35
Massive Transfusion and Massive Transfusion Protocols Robert T. Russell, MD, MPH November 2019 Pediatric Trauma Society
Massive Transfusion and
Massive Transfusion Protocols
Robert T. Russell, MD, MPH
November 2019
Pediatric Trauma Society
Massive Transfusion and
Massive Transfusion Protocols
No Disclosures
Objectives
• Review data associated with massive transfusion in adults and children
• Defining Massive Transfusion
• Predictors for activation
• Outcomes from utilization
• MTP creation
• Resources
• Monitoring response
• Use of simulation
Damage Control Resuscitation
Hemorrhage control
Permissive hypotension
Hemostatic resuscitation
The “Old” Approach
20 mL/kg isotonic crystalloid
Reassess
20 mL/kg isotonic crystalloid
Reassess
20 mL/kg isotonic crystalloidconsider 10-20 mL/kg packed red cells
Crystalloid Based“Resuscitation”
• Dilutional coagulopathy
• Excessive third spacing
• Abdominal compartment syndrome
• Pulmonary edema
• Cerebral edema
• Ileus
• Hypothermia
• Acidosis (hyperchloremia)
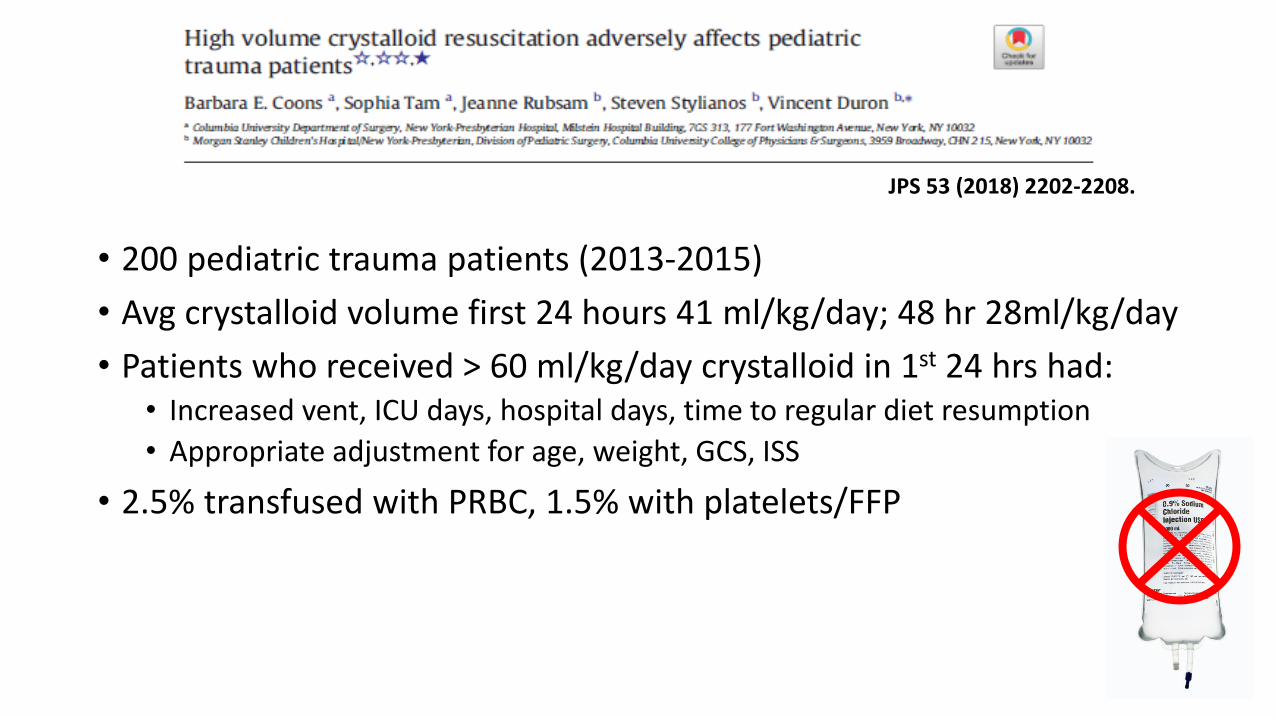
• 200 pediatric trauma patients (2013-2015)
• Avg crystalloid volume first 24 hours 41 ml/kg/day; 48 hr 28ml/kg/day
• Patients who received > 60 ml/kg/day crystalloid in 1st 24 hrs had: • Increased vent, ICU days, hospital days, time to regular diet resumption
• Appropriate adjustment for age, weight, GCS, ISS
• 2.5% transfused with PRBC, 1.5% with platelets/FFP
JPS 53 (2018) 2202-2208.
Massive Transfusion Protocols
• Provide large amounts of blood products to critically injured patients in an immediate and sustained manner
• Predefined ratios of platelets, plasma and RBCs
Defining Massive Transfusion?
