52
Marcus Nesbeth PA- C
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | tobias-edwards |
| View: | 221 times |
| Download: | 0 times |

Marcus Nesbeth PA-C
ABG: is a test that measure the arterial Oxygen and Carbon dioxide concentration, acidity, and oxyhemoglobin saturation.
Note that HCO3 from the ABG is a calculated value and should not be used in the interpretation soley.
Instead the HCO3 from the Chemistry panel should be used.
Important test for ICU Patients with critical illness and respiratory diseases.

To evaluate acute respiratory distress and assist in determining therapeutic interventions.
To document the existence and severity of a problem with oxygenation or carbon dioxide exchange.
To analyze acid-base balance. To evaluate the effectiveness of
respiratory interventions, for eg., continuous ventilatory assistance or oxygen therapy.

Proceed with caution and avoid arterial sticks in the following circumstances:Previous surgery in the areaPts on anticoagulants or with known
coagulopathy. Or pts on fibrinolytics or candidates for it.
Skin infection or other damage to the skin (eg. Burns, cellulitis) at he puncture site.
Decreased collateral circulationSevere atherosclerosis, aneurysm, or
vasospasmsSevere injury to the extremity

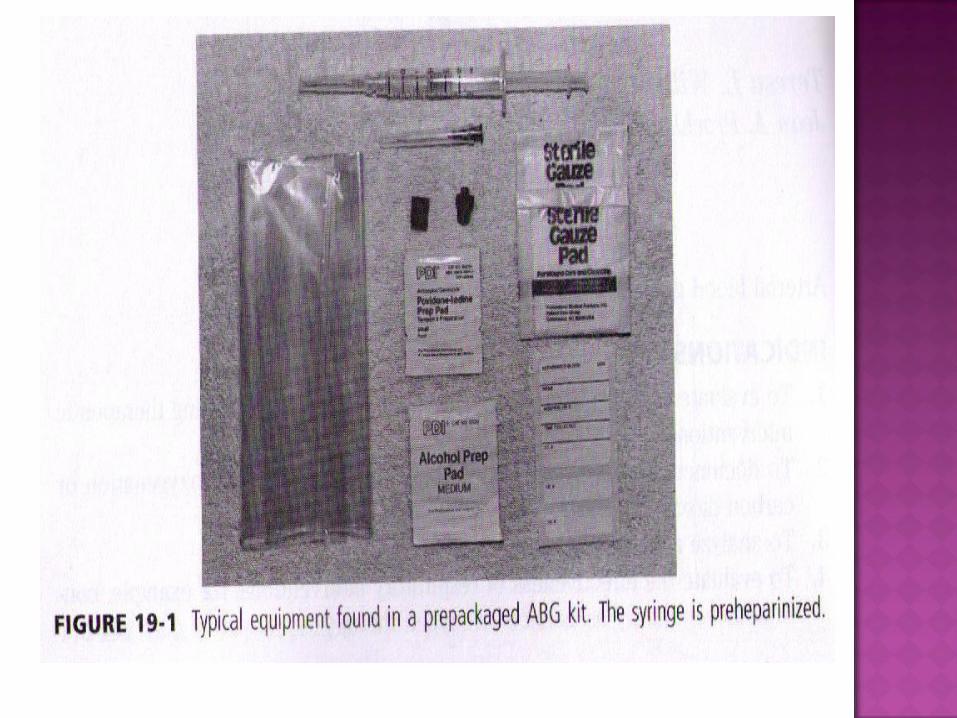
3-5 ml sterile syringe with freely movable plunger
25 gauge, 5/8inch needle for radial, brachial, dorsalis pedis, and femoral sticks.
Antiseptic skin preparation ( betadine..) 3ml syringe with 25 gauge, 5/8 inch needle
for 1% lidocaine w/o epinephrine (optional) Container of crushed ice for sample transport Sterile Gloves. Possible goggles or eye protection Heparin 1:1000 if syringe is not heparinized

