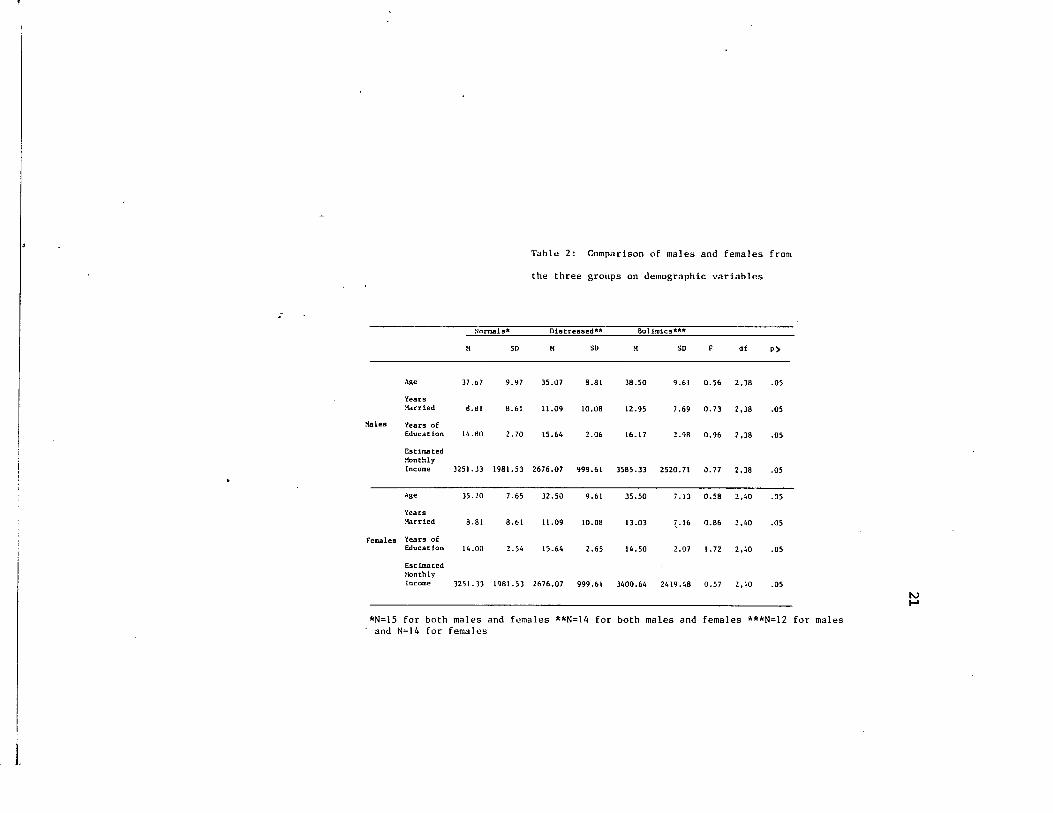
Louisiana State University LSU Digital Commons LSU Historical Dissertations and eses Graduate School 1987 Marital Relationships and Conflict Resolution Skills of Bulimics. Dorothy Jo Van buren Louisiana State University and Agricultural & Mechanical College Follow this and additional works at: hps://digitalcommons.lsu.edu/gradschool_disstheses is Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Historical Dissertations and eses by an authorized administrator of LSU Digital Commons. For more information, please contact [email protected]. Recommended Citation Van buren, Dorothy Jo, "Marital Relationships and Conflict Resolution Skills of Bulimics." (1987). LSU Historical Dissertations and eses. 4479. hps://digitalcommons.lsu.edu/gradschool_disstheses/4479
Transcript
Louisiana State UniversityLSU Digital Commons
LSU Historical Dissertations and Theses Graduate School
1987
Marital Relationships and Conflict ResolutionSkills of Bulimics.Dorothy Jo Van burenLouisiana State University and Agricultural & Mechanical College
Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_disstheses
This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion inLSU Historical Dissertations and Theses by an authorized administrator of LSU Digital Commons. For more information, please [email protected].
Recommended CitationVan buren, Dorothy Jo, "Marital Relationships and Conflict Resolution Skills of Bulimics." (1987). LSU Historical Dissertations andTheses. 4479.https://digitalcommons.lsu.edu/gradschool_disstheses/4479
The most advanced technology has been used to photograph and reproduce this manuscript from the microfilm master. UMI films the original text directly from the copy submitted. Thus, some dissertation copies are in typewriter face, while others may be from a computer printer.
In the unlikely event tha t the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyrighted material had to be removed, a note will indicate the deletion.
Oversize m aterials (e.g., maps, drawings, charts) are re produced by sectioning the original, beginning at the upper left-hand corner and continuing from left to right in equal sections with small overlaps. Each oversize page is available as one exposure on a standard 35 mm slide or as a 17" x 23" black and white photographic print for an additional charge.
Photographs included in the original manuscript have been reproduced xerographically in this copy. 35 mm slides or 6" x 9" black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order.
UMIAccessing the World’s Information since 1938
300 North Zeeb Road, Ann Arbor, Ml 48106-1346 USA
Order N u m b er 8811440
M arital relationships and conflict resolution skills o f bulimics
Van Buren, Dorothy Jo, Ph.D.
The Louisiana State University and Agricultural and Mechanical Col., 1987
UMI300 N. Zeeb Rd.Ann Arbor, MI 48106
PLEASE NOTE:
In all cases this material has been filmed in the best possible way from the available copy. Problems encountered with this document have been identified here with a check mark V .
1. Glossy photographs or p ages_____
2. Colored illustrations, paper or print______
3. Photographs with dark background_____
4. Illustrations are poor copy______
5. Pages with black marks, not original copy______
6. Print shows through as there is text on both sides of p a g e _______
7. Indistinct, broken or small print on several pages l /
8. Print exceeds margin requirem ents______
9. Tightly bound copy with print lost in sp ine_______
10. Computer printout pages with indistinct print______
11. Page(s)____________lacking when material received, and not available from school orauthor.
12. Page(s)____________seem to be missing in numbering only as text follows.
13. Two pages num bered . Text follows.
14. Curling and wrinkled pages _ _ _
15. Dissertation contains pages with print at a slant, filmed a s received_________
(1985). The psychophysiology of bulimia. Advances in Behaviour
Research and Therapy. 7, 163-172.
