52
COVID-19 in Vermont Mark Levine, MD Patsy Kelso, PhD Jennifer S. Read, MD, MS, MPH, DTM&H, FAAP Breena Holmes, MD, FAAP

COVID-19 in Vermont
Mark Levine, MD
Patsy Kelso, PhD
Jennifer S. Read, MD, MS, MPH, DTM&H, FAAP
Breena Holmes, MD, FAAP

2Vermont Department of Health
Title of Program: Pediatric Grand Rounds
Title of Talk: “COVID19 and Children: Public Health and Clinical Medicine Integration at Its Best!”
Speaker/Moderator: Mark Levine, MD, Patsy Kelso, PhD, Jennifer S. Read, MD, Breena Holmes,
MD
Planning Committee Members: Jill Rinehart, MD, Amelia Hopkins, MD, Anna Zuckerman, MD
Date: 6/17/20
Workshop #: 20-125-51
DISCLOSURE:
Is there anything to disclose? No
Please list the Potential conflict of Interest (if applicable): _
All Potential Conflict of Interest have been resolved prior to the start of this program: Yes
(If no, credit will not be awarded for this activity.) There is No Commercial Support for this
Activity.
**Please note- CME credit must be claimed in HighMarks within 30 days of this
presentation.**

Today’s Objectives
• Review health equity, Vermont’s vision expressed in the State Health Improvement Plan, and a public health framework for reducing health inequities
• Explore racial disparities in COVID-19 in Vermont.
• Review data informing RESTART VT
• Review pediatric COVID-19 and Multisystem Inflammatory Syndrome in Children (MIS-C)
• Review pediatric experience including reopening childcare, summer programs and schools
3Vermont Department of Health

