13).
A fear of litigation associated with a lack of clear and uniform guidelines for practice emerged from the participants’ discussion of the need for standardised structural supports for the role. A hesitancy to document a case of abuse as being substantiated was a frequent feature of the participants’ discussion of their case management. As one participant explained, this hesitancy arose from a sense of legal vulnerability associated with a lack of structural support for consistent interpretation of the forms:
I’m also very mindful, I don’t want to put down substantiated and then there’s a freedom of information act going around and somebody wants to drag out a file and all pertinent paper work … I don’t want to be in a court situation trying to explain myself so to be quite honest … I’m not going to get myself into hot water for a silly bloody form (P01).
Similarly, another participant called for increased standardisation of practice in relation to the administrative duties associated with the role. The participant spoke about the need for consistency in protocols for report-writing and record-keeping particularly as the standardisation of these procedures would offer protection to the participant from legal scrutiny:
I would like very much for my files, my records to be fully scrutinised. And I would like a legal professional measurement done on them so that if I found myself in court or found myself defending my practice then at least I would know that I had a proper structured documentation or recording process (P09).
The procedures for documenting and receiving referrals also emerged from the participants accounts as an area of their practice which required greater consistency in terms of the information requirements for referrals. Some of the participants spoke about amending the referral form in order to make it a better fit for their purpose. One participant, for example, spoke about requesting more information from the referrer which would assist them in prioritising the case:
The referral form, we got one, but I amended it myself a couple of times, and I’ve asked for more information … and I devised a little system where I could prioritise … is the old person aware of the referral? … and if not, well why not? And if yes, what is their response or reaction to it? … names and addresses and telephone numbers of agencies involved … relationship to the older person for the abuser, and do they know this is coming in, and again if they do, what is their reaction? If they don’t, why don’t they? … (P02).
While the participants were largely in favour of the implementation of standardised procedures to guide their practice they cautioned for the need to safeguard some existing informal procedures which were working well. In particular, they spoke about the danger of enforcing a mandatory reporting relationship between the protection service and the Gardaí. As one participant explained, an informal relationship with the Gardaí is often more effective for safeguarding the protection of older people. Furthermore, the participant cautioned that this effectiveness could be undermined through the enforcement of formal reporting procedures:
Say the community Guard network … they would be able to tell you an awful lot in a very informal manner … if you go down the mandatory reporting route … I think sometimes when you have to report something compulsory it makes people think about it much more … you have to really think am I going to make this a formal complaint (P07).
The findings presented according to this sub-theme identified a need for standardised procedures and increased consistency across the service as to best practice guidelines. Inconsistent procedures for the referral and documenting of cases as well as the recording of case statistics were highlighted as creating a need for uniform interpretation of reporting requirements
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience58
Chapter 6 Findings Part 3: Developing Service Capacity
and consistency in terms of form-filling. The lack of widely recognised policy guidelines for current practice and procedures were found to be contributing to the participants’ sense of vulnerability to legal scrutiny of their accountability. However, the call for greater standardisation and consistency in practice was issued with a caution in terms of safeguarding the existing informal reporting relationships between agencies.
6.4.2 Uniform Risk Assessment
The findings presented within this sub-theme were concerned with the participants’ recognition for the need for standardised practices and protocols with a particular focus on their experience of working without a uniform tool for undertaking risk assessments. Assessment of risk was identified by the participants as a key aspect of their case management and began with the initial referral and information gathering followed by a meeting with the older person at the centre of the case. However, emerging from the participant’s discussion of this aspect of their case management was the finding that there was no standardised method for assessing risk which was shared by the participants. One participant for example explained current practice in relation to assessment as being undertaken on a case-by-case basis and argued for a more structured approach to this aspect of their case management:
We’re not using a risk assessment tool, a uniform risk assessment tool … maybe if a person scored twenty they might be in this category and if this person scored under fifteen we might put them in this category like … it’s just case by case we’re working at the minute … I suppose make it more uniform, to make it more structured … that everybody is kind of working the same like (P03).
Similarly, another participant highlighted the role of risk assessment in the prioritisation of cases in terms of the scale or degree of risk to the client. The participant identified the need to evaluate risk in terms of the perspective of the client:
People are hoping for a specific risk assessment tool … that is what we are waiting for … the scale of the degree of risk and how to value it in terms of the client’s perspective, how they see the risk and how we see the risk and how they could manage it (P13).
Some participants described their own ad hoc system for assessing risk which was devised in response to the deficit of a standardised and uniform tool. The participants described assessing risk in terms of degree and assigning priority levels according to the assessment. The participants spoke about the importance of these assessment tools in terms of informing their management of an increasing and demanding caseload. One participant, for example, outlined this priority scale for the assessment of risk and explained the relationship between this scale and case management:
… like a priority scale and we are looking at 1 to 4, so 1 being a case that comes in and you need to act on it that day, that minute … category 2 would be within 7 working days or within a week, depending on where you are … the third one … that would be within the next 6 to 8 weeks … and even to write out to a referrer to say, look we are not following up on this case because we have classified it at this category (P15).
This sub-theme identified a standardised risk assessment tool as a resource deficit currently experienced by the participants. The findings suggested the need to develop a tool which would assess risk from the perspective of the client and facilitate the prioritisation of cases according to degree of risk.
6.5 SummaryThis chapter was composed of three major themes which emerged from the data analysis: Supporting the senior case worker, authority to act, standardised practices and protocols. The first of these major themes; supporting the senior case worker, was divided into three sub-themes which explored the participants’ perspectives on the structural supports and resources necessary to enhance their capacity to deliver the service. They noted the relatively recent establishment of the service for the protection of older people and made suggestions for the future progression of the organisation. In particular they identified the need for a team-based approach to the protection of vulnerable adults and the management of elder abuse cases. This structural concern was related to the participants’ experiences of their supervision and management supports, in particular their call for increased clinical supervision.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 59
Chapter 6 Findings Part 3: Developing Service Capacity
A further key finding which emerged from this major theme was a discussion of the impact of resource limitations on service capacity. These limitations were perceived as structural barriers impacting upon the efficacy of the service. They contributed to the participants’ sense of working on their own without support and they disadvantaged older people living in rural and isolated areas. The particular resources identified by the participants included; administrative support, travel allowance and access to community-based care services such as respite, home and day care as well as counselling services. Finally, the major theme presented the participants’ arguments for needs-based training which would reflect the multifaceted nature of elder abuse cases. The areas identified for future training included: The health conditions of older people, intervention strategies for situations of family conflict, as well as report-writing. Furthermore, the participants identified financial abuse as being an area of their practice in which they required greater training as to their role and the legal implications of this type of abuse. The participants also argued for more training in relation to legislation which impacts older people’s lives and the practice of protecting older people from abuse.
The second major theme presented in this chapter was ‘Authority to Act’. This major theme was divided into two sub-themes which identified a need for increased protective legislation for older people as well as greater statutory powers for the role of protecting older people from elder abuse. The findings which emerged from this major theme highlighted the legislative void in which the participants work to protect older people. This void was shown to be particularly evident in cases which involved a client with diminished capacity. Furthermore the negative impact of this void was clearly demonstrated in the participants’ discussion of cases of financial abuse. A key finding from this major theme was the need for better regulation of both solicitors and care professionals in order to reduce the vulnerability of older people to all forms of abuse. A further significant finding, emerging from this major theme, was the identification of the need for increased structural support for the role of protecting older people in the form of greater statutory authority for the role. Direct access to key protective services, as well as greater authority in interagency working, were identified as key potential benefits of increased statutory authority for the role.
Finally, the chapter explored the participants’ perspectives on current practice and procedures and identified a need for standardised procedures and increased consistency across the service as to best practice guidelines. A key finding emerging from this major theme of the chapter was the participants’ sense of vulnerability in terms of their accountability to legal scrutiny. The lack of widely recognised policy guidelines for current practice was found to be a significant contributing factor to this sense of vulnerability. Procedures for the referral and documenting of cases as well as the recording of case statistics emerged from this major theme as key areas requiring greater standardisation and consistency. An important point, raised in the discussion of standardised practices and procedures, was the caution issued by the participants to safeguard existing informal reporting relationships between the agencies. While the need for increased standardisation across the service was identified as a key area for future capacity development, it was tempered by the recognition of the danger of increased bureaucratisation on effective informal relationships.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience60
Chapter 7 Discussion
7.1 IntroductionThe aim of this study was to explore the experience of managing cases of elder abuse from the perspective of senior case workers. The objectives were to:
• Explore senior case workers’ experiences in managing cases of elder abuse
• Examine current practices adopted by the senior case workers
• Examine the challenges and dilemmas faced by senior case workers in managing cases of elder abuse and how these are overcome
• Identify good practice in the management of elder abuse cases, as perceived by the senior case workers
• Ascertain priorities for future service development and provision for elder abuse, as perceived by the senior case workers.
The findings of this study make an important contribution to understanding the complex phenomenon of elder abuse in Ireland by revealing the nuanced and multifaceted experiences of 18 Irish senior case workers responsible for managing cases of elder abuse. This chapter discusses the findings of the study in the light of existing literature. The chapter begins with a reprise of the main study findings derived from the analysis of interview data.
The study findings highlighted the interlocking forms of abuse encountered by the senior case workers and the fluid boundaries between the various forms of abuse. This meant that elder abuse was experienced as a complex phenomenon and therefore difficult to recognise, detect and manage. The senior case workers recognised the particularities of elder abuse cases, which presented their own unique challenges, issues and dilemmas for social work practice. These particularities included the challenge of reconciling the autonomy and self-determination of their clients with issues of capacity, risk and vulnerability. Additionally, they described the necessity to manage cases of family conflict and entrenched patterns of familial behaviour. The management of this unique phenomenon was understood by the study participants to be highly demanding, in terms of assessing client capacity, making ethical judgements and using interpersonal skills.