Yudkovitz, E. (1983). Bulimia: Growing awareness of an eating disorder.
Social Work. 28* 472-478.
Appendix A: Diagnostic criteria for bulimia from the Diagnostic and
Statistical Manual of Mental Disorders (3rd ed.).
1) Repeated binge eating with binge defined as the ingestion of a
great deal of food in a relatively short period of time (two hours
or less)
2) The belief that one’s eating pattern is not normal and fear of
of losing control over one’s eating
3) Depression and negative self-thoughts following a binge
4) At least three of the following:
a. binging on easy to eat foods or high calorie junk foods
b. binging when alone or otherwise attempting to be secretive about
binging
c. The binge eating stops when the individual self-lnduces vomiting,
is interrupted, experiences stomach pain, or goes to sleep
d. a history of severe dieting and/or the use of purgative methods
following binging (i.e., self-Induced vomiting, laxative abuse,
and/or diuretic abuse)
e. fluctuations in weight of ten or more pounds as a result of
binging and restricting
5) Anorexia nervosa or other physical health problems must be ruled out
as causes of the bulimic symptoms
43
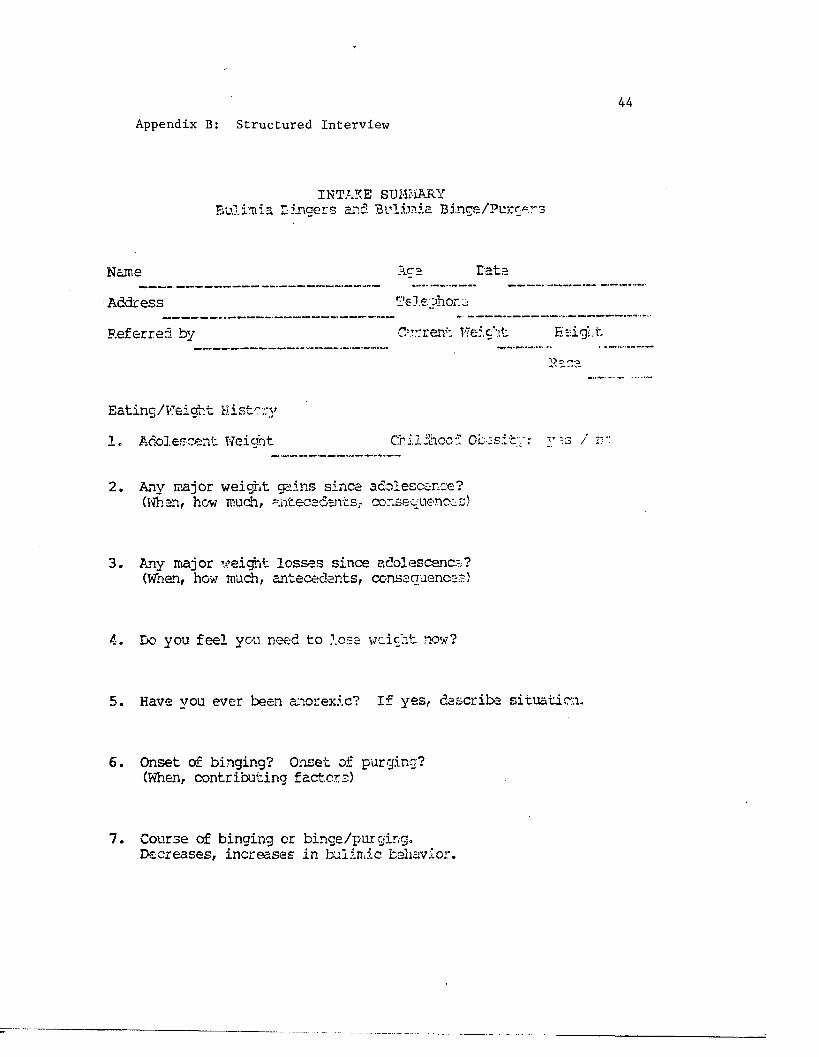
Appendix B: Structured Interview
INTAKE SUMMARY Bulim ia Lingers and Bulim ia Binge/Purgens
Name Eata
Address L'ele ohor
Referred by Current Weight Eaig'
Eating/W eight H istory
1 . Adolescent Weight Childhood Ob:-s. v is /
2 . Any major weight gains since adolescence? (Whan, how much, antecedents,- consequences)
3 . Any iriajor weight lo s se s since adolescence? (When, how much, antecedents, consequences)
4. Bo you f e e l you need to lo se weight now?
5 . Have you ever been anorexic? I f y e s , describe s itu ation -
6 . Onset of binging? Onset of purging? (When, contributing factors)
7 . Course of binging or binge/purging.Decreases, increases in bulim ic behavior.
45
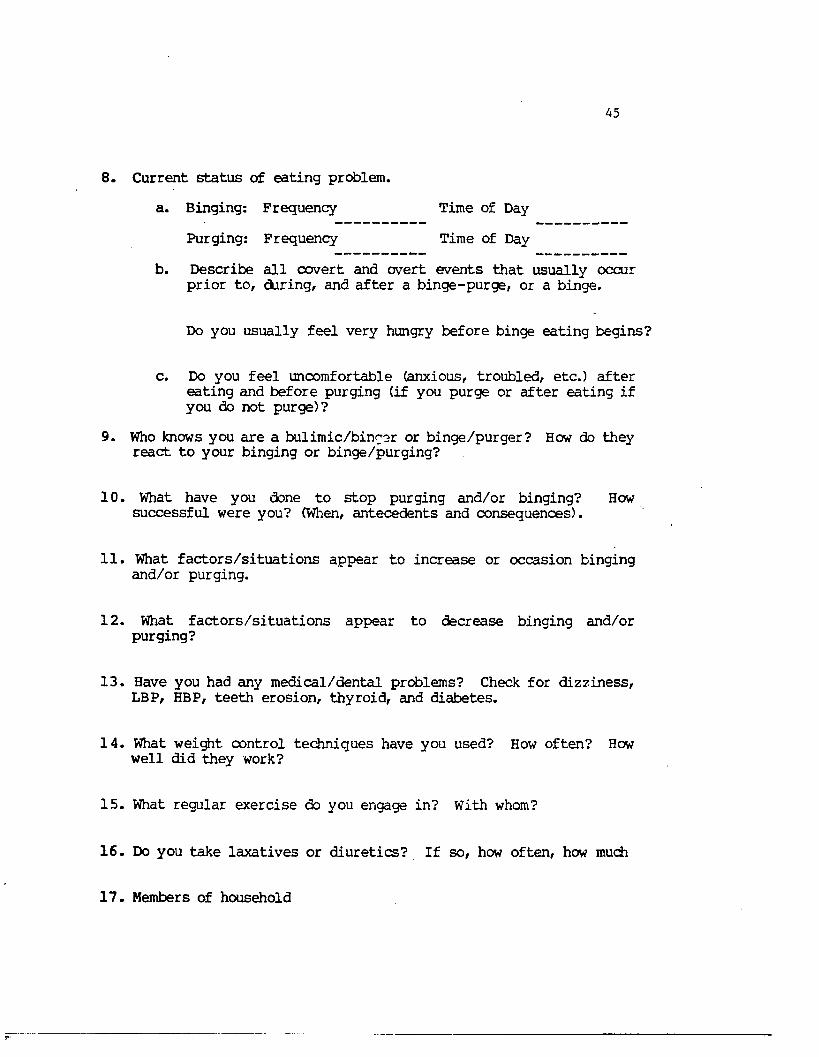
8 . Current sta tu s o f eatin g problem.
