64
Marine Trauma and Envenomations Andrew Butterfass, MD FACEP Cabrini Medical Center
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | dayna-lane |
| View: | 215 times |
| Download: | 0 times |

Marine Trauma and Envenomations
Andrew Butterfass, MD FACEP
Cabrini Medical Center

Key Points
• Identify Hazardous Marine Life.
• Manage minor exposures.
• Identify and stabilize major envenomations.
Introduction
• Marine life injuries are extremely diverse.• Many organisms are endemic to one region.• Most injuries occurs in populated costal
waters or freshwater inland area’s.• High profile injuries include shark and
alligator attacks.• Reality about 100 attacks a year worldwide
with only about 5-10 deaths.




Introduction
• Traumatic Encounter– Bite or puncture with fin, spine, scale.– Examples- Shark, barracuda, alligators, moray
eels, and sea urchins.– Cause direct and indirect injury by force and
secondary infection.
Introduction
• Envenomation- toxin involved – Can cause hypersensitivity reactions,
anaphylaxis and specific toxic venom reactions.– Puncture
• Examples include Cone shells, Octopus, and Sea snakes.
– Contact• Usually caused by invertebrates including
coelenterates (jellyfish), sponges and bristle worms..
Coelenterates
• Only 12 out of 500 species of jelly fish are venomous.
• Reaction is dose and individual dependant.
• Most Coelenterates cause local reaction.
• Box Jelly Fish and Man-of-War are exceptions.
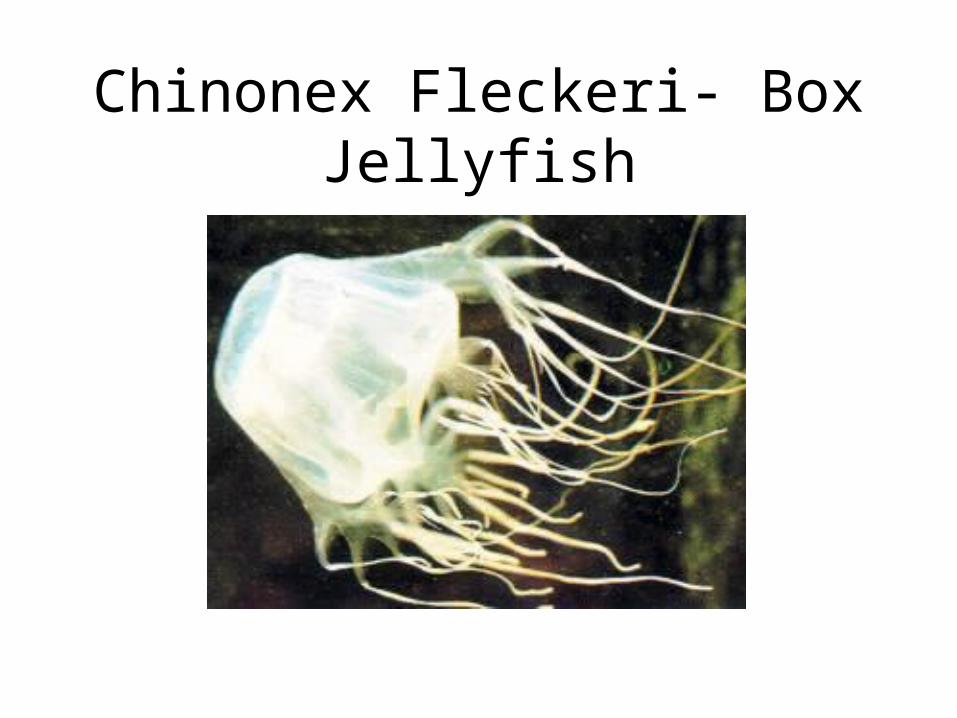
Chinonex Fleckeri- Box Jellyfish

Box Jellyfish

Box Jellyfish Victim

Box Jellyfish and Man-of-War
• Box Jellyfish may be most potent marine envenomations.
• Stings can be severe enough to cause loss of consciousness.
• Sting can cause muscle cramps, abdominal pain, fever, chills, nausea, vomiting, respiratory distress, delirium, paralysis and death.
• Most causes of death are from drowning secondary to panic or cardiovascular collapse.