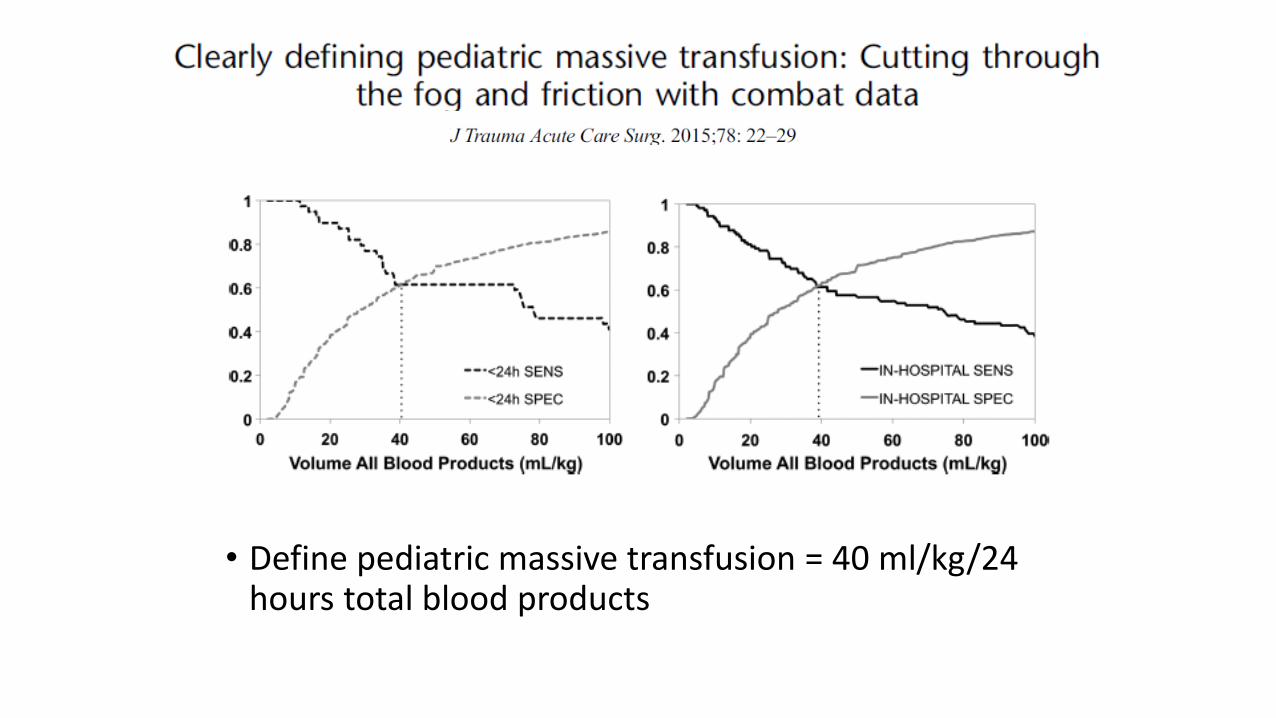
• Define pediatric massive transfusion = 40 ml/kg/24 hours total blood products
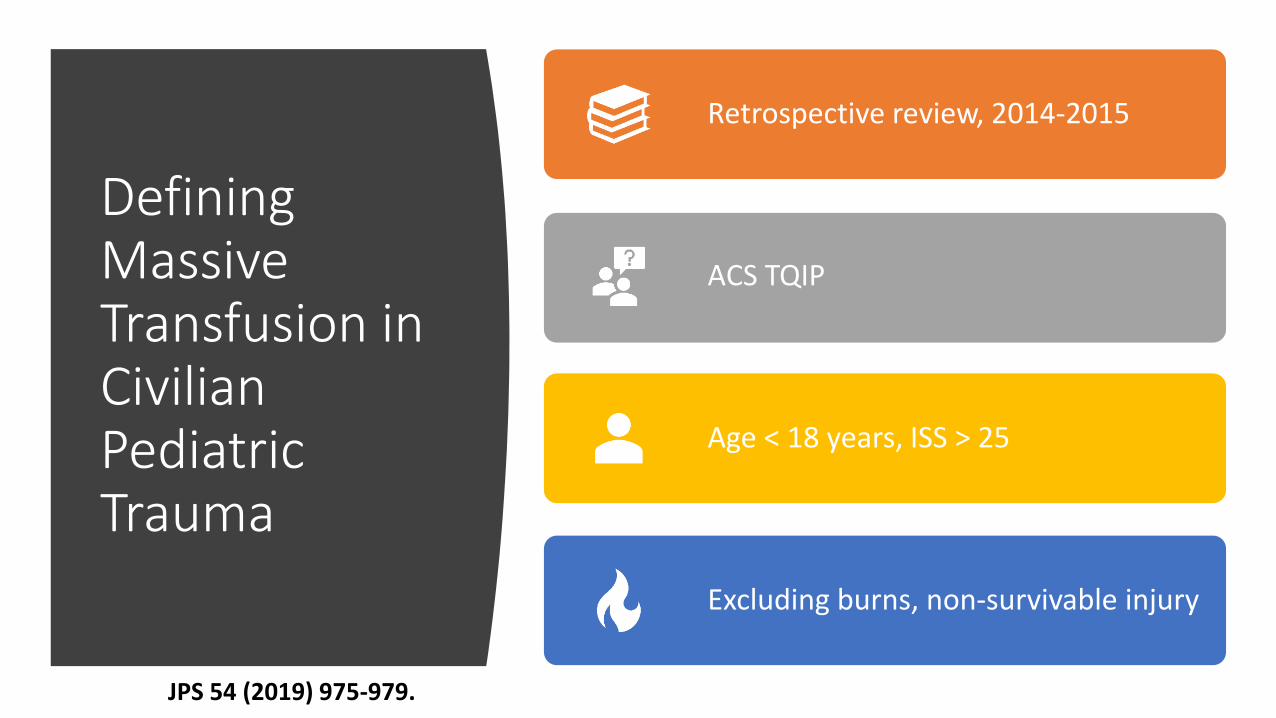
Defining Massive Transfusion in Civilian Pediatric Trauma
Retrospective review, 2014-2015
ACS TQIP
Age < 18 years, ISS > 25
Excluding burns, non-survivable injury
JPS 54 (2019) 975-979.