Senior case workers provided accounts of case management, from the initial referral to the final case evaluation, showing how the multifaceted nature of elder abuse and its unique complexities and challenges determined the day-to-day practicalities and functions involved in case management and the provision of protective interventions. They spoke about the critical importance of effective interagency relationships and highlighted some of the challenges that they experienced in establishing and maintaining these relationships. The negotiation of role boundaries and responsibilities and the need to reconcile medical and social work discourses concerning best practice were described as potential sources of inter-disciplinary tension. The senior case workers pointed to the role of awareness-raising and training as a way to address this challenge. They provided evaluative data concerning the structural and resource contexts in which they operated, pointing to the need to balance resources and case management, which has implications for the delivery of services to those deemed to be at low risk or living in isolated rural locations.
The senior case workers offered their perspectives on the development of protective services, with reference to the capacity of the senior case worker service and the policy and legal framework in which the service is located. Many advocated a team-based approach to the protection of vulnerable adults and the management of cases of elder abuse. They perceived limited resources, inadequate training and a lack of clinical supervision as factors impacting on their service capacity. These structural limitations were described by the senior case workers as contributing to their sense of working on their own and disadvantaging older people living in isolated areas.
The senior case workers identified a need for increased protective legislation for older people and greater statutory powers for the role of the senior case worker. They also spoke of the need for better regulation of solicitors and care professionals and greater statutory authority for their own role in protecting older people from abuse. The senior case workers gave their perspectives on current practice and procedures, identifying a need for standardised procedures, greater consistency across the service regarding best-practice guidelines, procedures for case referral and documentation, and the maintenance of case statistics.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 61
Chapter 7 Discussion
7.2 The Complexity of Elder Abuse in ContextThe analysis of the participants’ accounts highlighted the multiple causes and outcomes associated with elder abuse cases. This complexity was revealed as posing challenges to the participants in terms of detection, assessment, intervention and prognosis. The participants described the many sources of vulnerability for an older person which contributed to the complexity of managing elder abuse cases. The most commonly encountered forms of direct abuse were financial, neglect and physical abuse as well as self-neglect cases. The research participants revealed that elder abuse often traverses the boundaries of the different types of abuse and it may have multiple dimensions requiring complex and often parallel intervention processes. This finding of the multifaceted nature of elder abuse is supported by international research which recognised that elder abuse is often difficult to define and is problematic in terms of identifying specific causes and determining outcomes (Fulmer et al. 2004, Kurrle 1993, Killick and Taylor 2009). This section of the chapter discusses the findings which provided a nuanced insight into the nature of elder abuse from the perspective of the senior case workers interviewed for this study.
7.2.1 Sources of Vulnerability
Psychological abuse emerged as a form of abuse frequently encountered by the participants in their management of elder abuse cases. This form of abuse was found to coincide with other, more direct, types of abuse such as financial exploitation, neglect and physical abuse. This finding is supported by previous research, which investigated the prevalence and nature of elder abuse in Ireland. This research found that psychological abuse was the most common form of elder abuse reported by older people since turning 65 years of age (Naughton et al. 2010). Furthermore, HSE referral statistics show that psychological abuse has been the most common type of abuse referral to the HSE and accounted for 26 percent of cases in 2011 (HSE 2011). A finding which emerged from the present study was the challenge for case management associated with the prevalence of psychological abuse. In particular, the participants spoke of the necessity to build the self-esteem of their clients and to empower older people to make decisions to end their abuse. This work was
undertaken by the participants with respect for the cultural and social forces which may influence an older person’s decisions as well as the right of an older person to self-determination. This finding is supported by the literature which identified low self-esteem as a risk factor for elder abuse and argued for the necessity of increasing the psychological resources of an older person as a preventative or coping mechanism (Podnieks 2006).
The legacy effects of historical abuse, endured over a long period of time, emerged from the data and provided insight into a nuanced understanding of elder abuse. This finding revealed the necessity of recognising the influence of the life course on an older person’s interpretation of their situation of abuse and their willingness for change. The findings revealed that spousal abuse in later life often presented as a historical abuse that had occurred throughout the marriage. The manifestations of this abuse tended to be multi-dimensional, shifting from physical to financial abuse with often chronic and long-term psychological abuse. These cases were particularly challenging and difficult to resolve as they involved complex negotiations of power and control over the lifetime of a marriage (Cosc 2010). Previous research has identified differentiation among types of domestic and intimate partner violence and noted the importance of recognising the evolution of domestic violence over the lifetime of a marriage (Cosc 2010, Kelly and Johnson 2008). In particular, Kelly and Johnson (2008) found that differentiation among types of domestic violence may have implications for the efficacy of particular interventions and so should be considered when designing protection plans.
The necessity to manage an older person’s caring relationships emerged from the findings as important for understanding the particularities of the role of protecting older people as well as the complex phenomenon of elder abuse. In the cases of financial abuse described by the participants, the abuser was most often a relative who was a primary care provider for the older person. Furthermore, neglect emerged as a common form of abuse, which often involved complex negotiations of care and a management of the expectations for care provision. The participants spoke about the need to balance the risk of abuse with the older person’s dependency on a perpetrator for their care. Social isolation was identified by the participants as a risk factor for abuse, particularly as it increased the dependency of the older person in
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience62
Chapter 7 Discussion
terms of their care relationships (WHO 2011). This finding is supported by the literature, which proposed community-based support groups to counteract social isolation, to relieve carer burden and to decrease the dependency of an older person (Podnieks 1999, Hightower et al. 2006, Dong and Simon 2008).
The necessity to account for the care dynamic in situations of elder abuse impacted the interventions of the participants and ensured that management of an older person’s care was embedded within their protection plans. The importance placed upon care interventions in the protection plans implemented by the participants is supported by other research, which reported that care services were the most common form of protective intervention targeted at reducing the vulnerability of an older person to abuse (Shibusawa et al. 2005, HSE 2011). Furthermore, it was reported that the provision of care interventions, such as home-support, meal delivery, visitations and community transportation, may help to promote the independence of an older person, reduce their social isolation as well as alleviating care-giver burden (Pritchard 2000, Pillemer et al. 2007, Nerenberg 2008).
A further dimension of this element of the participants’ protection planning was the necessity to negotiate the complexities of their clients’ inter-personal relationships, their expectations for care provision and their dependency on familial members for their care. The participants reflected upon their encounters with problematic patterns of inter-personal and familial behaviour which have become entrenched over a long period of time. This contributed to the complexity of elder abuse as a phenomenon which, like many forms of inter-personal abuse, must account for the dynamics of power and control in situations of vulnerability and potential dependency (Cosc 2010).
It is increasingly recognised that the distinct causal factors and myriad manifestations of elder abuse, alongside differences in geography, culture and community size and structure necessitate diverse approaches to managing cases of elder abuse (Fitzgerald 2006, Nerenberg 2008, Perel-Levin 2008, Podnieks 2008). The findings of the present study indicate that the causes, characteristics and outcomes of elder abuse are multi-dimensional. This complexity was manifested in the interlocking forms of abuse and the fluid boundaries between the types of abuse encountered by the
participants in their work. Accordingly, elder abuse was reported to be difficult to recognise, detect and manage. In particular, the challenge of reconciling the autonomy and self-determination of their clients with issues of capacity, risk and vulnerability emerged from the accounts as a facet of elder abuse which presented ethical dilemmas for the participants. These particularities distinguished elder abuse from other areas of social protection that the participants may have encountered in their prior professional experience. This finding is supported by the literature which reported that the management of elder abuse frequently necessitates difficult decision-making involving ethical dilemmas, which challenge the limits of professional knowledge and training (Donovan and Regehr 2010, Cambridge and Parkes 2004b, Pritchard 2000).
Enhancing the psychological resources of an older person is viewed as a preventative or coping mechanism (Podnieks 2006). The study participants recognised their role in addressing situations of psychological abuse through client esteem-building and counselling, pointing to the importance of interpersonal mediation and counselling skills as necessary attributes for successful management of elder abuse cases. The management of an older person’s care relationships was seen as integral to the protection plans implemented by the senior case workers and this indicated the importance of support service access and delivery, which others have highlighted as important care interventions for the prevention and management of elder abuse (Pritchard 2000, Pillemer et al. 2007, Nerenberg 2008). The senior case workers’ negotiation of inter-personal relationships in order to address dependency or vulnerability to abuse presented them with ethical challenges and necessitated difficult decision-making that may have implications for their professional training (Donovan and Regehr 2010, Cambridge and Parkes 2004b, Pritchard 2000).
7.3 The Practice of Protecting Older PeopleBoth researchers and practitioners advocate the need for varying models of intervention in elder abuse on the basis that no one model is likely to work for all older people (Podnieks 2008, Kurrle 1993, Killick and Taylor 2009). This study found that the multifaceted and complex nature of elder abuse necessitated a unique response from the
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 63
Chapter 7 Discussion
participants in terms of their case management practices and the implementation of protection plans.
Elder abuse involves multiple and complex dynamics between an individual at the centre of a case, the perpetrator of abuse, as well as the social and environmental contexts (Killick and Taylor 2009, Donovan and Reghr 2010, Kurrle 1993, Pratt et al. 1983). The study participants reported that they typically dealt with an average of 43 cases at any one time. Each case of elder abuse presents its own particular challenges and demands a unique response from the senior case worker, in terms of evaluation, intervention, long term prognosis and ascertaining outcomes. The participants’ accounts of their case management work revealed that the practice of protecting older people was located within particular legal, ethical and social frames of reference, which inform interventions as well as outcomes and prognosis. Donovan and Reghr (2010) noted that professional decision-making in cases of elder abuse must account for clinical, legal and ethical considerations. The participants’ practice involved complex negotiations of inter-personal relationships and balancing the concerns of the relevant professional agencies involved in the delivery of a holistic protection plan.
7.3.1 Assessment and Intervention
In their step-by-step accounts of their case management, the participants noted the importance of gathering contextual information relating to the older person from the referrer. They spoke about ensuring that the appropriate and necessary information was obtained in the early stages of the case management and intervention. This early information gathering was noted by the case workers as vital for determining the urgency of a situation and for assessing risk to an older person’s safety. This aspect of their practice is in line with international best practice as reported in the literature (Dayton 2005, Fulmer et al. 2003, Cambridge and Parkes 2004b, Donovan and Regeher 2010).