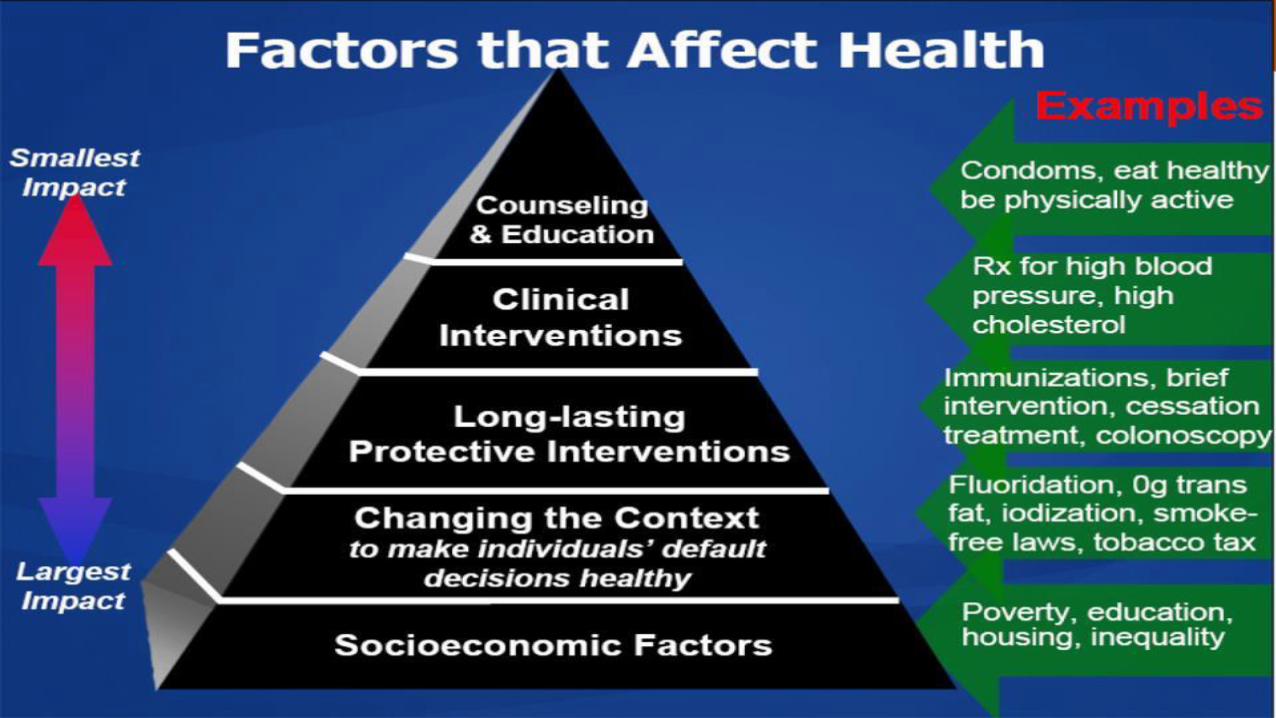
A Public Health Framework for Reducing Health Inequities; Racial Disparities in COVID-19 in Vermont
Mark Levine, MD
Commissioner of Health/VDHProfessor of Medicine/UVM
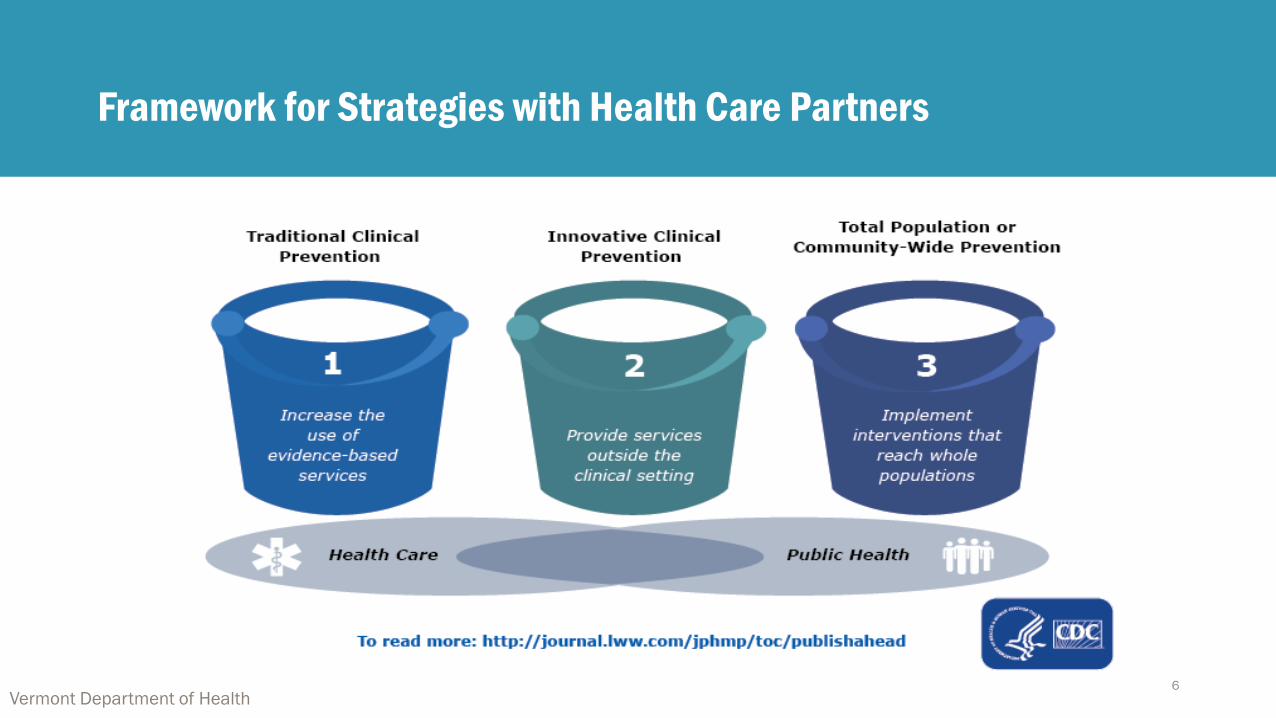
Framework for Strategies with Health Care Partners
Vermont Department of Health6

State Health Assessment and Improvement Plan
State Health Assessment •What do we know about the health of Vermonters?
State Health Improvement Plan – Vermont Priorities
•What are we going to do about it?
•What is the plan for all state partners, public and private, to improve health outcomes?
Vermont Department of Health

Priorities from the State Health Assessment
Health Conditions/Outcomes
• Child Development
• Chronic Disease
• Mental Health
• Oral Health
• Substance Use Disorder
Social Conditions (SDOH)
• Housing
• Transportation
• Food
• Income/Economic Stability
http://www.healthvermont.gov/about/reports/state-health-assessment-2018
Vermont Department of Health8

Health Equity
Health equity exists when all people have a fair and just opportunity to be healthy, especially those who have experienced socioeconomic disadvantage, historical injustice and other avoidable inequalities that are often associated with social categories of race, gender, ethnicity, social position, sexual orientation and disability.
Vermont Department of Health9

Populations in Focus
• Race, Ethnicity and Culture
• LGBTQ Identity
• People Living with Disabilities
• Social Class and Socioeconomic Status
• Rurality
Vermont Department of Health11


Preserving our Children’s Brains
• Lead in school drinking water
• A trio of laws to combat vaping
• A focus across state government on building resilience and preventing toxic stress
• Creation of Substance Misuse Prevention Council
13Vermont Department of Health

Racial Disparities in the Covid-19 Era
• The data
• The possible explanations
14Vermont Department of Health

