40
Managing falls in the elderly: real world approach DR PRISCILLA NG
| Date post: | 20-Aug-2018 |
| Category: |
Documents |
| Upload: | nguyenthien |
| View: | 217 times |
| Download: | 0 times |

Managing falls in the
elderly:
real world approachDR PRISCILLA NG

”
“A fall is defined as an event which
results in a person coming to rest
inadvertently on the ground or floor
or other lower level.
FALL: WHO DEFINITION
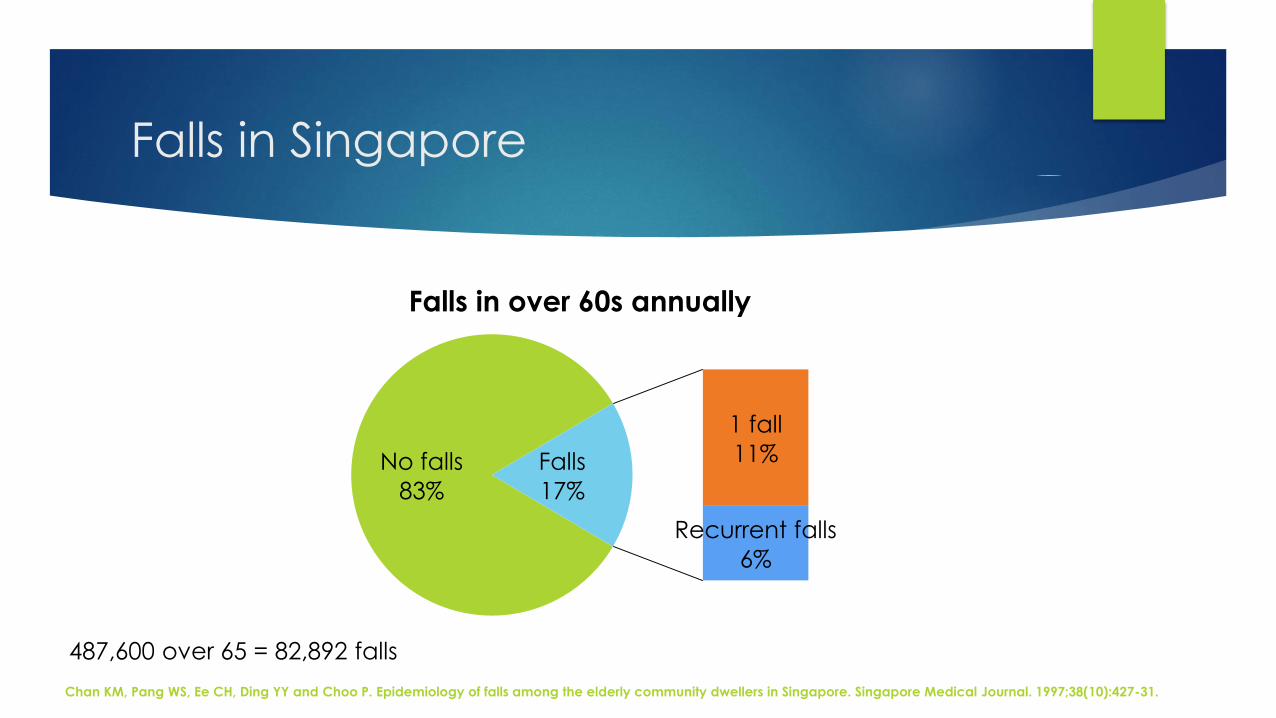
Falls in Singapore
No falls
83%
1 fall
11%
Recurrent falls
6%
Falls
17%
Falls in over 60s annually
487,600 over 65 = 82,892 falls
Chan KM, Pang WS, Ee CH, Ding YY and Choo P. Epidemiology of falls among the elderly community dwellers in Singapore. Singapore Medical Journal. 1997;38(10):427-31.