Information gathering from relevant referral agencies, which was most typically public health nurses (HSE 2011), as well as from clients themselves provided the foundation for the establishment and implementation of the participants’ protection plans. Fulmer et al. (2003) found that much consideration was given to contextual information relating to the older person and their caregivers when assessing for potential neglect. This
practice was echoed in the accounts of the participants in this present study, who spoke about gathering information from relevant agencies concerning the health and capacity of the older person at the centre of the case as well as their caregiver. Furthermore, where possible they attempted to validate this information from multiple agency sources, including public health nurses, professional carers and general practitioners as well as the client themselves and their family members.
Donovan and Regehr (2010) have argued that case workers must describe the options available to older clients so that they, together with the professional, can choose which interventions best suit their beliefs, culture, community and philosophy of life. The accounts of the participants for this present study emphasised client direction and respect for an older person’s autonomy and right to self-determination. They spoke about the importance of supporting the client to lead the direction of the intervention and empowering them to take control of their situation. Accounts of intervention planning referred to the importance of ascertaining the perspective of a client on their situations of abuse. Ascertaining client direction emerged from the findings of this study as well as from the review of literature as crucial to the effective management of cases of elder abuse and the delivery of appropriate interventions (Pritchard 2000, Anetzberger 2004, Kalaga et al. 2007, Pratt et al. 1983, Cambridge and Parkes 2004b).
Cambridge and Parkes (2004b) reported that adult protection cases are frequently complex and do not necessarily follow a sequential model; in many cases there may be multiple or parallel investigations and concurrent planning or case conferences as new evidence emerges. In their reflections on their practice, the participants of this present study revealed how the multifaceted nature of elder abuse determined the day-to-day practicalities and functions involved in case management and the provision of protective interventions. In particular, they noted the multi-dimensional aspects of their protection plans which might involve actions to address client social isolation or to limit dependency on strained care relationships and address carer burden. Their protection plans included direct actions such as linking the client to available services for the provision financial management, care, welfare and housing, counselling, legal advice and advocacy.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience64
Chapter 7 Discussion
Findings report the complexity of elder abuse cases and participants explained that this complexity must be accounted for when evaluating the outcomes of a case. In particular, they reported that their client-centred approach to case management determined that they evaluate outcomes of a case in relation to the older person’s expectations and wishes. They also spoke about the need to balance a professional desire to implement protective interventions against the client’s right to self-determination as being a key challenge to successful case resolution. This was particularly evident in the face of client refusal or withdrawal from protective services. This finding is supported by the literature reviewed for this study (Cambridge and Parkes 2004b, Wilson and Micucci 2003, Killick and Taylor 2009, Dayton 2005, Donovan and Regehr 2010, Neale et al. 1997). In particular, Wilson and Micucci (2003) highlighted the difficulty of ascertaining outcome measures in cases of elder abuse which necessitate respect for client autonomy and self-determination.
The research reviewed for this study referred to the importance of a multi-disciplinary approach to elder abuse case management for the on-going monitoring of situations post-intervention (Anetzberger et al. 2005, Penhale 2008). In this study, participants spoke about the strategies they employed to overcome challenges to case closure and successful case resolutions. In particular, they spoke about effective interagency working in the establishment of life-lines for their clients which would facilitate them to re-engage with protective services. They also spoke about establishing an interagency team-based approach in their case management, which allowed them to monitor potentially abusive situations from a distance. Multi-disciplinary teams and interagency working emerged from this study, as well as from the reviewed research as important for addressing the dilemma of having to close a case despite a suspicion of on-going abuse or vulnerability of the older person (Perel-Levin 2008, Baker and Heitkemper 2005, Nerenberg 2006, Penhale 2008).
7.3.2 Interagency Working
International research points to the importance of a multi-disciplinary approach to elder abuse case management, which enables on-going monitoring of situations in the post-intervention phase of a case (Anetzberger et al. 2005, Penhale 2008, Cambridge and
Parkes 2004a). A recent review of Protecting Our Future (DoHC 2002) also reported a recognized need for increased interagency working in elder abuse services and suggested that protocols are needed to underpin and strengthen governance structure and the ‘whole system’ (NCAOP 2009). Interagency working emerged from the findings as central to the role of the senior case worker in undertaking assessments and implementing interventions and protection plans. The participants spoke about building up referral networks with agencies and organisations working with older people in the community. Public health nurses were noted as being particularly important interagency network members and were the most common source of referrals to the participants (HSE 2011). The emphasis placed on effective interagency working by the participants is in line with international best practice for adult protection services (Perel-Levin 2008, Baker and Heitkemper 2005, Nerenberg 2006, Penhale 2008). Furthermore, research which has evaluated models for adult social protection has indicated the importance of establishing integrated multi-disciplinary teams with a range of expertise and resources to deal with the diverse and complex circumstances in which elder abuse occurs (Baker and Heitkemper 2005, Nerenberg 2006, Penhale 2008). Inter-disciplinary teams are considered to be imperative to successfully develop and implement effective integrated strategies for the protection of older people (Perel-Levin 2008).
In discussing their practice the participants for this present study acquired specialist input from different disciplines throughout the process of identifying, assessing, intervening, planning and monitoring their elder abuse cases. In this way, the inter-disciplinary approach adopted by them reflected the models of best practice described in the literature (Anetzberger et al. 2005, Penhale 2008). One of the predominant features of the protection plans, outlined by the participants, was their holistic approach to establishing and managing the care situation of the older person. In particular, the participants frequently mentioned employing the services of home help, public health nurses, respite facilities, day care facilities as well as private care options. The under-developed nature of services for older people in the HSE has been viewed as a constraint on the senior case worker’s ability to connect more widely with other social workers and psychiatric services and multi-disciplinary teams in delivering primary care for older
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 65
Chapter 7 Discussion
people in the HSE (NCAOP 2009). Nerenberg (2008) noted the importance of creating a network of support services around a vulnerable older person which would reduce their risk of abuse by addressing social isolation, increasing the client’s independence and relieving informal caregiver burden.
While many of the senior case workers acknowledged the importance of interagency networking for effective protective planning, they also noted that this work demanded a high degree of leadership, administrative, and particularly interpersonal communication skills. They highlighted effective communication and relationship building as being integral to the efficacy of their interagency working, particularly in guaranteeing successful case conferences and devising a holistic protection strategy. A key finding of this study, as well as the reviewed research, was the necessity of establishing trust and rapport within the multi-agency teams (Penhale 2008, Teaster et al. 2005). The participants for the present study noted that these relationships were established over time and required a high degree of inter-personal skills to maintain their efficacy. Perel-Levin (2008) noted that the strength of an interagency and multi-disciplinary approach to the management of elder abuse is an acknowledgement of the limitations of individual disciplines and the acceptance of different points of view and approaches. International research in this area acknowledges the importance of tackling elder abuse using a broad spectrum method and also recognises the challenges that can emerge from this interagency approach (Lachs and Pillemer 2004, Nerenberg 2006, Perel-Levin 2008, Donovan and Regehr 2010).
7.3.3 Client Relationship Management
In their accounts of their case management practice the study participants reflected on the work that they do with an older person in terms of ascertaining their wishes and empowering them to control their situation. They spoke about their case management practice as being client-centred and they depicted themselves as following the direction, wishes and pace of the client. International research has indicated the importance of establishing a personal connection with an older person and their family for effective interventions in cases of abuse (Pratt et al. 1983, Nerenberg 2008, McKenzie 1999, Kalaga et al. 2007, Anetzberger 2004). The participants argued that rapport and trust building with a client was central to
their effective protection of older people and ensured client direction in the delivery of interventions.
The senior case workers’ spoke of the need to negotiate the complex dynamics of family relationships in the delivery of protective interventions and of the need for communication and engagement with family members in implementing protective plans. Their practice in this regard is supported by a number of authors (Groh 2005, Kalaga et al. 2007, Podnieks 2008) and is informed by an awareness of the older person’s potential dependency on familial relations for their care and social contact (Parra-Cardona et al. 2007). A significant feature of the SCWs work was the delivery of interventions and supports to the perpetrators of the abuse. Previous research reported that interventions targeted at abusive caregivers may help to prevent re-offending (Nahmiash and Reis 2000, Reay and Browne 2002) and may include the establishment of restorative justice (Nerenberg 2008). This approach necessitates working to restore client relationships and resolve conflict. Engagement in family mediation and conflict resolution was a feature of the senior case workers’ effective case management, although they faced challenges in realising a positive outcome for an older person in situations of family conflict (Groh 2005).
In summary, the delivery of a client directed intervention was crucial to effective protection planning (Pritchard 2000, Anetzberger 2004, Kalaga et al. 2007, Pratt et al. 1983, Cambridge and Parkes 2004b). The complexity of the protection plans implemented by the study participants reflected the best practice advocated by international research (Cambridge and Parkes 2004b). These plans integrated multiple protective pathways to available supports and services and were tailored towards the needs and direction of the clients. Multi-disciplinary teams were considered crucial for the delivery of a holistic protective service in terms of assessment, intervention, prognosis and monitoring (Perel-Levin 2008, Baker and Heitkemper 2005, Nerenberg 2006, Penhale 2008). This was particularly significant in addressing the participants’ dilemma of having to close cases despite continued concerns over vulnerability (Anetzberger et al. 2005, Penhale 2008). A key finding of this study was the necessity of establishing trust and rapport within the multi-agency teams (Penhale 2008, Teaster et al. 2005). Furthermore, the necessity to maintain and safeguard client relationships, even in situations of abuse or
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience66
Chapter 7 Discussion
concern, emerged as a significant aspect of senior case workers’ practice of protection planning. These interventions to reduce an older person’s vulnerability to abuse were undertaken within the context of care dependency and a desire to limit a client’s risk of social isolation. However, conflict resolution, family mediation and perpetrator interventions were found to be time consuming, costly and particularly challenging in terms of securing a successful outcome for the older person at the centre of a case (Groh 2005).
7.4 Challenges to Managing Elder AbuseThe participants for this study identified the key challenges to their work and the barriers to an effective protection plan. These barriers included structural limitations such as an increasing caseload, a lack of resources, regional inconsistencies in procedure, a lack of interagency co-operation as well as access to clinical supervision. The barriers and limitations that they identified are supported by previous research which highlighted similar issues as impacting upon the efficacy of the response provided by this specialist service in Ireland (NCAOP 2009). The complexity of elder abuse necessitates the balancing of risk with self-determination and managing the values and expectations of various multi-disciplinary agencies. It would appear that structures and resources continue to act as barriers to a consistent and holistic approach to tackling elder abuse across Ireland.