a. Binging: Frequency Time of Day
Purging: Frequency Time of Day
b. Describe a l l covert and overt events th at usually occur prior to , during, and a fter a binge-purge, or a binge.
Do you usu ally f e e l very hungry before binge eating begins?
c. Do you f e e l uncomfortable (anxious, troubled, e tc .) a fter eating and before purging ( if you purge or a fter eating i f you do not purge)?
9 . Who knows you are a bu lim ic/b inger or binge/purger? How do they react to your binging or binge/purging?
1 0 . What have you done to stop purging and/or binging? How su ccessfu l were you? (When, antecedents and consequences).
1 1 . What fa c to r s /s itu a t io n s appear to increase or occasion binging and/or purging.
1 2 . What fa c to r s /s itu a t io n s appear to decrease binging and/or purging?
1 3 . Have you had any m edical/dental problems? Check for d izz in ess, LBP, HBP, teeth erosion , thyroid , and diabetes.
1 4 . What weight control techniques have you used? How often? How w ell did they work?
1 5 . What regular exercise do you engage in? With whom?
1 6 . Do you take la x a tiv es or d iu retics? I f so , how often , how much
1 7 . Members o f household
46
1 8 . Are there any s ig n if ic a n t others who would p a r tic ip a te in your treatm ent?
1 9 . Are there any s ig n if ic a n t others who would in ter fere w ith your treatm ent? Describe any ob stacles.
2 0 . Other Comments:
47
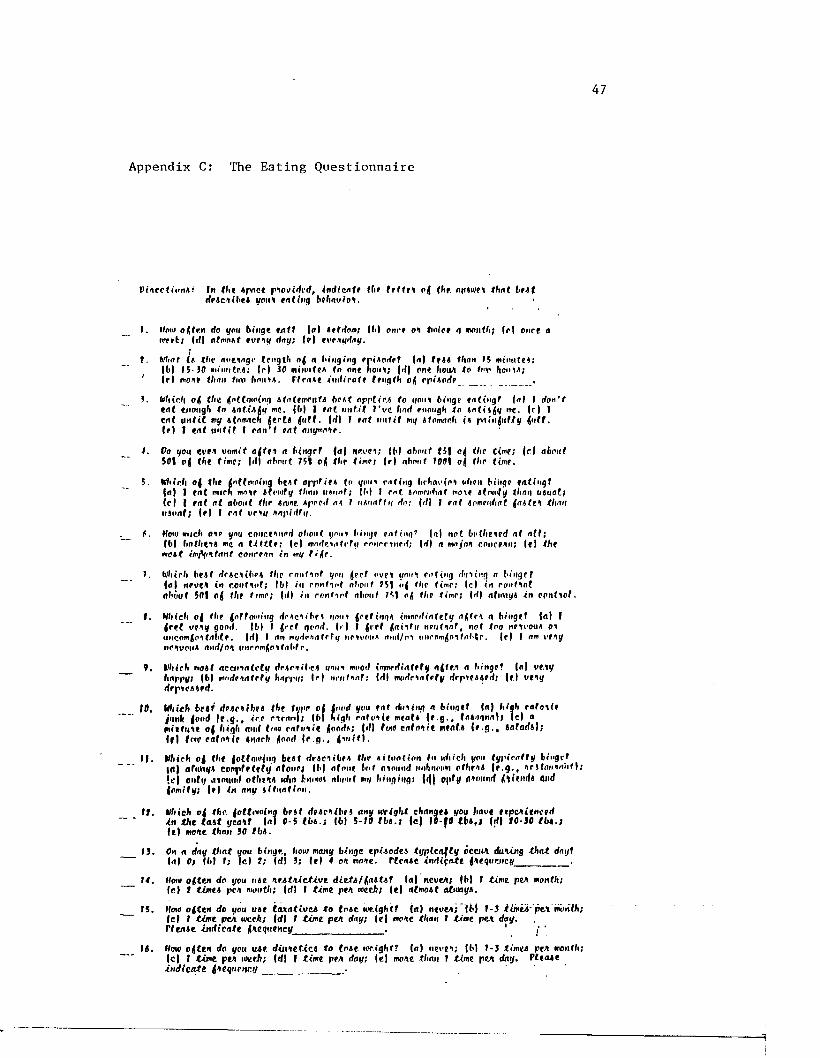
Appendix C: The Eating Questionnaire
In {he Apace p iov irti'd , in d ic a te the f e l tM o | {Fir. flfMWCt th a t ItAf rfpAc'ii.beA you* e a t (Mi) behav io l.
f . lloio oftr.n Ho yon binge t u f f | a | aefrtom; |b | once o* finite g month; | r | once ainert; |rf| rtfmoAf eveny fhty; I f ) ewnyrtoy.
