1 Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage M. Karoshi, J. M. Palacios-Jaraquemada and L. G. Keith INTRODUCTION Treatment of postpartum hemorrhage (PPH) is never simple, and many paradigms have been presented for consideration over the past several years. Most advo- cate straightforward approaches directed toward a spe- cific cause of PPH. Rarely have authors put forward a series of treatment plans in the same document that describe treatment related to a variety of causes. The impetus to prepare this chapter derives from a thor- ough review of published data relating to specific deaths from PPH as described in the Confidential Enquires of the UK 1 , Australia 2 and Canada 3 . Ameri- can data 4 , in contrast, are mostly descriptive and contain statistical elements relating to maternal deaths without individual case analyses. The recurring theme of these reports is quite simple: TOO LITTLE, TOO LATE. Because PPH is episodic in nature and almost always unexpected, birth attendants are not prepared to deal with it on a regular and recurring basis. This is especially true if the PPH appears at night, on weekends, or on holidays, or if the care provider is alone in the delivery unit at the time of its occurrence and is unwilling or unable to seek competent help in a timely manner or if such help is unavailable. Figure 1 (also shown in Chapter 20 by Gangopadhyay et al.) shows a 25-year analysis of deaths in the UK reports in which 60–70% of patients received what was described as substandard care. After analysis of existing reports, we selected ten com- mon PPH scenarios which might be seen by an average obstetrician in his or her practice. All invariably commence as simple challenges which, when appropri- ate actions are not taken in a timely manner, may lead to serious morbidity and eventually death. The late Steve Jobs, founder of Apple Computers, was fond of saying that it was extremely difficult to make complex things simple, whereas it was easy to make simple things complex. This statement applies directly to the therapy of PPH because, as the ten sce- narios show, the causes of the PPH vary from simple to complex at their onset, and even simple cases become complex with a very short passage of time. This latter thought was described in various terms by authors in the first edition of this text, but no author made the point illustrated in the following box. The passage of time is likely to increase the com- plexity of any given case because continuous bleed- ing, not appropriately and adequately controlled on a timely basis, invariably leads to coagulopathy. Once coagulopathy sets in, the simplest case takes a different path, as the need to treat coagulopathy complicates any other planned interventions. Thus, one hears of cases in which compression sutures, embolizations, the use of factor VIIa or even hysterec- tomies failed to control PPH. When these cases are analysed retrospectively, however, it becomes clear that the practitioners failed to realize they were attempting to correct bleeding from coagulopathy which had not been recognized or even considered. Seven of the ten scenarios are preceded by an algo- rithm, and study of these algorithms in conjunction with the proposed therapy reinforces the need to progress from one step to the next in a logical manner. These algorithms have been prepared in such a man- ner that the reader understands therapy not only pro- gresses logically, but also does so with one eye on the clock. Stated another way, if medical therapy using three or four uterotonic agents has not worked within 1 hour, there is no logical reason to think that it will work in the next hour. Similarly, if compression sutures are delayed until the onset of coagulopathy, 3 Trinnea 0 20 40 60 80 100 Percentage of total cases Substandard care 1985–87 1988–90 1991–93 1974–96 1997–99 2000–02 2003–05 2006–08 Figure 1 Trends in substandard care (see Chapter 20)
Transcript
1Managing the Ten Most CommonLife-Threatening Scenarios Associated withPostpartum HemorrhageM. Karoshi, J. M. Palacios-Jaraquemada and L. G. Keith
INTRODUCTION
Treatment of postpartum hemorrhage (PPH) is neversimple, and many paradigms have been presented forconsideration over the past several years. Most advo-cate straightforward approaches directed toward a spe-cific cause of PPH. Rarely have authors put forward aseries of treatment plans in the same document thatdescribe treatment related to a variety of causes. Theimpetus to prepare this chapter derives from a thor-ough review of published data relating to specificdeaths from PPH as described in the ConfidentialEnquires of the UK1, Australia2 and Canada3. Ameri-can data4, in contrast, are mostly descriptive andcontain statistical elements relating to maternal deathswithout individual case analyses.
The recurring theme of these reports is quitesimple: TOO LITTLE, TOO LATE. Because PPH isepisodic in nature and almost always unexpected, birthattendants are not prepared to deal with it on a regularand recurring basis. This is especially true if the PPHappears at night, on weekends, or on holidays, or ifthe care provider is alone in the delivery unit at thetime of its occurrence and is unwilling or unable toseek competent help in a timely manner or if suchhelp is unavailable. Figure 1 (also shown in Chapter 20by Gangopadhyay et al.) shows a 25-year analysis ofdeaths in the UK reports in which 60–70% of patientsreceived what was described as substandard care.
After analysis of existing reports, we selected ten com-mon PPH scenarios which might be seen by an averageobstetrician in his or her practice. All invariably
commence as simple challenges which, when appropri-ate actions are not taken in a timely manner, may lead toserious morbidity and eventually death.
The late Steve Jobs, founder of Apple Computers,was fond of saying that it was extremely difficult tomake complex things simple, whereas it was easy tomake simple things complex. This statement appliesdirectly to the therapy of PPH because, as the ten sce-narios show, the causes of the PPH vary from simpleto complex at their onset, and even simple casesbecome complex with a very short passage of time.This latter thought was described in various terms byauthors in the first edition of this text, but no authormade the point illustrated in the following box.
The passage of time is likely to increase the com-plexity of any given case because continuous bleed-ing, not appropriately and adequately controlled ona timely basis, invariably leads to coagulopathy.
Once coagulopathy sets in, the simplest case takesa different path, as the need to treat coagulopathycomplicates any other planned interventions. Thus,one hears of cases in which compression sutures,embolizations, the use of factor VIIa or even hysterec-tomies failed to control PPH. When these cases areanalysed retrospectively, however, it becomes clearthat the practitioners failed to realize they wereattempting to correct bleeding from coagulopathywhich had not been recognized or even considered.
Seven of the ten scenarios are preceded by an algo-rithm, and study of these algorithms in conjunctionwith the proposed therapy reinforces the need toprogress from one step to the next in a logical manner.These algorithms have been prepared in such a man-ner that the reader understands therapy not only pro-gresses logically, but also does so with one eye on theclock. Stated another way, if medical therapy usingthree or four uterotonic agents has not worked within1 hour, there is no logical reason to think that itwill work in the next hour. Similarly, if compressionsutures are delayed until the onset of coagulopathy,
3
Trinnea
020406080
100
Per
cent
age
of to
tal c
ases
Substandard care
1985
–87
1988
–90
1991
–93
1974
–96
1997
–99
2000
–02
2003
–05
2006
–08
Figure 1 Trends in substandard care (see Chapter 20)
there is no reason to think that they will work unlessthe coagulopathy has been treated.
It is our earnest hope that this chapter will providethe practitioner with the realization that one specifictherapy cannot possibly work for all causes of PPH andthat different therapeutic pathways must be chosendepending upon the inherent cause of bleeding. Tothis end, this chapter makes full use of web links, videoclips, illustrations and hyperlinks to other supportingmaterials, these can be accessed through The GlobalLibrary of Women’s Medicine at www.glowm.com.
SCENARIO 1 – VAGINAL DELIVERY AND PPH
The key to appropriate initiation of therapy in thisscenario is to immediately recognize when the patienthas lost more than 500 ml of blood or when the hem-orrhage has begun to compromise vital signs, as mightoccur in a woman who entered labor with a hemoglo-bin of less than 7 g/dl and subsequently loses a mere200 ml of blood.
At the same time, it is important to recognize thatif the woman in the algorithm has had a labor lasting24 hours or more, her blood loss may be from at leasttwo additional causes besides atony, as both genitaltract trauma and associated postlabor dehydrationmay accentuate the severity and rapid deterioration ofclinical parameters.
Because uterine atony is the most logical cause ofbleeding in such cases, the use of uterotonic agentsrepresents an appropriate initial therapeutic pathway.Discussions as to which specific uterotonic agent toadminister and how to do it are found in otherchapters of this book (Section 8). In general oxytocin,Syntocinon®, methergin, prostaglandins and carbe-tocin are used with similar degrees of success insettings that can provide proper storage of these agents.In contrast oral, vaginal and rectal doses of misoprostolare particularly valuable in areas of the world wherestandard oxytocics are not available (see Section 6).