Sequelae of falls
Fractures
Head injuries
Fear of falling
Loss of mobility
Loss of independence
Institutionalisation
Death
Ambulant
18%
Decreased
ambulation
42%
Functionally
dependent
20%
Death
within 2
years 20%
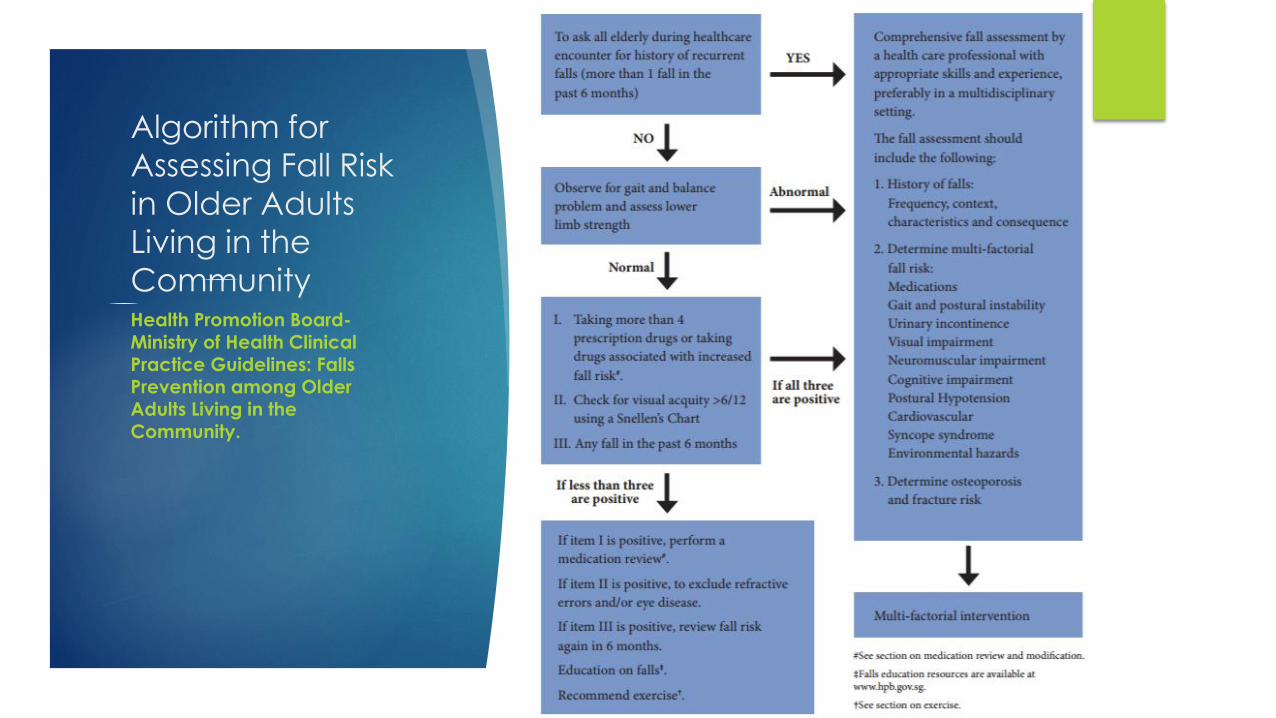
Algorithm for
Assessing Fall Risk
in Older Adults
Living in the
CommunityHealth Promotion Board-
Ministry of Health Clinical Practice Guidelines: Falls Prevention among Older Adults Living in the Community.