Man-of-War
Nematocyst
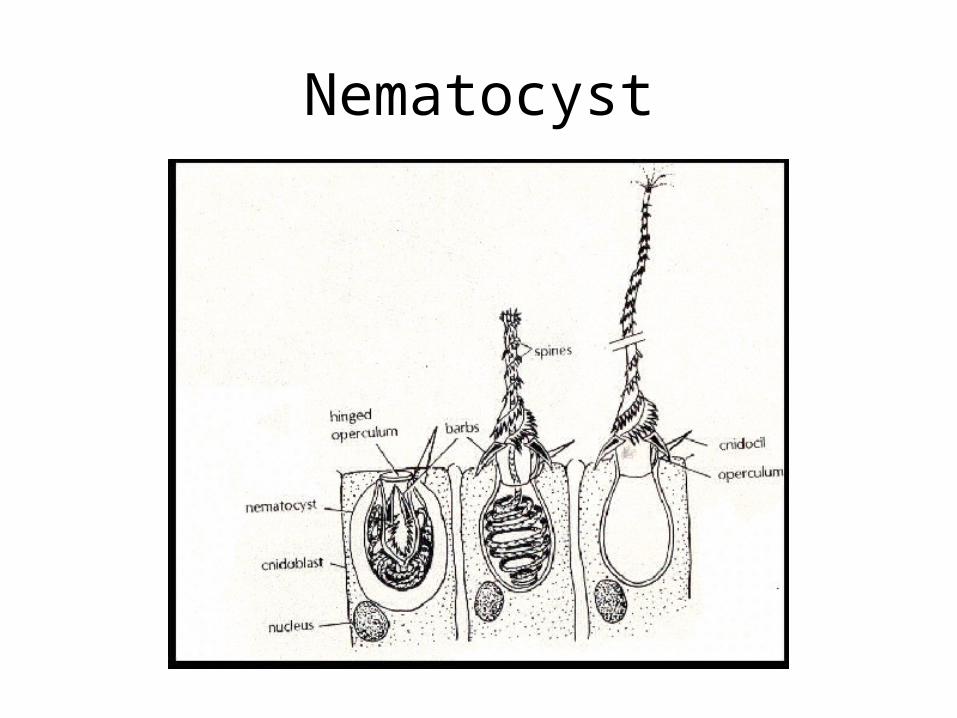
• Nematocyst- Stinging Cell activated by direct contact, changes in temperature and osmolality.
• Initial response is pain or prickling.• Red hot and swollen rash with pustule and vesicle
formation.• Venom is complex
– Nerve conduction affects due to tetramine which is similar to curare.
– Pain and local histamine effects are due to 5-hydroxytryptamine.
Nematocyst
Coelenterate Sting Treatment
• Initial treatment includes washing area with salt water. (fresh water will destabilize nematocysts.)
• Denature the neomocyts with 5% acetic acid (vinegar) for 30 min.
• Remove nematocyst with forceps.• Howell suggests using shaving cream and
shaving affected area.
Coelenterate Sting Treatment
• Apply topical analgesics and steroids.
• For extreme hypersensitivity and systemic reactions– ABC’s– IV analgesics and steroids if needed.– Cardiovascular monitoring and support as
needed.