15
White Vermonters represent the majority of COVID-19 cases. African American Vermonters have the highest rate.Rate per 10,000 Vermonters
Non-Hispanic Vermonters represent the majority of COVID-19 cases. Hispanic Vermonters have the higher rate.Rate per 10,000 Vermonters
Note: Race is unknown in 3% of cases and ethnicity is unknown in 10% of cases. Ca
se
De
mo
gra
ph
ics
American Indian or
Alaskan Native, 0.2%
Asian, 3.9%
Black or African
American, 7.8%
White, 84.1%
Other Race, 1.1%
11.5
7.6
15.8
36.3
114.2
American Indian or
Alaskan Native
Other Race
White
Asian
Black or African American
15.9
22.5
Non-Hispanic
Hispanic
Vermont Department of Health
Hispanic,
2.5%
Non- Hispanic,
88.0%

Approximately 62% of people* with COVID-19 have a pre-existing condition.
16Vermont Department of Health
Condition Count Percentage
Heart Disease 122 15%
Chronic Lung Disease (includes asthma and COPD) 118 14%
Chronic Liver Disease 8 1%
Chronic Kidney Disease 26 3%
Current/Former Smoker 222 26%
Diabetes 87 10%
Immunocompromised Condition 43 5%
Neurologic Condition/Intellectual Disability 33 4%
Other Chronic Condition** 263 31%
Pregnant 8 1%
50% of people with a pre-
existing condition have
two or more conditions.
**Not mutually exclusive, includes things like arthritis, thyroid conditions, multiple free text entries.
The Health Department has information about pre-existing conditions in 76% (844) of 1,109 total COVID-19 cases.
*of the 844 people that the Health Department has pre-existing condition data for.
Ca
se
De
mo
gra
ph
ics

16%Of those hospitalized who
were on a ventilator
17Vermont Department of Health
Vermonters 80 years and older are more likely to be hospitalized for COVID-19.Rate per 10,000 Vermonters
Most Vermonters with COVID-19 are not hospitalized.
Clin
ica
l C
ou
rse
Not
hospitalized =
890
Hospitalized
= 126
Unknown =
93
0.0 0.0 0.0 0.41.1
2.32.9
6.1
13.0
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 ≥80
36%Of those hospitalized who
were in the ICU
8 days Average hospital stay
(range: 0-39 days)
Other Race 2%
Asian 2%
White
94%
Black or African American 2%
1.3
2.5
1.9
2.6
Other Race
Asian
White
Black or African
American
Please note 5 hospitalized persons are missing race information.
*The number of Asian, black, and persons in the other race category is less than 5.
White Vermonters represent a majority of hospitalized COVID-19 cases. African
American and Asian Vermonters have the highest rate of COVID-19 hospitalizations.Rate per 10,000 Vermonters

18Vermont Department of Health
Most COVID-19 deaths occurred in an inpatient hospital setting
or a long-term care facility.
Males and females have similar rates of COVID-19 death.Rate per 10,000 Vermonters
Vermonters 80 years and older have higher rates of COVID-19
death than other age groups.Rate per 10,000 Vermonters
Note: No deaths have identified as Hispanic or Latino.
White Vermonters represent a majority of COVID-19 deaths.
However the rate is higher among racial minorities.Rate per 10,000 Vermonters
Clin
ica
l C
ou
rse
0.0 0.0 0.0 0.1 0.1 0.20.9
3.6
8.7
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 ≥80
1.0 0.8
At Home 2%
Inpatient
42%Long Term
Care Facility
51%
Out of state facility 5%
Asian
4%
Other
Race
2%
White
95%
0.9
0.6
1.7
White
Other Race
Asian

Data Informing RESTART VT
Patsy Kelso, PhD
State Epidemiologist for Infectious Diseases/VDH
Clinical Assistant Professor of Medicine/UVM

CDC Mitigation Guidance by Phase
CDC Phase Measures Guidelines
Phase 0
Significant,
uncontrolled
transmission
• Downward trajectory of cases over
14-day period
• Downward trajectory of CLI over
14-day period
• Downward trajectory of ILI over 14-
day period
• Downward trajectory of % positive
tests over 14-day period
• Treating all patients without crisis
standards of care
• Robust testing program (e.g.,
median time from collection to
result < 5 days)
Stay at home, shelter in place
Phase 1
Significant,
controlled
transmission
Vulnerable shelter in place; telework and close common areas; schools are closed;
childcare facilities only for essential workers; no elective procedures; restrict visitors to
health care facilities; group size limited to 10
Phase 2
Significant,
controlled
transmission
Vulnerable shelter in place; telework and close common areas; schools can open with
social distancing; childcare facilities open with social distancing; elective procedures on a
case-by-case basis; restrict visitors to health care facilities; group size limited to 50
Phase 3
Low,
controlled
transmission
Vulnerable practice physical distancing; telework flexibility; schools can open with social
distancing; childcare facilities open with social distancing; schedule elective procedures;
consider relaxing health care facility visitor restrictions; social gatherings with distancing
20Vermont Department of Health

