53
Many problems with transfusions are related to infection. In 1985, the chance for hepatitis was 10% and HIV 0.5%
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | estella-underwood |
| View: | 214 times |
| Download: | 0 times |

Many problems with transfusions are related to infection. In 1985, the chance for hepatitis was 10% and HIV 0.5%

TABLE 47-11Percentage Risk of Transfusion-Transmitted Infection
With a Unit of Screened Blood in the United States
RISK WINDOW PERIOD (DAYS)
HIV 1/800,000 22 11
HTLV I & II 1/641,000 51
Cytomegalovirus < 1.0% rapidly
HCV 1/600,000 82 8-10
HBV 1/200,000 59
HIV human immunodeficiency virus type 1: HTLV human T-cell lymphotropic virus: HCV hepatitis C virus: HBV hepatitis B virus

TABLE 47-12Infectious Disease Testing For Blood Transfusions (1998)
1. Discontinue serum alanine aminotransferase testing
2. Hepatitis C antibody testing
3. Antibody to hepatitis B core antigen
4. HIV-1
5. HIV-2
6. HIV Ag (p24 antigen)
7. HTLV I/II
8. Serologic test for syphilis)
From JAMA 1995;274:1374
HIV, human immunodeficiency virus:HTLV, human T-cell lymphotropic virus
IMPROVE TESTING
• Molecular testing
• Viral inactivation
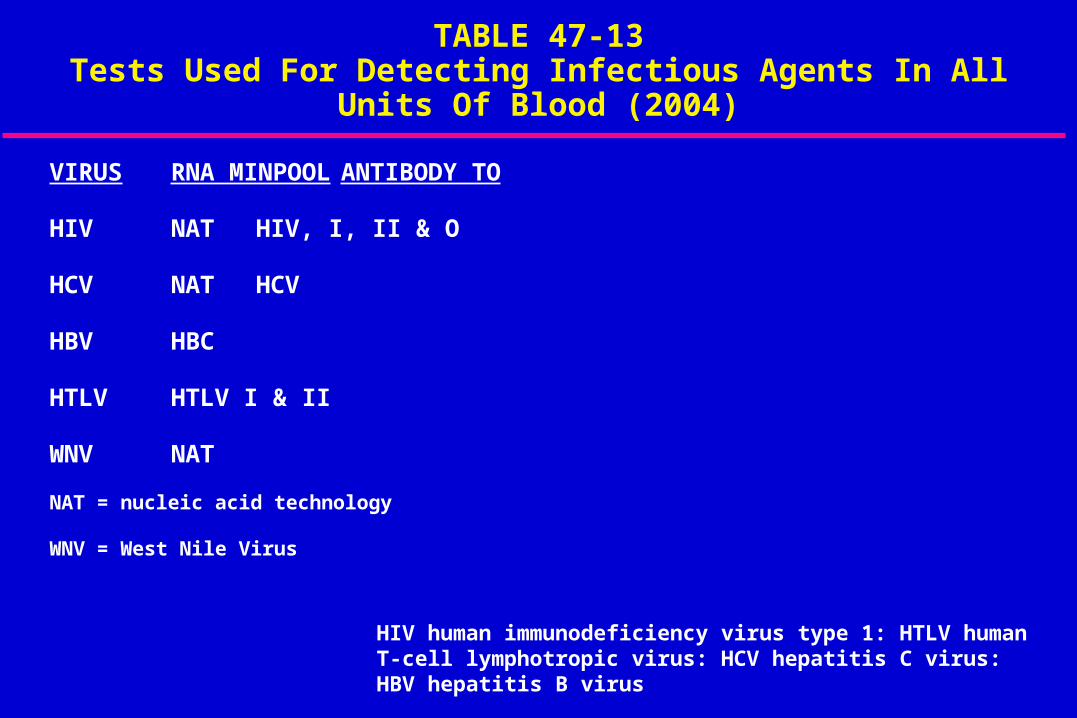
TABLE 47-13Tests Used For Detecting Infectious Agents In All Units Of Blood
(2004)
VIRUS RNA MINPOOL ANTIBODY TO
HIV NAT HIV, I, II & O
HCV NAT HCV
HBV HBC
HTLV HTLV I & II
WNV NAT
NAT = nucleic acid technology
WNV = West Nile Virus
HIV human immunodeficiency virus type 1: HTLV human T-cell lymphotropic virus: HCV hepatitis C virus: HBV hepatitis B virus
NUCLEIC ACID TECHNOLOGY (NAT) TESTING WILL BE USED ON:
• HBV
• Hepatitis A
• Parvovirus 19
• West Nile Virus
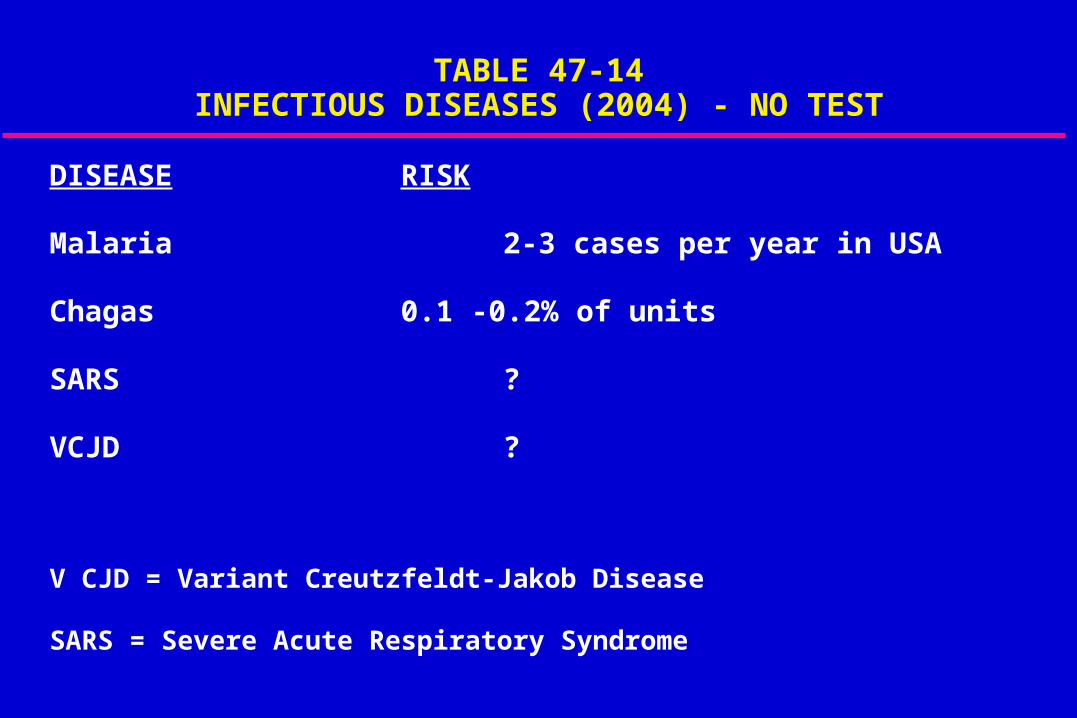
TABLE 47-14INFECTIOUS DISEASES (2004) - NO TEST
DISEASE RISK
Malaria 2-3 cases per year in USA
Chagas 0.1 -0.2% of units
SARS ?
VCJD ?
V CJD = Variant Creutzfeldt-Jakob Disease
SARS = Severe Acute Respiratory Syndrome

