64
Manual Functional Analysis Lecture 1
| Date post: | 15-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | samer-mheissen |
| View: | 625 times |
| Download: | 0 times |
Manual Functional Analysis Lecture 1
بسم هللا الرحمن الرحیم (( و فوق كل ذي علٍم علیم ))
1935-1949 Charles Sidney Burwell
Dr. Burwell was a cardiologist who specialized in circulation changes associated with heart disease. He is credited with bringing attention to obstructive sleep apnea syndrome.
In 1944, Dean
"Half of what we are going to teach you is wrong, and half of it is right. Our problem is that we don't know which half is which."
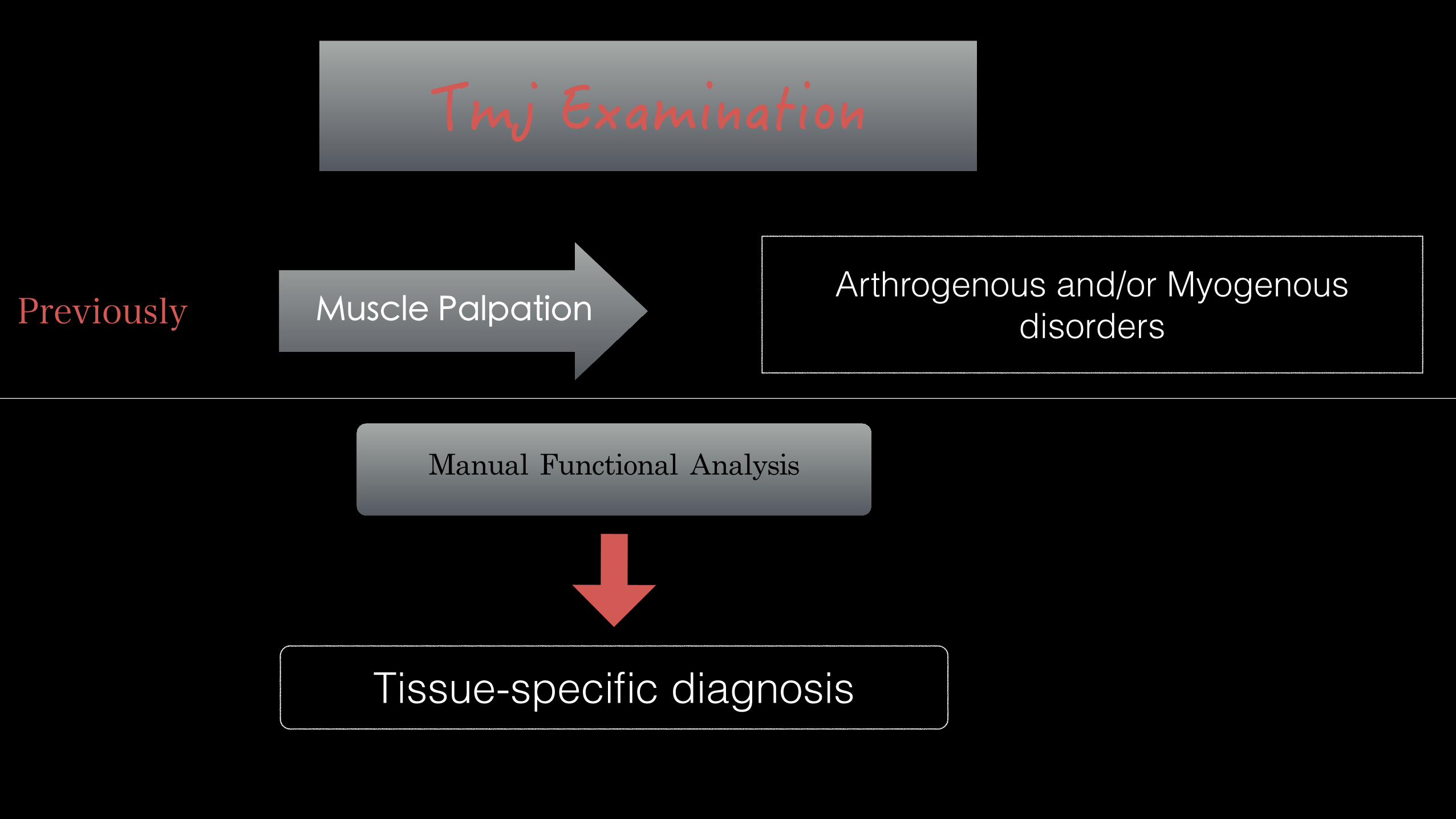
ManualFunctionalAnalysis
Muscle Palpation
Tissue-specific diagnosis
Arthrogenous and/or Myogenous disorders Previously
Tissue-Specific Diagnosis
Anatomical structure which is responsible on patiant’s
pains and symptoms
Adaptation Compensation
Mechanisms of Biological System when it exposed to many influences
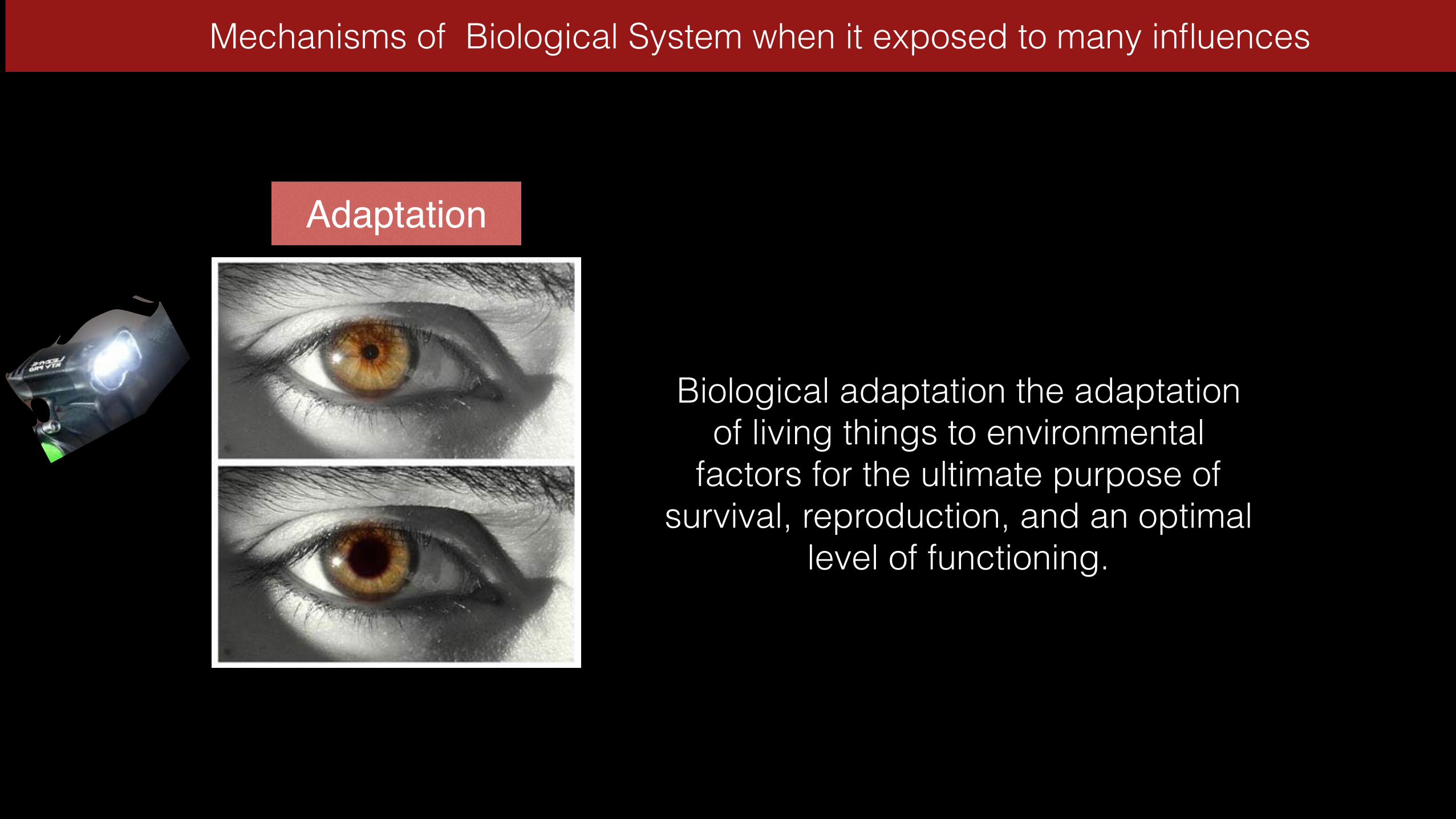
Adaptation
Mechanisms of Biological System when it exposed to many influences
Biological adaptation the adaptation of living things to environmental
factors for the ultimate purpose of survival, reproduction, and an optimal
level of functioning.
Compensation
Mechanisms of Biological System when it exposed to many influences
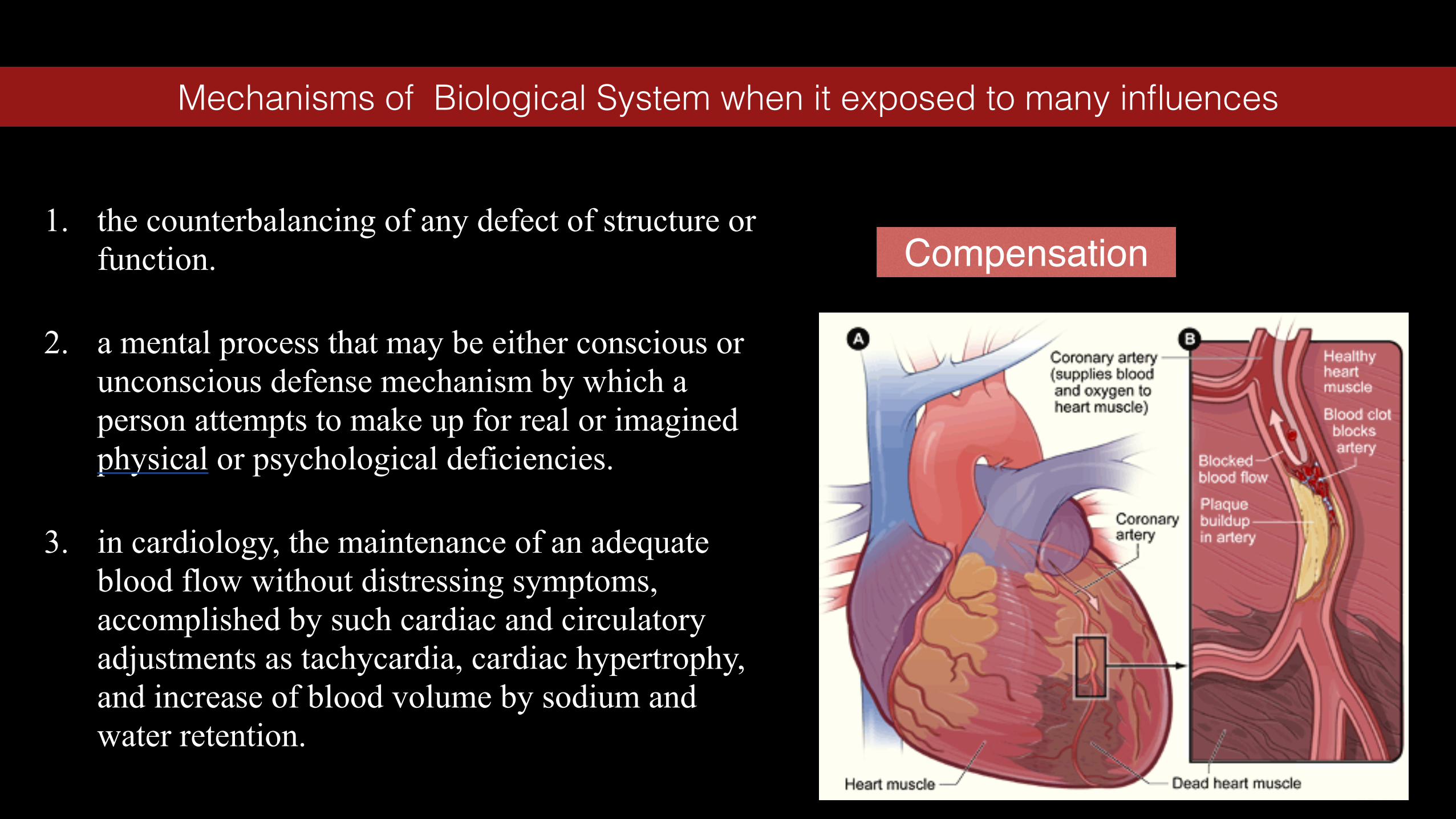
1. the counterbalancing of any defect of structure or function.
2. a mental process that may be either conscious or unconscious defense mechanism by which a person attempts to make up for real or imagined physical or psychological deficiencies.
3. in cardiology, the maintenance of an adequate blood flow without distressing symptoms, accomplished by such cardiac and circulatory adjustments as tachycardia, cardiac hypertrophy, and increase of blood volume by sodium and water retention.

Adaptation CompensationInfluences
Stat.occlusion Dyn.Occlusion Bruxism Dysfunction
Individual capacity for adaptation and compensation
Influences Duration Number Intensity Frequency

Dental treatment, including functional prophylactic measures
Physiological structures or progressive adaptation
Compensation
No definitive measures that affect the occlusion without further diagnostic
clarification
Dental treatment that will not upset the fragile equilibrium
Cause-related functional therapy prior to definitive dental treatment
Decompensationor
regressive adaptation
Functional therapy prior to definitive dental treatment
No occlusal functional therapy if thereare no occlusal etiological influences
Symptomatic functional therapy for the transition to a compensated status
1
3
2
The Role of Dentistry in Craniofacial Pain
psychological factors occlusal factorsVs
21
Every patient with head and neck pain should be seen by a dentist in order to clarify the following questions: Do the symptoms arise from a structure in the masticatory system (presence of a loading vector)? Is the loading vector related to the occlusion? Can the occlusion-related portion of the total loading vector be reduced with reasonable effort and expense? Would symptomatic treatment in the dental office be reasonable?
The Role of Dentistry in Craniofacial Pain