The use of tranexamic acid is well characterized inthe trauma literature, but not well described in theobstetric literature, although anecdotal reports of itswidespread use and success in the treatment of PPHabound. In addition, it is commonly used by cardio-thoracic and hepatobiliary surgeons to control bleed-ing. It does so by stabilizing the clot.
If bleeding continues or even accelerates during theprocess of medical therapy, it is prudent to conduct athorough examination of the vaginal walls and vaultas well as to examine the cervix for tears whilstusing some form of anesthetic. In order to performsuch an examination, it is necessary to have at leastone assistant, suitable equipment and a light sourcethat illuminates the vaginal vault. Whilst this is takingplace, a team member should examine or re-examinethe placenta for the missing cotyledons.
Assuming that no obvious vaginal or cervicaltrauma is recognized and the bleeding continues, anyone of the available uterine balloons should be used(for details see Chapters 46–48 and 54).
If vaginal trauma is found to be the principal causeof the bleeding, practitioners may be confronted withone of three different circumstances. In the first, theremay be one or two tears of the vagina which are ame-nable to simple corrective suturing. If, on the otherhand, tears are of an explosive nature, i.e. multiplesmall tears not amenable to individual suturing, orif sutures pull through the edematous tissue therebycausing more bleeding, it is reasonable to inflate aballoon which compresses the entire vaginal wallthroughout its circumference. If no balloons are avail-able, packing the vagina with antiseptic impregnatedgauge can also be of value. The third variation is themost serious. It is the deep vaginal tear that extendsinto the abdominal cavity causing either a retro-peritoneal hematoma(s) or compromising the urinarytract. An illustration of this variation is found in theChapter 23 by B-Lynch. It is important to rememberthat a simple suture of the vaginal wall over what looksto be a deep tear in the posterior or lateral wallmay include the rectum, bladder and/or ureter, eventhough ureteric injury with a tear is most unlikely.
Adequate exposure may be needed and can beachieved by performing an episiotomy (if not presentalready or if it is too small can be extended) and using aDever’s retractor for the posterior vaginal wall and aLangden or vaginal retractor for the anterolateral vagi-nal wall. Long Aliss tissue forceps are useful to apply to
4
POSTPARTUM HEMORRHAGE
Normal vaginaldelivery
PPH
Uterotonics +tranexamic acid
Still bleeding
Examination under
anesthesia
Consider uterine balloon after ruling out
trauma
If traumatic cause
AccessibleSimple corrective
suturing +/− packing
Notaccessible
Embolization or if facilities do not exist – Aortic compression – Laparotomy – Variety of methods to employ. One should remember
ureters are at risk
Scenario 1 – Vaginal delivery and PPH
the vaginal wall near the apex of the tear. It is adequateand better to suture each side of the vaginal wall sepa-rately without trying to approximate adjacent walls ofthe tear to avoid obliterating the view higher up andalso causing tension tears of the vagina. The gap leftbehind will epithelialize rapidly in a few weeks. Asuture position as high as possible should be used as astay suture and traction applied to the suture higher upto arrest bleeding. The consecutive sutures can be heldtogether as stay sutures to prevent tearing of the vagi-nal wall. Usually bleeding is from an artery that hadretracted under the vaginal wall and hence the sutureneeds to be higher than and lateral to the apex of thetear. Treatment of this variation may involve a com-bined vaginal–abdominal approach on either side ofthe trauma (see Chapter 24).
If concerns exist about ureteric injury, immediatecystoscopy can confirm the presence of urinary effluxon both sides of the bladder demonstrating the integ-rity of the ureters. If cystoscopy cannot be accom-plished immediately, an intravenous pyelogram (IVP)can be performed the next day.
In some circumstances, especially those cases beingconducted in tertiary centers with full facilities, it maybe prudent to correct the coagulopathy and instituteembolization before embarking on laparotomy (seeChapters 49 and 50). In other circumstances it is nec-essary to consider transfer of the bleeding patient to aspecialist center with capability for arterial emboliz-ation. Two cautionary points are important. First, it isinappropriate to transfer a patient in shock, becausethe condition will only deteriorate during the transferprocess and waiting for the procedure. Second,patients in shock and with coagulopathy are notsuitable candidates for embolization. Under such cir-cumstances, the vascular system is in a state of constric-tion which impedes blood flow in the bleeding vessels.The actual average procedure time for a fully trainedinterventional radiologist is 1 hour. This does notinclude transfer and preparation time. One should notforget that fluids and hemostatic support must beprovided during the transfer and procedure. Furtherdiscussion is found in Chapter 49, in addition, Chap-ters 38 and 39 describes the use of non-pneumaticantishock garment (NASG) which redistributes bloodfrom the lower extremities to the central circulatorysystem of the major organs (heart, kidneys, brain).
SCENARIO 2 – INSTRUMENTAL DELIVERY ANDPPH
Scenario 2A – ventouse delivery and PPH
When bleeding begins after a ventouse delivery, it isimportant to distinguish whether it is from a vaginallaceration(s) per se or a combination of uterine atonyplus vaginal laceration(s). If uterine atony is present,blood will be coming from the cervix in addition toany bleeding that flows from the vaginal walls second-ary to trauma. Treatment of the atonic bleedingshould follow directions given in Scenario number 1
as well as information provided in chapters inSection 8.
Ventouse related lacerations often are circular innature because of the physical nature of the instrumentused. The lacerations are caused by the inadvertentincorporation of vaginal tissue into the ventouse whenit slips. Unlike traumatic lacerations which normallytake a linear form, these lacerations may actually repre-sent an area of missing vaginal tissue which has beendenuded. Because of the friable nature of the vaginalwalls, packing is generally advocated using long cottongauze previously moistened with saline or antisepticsolution. This can remain in place for 24 hours when itcan be gently removed. More recently, a speciallydevised vaginal balloon has been used successfullyin these cases (see Chapter 54). Both methodologiesprovide pressure against the bleeding surfaces.
Rectal and bladder injuries are rare but may occurwith instrumental vaginal deliveries (Figure 2). Henceit is important to determine that neither the bladdernor the rectum has been injured after each ventousedelivery. Non-recognition of a bladder or rectallaceration will result in fistula formation and is oftenfollowed by litigation issues. Effective anesthesia isparamount for repair efforts. In such cases transfusionmay or may not be indicated depending upon theextent of the blood loss and deterioration of vitalsigns.
5
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
Instrumental delivery and PPH
Venouse delivery and PPH
Forceps delivery & PPH
Lower genital tract trauma can be associated with third and fourth degree
perineal tears
If bleeding not controlled in time, patient can develop coagulation failure, because two situations i.e., trauma and uterine atony
may coexist together
Known to causesemicircular tears
Correct and maintain hemostasis by doing corrective suturing as early as possible under good
anesthesia. In some cases vagi-nal packing may be necessary. If bleeding is massive, abdomi-nal aortic compression should be considered till the defi nitive
measures are instituted
Early recourse to repair of perineal tears under good
anesthesia
CT – abdomen + pelvis +/− embolization
If necessary, vaginal packing and correction of coagulation abnormality
and high dependency unit monitoring
If facilities do not exist or patient not improving early recourse
to laparotomy while correcting the coagulation abnormality if
present
Scenario 2 – Instrumental delivery and PPH
Scenario 2B – forceps delivery and PPH
Bleeding after a vaginal delivery with forceps can becomplicated by factors that occur prior to delivery. Ifthe woman has had a prolonged labor with or withouta prolonged second stage, the likelihood of the coexis-tence of different causes of PPH is high. For example,such a woman is likely to be dehydrated, uterine atonyis more likely to be present, and genital tract traumamay be so severe that its repair by an inexperiencedoperator would be prolonged, and ineffective incontrolling blood loss.