*DONATED BLOOD WILL BE BANNEDFROM DONORS WHO:
• Lived in UK 3 months or longer since 1980
• Lived in Europe 6 months since 1980
• Anyone who has received blood in UK
• Will decrease donors by 8-9%
* American Red Cross

MALARIA
• 2 to 3 cases/year for 40 years
• Since 1982, all cases were from emigrants or residents from endemic areas
WEST NILE VIRUS
• 4,000 cases of which 21 are transmitted by transfusion*
• In 2002, 23 cases**
• 43% were immunocompromised
• 8% were > 70 years
Science 2003; 299:1824
** N Engl J Med 2003; 349:1236

TABLE 47-8TRANSFUSION FATALITIES (2001-2002) IN THE UNITED STATES*
• Bacterial contamination - 17
• TRALI - 16
• Mistransfusion - ABO mismatch - 14
*From the Federal Drug Administration (Oct. 1, 2001 to September, 30, 2002)
TRALI = transfusion related acute lung injury
PLATELET INDUCED SEPSIS
• 33 year old male with chronic pancytopenia from failed allogeneic bone marrow Tx
• Platelets caused hypotension refractory to pressor respiratory failure, acidosis, etc.
• Klebsiella pneumonia

PLATELET INDUCED SEPSIS
• 57 year old post blood stem cell transplant for multiple myeloma
• Post MI & CABG; deep vein thrombosis
• Neutropenic fever
• Gave platelets
• 40°C, dyspnea, 85% SAT, AF
• Culture positive for klebsiella pneumonia
RULE
If a patient has a fever within 6 hours after receiving platelets, then it is platelet induced sepsis until proven otherwise.

BACTERIAL CULTURE
Prior to culture, risk was:
RBC 1/300,000
Platelets 1/25,000
WHAT IS THE DIFFERENTIAL DIAGNOSIS WHEN HYPOTENSION OCCURS DURING BLOOD ADMINSTRATION?
Hemolytic transfusion reaction ++
Sepsis ++
Anaphylaxis
TRALI +/-
Isolated
++ = Body temperature
Should all blood (packed red cells) have the white blood cells removed?

Table 1A: Adverse Effects Associated with Donor Leukocytes (4)
Definitive:
• Nonhemolytic febrile transfusion reactions
• Transmission of leukocyte-associated viruses
• Cytomegalovirus (CMV), Epstein-Barr virus (EBV), HTLV-1
• Alloimmunization
Table 1B: Adverse Effects Associated with Donor Leukocytes (4)
Probable:
• Immunomodulatory effects
• Cancer recurrence
• Postoperative infections
WHAT’S NEW?
• Leukoreduction of all red cells and platelet products
• Europe uses it
• Canada - only platelets for cost
• Should eliminate CMV

INDICATIONS FOR BLOOD *
• Should not be dictated by single hemoglobin
• Should be based on patient’s risk of inadequate oxygenation
• BUT, rarely indicated Hbg > 10 gm/dl and always indicated < 6 gm/dl
• Abstract not written by committee
* Anesthesiology 1996;84:732

TRANSFUSION TRIGGER 1998 *
What are these patient risks that should increase transfusion trigger?
* Weiskopf et al. JAMA 1998;279;217-221
• patients who have a rapid HR (cannot compensate)
• patients who do not increase CO appropriately (cannot compensate)
• presence of vital organ dysfunction
• more blood loss

SHOULD POSTOPEATIVE HEMOGLOBIN BE MORE THAN 8.5gms/%? (Mayo Clinic)
The incidence of post-CPB blindness from optic neuropathy is decreased.

Can The Oxygen Dissociation Curve Be Shifted To The Right In Patients? *
• Allosteric modification of oxygen - Hbg
• 10 mm Hg shift by RSP 13
* Wahr et al: Anesth Analg 2001; 92:615-20

BLOOD GROUPS- A REVIEW
• Human erythrocytes >300 antigenic determinants
• Only ABO and Rh important in the majority of blood transfusions
• Most severe transfusion reactions due to ABO incompatibility
Alicia Gruber-Kalamas, MD, University of California San Francisco

ABO INCOMPATIBILITY
Intravascular HemolysisHemoglobinemiaHemoglobinuria
DEATH
DICProfuse Bleeding
Acute Circulatory CollapseAnuria
Donor blood antigen+
Recipient antibodies (IgM)Activates Complement
Alicia Gruber-Kalamas, MD, University of California San Francisco

THE Rh SYSTEM• Rh gene 3 chromosomal loci with 6 alleles
• D antigen is the most common and most immunogenic
• Approximately 80-85% Caucasians have D antigen
• Individuals lacking this allele are called “Rh-negative”
• Only develop antibodies against the D antigen after exposure (transfusion/pregnancy)
Alicia Gruber-Kalamas, MD, University of California San Francisco

Rh ANTIBODIES• IgG class of immunoglobulins
• Lack capacity to bind complement
• Elimination of red cells primarily in the spleen
• Clinical symptoms mild, generally limited to fever/chills
Alicia Gruber-Kalamas, MD, University of California San Francisco