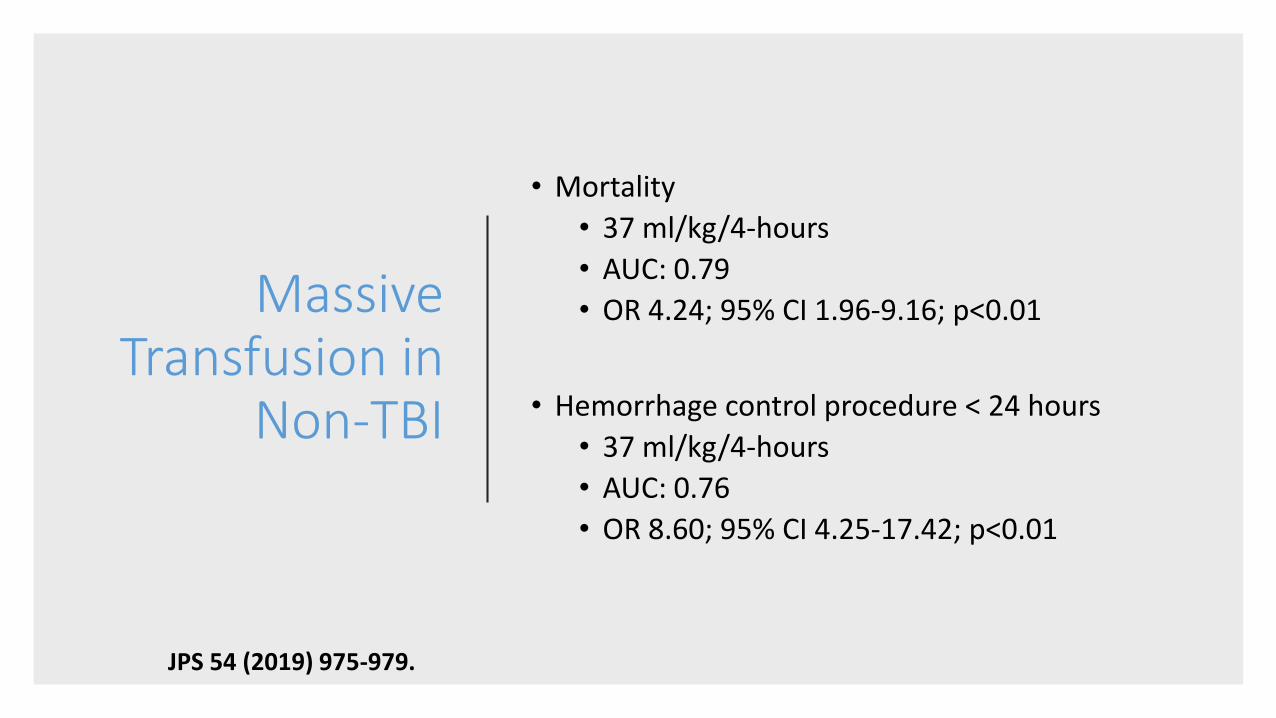
Massive Transfusion in
Non-TBI
• Mortality
• 37 ml/kg/4-hours
• AUC: 0.79
• OR 4.24; 95% CI 1.96-9.16; p<0.01
• Hemorrhage control procedure < 24 hours
• 37 ml/kg/4-hours
• AUC: 0.76
• OR 8.60; 95% CI 4.25-17.42; p<0.01
JPS 54 (2019) 975-979.
When should we activate an MTP?
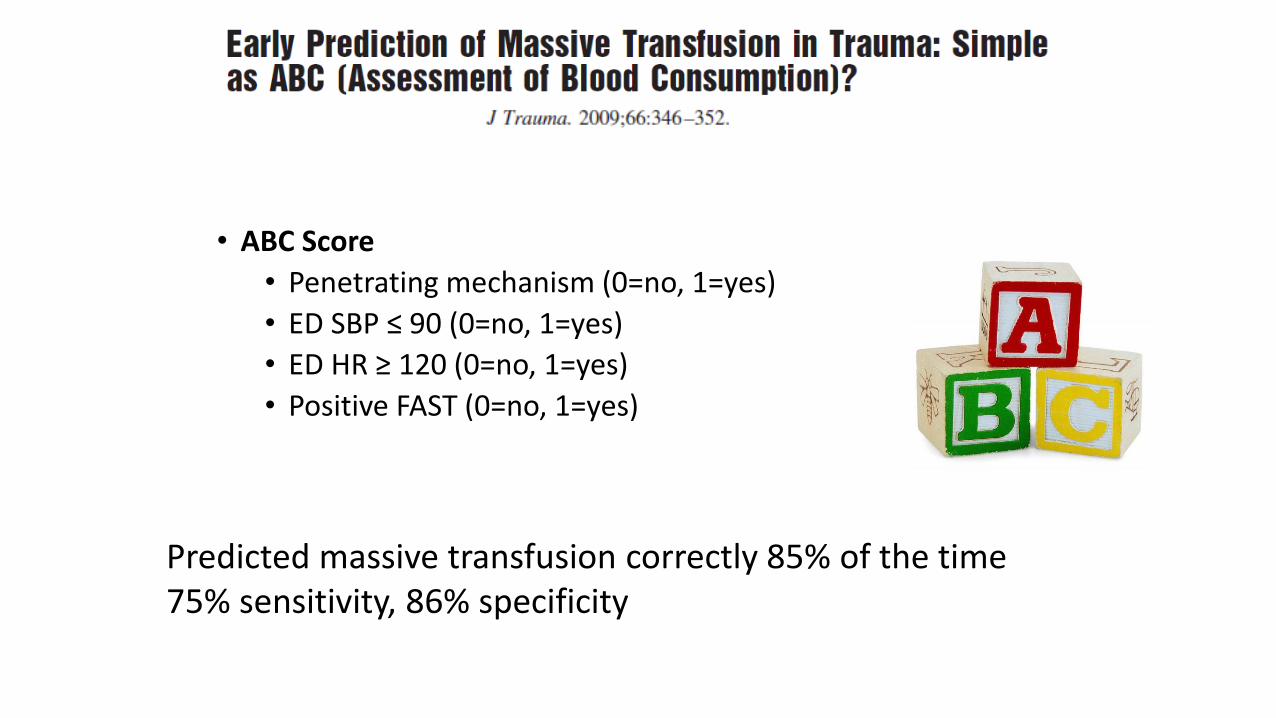
• ABC Score
• Penetrating mechanism (0=no, 1=yes)