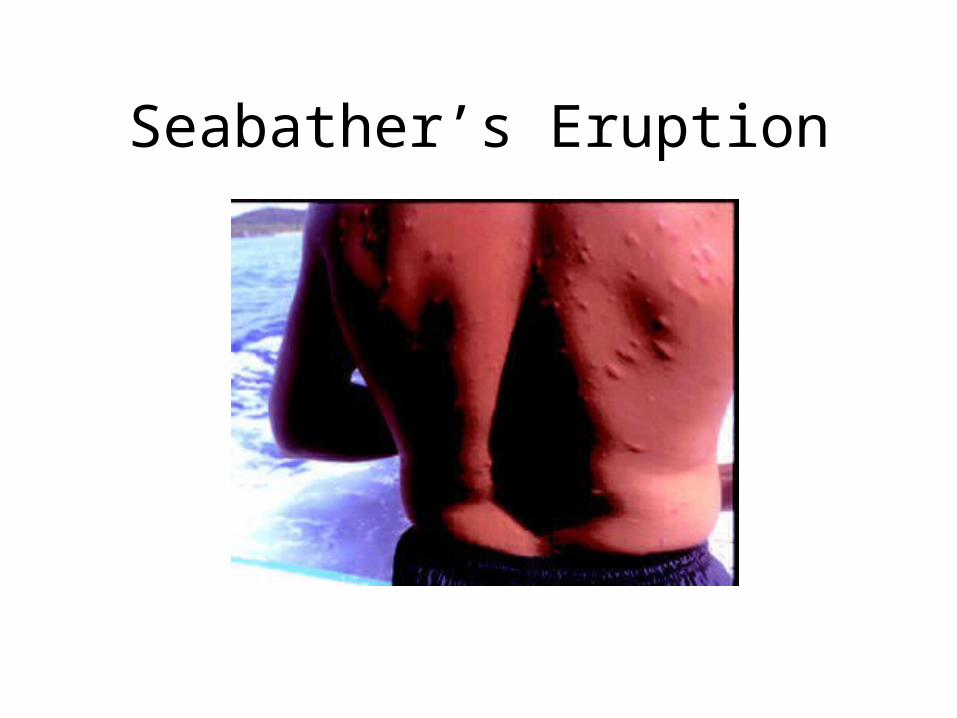
Seabather’s Eruption
• Jelly Fish Larvae- Linuche unguiculata• Contact Dermatitis• Occurs in eastern coast of Florida between March
and August.• Puritic, erythematous, papules that appear in
distribution of bathing suit.• Present within 24 hours of exposure, but may be
delayed 3 to 4 days.• Treatment includes systemic and topical steroids
and antihistamines.

Seabather’s Eruption
Seabather’s Eruption
Sponges
• Of 5000 known species, 12 are toxic.• Three produce contact dermatitis
– Red-beard sponge Micronia prolifera.– Fire sponge Tedania ignis.– Poison-bun sponge Fibulila sp.
• Treatment similar for jellyfish.• Small needle like spicules can be removed
with piece of tape.
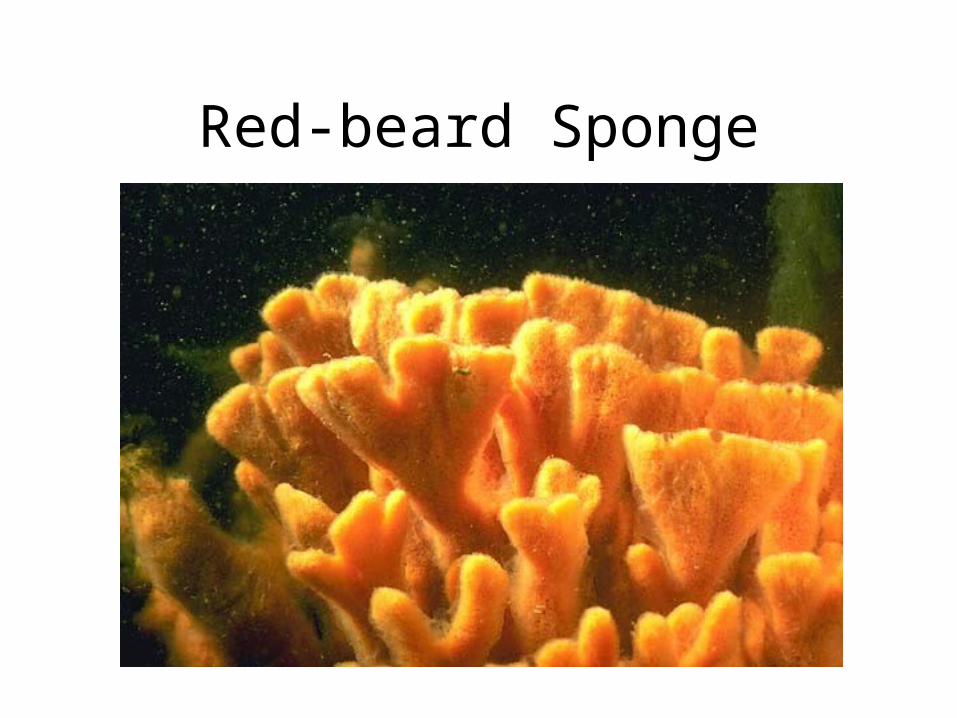
Red-beard Sponge