The preferred site in most pts is the Radial Artery
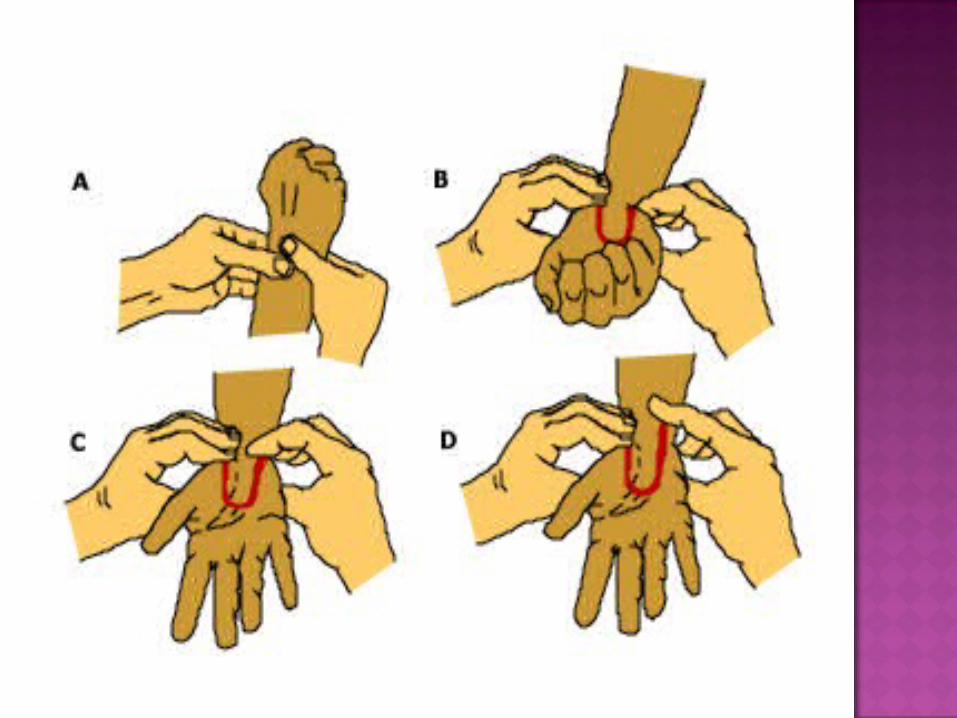
Check for patency of collateral circulation with the Allen’s Test
Prep the skin in an aseptic manner and put on gloves
Position the Extremity:Radial: Stabilize the wrist over a small
rolled towel or washcloth. The wrist should be dorsiflexed about 30 degrees.
Brachial: Place a rolled towel under the pt’s elbow while hyperextending the elbow. Rotate the pt’s wrist outward.
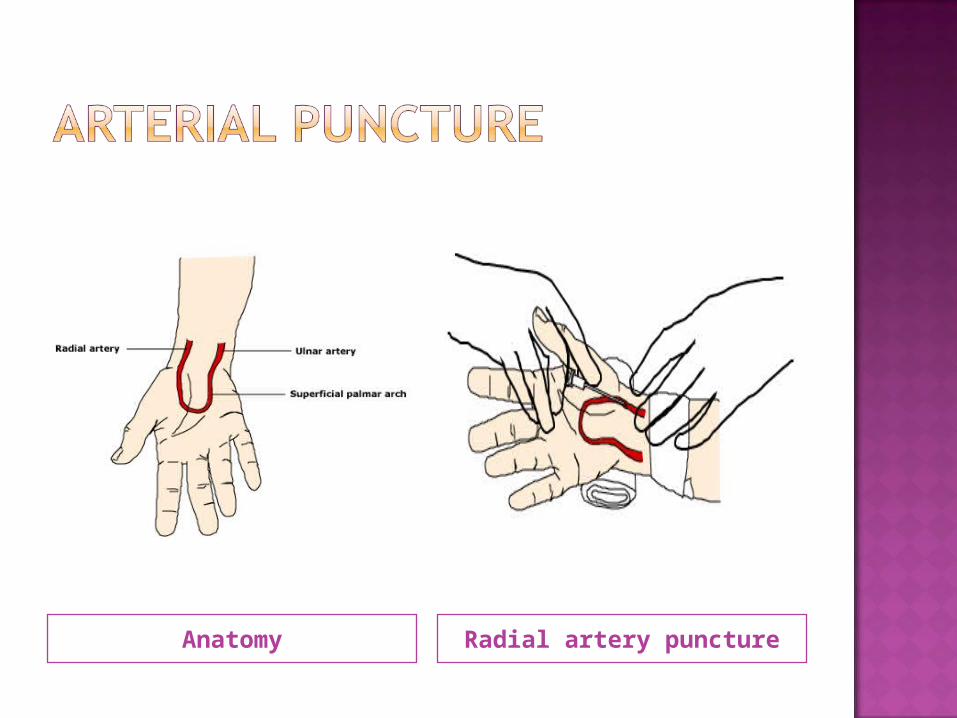
Anatomy Radial artery puncture