Screening

#1: Falls history

#1: Falls history
1. Presenting with a fall
2. More than 1 fall in past year
3. Report gait or balance problems
AGS/BGS Clinical Practice Guideline: Prevention of Falls in Older Persons 2010
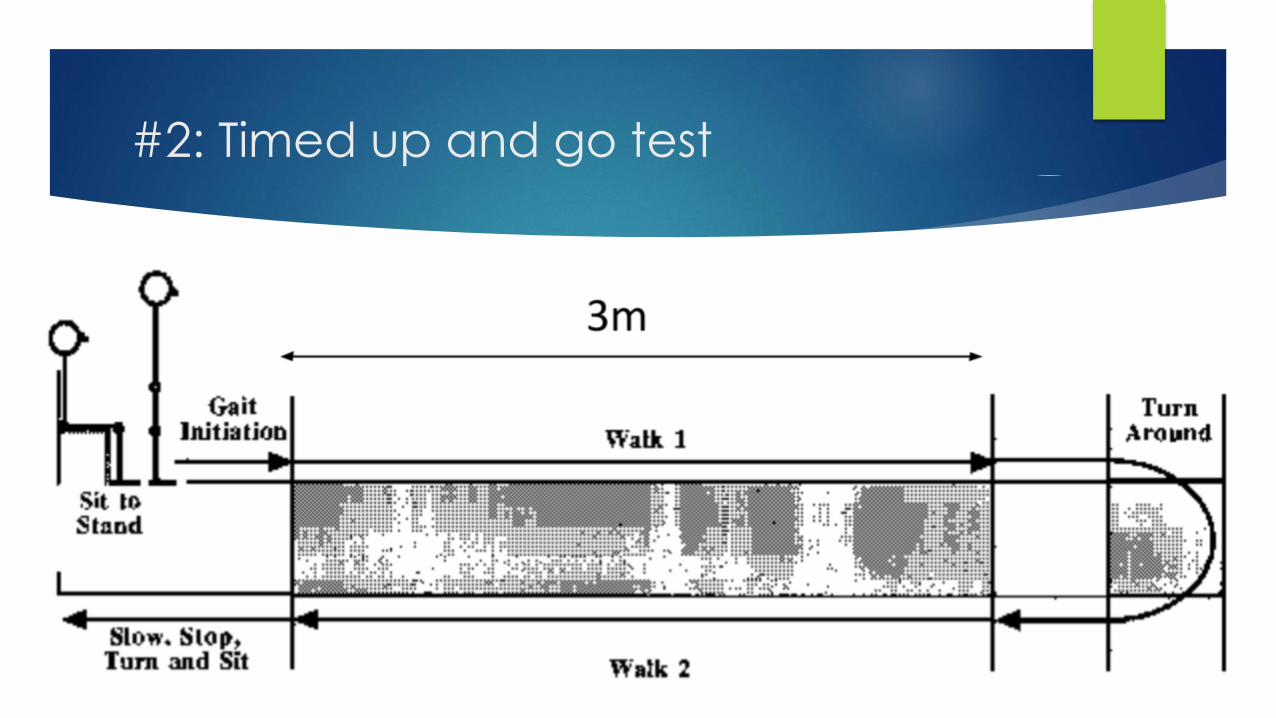
#2: Timed up and go test

Timed up and go test interpretation
< 10 s: freely mobile
< 20 s: mostly
independent
> 30 s: impaired
mobility
Podsiadlo D, Richardson S. The timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142-8.
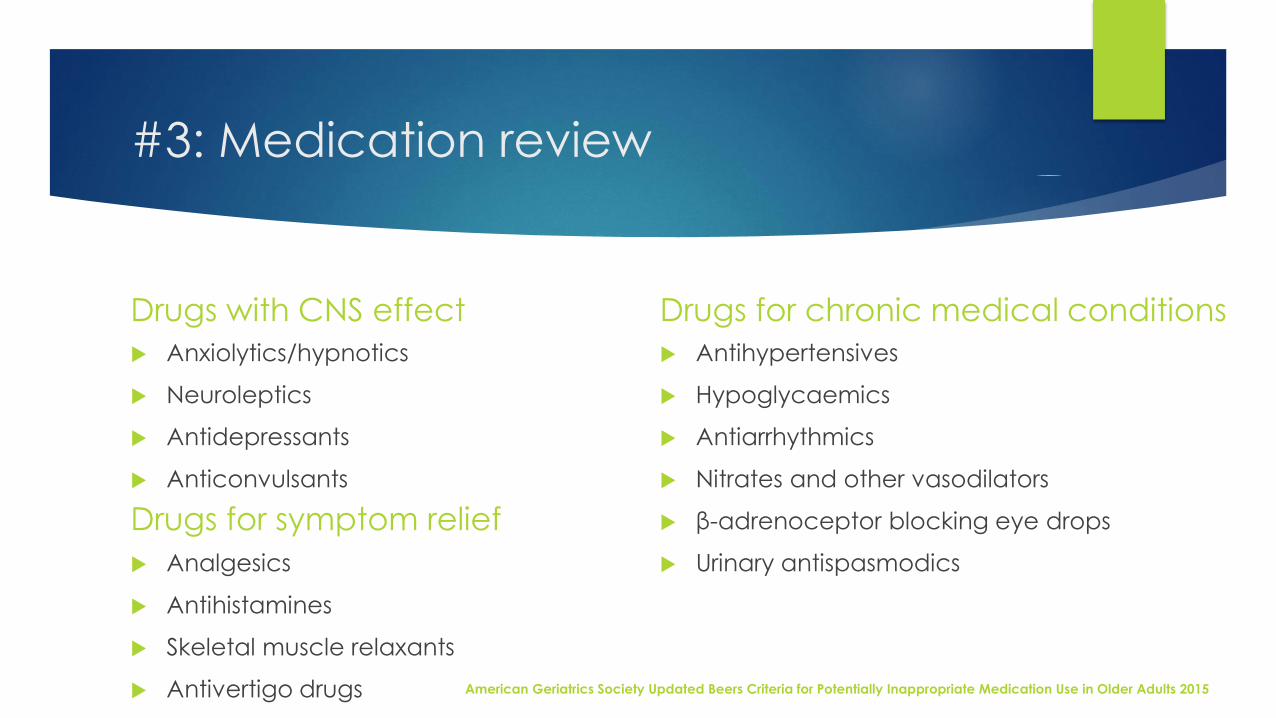
#3: Medication review
Drugs with CNS effect
Anxiolytics/hypnotics
Neuroleptics
Antidepressants
Anticonvulsants
Analgesics
Antihistamines
Skeletal muscle relaxants
Antivertigo drugs
Drugs for chronic medical conditions
Antihypertensives
Hypoglycaemics
Antiarrhythmics
Nitrates and other vasodilators
β-adrenoceptor blocking eye drops
Urinary antispasmodics
Drugs for symptom relief
American Geriatrics Society Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults 2015