Fire Sponge
Venomous Fish
• 200 known species of venomous fish
• Most Common – STINGRAY– LIONFISH/SCORPIONFISH– STONEFISH– SALTWATER CATFISH– WEEVERFISH

Stingray
• Cause tissue damage with sharp tail.
• Tail has one to four sharp spines on dorsal surface.
• Spines have membrane that tears to release venom.
• Most injuries occur when ray is stepped on.
• Spines are fired into foot or leg.

Stingray
Stingray Venom
• Venom is Thermolabile.• Symptoms include blue discoloration at
wound site secondary to vasoconstriction.• Intense pain at site, local ischemia and
edema.• Systemic effects include -Salivation,
sweating, vomiting, diarrhea, cramps, hypotension, and cardiovascular collapse.
Stingray EnvenomationTreatment
• Keep person quiet- activity circulates venom.• Place constricting band above wound if on a limb
(not tourniquet)• Venom is Thermolabile- Soak wound in hot water
(110-113 degree F) for 30-60 minutes or until pain subsides. Heat denatures venom proteins.
• Irrigate and remove any remaining spine.• Wound care including antibiotic coverage and
tetanus prophylaxis.• Pain relief

Lionfish/ScorpionfishStonefish
• Lionfish/Scorpionfish found in tropical seas including Red sea, Indian ocean and Pacific ocean.
• Stonefish found in waters of Australian coast.