Brachial Artery Puncture Femoral Artery Puncture
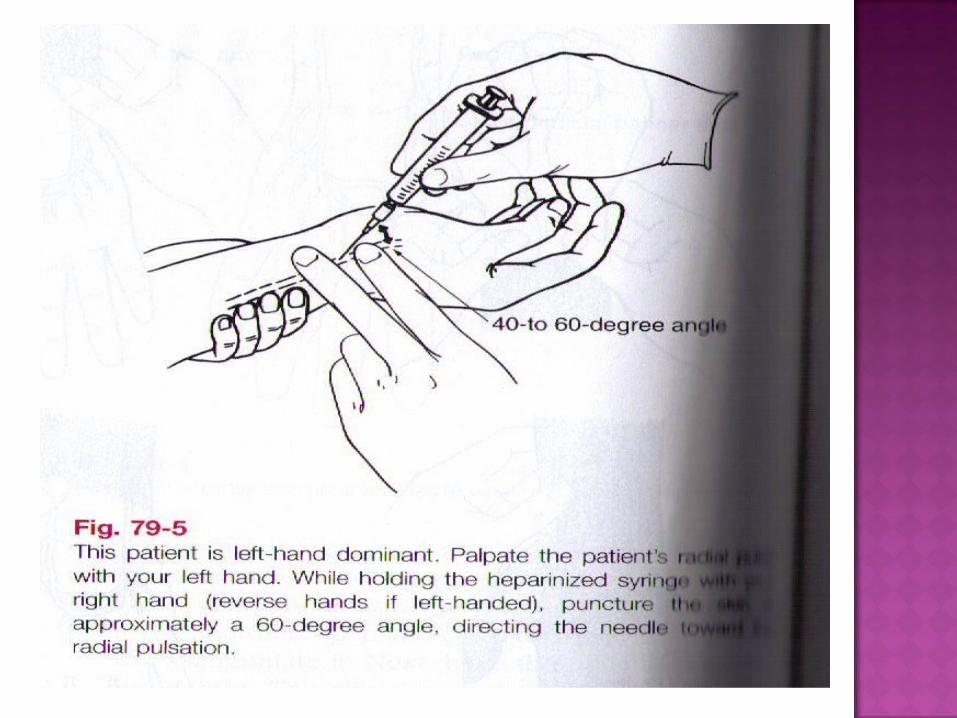
Palpate the pulse and determine the point of maximal impulse.
Inject 0.2 – 0.3ml of 1% lidocaine subcutaneously on either side and above the artery (optional).
Palpate the selected artery with the balls of two fingers, and immobilize it with these fingers along its course.
Grasping the syringe as if holding a pencil. Direct the needle with the bevel up, and puncture the skin slowly at approximately a 40-60 degree angle to the radial or brachial artery ( 60-90 degrees to the femoral artery).