Rh AND THE PREGNANT WOMAN
• Transplacental passage of D-positive fetal RBC’s into D-negative mother produces anti-D (IgG)
• Anti-D IgG traverses the placenta and coats fetal RBC’S leading to extravascular hemolysis
• Clinically manifest as hemolytic disease of the fetus and newborn- anemia, hepatosplenomegaly, hydrops fetalis, and death
Alicia Gruber-Kalamas, MD, University of California San Francisco
Rh PROPHYLAXIS- Rhlg
• 1968 RhIg first licensed for prophylactic administration via IM route (RhoGam)
• IgG anti-D derived from human plasma
• Exact mechanism unknown
• 20 mcg purified RhIG provides protection against 1 ml Rh-positive blood
• WinRho IV preparation
Alicia Gruber-Kalamas, MD, University of California San Francisco

PREVENTION OF POST-TRANSFUSION Rh-ALLOIMMUNIZATION
The protective effect of RhIg is dose dependent
RhIg can prevent Rh immunization if:1) Sufficient dose is administered2) RhIg is given within 72 hours of exposure
Alicia Gruber-Kalamas, MD, University of California San Francisco

Succesful Prevention of Post-Transfusion Rh Alloimmunization by IV WinRho
Anderson, et al A. J. Hematology 1999; 60:245
Case Report• 10 mo old D-negative female• Received 40 ml D-positive PRBC’s• Administered 1200mcg IV WinRho • At 1 year follow-up, no evidence of Anti-D
Alicia Gruber-Kalamas, MD, University of California San Francisco

RBC Exchange with Rh-negative Cells: An Alternative Approach
Werch et al Transfusion 1993; 33:530
• 22 y/o Rh-negative woman received 10 units Rh-positive PRBC’s
• RBC exchange with Rh-negative cells 12 hours post-exposure in addition to RhIG
• 11 months later delivered healthy, Rh-negative child; no evidence of Anti-D
Alicia Gruber-Kalamas, MD, University of California San Francisco

FOLLOW-UP• Blood Bank informed of the error
• Calculated dose was 27,000 IU WinRho
• 3000 IU IV Q8hrs x 9 doses ($$$$$$)
• Pt will require follow-up at 6 months to check for presence of anti-D antibodies
Alicia Gruber-Kalamas, MD, University of California San Francisco
PROCEDURE AT SFGH• Blood bank alerted to activation of “911”
• If pt male, 2U O-positive sent to ED; if pt female, 2U O-negative sent to ED
• 6U O-positive is kept in OR at all times
• O-negative must be sent from Blood Bank
Alicia Gruber-Kalamas, MD, University of California San Francisco
IN SUMMARY• Rh D Antigen is of huge clinical significance for
young females and women of child-bearing age
• If a Rh-negative women inadvertently receives Rh-positive PRBC’s, whole blood, or platelets, the appropriate calculated dose of WinRho must be administered within 72 hours of exposure
Alicia Gruber-Kalamas, MD, University of California San Francisco

WHAT IS CORRECT BLOOD TYPE?
Type O OK No No No
Type A OK OK No No
Type B OK No OK No
Type AB OK OK OK OK
FFP Type O Type A Type B Type AB

Blood to lab4 units PRBC (0+)in ED (0-) women
From blood sample:• CBC including platelets• PT, PTT• Fibrinogen
Crystalloids + re-evaluateIndication for immediatetransfusion
Give 2 units PRBC
Review labsCoagulopathy present?
Hct < 30 percent?
PT > transfusion threshold
Anticipated ongoing blood loss
De-activate massivetransfusion protocol
Crystalloids +blood by lab values
Give 4 units of FFP and6 packs of platelets
Give whole blood (preferred)or packed cells to HCT 30
Transfuse to maintain thresholds:• Hct < 30 percent• FFP with PC ratio of 1:1• Platelets with PC in ratio of 1:1
Indications for type O blood:• BP < 70 mm Hg• PT, PTT• get fibrinogen
Indications for transfusion protocol:• BP < 90 mmHg after 2 PRBC• Blood loss = circulating blood volume
Monitoring protocol:• Hct, PT, PTT, fibrinogen and platelets• Create flow sheet• EBV70-90 ml/kg
Transfusions thresholds• HCT, PT, PTT• INR > 2.0 usually• INR > eye, brain, airway, 1.7 bleeding• platelets < 75,000 usually• fibrinogen < 100 mg/dl
PC < transfusion threshold?
No
YesNo
Yes
Yes
No
Yes
No
NoGive platelets, 6 packs toPC 25-50, 000Yes
No
No
TABLE 47.5
An Algorithm for Massive Transfusion*