Lionfish

Stonefish

Lionfish and Stonefish Treatment
• Venom is similar to stingray.• Antivenin is available through the Australia
Commonwealth serum lab.• Symptoms include immediate intense pain,
erythema, cyanosis, edema, nausea, vomiting, hypotension, delirium and cardiovascular collapse.
• Irrigate, debride and soak wound in hot water 30-60 minutes to denature venom.
• Analgesia and wound care.
Saltwater Catfish
• Found in the warm tropical of Indo-pacific.• Fins contain complex venom• Symptoms include Intense pain. Systemic
response is rare, but may include muscle cramps, tremor, fatigue, syncope, and cardiovascular collapse.
• Venom is thermolabile.• Wound care including broad-spectrum antibiotics
(Vibrio species).
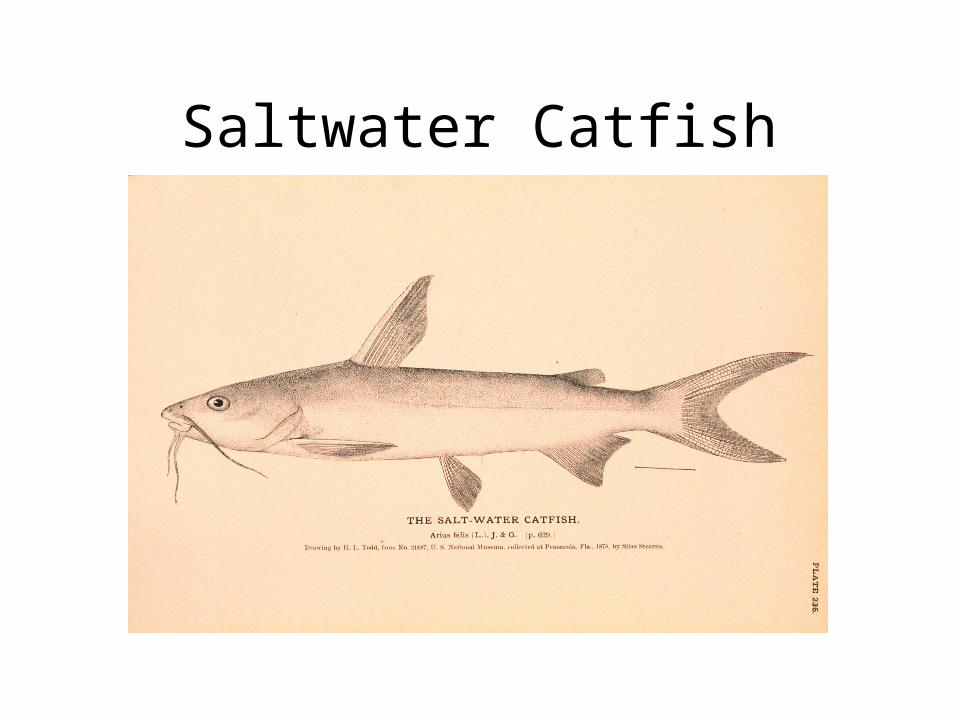
Saltwater Catfish
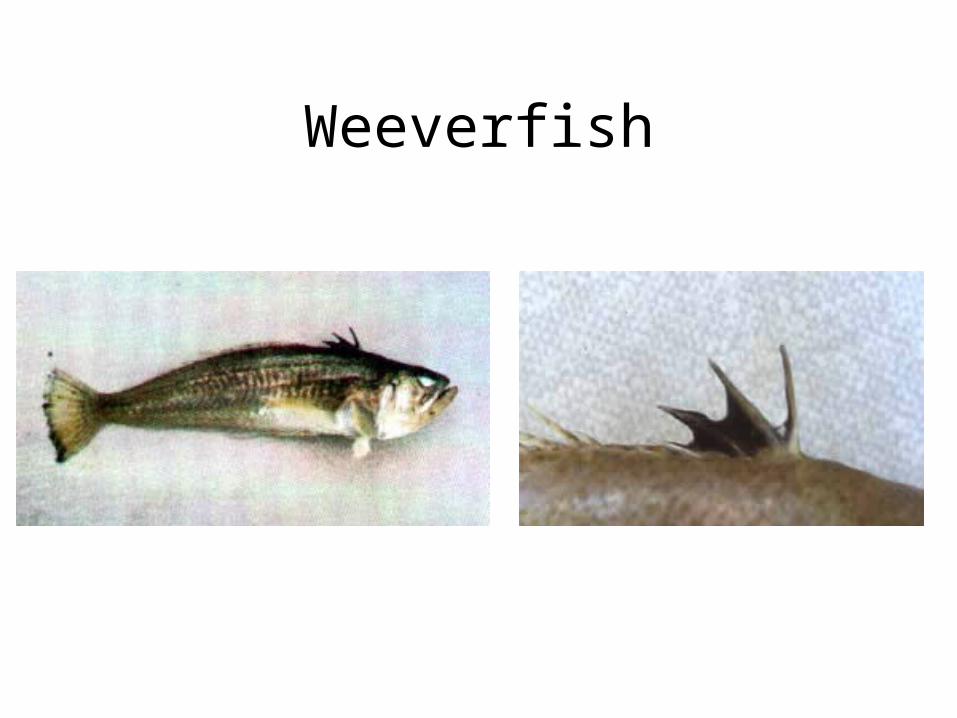
Weeverfish
• Found in English channel.
• Venom is on dorsal fin.
• Venom is thermolabile.
• Similar treatment to other fish.
Weeverfish
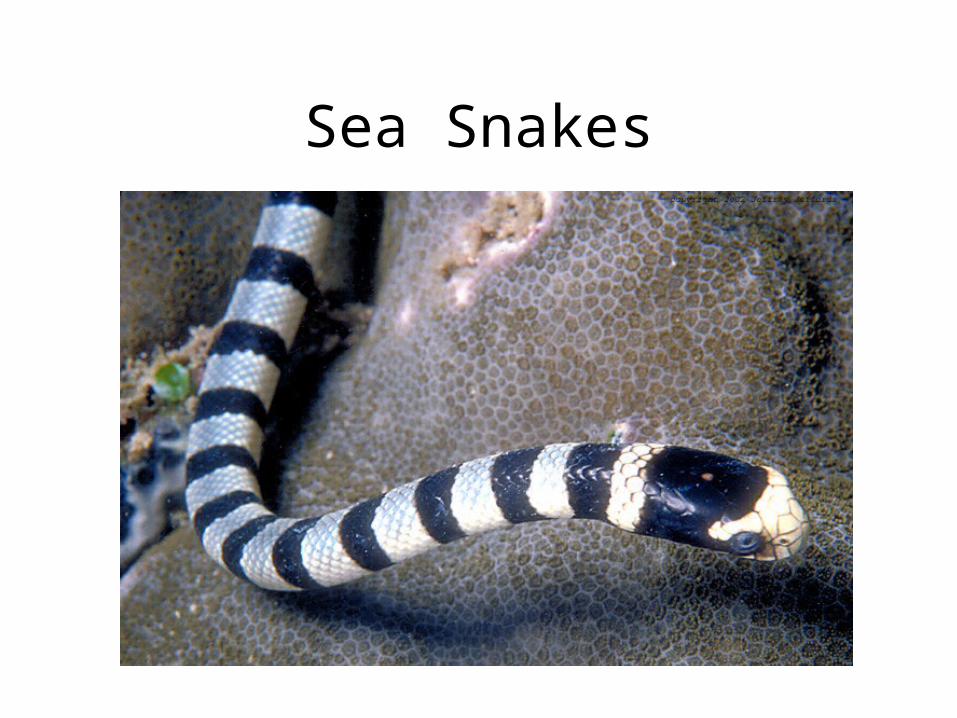
Sea Snakes
• Found in warm tropical waters in the Indo-pacific and off the coast of Australia.
• Air breathing and usually not aggressive.• Venom is extremely toxic. (more than cobra
venom.)• Most sea snake bites can not penetrate a 1/8
inch wetsuit and do not envenomate with every bite.