The bleeding from uterine atony appropriately hasbeen described as S1 segment bleeding (Figure 3), aterm which is related to the fact that it comes from theupper part of the uterus which is supplied mainly bythe ascending branch of the uterine artery (90%) andsecondarily by the ovarian artery (10%)5. At the sametime, bleeding from cervical lacerations or the superioraspect of the vaginal vault is characterized as S2 seg-ment bleeding. Such bleeding mainly derives fromtwo vessels: first, the descending branch of the uterineartery; and second, the vaginal artery which usuallyarises from the posterior division of internal iliac artery(see Chapter 1).
In such instances, if the patient is taken for anembolization procedure, it is important that the radi-ologist realize that the vaginal artery is not a branch ofthe anterior division of the internal iliac artery and thatthe embolization catheter must enter the posteriorinternal iliac branch. If the radiologist embolizes theposterior division of the internal iliac to control lowervaginal bleeding, the patient is at risk of having anon-target embolization of the inferior gluteal vesselwhich supplies the sciatic nerve.
In order to avoid this problem, the bilateral inser-tion of a balloon into the common iliac arteries isrequired to provide time (90 min) ( Jose PalaciosJaraquemada – personal communication, 31 October2011) for the surgeon to reach the bleeding field withappropriate instruments or the interventional radiolo-gist to attempt embolization a second time (Figure 4).
The nature and extent of vaginal lacerations cannotbe properly assessed in the absence of good light andproper assistance with long retractors. Vaginal lacera-tions may be simple linear tears or explosive in nature.In addition, they may extend deeply into one or bothfornices.
If good assistance is not obtained rapidly and themultiple causes of bleeding are not addressed promptlyand adequately, the patient’s chance of developingacute coagulation failure and its resultant co-morbidities is extremely high.
Depending upon the extent and quantity ofthe blood loss, external (and sometimes internal)aortic compression (Videos 1 and 2) may be of greatuse to gain extra time when the patient is beingassessed for the extent of her injuries and earlyresuscitative measures are being applied. It goes with-out saying that volume replacement and correctionof anemia, acidosis and prevention of hypothermia
6
POSTPARTUM HEMORRHAGE
Figure 2 Schematic diagram showing incorrect application ofventouse cup in occiput-posterior position which potentially maycause fourth degree tear causing rectovaginal fistula
Figure 3 Segment S1 and S2 bleeding: S1, the upper part ofthe uterus which is supplied mainly by the ascending branch ofthe uterine artery (90%) and secondarily by the ovarian artery(10%) and S2 the lower part of the uterus supplied by the descendingbranch of the uterine artery and the vaginal artery. Courtesy ofPalacios-Jaraquemada
Figure 4 Interventional radiology X-ray image of common iliacballoon. Courtesy of Dr Shih, Jin-Chung, Department of Obstetricsand Gynecology, National Taiwan University Hospital andNational Taiwan University College of Medicine, Taipei, Taiwan
must take place while these other interventions arebeing carried out. In addition, it must be rememberedthat the continuation of bleeding will precede theonset of coagulopathy. A full discussion of the recentchanges in the ratios of fibrinogen to red cells invarious transfusion protocols is provided in Chapters3, 4 and 6.
The present scenario illustrates the concept thatPPH cannot be considered solely a uterine problem.Rather, PPH is a condition which affects the entiresystem and has the potential to have adverse conse-quences on multiple organs if not treated properly andin a timely manner.
The tendency to perform hysterectomy often isseen in situations such as the one described above.What the practitioner may not realize is that hysterec-tomy is designed to treat bleeding from the uterinefundus (S1 area) and will not effectively treat bleedingfrom the lower uterine segment/cervix, parametriumand upper vagina (S2 area), because the bleeding pedi-cles are different. In fact, performing hysterectomyin such instances may worsen the overall condition of
the patient. Moreover, performing hysterectomy willdeplete at least 1.5 liters of blood from the alreadycompromised patient’s circulation.
SCENARIO 3 – PPH IN THE RECOVERY AREAFOLLOWING ELECTIVE CESAREAN DELIERY
A cesarean section is always major surgery. Therefore,it can cause complications like any other majorsurgery. PPH following elective cesarean is notan uncommon event. Close vigilance, appropriatemonitoring (modified early warning score (MEWS)chart) and seeking help at the appropriate time willavert further serious complications and death.
Patient deterioration can be secondary to revealedPPH or concealed PPH. Concealed PPH is more dan-gerous than the revealed. Common reasons for thepatient to suffer PPH following elective cesarean areatonic uterus, retained fragments of placenta, bleedinguterine angle and rectus sheath hematoma. Detailedexamination including checking for vitals signs and
7
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
Elective cesarean section
PPH in the recovery (revealed)
Possibilities: Atonic uterus
Retained fragments of placenta
If uterus soft and boggy, express the clots by performing bimanual examination, making sure that patients pain relief is suffi cient and commence uterotonic infusion if not already being administered; if being given, can use second uterotonic
Bed side hemoglobin estimation is helpful in deciding need for blood product request and transfusion. If facilities exist, perform a bedside ultrasound scan to assess the uterine cavity
Adjuncts that are helpful are MEWS chart, regular assessment of uterine tone and assessment for bleeding per vaginum
If bleeding continues to be a problem not resolved by routine measures, then examination under anesthesia may be advisable. This will give the operator a chance to assess the uterine cavity and also to express further clots.
Also, one should consder using prostaglandins, tranexamic acid and address coagulopathy if present
Perform a compression test with patient in lithotomy position, and fi nd out whether the bleeding is intermittent or continuous. If the bleeding is intermittent, then uterine balloon tamponade should be considered before re-opening the patient.
If the bleeding in continuous, then patient needs re-opening, uterine angles need to be checked and, if the bleeding is from uterine fundal origin, then one of the uterine compression sutures should be considered. In few cases ‘sandwich technique’ is considered, where in uterine compression suture and uterine balloon tamponade are applied simultaneously. One should
be aware that the above procedures will only work if the patient’s coagulation status is corrected.
If bleeding still continues, then subtotal hysterectomy or uterine packing should be considered. One should make sure that the coagulation abnormality is corrected
Such patients will need HDU/ITU care
Rarely bleeding may still continue; in that case abdominal packing with large gauzes and closing the abdomen with a view to correct coagulopathy and replace necessary blood products and further monitoring in ITU is needed. Once the patient is
stabilized then patient needs to be taken back to theater for removal of the pack
Scenario 3 – PPH in the recovery area following elective cesarean delivery
abdominal and bimanual examination by an experi-enced professional will usually yield clues as to the ori-gin of the bleeding. If the bleeding is of uterine origin,the uterus is usually soft and markedly enlarged.
If uterine atony is the cause of the PPH, the uteruswill be filled with clots, and the patient requires exam-ination under anesthesia, preferably in an operatingtheater. Clots must be expressed from the uterinecavity and uterine tone sustained or increased by use ofan additional uterotonic, assuming that one is alreadyin use.
If bleeding still continues to be a problem and is notrelieved by the above measures, then examinationunder anesthesia should be considered in order toallow assessment of the uterine cavity, expression offurther clots and, if necessary, insertion of a uterineballoon tamponade (see Scenario 1).
A uterine compression test should be performed.If bleeding is intermittent, the balloon tamponadeshould work (see Chapters 45, 47 and 48). If bleedingis continuous, however, the patient will requirere-opening. Uterine compression sutures/sandwichtechnique will only work if there is no coagulopathy.
If bleeding is still not under control, then thereshould be no hesitation to recourse to subtotal hyster-ectomy. Following any of the above procedures suchpatients will need care in a high dependency unit(HDU) or intensive care unit (ITU).
Rarely bleeding may continue from the cervicalstump (in the case of subtotal hysterectomy) (seeChapter 55) and, in that case, local sealants may beused if available. In difficult cases abdominal/pelvicpacking with larger gauzes and closing the abdomenwith a view to correcting the coagulopathy andreplacing the necessary blood products, and furthermonitoring in ITU will be required. Once the patientis stabilized, the patient must be returned to theater forremoval of the packing.
SCENARIO 4 – EMERGENCY CESAREAN IN THEFIRST STAGE OF LABOR
Bleeding in emergency cesarean sections in the firststage of labor most commonly occurs from atony orlacerations of the uterine artery at one or both anglesof the uterine incision. Therapy of uterine atony iswell described in Scenario 1 and chapters in Section 8.The bleeding from incisional angles can be controlledby one of two means, both of which are much moreeasily accomplished when the uterus is exteriorizedand held upwards by an assistant.