1. Miitf | a the n o t ing r leng th o f n binging eniAortpf Ml than 15 minute*;| b | 15-30 monitrA; | r | 30 minufeA to one non*; |r t| one fioaA to imp Fiouia;
4 j r i moor than f«v h n i m . rtrnAe in r t i r n t f leng th of cpiAnrlp __
3. Which o f (ftt ((nffoiaiMg AtotfmPnfA b f t t a p p tir i to uout binge foCtngf Ml I rfon'fc o t enough to in t i J fy me, |( i| I eat u n fit I ' v e hart enough to m t i s f y me. f r | I en t u n f i t mg etnmncli ( e r (4 fluff. Ml I eat u n t i l mg Afomarh i* pninfluf/y fluff.( r | I eat u n l i t I can 't eat anymn^p.
•I. Vo you eve* uomif a f f e i a binget M l iievci; IM about f5 f of (he time; | c | about501 ofl th t tin e ; Ml about 751 o f the time; | r | nbmif 1001 of tl i p t in P.
5. Which of the flnffotuing beAf oppfifA (n youi r a t in g brhavcot (jfipti binge f a t i n g !Ml I fn{ much mnie Afoinfy than HAnnf; jb| I ro t AnmrjWtdf mole Aton'fy l i m n UAuflt;(c l ( fat at flhotil the Aarne. Aprprt a*, 1 vAuafiu Ho: Ml I eat iomenbat fasten thanusual; | f | I rat vriy napirity.
f . How much ate you concerned a b o u t , ynui binge r u l i n g 9 Ml n o t botheied a t o f f ;|b | hofhe*** me a tittle; (cl mortem left# coiirrinrrt ; |rt| a roa/oA concern; (e | fhfmo*{ jnfyltant court An in mg f i f e .
1. Which beat rtrActlbM Ihc rniiMnf you fleet nvpi ynnt ea t ing rtmi’ng o binge 7 Ml nevCA in r.cnMuf; Ibl in rontyot nbouf 751 of Ihr limp; (cl in ronMol about 501 o j Ihf lime; |rt| i n r o n t io f abotif 751 ofl the tine; Ml afnviyi in c m l i o l .
f . Which of Ibp floffowing rtcac*nbpA i/oui fleeting* iwriprtinf ef y afltr* a binge! Ml Ii e t t v tay goort. |b l I fleet genrt. (» | I fleet flatit i; n r u l in f , no! too neivouA on luicomfloitnbtf. Ml I am mortcAafrfi/ iipivpiia mirt/ni uncom^o'tfrtbM. Ml I am w a y ncauoua rtnrl/on intromM^labf r .
9. Which moat accuialctif rtparaibea uona moort ifrvnrrtiateti/ a^tM a binge! Ml ve.iyhappy; |b l morfpirtfpfg hrtppg; Ir | nrutaaf; (rt| morfranfefy drpieaaert; jf.l VMJrtppiraarrf.
10, WIiMh beat deJicAihvi the twpr o l invd you t a t itming a bingef M) high r a t o i / f junfc food ( e . g . , 4e.* cirnmli |b | high c a fo i ie meafa M>9*» taa«igna|) (cl a mil l in e of high anrt Imo cafonie |oorta; |r!) foio c a fo i i e meat, a ( e g . , aafflrfal;Ml fo() turtrfr <onrf ( e . g . , <ii iU I .
I | . Wiirli o | th t |o((mi'{ng t«»( rfraciifcr* tliv aifimfion in nViich you <«/|*/rnff «/ Kiigtf| d | af iiMi/* c c m f i f f U f y n f o i i f j | l> | f l f n u e ( m f n m m i r f im f t i i r im c t h r i t | r . g . , a r j ( r t i i ' i n i i » | ; • c | outi/ Jintiml o th in t wlio fcniidt nliciif mi/ liingtitg; ' " . _ (lafiimrf ftUiirfa anrf (omity; | » | in nny iitiintlon.
I t . tlhieh o t the. lottmoiog be i t i t t tc t ib e i any weight changtt you have txp v iltn c tilin th t ta .it ycalT 1*1 0-5 I b t . ; Ibl S-10 th s . i ( e | 10-fO lb * .I Ml I0 -J0 t b i . ile i moae than 30 tb i .
13. On a day th a t you binge, how many binge tp i io d t i tijp lca fty occi*A dating th a t daijtMl 0; (M I; l e t ?; Irfl 3; le i 4 on mote, r tc n a e in d ig a tt fa tq iiuici/____________.
14. How o ften do you m e le i tA ic t iv e d i e t i / f a i t e t la) nevea; IM I t ime pea month;( e | t timet, pea month; Id I I tim e pen uieth; | e | ntmojf aJbaayt.
15. How o f te n do you u te la x a tiu e i to l o t c u’e.igfitf Ml nevea; ( t | 1-3 itmejj- p t t iwit t t ;I d I tim e pea weeft; Ml I t im e pea day; ( e | mote than 1 time pea day.r f e m e ind ica te laeaueMey_________________ . 1 ‘
16. How o | t e n do you utt. d i i i ie t ic i to tm e loeight? Ml ne»*ea; IM 1-3 timea pea monlli; | c | I tim e pen we eh; Ml I tim e pea day; | e | moae tlmn I t ime pea day. f le a te in d ic a te fteq uc.nr.y_________________ .
^
PLEASE NOTE:
Copyrighted materials in this document have not been filmed at the request of the author. They a re available for consultation, however, in the author’s university library.
These consist of pages:
APPENDIX D: The Bulimia Test bv Smith and Thelen (1984)DD. 48-52.
APPFNDTX F- Thp Dvarlir Adiustment. Scaleby Spani'er (1976); pp. 54-55
APPENDIX G: The Conflict Inventory; pp. 56-80
APPFNDTX H: The Relationship Belief Inventory; PP. 81-
UniversityMicrofilms
International300 N Zeeb Rd., Ann Arbor, Ml 48106 (313) 761-4700
53
Appendix E: Consent Form
Too a r e being noised to p a r t i c i p a t e t h n r e aen rch p r o j e c t being conduc ted by Itonnld A. WllliemBoMi 1'h.D. end Dorothy J . Vpn Burpn, II. A. through thn Ile'pnrtmpnl o f I’aycliology e l l ou l a tn nn B tn l e U n lv e r a l t y . P l eaae rend Hie fo l l owing d e nc r f p l l o n of llip p r eae n t a tudy c a r e f u l l y .