Sea Snakes
• Venom is a heat-stable nonenzymatic protein.• Venom blocks acetylcholine.• Asymptomatic latent period of 10 minutes to 6-8
hours.• Symptom’s include malaise, anxiety, and stiffness.• Late symptom’s include aching, paralysis, trismus,
ptosis, hepatic, renal, and respiratory instability.• Cardiovascular collapse and death.• 10% of untreated cases are fatal.
Sea Snakes

Sea Snakes
Sea Snake’sTreatment
• Immobilize site, soaking in hot water not effective.
• ABC’s, may require hemodialysis and respiratory support.
• Hospitalize and administer antivenin.• Polyvalent sea snake antivenin from Australia
Commonwealth serum lab.• Use polyvalent land snake antivenin if sea snake
antivenin is unavailable.

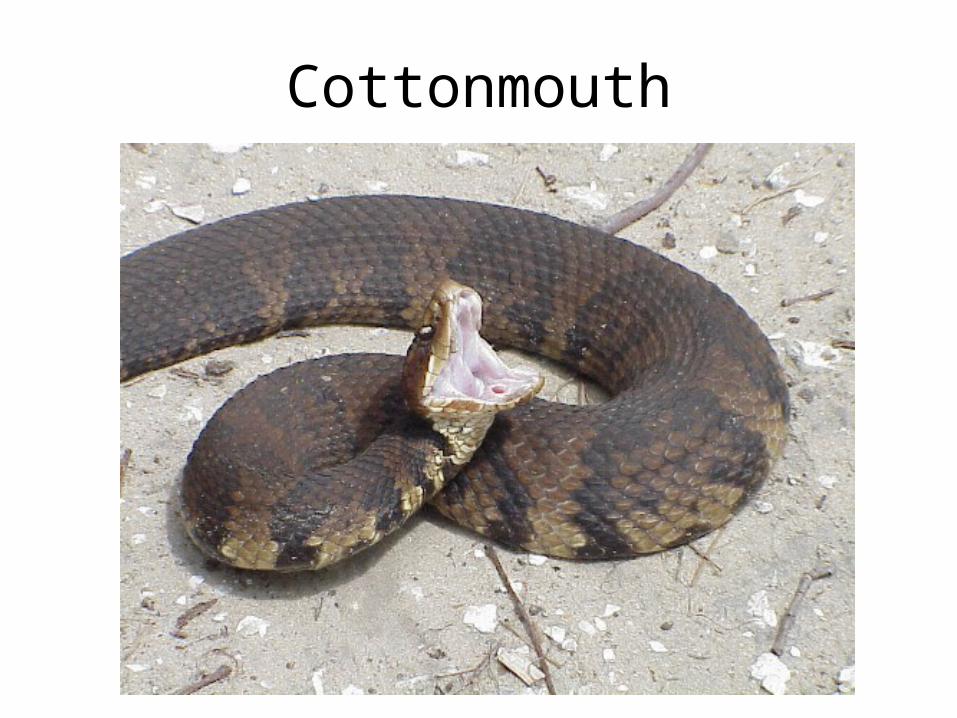
Cottonmouth
• Also know as Water Moccasin.• Snake found in fresh water area’s.• North American cottonmouth found in southern
states as far north as Virginia and as west as Texas.
• Aggressive, territorial snake with lightning-fast, bacteria-rich hemotoxic bite.
• Symptoms include nausea, vomiting, hypotension, DIC, hemolysis, seizures and respiratory paralysis