7.4.1 Structural Barriers and Limitations
The detection and reporting rates of elder abuse will continue to grow alongside increasing public awareness and education concerning elder abuse (Baker and Heitkemper 2005, Perel-Levin 2008, Cooper et al. 2009). In discussion of their practice in protecting older people from abuse, the participants identified an increasing caseload and limited resources as key challenges. They noted the necessity to prioritise cases and to juggle risk assessment with the practicalities of a demanding caseload. They recognised that this increasing caseload was an indication of success in relation to raising awareness of elder abuse among community organisations and agencies working with older people.
Pritchard (2000) described the pressure that adult protection workers experience in managing cases with limitations on their time, resulting in rushed investigations and an overemphasis on the administrative elements of the work rather than on clients’ needs and interaction. The participants for this present study spoke of their increased caseload and the resulting pressure on their time and resource management. They described feeling overwhelmed at times by the caseload demands. Risk assessment and prioritisation were identified by the participants as key strategies for assessment and intervention planning. Prioritisation on the basis of risk has been reported in other research as a key decision-making strategy for elder abuse case management (Cambridge and Parkes 2004b, Donovan and Regehr 2010). Similarly, in their accounts of managing an increasing caseload and limited resources, the participants for this present study described prioritising cases according to risk. However, they recognised the repercussion of this strategy for those cases which are pushed down their priority lists as well as those in isolated geographical areas.
Research has highlighted the availability of resources and the size of practitioners’ caseloads as potential structural barriers to effective decision-making, impacting upon case outcomes (Jogerst et al. 2001, Cambridge and Parkes 2004b). In their accounts of their case management, the study participants reported that the challenge of managing a demanding caseload was compounded by a lack of structural supports, including administrative support, clinical supervision and sufficient social or health care resources. A recent review of the dedicated elder abuse service noted that the lack of ring-fenced funding for resources such as respite and emergency beds makes it difficult for senior case workers to source alternative accommodation, particularly for older people who may be in dangerous situations (NCAOP 2009). The participants noted that they had the sole responsibility for the delivery of the elder abuse protection services within their assigned geographical borders. They reflected on their sense of isolation in coping with distressing and complex cases. This may be attributable to the fact that the senior care workers’ role is not fully integrated with other HSE services for older people across the four HSE regions (NCAOP 2009). This difficulty presented a challenge to their personal well-being and, in some cases, to their safety. Schwiebert et al. (2000) noted there is often a pressure on social
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 67
Chapter 7 Discussion
workers to equip themselves with expertise on a diverse range of issues, including legal, well-being, finances and human rights. Best practice in managing cases of elder abuse requires access to specialist advice and resources which enhance service delivery and ensure greater structural support for the individual case worker (Schweibert et al. 2000, Pritchard 2000).
Access to clinical guidance and impartial supervision from professional colleagues, as well as specialist advice, have been identified as key to successful protective service delivery (Cambridge and Parkes 2004b, Bergerson 1999, Pritchard 2000). In this study all participants received some degree of managerial supervision. However alongside the limitations of structural supports, such as administration and community-based social and health care resources, some study participants identified a lack of access to regular peer support and clinical supervision as representing a challenge to their practice. They noted that these structural limitations may have a particularly detrimental effect on their decision-making processes. A review of the dedicated elder abuse services noted an absence of professional supervision arrangements and indicated that having no facility to get second opinions on intricate cases may mean that senior case workers may be more reluctant to close cases, thus causing delays in case management (NCAOP 2009). Furthermore, it may curtail the opportunity for CPD on best practice in relation to managing elder abuse cases (NCAOP 2009). Pritchard (2000) reported that managers and supervisors of adult protection workers must have sufficient clinical knowledge and experience of the area in order to adequately support those delivering a service.
7.4.2 Effective Interagency Communication
The study participants highlighted the difficulties presented by multi-agency working, particularly in having to reconcile different disciplinary approaches to elder abuse and negotiate the specific responsibilities and role boundaries. They experienced a challenge in combining medical and social work models in their approach to protecting older people from abuse and they highlighted the frustrations of working within inflexible disciplinary procedures and contradictory disciplinary discourses. Research has found that the practice of respecting client autonomy often involves a social worker in conflict between a concern for the individual’s rights and professionals’ views of the best interests of an older
person (Donovan and Regehr 2010). This finding was echoed in the participants’ accounts of their contact with mental health services and their encounters with inter-disciplinary perspectives on their practice of establishing a client-directed service. These challenges of reconciling different disciplinary approaches and perspectives are confirmed in the literature (Beaulieu and Leclerc 2006, Donovan and Regehr 2010).
The importance of raising awareness for addressing interagency tension, ensuring effective communication and recognising role responsibilities has been identified as being important for the effective management of elder abuse cases (O’Loughlin and Duggan 1998, Penhale 2006, Bonnie and Wallace 2003, Halphen et al. 2009, McCreadie et al. 1998, McCreadie et al. 2000, Oswald et al. 2004). The interagency tensions that arose from a negotiation of role boundaries and differing disciplinary perspectives represented a significant challenge for the participants in the present study. A particular source of interagency tension was associated with inappropriate referrals and a lack of understanding among the agencies of the role of the case worker in protecting older people. The participants spoke of their work in raising awareness, delivering interagency training and effective interpersonal and interagency communication as playing a positive role in addressing this challenge.
Teaster et al. (2005) identified the main challenge facing multi-disciplinary teams as a lack of participation and engagement by certain disciplines, including law enforcement, medical professions, prosecutors, attorneys, financial institutions and regulatory agencies. Similarly, the participants in this present study noted the challenges they experienced in establishing a team-based approach to the protection of older people. This challenge arose from a lack of awareness among relevant agencies of their respective responsibilities in safeguarding the protection of older people and supporting the protection and care plans implemented by the case workers. In particular, the legal, financial and geriatric medical services were highlighted by the participants as being particularly relevant to a discussion of the need for greater awareness among agencies of elder abuse issues and their responsibilities towards vulnerable older people.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience68
Chapter 7 Discussion
7.4.3 Balancing Self-determination with Risk
This study confirms that best practice in protecting older people from abuse is grounded in the principle of respecting client autonomy and self-determination (Donovan and Regehr 2010, NASW 2008, Regehr and Antle 1997). A key challenge to the practice of implementing this principle is the sometimes competing imperative to reduce risk and vulnerability (Donovan and Regehr 2010, Beaulieu and Leclerc 2006). This emerged as a key aspect of the participants’ accounts of their practice. The literature has highlighted the difficulty shared by many adult protection practitioners in accepting a client’s refusal of services and their withdrawal from protection plans, despite on-going risk and vulnerability, and this challenge is integral to the complexity of managing elder abuse cases (Dayton 2005, Cambridge and Parkes 2004b, Wislon and Micucci 2003). Wilson and Micucci (2003) noted that the necessity to respect client autonomy often has negative implications on the decision-making process of an adult protection practitioner regarding case closure and assessing outcomes.
Cambridge and Parkes (2004b) reported that when advocacy occurs from within a health and social care setting a conflict may arise between the desire to promote the needs of clients and the perspectives of professional organisations within which the advocate works. The participants in this study referred to the ethical dilemma experienced in representing and advocating for the best interests of their clients. They spoke about having to reconcile their values as well as the perspectives and values of other relevant professionals with a client’s understanding of their situation, their choices regarding their living circumstances and their desired outcomes for an intervention. Podnieks (2008) has argued that advocacy services should always be independent from formal service delivery systems.
Part of the ethical challenge experienced by the participants in managing cases was a concern for an assessment of a client’s cognitive capacity to make choices about their living circumstances and to appreciate their risk and vulnerability. Their practice of representing the best interests of their clients and designing a client-directed intervention was contingent upon a client’s capacity to make decisions. Beaulieu and Leclerc (2006) found that practitioners tend to be
comfortable ceasing intervention when the older person is autonomous and has the necessary cognitive capacity to make an informed choice.
Situations in which there is doubt about an older person’s capacity to make decisions for their own protection represent a challenge to case closure and effective protection planning (Beaulieu and Leclerc 2006, Donovan and Regehr 2010). Donovan and Regeher (2010) have argued that crucial to the effective management of elder abuse is ready access to appropriate advice and skills for assessing and determining cognitive capacity. The participants for this present study described their anxiety and frustration in having to rely on other services for capacity assessments. This reliance represented an acute challenge to their protective practice as they encountered inter-disciplinary barriers in attempting to access these services.
The complex and multifaceted nature of elder abuse constituted the key challenges to managing elder abuse, as identified by the senior case workers who participated in this study. They described their experience of managing an increasing and demanding caseload in the context of structural barriers and limited resources. Of particular concern, was their perceived lack of administrative support for their role and limited or inconsistent access to clinical supervision, which has potentially negative repercussions for effective decision-making and case outcomes. Best practice in managing cases of elder abuse requires access to specialist advice and resources, which would enhance service delivery and ensure greater structural support for the individual case worker (Schweibert et al. 2000, Pritchard 2000, Cambridge and Parkes 2004b, Bergerson 1999, Jogerst et al. 2001).
A further key challenge to the effective management of elder abuse, identified by the senior case workers, was interagency tension with regard to role boundaries and responsibilities as well as reconciling different disciplinary approaches (Beaulieu and Leclerc 2006, Donovan and Regehr 2010, Teaster et al. 2005). The importance of raising awareness for ensuring effective communication and recognising role responsibilities was identified as important for addressing this tension. The necessity to balance client self-determination with risk presented ethical challenges to the participants, which impacted on their decision-making regarding case closure (Wilson and
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 69
Chapter 7 Discussion
Micucci, 2003). This challenge had implications for their role in advocating for their clients as well as their access to capacity assessment.