CDC Gating Indicator: COVID-like Illness (CLI) Surveillance
21Source: Electronic Surveillance for the Early Notification of Community-based Epidemics (ESSENCE), 2020.
Regression method: Binomial regression
0
1
2
3
4
5
6
7
8
9
3/1 3/8 3/15 3/22 3/29 4/5 4/12 4/19 4/26 5/3 5/10 5/17 5/24 5/31
Percent of ED and Urgent Care Visits for COVID-like Illness (CLI) Syndromic Surveillance for 13 of 14 Vermont Hospitals and 2 Urgent Care Centers
March 22nd last
rebound or
statistically
significant increase
in visits for CLI
<10 CLI visits in a day
Statistically significant
decrease in visits for
CLI

CDC Gating Indicator: Test Volume and Percent Positive
22Vermont Department of Health
0
200
400
600
800
1000
0%
2%
4%
6%
8%
10%
COVID-19 Percent Positive Test Rate (14-Day) by Specimen Collection Date
14-Day Percent Positive Average Tested Per Day
Peak 4/5 (9.4%)
Lowest 4/28
5/29 - 6/5 significant
increase in % positive
(0.31% to 0.78%)

CDC Gating Indicator: Incidence
23

Pediatric COVID-19 and Multisystem Inflammatory Syndrome in Children (MIS-C)
Jennifer S. Read, MD, MS, MPH, DTM&H, FAAP
Medical Epidemiologist/VDHClinical Professor of Pediatrics/UVM

•84,016 total confirmed
child COVID-19 cases
reported
•Children represented
5.2%
(84,016/1,623,334) of
all available confirmed
cases

COVID-19 Cases in the U.S.: Cumulative Rate per 100,000 Population According to Age (CDC, 6/12/20)
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
Age (years) Rate
Overall 89.3
0-4 5.6
5-17 3.1
18-29 27.3
30-39 52.5
40-49 84.6
50-64 136.1
65-74 198.7
75-84 329.3
85+ 513.2

SARS-CoV-2 PCR+ in Vermont (as of 6/14/2020)• Overall: 1037 cases
• Adults (≥ 18 years): 977 (94%) (191.45/100,000)• Hospitalizations: 112 (11.5%)• Deaths: 54 (5.5%)
• Children (< 18 years): 60 (6%) (51.74/100,000)• Hospitalizations: 0• Deaths: 0
• Children:• Sex: 55% female, 45% male • Race: black 52%; white 37%; Asian 12% • Ethnicity: 98% non-Hispanic • Age: No infants;
• n=20 (1/3) aged 1-9 years• n=40 (2/3) aged 10-17 years

Symptoms of COVID-19 in Vermont Children
• 68%: fatigue
• 53%:• ageusia, dysgeusia, and/or anosmia; headache
• 47%:• cough; nasal congestion or rhinorrhea
• 37%: loss of appetite
• 32%:• fever; chills; myalgia
• 26%:• sore throat; diarrhea
• 21%: shortness of breath
• 10%: abdominal pain
• 5%: nausea; “purple toes” (may represent acute acro-ischemia (manifestation of micro-thrombosis))
Symptomatic42%
Asymptomatic 47%
Unknown, 11%