• ED SBP ≤ 90 (0=no, 1=yes)
• ED HR ≥ 120 (0=no, 1=yes)
• Positive FAST (0=no, 1=yes)
Predicted massive transfusion correctly 85% of the time75% sensitivity, 86% specificity
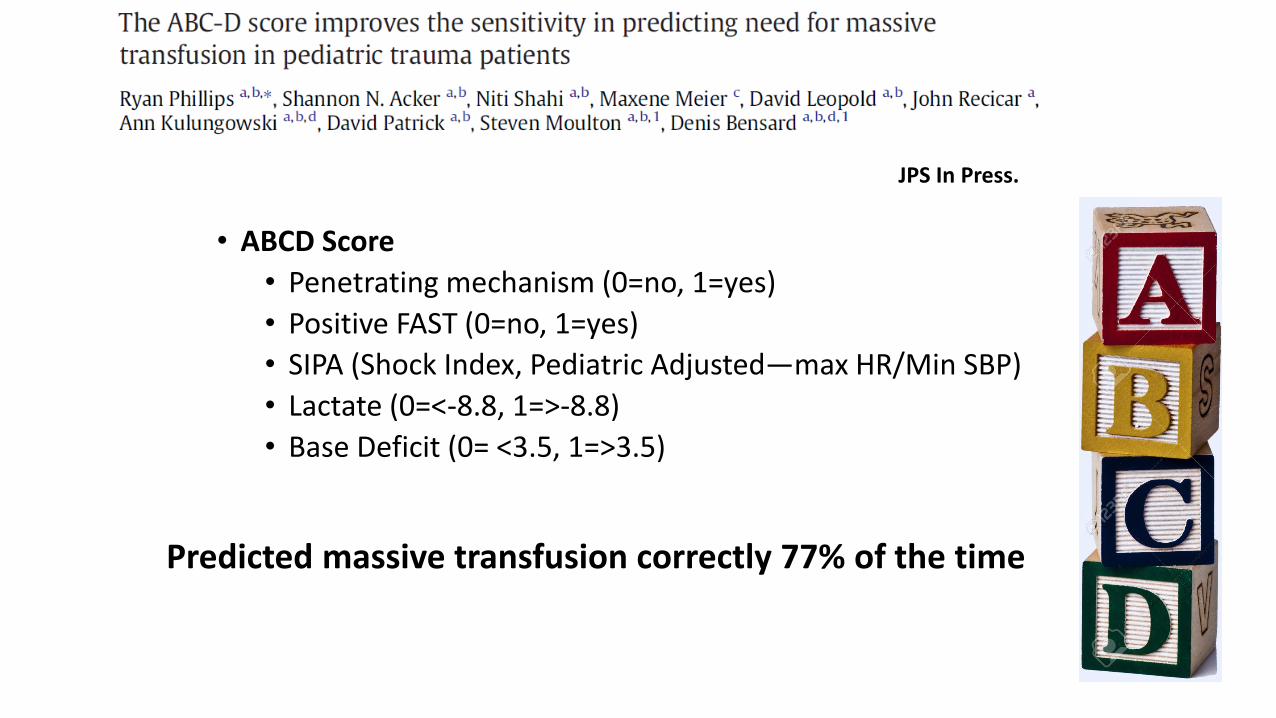
• ABCD Score
• Penetrating mechanism (0=no, 1=yes)
• Positive FAST (0=no, 1=yes)
• SIPA (Shock Index, Pediatric Adjusted—max HR/Min SBP)
• Lactate (0=<-8.8, 1=>-8.8)
• Base Deficit (0= <3.5, 1=>3.5)
JPS In Press.