TABLE 47-6CORRELATION BETWEEN PLATELET COUNT
AND INCIDENCE OF BLEEDING
Platelet Count Total No. No. of Patients
> 100,000 21 0
75,000 - 100,000 14 3
50,000 - 75,000 11 7
< 50,000 5 5
(Cells/mm3) of Patients With Bleeding
Data from Miller et al 58

A New Treatment For Transfusion Induced Coagulopathy
• Recombinant activated coagulation Factor VII (r FVIIa) (NovoNordisk)
• Rx coagulopathic intraoperatively
• Expensive
• Should be viewed as “rescue” therapy until FDA is more evident
LIMITATIONS OF BLOOD TRANSFUSIONS
• Transmission of infectious diseases
• Dependent on volunteer donors (shortage?)
• Need for typing and cross-matching
• Short shelf-life
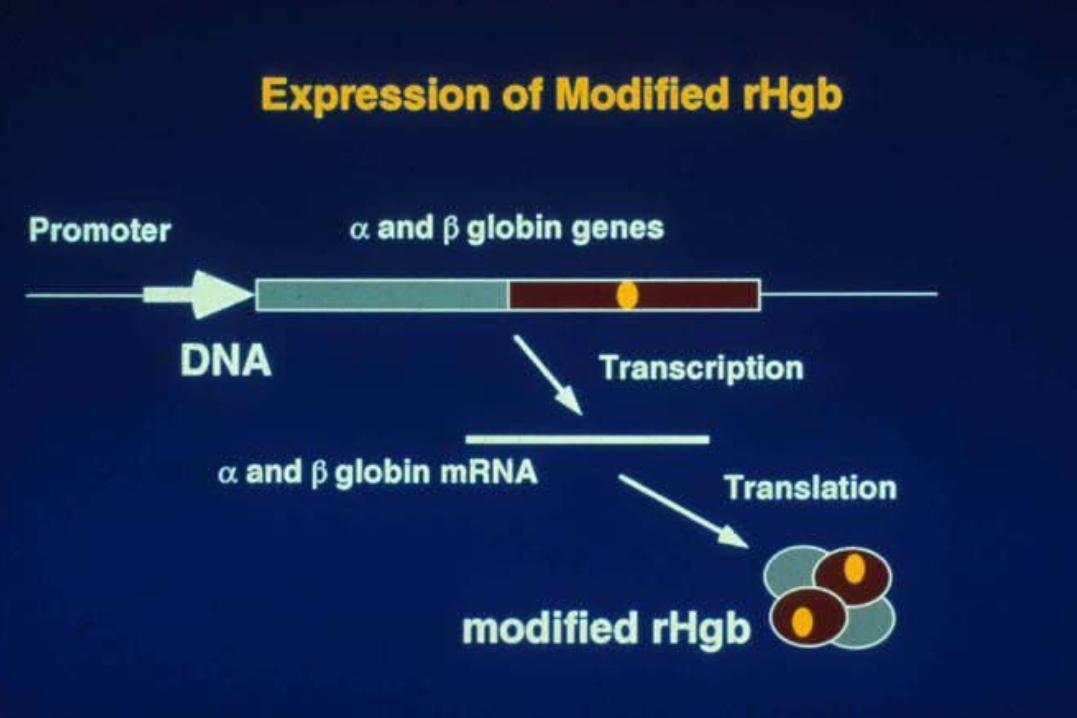
RECOMBINANT HEMOGLOBIN (rHb)
A genetically engineered recombinant human hemoglobin which can be used as red blood cell substitute