✤ Muscles ✤ Joint Capsule ✤ Disk
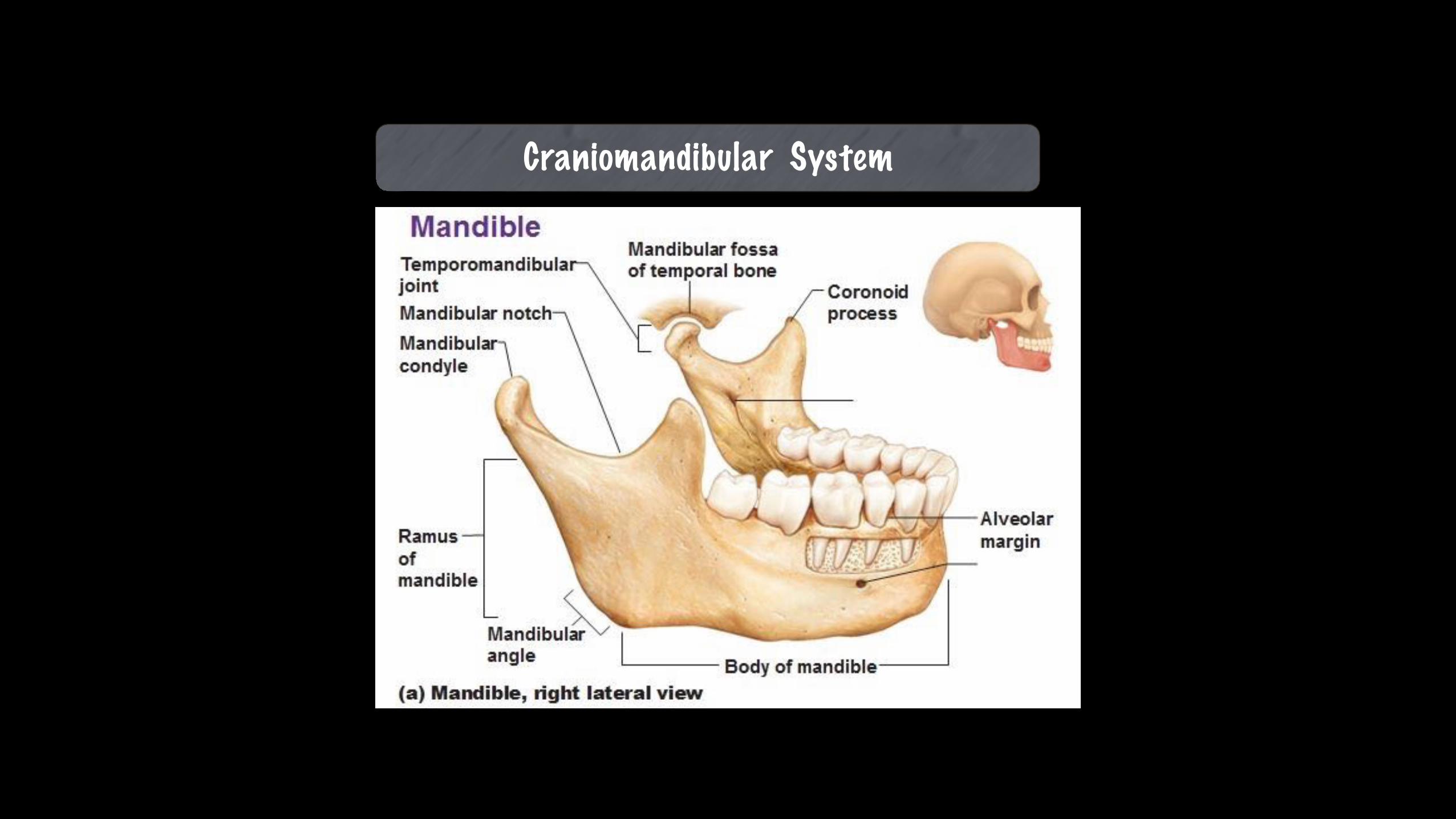
Craniomandibular System

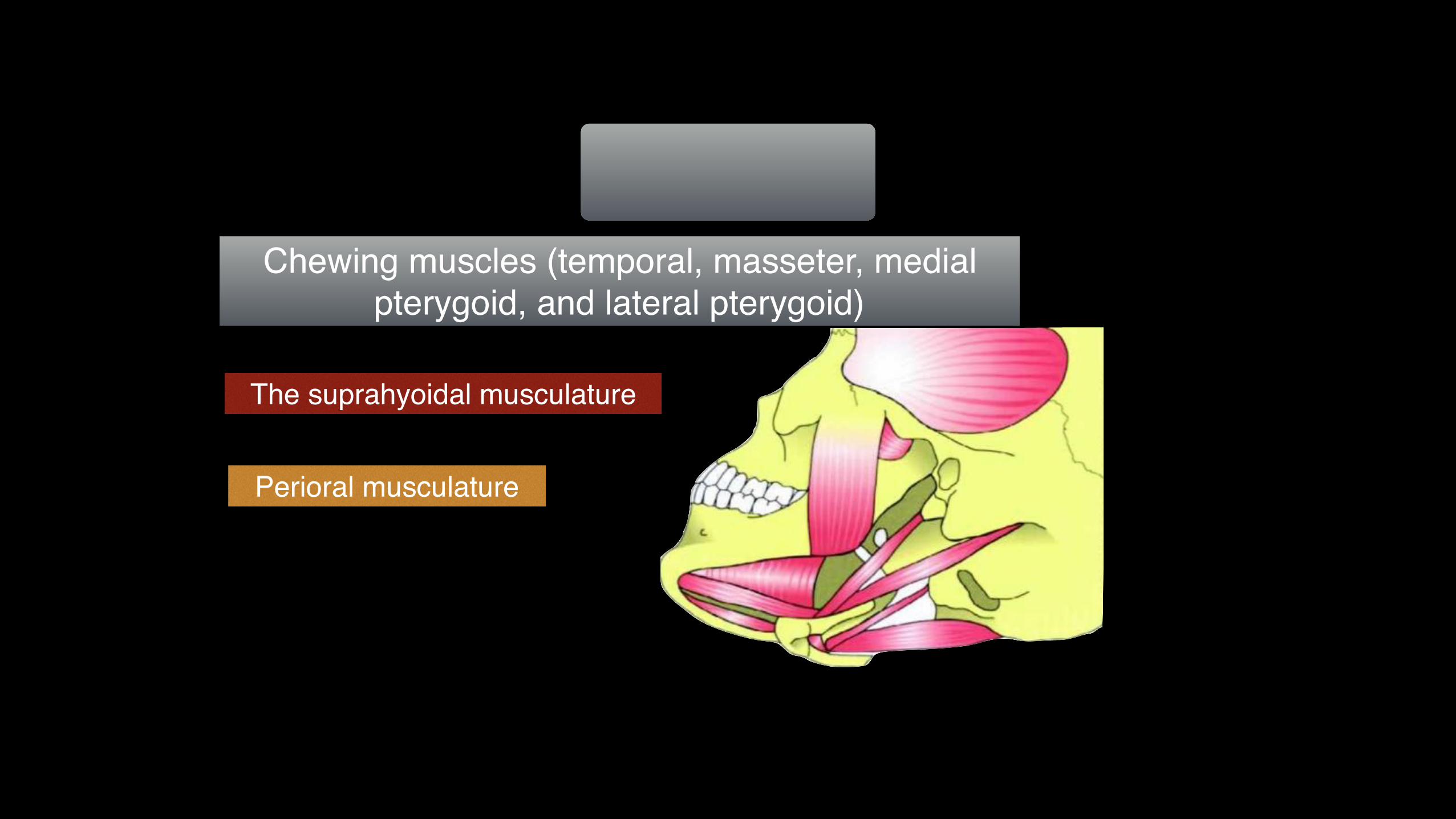
The suprahyoidal musculature
Chewing muscles (temporal, masseter, medial pterygoid, and lateral pterygoid)
Perioral musculature
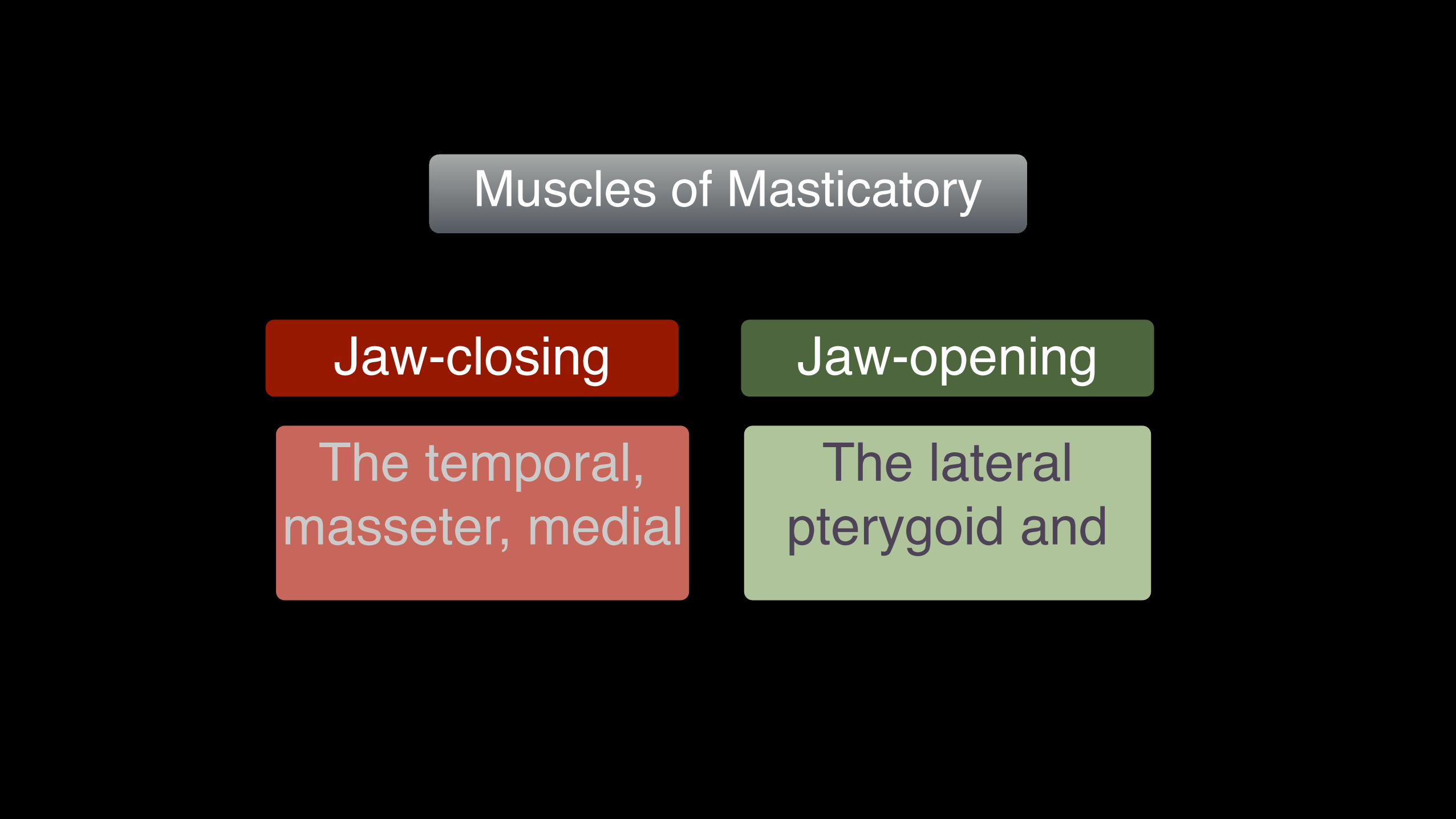
Jaw-closing
Muscles of Masticatory
The temporal, masseter, medial
The lateral pterygoid and
Jaw-opening

The muscle comprises a pars anterior (1), pars
media (2), and pars posterior (3).
The Temporal Muscle
Jaw
-Clo
sing
Muc
sles

The Masseter Muscle
Jaw
-Clo
sing
Muc
sles

The Masseter
Jaw
-Clo
sing
Muc
sles
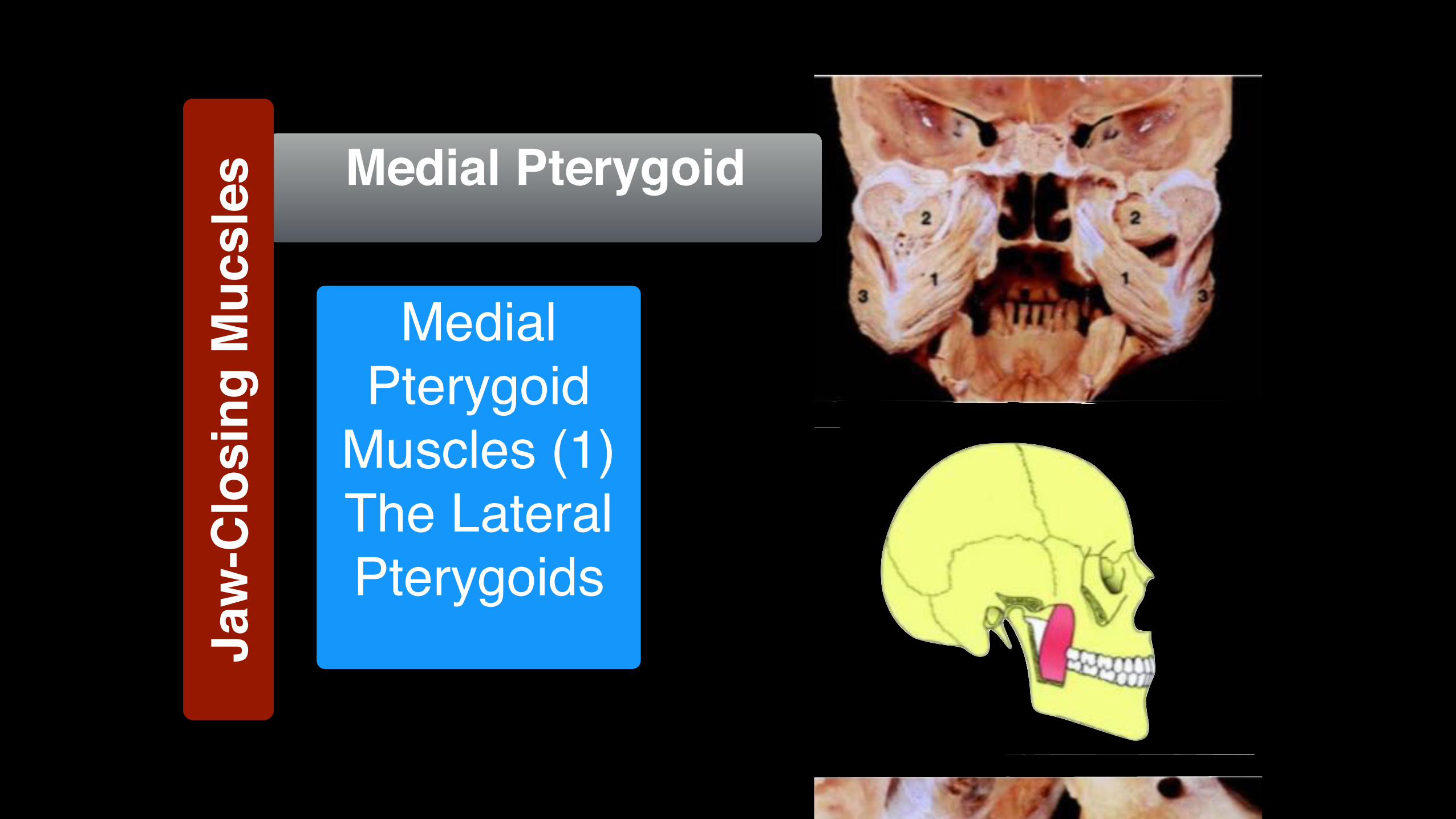
Medial Pterygoid
Medial Pterygoid
Muscles (1) The Lateral Pterygoids
Jaw
-Clo
sing
Muc
sles