#4: Visual acuitySnellen chart

Comprehensive
assessment
1. History
2. Physical examination
3. Functional assessment
4. Environmental assessment
1. History: Anatomy of a fall
ComplicationsFallPrecipitating
factorsPredisposing
factors
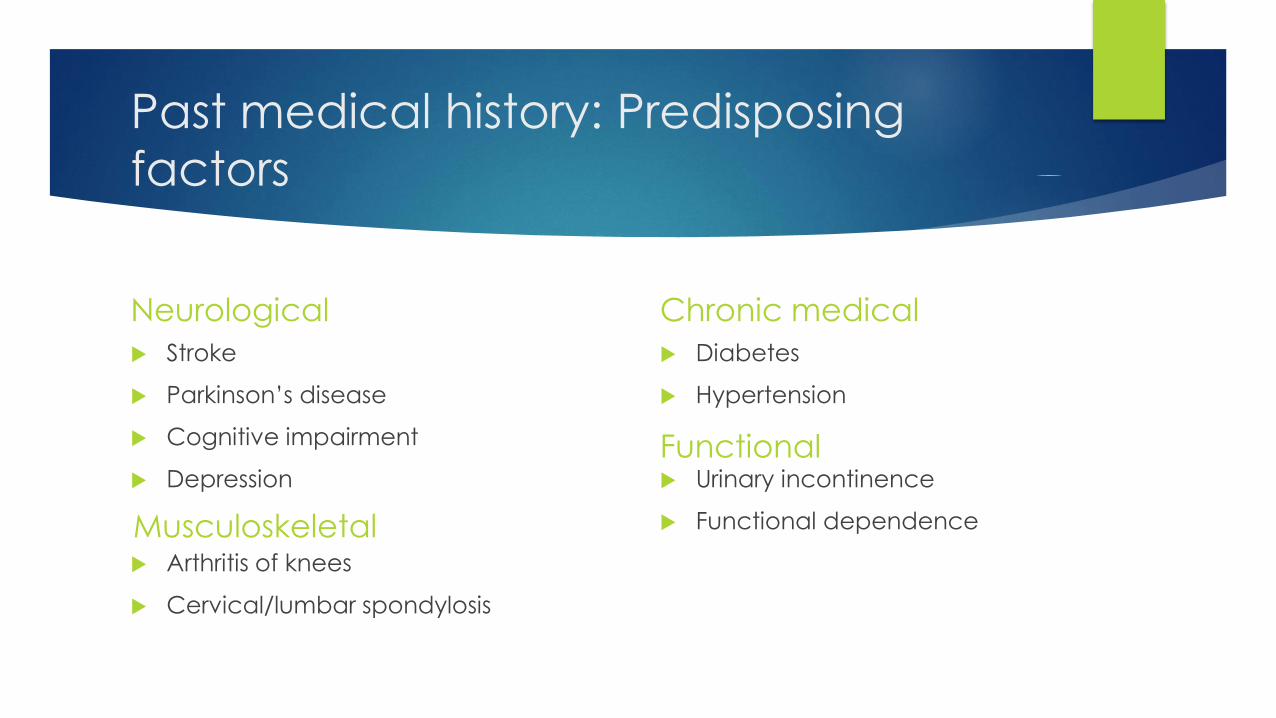
Past medical history: Predisposing
factors
Neurological
Stroke
Parkinson’s disease
Cognitive impairment
Depression
Arthritis of knees
Cervical/lumbar spondylosis
Chronic medical
Diabetes
Hypertension
Urinary incontinence
Functional dependenceMusculoskeletal
Functional
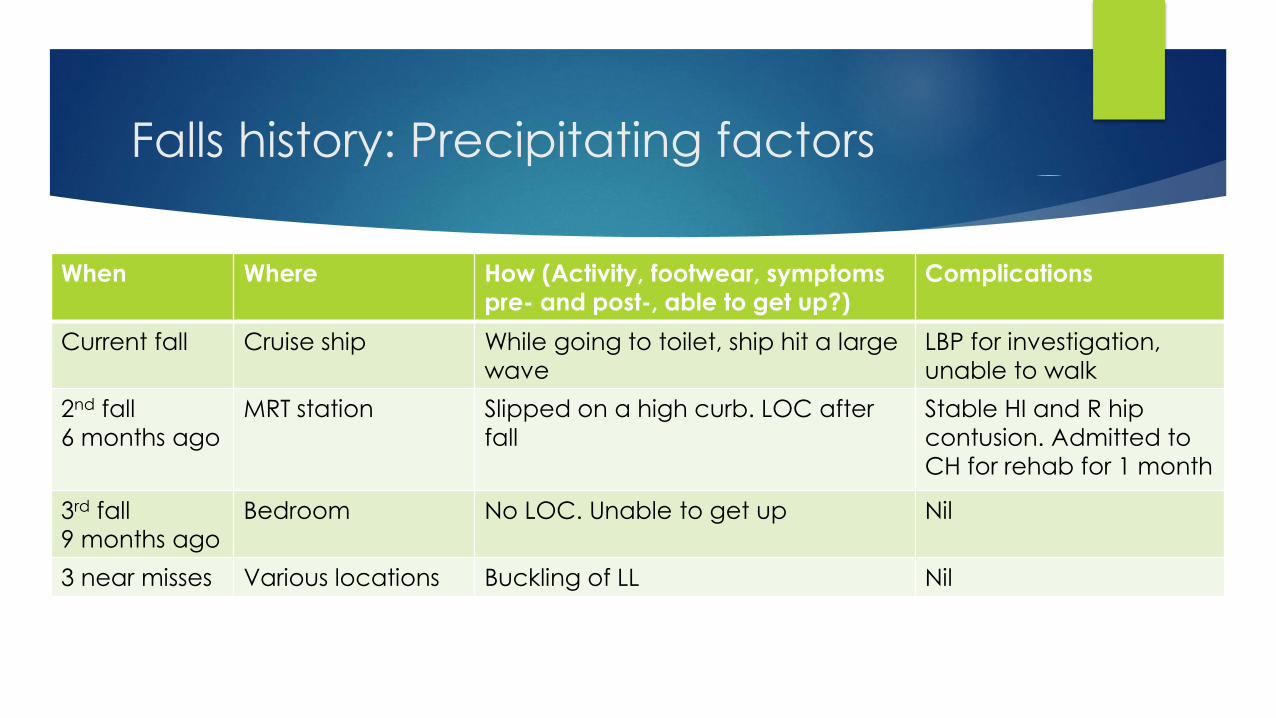
Falls history: Precipitating factors
When Where How (Activity, footwear, symptoms
pre- and post-, able to get up?)
Complications
Current fall Cruise ship While going to toilet, ship hit a large
wave
LBP for investigation,
unable to walk
2nd fall
6 months ago
MRT station Slipped on a high curb. LOC after
fall
Stable HI and R hip
contusion. Admitted to
CH for rehab for 1 month
3rd fall
9 months ago
Bedroom No LOC. Unable to get up Nil
3 near misses Various locations Buckling of LL Nil
”
“Syncope is defined as a transient,
self-limited loss of consciousness with
an inability to maintain postural tone
that is followed by spontaneous
recovery.