7.5 Augmenting the Protection of Older PeopleIn referring to the challenges and barriers to their protective practice, the participants for this study argued for a needs-based analysis and approach to decision-making regarding the progression of the elder abuse service in Ireland. In particular, they identified the structural limitations in which they operated their protective service and reflected upon the ethical dilemmas associated with the complexity of elder abuse. In making recommendations for the development of protective service capacity it was therefore necessary to explore the perceived needs as experienced by the participants and their perceived unmet needs of clients. Key areas for the recommendations for future service development included structural supports such as resources, assessment tools and the standardising of best practice. Furthermore, the broader legal and policy context for service delivery was evaluated from the participants’ perspective on the current inadequate protective legislation and the statutory basis for their role.
7.5.1 Developing Resources
In their evaluation of the resources available to support their role in protecting older people the study participants highlighted a lack of access to sufficient support resources. Perceived resource deficits, identified by the participants, included a lack of administrative support, budgetary restrictions and limitations on travel allowance. Community-based care resources were also identified as deficient by the participants. In particular, they spoke about a lack of reliable and consistent access to respite services, home-help, day care facilities, advocacy and counselling services. These resource limitations were perceived as structural barriers impacting upon the capacity of the participant and the efficacy of the protective service. Furthermore, they contributed to the participants’ sense of working on their own and they were viewed as disadvantaging older people living in rural and isolated areas.
The participants’ discussion of their resource limitations highlighted the need for a structured and integrated
service for the protection of all vulnerable adults in Ireland. In particular, a multi-disciplinary team-based approach to the management of adult protection was identified as key to overcoming some of the structural barriers, including limited access to clinical supervision and the sense of working in isolation. International practice in relation to managing elder abuse indicates the efficacy of generic adult protection services in the United States and Great Britain (Bonnie and Wallace 2003, Steigel and Klem 2007, Department of Health 2000). Many of the study participants referred to the child protection model as an example of a team approach to the protection of all vulnerable adults. They argued that this team approach would ensure greater consistency in service delivery and would facilitate the management of an increasing and demanding caseload. A multi-disciplinary team approach to adult protection which would encompass elder abuse is in line with national guidance in the UK (No Secrets), which recommends the establishment of multi-disciplinary adult protection committees at local level to facilitate interagency collaboration and partnership working (Department of Health 2000).
The experiences of the senior case workers, interviewed for this present study, indicated a lack of consistency with regard to training and professional development. They stressed the importance of on-going training for their role, which would include input on client needs and the multifaceted nature of elder abuse cases. They noted that the management of elder abuse often involves complex family dynamics and may have legal and medical implications for protection planning. The literature has identified the diverse skills, knowledge and training necessary to manage the complex multifaceted nature of elder abuse (Schaffer 1999, Pritchard 2000). The training areas identified by the participants included: the health conditions of older people, intervention strategies for situations of family conflict, financial abuse, legal implications and the senior case worker’s role and report writing. They also argued for more training in relation to legislation which impacts older people’s lives and the practice of protecting older people from abuse. An implication for these self-reported training needs is the necessity to monitor the training needs of the senior case workers managing elder abuse, in order to identify and target unmet needs with specific tailored training programmes (Schaffer 1999, Pritchard 2000).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience70
Chapter 7 Discussion
Assessment of risk was identified by the participants as a key aspect of their case management practice and this began with the initial client referral and information gathering, followed by a meeting with the older person at the centre of the case. However, many of the participants remarked that there was no standardised method for assessing risk available to them in their work. This finding indicates a need to develop, or have available, a risk assessment tool. The literature, reviewed for this study, discussed the efficacy of numerical and standardised measures of risk (Bonnie and Wallace 2003, Anetzberger 2001, 2004). Anetzberger (2001, 2004) argued that screening tools, which would provide a measure of risk, may facilitate professionals who are in contact with older people to recognise vulnerability and guide them through a systematic process of observation and inquiry. This could lead to more appropriate referral of cases as well as making transparent the processes by which cases are prioritised. The findings of this present study support the literature which indicates the potential for standardised risk assessment and screening tools to contribute to the effective management of caseloads and the accountability of protective service delivery and intervention.
7.5.2 Standardising Practice
During accounts of their practice the study participants highlighted the need to establish consistency across the elder abuse service in relation to best practice. They reflected upon the delivery of protective interventions for older people at risk of abuse and noted that current practice was not standardised by recognisable protocols or procedures. Inconsistencies in ways of working at local level were also reported in a review of the service which was commissioned by the National Council on Ageing and Older People (NCAOP 2009). This review highlighted that these inconsistencies may be attributable to the absence of agreed HSE protocols and policies to guide case management and engagement with other agencies (NCAOP 2009). Although the HSE has developed a staff policy called Responding to Allegations of Abuse, the review found that current approaches to case management is driven largely by the personal commitment and dedication of the senior case workers and on the effectiveness of their networks (NCAOP 2009). The lack of widely recognised policy guidelines for current practice and procedures was perceived by participants as contributing to their sense of vulnerability
to legal scrutiny of their practice. Procedures for the referral and documenting of cases as well as the recording of case statistics were identified by them as key areas requiring greater standardising and consistency. Specific guidelines and protocols for identifying and responding to elder abuse are seen as essential in almost all health and social service professional organisations (Fulmer et al. 2004). Many authors have argued that protocols may be useful to ensure responses to suspected cases of elder abuse are consistent, highlighting key steps in the process (O’Loughlin and Duggan 1998, Lachs and Pillemer 2004, Saliga et al. 2004). Furthermore, standardised processes may be especially helpful in clarifying roles, responsibilities and accountability when there are multiple services and agencies involved in handling elder abuse cases (Anetzberger 2001). However, it has been reported that when practioners are faced with complex ethical dilemmas, they do necessarily follow procedural guidelines but tend to act on their professional assessment (Killick and Taylor 2011).
An important point raised by the participants, during their discussion of the need for greater standardisation and consistency in practice, was their caution to safeguard some existing informal procedures. While the need for increased standardisation across the service was identified as a key area for future capacity development, it was tempered by the recognition of the danger of increased bureaucratisation on effective informal relationships. Of particular concern to the senior case workers was the need to guarantee the interagency relationships that they had established with relevant professional organisations over time. They argued that imposing mandatory reporting and bureaucratic regulation of these relationships may damage existing informal lines of communication. This caution is echoed in research which recognised that structured and standardised protocols may be overly simplistic to deal with the complexity surrounding many cases of elder abuse (O’Loughlin and Duggan 1998, Lachs and Pillemer 2004). In light of this caution, a key finding of this report is the need for flexibility in the design of a standardised response to elder abuse to allow for the professional judgement of the case worker responsible for establishing the protective plans.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 71
Chapter 7 Discussion
7.5.3 Legislative and Statutory Implementation
Emerging from the participants’ evaluation of the legal and policy context which informed their practice was their identification of the ‘legal void’ in which they operated to protect vulnerable older people. This void concerned the legislative protection of older people as well as the legal authority of the senior case worker to act effectively to protect older people from abuse. International research has pointed to inadequate protective legislation for the protection and defence of older people experiencing abuse. Dyer et al. (2005) found that legal interventions are used in a small minority of cases in the United States. Furthermore, some researchers have found legal interventions to be restrictive, often deriving from domestic violence models which do not account for the dependency relationship that may exist between the perpetrator of elder abuse and the older victim (Bonnie and Wallace 2003, Dyer et al. 2005, Wolfe 2003, Pillemer et al. 2007).
The deficit of adequate protective legislation for older people, vulnerable to abuse, was identified by the senior case workers interviewed for this study. This was particularly relevant in cases where the older person’s capacity status increased their vulnerability to financial abuse and exploitation. A key aspect of this finding was the identification of the need for better regulation of solicitors and care professionals, which would assist the case workers in their role of protecting older people from abuse. Mental capacity legislation emerged from the literature as particularly pertinent in protecting older people from abuse, especially in terms of financial exploitation (Nerenberg 2006). The senior case workers spoke about the need for enhanced capacity legislation in Ireland. The Mental Capacity Act 2005, which applies to England and Wales, was cited by them as a model for this legislation and in particular the introduction of a criminal offence of neglect. The law on mental capacity in Ireland is currently being updated and a new Mental Capacity Bill is soon due to be published. The proposed Mental Capacity Bill will be based on a set of guiding principles including a presumption of capacity unless otherwise established. This will give older people greater control over making decisions that affect them and their lives (Lyons et al. 2009).
The participants also called for greater statutory powers for their role, which would increase their authority to act.
Many argued that their role required greater legislative authority in order to realise effective protective interventions. Direct access to key protective services, as well as greater authority in interagency working, were identified as potential benefits of increased statutory authority for the role. However, the complexity of this issue was highlighted in the participants’ discussion of the need to safeguard an individual’s right to self-determination. This indicated their commitment to the doctrine of self-determination, which underpins best practice in social work (Regehr and Antle 1997). While legal guardianship has traditionally involved the permanent removal of a person’s right to make their own decisions (Dyer et al. 2005), there is an increasing trend internationally towards legislative reform to empower vulnerable adults to remain at the centre of decision-making as much as possible (Heath and Phair 2007, Donovan and Regehr 2010). Greater statutory power and authority for the role of the senior case worker, therefore, must be tempered with a need to respect the client’s right to self-determination.
7.6 LimitationsThe focus of this study was on generating valid and reliable evidence with which to describe the experiences of senior case workers in managing cases of elder abuse. A qualitative design involving in-depth semi-structured interviews was the chosen method to generate this evidence. This type of design has inherent limitations that relate to its capacity to examine pre-determined constructs related to the topic of concern and to offer empirical data from which generalisations can be made. While the use of purposive sampling increased the reliability and validity of the qualitative data, the findings cannot be generalised to populations of senior case workers beyond the immediate study sample.
The aim of the study was to explore the experience of managing cases of elder abuse from the perspective of senior case workers. This required in-depth interviews, which ultimately relied on participant self-reports. It is recognised that self-reports of experiences and practices are inherently limited in that they can give rise to issues of the validity of reports and causal conclusions. In addition, many participants’ may have tempered their reports of experiences with the need to maintain confidentiality in relation to particularly sensitive cases.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience72
Chapter 8 Conclusion and Recommendations
8.1 ConclusionThe literature has revealed that the management of elder abuse often involves difficult cases with many ethical challenges and complex dynamics involving the older person, the perpetrator, the practitioner and the service provider. Through a qualitative descriptive research design, this study explored the complexity and challenges of the processes involved in managing cases of elder abuse from the perspective of 18 senior case workers in Ireland.