Medial view
Medial Pterygoid
Jaw
-Clo
sing
Muc
sles
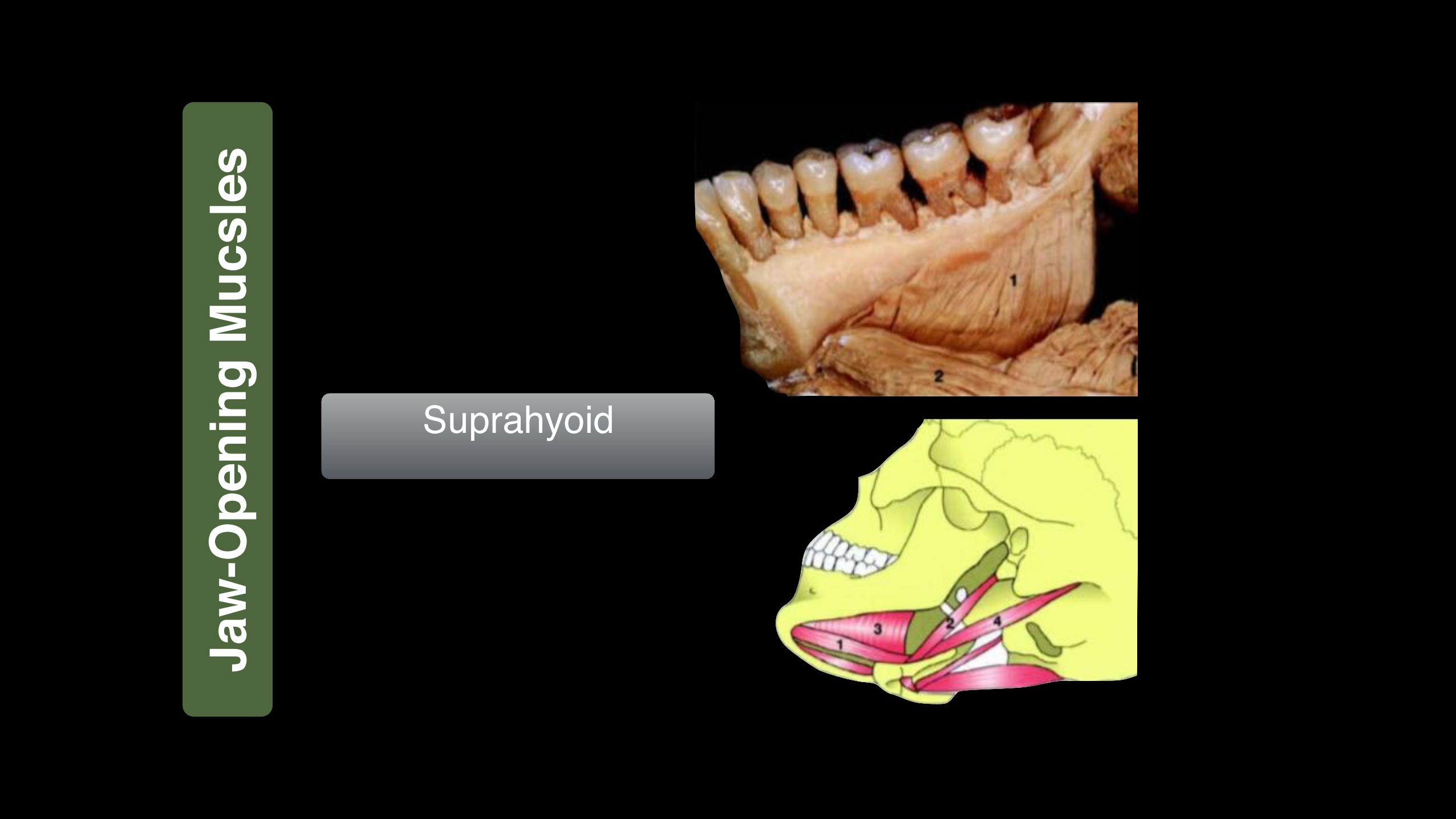
Suprahyoid
Jaw
-Ope
ning
Muc
sles

Posterior view
Suprahyoid Ja
w-O
peni
ng M
ucsl
es

Lateral Pterygoid Muscle
1 Upper head 2 Lower headEMG activity of the
muscles of mastication at rest
and during jaw
EMG activity during grinding of the teeth
Jaw
-Ope
ning
Muc
sles
?