The first method is to grasp the angle with a non-traumatic forceps and insert one or more figure-of-8sutures. The second is to examine the lateral margin ofthe uterus for the uterine artery itself, because the lac-eration may be in the ascending, middle or descendingbranch. If circumstances require ligation of the trau-matized artery at the lateral margin of the uterus, it isimportant to place sutures above and below the levelof the lacerated angle and include 1–2 cm of the myo-metrial tissue. This is because the ascending branch of
the uterine artery anastomoses with the descendingbranch of the ovarian artery, and the descendingbranch of the uterine artery anastomoses in turn withthe ascending branch of the vaginal artery. The liga-tion of the uterine arteries is totally without conse-quence to the uterine function because of the richanastomotic system that exists. A word of caution isnecessary, because if the laceration extends laterallyand inferiorly, it is possible to inadvertently includethe ureter (Figure 5 and Video 3).
8
POSTPARTUM HEMORRHAGE
Rule out atonia and bleeding from the lacerations of the uterine arteries at the angles of the inci-
sions. Other less common causes include placental abnormalities as shown in Scenarios 9 and 10
Use range of measures including uterotonics
Perform compression test
If no bleeding, perform compression suture
If bleeding still continues
Do not hesitate to perform hysterectomy if none of the
measures are working
Beware of stump bleeding, which can be controlled by local
hemostatic agents
Seek second obstetrician’s help
Scenario 4 – Emergency cesarean in the first stage of labor
Figure 5 Posterior and right view of female pelvis in a freshcorpse: the image shows the pelvic ureter over the iliac vessels andinside and parallel to the ovary pedicle. Palacios-Jaraquemada,20126, with permission
At the same time as these measures are being carriedout, the previously described uterotonic therapy isadministered (Scenario 1). Fluid replacement and, ifnecessary, blood and blood products should also beadministered (see Chapters 3–6). If blood is deemednecessary, one should not wait until the laboratoryresults (hemoglobin, hematocrit, clotting factors, etc.)are present because continued bleeding will lead tocoagulopathy7.
If the uterus appears to be atonic in spite of theuterotonic agents having been administered, bimanualcompression of the uterus should be performed withthe view to assess the need for placement of compres-sion sutures. It is necessary to be sure that no clottingabnormality is present when the compression testis attempted. Compression should not be performedwith the patient in the supine position. Rather, thepatient should be placed into the frog-leg position andthe uterus should be exteriorized. If the compressiontest is positive, the operator should place the type ofuterine compression suture he/she is most comfortableto perform.
Surgeons competent to perform cesarean sectionsMUST also be competent to perform one of theavailable uterine compression sutures in a timelymanner (see Chapters 51–53). The advantage ofearly compression suture is that the hemorrhagehas not extended to the point where clottingabnormalities begin. In the recent article byPalacios describing 539 cases, most surgicalhemostatic failures that lead to hysterectomyoccurred in women with severe hemodynamicdeterioration and coagulopathy7.
If, in the unfortunate event that none of theabove-mentioned interventions are effective and thepatient continues with bleeding, a second and seniorobstetrician should be called to determine whetherhysterectomy is warranted. Here too, it is crucial tohave stability within the coagulation system.
If a decision is made to perform a hysterectomy, thesubtotal type is faster, equally effective and less likelyto be associated with surgical complications such asureteric injuries. Bleeding may occur from the cervicalstump, the side walls of the pelvis, or even the ovarianpedicles. Usually this can be controlled with localhemostatic agents (see Chapters 57 and 58) or with alarge pelvic pack consisting of a gauze tube filled withlaparotomy pads (Figure 6). If a hysterectomy alreadyhas been performed, a plastic bag filled with gauze canbe placed in the pelvis with the opening of the bagbrought out through the vaginal apex which had beenleft open (see Chapter 54).
Packing can be removed 24 hours later. Patientswho have had this intervention should be observedin the intensive care unit for 24–48 hours to monitorfor pulmonary edema and diminished urinary out-put, pain control and restoration of full clottingparameters.
SCENARIO 5 – FAILED SEQUENTIALINSTRUMENTAL DELIVERY/EMERGENCYCESAREAN AT SECOND STAGE OF LABOR
9
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
Failed instrumental/second stage
Bleeding from lower segment or upper genital tract/upper vagina
Important points to remember
Careful closure of the traumatized area. Sometimes it is necessary to dissect the ureters, bladder and broad
ligament
Do not forget bleeding from the upper uterine segment may also coexist
– Diffi cult access– Ureters are at risk of injury
Do not hesitate to seek opinion from urologist/oncologist
Scenario 5 – Failed sequential instrumental delivery/emergencycesarean at second stage of labor
Figure 6 (a) Gauze tube filled with laparotomy pads. (b) Packingwith gauze tube filled with laparotomy pads into the pelvis
(a)
(b)
Bleeding from failure of an instrumental delivery fol-lowed by a difficult fetal extraction during a cesarean isparticularly challenging. This is because the source ofbleeding could be from atony or the upper genitaltract (S1), the lower uterine segment (trauma with orwithout obvious evidence) or the upper vagina, cervixand parametrium (S2).
The challenges here are to differentiate rapidlywhich is the most likely cause and whether more thanone cause of bleeding is operating concurrently. Timeis required to make this differentiation, and the use ofintraoperative aortic compression (Video 2) permitsthe operator to make careful intraoperative assessmentin the presence of the markedly reduced bleeding.
Three causative possibilities must be mentioned.The first is that the operator is able to find the trauma-tized area and place several simple sutures that controlthe bleeding. In order to do this, the bladder musthave been pushed down to make sure that it is pro-tected from getting accidentally included into a suture.
The second is that the operator is unable to controlthe bleeding from the lower uterine segment or theupper vagina (Video 4). In this case, it is mandatory todissect the ureter(s) laterally until it (they) enters thebladder. It is not enough to say the operator visualizedthe ureter, because the traumatized area may actuallyinvolve it (Figure 5 and Video 3). At this point, it ishelpful to encircle the lower uterine segment with awide rubber catheter and secure it tightly with a firmclamp placed at its center (Video 5).
The third option relates to trauma at the middle tolower part of the vagina and the levator ani muscle asdescribed below in Scenario 9.
Comments related to proper fluid and bloodreplacement as described above also apply here.