Interview data contained senior case workers’ reflections on their current practices in relation to elder abuse case management. These reflections indicated that the causes, characteristics and outcomes of elder abuse are multi-dimensional and complex. This complexity was manifested in the interlocking forms of abuse and the fluid boundaries between the types of abuse encountered in protective case management. The complexity of the protection plans implemented by the study participants reflected best practice advocated by international research. These plans integrated multiple protective pathways to available supports and services and were tailored towards the needs and direction of their clients. Furthermore, while presenting some difficulties, a multi-disciplinary team approach to the management of elder abuse emerged from the study data as crucial for the delivery of a holistic protective service, in terms of assessment, intervention, prognosis and case monitoring.
The complex and multifaceted nature of elder abuse constitutes a challenge in managing elder abuse. The need to balance client self-determination against risk was found to present an ethical challenge to decision-making with regard to case closure and client advocacy. This challenge was particularly pertinent to a discussion of capacity assessment. Crucial to effective management of elder abuse is ready access to appropriate advice and skills for assessing and determining capacity. Inter-disciplinary barriers to accessing capacity assessment services represented an acute challenge to protective practice. This challenge was related to the different disciplinary approaches in which the elder abuse protective services are situated. The differing discursive approaches represented by the medical and social work models were a challenge to effective interagency
communication as well as the negotiation of role boundaries and responsibilities.
Structural barriers, such as a limited access to clinical supervision and access to protective services and resources, were a challenge to senior case workers’ decision-making and effective protection practice. In their delivery of a protective service to older people vulnerable to abuse, the current strategies and practices adopted by the senior case workers centred on identifying best practice from their perspective. The experiences of the participants reported in this study are not peculiar to the Irish context but, as reflected in Chapters 2 and 7 these experiences are also reported in a number of countries where elder abuse is being addressed. They highlight the unique challenges presented when working to manage elder abuse.
8.2 RecommendationsThe senior case workers’ reports of their practice in light of the challenges and dilemmas faced by them in managing cases of elder abuse suggest a number of recommendations. Arising from the study data, these recommendations are targeted at augmenting the existing service for the protection of older people in Ireland. The following recommendations are offered within the limitations of this study.
Recommendations for assessing risk and preventing elder abuse
• Low self-esteem is a risk factor for elder abuse (Podnieks 2006). The study findings highlighted senior case workers’ views of the importance of building self-esteem among older people and draws attention to the importance of enhancing older people’s psychological resources, both to prevent and to cope with the experience of abuse. It is recommended that targeted interventions for promoting older people’s self-esteem and enhancing their own psychological resources be further explored.
• Social isolation was highlighted by the senior case workers as a factor in elder abuse, due to the dependency it created and social isolation has also been identified in the literature as a risk factor for abuse. In addition, as a result of interventions to remove older people from
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 73
Chapter 8 Conclusion and Recommendations
abusive situations, older people may experience loneliness and social isolation (Lafferty et al. forthcoming). Community-based support groups can counteract social isolation, relieve carer burden, and decrease dependency of older people (Podnieks 1999, Hightower et al. 2006, Dong and Simon 2008). It is recommended that when assessing risk of elder abuse, the social networks of older people should continue to be examined and efforts to secure a supportive social network be considered as part of the management of cases of elder abuse.
Recommendations for managing cases of elder abuse
• SCWs drew attention to a need for greater statutory powers for their role, which would increase their authority to act. However, elsewhere, legal interventions are infrequently used as a model of case management (Dyer et al. 2005), can be restrictive and can fail to account for the relationships of dependency that may exist between the perpetrator of abuse and the abused person (Bonnie and Wallace 2003, Dyer et al. 2005, Wolfe 2003, Pillemer et al. 2007). SCWs also suggested the need for better regulation of solicitors and care professionals to assist them in their role of protecting older people from abuse and the need for enhanced capacity legislation in Ireland. It is recommended that any increase in the statutory power and authority for the role of the senior case worker or other proposed legislative changes be tempered with a need to respect the older person’s right to self-determination.
• Balancing the professional imperative to implement protective interventions with a client’s right to self-determination was experienced by SCWs as a challenge to successful case resolution. Multi-disciplinary teams and effective interagency working were considered critical to overcoming these challenges. Research elsewhere has referred to the importance of a multi-disciplinary approach for elder abuse case management (Anetzberger et al. 2005, Penhale 2008). It is recommended that a multi-disciplinary approach and interagency working should continue to be promoted and that ways to
formalise existing inter-professional communications and effective interagency and multi-disciplinary working be considered.
• Access to care services was among the repertoire of interventions used by SCWs in managing cases of elder abuse; however they reported experiencing inconsistent access to care services such as respite services, home-help and other resources. As these various services form part of the intervention response of SCWs in managing cases of elder abuse, it is recommended that senior case workers’ access to and use of these services as a form of intervention be monitored.
• The study findings indicated that no single model was appropriate for managing cases of abuse and protecting older people, since each case of elder abuse was different and required a unique response. The practice of protecting older people is located within particular legal, ethical and social contexts, which inform interventions and outcomes. Complexity in case management is also acknowledged in the literature. It is recommended that caution be applied in drawing on a single case management model and that flexibility in the use of models for managing cases of elder abuse should be considered, so that a chosen model is capable of addressing the complexity that inheres in individual cases of elder abuse.
Recommendations for supporting SCWs in their role
• In light of a perceived absence of recognised policy guidelines for their case management practices, SCWs highlighted a need for consistency across the elder abuse service. They highlighted a need for policy guidelines that would address their current practice and thereby reduce their sense of vulnerability to legal scrutiny of their practice. Procedures for the referral and documentation of cases and the recording of case statistics were identified by them as key areas requiring greater standardisation and consistency. It is recommended that current policy guidelines for the SCW role be evaluated, with the aim of ensuring that the SCW practice role is supported by clear guidelines that give direction, but also
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience74
Chapter 8 Conclusion and Recommendations
take into account the need for flexibility and the retention of existing informal procedures that are effective in managing cases of elder abuse.
• The study findings indicated that a reported increase in cases of elder abuse, coupled with finite resources for their management represent a challenge for SCWs in their service delivery. Risk assessment and prioritisation were adopted as strategies to manage cases of elder abuse; however senior case workers experienced a lack of structural supports, including administrative support and other social or healthcare resources. Research points to the impact of caseload size and resources on case management (Jogerst et al. 2001, Cambridge and Parkes 2004). It is recommended that resources to support SCWs’ case management be further explored.
• The study findings indicated that SCWs perceived a lack of peer support associated with geographical and work factors and an absence of clinical supervision as representing a challenge to the practice of elder abuse case management. It is suggested that access to clinical guidance and supervision from professional colleagues and to specialist advice are key to successful protective service delivery (Cambridge and Parkes 2004, Pritchard 2000). It is recommended that issues of clinical supervision and peer support for SCWs in their role be further explored.
• The SCWs drew attention to a need for ongoing training for their role, given the multifaceted and complex nature of elder abuse and the challenges experienced in managing clients’ needs in the face of this complexity. It is recommended that the training needs of SCWs be reviewed on a regular basis and consideration be given to the provision of appropriate training opportunities.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 75
References
Action on Elder Abuse (2004) Hidden voices: Older people’s experience of abuse – An analysis of calls to the Action on Elder Abuse helpline. Action on Elder Abuse, London.
Alberta Elder Abuse Awareness Network (2009) Getting Help: Calgary. Available online at: http://www.albertaelderabuse.ca/page.cfm?pgID=36 (Accessed: 21 September 2009).
Anetzberger, G.J. (2001) Elder abuse identification and referral: The importance of screening tools and referral protocols. Journal of Elder Abuse and Neglect, 13(2), 3–22.
Anetzberger, G.J. (2004) Clinical management of elder abuse: General considerations. Clinical Gerontologist. Special Issue: The Clinical Management of Elder Abuse, 28, 27–41.
Anetzberger, G.J., Dayton C. and McMonagle, P. (1997). A community dialogue series on ethics and elder abuse: Guidelines for decision-making. Journal of Elder Abuse and Neglect, 9(1), 33–50.
Anetzberger, G.J., Dayton, C., Miller, C.A., McGreevey, J.F. and Schimer, M. (2005) Multi-disciplinary teams in the clinical management of elder abuse. Clinical Gerontologist, 28(1/2), 157–171.
Baker, M.W. and Heitkemper, M.M. (2005) The roles of nurses on interprofessional teams to combat elder mistreatment. Nursing Outlook, 53, 253–259.
Beaulieu, M. and Leclerc, N. (2006) Ethical and psychosocial issues raised by the practice in cases of mistreatment of older adults. Journal of Gerontological Social Work, 46(3/4), 161–186.
Bergeron L. (1999) Decision-making and adult protective services workers: Identifying critical factors. Journal of Elder Abuse and Neglect, 10(3/4), 87–113.
Bonnie, R.J. and Wallace, R.B. (2003) Elder mistreatment: Abuse, neglect and exploitation in an aging America. National Research Council, Washington D.C.
Braun, V. and Clarke, V. (2006) Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101.
Brownell, P. (2010) Social issues and social policy response to abuse and neglect of older adults. In Gutman, G. and Spencer C. (eds) Aging, Ageism and Abuse: Moving from Awareness to Action. Elsevier, London, pp 1–15.
Brownell, P. and Heiser, D. (2006) Psycho-educational support groups for older women victims of family mistreatment: A pilot study. Journal of Gerontological Social Work, 46, 145–160.
Brownell, P. and Wolden, A. (2002) Elder abuse intervention strategies: Social service or criminal justice? Journal of Gerontological Social Work, 40(1–2), 83–100.
Bryman, A. (2008) Social research methods (3rd ed). Oxford University Press, Oxford.
Burston, G.R. (1975) Granny Battering. British Medical Journal, 3(6), 592.
Cambridge ,P. and Parkes, T. (2004a) The case for case management in adult protection. Journal of Adult Protection, 6(2), 4–14.
Cambridge, P. and Parkes, T. (2004b) Good enough decision-making? Improving decision-making in adult protection. Social Work Education, 23(6), 711–729.