Cottonmouth
Cottonmouth

Cottonmouth

Cottonmouth
Cottonmouth Treatment
• Remove jewelry and tight fitting clothing around wound.
• Clean (Betadine), immobilize, pressure dressing.• Administer antivenin (horse serum, test for
hypersensitivity,).• IV sedation, analgesics and antibiotics.• Do not use ice, tourniquets, incision and oral
suction.

Blue-Ringed Octopus
• Found in costal waters of New Zealand and Australia.
• Painless bite followed by abnormal sensation in mouth, neck and head.
• Nausea, vomiting, dyspnea, and apnea.• May also have visual disturbances,
impaired speech and swallowing, weakness and paralysis.

Blue-Ringed Octopus

Blue-Ringed OctopusTreatment
• Neurotoxin blocks peripheral nerve conduction.
• May need cardiovascular and ventilatory support.
• Immobilize the affected limb.
• Pressure dressing.
• Clean bite- tetanus and antibiotic coverage.
Cone Shells
• Found in costal reef’s throughout the world.
• Shelled animal have detachable, dart-like, muscular, extensible proboscis.
• Venom is complex. It inhibits acetylcholine and effects sodium channels causing sustained contractions.
• Venom is Thermolabile.

Cone Shells

Cone Shells

Cone Shells
• Stings usually occur on hand or foot.
• Minor sting cause local blanching, cyanosis and edema.
• Systemic findings include pain, numbness and paresthesia of mouth and lips.
• Paralysis and respiratory failure possible.
• No antivenin is available.
Cone ShellsTreatment
• Immobilize the limb and apply pressure dressing (not tourniquet).
• Soak in hot water 30 to 90 minutes.• Severe reactions including paralysis may require
CPR and ventilatory support.• Edrophonium 10mg IV may be used for paralysis• Naloxone 2-4mg IV may help severe hypotension.
(blocks beta-endorphin vasodepressor response.• Wound care including tetanus, analgesia, and
antibiotics.

Anaphylaxis
• ABC’s– Airway protection – 100% Oxygen– Two IV lines- fluid resuscitation with RL or NS
• Epinephrine 1:1000 .2-.5mg SC/IM• May repeat every 30min• In severe cases consider Epinephrine
1:10,000 .2-.5mg IV.• Benadryl and Steroids IM/IV.
General Wound Care
• Irrigate wounds and keep clean and dry.
• Pressure dressings.
• Remove any foreign bodies.
• Broad spectrum antibiotic coverage. (include Vibrio sp.)
• Analgesia and steroids (topical or systemic).
• Tetanus prophylaxis.
Review
• Remember ABC’s including c-spine immobilizations in suspected marine trauma.
• Puncture wounds due to saltwater catfish, scorpionfish, sea-urchins, starfish, stingrays, cone shells and weever fish should be immersed in hot water (113 degree F) for 30-90 minutes or until pain subsides.
Review
• Treat rash associated with anemone, fire coral, jellyfish, and sponges with seawater bath or 5% acetic acid.
• Handle and remove nematocysts with care.• Be prepared to treat anaphylaxis and
cardiovascular instability.• Wound Care• Contact local poison control center or toxicologist
for possible antivenin administration and transport of severe reactions.


Drowning and Near Drowning

Definition
• Near Drowning– Suffocation by submersion, with at least 24
hours of survival.
• Drowning– Death within 24 hours of suffocation by
submersion.

