Predicted massive transfusion correctly 77% of the time
MTP in Adults
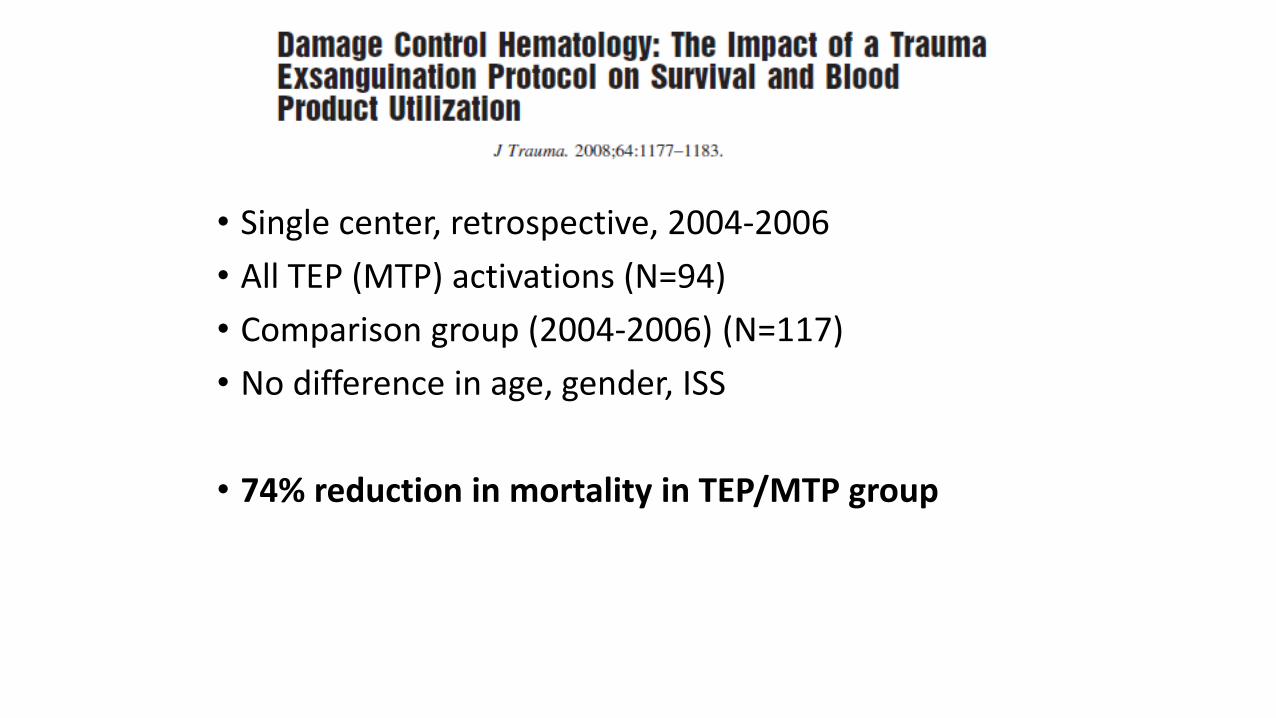
• Single center, retrospective, 2004-2006
• All TEP (MTP) activations (N=94)
• Comparison group (2004-2006) (N=117)
• No difference in age, gender, ISS
• 74% reduction in mortality in TEP/MTP group
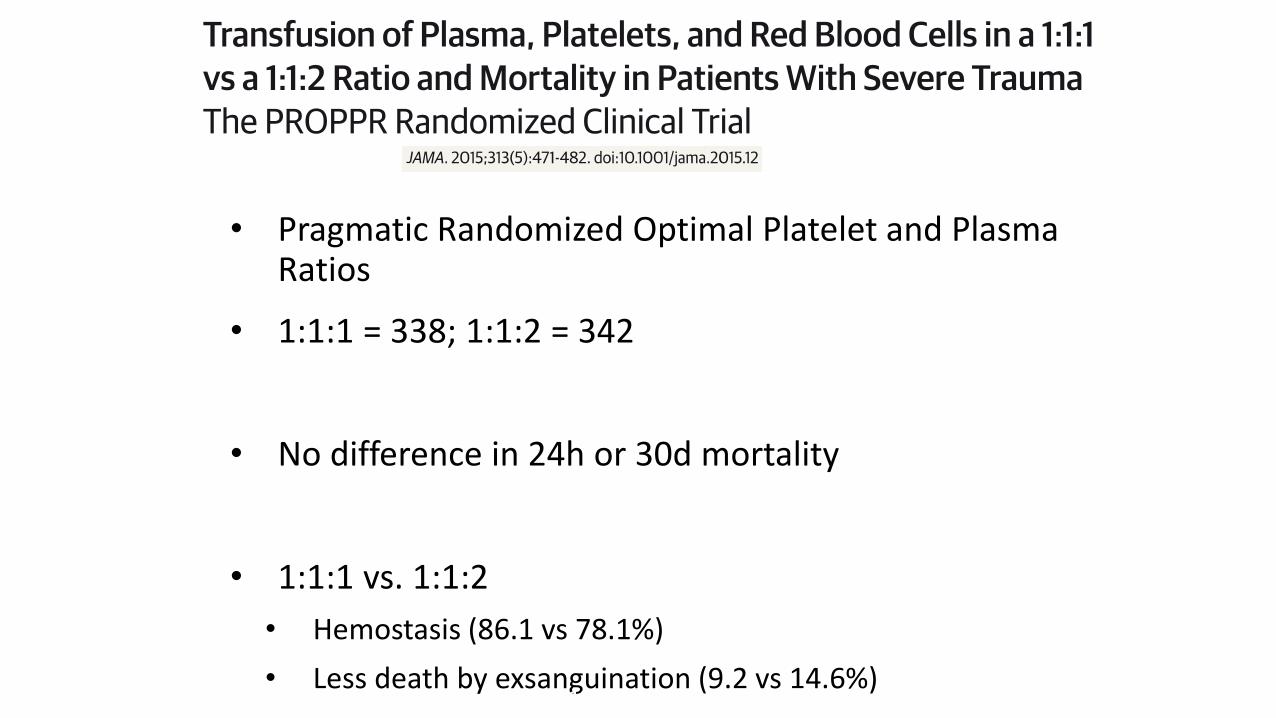
• Pragmatic Randomized Optimal Platelet and Plasma Ratios
• 1:1:1 = 338; 1:1:2 = 342
• No difference in 24h or 30d mortality
• 1:1:1 vs. 1:1:2
• Hemostasis (86.1 vs 78.1%)
• Less death by exsanguination (9.2 vs 14.6%)Month 2016
Massive Transfusion in Children
• Single center, retrospective, 2005-2014
• ED presentation, RBC administered < 24 hours
• Pre (125) vs post (115) MTP implementation
• MT: > 40 ml/kg RBC or >80 mg/kg total blood products in 24-hours
• MT were more severely injured and coagulopathic