Canadian Association of Social Workers (CASW) (2005) Code of ethics. Canadian Association of Social Workers, Ottawa.
Comhairle (2003) Advocacy is also for older people. Speaking Up for Advocacy, 1(1). Available online at: http://www.citizensinformationboard.ie/publications/social/downloads/speaking_up_for_advocacy_issue1.pdf (Accessed: 21 September 2009).
Cooper, C., Maxmin, K., Selwood, A., Blanchard, M. and Livingston, G. (2009) The sensitivity and specificity of the modified conflict tactics scale for detecting clinically significant elder abuse. International Psychogeriatrics, 21, 774–778.
Cork Independent (2009) Dervil Dunne - Director of Westgate counselling services and SOS. Available online at: http://archive.corkindependent.com/profiles/profiles/dervil-dunne-%11-director-of-westgate-counselling-services-and-sos-/ (Accessed: 10 October 2010).
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience76
References
Cosc (2010) National strategy on domestic, sexual and gender-based violence 2010-2014. The Stationary Office, Dublin.
Cripps, D. (2001) Rights focused advocacy and elder abuse. Australasian Journal on Ageing, 20(1), 17–23.
Daly, J.M. and Jogerst, G.J. (2005) Definitions and indicators of elder abuse: A Delphi survey of APS caseworkers. Journal of Elder Abuse and Neglect, 17(1), 1–19.
Davis, R.C., Medina, J. and Avitabile, N. (2001) Reducing repeat incidents of elder abuse: Results of a randomized experiment: Final report. Research report submitted to U.S. Department of Justice. Available online at: http://www.ncjrs.gov/pdffiles1/nij/grants/189086.pdf (Accessed: 12 August 2009).
Davis, R.C. and Medina-Ariza, J. (2001) Results from an elder abuse prevention experiment in New York City. In National Institute of Justice research in brief (pp. 1-7). Available online at: http://www.ncjrs.gov/pdffiles1/nij/188675.pdf (Accessed: 12 August 2009).
Dayton, C. (2005) Elder abuse: The social worker’s perspective. Clinical Gerontologist, 28(1-2), 135–155.
Department of Health (DoH) (2000) No secrets: guidance on developing and implementing multi-agency policies and procedures to protect vulnerable adults from abuse. Department of Health, London.
Department of Health (DoH) (2010) Written ministerial statement. Government response to the consultation on safeguarding adults: the review of the no secrets guidance. Tuesday 19 January 2009. Available online at: http://www.dh.gov.uk/en/Consultations/Responsestoconsultations/DH_111286 (Accessed: 7 May 2010).
Desmarais, S.L. and Reeves, K.A. (2007) Gray, black, and blue: The state of research and intervention for intimate partner abuse among elders. Behavioral Sciences and the Law, 25, 377–391.
Dong, X. and Simon, M.A. (2008) Is greater social support a protective factor against elder mistreatment? Gerontology, 54, 381–388.
Donovan, K. and Regehr, C. (2010) Elder abuse: clinical, ethical, and legal considerations in social work practice. Journal of Clinical Social Work, 38, 174–182.
Dooley, A. (2007) Finglas volunteer advocacy programme. Age Action Ireland Conference: Empowering Older People – Best Practice in North Dublin, April 2007. Available online at: http://www.ageaction.ie/userfiles/file/finglas-vol-advocacy-prog.pdf (Accessed: 21 September 2009).
Douglass H. (2005) The development of practice theory in adult protection intervention: insights from a recent research project. The Journal of Adult Protection, 7(1), 32–45.
Dyer, C.B., Heisler, C.J., Hill, C.A. and Kim, L.C. (2005) Community approaches to elder abuse. Clinics in Geriatric Medicine, 21(2), 429–447.
Edmond, E. (2007) Dementia rights advocacy project north Dublin. Age Action Ireland Conference: Empowering Older People – Best Practice in North Dublin, April 2007. Available online at: http://www.ageaction.ie/userfiles/file/dementia-rights.pdf (Accessed: 21 September 2009).
Filinson, R. (1993) An evaluation of a program of volunteer advocates for elder abuse victims. Journal of Elder Abuse and Neglect, 5(1), 77–93.
Filinson, R. (2006) “No Secrets” and beyond: recent elder abuse policy in England. Journal of Elder Abuse and Neglect, 18(1), 1–18.
Fitzgerald, G. (2006) The realities of elder abuse. In Wahidin A. and Cain M. (eds), Ageing, Crime and Society. Willan Publishing, US, pp.90–106.
Fulmer, T., Firpo, A., Guadagno, L., Easter, T.M., Kahan, F. and Paris, B. (2003) Themes from a grounded theory analysis of elder neglect assessment by experts. The Gerontologist, 43(5), 745–752.
Fulmer, T., Guadagno, L., Dyer, C.B. and Connolly, M.T. (2004) Progress in elder abuse screening and assessment instruments. Journal of the American Geriatrics Society, 52, 297–304.
Fulmer, T., Paveza, G., Vende Weerd, C., Guadagno, L., Fairchild, S., Norman, R., Abraham, A. and Bolton-Blatt, M. (2005) Neglect assessment in urban emergency
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 77
References
departments and confirmations by an expert clinical team. Journal of Gerontology, 60(8), 1002–1006.
Geroff, A.J. and Olshaker, J.S. (2006) Elder abuse. Emergency Medicine Clinics of North America, 24, 491.
Groh, A. (2005) Restorative justice: A healing approach to elder abuse. 6th International Conference on Restorative Justice, June 2003. Available online at: http://www.sfu.ca/cfrj/fulltext/groh.pdf (Accessed: 21 September 2009).
Halphen, J.M., Varas, G.M. and Sadowsky, J.M. (2009) Recognizing and reporting elder abuse and neglect. Geriatrics, 64, 13–18.
Health Information and Quality Authority (HIQA) (2009) Protected Disclosure. Available online at: http://www.hiqa.ie/protected_disclosure.asp (Accessed: 7 July 2009)
Health Service Executive (HSE) (2009) Open Your Eyes: HSE Elder Abuse Service Developments 2008. Health Service Executive, Dublin.
Health Service Executive (HSE) (2010) Open Your Eyes: HSE Elder Abuse Service Developments 2009. Health Service Executive, Dublin.
Health Service Executive (HSE) (2011) Open Your Eyes: HSE Elder Abuse Service Developments 2010. Health Service Executive, Dublin.
Heath, H. and Phair, L. (2007) Emerging agendas. Nursing Older People, 19, 16–17.
Hepworth, D.H., Rooney, R.H., Rooney, G., Strom-Gottfried, K. and Larsen, J. (2010) Direct social work practice: Theories and skills (8th ed). Brooks/Cole Cengage Learning, CA.
Hightower, J., Smith, M.J. and Hightower, H.C. (2006) Hearing the voices of abused older women. Journal of Gerontological Social Work, 46, 205–227.
House of Commons Health Select Committee (2004) Elder abuse: Second report of session 2003-4 Volume 1. The Stationery Office, London.
Jogerst, G.J., Daly, J.M. and Ingram, J. (2001) National elder abuse questionnaire: Summary of adult protective service investigator responses. Journal of Elder Abuse and Neglect, 13(4), 59–71.
Johns, S and Juklestad, O. (1995) Norway: Developing elder protective services. Social Work in Europe, 2(3), 2–7.
Juklestad, O. (2004) Elderly people at risk: A Norwegian model for community education and response. The Journal of Adult Protection 6(3), 26–33.
Kalaga, H., Kingston, P., Penhale, B. and Andrews, J. (2007) A review of literature on effective interventions that prevent and respond to harm against adults. Scottish Government Social Research, Edinburgh.
Kelly, J.B. and Johnson, M.P. (2008) Differentiation among types of intimate partner violence: research update and implications for intervention. Family Court Review, 46(3), 476–499.
Killick, C. and Taylor, B.J. (2009) Professional decision-making on elder abuse: A systematic review. Journal of Elder Abuse and Neglect, 21, 211–238.
Killick, C. and Taylor B.J. (2011) Judgements of social care professionals on elder abuse referrals: A factorial survey. Available online at: http://eprints.ulster.ac.uk/20841/1/bjsw.bcr109.full.pdf (Accessed: 9 September 2011).
Kurrle, S. (1993) Responding to elder abuse–A follow-up study of interventions and outcomes. Australasian Journal on Ageing, 12(4), 5–9.
Lachs, M.S. and Pillemer, K. (2004) Elder abuse. The Lancet, 364, 1263–1272.
Lafferty A., Treacy M.P., Fealy G., Phelan A. and Lyons I. (forthcoming) Older people’s experiences of mistreatment and abuse. National Centre for the Protection of Older People, Dublin.
Lai, S. (2008) Elder abuse and policing issues: A review of the literature. Available online at: http://www.uscont.ca/pdf/elder_abuse_and_policing_issues.pdf (Accessed: 12 March 2009).
Lithwick, M., Beaulieu, M., Gravel, S. and Straka, S.M. (2000) The mistreatment of older adults: Perpetrator-victim relationships and interventions. Journal of Elder Abuse and Neglect, 11(4), 95–112.
Lowndes, G., Darwins, P., Wainer, J., Owada, K. and Michaljcic, T. (2009) Financial abuse of elders: a review of the evidence. Protecting elders’ assets study. Monash University, Australia.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience78
References
Luu, A.D. and Liang, B.A. (2005) Clinical case management: a strategy to coordinate detection, reporting and prosecution of elder abuse. Cornell Journal of Law and Public Policy, 15, 165–196.
Lyons, I., Treacy, M.P., Drennan, J., Quin, S., Phelan, A. et al. (2009) Protection of older people and legislation in Ireland. National Centre for the Protection of Older People (NCPOP), Dublin.
McCreadie, C., Bennett, G. and Tinker, A. (1998) Investigating British general practitioners’ knowledge and experience of elder abuse: Report of a research study in an Inner London Borough. Journal of Elder Abuse and Neglect, 9(3), 23–29.
McCreadie, C., Bennett, G., Gilthorpe, M.S., Houghton, G. and Tinker, A. (2000) Elder abuse: do general practitioners know or care? Journal of the Royal Society of Medicine, 93, 67–71.