Newly RECOGNIZED Syndrome
• U.S.: Multisystem Inflammatory Syndrome in Children (MIS-C)• California
• Delaware
• District of Columbia
• Illinois
• Kentucky
• Louisiana
• Massachusetts
• Europe and the U.K.: Paediatric Multisystem Inflammatory Syndrome temporally associated with SARS-CoV-2 infection (PMIS-TS or PIMS)
• Michigan
• Minnesota
• Mississippi
• Missouri
• New Jersey
• New York
• Ohio
• Oregon
• Pennsylvania
• Tennessee
• Utah
• Washington
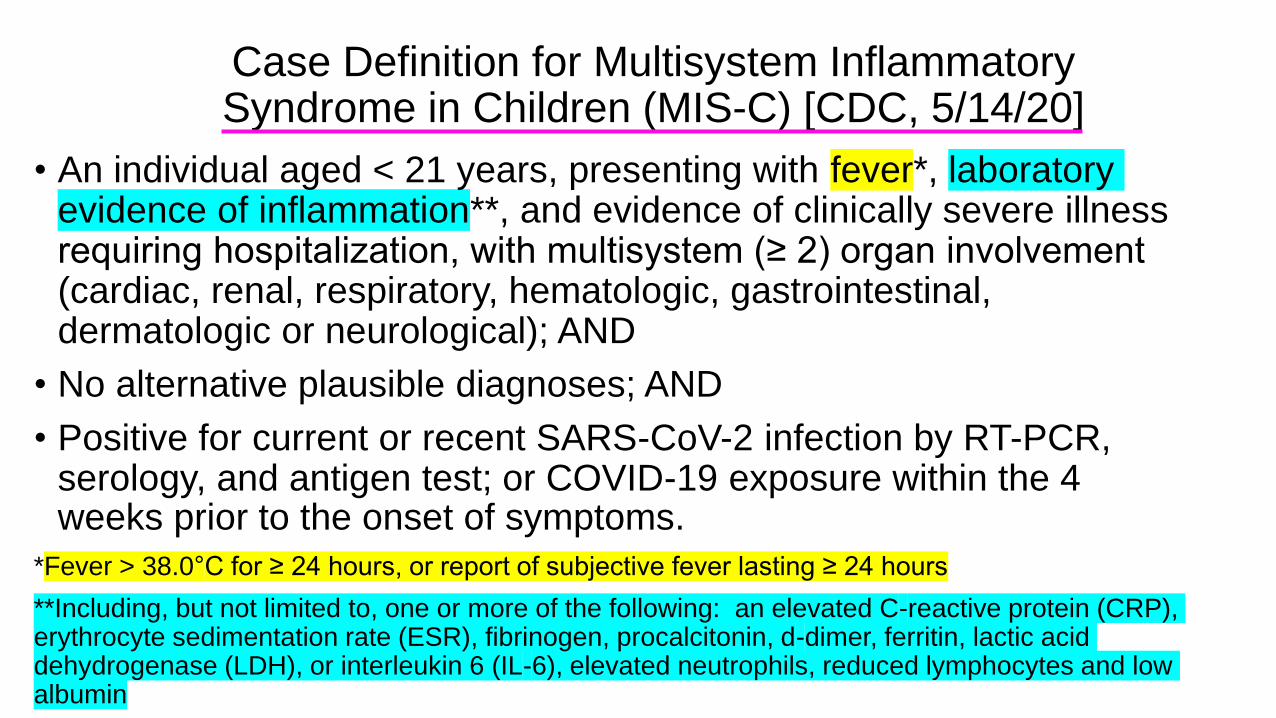
Case Definition for Multisystem Inflammatory Syndrome in Children (MIS-C) [CDC, 5/14/20]
• An individual aged < 21 years, presenting with fever*, laboratory evidence of inflammation**, and evidence of clinically severe illness requiring hospitalization, with multisystem (≥ 2) organ involvement (cardiac, renal, respiratory, hematologic, gastrointestinal, dermatologic or neurological); AND
• No alternative plausible diagnoses; AND
• Positive for current or recent SARS-CoV-2 infection by RT-PCR, serology, and antigen test; or COVID-19 exposure within the 4 weeks prior to the onset of symptoms.
*Fever > 38.0°C for ≥ 24 hours, or report of subjective fever lasting ≥ 24 hours
**Including, but not limited to, one or more of the following: an elevated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), fibrinogen, procalcitonin, d-dimer, ferritin, lactic acid dehydrogenase (LDH), or interleukin 6 (IL-6), elevated neutrophils, reduced lymphocytes and low albumin
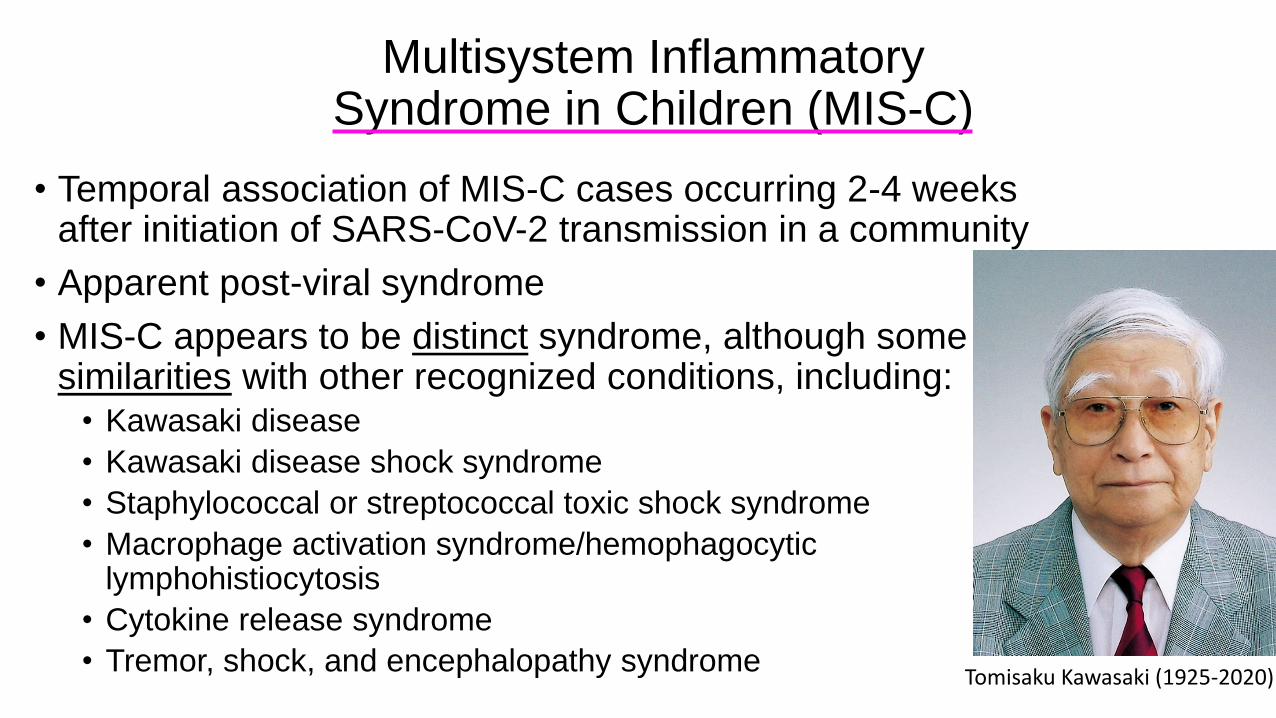
Multisystem Inflammatory Syndrome in Children (MIS-C)
• Temporal association of MIS-C cases occurring 2-4 weeks after initiation of SARS-CoV-2 transmission in a community
• Apparent post-viral syndrome
• MIS-C appears to be distinct syndrome, although some similarities with other recognized conditions, including:
• Kawasaki disease
• Kawasaki disease shock syndrome
• Staphylococcal or streptococcal toxic shock syndrome
• Macrophage activation syndrome/hemophagocytic lymphohistiocytosis
• Cytokine release syndrome
• Tremor, shock, and encephalopathy syndromeTomisaku Kawasaki (1925-2020)