• No difference in mortality
• ↓ Time to plasma and platelet administration
• ↑ Plasma and PLT:RBC ratios
Month 2016
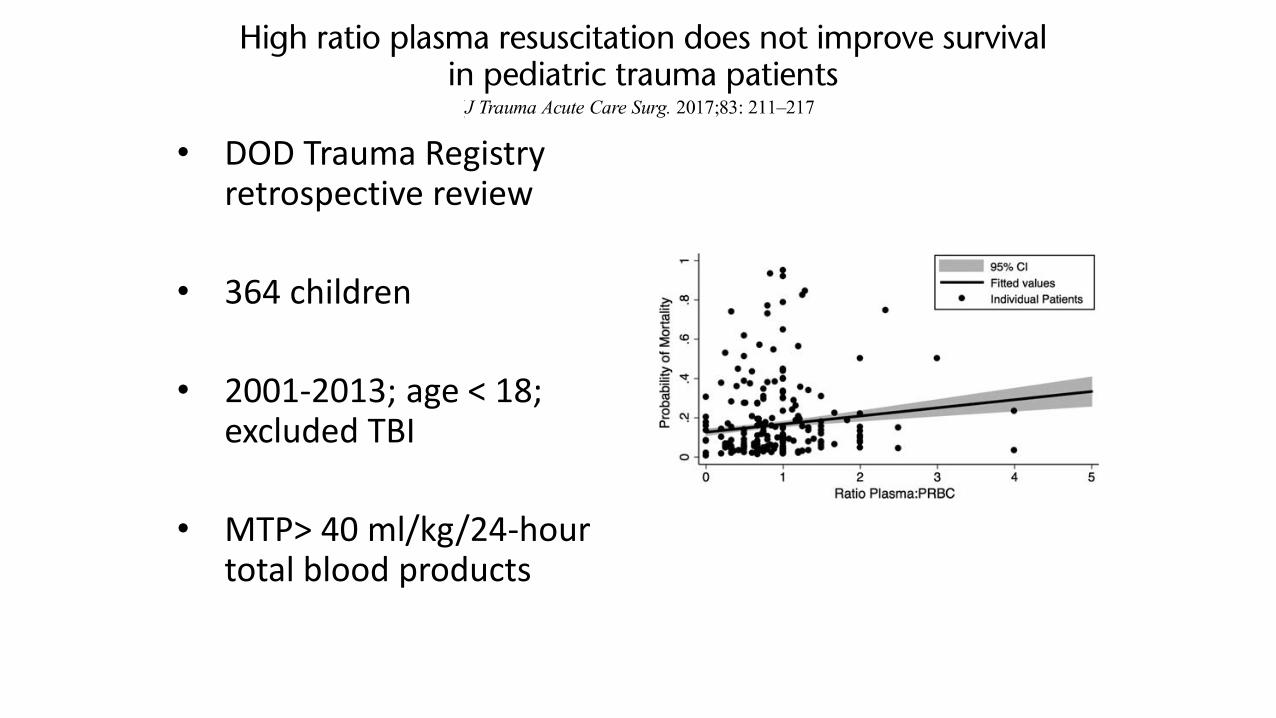
• DOD Trauma Registry retrospective review
• 364 children
• 2001-2013; age < 18; excluded TBI
• MTP> 40 ml/kg/24-hour total blood products
Month 2016
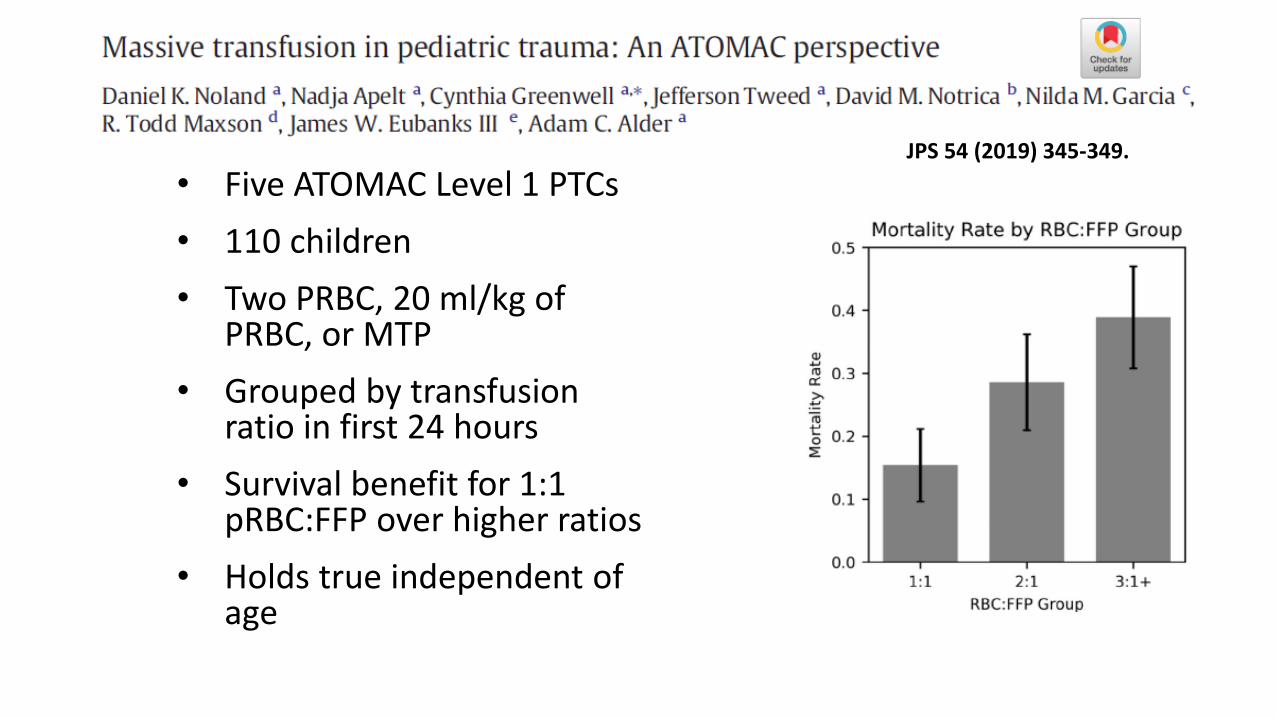
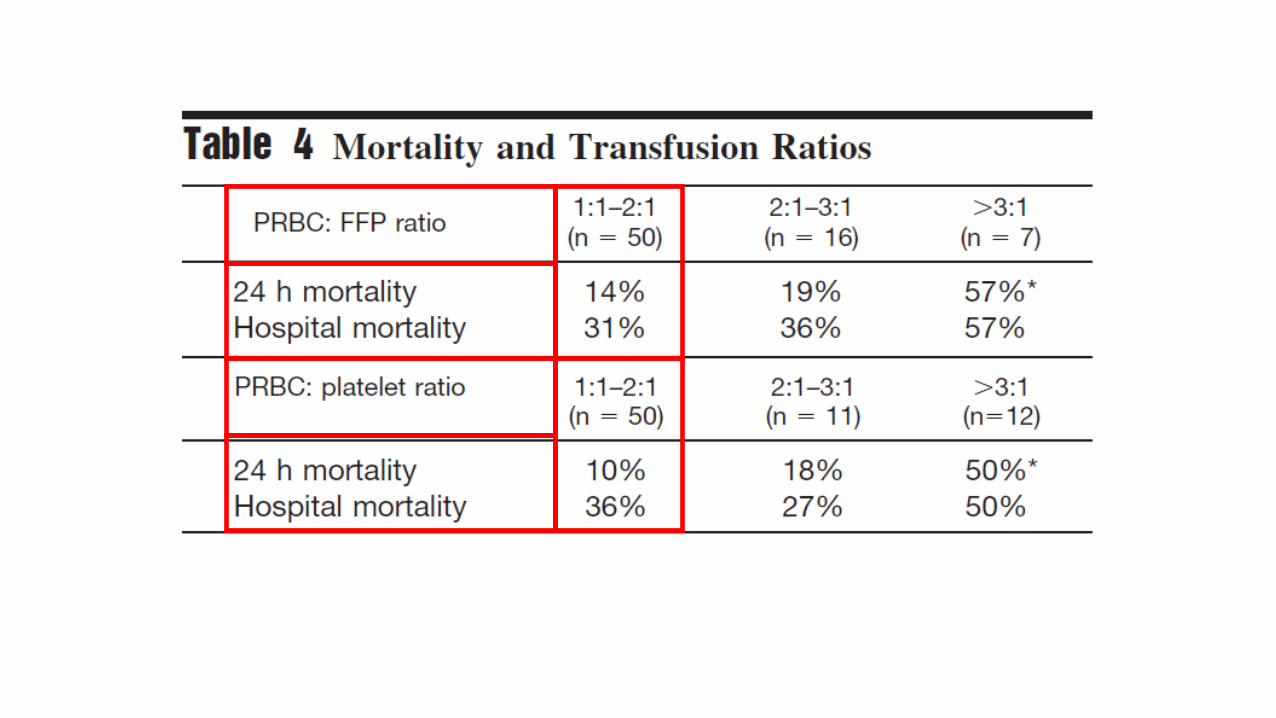
• Five ATOMAC Level 1 PTCs
• 110 children
• Two PRBC, 20 ml/kg of PRBC, or MTP
• Grouped by transfusion ratio in first 24 hours
• Survival benefit for 1:1 pRBC:FFP over higher ratios
• Holds true independent of age
Month 2016
JPS 54 (2019) 345-349.
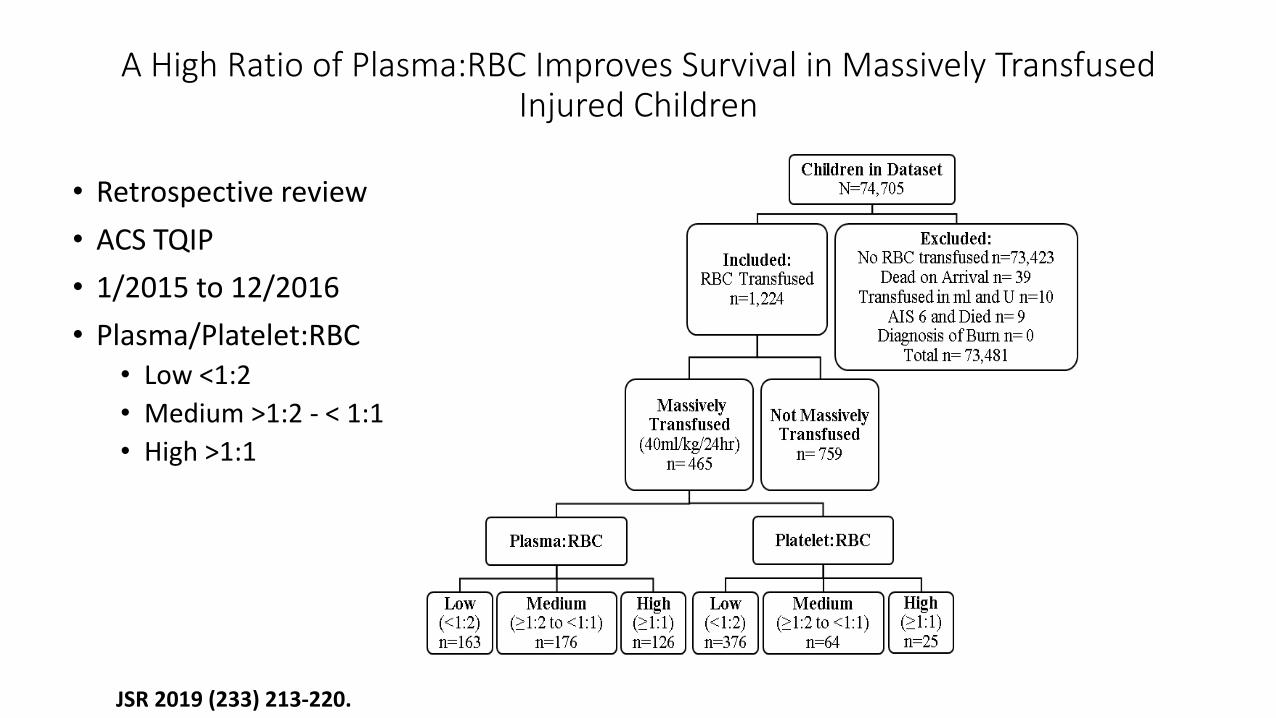
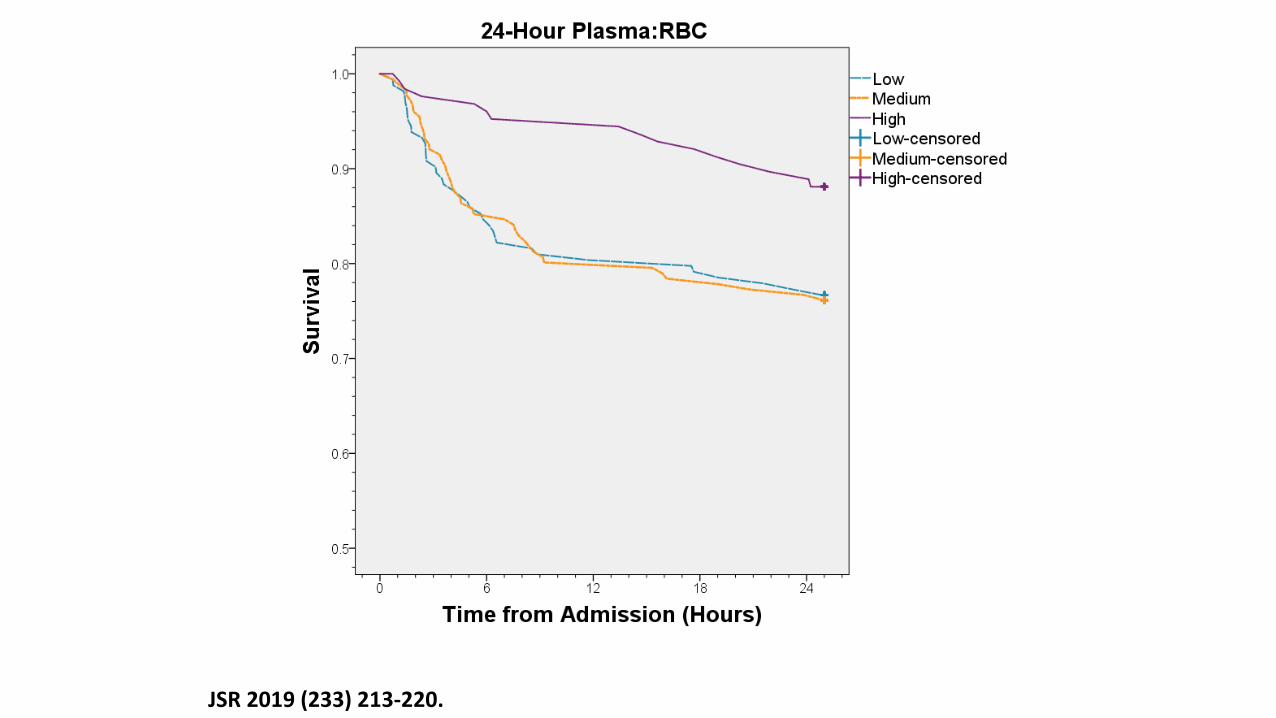
A High Ratio of Plasma:RBC Improves Survival in Massively Transfused Injured Children
• Retrospective review
