21
Maryland's New Demonstration Waiver Michael B. Robbins, Senior Vice President April 28, 2015
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | alexander-short |
| View: | 216 times |
| Download: | 0 times |

Maryland's New Demonstration Waiver
Michael B. Robbins, Senior Vice President
April 28, 2015

• History – What is the Maryland “waiver?”
• New waiver’s key metrics
• How the Affordable Care Act interacts with the waiver
• How does this impact your community?
2
AGENDA
• Health Services Cost Review Commission (HSCRC) created in 1971 with jurisdiction over hospital costs (IP & OP facility only) with rate setting authority for commercial payers
• Began negotiations with Medicare (HCFA) in 1972 for an all-payer waiver (in effect when all hospital rates set: 1977)
• The “Medicare waiver” (initially a demonstration waiver) made the system “all-payer” allowing for Medicare and Medicaid to be paid using rates set by the HSCRC
• System was based on historical costs – (with a focus on outliers)
• Established a prospective rate setting system - annual rate updates
• System of Financing “reasonable” Uncompensated Care”
3
History

• Maryland – only state where hospitals don’t decide how much to charge for care
• Allows Maryland to “waive” Medicare payment rules, set rates hospitals charge
• As long as we meet waiver “test” Growth in Medicare spending per inpatient hospital
stay less than nation
4
History

• Emphasis on Quality and Payment Changes nationally spurred a round of similar change in Maryland 2003-2011
• Quality Related Programs:
• Quality-Based Reimbursement (P4P system of rewards and penalties for performing evidence-based process measures), similar to national VBP program
• Maryland Hospital Acquired Conditions Policy (P4P system of significant rewards/penalties for risk adjusted rates of complications across 65 categories)
• Cost/Utilization Programs:
• Admission-Readmission Revenue (ARR) policy which bundled admissions and all-cause readmissions (31 of 46 hospitals adopted)
• One-day Stay Policy
• Re-instituted Volume Adjustment at 85% VC and 15% FC
• Negotiated 10 Total Patient Revenue (TPR) agreements
5
History

6
History
The 40-year-old waiver “test” quickly becomes out of date, a new five-year demonstration waiver is approved
Through 12/31/14
As of 1/1/14
Inpatient care All hospital care
Medicare only All payers
Cost of care per hospital stay
Cost and quality of care
7
New Waiver Objectives
Opportunity for Maryland to continue to be a NATIONAL LEADERin health care
CHANGEthe way we pay for and provide health care
BUILDon the great system we have and make it even better: • More affordable • Safer • A healthier Maryland
• Work together to slow growth in spending for hospital care
• Continue Maryland’s unique way of setting hospital prices
• Change how hospitals are paid, to reward the right things
8
Starts with Hospital Care

9
New Waiver Financial Tests
Annual hospital SPENDING CAP − 3.58% all payer per capita growth
Medicare dynamic hospital SAVINGS TARGET − $330 million over 5 years
GROWTH in total Maryland Medicare spending per capita cannot exceed national rate of growth

10
New Waiver Quality Targets
READMISSIONS: patients who return to the hospital within 30 days of hospital discharge
Maryland ranks poorly(almost last)– 49 of 51 states and D.C.
Bring Maryland readmission rates to NATIONALAVERAGE in 5 years
Better, SAFER care

11
New Waiver Quality Targets
HOSPITAL ACQUIRED CONDITIONS: patients who get infections while in the hospital
Maryland rates of infection HIGHER than nation
REDUCE infections and other “hospital-acquired conditions” by 30% in5 years
Better, SAFER care

Change how hospitals are paid to reward the right things•Volume – no; Value - YES
•Success under new spending caps requires volume control and cost reduction
•The key: population health management
•Care for patients in the community lower cost settings; reduce unnecessary care
12
A Healthier Maryland

• Never been tried or tested before on a scale of this magnitude
• Hospitals in serious financial condition – 40% losing money at the time waiver was approved
• New hospital spending limits tight
• Will require hospitals to redefine themselves
• Will require hospitals to develop new partnerships
• Will require communities to work together to keep people healthy
• Will require patients and families to truly engage in their care
13
Challenges