the muscle becomes segmented into three parts in week 12 of embryonic development to form an upper (1), middle (2), and lower (3)
Lateral Pterygoid Muscle
Jaw
-Ope
ning
Muc
sles
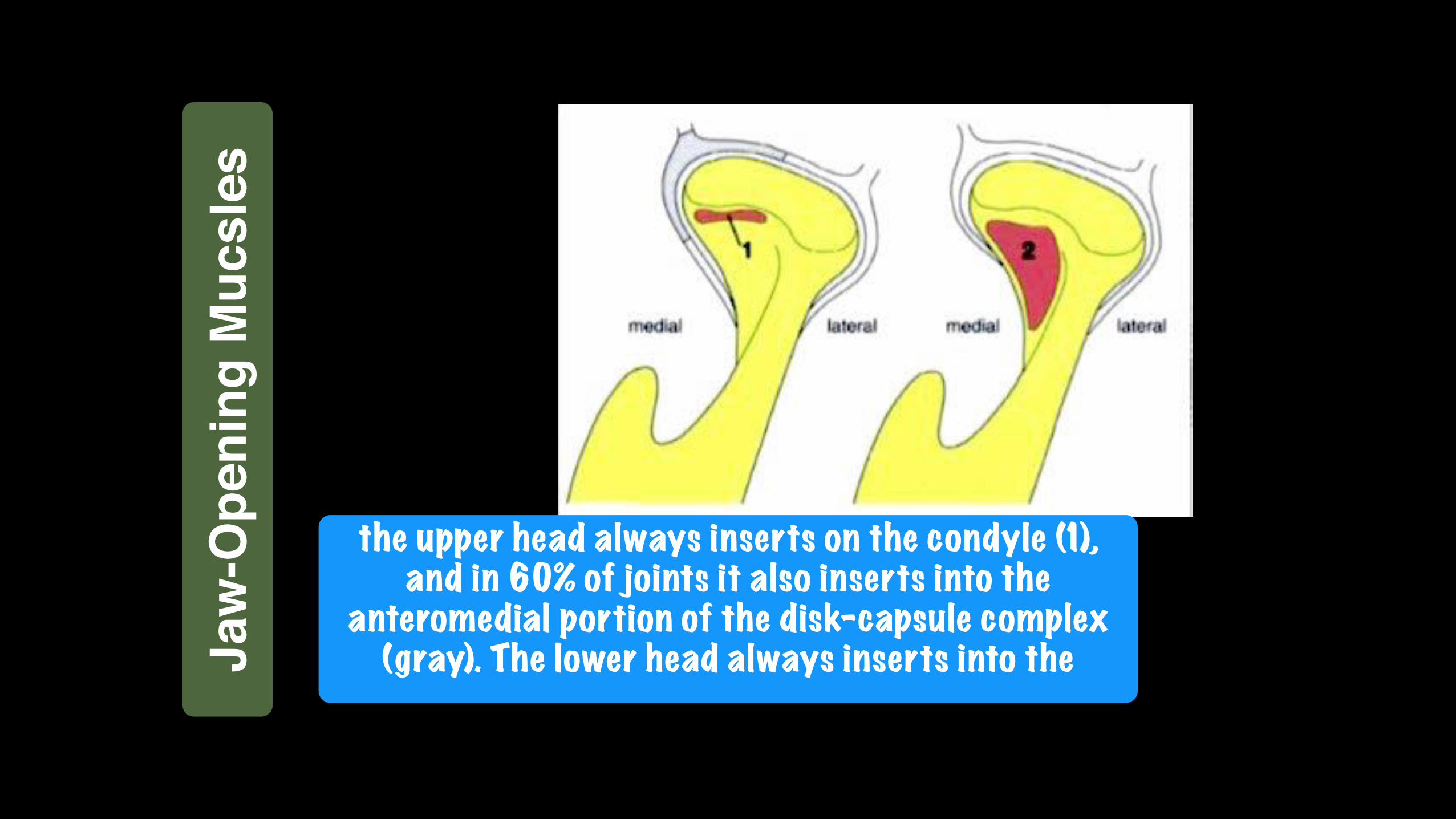
the upper head always inserts on the condyle (1), and in 60% of joints it also inserts into the
anteromedial portion of the disk-capsule complex (gray). The lower head always inserts into the Ja
w-O
peni
ng M
ucsl
es
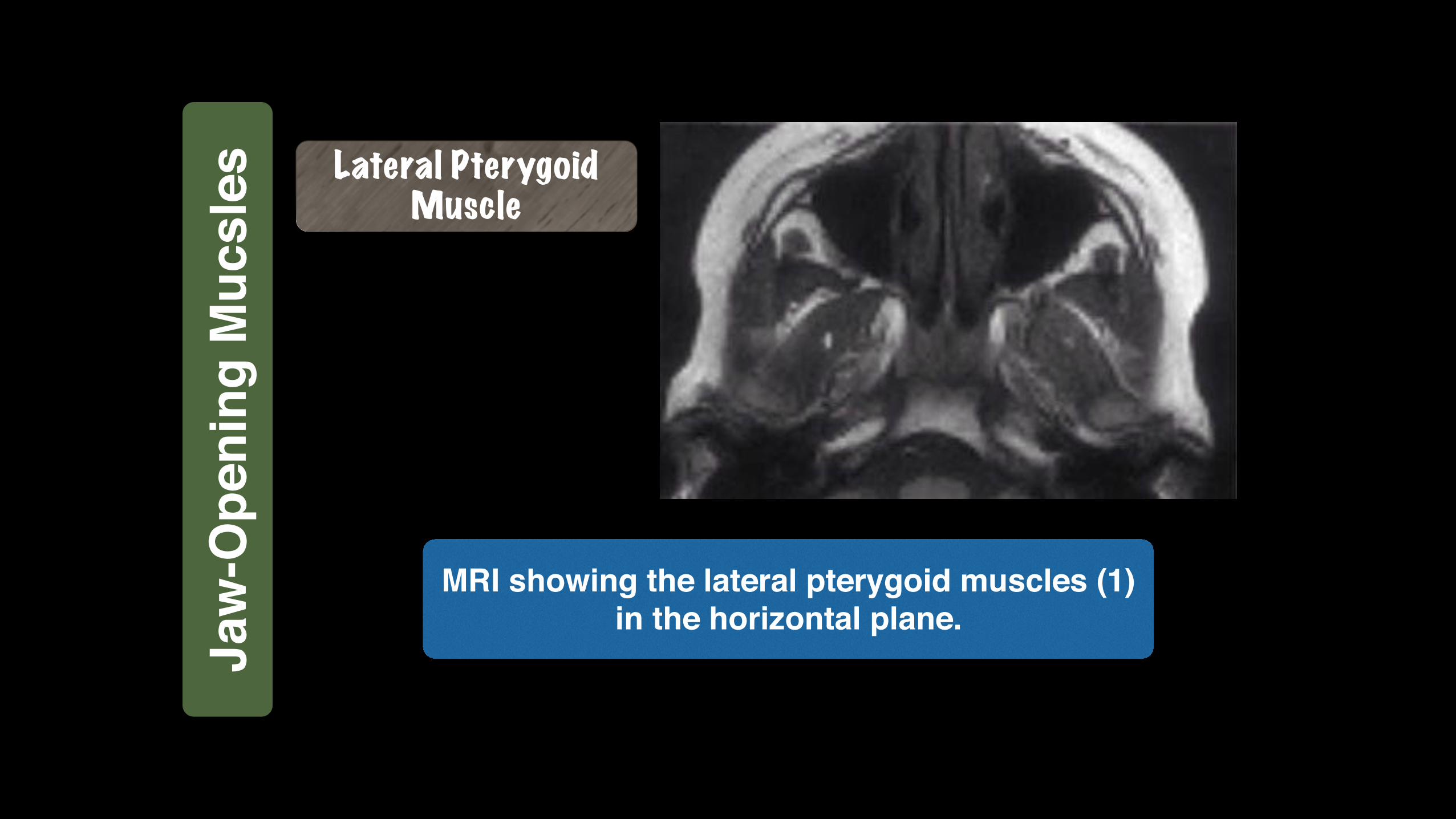
MRI showing the lateral pterygoid muscles (1) in the horizontal plane.
Lateral Pterygoid Muscle
Jaw
-Ope
ning
Muc
sles
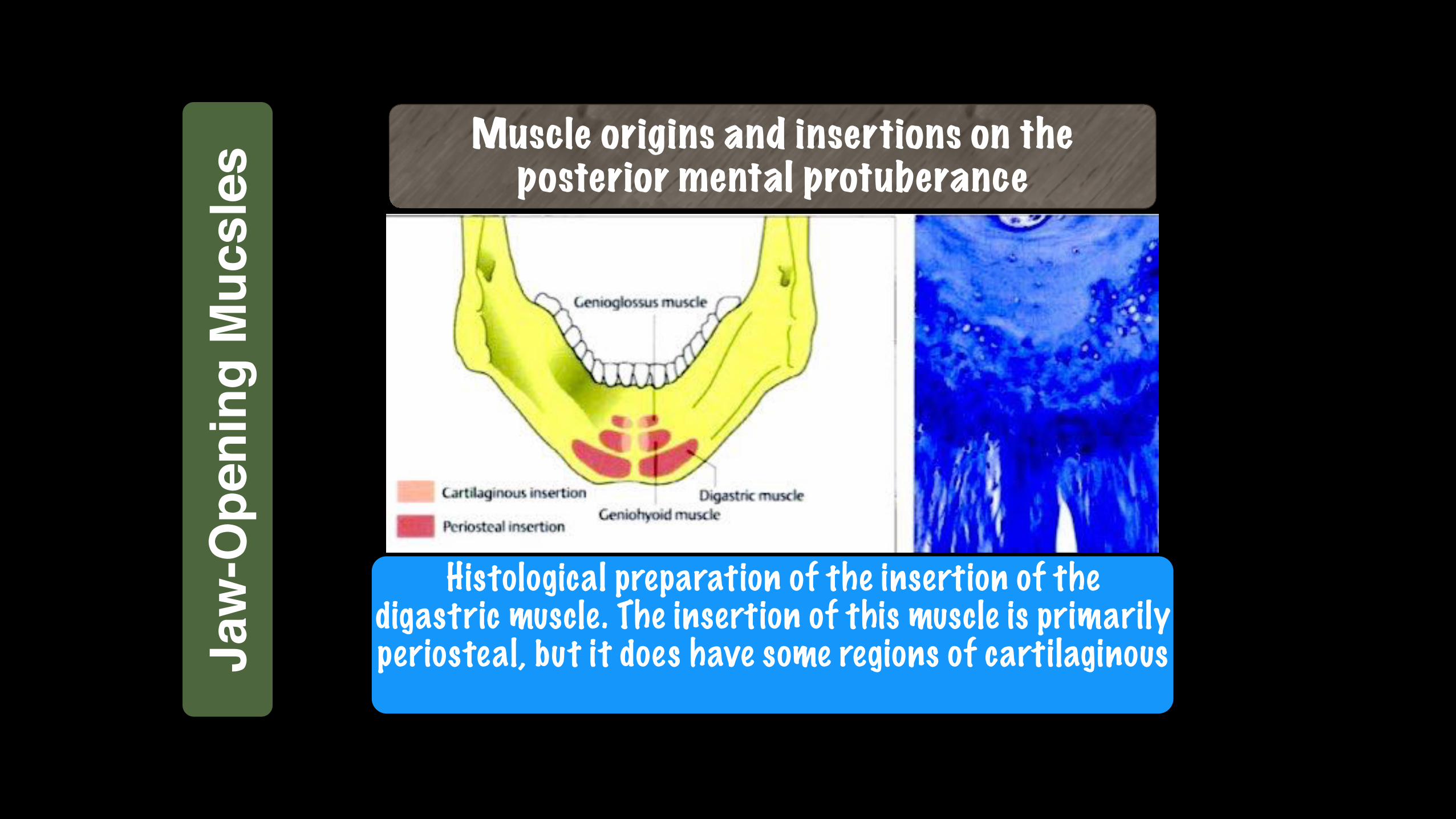
Muscle origins and insertions on the posterior mental protuberance
Histological preparation of the insertion of the digastric muscle. The insertion of this muscle is primarily periosteal, but it does have some regions of cartilaginous Ja
w-O
peni
ng M
ucsl
es
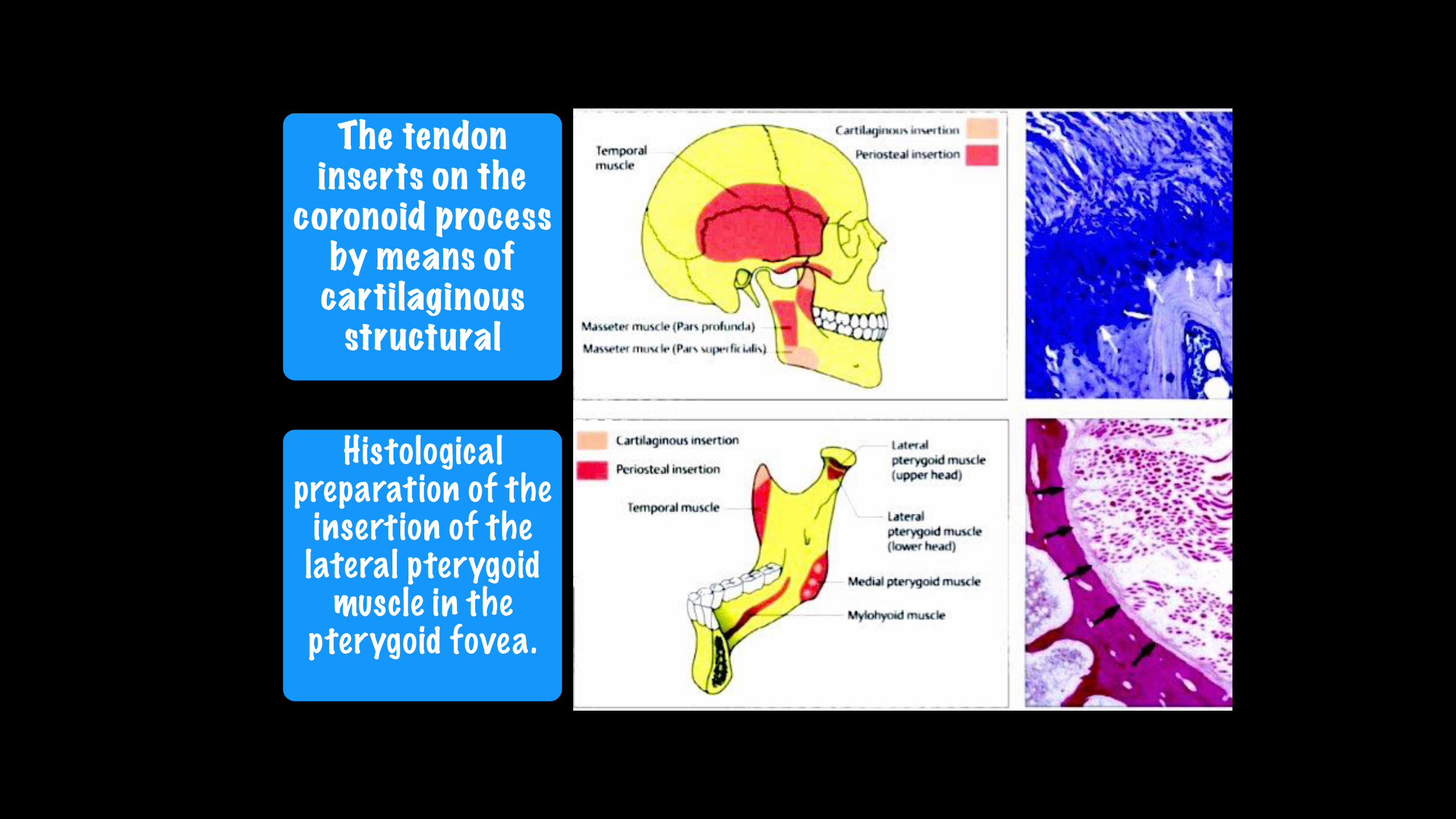
The tendon inserts on the
coronoid process by means of
cartilaginous structural
Histological preparation of the
insertion of the lateral pterygoid
muscle in the pterygoid fovea.
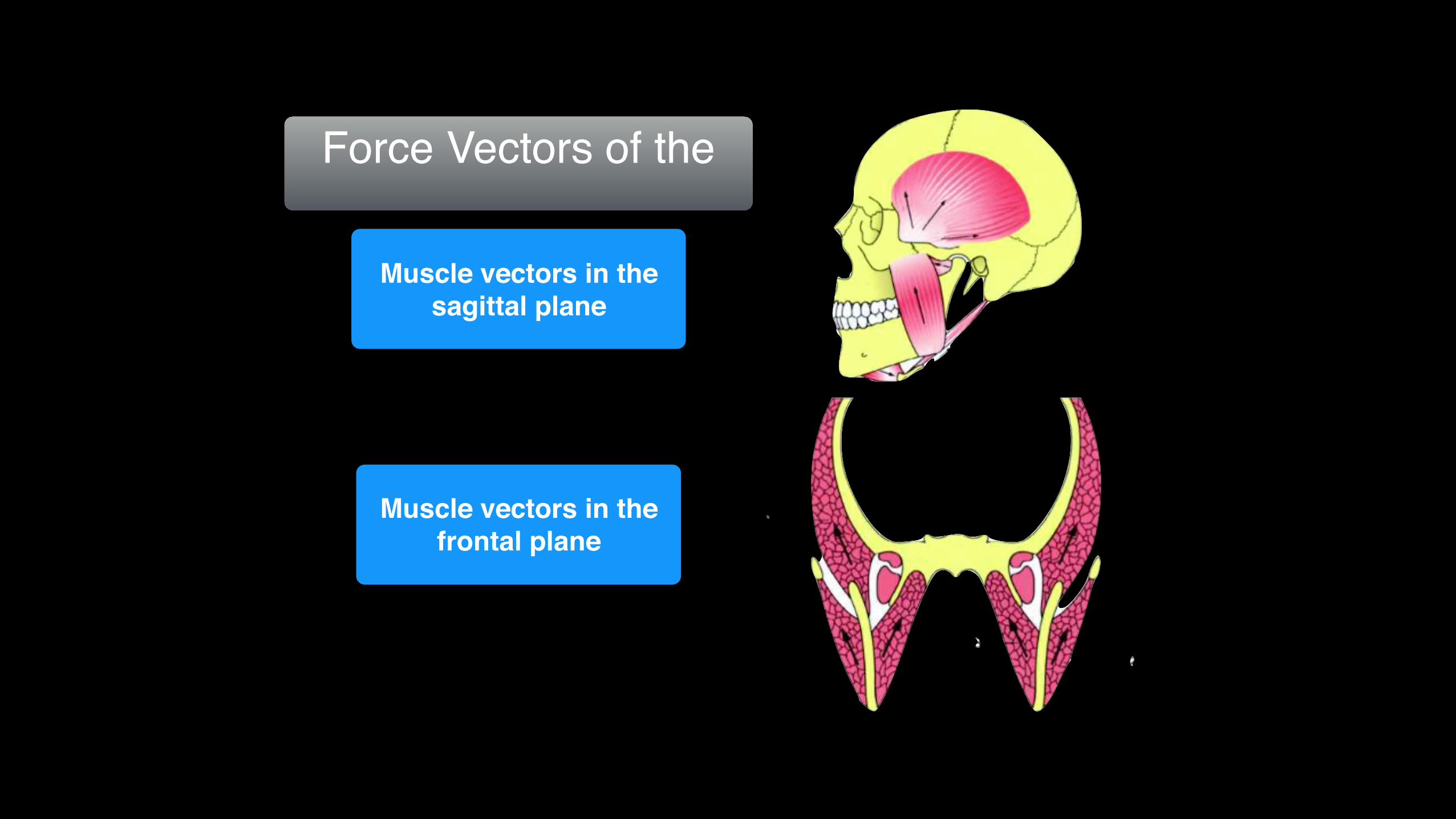
Force Vectors of the
Muscle vectors in the frontal plane
Muscle vectors in the sagittal plane
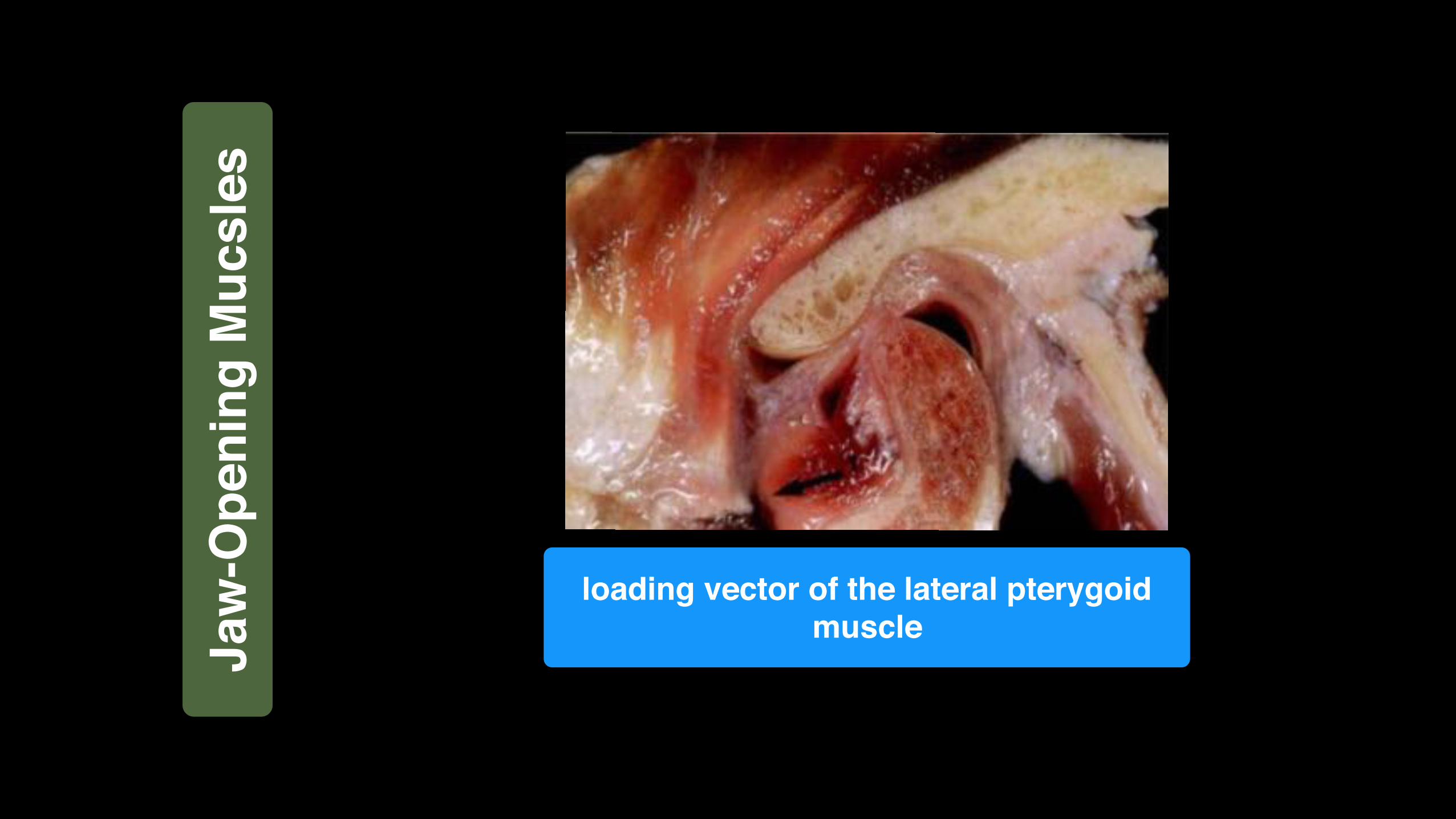
loading vector of the lateral pterygoid muscleJa
w-O
peni
ng M
ucsl
es
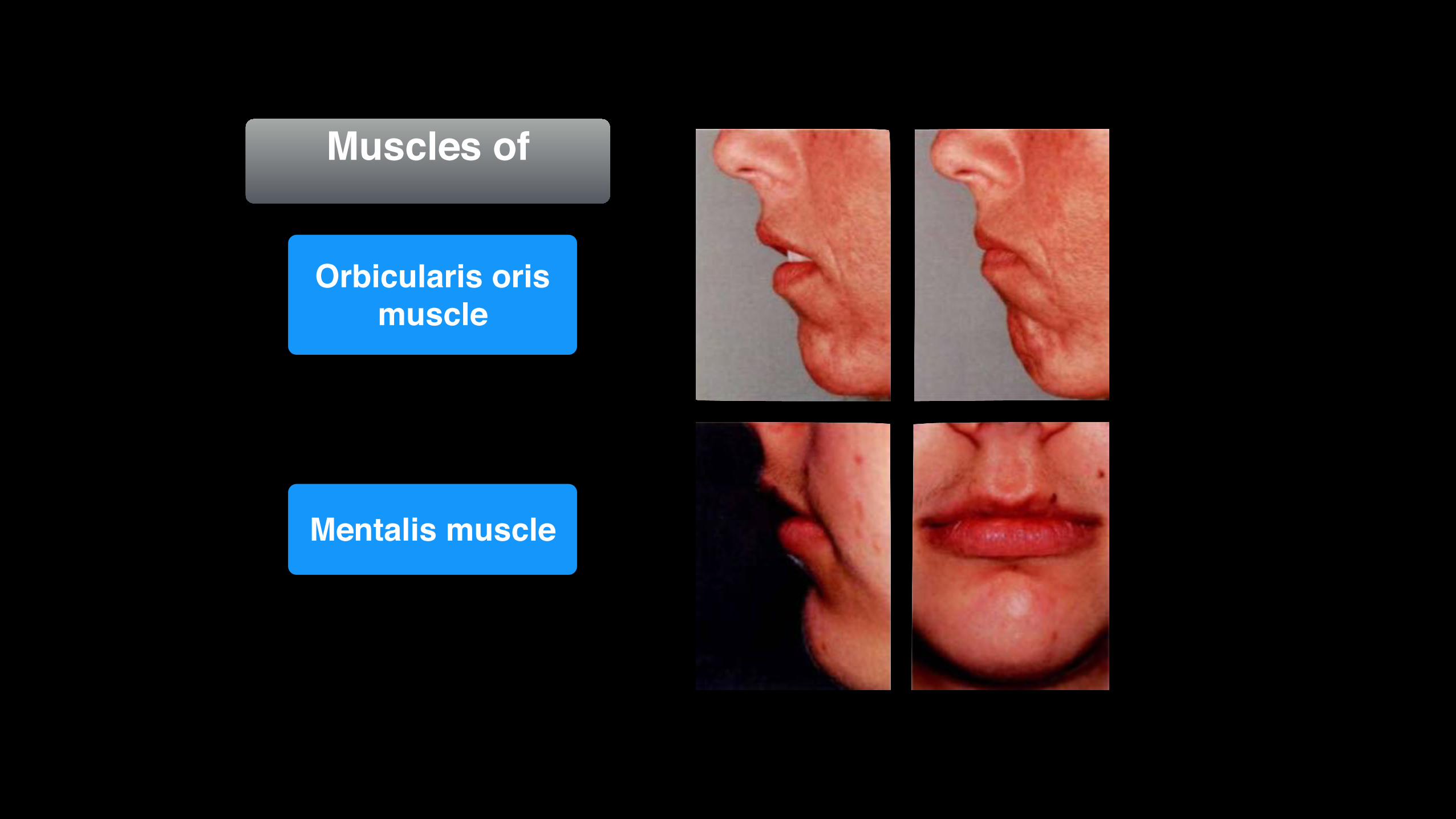
Muscles of
Mentalis muscle
Orbicularis oris muscle
Influence of head and body posture on the mandible . As an example, the sternocleidomastoid muscle is always active
during bruxism; however, an activity level of 50% is necessary in the masseter muscle before a 5% level is reached in the
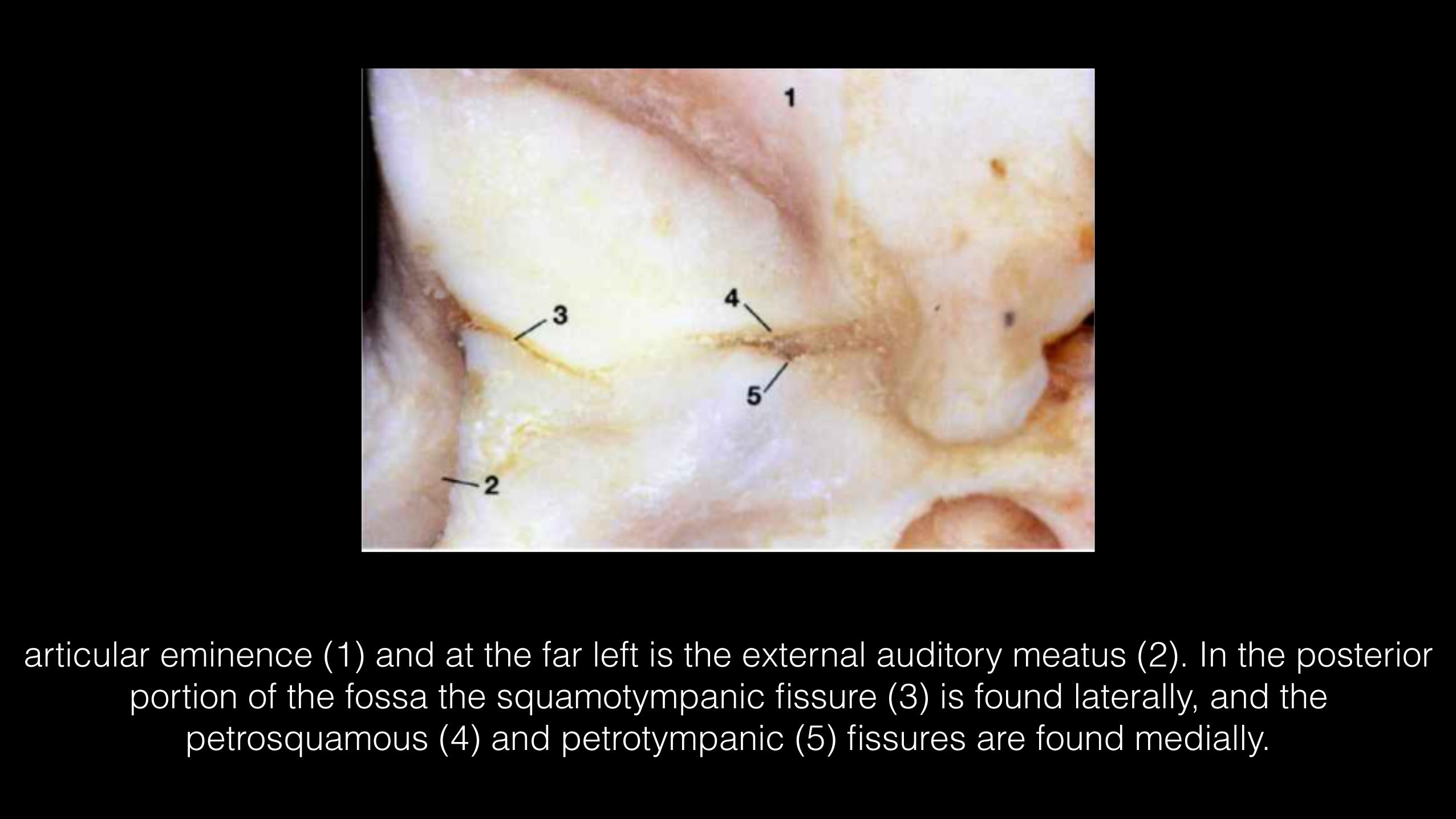
articular eminence (1) and at the far left is the external auditory meatus (2). In the posterior portion of the fossa the squamotympanic fissure (3) is found laterally, and the
petrosquamous (4) and petrotympanic (5) fissures are found medially.