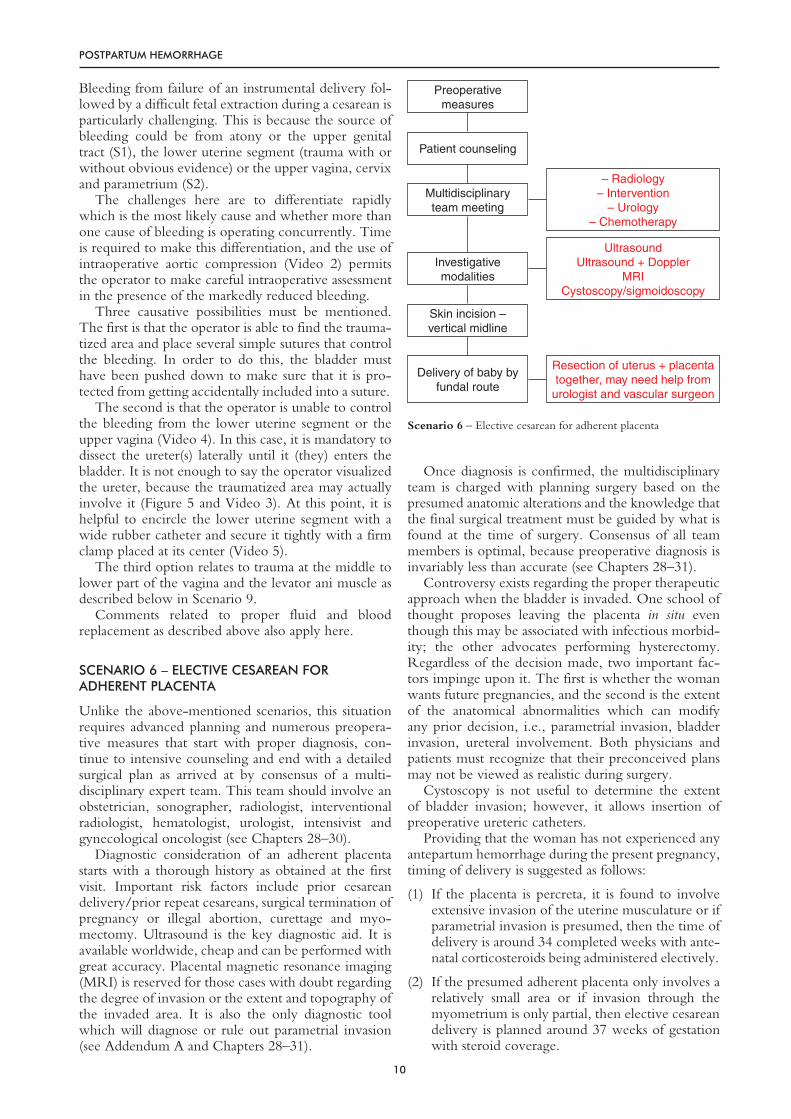
Unlike the above-mentioned scenarios, this situationrequires advanced planning and numerous preopera-tive measures that start with proper diagnosis, con-tinue to intensive counseling and end with a detailedsurgical plan as arrived at by consensus of a multi-disciplinary expert team. This team should involve anobstetrician, sonographer, radiologist, interventionalradiologist, hematologist, urologist, intensivist andgynecological oncologist (see Chapters 28–30).
Diagnostic consideration of an adherent placentastarts with a thorough history as obtained at the firstvisit. Important risk factors include prior cesareandelivery/prior repeat cesareans, surgical termination ofpregnancy or illegal abortion, curettage and myo-mectomy. Ultrasound is the key diagnostic aid. It isavailable worldwide, cheap and can be performed withgreat accuracy. Placental magnetic resonance imaging(MRI) is reserved for those cases with doubt regardingthe degree of invasion or the extent and topography ofthe invaded area. It is also the only diagnostic toolwhich will diagnose or rule out parametrial invasion(see Addendum A and Chapters 28–31).
Once diagnosis is confirmed, the multidisciplinaryteam is charged with planning surgery based on thepresumed anatomic alterations and the knowledge thatthe final surgical treatment must be guided by what isfound at the time of surgery. Consensus of all teammembers is optimal, because preoperative diagnosis isinvariably less than accurate (see Chapters 28–31).
Controversy exists regarding the proper therapeuticapproach when the bladder is invaded. One school ofthought proposes leaving the placenta in situ eventhough this may be associated with infectious morbid-ity; the other advocates performing hysterectomy.Regardless of the decision made, two important fac-tors impinge upon it. The first is whether the womanwants future pregnancies, and the second is the extentof the anatomical abnormalities which can modifyany prior decision, i.e., parametrial invasion, bladderinvasion, ureteral involvement. Both physicians andpatients must recognize that their preconceived plansmay not be viewed as realistic during surgery.
Cystoscopy is not useful to determine the extentof bladder invasion; however, it allows insertion ofpreoperative ureteric catheters.
Providing that the woman has not experienced anyantepartum hemorrhage during the present pregnancy,timing of delivery is suggested as follows:
(1) If the placenta is percreta, it is found to involveextensive invasion of the uterine musculature or ifparametrial invasion is presumed, then the time ofdelivery is around 34 completed weeks with ante-natal corticosteroids being administered electively.
(2) If the presumed adherent placenta only involves arelatively small area or if invasion through themyometrium is only partial, then elective cesareandelivery is planned around 37 weeks of gestationwith steroid coverage.
10
POSTPARTUM HEMORRHAGE
Preoperative measures
Patient counseling
Multidisciplinary team meeting
Investigative modalities
Skin incision – vertical midline
Delivery of baby by fundal route
– Radiology– Intervention
– Urology– Chemotherapy
UltrasoundUltrasound + Doppler
MRICystoscopy/sigmoidoscopy
Resection of uterus + placenta together, may need help from
urologist and vascular surgeon
Scenario 6 – Elective cesarean for adherent placenta
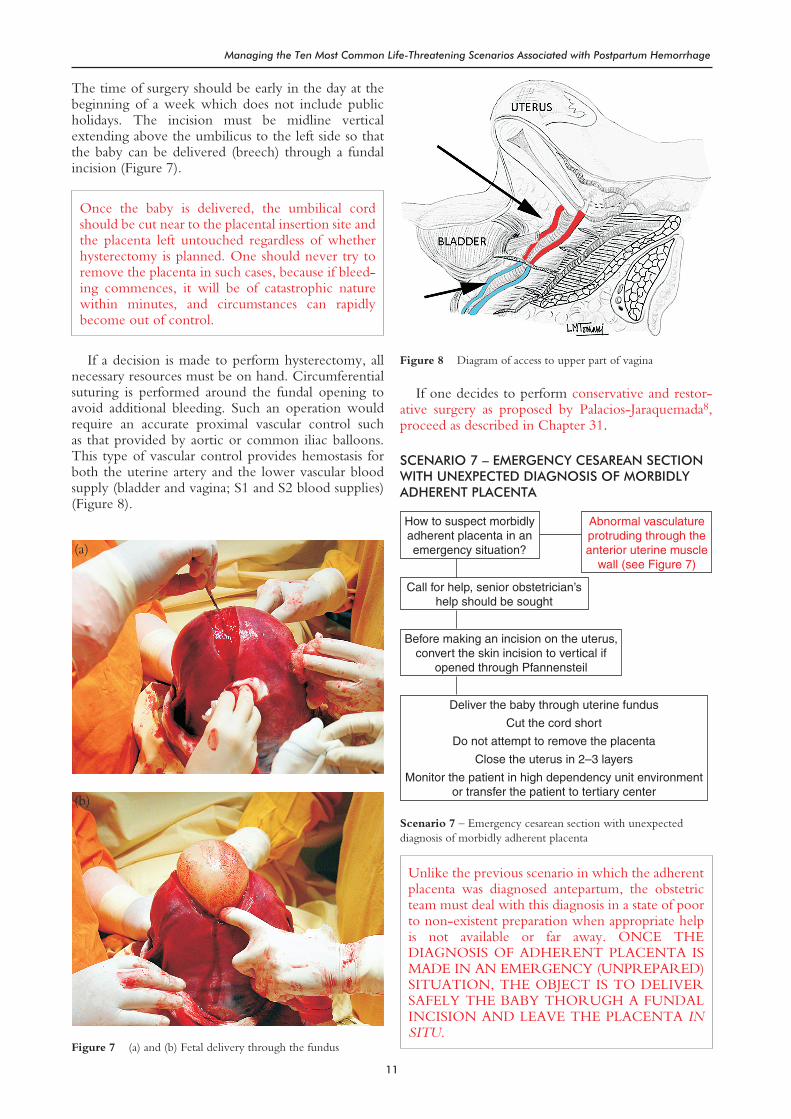
The time of surgery should be early in the day at thebeginning of a week which does not include publicholidays. The incision must be midline verticalextending above the umbilicus to the left side so thatthe baby can be delivered (breech) through a fundalincision (Figure 7).
Once the baby is delivered, the umbilical cordshould be cut near to the placental insertion site andthe placenta left untouched regardless of whetherhysterectomy is planned. One should never try toremove the placenta in such cases, because if bleed-ing commences, it will be of catastrophic naturewithin minutes, and circumstances can rapidlybecome out of control.
If a decision is made to perform hysterectomy, allnecessary resources must be on hand. Circumferentialsuturing is performed around the fundal opening toavoid additional bleeding. Such an operation wouldrequire an accurate proximal vascular control suchas that provided by aortic or common iliac balloons.This type of vascular control provides hemostasis forboth the uterine artery and the lower vascular bloodsupply (bladder and vagina; S1 and S2 blood supplies)(Figure 8).