Watch the needle hub constantly for the appearance of blood.
When blood appears, stop advancing the needle, and allow the blood to flow freely into the syringe.
If the syringe fails to fill after an initial flash of blood both walls of the artery may have been pierced.
Withdraw the needle slightly until the tip reenters the artery and blood flows into the syringe.

Obtain a sample of 2 to 3 ml. Remove the needle from the artery.
Immediately apply direct pressure to the puncture site with dry gauze for 3 to 5mins.
And at least 10mins for pts taking anticoagulants, fibrinolytics, or glycoproteins.
Hold the syringe with the needle tip upright and expel any air bubbles. Tapping the syringe may help expel bubbles clinging to the sides.

Most common are bleeding, hematoma, and thrombosis formation.
Compression neuropathies may occur secondary to hematomas.
Nerve injury may occur with inadvertent puncture of the nerve.
If air bubbles are not removed from the sample, the PO2 can increase and yield inaccurate test results.
The blood sample may clot if the heparin and blood are not mixed adequately.
pH 7.36-7.44
pCO2 38-42 mm Hg
HCO3- 22-28 mEq/L
FICTION!
A pCO2 < 40 mm Hg always implies a respiratory alkalosis
FICTION!
A patient with a metabolic acidosis will have a compensatory respiratory alkalosis


Step 1. Is there an acidemia or alkalemia?

Step 2. Is the primary process metabolic or respiratory?

Step 3: If the primary process is respiratory, is it
acute or chronic?
This step is only applied if the primary cause is respiratory.
For each 10mm Hg that the pCO2 changes, the pH should move in the opposite direction. If the pCO2 drops, the pH should rise, and vice versa.
The amount that the pH changes tells us whether the change is acute or chronic.
A change in the pH of 0.08 for each 10mm Hg indicates an ACUTE condition.
A change in the pH of 0.03 for each 10mm Hg indicates a CHRONIC condition.
Step 4: Is there an anion gap?
Na+ - (Cl- + HCO3-) >
12?

Step 5: Is the respiratory compensation
adequate?
Expected pCO2 range =
[1.5(measured HCO3-)]+8+/- 2

This step is only applied if the primary cause is metabolic (acidosis or alkalosis)
Expected pCO2 =
(1.5 * serum HCO3-) + 8 [+/- 2]
If metabolic acidosis: If measured pCO2 > expected pCO2, a respiratory acidosis is present in addition to the already diagnosed metabolic acidosis.
If metabolic alkalosis: If measured pCO2 > 55, a respiratory acidosis is present in addition to the already diagnosed metabolic alkalosis.
Step 6: Are there any other metabolic disturbances?
Corrected HCO3- =
(Measured HCO3-) + (AG-12)

This step is only applied if there is an increased anion gap metabolic acidosis (if you had to do the math in step 4)
Corrected HCO3- =
Measured HCO3- + (anion gap - 12)
If corrected HCO3- < 24, a second acidosis is
present in addition to the already diagnosed metabolic acidosis.
If corrected HCO3- > 24, there is a co-existing
metabolic alkalosis in addition to the already diagnosed metabolic acidosis.
If corrected HCO3- = 24, then the already
diagnosed metabolic acidosis is the sole problem.

30 year old female BMT patient with neutropenic fever has been receiving multiple antibiotics including amphotericin B. You are called to the bedside for her fevers, rigors, and dyspnea
Na+ 125 Cl- 100 HCO3-
8
pH 7.07 pCO2 28 K+ 2.5

Step 1. Is there an acidemia or alkalemia?
Acidemia

Step 2. Is the primary process metabolic or respiratory?
pCO2 = 28 should drive pH ↑
HCO3- = 8 should drive pH ↓

Step 3: If the primary process is respiratory, is it acute or
chronic?
Skip this step as primary process is metabolic!