In t l i l a otudy your name w i l l bo Isept o t r l c l l y do n f l d n n t i a l and a l l forma you f i l l ou l w i l l Uae code numbere ao t h a t you w i l l nol need lo i d e n t i f y yo o rBo l t . Too wi l l bp naltod to p a r t i c i p a t e In a e t r u c t t i r e d i n t e r v i e w I f you lieve nol nl r endy done no, In a d d i t i o n you w i l l be anlsed lo f i l l out anmn q ue a t l on nn l r e a having lo do wi th your e a t i n g b e b i t n and your mn r l t n l r e l a t i o n s h i p . Ton w i l l f i l l t lie no q un n l i o nn a l r ea oul I n a room appa rn le from your rpnuno. Tou end your ennuae wi l l tbnn bo r e - j o in e d and yon w i l l bp nelied lo dlncuna o i i p of the Innt ruraentn yon f i l l e d o u l . Till p d l a cu an lon wi l l be r e co rded on v ideo t ape ,Tou may acl iedule an Appointment wltli t he expe r imen t e r lo r e ce i ve fpodbacls r e g a r d in g H i p I n fo rma t ion H i p quent.J onnal r o r y i e l d conce rn ing your o n l i n e h a b i l e end t he a t r eng l i r and wenisneaRea of your mnr l t n ] r e l a t l o n o b l p . I f you a r e e n r o l l e d In an I n t r o duc tory naycliology COUran you wil l rocnlve exit n c r e d i t pn ln t a for yonr p a r t i c i p a t i o n In t h i n atudy.
Tour parllclpntlon In tlila atudy la nlrlclly voluntary olid you may withdraw your parti cl ration at any lime wlllmul penalty. If you bnve any queationa plepse aali Hie Individual wbo ndml nl alered tlila conaent form to you. It you npr»e to participate In Ibl a atudy and If all of your queationa have lienu nnawercd to your ant la tnc II o n , pi Pane algo yonr nnmn below.
1 bnve r ead tbn above d e a c r l p t i o n ot t l i l a atudy and a l l hy quaRtlonh have bean anrwerpd to may e n t l n f a c t i o n . 1 hereby vo l u n t ee r to p a r t i c i p a t e I n t l i l a p r o j e c t an I n d i c a t e d by my a lg nn tu r e .
(Hama) (bate)
(tllheen )
83.
Appendix I:
Handbook for the Communication Skills Test
General, description:
The CST requires observers to make a 5-point rating of each statement emitted by subjects during their problem-solving interaction.
The observer attends only to the speaker and rates the speaker's statement: very negative — 1 negative — 2 neutral — 3 positive — A very positive — 5
Observers follow a two-step procedure in making CST ratings.First: As the speaker talks, the observer scans the speaker's statement
for the occurrence of Individual positive, very positive, negative, and very negative communication/problem-solving behaviors (as defined within this booklet).
Second: When the speaker is finished, the observer then makes a judgement of the overall "positiveness" of the entire statement on the basis of the individual behaviors emitted by the speaker during that statement using the scoring sheet.
These ratings reflect the degree of communication proficiency exhibited by the speaker.
Observers are given the following guidelines for judging CST scores:
When either positive, very positive, negative, or very negative behaviors occur within the context of otherwise neutral behaviors, the entire statement is rated in accordance with the type of positively or negatively valued behavior that occurred.
When both positive and very positive or both negative and very negative behaviors are combined in the same statement, the more extreme rating of very positive (5) or very negative (1) is given to the statement.
Statements containing only neutral behaviors are rated neutral (3).
Frequently behaviors with different positive and negative valences occur in the same statement. In this case observers are Instructed to judge the relative contributions of the individual behaviors to the statement as a whole and to produce one CST rating that best reflects the overall level of communication skill exhibited in the statement.
The Communication Skills TestVfijci Positive = 5 pointsA) Summarizing other or both:
Reneating back the content of what the partner has said and/or what both partners have said up until that point before going on to present another point of view or solution.Ex: "So what you're saying is ..."
"What you've said so far is...""What I understand is that..."
Your notes:
B) Checking out:Similar to summarizing but the goal is to make sure that the listener actually heard what was really meant by the speaker. To see if intent equals impact.Ex: "I don't think you've been a spendthrift ijt that's
what you felt I was saying...""I feel like you're making fun of me; Is that what you mean tn do?"
Your notes:
Very Positive continued = 5 pointsC) Opinion/feeling probe:
The speaker asks the listner how s/he feels or thinks about what was said or the topic at hand.Ex: "What do you think febout that idea?"
"How do you feel about going out?""What's on your mind?"
Your notes:
D) Specific plan:The speaker suggests a specific plan for solving the problem under discussion. To be specific, the plan is to include who is to do what under what circumstances (who, when, where).Ex; "I think we should divide up the housework so
that I do the dusting and vacuuming on Saturday mornings and you clean the bathrooms and mop on your day off.""I could get the children bathed while you cook dinner on week nights and on the weekends we could switch."
Your notes:
E) Specific feedback:The speaker tells his/her partner what he/she thinks about what the partner has done or :said and why.Ex: "I like your idea because it gives each of us
some time to ourselves.""I got angry when you criticized me in front of your mother."
Very Posjtive continued = 5 pointsH) Validation:
Similar to summarizing except that in addition to repeating back the content of the speaker's message the partner also repeats back the feelings the speaker has expressed. Validation deals more with the affect of the cnmmunicat'* on.Ex: "You're feeling real bummed out about not getting
that promotion.""It's exciting for you to get to plan this year's family reunion."
"It makes you angry when I talk to other women at parties."Your notes:
87
Very positive continued = 5 pointsYour notes:
F) Back on beam:
The speaker says something to get the discussion back on the original topic. This usually occurs in response to the partner having gotten off the topic but the speaker can also pull him/herself back on track if s/he has strayed from the discussion.Ex: "Let's get back to discussing how to discipline
Tommy""I'm sorry, I think I got off track. What were we talking about?"
"We need to stay focused on the problem at hand before we start talking about that."