If one decides to perform conservative and restor-ative surgery as proposed by Palacios-Jaraquemada8,proceed as described in Chapter 31.
Unlike the previous scenario in which the adherentplacenta was diagnosed antepartum, the obstetricteam must deal with this diagnosis in a state of poorto non-existent preparation when appropriate helpis not available or far away. ONCE THEDIAGNOSIS OF ADHERENT PLACENTA ISMADE IN AN EMERGENCY (UNPREPARED)SITUATION, THE OBJECT IS TO DELIVERSAFELY THE BABY THORUGH A FUNDALINCISION AND LEAVE THE PLACENTA INSITU.
11
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
How to suspect morbidly adherent placenta in an emergency situation?
Call for help, senior obstetrician’s help should be sought
Before making an incision on the uterus, convert the skin incision to vertical if
opened through Pfannensteil
Deliver the baby through uterine fundus
Cut the cord short
Do not attempt to remove the placenta
Close the uterus in 2–3 layers
Monitor the patient in high dependency unit environment or transfer the patient to tertiary center
Abnormal vasculature protruding through the anterior uterine muscle
wall (see Figure 7)
Scenario 7 – Emergency cesarean section with unexpecteddiagnosis of morbidly adherent placenta
Figure 7 (a) and (b) Fetal delivery through the fundus
(a)
(b)
Figure 8 Diagram of access to upper part of vagina
The first challenge is to suspect or make the diagnosis.In most instances the visual appearance of the anterioruterine serosa and lower uterine segment at the levelof the superior limit of the bladder is sufficient tosuggest that something is drastically abnormal. Thepicture is one of a bulging lower uterine segmentwith numerous tortuous vessels directly under theserosa or on the peritoneum overlying the bladder(Video 6).
This anatomic distortion is visible immediatelyupon opening of the peritoneum, especially when aPfannensteil incision is used. It is important that theobstetrician realize the seriousness of the condition andNOT attempt any manipulations or incisions at thispoint. Rather, the skin incision should immediately beconverted to a vertical incision to the level of theumbilicus or higher in order to have access to the uter-ine fundus for safe delivery of the baby. Any thoughtsof continuing surgery through the Pfannensteil inci-sion should be immediately abandoned, as continua-tion of surgery will be dangerous and put the mother’slife at great risk.
After converting the skin incision and prior to mak-ing any uterine incision, help should be requestedfrom the most senior obstetricians and anesthesiolo-gists. In addition, the blood bank should be alertedand samples should be sent for typing and cross-matching.
Delivery of the baby is safest via the fundal route(Figure 7), as this avoids any bleeding complicationassociated with abnormal placental attachment, espe-cially that which involves the bladder. Once the babyis delivered, the fundal incision can be closed asdescribed in Scenario 6.
Placental delivery should not be attempted in anymanner. Similarly, the bladder and its attachmentsshould remain undisturbed, as both can be effectivelydealt with at a later time by more experienced person-nel with full resources. It is NOT NECESSARY toperform an emergency hysterectomy in this situation.
It is also not necessary to use methotrexate forenhanced placental resorption, because the term pla-centa has a low level of mitotic activity (less than 1%).However, this statement does not meet with universalagreement.
Even if the patient appears stable after surgery,observation is recommended in a high dependencyenvironment whilst preparations for further care aremade.
Additional care at a tertiary center may involve oneof three options: first, to leave the placenta in situ untilspontaneous expulsion or resorption; second, to per-form hysterectomy with full resources for the compli-cations that are described in Scenario 6; and third,to perform reconstructive surgery as described inChapter 31.
SCENARIO 8 – PROGRESSIVE INTERMITTENT PPH
The bleeding in this scenario may follow normal oroperative (ventouse, forceps or cesarean) delivery, may
commence within a few hours and may last for a fewweeks. In other cases, its onset is later (possibly a fewdays to a week) but its continuation is similar. Becausethis form of postpartum bleeding is progressive andintermittent, assessment and care may be less thanoptimal for a number of reasons: (1) failure to keep arunning total of the individual episodes of blood losssince delivery or misinterpretation of blood loss aslochia rubra; (2) failure to recognize missing placentalcotyledons and/or incompleteness of membranes; and(3) failure to monitor.
The potential gravity of the situation is augmentedif the patient’s symptoms of dizziness, feeling cold andbeing weak and tired are ignored or if strict input/output monitoring has not taken place. This latterpossibility is more important if the patient has receivedlarge quantities of intravenous fluids containinguterotonic agents, and the care givers assume that thesituation will correct itself. Other contributing factorsinclude failure to use simple diagnostic aids such asdetailed genital examination and/or abdominal andvaginal ultrasound especially after the first 24 hours.The latter may not clearly differentiate betweenclots and small pieces of retained placental tissueimmediately after delivery when the uterus is not fullycontracted. Furthermore, the caregiver may under-estimate the extent of the blood loss because thepatient is hemodynamically stable and her vital signsare well maintained. Finally, if the patient is goingto be discharged, she and her family as well as thecommunity health workers or local doctors must beinformed about the nature of the small and continuingblood loss. Any patient who leaves the hospital mustreceive clear and written information about what isconsidered to be sufficiently abnormal as to requirereturn to the hospital for further care. If she lives along way from the hospital, she should be given a copyof the discharge summary or some notation as to thenature of the problem and whom to contact withtelephone numbers and email addresses if a problemarises.
The following points are provided to ensureoptimal follow-up in patients who have intermittentbleeding.
● Intermittent/recurrent bleeding per vaginumfollowing delivery in the first 42 days should betreated as PPH
● Even if the patient’s vital signs are stable, it isworthwhile performing an ultrasound scan basedon the health center’s equipment and resources. Ifultrasound is used, it is important to obtain bothabdominal and vaginal scans so that the fundal andlower uterine segments can be examined with simi-lar accuracy. If ultrasound scans detect a possibleplacental segment attachment to a prior cesareanscar, one should be careful with any attempts toremove it manually or by curettage, as such removalmay require specialist attention as there is a risk ofuterine scar dehiscence, bladder injury or secondarybleeding into the peritoneum
12
POSTPARTUM HEMORRHAGE
● If possible, the total blood loss from the point ofdelivery to the current patient encounter should becalculated; do not be afraid to repeat the hemo-globin assessment, if necessary, especially if thepatient complains of being tired and weak
● Undocumented blood losses should be carefullyassessed, as they may occur with change of bedpans/bed sheets/clothes, or passing of big clots inthe toilet pans
● If possible, and if the placenta is still available,it should be re-examined to account for everycotyledon
● If facilities for ultrasound examination do not exist,then examination under anesthesia is required toassess the uterine cavity and remove placental tissueand fragments if they are present. Undetectedcervical tears may require simple suturing
● If the operator decides to perform curettage, greatcare should be exercised to avoid perforation,because the uterine musculature may still be softand perforations may go unrecognized
● If the bleeding is heavy and intermittent after a fewweeks or a month, the most likely diagnosis isnot retained placental fragments but PSEUDO-ANEURYSM OF THE UTERINE ARTERY(Figure 9). This condition should be consideredwhen patients have undergone a difficult instru-mental delivery, curettage for retained placentalfragments, or difficult fetal extraction during acesarean section. This diagnosis is suspected if thepatient has had one, two or more negative ultra-sound scans. Diagnostic confirmation is by colorDoppler or angiography of the pelvic vessels withthe capacity to embolize at the same time. Oneshould not attempt curettage or hysterectomybecause the tissues are exceedingly friable and alsothere is real risk of massive hemorrhage.
SCENARIO 9 – CONCEALED PPH
Concealed PPH is an important cause of maternaldeath, because either the clinician is not alerted to itspresence until late in its course or the obstetricianis unable to control the bleeding at its source. Thisscenario presents the relevant material in a moretraditional manner, as one algorithm would not fit.