Multisystem Inflammatory Syndrome in Children (MIS-C)
• Symptoms at presentation (among hospitalized children):• Fever
• Gastrointestinal symptoms (abdominal pain, diarrhea)
• Most (65%+) progress to shock
• All develop 1+ organ dysfunction:• Most frequently - myocardial impairment, myocarditis-like injury
• Renal/acute kidney injury
• Gastrointestinal/hepatitis
• Hematologic
• Central nervous system/neurologic
• Few patients with respiratory symptoms (mechanical ventilation, when used, more often to support cardiac function)
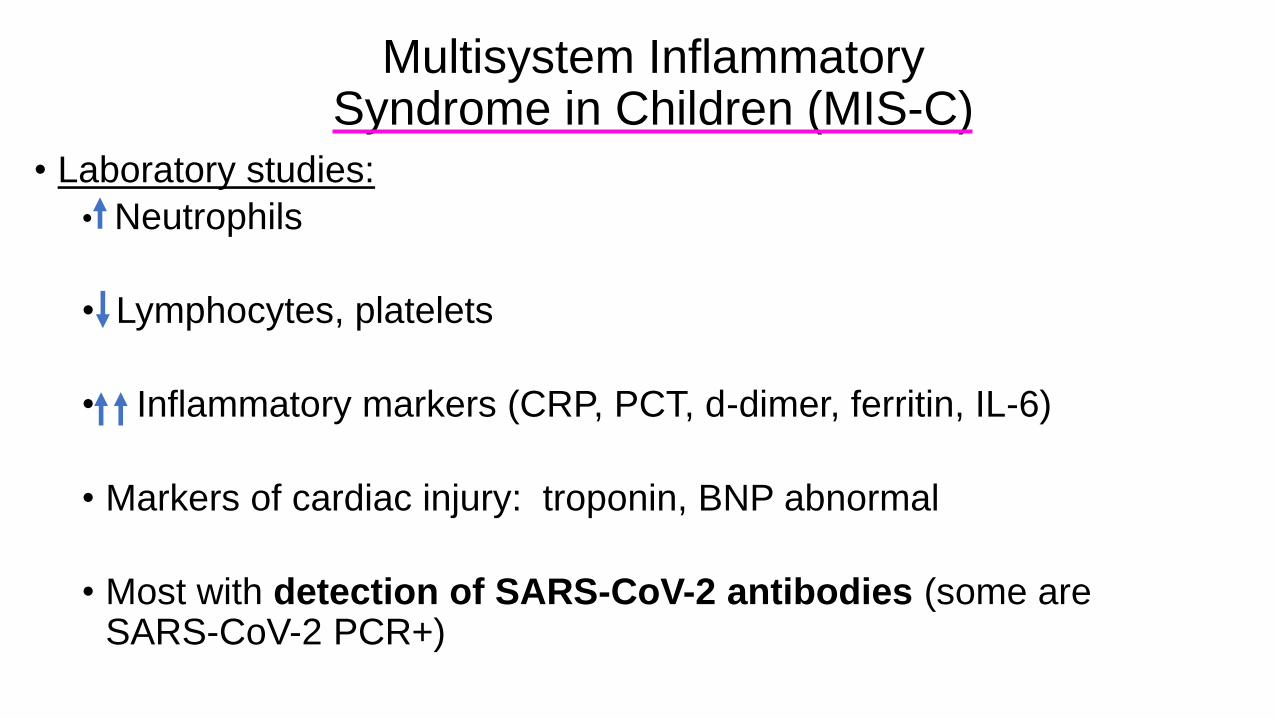
Multisystem Inflammatory Syndrome in Children (MIS-C)
• Laboratory studies:
• Neutrophils
• Lymphocytes, platelets
• Inflammatory markers (CRP, PCT, d-dimer, ferritin, IL-6)
• Markers of cardiac injury: troponin, BNP abnormal
• Most with detection of SARS-CoV-2 antibodies (some are SARS-CoV-2 PCR+)