• Continue our unique hospital rate-setting system
• More equitable care for low income and uninsured people
• Should lead to slower growth in insurance premiums
• Lead nation in reforming health care
• Statewide focus on quality and safety
14
Opportunities

• Rate-Setting Commission implements numerous policy changes through multi-stakeholder work group process (Including new work groups on Consumer Engagement and Care Coordination)
• Hospitals negotiate and adopt global budgets, and begin to invest in IT, care coordinators, and more to help manage community health
• Hospitals look to develop new partnerships15
Initial Steps
16
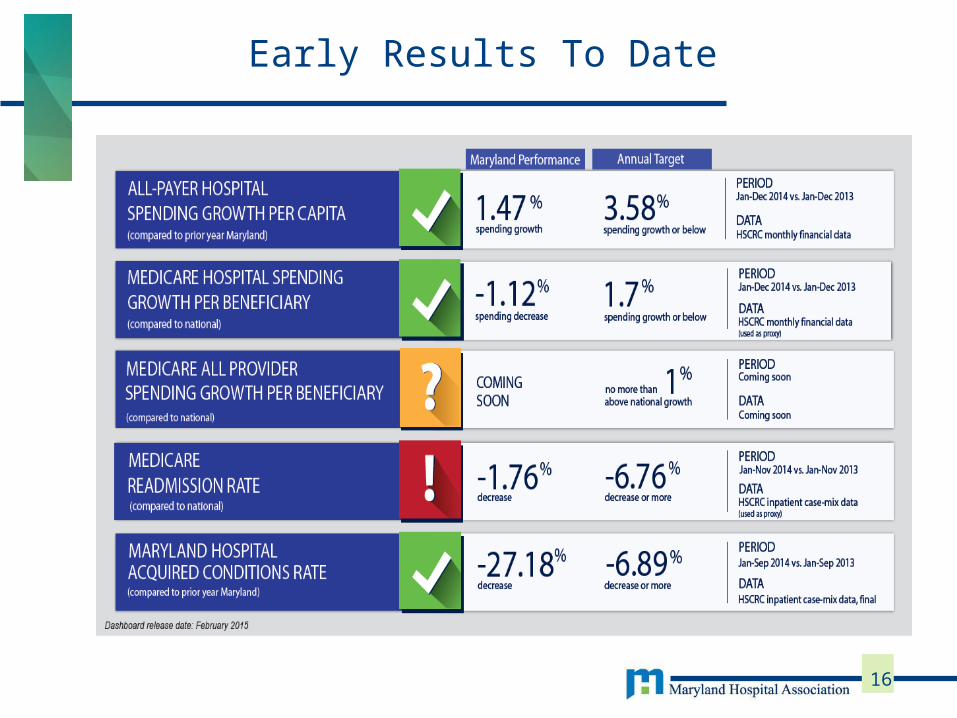
Early Results To Date

• Expansion of coverage: enrollment in Medicaid has grown by 300,000 since January 1, 2014
• Estimated 100,000 enrollees in private exchange plans
• The result: significant reduction in hospital uncompensated care
• HSCRC reduced amounts in hospital rates by 1% in 2015; with another reduction of about 1% expected for next year
17
Affordable Care Act Impact

• What is hospital source of funding for innovation in a world where total revenue growth is constrained?
• How do we insure that the promise of targeted disease management is realized?
• Opportunities to partner: Population health management and funding opportunities outside of the rate regulatory process
18
Impact on Manufacturers

• Railroads went out of business because they thought they were in the railroad business instead of recognizing they were in the transportation business
• Hospitals realize they are in the health care business, not the hospital business
19
“Railroad Moment”
Source: 2012 Kaufman, Hall & Associates, Inc; Jason Sussman

QUESTIONS?
20

Maryland's New Demonstration Waiver
Michael B. Robbins, Senior Vice President
April 28, 2015

