2. Physical examinationHigher cortical function:
Cognition, safety awareness,
fear of falls, mood
Neurological: Parkinsonism, stroke,
neuropathy, spinal degeneration,
vestibular disorders, gait
Musculoskeletal: Osteoarthritis,
foot deformities, muscle
weakness
Nutritional status
Frailty
Vision: Cataracts, vision aids
Cardiovascular: Structural heart
disease, arrhythmias, orthostatic
hypotension
Footwear
Walking aids

Risk factors for falls
Intrinsic Age >80 Female Lower extremity weakness Previous falls Gait & balance disorder Visual impairment Depression Functional and cognitive impairment Dizziness Low BMI Urinary incontinence Orthostatic hypotension
Extrinsic
Polypharmacy (> 4 medications)
Psychotropic medications
Environmental hazards e.g. poor lighting, loose carpets, lack of
bathroom safety equipment
Interventions
Single interventions
Multicomponent / multifactorial interventions
• Exercise
• Environment
• Medication
• Medical
• Education

1. Exercise

1. Exercise
Most positive trials consisted of a
programme > 12 weeks, 1-3 times per
week, up to 90 minutes
16% reduction in falls
NNT 16
Balance
Gait
Strength
Tai Chi
Chang JT et al. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ. 2004 Mar 20;328(7441):680.

2. Enviroment

Enhancement For Active Seniors (EASE)
www.hdb.gov.sg/EASE-Application
8 or 10 grab bars for first
toilet and within flat,
and 6 grab bars for second toilet
Slip-resistant treatment
to existing floor tiles of 2 bathrooms/ toilets
Up to 5 ramps within
flat to negotiate one
level difference in the
flat and/ or at single-step main entrance

Enhancement For Active Seniors (EASE)
An elderly member in the household is 65 years old and above
An elderly member in the household aged between 60 and 64 years
requires assistance for one or more of the Activities of Daily Living (ADL)
Functional Assessment Report required
Singapore Citizen Households
Flat type 1-/ 2-/ 3-Room 4-Room 5-Room ExecutiveYou pay $125 (5%) $187.50 (7.5%) $250 (10%) $312.50
(12.5%)Government pays
$2,375 (95%) $2,312.50 (92.5%)
$2,250 (90%) $2,187.50 (87.5%)

Footwear
No loose laces
Wide toe box
Low heel Slip-resistant sole
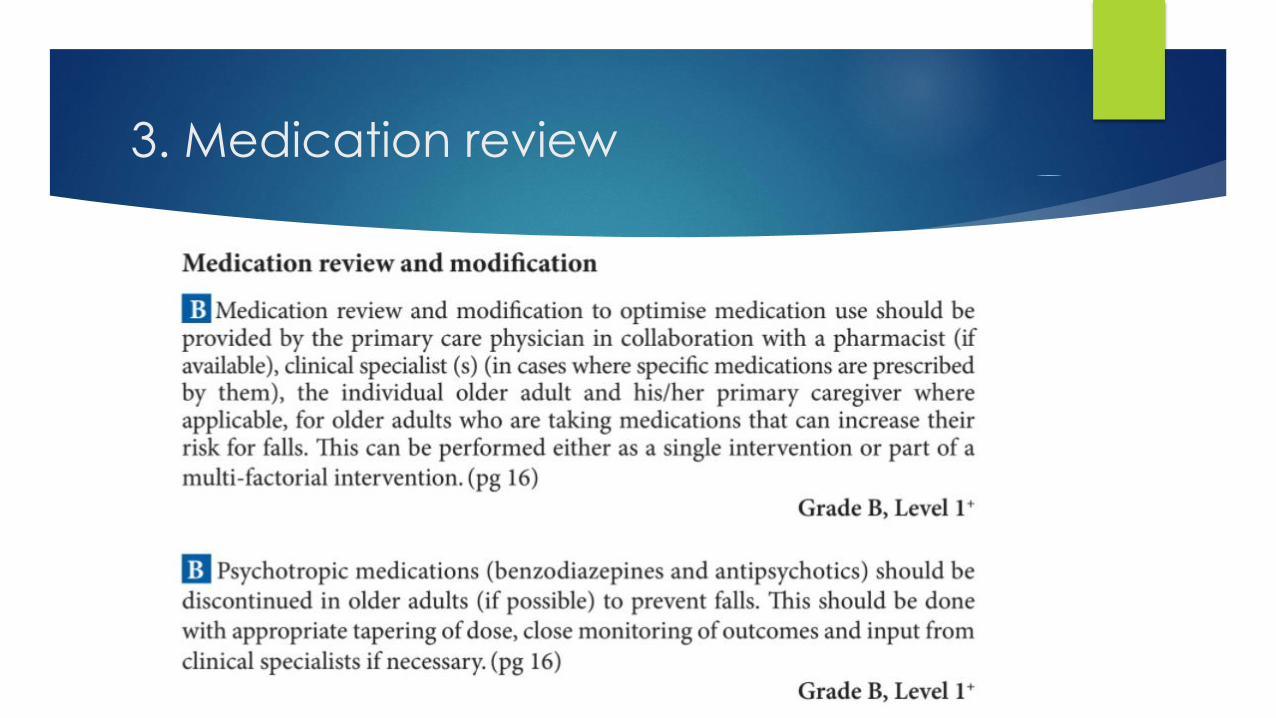
3. Medication review
4. Medical interventions