Multisystem Inflammatory Syndrome in Children (MIS-C)
• Echocardiography:
• Impaired left ventricular function of variable severity
• Coronary artery dilations, rarely coronary artery aneurysms
• Anticipate need for serial echocardiography/follow-up with cardiology

Multisystem Inflammatory Syndrome in Children (MIS-C)
• Optimal management (beyond ICU care) = unknown• Best practices evolving;
• Some centers have used:• IVIG
• Immunomodulators (corticosteroids, IL-6 blockers such as tocilizumab)
• Important to collaborate to develop best management plans• Intensive care
• Rheumatology
• Cardiology
• Hematology
• Other sub-specialties
• NEEDED: further systematic studies; collaborative, multidisciplinary research

REQUESTED ACTIONS:
1. Report any patient who meets this case definition to the Vermont
Department of Health in order to increase understanding of risks factors,
pathogenesis, clinical course, and management of MIS-C. Some patients may
fulfill all or some criteria for Kawasaki disease, but they should still be reported if
they meet the case definition for MIS-C. Call (802) 863-7240, ext. 3 to report.
2. Consider MIS-C in any pediatric death with evidence of SARS-CoV-2 infection.

Pediatric COVID-19: Reopening Childcare, Summer Programs, and Schools
Breena Holmes, MD, FAAP
Director, Maternal and Child Health/VDHClinical Associate Professor of Pediatrics, UVM

Health Guidance for Childcare, Summer Programs and Schools
• Health Guidance for Childcare and Summer Programs• Emergency childcare and school age programs for essential workers-early April 2020
• Childcare re-opening and summer programs(including day camps) health guidance- June 1, 2020
• Revised childcare and summer program guidance – 3rd set of revision this week
• Health Guidance for Re-opening Schools- this week (June 16)
• Agency for Commerce and Community Development• Overnight camp opening guidance
• Colleges and Universities re-opening-other leaders
40Vermont Department of Health

Health Guidance
41Vermont Department of Health
> Health Guidance for Childcare and Summer Programs
(Effective June 1)
> Safe & Healthy School Guidance
(Coming Soon)