These fissures are ossified in more than 95% of patients with disk displacement, whereas in joints without disk displacement normal fissure formation prevails (Bumann et al. 1991).
Squamotympanic fissure is completely ossified

Inferior view of the temporal cartilaginous joint surface and capsule attachment
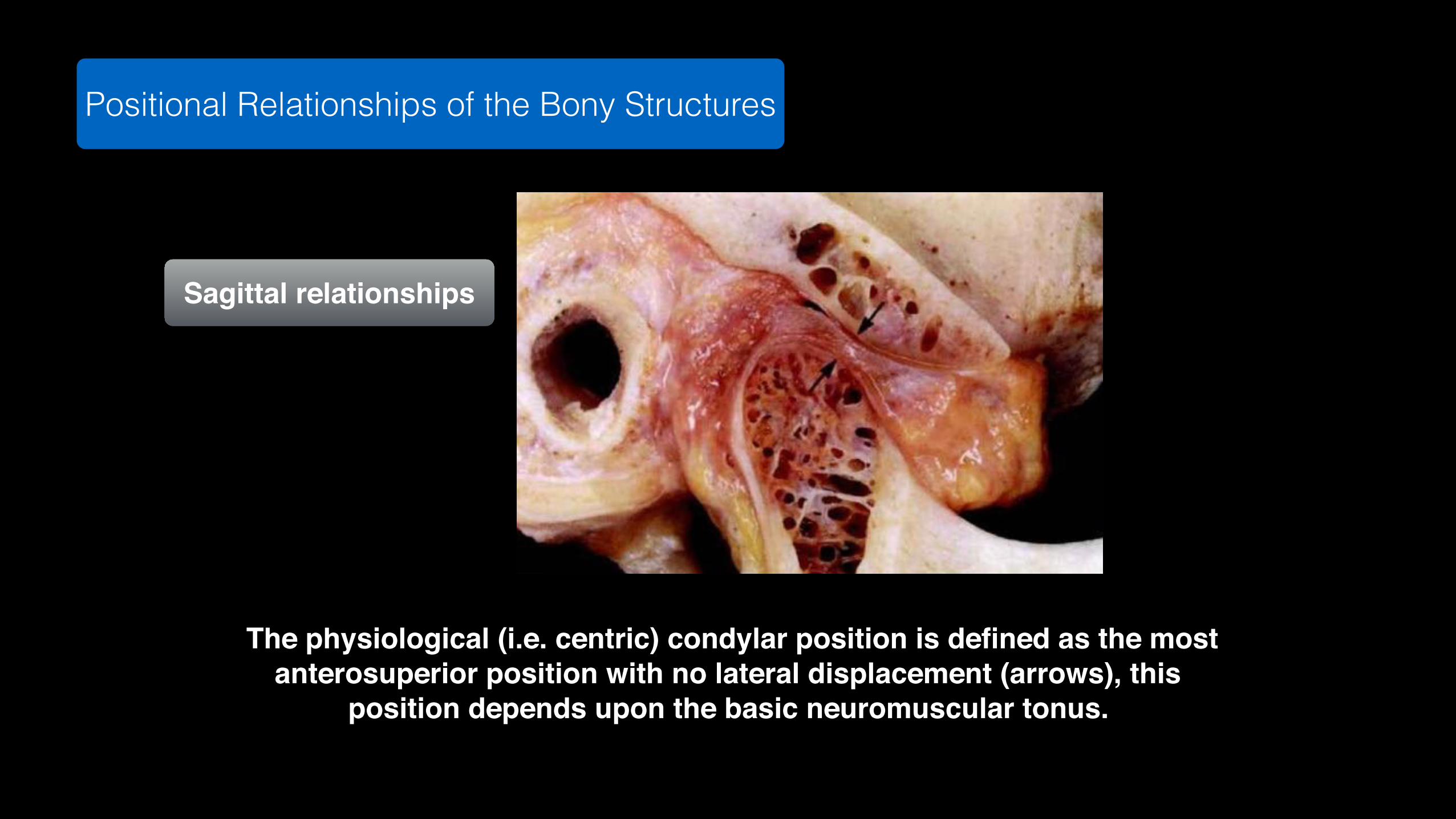
Positional Relationships of the Bony Structures
The physiological (i.e. centric) condylar position is defined as the most anterosuperior position with no lateral displacement (arrows), this
position depends upon the basic neuromuscular tonus.
Sagittal relationships

By applying artificial traction on the specimen, the anterior portions of the upper and lower joint capsules (arrows) have been made more clearly visible. Posteriorly the joint spaces are bounded
by the superior stratum (1) and inferior stratum (2). The posterior capsule wall lies behind the genu vasculosum. The type-Ill receptors of the capsule are only activated by heavy tensile loads
on the lateral ligament and serve then to stimulate the elevator muscles (Kraus 1994)
Joint capsule in the sagittal plane
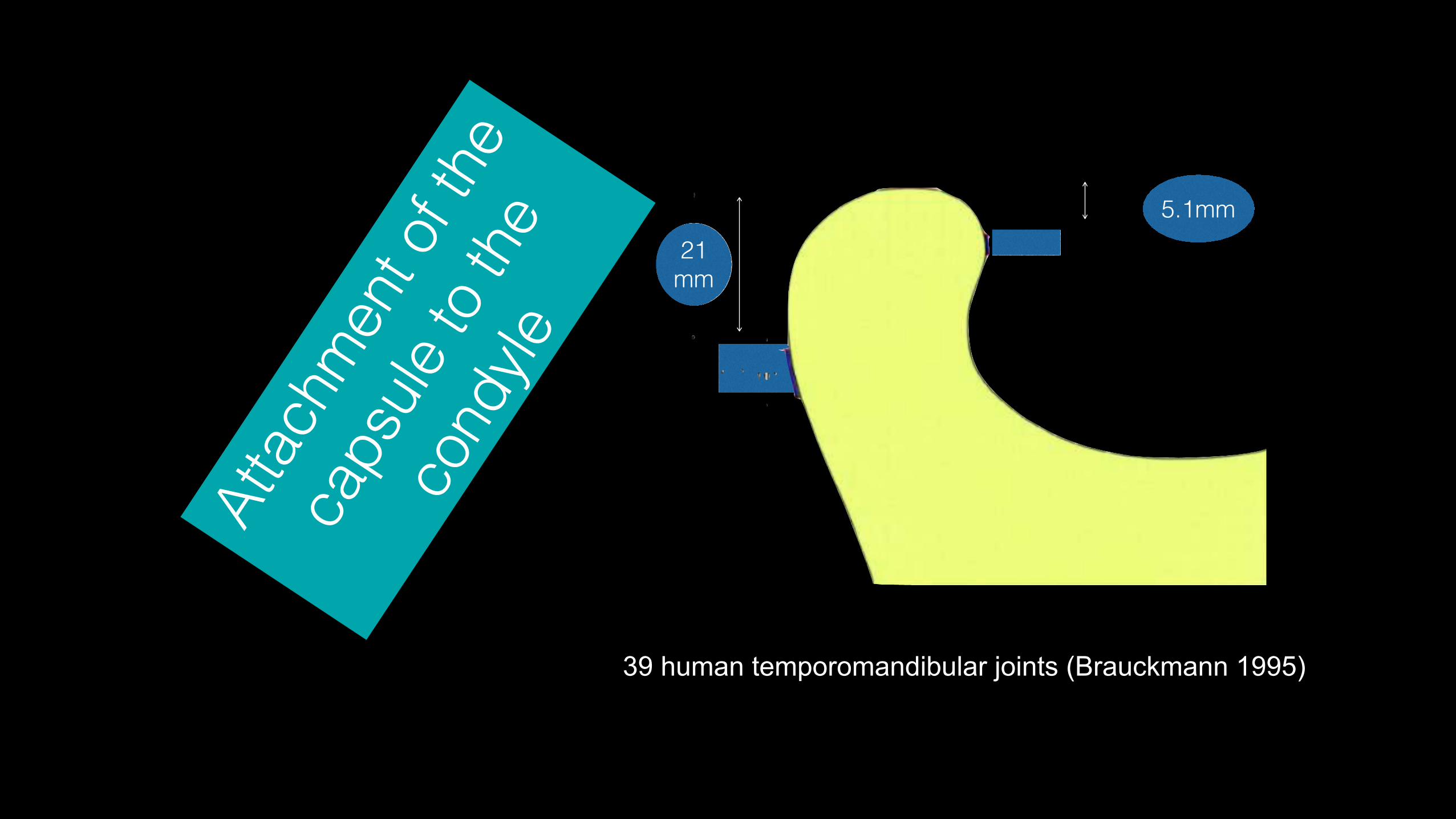
21 mm
5.1mmAt
tachm
ent o
f the
caps
ule to
the
cond
yle
39 human temporomandibular joints (Brauckmann 1995)

Overdistended capsuleAnterior disk displacement requires not only a stretching of the inferior stratum (1), but also a distention of the lower anterior wall of the joint capsule (arrows). However, because the connective tissue of the anterior capsule wall is much looser, disk displacement depends almost exclusively on posterior loading
vectors and the adaptability of the inferior stratum. A downward movement of the condyle as shown here without downward movement of the disk is possible only
with extensive stretching of the inferior stratum.