Situations which lead to concealed PPH
● Successful but difficult instrumental deliverycausing subperitoneal/retroperitoneal/pre-peritonealspace of Retzius hematoma (Figure 10), injury tothe puborectal fascicle or to the external muscularcovering of the vagina (Figure 11)
● Failed instrumental delivery leading to emergencycesarean section with or without difficult fetalextraction. (Unsuspected broad ligament hema-toma, difficult access to the deep uterine angle
extensions, undiagnosed posterior uterine wall inju-ries, hesitation in closure of uterine angles as theoperator is concerned about ureteric ligation andproceeding to close the angles without caution)
13
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
Figure 9 Pseudoaneurysm of the uterine artery – angiographyimages. Courtesy of Dr Garcio-Mónaco, Buenos Aires, Argentina
● If elective cesarean is performed in a woman whosecervix was never dilated in the past, she is particu-larly at risk of uterine atony with the accumulationof a large amount of intrauterine blood clots beforeclinical deterioration becomes evident. Detectionof clinical deterioration may be so late that thepatient succumbs despite emergency measures
● Another contributory factor for accumulation ofclots after elective cesarean section followed byatony is the lack of response to oxytocic agents,which although uncommon, must be considered.Therapy consists of restoration of uterine tone andexpression of the clots
● Uterine rupture can also be easily missed. Classi-cally, such patients are multiparous and their laborshave been augmented with uterotonics, inducedwith prostaglandins, or were precipitate in nature.It is also possible following a midcavity forcepsdelivery. Such patients are well for a few minutesfollowing delivery, but bleeding continues intra-abdominally without overt deterioration at first. Bythe time it is recognized, the clinical picture may begrave and resuscitative measures may be futile
● Rectus sheath hematomas, where bloodaccumulates above the abdominal cavity without
external bleeding, can also cause similar deteriora-tion.
Other contributory factors
● Operator inexperience
● Delivery time of the day with misses more commonlate at night
● Poor/inexperienced assistant
● Failure to exteriorize uterus to check posterior wall,especially after difficult head extraction
● Operator thinks that small amount of bleeding maydiminish over time
● Fast surgery, too much time pressure, too manythings to do
● Ignoring clinical signs of deterioration, i.e., worsen-ing tachycardia, falling blood pressure, increasingrespiratory rate, increasing abdominal girth, fallingurine output and increasing patient demand foranalgesic use are all pointers of concealed PPH.
Solutions
● If uterine rupture is suspected, speed and efficiencyof the whole team are required. Everyone has a keyrole starting from the switchboard, to porters,to hematology and blood bank technicians, tomidwifery and obstetric and anesthetic teams
● Close monitoring of all patients who need operativeintervention is mandatory
● Bedside facilities such as hemoglobin measurementby simple equipment such as Hemacue will aidclinicians rapidly to detect patient deterioration
● Use the modified obstetric early warning scoringsystem (MOEWS) chart in all at risk patients (seeAddendum B of this chapter for a sample chart)
● Education and training of all staff must take place atregular intervals
● Patient counseling must recognize that no cesareandelivery is risk free (either elective or emergency)
● Prompt action by the attending physician isrequired to establish the cause of a patient’s physicaldeterioration
● From the obstetric point of view, if uterine ruptureis suspected and if the patient’s situation permits, abedside ultrasound scan is helpful to diagnose thepresence of intraperitoneal bleeding. However, oneshould also remember not to waste time trying toestablish a specific cause, as every second counts incombating situations involving uterine rupture
● If an expanding broad ligament hematoma is sus-pected, then computed tomography (CT) scanningand embolization of the bleeding vessel has a role.Even if such patients undergo laparotomy, it will be
14
POSTPARTUM HEMORRHAGE
Figure 10 Retroperitoneal hematoma
Figure 11 Sutured injury of internal fascicle of levator ani muscle
extremely difficult to identify the exact source ofbleeding vessel and tissues will be very fragile.
If patient is taken back for re-laparotomy, whatnecessary steps should be taken?
● Resuscitation and correction of volume deficiencyshould happen simultaneously
● It is very easy to miss coexisting coagulopathy;hence there is a high possibility that the patient willrequire replacement of clotting factors (see Chap-ters 4 and 6 for discussion of controversy regardingthe proper ratio of RBC and fibrinogen productsduring replacement)
● The team should involve a senior obstetricianwith support from another senior obstetrician,senior anesthetist, hematologist and occasionally anintensivist and an interventional radiologist
● During re-laparotomy, meticulous attention shouldbe given to each abdominal layer, and the uterusshould be exteriorized and its cavity either checkedwith intraoperative ultrasound or re-opened. Ifuterine atony was the cause of patient deterioration,then it may be worthwhile inserting a uterine com-pression suture or uterine tamponade balloon
● If bleeding is from the uterine parametrium, thenone should seek help from the urologist or gyneco-logical oncologist, as the ureters are at risk of beinginjured while achieving hemostasis
● If time and the situation permit, the patient shouldbe counseled about the risks of hysterectomy.Patients also should be counseled that there is asmall possibility of not being able to identify theexact source of bleeding and that even if hysterec-tomy is performed, bleeding may still continue. Insuch circumstances, the clinician may decide to putseveral abdominal packs in situ and request furthermonitoring in the intensive care setting (see above).Once the patient’s clinical condition improves, usu-ally after 24 hours, the patient would need anotherlaparotomy to remove the abdominal packs. Occa-sionally, the patient may still require radiologicalembolization of bleeding pelvic vessels.
SCENARIO 10 – UTERINE INVERSION AND PPH
Usual scenario
Uterine inversion is almost always secondary to strongtraction on the umbilical cord which is attached to theplacenta when it is implanted in the fundus. Theproblem here is not that the placenta is abnormallyadherent but rather that the traction is too forceful andtoo early (before the placenta is normally separated).Inversion can be avoided by simple measures: notattempting the forceful cord traction before the signsof placental separation are seen (lengthening of thecord, fresh gush of bleeding, desire to push by thewoman) and placement of one hand on the fundus
while the other hand guides the cord. Of those whoexperience uterine inversion, one in six women willdie if appropriate corrective measures are not appliedin a timely manner. Always suspect uterine inversion ifthe patient becomes shocked immediately after birthwithout an obvious reason.
Inversion of the uterus may be partial or complete.The upper panel illustrates an incomplete inversion inwhich the most important physical finding is the pres-ence of a dimple in the uterine fundus. The middlepanel demonstrates the three degrees of inversion. Instage ‘3’ and ‘4’, the fundus is completely outside ofthe vulva, and these two variations are the most cata-strophic, as any delay in recognition of the inversionand the urgency of correction may be followed bydeath of the patient.
Symptoms
The initial symptoms depend upon the severity of theuterine inversion. If inversion is only partial, thensevere cramping lower abdominal pain and signs ofmild shock, i.e., bradycardia and hypotension, may bethe initial signs. Massive bleeding will not be present.On the other hand, if the inversion is complete, it isaccompanied by a brief period of neurogenic shockshortly followed by massive PPH. Shock is primarilybecause of parasympathetic activation of the nervoussystem because of traction on the peritoneum throughligaments supporting the uterus.
Management
It is imperative that the condition be recognizedinstantaneously and managed promptly and by theperson attending the delivery. The uterus (a dark pink/purple fleshy mass) is observed as lying outside thevulva immediately after birth. If the placenta is still insitu, manual repositioning should be attempted withoutremoving the placenta. If separation has not occurredand if the situation is ignored, the patient will bleedmassively and possibly precipitate further deep shock.
Help should be called for immediately, as the replace-ment must be performed with the patient in shock. If thebirth attendant cannot immediately replace the fundusand the shock continues, a single dose of atropine (oneampoule) should be administered preferably by the intra-venous route to address the neurogenic origin of theshock (parasympathetic blockade).
The initial attempt to replace the uterine fundusentails manual replacement through the vagina past thecervical ring. If the patient is receiving a uterotonic(oxytocin) infusion or is about to receive it as a pro-phylaxis for third stage bleeding, the infusion shouldbe stopped or withheld whichever is appropriate.
The typical maneuver in repositioning the fundusinvolves the birth attendant’s hand being placed insidethe vagina (for stage 3) or on the fundus for stage 4,with the cup of the inverted fundus in the palm of theoperator’s hand and the tips of fingers directed towardthe uterosacral ligaments. The fundus is then forcefully
15
Managing the Ten Most Common Life-Threatening Scenarios Associated with Postpartum Hemorrhage
pushed inside the abdominal cavity above the level ofumbilicus and held in that position for 3–5 minutesuntil the passive action of uterine ligaments correctsthe uterine inversion. Care should be taken not toapply so much pressure as to perforate the uterus withthe fingertips.