Your notes:
G) Metacommunication:The speaker makes a statement that ties together the preceding discussion.Ex: "Not only have we discussed how little time we've
been getting to spend with each other but we've actually come up with some good solutions.""Although the problem seemed to be that my mother interferes with us it has turned out that I'm really not assertive enough with her."
Your notes:
Positive = 4 pointsA) Feeling statement:
The speaker expresses his/her own feelings in a direct and specific way. I feel _______ because________.Ex: "I was angry when you came home.late last night."
"I feel good when you compliment me.""I get upset because you are yelling at me."
Your notes:
B) Agree or disagree with rationale provided:The speaker agrees or disagrees with what his/her partner has said and gives a reason for his/her disagreement or agreement.Ex: "I agree that we need to take more time with the
children because our work schedules have gotten busier.""I don't think that is such a good plan since we already told our parents that we would alternate spending holidays with them."
Your notes:
C) Plan suggestion that is not specific:The speaker makes a general statement about a possible course of action or problem solution but does not describe the who, were, when, and how of implementing the solution.Ex: "We need to do more things together."
"The problem is that we have too many debtd so we need to spend less money."
89
P.o.sLtiye continued = b points Your notes:
D) Compliment:The speaker says something nice to his/her partner or makes some other positive comment to the partner regarding his/her appearance, behavior, and/or ideas.Ex: "You sure have a way with words."
"You did a nice job re-papering the kitchen." "That's a great idea*"
Your notes:
E) Clarification request:The partner is asked to be more specific in his/her communication or is asked to clear up a possible mi scommunication.Ex: "I'm not sure I understand what you're trying to
say.""Would you explain what you mean?"
Your notes:
F) Accept responsibilityThe speaker describes some way he/she is involved in the problem under discussion.Ex: "I know that I have a tendency to interrupt youand that this makes it difficult to talk with me."
Positive continued = k points"I probably haven't been doing as much housework as I should."
Your notes:
G) Empathy:An expression of understanding that is less specific than that found in validation.Ex: "I know how you must feel."
"I can understand that you're upset.""That must be tough to take."
Your notes:
H) Summarizing self concisely or to clarify a point:The speaker repeats what s/he was trying to say in a sentence or two without more elaboration. S/he may use this to clear up a possible misunderstanding.Ex: "What I was trying to say is that I care about you
"As I said, I disagree with that plan."Your notes:
I) HumorA partner says something light or funny during the discussion that does not appear to be sarcastic or a put down.
Occurs when discussion of one problem area drifts into discussion of other problem areas without any of the problems getting resolved.Your notes:
B) Kitchen sinking:Occurs when the discussion starts on one issue and, before there is time to explore that issue, one partner or the other drags in other gripes that may or may not be related.Your notes:
C) Mind reading with negative affect:Mind reading occurs whenever one person assumes what another person is either feeling or thinking without asking.Ex: "I know you like romantic-type movies, so I made arrangements to go to see the new picture in town tonight —
I'm sure you'll like it.""The problem is that you feel that the house is a mess all the time — and that's just not true."
Your notes:
D) PutdownEx: "You're an idiot."
"I can't get over how dense you are."
Your notes:
96
Very negative continued = 1E) Summarizing self
Occurs when each person continues restating his or her won position. Each person is so sure he or she is right that they both think it's a waste of time to try to hear and understand the other person’s viewpoint.Your notes:
F) BlamingEx: "It's all your fault that it's taking so long."
"If it weren't for you, I'd be a lot happier."Your notes:
G) Character assassinationOccurs when one partner attributes bad or insulting characteristics or qualities to the other partner.Ex: "You're an insensitive person."
"You're just like your mother, never satisfied,""You don't help around the house because you're lazy."Your notes:
H) Yes, but...Occurs when one partner's every attempt to make a suggestion or to state apoint of view has something wrong with it.Ex: "I know, but..."
"But I do things that way because I love you."Your notes:
Date Rater_______________ Couple # ___________ Tape #Inch Mark Begin_________ End
Sneaker Statement #MF
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5
Sneaker Statement #MF
Rating 1 2 3 4 5Speaker Statement it ...
M FRating 1 2 3 4 5
Speaker Statement H MF
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5Speaker Statement it , M
FRating 1 2 3 4 5
Speaker Statement it M F
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5SpSgtaeh Statement it M
FHating 1 2 3 4 5
Speaker Statement it MF
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5I Sneaker Statement it
M F
j Rating 1 2 3 4 5
Sneaker Statement it MF
Rating 1 2 3 4 5
Speaker Statement it M F
Rating 1 2 3 4 5I Sneaker Statement #! 1 F
Rating 1 2 3 4 5
Speaker Statement it M F
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5Sneaker Statement #
MF
Rating 1 2 3 4 5
Speaker Statement it M F
Rating 1 2 3 4 5
Speaker Statement it MF
Rating 1 2 3 4 5Sneaker Statement it
M FRatibg 1 2 3 4 5
Sneaker Statement #MF
Rating 1 2 3 4 5
Sneaker Statement it M F
Rating 1 2 3 4 5
Vita
Dorothy Jo Van Buren
A pril 12. 1987
Eejispna.i InifiiM.tJLon
Date o f B ir t h : January 20, 1958P la c e o f B ir t h : Johnson C i t y , TennesseeM a rita l S t a t u s : Married
O f f i c e Add r e s s
T albot O u tp a t ie n t Center 5414 B r i t t a n y D rive S u i t e CBa,ton Rouge, L o u is ia n a 70809 (5 0 4 )7 6 7 -2 9 7 7
l lo je Ad d re ss
575 Burgln AvenueBaton Rouge, L o u is ia n a 70808(5 0 4 )7 6 9 -3 5 7 9
EducationB.A. U n iv e r s i t y o f Kansas
Double Major: Psychology/Hunan DevelopmentDegree awarded May 1980
M.A. L o u is ia n a S t a t e U n iv e r s i t yMajor: C l i n i c a l P sychology (APA-approved program)Minor: B ehav iora l NeurologyDegree awarded May 1983
Ph.D. L o u is ia n a S t a t e U n iv e r s i t yMajor: C l i n i c a l P sychology (APA-approved program)Minor: B e h a v io ra l NeurologyDegree a n t i c ip a t e d August 1987
Honors end Awards1980 Phi Beta Kappa
Graduation w ith d i s t i n c t i o n Graduation w ith honors In psychology
1983 Phi Kappa Phi
98
C l i n i c a l E xper ience
October I9R5 - p r esen t
November 1985 - March 1986
September 1984 - Angust 1995
August 1983 - Mav 1984
August 1982 - May 1983
Ia lb f i ! Ou t p a t i e n t Cen t e r . Baton Rouge. L o u is ia n a . Conducting In d iv id u a l and c o u p le s therapy w ith an a d u lt o u t p a t ie n t p o p u la t io n - F a c i l i t a t o r o f the parent tr a in in g /s u p p o r t group. Served as t h e r a p i s t for groups d e s ig n e d to t r e a t I n d iv id u a ls r a is e d In a l c o h o l i c or o th e r w ise d y s f u n c t io n a l homes.S u p e r v iso r s : Donald A. W ill iam son ,Ph.D. and Johnny Matson, Ph.D.