(Solberg et al, 1985, Bermejo et al. 1992) identify two separate connective tissue structures for attachment to the condyle, one for
the disk (1) and the other for the capsule (2).
Disk
and c
apule
attac
hmen
ts in
the
fronta
l plan
e
"diskocapsular system" (Dauber 1987)
Dr.Samer F.Mheissen
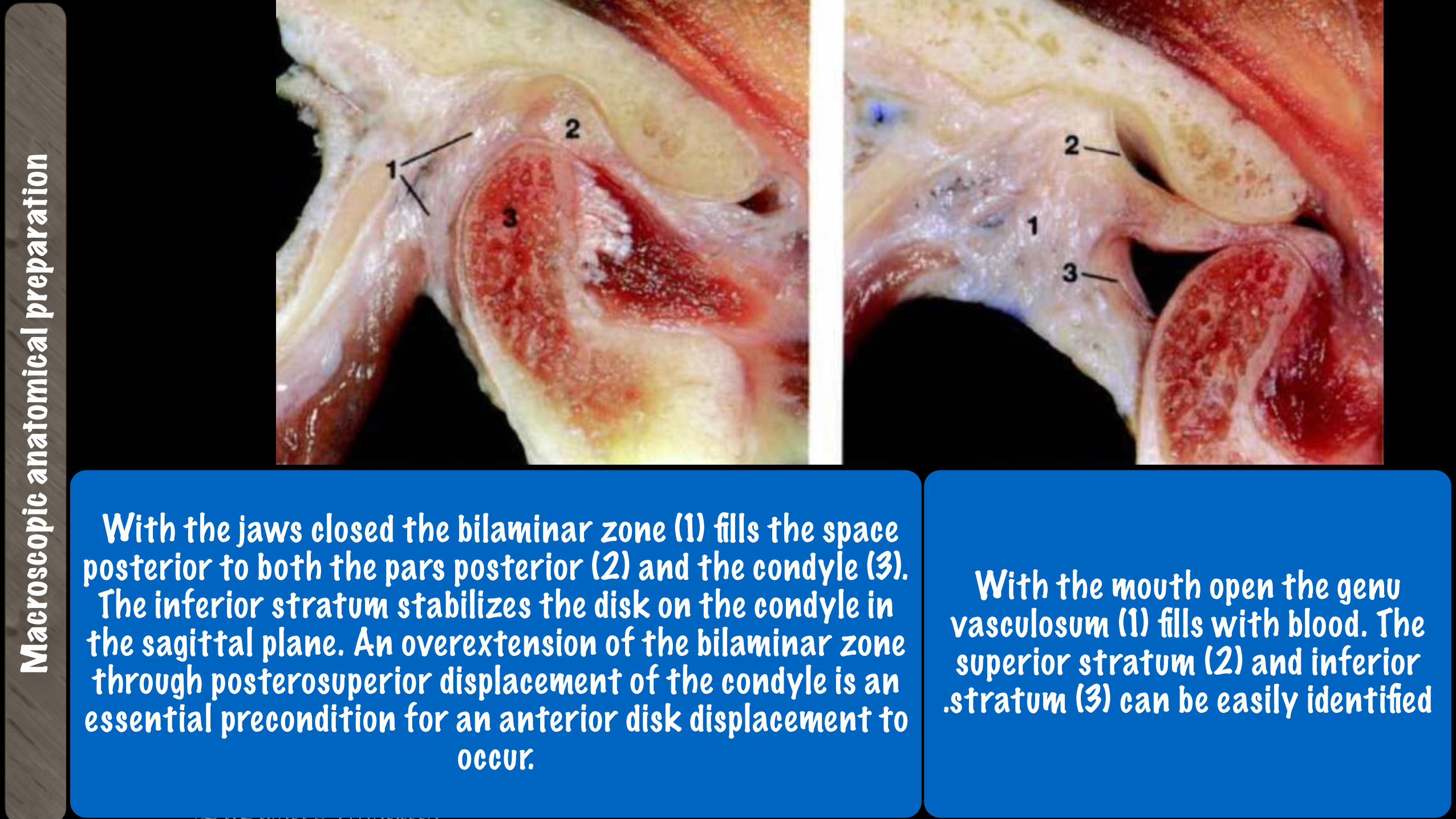
Mac
rosc
opic
anat
omica
l pre
para
tion
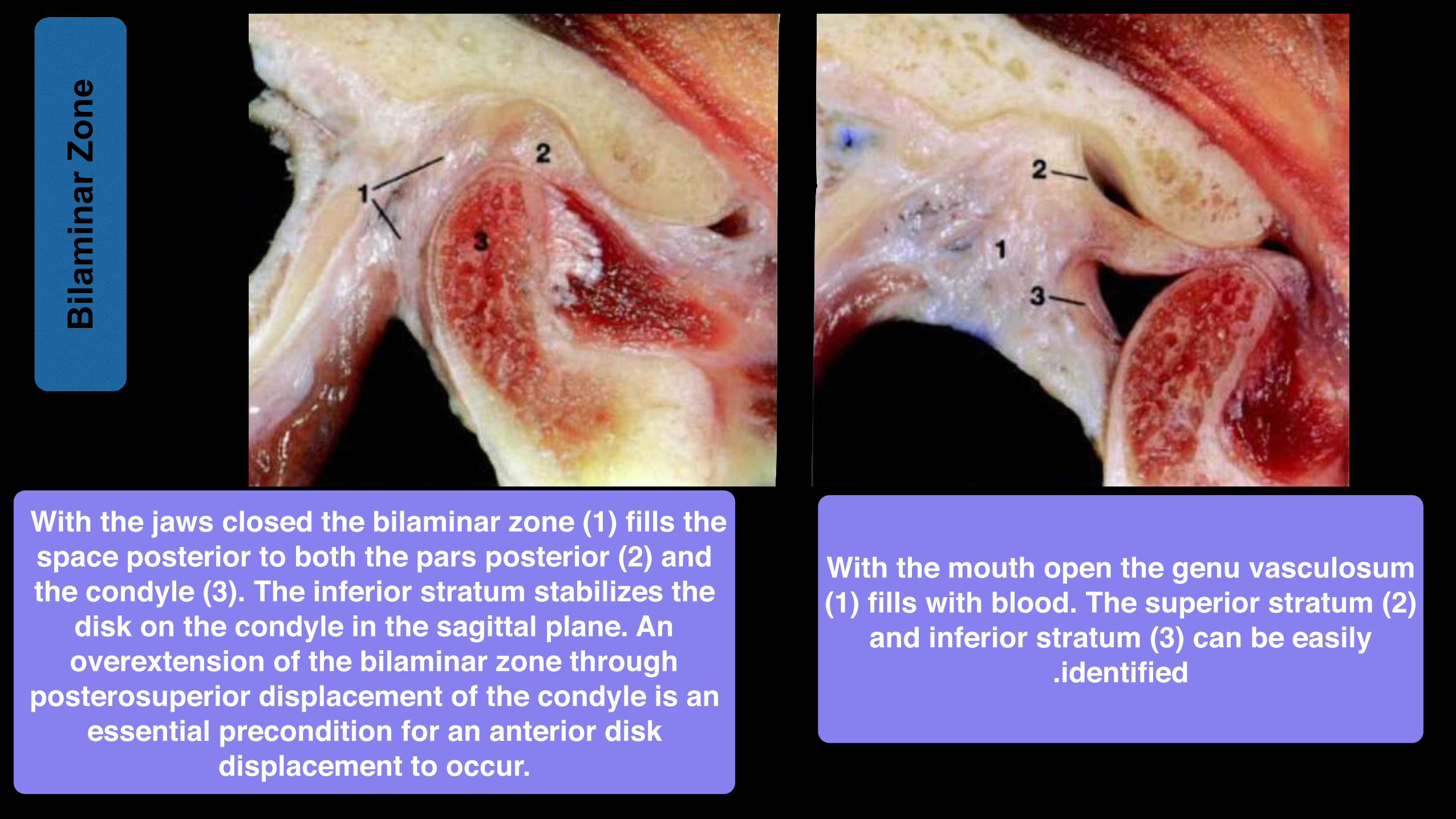
With the jaws closed the bilaminar zone (1) fills the space posterior to both the pars posterior (2) and the condyle (3). The inferior stratum stabilizes the disk on the condyle in
the sagittal plane. An overextension of the bilaminar zone through posterosuperior displacement of the condyle is an essential precondition for an anterior disk displacement to
occur.
With the mouth open the genu vasculosum (1) fills with blood. The superior stratum (2) and inferior.stratum (3) can be easily identified

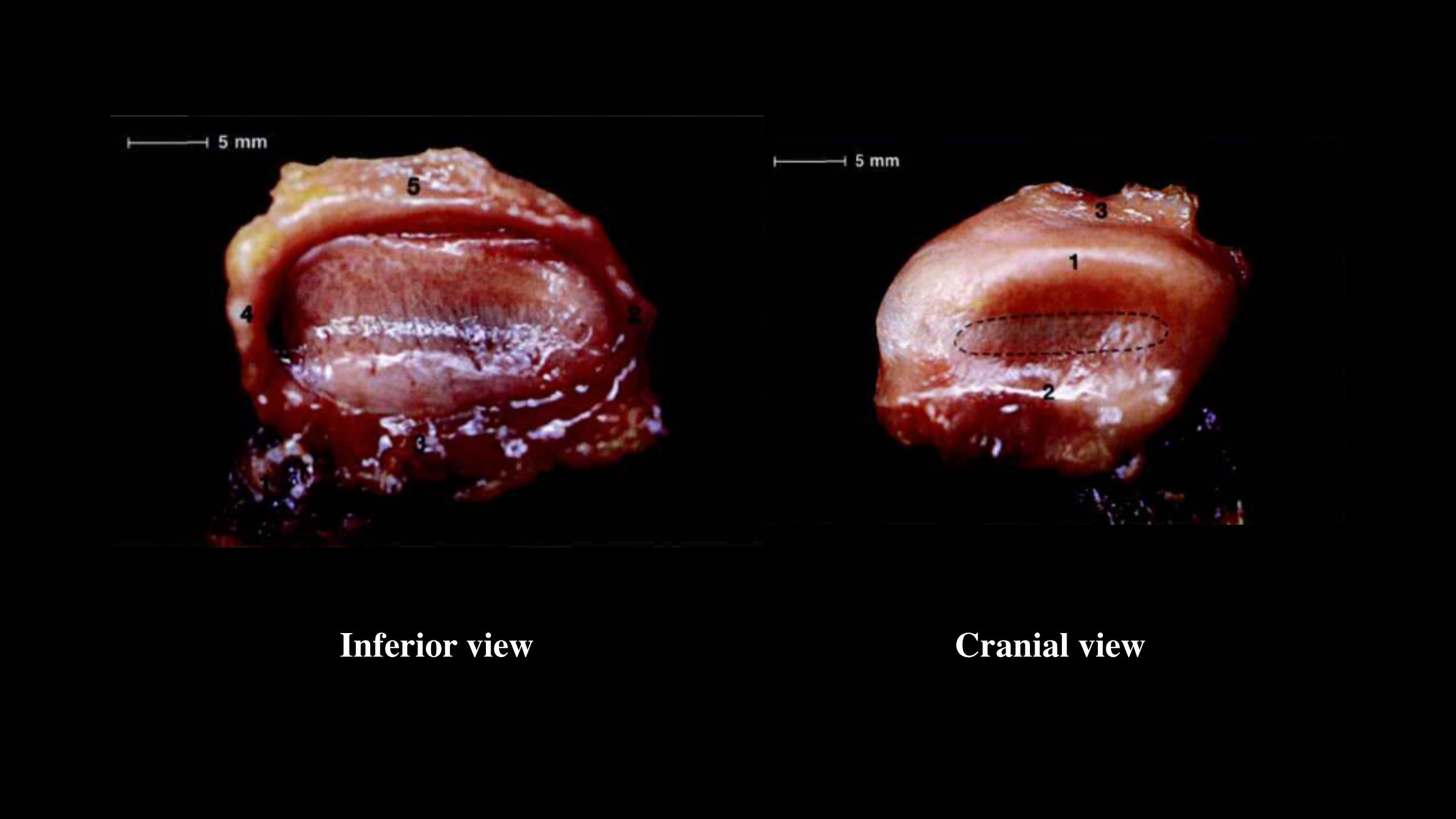
Inferior view Cranial view
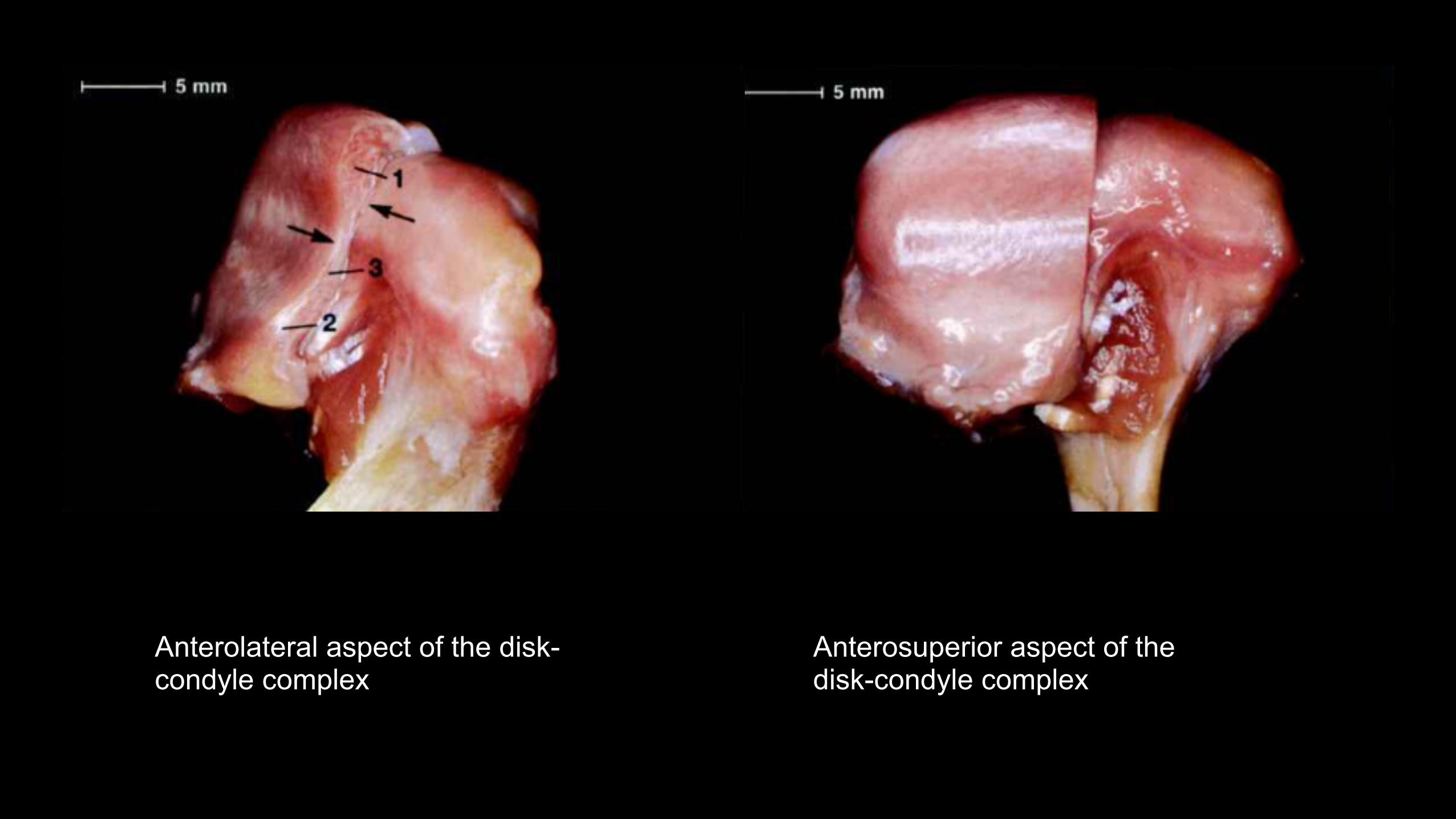
Anterosuperior aspect of the disk-condyle complex
Anterolateral aspect of the disk-condyle complex
With the jaws closed the bilaminar zone (1) fills the space posterior to both the pars posterior (2) and the condyle (3). The inferior stratum stabilizes the
disk on the condyle in the sagittal plane. An overextension of the bilaminar zone through
posterosuperior displacement of the condyle is an essential precondition for an anterior disk
displacement to occur.
With the mouth open the genu vasculosum (1) fills with blood. The superior stratum (2)
and inferior stratum (3) can be easily.identified
Bila
min
ar Z
one

Three Main Functions: 1. Stabilization 2. Guidance of Movement. 3. Limitation of Movement
Ligaments
What is the most important function ???