Step 4: Is there an anion gap?
Na+ - Cl- - HCO3- > 12?
125 - 100 - 8 = 17
Anion Gap Metabolic Acidosis

Step 5: Is the respiratory compensation adequate?
Expected pCO2 range = [1.5(measured HCO3
-)]+8+/- 2
[1.5 (8) +8] +/- 2 = [18-22]
pCO2 = 28, therefore this is a Respiratory Acidosis even though the value is below 40!!

Step 6: Are there any other metabolic disturbances?
Corrected HCO3- =
(Measured HCO3-) + (AG-12)
(8) + (17-12) = 13
Since this is below the normal range after correction, there is a non anion gap acidosis

60 y/o male presents to the ED from a nursing home. You have no history other than he has been breathing rapidly and is less responsive than usual.
Na+ 123 Cl- 99 HCO3- 5
pH 7.31 pCO2 10

Step 1. Is there an acidemia or alkalemia?
Acidemia
Step 2. Is the primary process metabolic
or respiratory?
pCO2 = 10 should drive pH ↑
HCO3- = 5 should drive pH ↓
Step 3: If the primary process is respiratory, is it acute or chronic?
Skip this step as primary process is metabolic!

Step 4: Is there an anion gap?
Na+ - Cl- - HCO3- > 12?
123 - 99 -5 = 19
Anion Gap Metabolic Acidosis

Step 5: Is the respiratory compensation adequate?
Expected pCO2 range = [1.5(measured HCO3
-)]+8+/- 2
[1.5 (5) +8] +/- 2 = [13.5 – 17.5]
pCO2 = 10, therefore it IS a respiratory alkalosis (as a 2nd process)
Step 6: Are there any other metabolic disturbances?
Corrected HCO3- =
(Measured HCO3-) + (AG-12)
(5) + (19-12) = 12
Since this does not correct bicarbonate back to normal, there is a normal anion gap acidosis

42 y/o female has the flu for four days with incessant vomiting. She presents to the ED two days after stopping insulin due to no food intake
Na+ 130 Cl- 80 HCO3- 10
pH 7.21 pCO2 25

Step 1. Is there an acidemia or
alkalemia?
Acidemia
Step 2. Is the primary process metabolic
or respiratory?
pCO2 = 25 should drive pH ↑
HCO3- = 10 should drive pH ↓

Step 3: If the primary process is respiratory, is it acute or chronic?
Skip this step as primary process is metabolic!

Step 4: Is there an anion gap?
Na+ - Cl- - HCO3- > 12?
130 - 80 - 10 = 40!!
Anion Gap Metabolic Acidosis

Step 5: Is the respiratory compensation adequate?
Expected pCO2 range = [1.5(measured HCO3
-)]+8+/- 2
[1.5 (10) +8] +/- 2 = [21 - 25]
pCO2 = 25, therefore this is normal respiratory compensation

Step 6: Are there any other metabolic disturbances?
Corrected HCO3- =
(Measured HCO3-) + (AG-12)
(10) + (40-12) = 38
Since this over corrects bicarbonate there is a metabolic ALKALOSIS!!

Methanol Uremia Diabetic
ketoacidosis Paraldehyde Isopropyl
alcohol & Iron
Lactic acidosis Ethylene glycol
Salicylates & Starvation
Rhabdomyolysis
Diarrhea Ureteral
diversion Renal tubular
acidosisProximalDistal
Mineralcorticoid deficiency
Carbonic anhydrase inhibitorAcetazolamideMefenamic acid
Post hypocapneic state

Early renal failure
Renal diseaseSLE interstitial
nephritisAmyloidosisHydronephrosisSickle cell
nephropathy
Acidifying agentsAmmonium
chlorideCalcium
chlorideArginine
Sulfur toxicity

