Cental an Problem Eating (COPE).Baton Rouge General Medical C enter,Baton Rouge, L o u is ia n a . Developed and saw to the Implementation o f an o u t p a t ie n t treatm ent program for i n d iv i d u a l s w ith e a t in g d i s o r d e r s . C l i n i c a l D ir e c t o r : Carol A la t a lo S u p e rv iso r : Donald A. W ill iam son , Ph.D.
C l i n i c a l P sychology In te r n . U n iv e r s i t y o f Alabama in Birmingham (UAB) School o f M edic ine , Department o f P sy c h ia tr y (APA-approved I n t e r n s h ip ) .S u p e rv iso r : W illiam B. Beldleman, Ph.D.
MuJLt C l in ic . ! P sy c h o lo g ic a l S e r v ic e s Center (PSC), L o u is ia n a S t a t e U n iv e r s i t y (LSU). C o - t h e r a p l s t for group troatment program for b u l im ic s . A lso conducted genera l a d u lt ou tp at ien t , a s s e s sm e n ts and trea tm ent.S u p e rv iso r : Donald A. W ill iam son , Ph.D.
Pedi a t r i c Psych o logy S e r v i c e . Eatl K. Long Memorial H o s p i t a l , LSU School o f M edic ine . C on su ltan t to I n p a t i e n t and o u t p a t ie n t p e d i a t r i c s e r v i c e . Performed I n t e l l e c t u a l and academic a ss e s sm e n ts . Provided parent t r a in in g and d eve lop ed c o n t in g e n c y management, programs to In c r e a se com pliance with m edica l regim ens.S u p e rv iso r : Mary Lou K e l l e y . Ph.D.
August 1981 - August 1982
Jnnuary 1981 - May 1981
August 1990 - December 1980
le a c h i n g , AdmLo.lstLatlve and Rqs.eejrch Exper t ence
January 1987 - p r e se n t
August 1983 - Mar 1991
August 1982 - Mav 1983
August 1981 Hay 1982
AdlU.t CLln-lE. PSC, LRU. Provided a ssessm en t and treatm ent to a du lt o u t p a t i e n t s - C o -In s tr u c to r for r e l a t i o n s h i p enhancement c l a s s o f f e r e d through I.SU's L e is u r e S e r v ic e s Program. S u p e r v i so r : Bernard .1. J ensen , Ph.D.
E s n i ix H edidDB GJLiniS. Earl K. Long Memorial H o s p i t a l , LSU School o f M edicine . S e iv e d as c o n s u l t a n t to f a n l l y p r a c t i c e p h y s i c i a n s . Provided in p a t i e n t and o u t p a t i e n t assessm ent and treatm ent to a d u l t s and c h i ld r e n . S u p e rv iso r : P h i l l i p J. B r a n t le y , Ph.D.
Community p s y c h o lo g y . LSU. P a r t i c i p a t e d In o r g a n i z a t i o n a l m eetings o f the River Region P erson a l Gtowth program. Attended r e p r e s e n t a t i o n a l workshops and a s s i s t e d w ith programmatic r e sea r ch . S u p e rv iso r : Ralph M. Dreger , Ph.D.
P a r t - t im e I n s t r u c t o r s h i p , LSU. Teaching a s e c t i o n o f C h ild P sychology at the undergraduate l e v e l .Su p e rv iso r : Johnny Matson, Ph.D.
Ic.Qc.hlog A s s i s t a n t , Adult C l i n i c , PSC, LSU. Provided s u p e r v i s io n to f i r s t and second year c l i n i c a l graduate s t u d e n t s In assessm ent and psychotherapy . Carried out a v a r i e t y o f a d m in i s t r a t iv e t a s k s .S u p e r v i s o r s : N a th a n ie l G o t t f r i e d ,Ph.D. and Bernard J . Jensen , Ph.D.
Reseaxcb A s s i s t a n t . LSU. Designed and Implemented new and e x i s t i n g resea rch p r o j e c t s In the a r ea s o f s o c i a l s k i l l s and m a r ita l d y s f u n c t io n . S u p e rv iso r : Bernard J . J ensen , Ph.D.
Teaching A s s i s t a n t . PSC, LRU. C arried out a d m i n i s t r a t i v e d u t i e s .S u p e rv iso r : N a th a n ie l G o t t f r i e d , Ph.D.
May 1081 •• Re.SDJUch A s s i s t a n t . Earl K. LongAugust tOSI Memorial H o s p i t a l , I.SU School n f
M edic ine . A s s i s t e d )n the c o l l e c t i o n and summarization o f data fo t ongoing research p i o j e c t s .S u p e rv iso r : P h i l l i p J. B r a n t le y . Ph.D.
l e a c h i n g AssJLsienJ;. LSU. Wrote and p.iaded exams. Su perv ised undergraduate r esearch a s s i s t a n t s .S u p e rv iso r : Yvonne Hardaway-Osborne. Ph.D.
Rotten teh Ass i s t a n t . Department o f Human Development. U n iv e r s i t y o f Kansas. Rated v id e o t a p e s o f c h i ld r e n ' s pla y b e h a v io r , c a l c u l a t e d r e l i a b i l i t i e s .1.rained nett r a t e r s , and developed beh a v io r a l d e f i n i t i o n s to accompany code c a t e g o i l e s .Su p e rv iso r : C. Jan Carpenter, d o c to r a lc a n d id a te
1979-1984 L e e lu te ? EiYen i o und e i e t aduate andgraduate c o u r s e s ! I n t io d u c t lo n to Reseatch Methods w ith C h ild ren ,Abnormal P sy ch o lo g y , T h eo r ie s o f P e r s o n a l i t y , Psychology o f Adjustment, and Psychotherapy Lab.