Lateral ligament
Lateral ligament
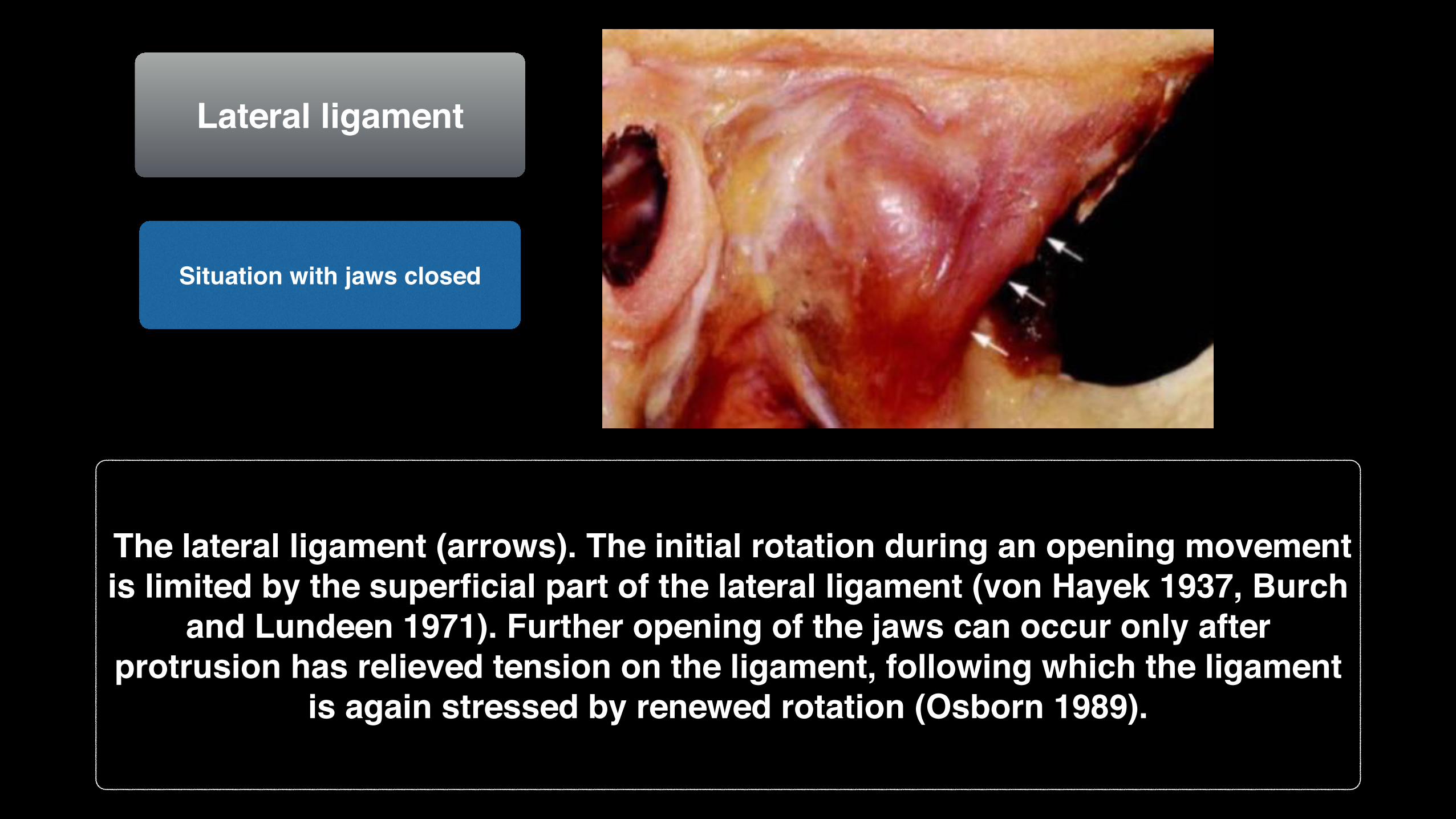
The lateral ligament (arrows). The initial rotation during an opening movement is limited by the superficial part of the lateral ligament (von Hayek 1937, Burch
and Lundeen 1971). Further opening of the jaws can occur only after protrusion has relieved tension on the ligament, following which the ligament
is again stressed by renewed rotation (Osborn 1989).
Situation with jaws closed
Lateral ligament
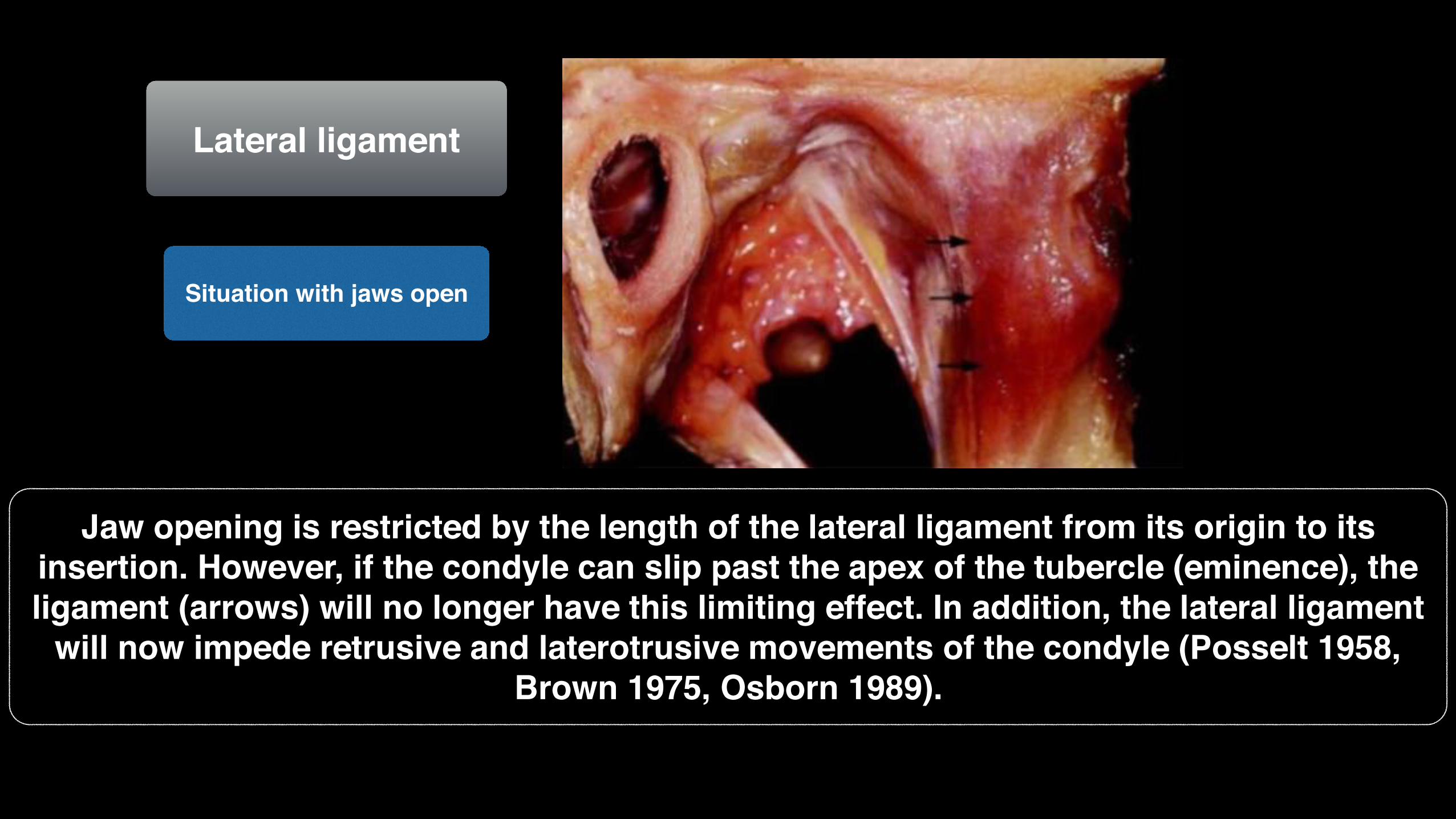
Situation with jaws open
Jaw opening is restricted by the length of the lateral ligament from its origin to its insertion. However, if the condyle can slip past the apex of the tubercle (eminence), the ligament (arrows) will no longer have this limiting effect. In addition, the lateral ligament
will now impede retrusive and laterotrusive movements of the condyle (Posselt 1958, Brown 1975, Osborn 1989).