• ACS TQIP
• 1/2015 to 12/2016
• Plasma/Platelet:RBC• Low <1:2
• Medium >1:2 - < 1:1
• High >1:1
JSR 2019 (233) 213-220.
JSR 2019 (233) 213-220.
Data Conclusions
• Tough question to study in retrospective fashion, heterogeneity of populations, rarity of event
• Those receiving massive transfusion and increased product are more severely injured
• Older children get more plasma and have higher plasma:PRBC ratios
• Children that get more higher plasma:pRBCratios may have improved survival, fewer vent days, but similar ICU LOS
• Ratio of platelets:pRBCs did not seem to affect mortality, vent days or LOS
A Survey of Pediatric Massive Transfusion Protocol Polices
• 46 Children’s hospitals
• Physician discretion was the most common activation criteria (89%)
• Most sites targeted equal ratios of plasma: PRBCs; 15% of respondents used antifibrinolytics
• Wide variation in MTPs among pediatric hospitals
• Activation criteria and products administered
Transfusion Med. 2016 Feb; 26(1): 49-56.
Development of MTP at your hospital
• Consider your local environment, resources, data to inform the process
• Trauma Program
• High Risk Surgeries—trauma, craniofacial, spinal fusion
• Blood Bank—evaluate potential availability of products, supply chain
• Utilize Pediatric Trauma Society Resources
https://pediatrictraumasociety.org/resources/clinical-resources.cgi
Who should be engaged in the process?
Surgery/Trauma
Emergency Medicine/NICU/PICU
Blood Bank
Anesthesia
Nursing
Transport Services
Communications
Conclusions
Highlighted data surrounding
• Pediatric MTP definition
• MTP activation triggers
• Outcomes of MTP in children
Creation and implementation of MTP

