McGarry, J. and Simpson, C. (2011) Domestic abuse and older women: exploring the opportunities for service development and care delivery. The Journal of Adult Protection, 13(6), 294–301.
McGivern, Y. (2006) The practice of market and social research (2nd ed). Pearson, Essex.
McKenzie, P. (1999) A community response to abuse of seniors. In Pritchard, J. (ed) Elder abuse work. Jessica Kingsley Publishers, London, pp.425–443.
Moon, A. (2000) Perceptions of elder abuse among various cultural groups: Similarities and differences. Abuse and Neglect of Older People, Summer, 75–80.
Mowlam, A., Tennant, R., Dixon, J., and McCreadie, C. (2007) UK study of abuse and neglect of older people: Qualitative findings. King’s College London and the National Centre for Social Research, London.
Nahmiash, D. and Reis, M. (2000) Most successful intervention strategies for abused older adults. Journal of Elder Abuse and Neglect, 12 (3-4), 53–70.
National Association of Social Workers (NASW) (2008) The National Association of Social Workers: Code of ethics. Available online at: http://www.sp2.upenn.edu/docs/resources/nasw_code_of_ethics.pdf (Accessed: 2 March 2011).
National Committee for the Prevention of Elder Abuse (NCPEA) (2009) Best practice models. Available online at: http://www.preventelderabuse.org/communities/best.html (Accessed: 22 September 2009).
National Council on Ageing and Older People (NCAOP) (1998) The law and older people: a handbook for service providers. National Council on Ageing and Older People, Dublin.
National Council on Ageing and Older People (NCAOP) (2009) Review of the recommendations of Protecting our Future: Report of the working group on elder abuse. National Council on Ageing and Older People, Dublin.
National Research Council (2003) Elder mistreatment: abuse, neglect and exploitation in an aging America. The National Academies Press, Washington D.C.
Naughton, C., Drennan, J., Treacy, M.P., Lafferty, A., Lyons, I., Phelan, A., O’Loughlin, A. and Delaney, L. (2010) Abuse and neglect of older people in Ireland: Report on the national study of elder abuse and neglect. National Centre for the Protection of Older People, Dublin.
Neale, A.V., Hwalek, M.A., Goodrich, C.S. and Quinn, K.M. (1997) Reason for case closure among substantiated reports of elder abuse. The Journal of Applied Gerontology, 16(4), 442–458.
Nerenberg, L. (2006) Communities respond to elder abuse. Journal of Gerontological Social Work, 46, 5–33.
Nerenberg, L. (2008) Elder abuse prevention: emerging trends and promising strategies. Springer Publishing, New York.
O’Keeffe, M., Hills, A., Doyle, M., McCreadie, C., Scholes, S., Constantine, R., Tinker, A., Manthorpe, J., Biggs, S and Erens, B. (2007) UK study of elder abuse and neglect of older people: Prevalence survey report. National Centre for Social Research, London.
O’Loughlin, A. and Duggan, J. (1998) Abuse, neglect and mistreatment of older people: An exploratory study. National Council on Ageing and Older People, Dublin.
Oswald, R.A., Jogerst, C.J., Daly, D.M. and Bentler, S.E. (2004) Iowa family physician’s reporting of elder abuse. Journal of Elder Abuse and Neglect, 16(2), 75–88.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 79
References
Parra-Cardona, J. R.N., Meyer, E., Schiamberg, L. and Post, L. (2007) Elder abuse and neglect in Latino families: An ecological and culturally relevant theoretical framework for clinical practice. Family Process, 46, 451–470.
Penhale, B. (2006) Global developments in elder abuse. In A. Wahidin and M. Cain (eds) Ageing, Crime and Society. Willan Publishing, Cullompton, pp.154–170.
Penhale, B. (2007) Elder abuse in Europe: an overview of recent developments. Journal of Elder Abuse and Neglect, 18(1), 107–116.
Penhale, B. (2008) Elder abuse in the United Kingdom. Journal of Elder Abuse and Neglect, 20(2), 151–168.
Perel-Levin, S. (2008) Discussing screening for elder abuse at primary health care level. World Health Organisation, Geneva.
Peri, K., Fanslow, J., Hand, J. and Parsons, J. (2008) Elder abuse and neglect: Exploration of risk and protective factors. Families Commission, New Zealand.
Pillemer, K.A., Mueller-Johnson, K.U., Mock, S.E., Suitor, J.J. and Lachs, M.S. (2007) Interventions to prevent elder mistreatment. In L.S. Doll, S.E. Bonzo, J.A. Mercy and D.A. Sleet (eds) Handbook of injury and violence prevention. Springer Science and Business Media, New York, pp.241–254.
Ploeg, J., Fear, J., Hutchison, B., Macmillan, H. and Bolan, G. (2009) A systematic review of interventions for elder abuse. Journal of Elder Abuse and Neglect, 21, 187–210.
Podnieks, E. (1999) Support groups: a chance at human connection for abused older adults. In Pritchard, J. (ed) Elder abuse work. Jessica Kingsley Publishers, London, pp.425–443.
Podnieks, E. (2006) Social inclusion: An interplay of the determinants of health-new insights into elder abuse. Journal of Gerontological Social Work, 46, 57–79.
Podnieks, E. (2008) Elder abuse: The Canadian experience. Journal of Elder Abuse and Neglect, 20, 126–150.
Pratt, C.C., Koval, J., and Lloyd, S. (1983) Service workers’ responses to abuse of the elderly. Social Casework, 64, 147–153.
Pritchard, J. (2000) The needs of older women: services for victims of elder abuse. The Policy Press, Bristol.
Pritchard, J. (2007) Working with adult abuse: a training manual for people working with vulnerable adults. Jessica Kingsley Publishers, London.
Reay, M. and Browne, K.D. (2002) The effectiveness of psychological interventions with individuals who physically abuse or neglect their elderly dependents. Journal of Interpersonal Violence, 17(4), 416–431.
Regehr, C., and Antle, B. (1997) Coercive influences: Informed consent in court-mandated social work practice. Social Work, 42(3), 300–306.
Reingold, D.A. (2006) An elder abuse shelter program: build it and they will come, a long term care based program to address elder abuse in the community. Journal of Gerontological Social Work, 46, 123–135.
Rodriguez, M., Wallace, S., Woolf, N., and Mangione, C. (2006) Mandatory reporting of elder abuse: Between a rock and a hard place. Annals of Family Medicine, 4(5), 403–409.
Ross, C. (2007) Detecting and preventing elder abuse. Nursing and Residential Care, 9, 504.
Sacks, D., Das, D., Romanick, R., Caron, M., Morano, C. and Fahs, M.C. (2009) The value of money management: an analysis of outcomes and costs. Brookdale Center for Healthy Aging and Longevity, Hunter College, New York. Available online at: http://www.brookdale.org/research_value_of_dmm.htm (Accessed: 21 September 2009).
Saliga, S., Adamowicz, C., Logue, A. and Smith, K. (2004) Physical therapists’ knowledge of physical elder abuse – signs, symptoms, laws, and facility protocols. Journal of Geriatric Physical Therapy, 27, 3–10.
Schaffer, J. (1999) Older and isolated women and domestic violence project. Journal of Elder Abuse and Neglect, 11(1), 59–78.
Schwiebert, V., Myers, J., and Dice, C. (2000) Ethical guidelines for counsellors working with older adults. Journal of Counselling and Development, 78(2), 123–129.
Scogin, F., Beall, C., Bynum, J., Stephens, G., Grote, N.P., Baumhover, L.A. and Bolland, J.M. (1989) Training for abusive caregivers: An unconventional approach to an
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience80
References
intervention dilemma. Journal of Elder Abuse and Neglect, 1(4), 73–86.
Shibusawa, T., Kodaka, M., Iwano, S. and Kaizu, K. (2005) Interventions for elder abuse and neglect with frail elders in Japan. Brief Treatment and Crisis Intervention, 5(2), 203–211.
Spencer, C. (2005) Harm reduction and abuse in later life. World Conference on Family Violence, Banff.
Stiegel, L. and Klem, E. (2007) Information about laws related to elder abuse. American Bar Association Commission on Law and Aging. Available online at: http://www.ncea.aoa.gov/NCEAroot/Main_Site/Library/Laws/InfoAboutLaws_08_08.aspx (Accessed: 13 July 2009).
Teaster, P.B., Dugar, T.A., Mendiondo, M.S., and Otto, J.M. (2005) The 2004 survey of state adult protective services: abuse of adults 60 years of age and older. National Center on Elder Abuse Washington, DC.
Victoria Government Department of Human Services (2009) With respect to age – 2009: Victorian Government practice guidelines for health service and community agencies for the prevention of elder abuse. Victoria Government Department of Human Services, Melbourne.
Wilson, G. (2004) Dilemmas and ethics: Social work practice in the detection and management of abused older women and men. Journal of Elder Abuse and Neglect, 14(1), 79–94.
Wilson, J. and Micucci, S. (2003) Interventions to prevent the recurrence of elder abuse. Available online at: www.hamilton.ca/PHCS/EPHPP/Research/Full-Reviews/ElderAbuse.pdf (Accessed: 5 September 2010).
Wolfe, D.A. (2003) Elder abuse intervention: Lessons from child abuse and domestic violence initiatives. In R.J. Bonnie and R.B. Wallace (eds) Elder mistreatment: Abuse, neglect and exploitation in an aging America. National Academies Press, Washington, D.C., pp.501–526.
Wolf, R.S. and Pillemer, K. (2000) Elder abuse and case outcome. Journal of Applied Gerontology, 19, 203–220.
Woodcock, R. (2011) Ethical standards in the NASW code of ethics: The explicit legal model, and beyond. Families in Society: The Journal of Contemporary Social Sciences, 92(1), 21–27.
Working Group on Elder Abuse (WGEA) (2002) Protecting Our Future. The Stationery Office, Dublin.
World Health Organization (WHO) (2002) World report on violence and health. World Health Organisation, Geneva.
World Health Organisation (WHO) (2011) European report on preventing elder maltreatment. World Health Organisation, Denmark.
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience 81
Managing Elder Abuse in Ireland: The Senior Case Worker’s Experience82