Stylomandibular ligament
Situation during rotational jaw opening
Situation with jaws closed
Situation during translation
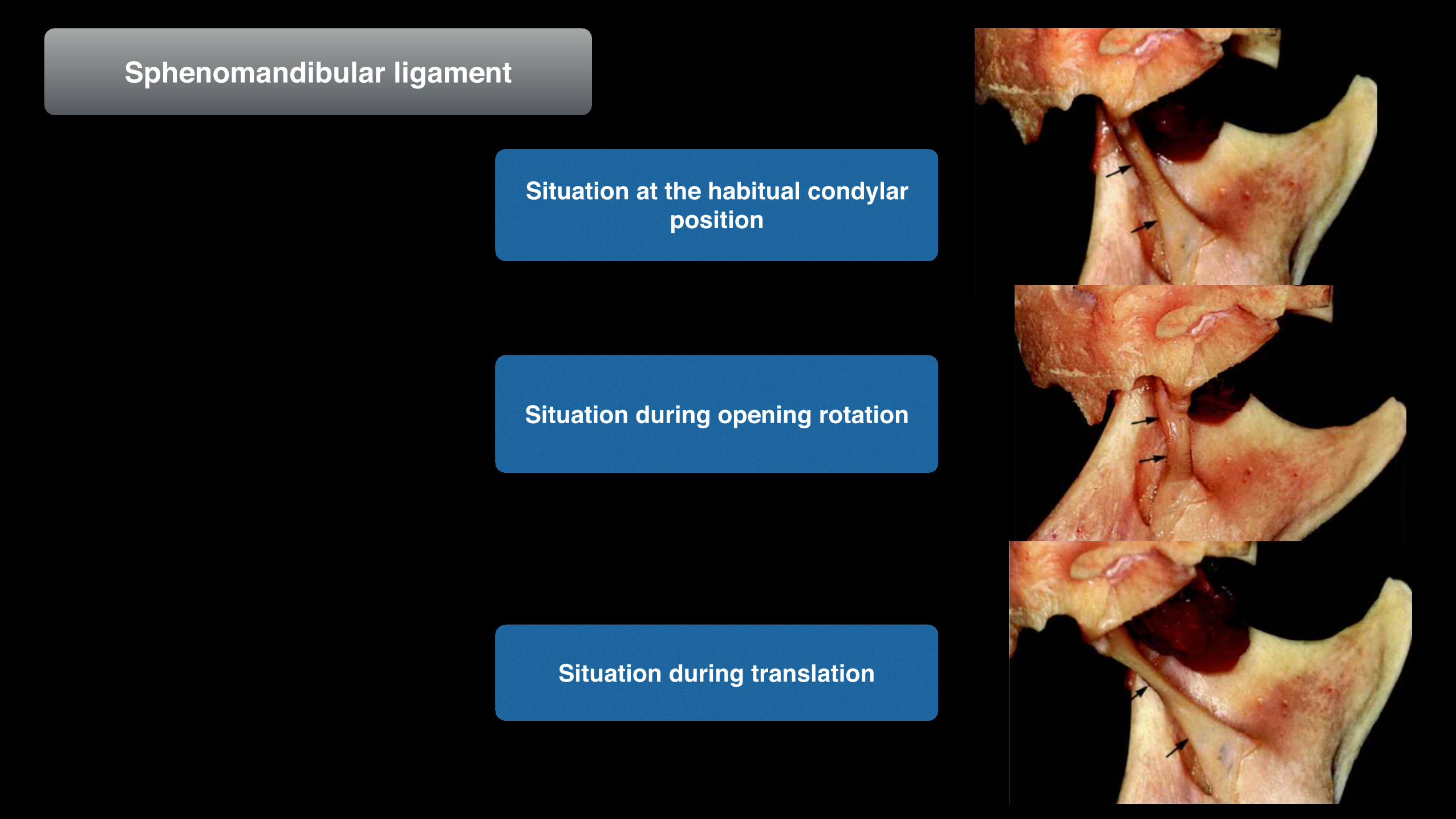
Sphenomandibular ligament
Situation during opening rotation
Situation at the habitual condylar position
Situation during translation
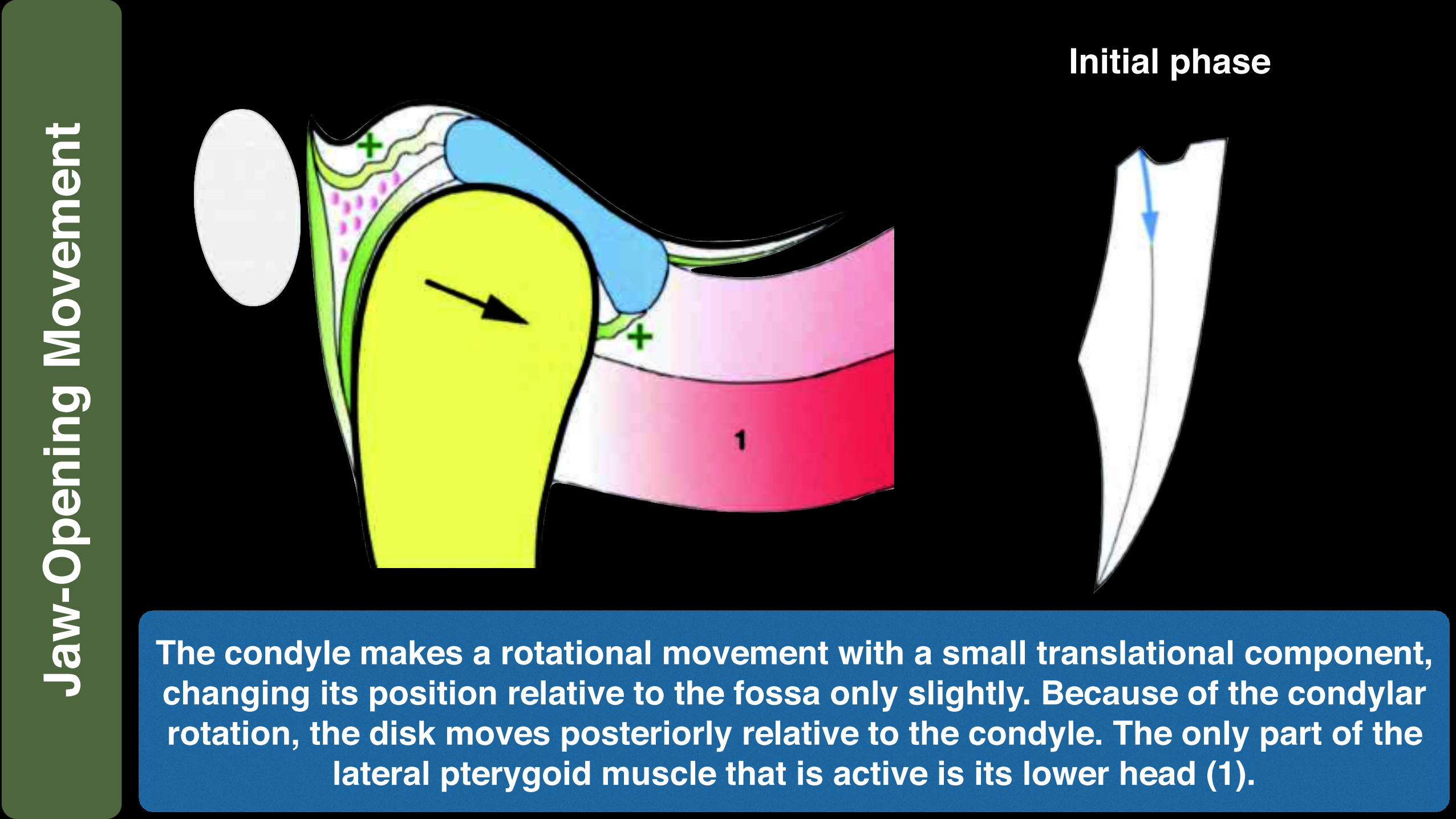
Initial phase
The condyle makes a rotational movement with a small translational component, changing its position relative to the fossa only slightly. Because of the condylar rotation, the disk moves posteriorly relative to the condyle. The only part of the
lateral pterygoid muscle that is active is its lower head (1).
Jaw
-Ope
ning
Mov
emen
t
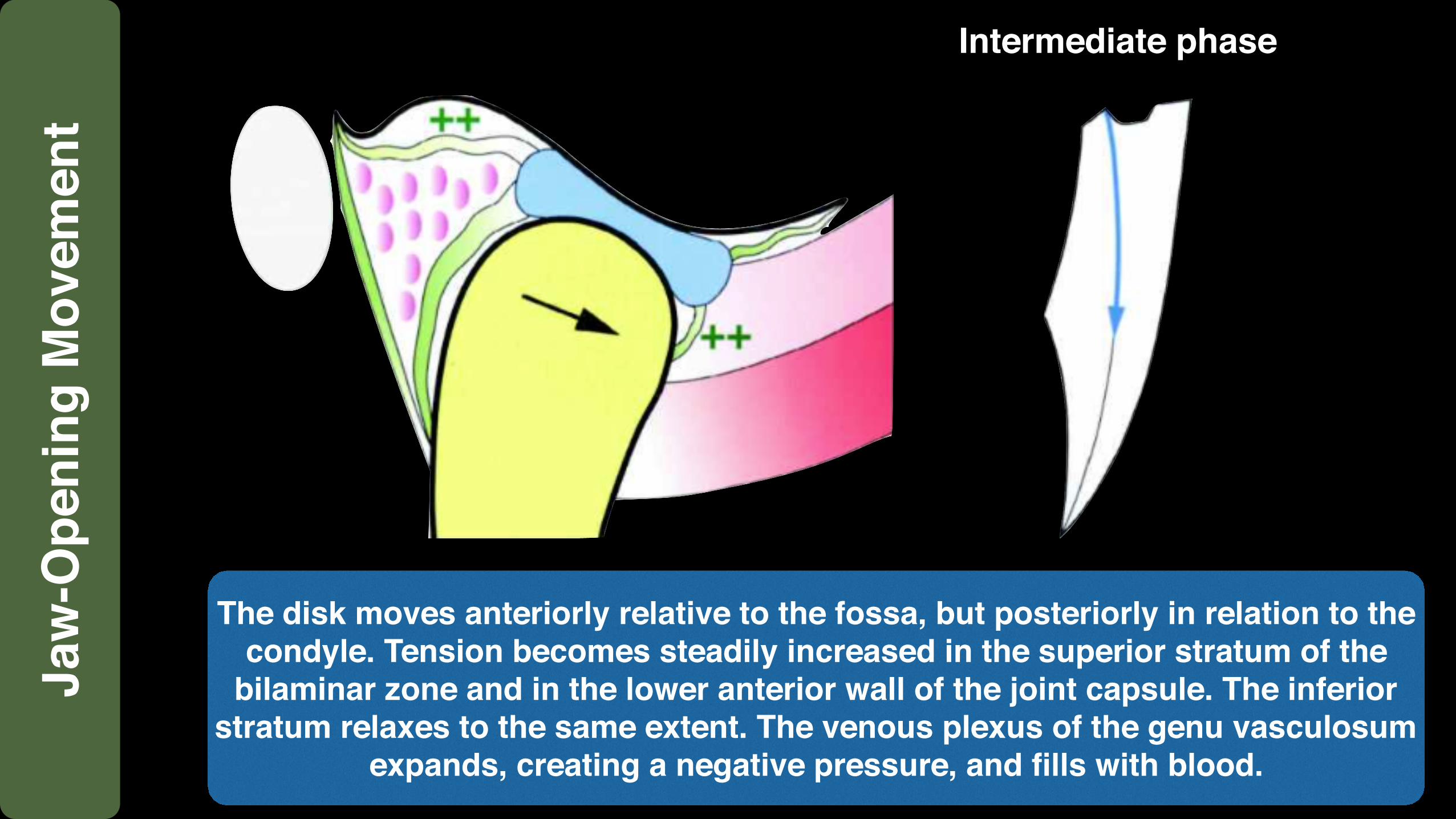
Intermediate phase
The disk moves anteriorly relative to the fossa, but posteriorly in relation to the condyle. Tension becomes steadily increased in the superior stratum of the
bilaminar zone and in the lower anterior wall of the joint capsule. The inferior stratum relaxes to the same extent. The venous plexus of the genu vasculosum
expands, creating a negative pressure, and fills with blood.
Jaw
-Ope
ning
Mov
emen
t
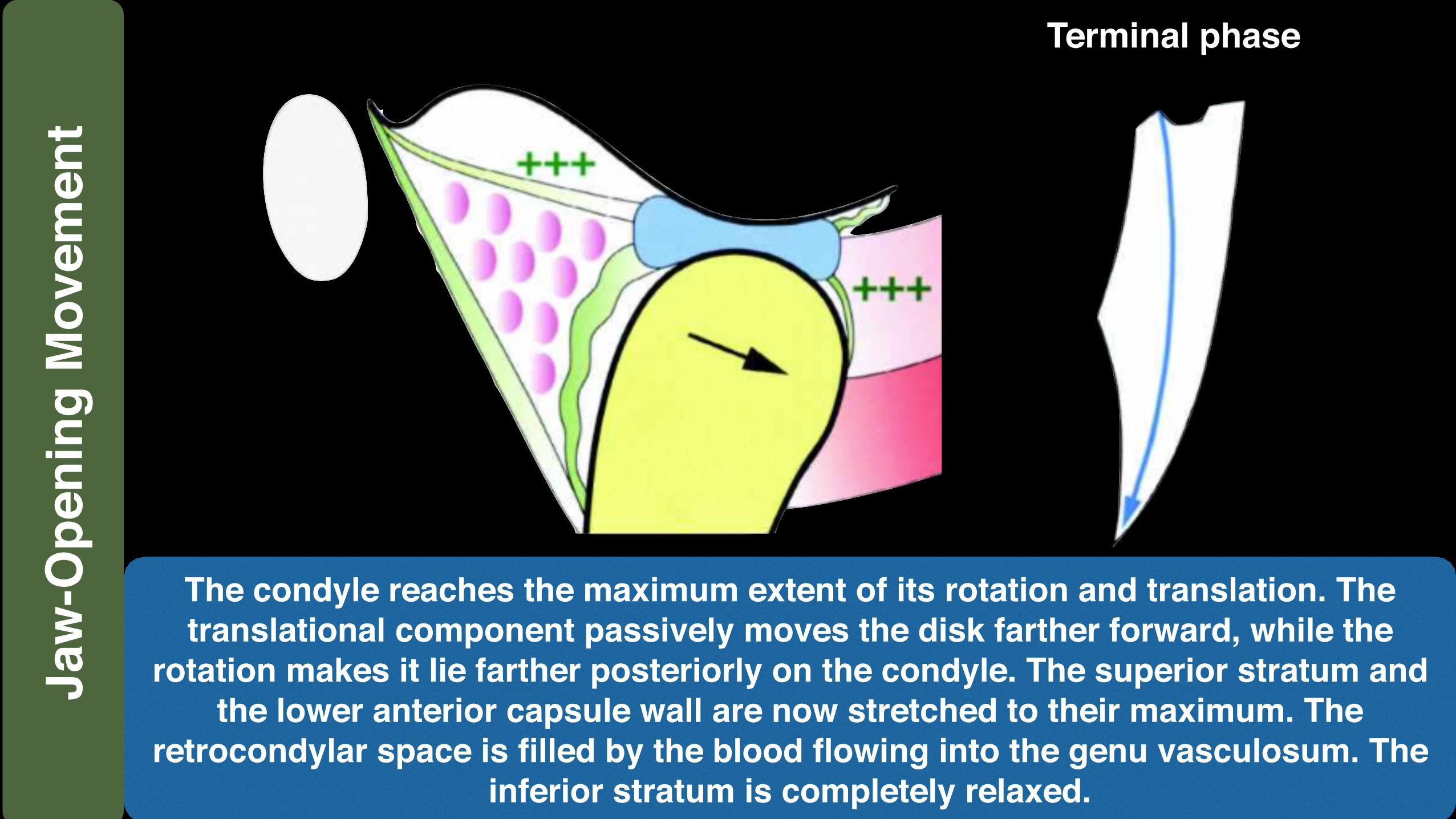
The condyle reaches the maximum extent of its rotation and translation. The translational component passively moves the disk farther forward, while the
rotation makes it lie farther posteriorly on the condyle. The superior stratum and the lower anterior capsule wall are now stretched to their maximum. The
retrocondylar space is filled by the blood flowing into the genu vasculosum. The inferior stratum is completely relaxed.
Terminal phaseJa
w-O
peni
ng M
ovem
ent
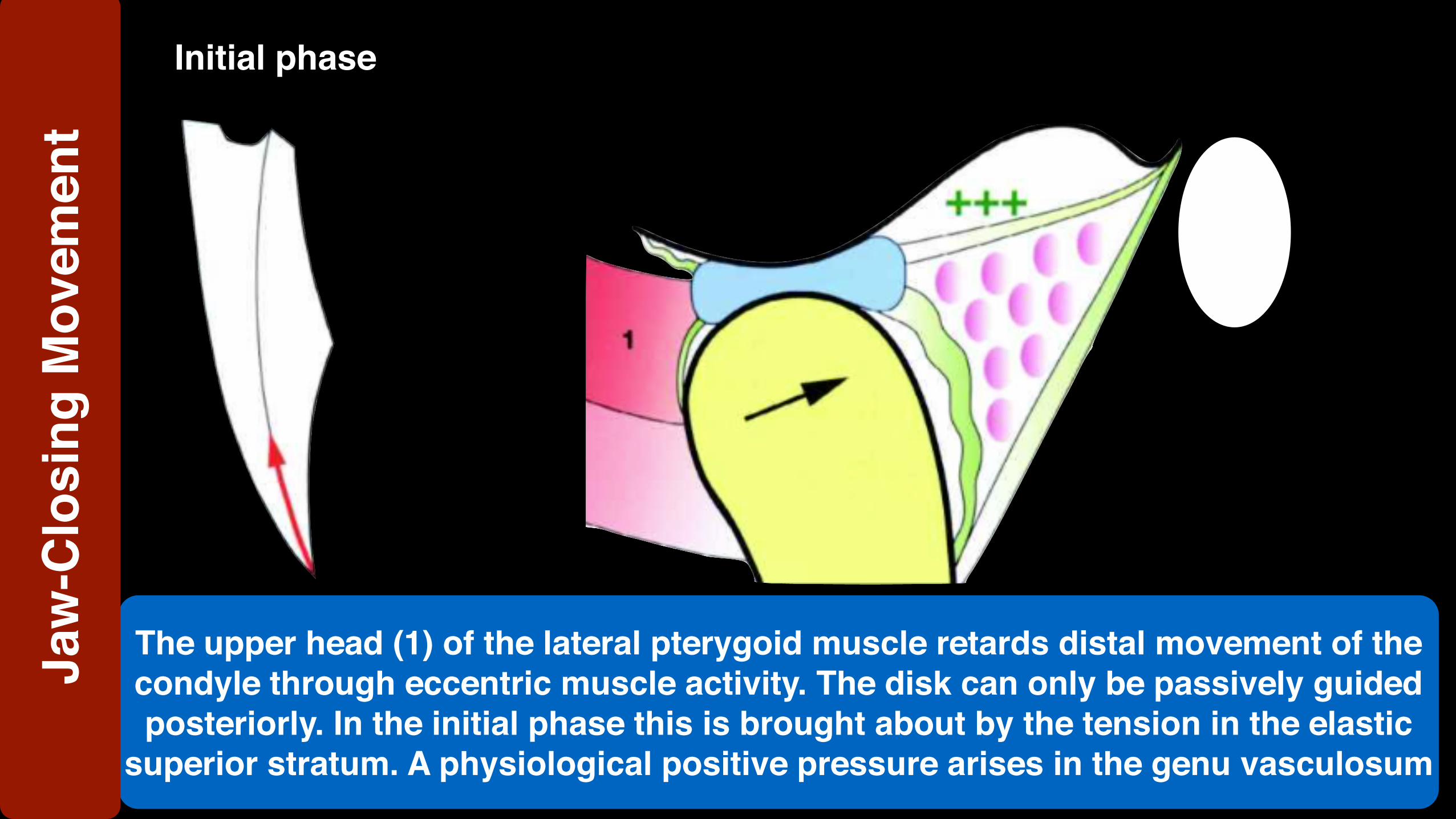
Initial phase
The upper head (1) of the lateral pterygoid muscle retards distal movement of the condyle through eccentric muscle activity. The disk can only be passively guided posteriorly. In the initial phase this is brought about by the tension in the elastic
superior stratum. A physiological positive pressure arises in the genu vasculosum
Jaw
-Clo
sing
Mov
emen
t
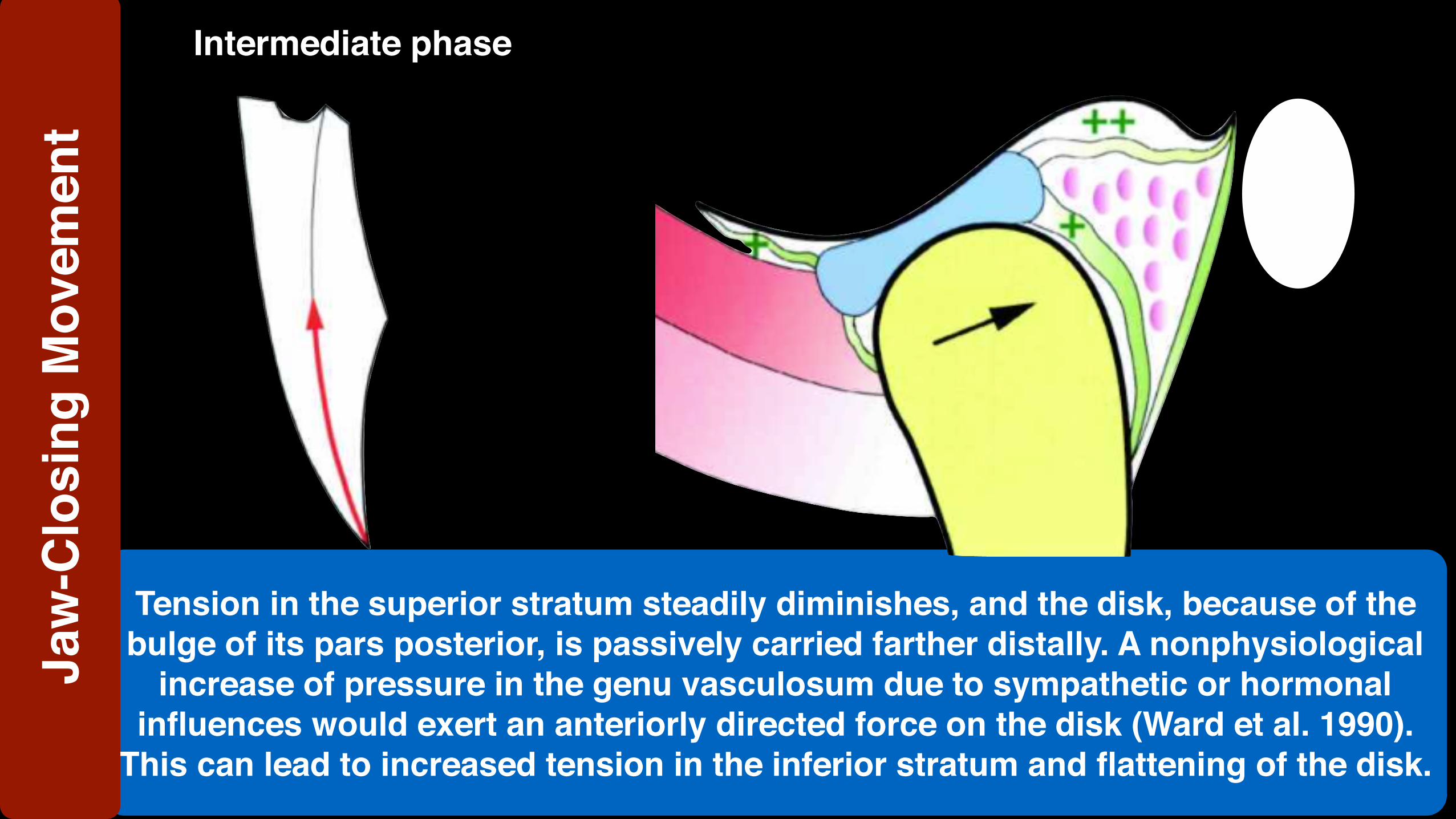
Tension in the superior stratum steadily diminishes, and the disk, because of the bulge of its pars posterior, is passively carried farther distally. A nonphysiological
increase of pressure in the genu vasculosum due to sympathetic or hormonal influences would exert an anteriorly directed force on the disk (Ward et al. 1990).
This can lead to increased tension in the inferior stratum and flattening of the disk.
Intermediate phaseJa
w-C
losi
ng M
ovem
ent

Terminal phase
The inferior stratum becomes increasingly tense and finally prevents anterior disk displacement in case the condyle moves too far distally. Anterior disk
displacement can occur only in the presence of an overstretched inferior stratum, with or without flattening of the pars posterior (Eriksson et al. 1992).
Jaw
-Clo
sing
Mov
emen
t

