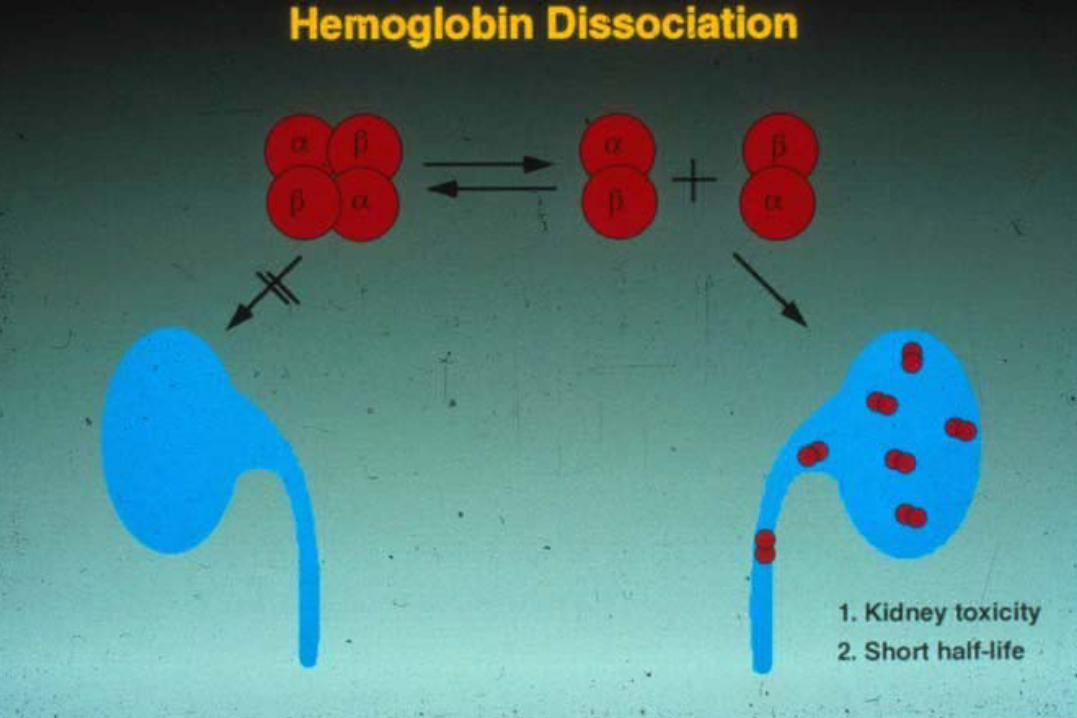
OLD HISTORIC PROBLEMS
• Kidney failure
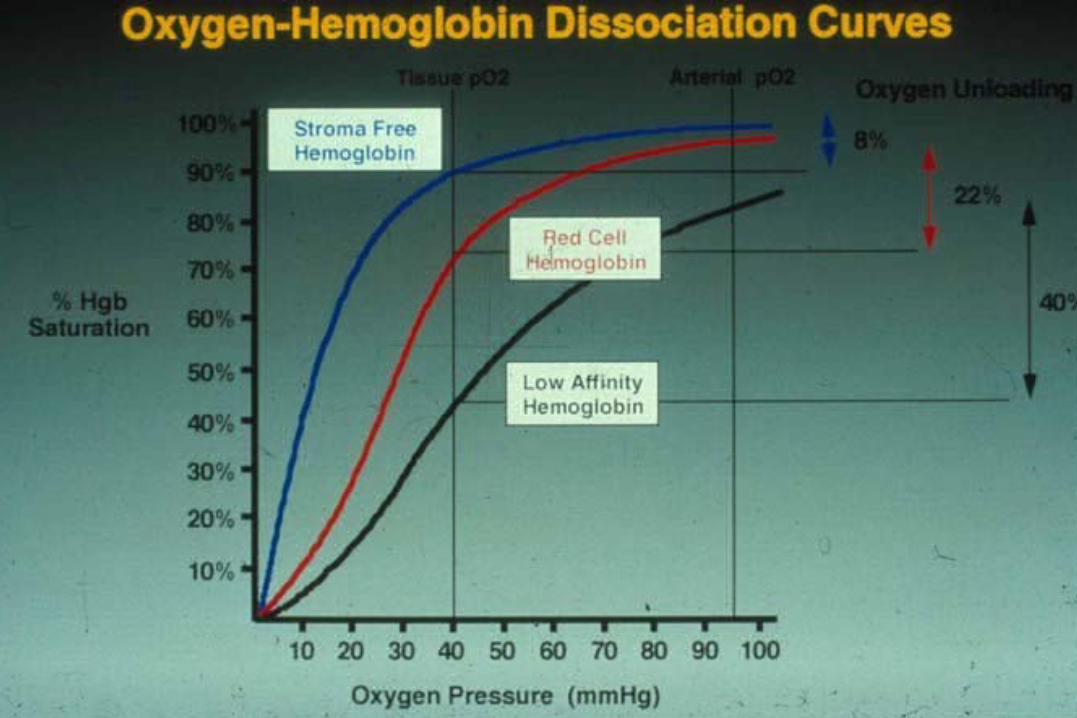
• Oxygen dissociation curve