Pr.esen.tn-tlons
Van Buren. D .J . A Jensen, B .J . Couples ' e v a lu a t io n s o f req uest making: A s o c i a l v a l i d i t y r ep o rt . Poster p r e se n ted at the18th annual convent ion o f the A s s o c ia t io n for the Advancement o f Behavior Therapy (AABT). P h i la d e lp h ia , P en n sy lv a n ia , November. 1981.
Von Buren. D . J . , B lenn , B . , Mc.Anulty, D . , T a r l s l . S . , A Jensen ,B .J . C o u p le s ’ e v a lu a t io n s o f a communication s k i l l s t t a l n l n g ptogiam . Poster p r e se n te d a t the annual co n v e n t io n o f the S o u th ea stern P s y c h o lo g ic a l A s s o c ia t io n (SEPA), N e w O i le n n s , L o u is ia n a , March 1984.
Van Buren, D . J . , B r a n t le y , P . J . , A M artin, J .D. The r e l a t io n s h ip between knowledge and m e ta b o l ic c o n t r o l In d i a b e t i c p a t i e n t s .P oster p r e se n ted a t the World Congress In Behavior Therapy/17th annual AABT c o n v e n t io n , Washington. D .C .. December 1983-
Van ntiron, D .J . A b eh a v io r a l approach for p r e v e n t in g m arita l d i s c o r d . Paper p r e se n ted In the symposium t i t l e d , " P revent ion o f m ar ita l d i s s a t i s f a c t i o n : Improving In t im a te r e l a t i o n s h i p s . " at theannual co n v e n t io n o f SEPA. A t la n ta . G eorg ia . March 1983.
August 1980 - May 1981
August 1979 - May 1980
102
Vnn Buren, D .J . llow such H u e Is enough: R ofroctory p e r io d s c o n s id e r e d .Paper prpson led In the symposium t i t l e d , "Maybe they w i l l grow out o f i t : Tlno ns a treatm ent v n r l n b l o , ” a t the annualco n v e n t io n o f RCPA, A t l a n t a , G eorg ia , March 1981.
Van Buren, p . . I . , Houston, A . , ft Holmes, D. The e f f e c t s o f gender s p e c i f i c i t y on p r e s c h o o l e r s ' p e r c e p t io n s o f non and women's a b i l i t y to p a r t i c i p a t e In v a r io u s o c c u p a t io n s . Paper p r e se n ted In the symposium t i t l e d . "An a n a l y s i s o f s o c i a l i z a t i o n f a c t o t s In the development o f young c h i l d r e n ' s sex typed b e h a v io r ," a t the annual co n v e n t io n o f the A s s o c ia t io n for B ehav iora l A n a ly s i s , Dearborn, M ichigan, May 1980.
PubUfiatlQUP
Jenson , B..I. A Van Buren, D .J . ( 1 9 8 7 ) . C o g n it iv e Behavior Therapy: Conceptual ntid h i s t o r i c a l overv iew . The Southern P s y c h o l o g i s t ,3, J -7 .
leraanek. K.l, A Van Buren, D .J . ( i n p r e s s ) . Medical and h e a l t h r e l a t e d d i s o r d e r s In sc h o o l -a g e d c h i ld r e n . In J.C . W it t , S .N.Hi) lo t t , A F M. Gteshem ( F d s . ) . Handbook o f behayj.or thojagy in pduyntl.on. New York: Plenum P r e s s .
Mcknight, C .T . . Cock. T -D -, Kin?, A . , Van Buren, D . J . . A B i a n t l e y .P..I. ( 1 9 8 1 ) . An e v a lu a t io n o f c l i n i c f u n c t io n in g in f i v e Harl K. Long Memorial H o s p i t a l o u t p a t ie n t c l i n i c s . Journal o f the Ipuis .inna S t a t e Medical S o c i e t y . .1,36, 29 -30 .
P ra th er , R . , Upton, L . . W ill ia m so n , D . , D a v is , C . .I . , Ruggiero , L . ,A Van Rttren. D. ( In p r e s s ) . B ul im ia , d e p r e s s io n , and genera l p sy c h o r e th o lo g y , ln te tn a . t jo n a l Journa.l p f Eating D iso r d e r s .
Pj-Q.fessjonal Membejshilps
American P s y c h o lo g ic a l A s s o c ia t io nA s s o c ia t io n fo r the Advancement o f Behavior TherapyO b e s l 'v and Hating D i so r d e r s S p e c ia l I n t e r e s t Croup o f AABTS o c i e t y for B e h a v io ra l M edic ineS o u th e a s te rn P s y c h o lo g ic a l A s s o c lo t lo n
RefflxencssBernard J . J e n sen , Ph.D. Department o f P sycho logy U n iv e r s i t y o f C entra l F lo r id a O rlando, F lo r id a 32816-0001 (3 0 5 )2 7 6 -2 2 1 6
Mary Lou K e l l e y , Ph.D. Department o f P sychology L o u is ia n a S t a t e U n iv e r s i t y Baton Rouge. L o u is ia n a 70803 (5 0 4 )3 8 8 -8 7 4 5
Johnny Matson, Ph.D. Department o f P sycho logy L o u is ia n a S t a t e U n iv e r s i t y Baton Rouge. L o u is ia n a 70803 (5 0 4 )3 8 8 -8 7 4 5
Donald A. W ill ia m so n , Ph.D. Department o f P sycho logy L o u is ia n a S t a t e U n iv e r s i t y Baton Rouge, L o u is ia n a 70803 (5 0 4 )3 8 8 -1 4 9 4 (5 0 4 )3 8 8 -8 7 4 5
DOCTORAL EXAMINATION AND DISSERTATION REPORT
Candidate: D orothy Jo Van Buren
Major Field: P sy ch o lo g y
Title of Dissertation: M a r ita l R e la t io n s h ip s and C o n f l ic t R e s o lu t io n S k i l l s o f B u lim ic s