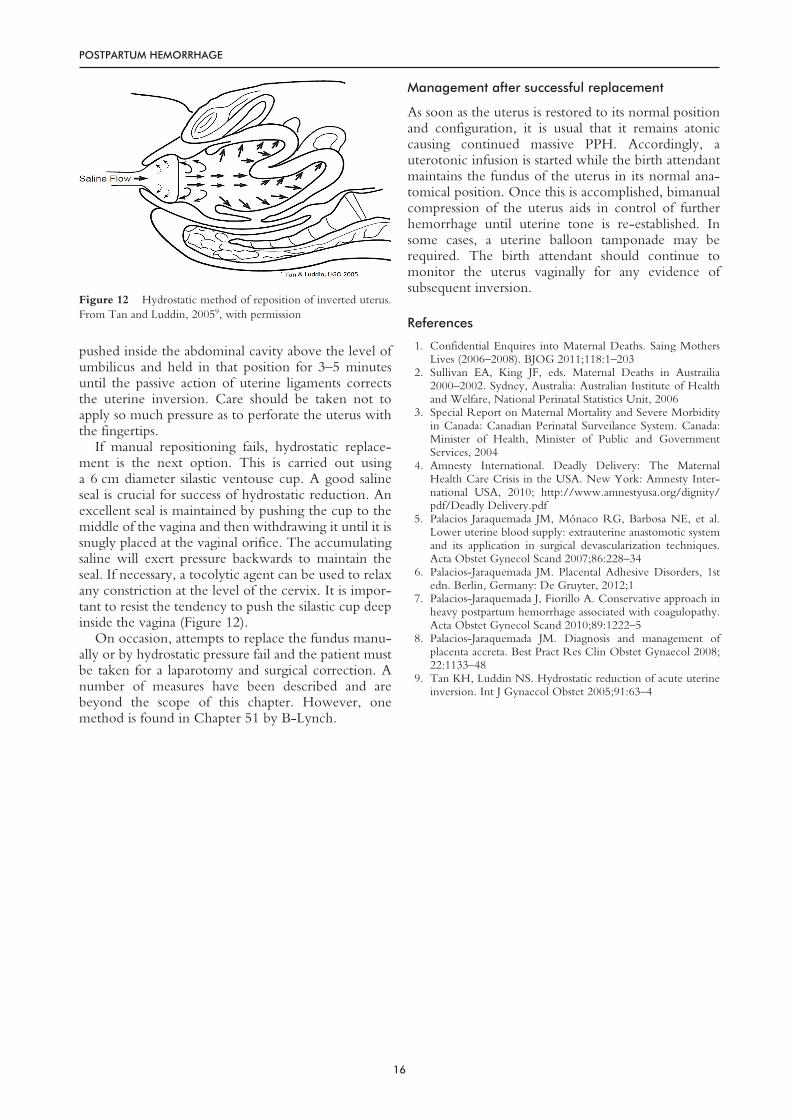
If manual repositioning fails, hydrostatic replace-ment is the next option. This is carried out usinga 6 cm diameter silastic ventouse cup. A good salineseal is crucial for success of hydrostatic reduction. Anexcellent seal is maintained by pushing the cup to themiddle of the vagina and then withdrawing it until it issnugly placed at the vaginal orifice. The accumulatingsaline will exert pressure backwards to maintain theseal. If necessary, a tocolytic agent can be used to relaxany constriction at the level of the cervix. It is impor-tant to resist the tendency to push the silastic cup deepinside the vagina (Figure 12).
On occasion, attempts to replace the fundus manu-ally or by hydrostatic pressure fail and the patient mustbe taken for a laparotomy and surgical correction. Anumber of measures have been described and arebeyond the scope of this chapter. However, onemethod is found in Chapter 51 by B-Lynch.
Management after successful replacement
As soon as the uterus is restored to its normal positionand configuration, it is usual that it remains atoniccausing continued massive PPH. Accordingly, auterotonic infusion is started while the birth attendantmaintains the fundus of the uterus in its normal ana-tomical position. Once this is accomplished, bimanualcompression of the uterus aids in control of furtherhemorrhage until uterine tone is re-established. Insome cases, a uterine balloon tamponade may berequired. The birth attendant should continue tomonitor the uterus vaginally for any evidence ofsubsequent inversion.
2. Sullivan EA, King JF, eds. Maternal Deaths in Austrailia2000–2002. Sydney, Australia: Australian Institute of Healthand Welfare, National Perinatal Statistics Unit, 2006
3. Special Report on Maternal Mortality and Severe Morbidityin Canada: Canadian Perinatal Surveilance System. Canada:Minister of Health, Minister of Public and GovernmentServices, 2004
4. Amnesty International. Deadly Delivery: The MaternalHealth Care Crisis in the USA. New York: Amnesty Inter-national USA, 2010; http://www.amnestyusa.org/dignity/pdf/Deadly Delivery.pdf
5. Palacios Jaraquemada JM, Mónaco RG, Barbosa NE, et al.Lower uterine blood supply: extrauterine anastomotic systemand its application in surgical devascularization techniques.Acta Obstet Gynecol Scand 2007;86:228–34
6. Palacios-Jaraquemada JM. Placental Adhesive Disorders, 1stedn. Berlin, Germany: De Gruyter, 2012;1
7. Palacios-Jaraquemada J, Fiorillo A. Conservative approach inheavy postpartum hemorrhage associated with coagulopathy.Acta Obstet Gynecol Scand 2010;89:1222–5
8. Palacios-Jaraquemada JM. Diagnosis and management ofplacenta accreta. Best Pract Res Clin Obstet Gynaecol 2008;22:1133–48
9. Tan KH, Luddin NS. Hydrostatic reduction of acute uterineinversion. Int J Gynaecol Obstet 2005;91:63–4
16
POSTPARTUM HEMORRHAGE
Figure 12 Hydrostatic method of reposition of inverted uterus.From Tan and Luddin, 20059, with permission
Addendum A: Guidelines for placental MRIs:technical aspects of MRI scan in morbidly adherentplacenta
Like other diagnostic methods placental MRI (pMRI)has certain technical details that can enhance oremphasize its diagnostic accuracy. The main aim ofthe imaging study is to obtain the best definitionof the uterine–placental interphase and its relation tothe bladder. Newly formed vessels (NFV) secondaryto the development of placenta accreta are under-developed in the middle layer. This particularityrequires the pMRI study to be performed with asemi-full bladder, to avoid false negatives as a result ofoverdistension and/or collapse of the NFV, as well asfalse negatives due to an empty bladder. It is importantthat the bladder is only partially full; an empty bladdernext to the pubic bone would prevent an adequatesign of the uterine–vesical interphase, resulting indiagnostic error. The use of ultrafast techniques thatminimize artifacts produced by fetal movement is rec-ommended. T2-weighted imaging highlights urine asa naturally white contrast, thus allowing better delin-eation of the vesical muscle in relation to the placenta
and the underlying myometrium. In the presence ofrisk factors (multiple D&C, myomectomies or correc-tive surgery), if there are clinical antecedents for theT2 mode allowing a naturally white contrast and asuspicion of posterior placenta accreta, the use ofgadolinium is recommended to improve diagnosticaccuracy. Without this, a combination of placenta,myometrium, abdominal viscera and the vertebraeform a complex image, which makes an adequatediagnosis of posterior myometrial placental invasionvirtually impossible. So far, gadolinium has not shownany side-effects during pregnancy, and there are notoxicity reports. However, and as a precaution, its useis generally recommended for cases in which diagnosisby other techniques is not possible. It is prudent to usepMRI in all cases with a resulting non-conclusiveultrasound or Doppler examination, when it is impor-tant to rule out or confirm the presence of parametrialinvasion. Therapeutic options depend on the size ofthe invasions and exact anatomy of the lesion
17
Addendum B: Modified obstetric early warningscoring chartReproduced, with permission