WHAT ABOUT THE
OXYGEN AFFINITY?


ADVANTAGES OF rHb
• No risk of blood-borne infection
• No need to type and cross-match
• Optimized oxygen delivery
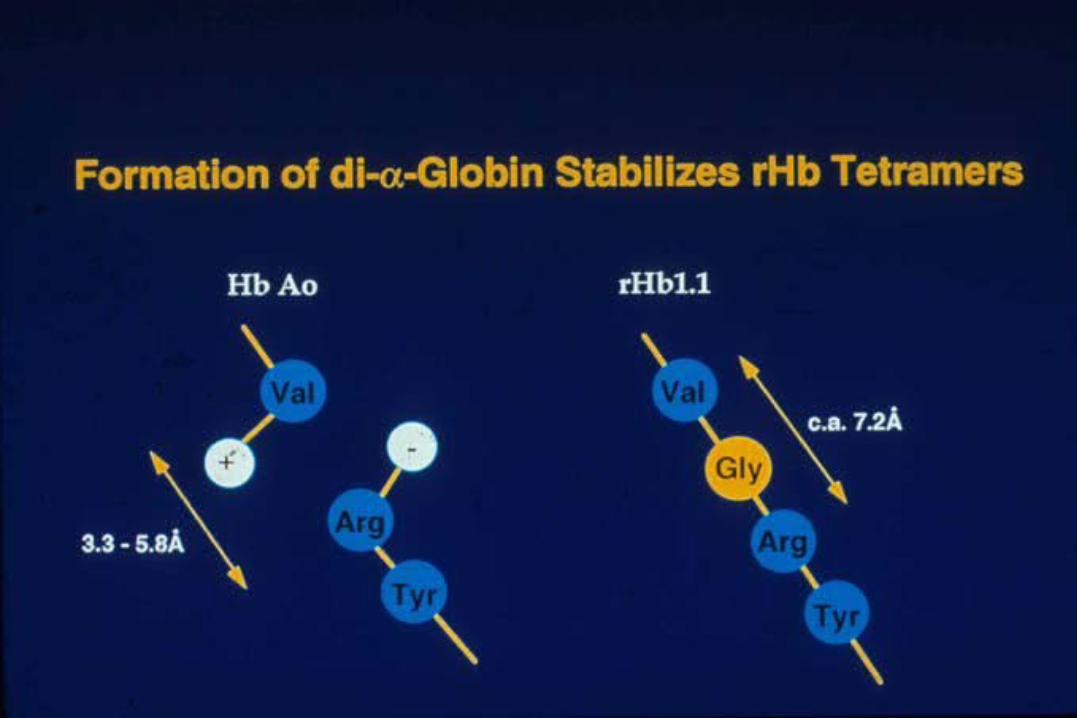
• No need for chemical modifications
• Improved shelf-life
• Economic scale-up, production, and supply

UPDATE SYNTHETIC BLOOD
Biopure produces a product named Hemopure. It is approved in South Africa and will be in the USA and Europe in a year.
Stealth Red Cell. Polyglycol covering preventing antibodies from getting to it, but still needs ABO testing. Will lengthen half-life by many days. (or 30 days.)

PREDICTION:
In 15 years, human blood will not be used as a blood transfusion (at least for the purpose of delivering oxygen.)


