Postural hypotension
Non-pharmacological
Slow rising
Ankle pumps
Adequate fluid intake
Elevate head of bed 20 degrees
TED stockings
Pharmacological
Fludrocortisone 0.05 -0.3 mg/day
Midodrine 2.5-10 mg tds
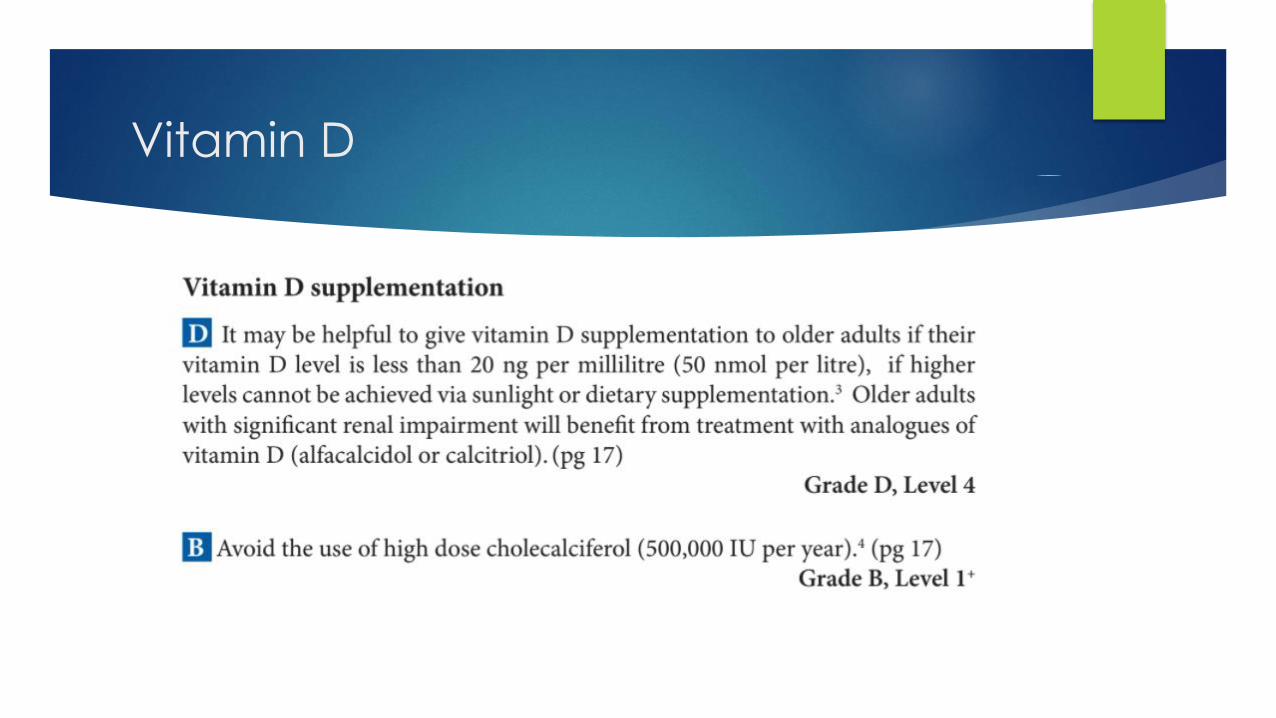
Vitamin D