Childcare/Summer Program Resource
42Vermont Department of Health
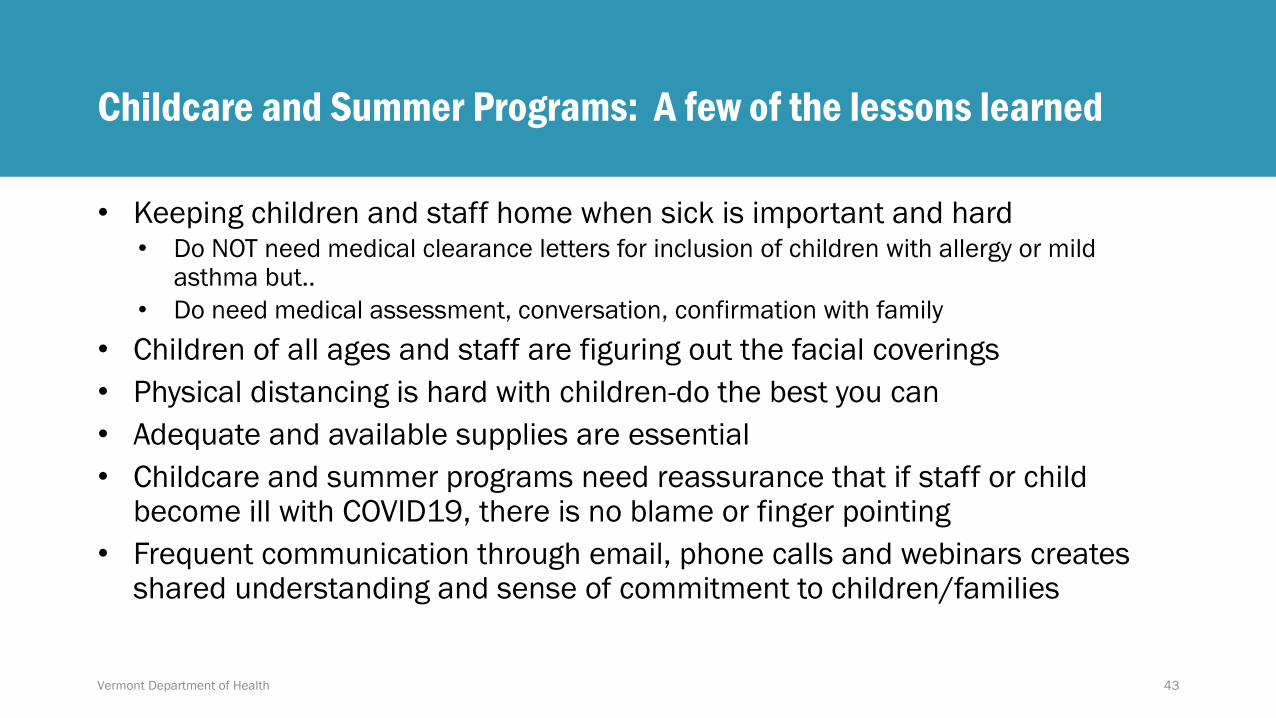
Childcare and Summer Programs: A few of the lessons learned
• Keeping children and staff home when sick is important and hard• Do NOT need medical clearance letters for inclusion of children with allergy or mild
asthma but..
• Do need medical assessment, conversation, confirmation with family
• Children of all ages and staff are figuring out the facial coverings
• Physical distancing is hard with children-do the best you can
• Adequate and available supplies are essential
• Childcare and summer programs need reassurance that if staff or child become ill with COVID19, there is no blame or finger pointing
• Frequent communication through email, phone calls and webinars creates shared understanding and sense of commitment to children/families
43Vermont Department of Health

Health Guidance: Cloth Facial Coverings for Children
Cloth facial coverings and children:
No cloth facial coverings for children under 2-years-old
No cloth facial coverings while sleeping, eating or swimming
Help children to understand the importance of wearing cloth facial coverings to prevent the spread of germs
Cloth facial coverings are developmentally appropriate for children when they can properly put on, take off, and not touch or suck on the coverage
Cloth facial coverings can be removed during outdoor activities where children and staff can maintain physical distancing and have ready access to put them back as needed when activity stops
Children who have a medical reason for not wearing a cloth facial covering must not be required to wear one
44Vermont Department of Health

45Vermont Department of Health

46Vermont Department of Health

School Health Guidance- a FEW of the Debated Areas
• Health Screenings including temperature checks
• home or entering bus or entering school building
• Children with Special Health and/or Educational Needs
• Staff over 65 or with chronic conditions
• Staying home when sick
• Facial Coverings
• Group size, Integrity of the group, distancing, cohorting
47

School Health Guidance: Facial Coverings
• Current approach after much discussion
• All staff are required to wear facial coverings
• Facial coverings are required for middle and high school students
• Facial coverings for elementary age students are required when developmentally appropriate based on child’s ability to wear without sucking, touching or pulling
48

School Health Guidance: Pediatricians Needed
• COVID Task Force with school nurse leader- need pediatrician involvement
• Children with special health and education needs: Team-based care with medical home
• Social emotional health in general also in age of COVID, supporting students and staff
• Food service guidance- advocacy for universal meals since many kids will be eating in classrooms. Let’s decrease stigma and feed everyone
• Ventilation-environment health leaders, including pediatricians needed
• Communication (staff, students, families, community): 8 times, 8 ways-please help
June 18, 2020 49

Health Questions Resource for Childcare Services
The Department of Health has public health nurses available to childcare, afterschool, and summer programs to answer health related childcare questions
8:00 AM to 3:00 PM Monday through Friday
Call: 802-863-7240, select the option for “Childcare Services”
After hours there will be a childcare question mailbox to leave a message and VDH staff will return your call the following business days.
50Vermont Department of Health

Help Me Grow Creates a Reliable Grid of Resources
• Help Me Grow offers a resource hub that helps connect children and their families to local resources and services
• Providers wanting to refer a family directly to resources themselves can call HMG staff to get the latest information on food resources, mental health services and support groups, and more
Dial 2-1-1 ext. 6, text HMGVT to 898211, or refer
at helpmegrowvt.org/form/referral-form
51Vermont Department of Health

Vermont Department of Health 52

