Vision

Pacemaker
5. Education

Multifactorial interventions
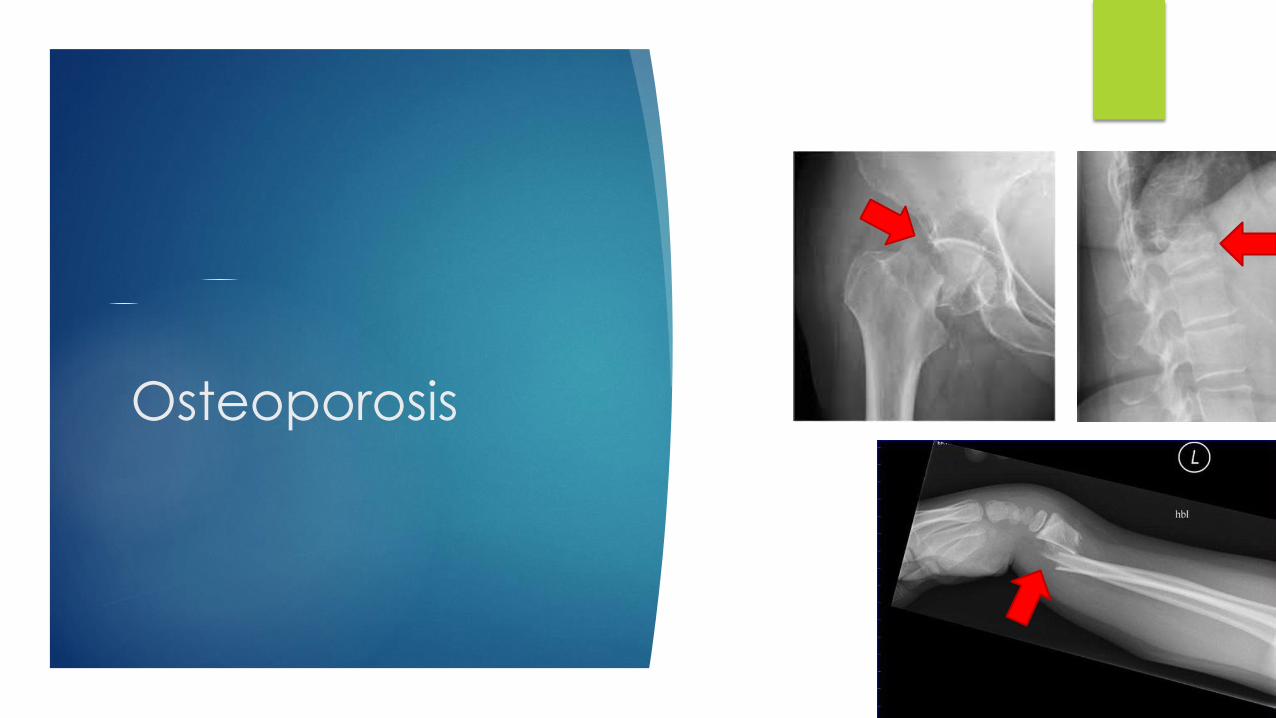
Osteoporosis

FRAX WHO Fracture
Risk Assessment Toolhttp://www.shef.ac.uk/FRAX/tool.jsp

When to treat?
BMD T-score Interpretation Management
<-2.5 + fracture Severe/established osteoporosis Treat
<-2.5 Osteoporosis Treat
-1 to -2.5 Osteopenia Treat if high risk
>3%>20%Vertebral, forearm,
humerus + hip
Treatment
Pharmacotherapy
Bisphosphonates
Oral: alendronate 70 mg, risedronate
35 mg weekly
IV: zoledronic acid 5 mg yearly
Denosumab: SC 60 mg 6-monthly
Supplements
Calcium: 1200mg/day
Vitamin D: 800 IU/day

Considerations regarding
bisphosphonate therapy
Indications
Functional mobility
Lifespan
Dysphagia/NGT/GERD
Inability to sit up
Renal impairment (CrCl <30)
Adverse effects
Oesophagitis
Osteonecrosis of jaw
Atypical femoral #
Bone/joint/muscle pain
?AF
Contraindications

Thank you

















