The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, research- related, and evidence-based nursing materials. Take credit for all your work, not just books and journal articles. To learn more, visit www.nursingrepository.org Item type Presentation Format Text-based Document Title Social Networking for Improved Maternal Child Health in Rural Settings Authors Argent, Autumn L.; Gavenus, Erika Ruth Downloaded 28-May-2018 23:18:09 Link to item http://hdl.handle.net/10755/622206
Transcript
The Henderson Repository is a free resource of the HonorSociety of Nursing, Sigma Theta Tau International. It isdedicated to the dissemination of nursing research, research-related, and evidence-based nursing materials. Take credit for allyour work, not just books and journal articles. To learn more,visit www.nursingrepository.org
Item type Presentation
Format Text-based Document
Title Social Networking for Improved Maternal Child Health inRural Settings
Vallary Migawi, Erin M. Milner, Elizabeth Bukusi, Lia C.H. Fernald1Organic Health Response-Ekialo Kiona Center, Mfangano Island, Kenya 2Atkinson Center for a Sustainable Future,
Cornell University 3Global Health Sciences, UCSF 4School of Public Health, University of California, Berkeley 5Arizona State University 6Kenya Medical Research Institute
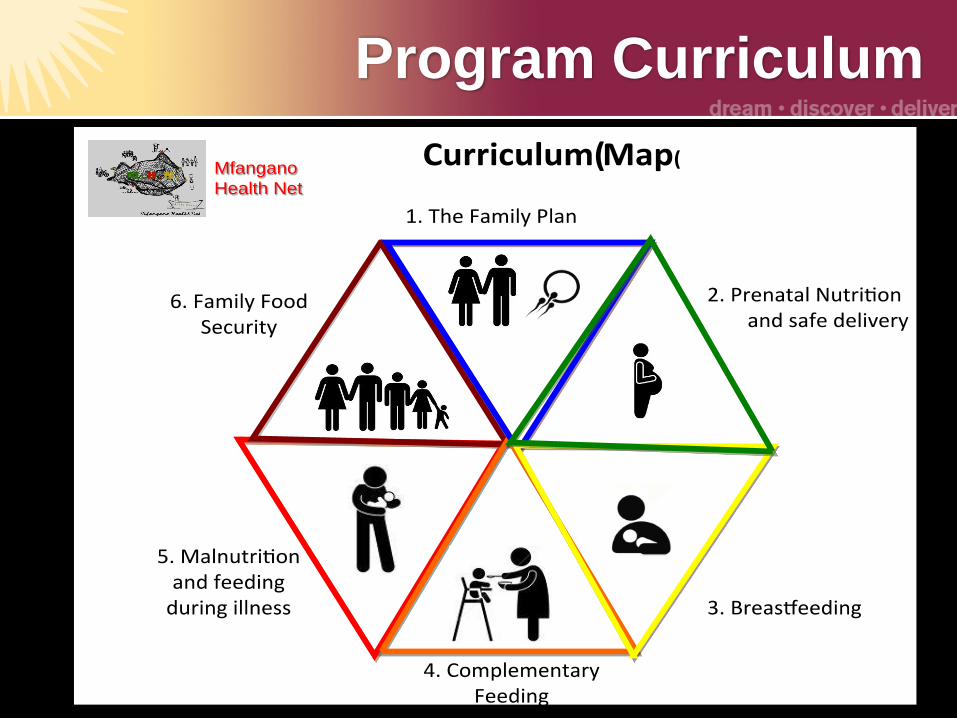
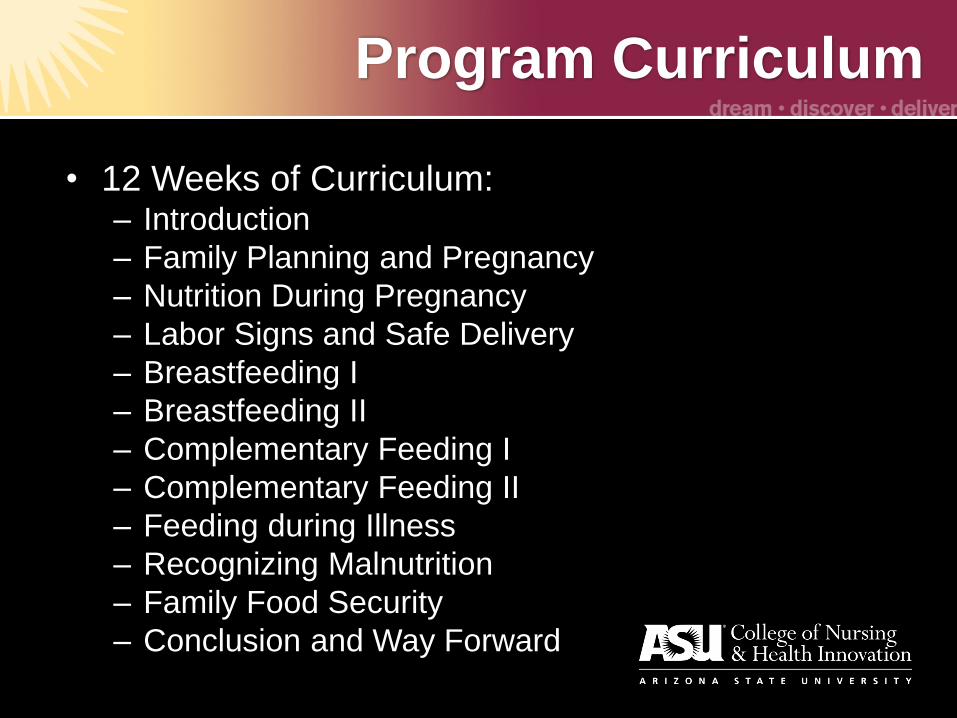
Objectives
• Identify the key qualitative aspects of developing a social networking nutrition program aimed at improving maternal child nutrition and health outcomes in rural and remote settings.
• Examine key areas of replication for a social networking nutrition program.
• Compare the population of Kenya and Northern Arizona for similarities and differences that will affect program development
• Explore the data analysis of the qualitative data obtained to date.
My background
• BS Nutrition
• BS Nursing
• MSN Nursing
Education
• 3rd year PhD,
CONHI
• RN for 11 years
• Maternal-Child
health focus
BETTERTHEFUTURE.ORG
Overview
• My work on with this project was to evaluate a nutrition intervention that uses a novel micro-clinic approach to treat whole social networks affected by maternal and child malnutrition.
• The key approach aims to foster social support for improved food security and nutrition-promoting behaviors by galvanizing support for these goals among not only mothers, but fathers, friends, and grandparents
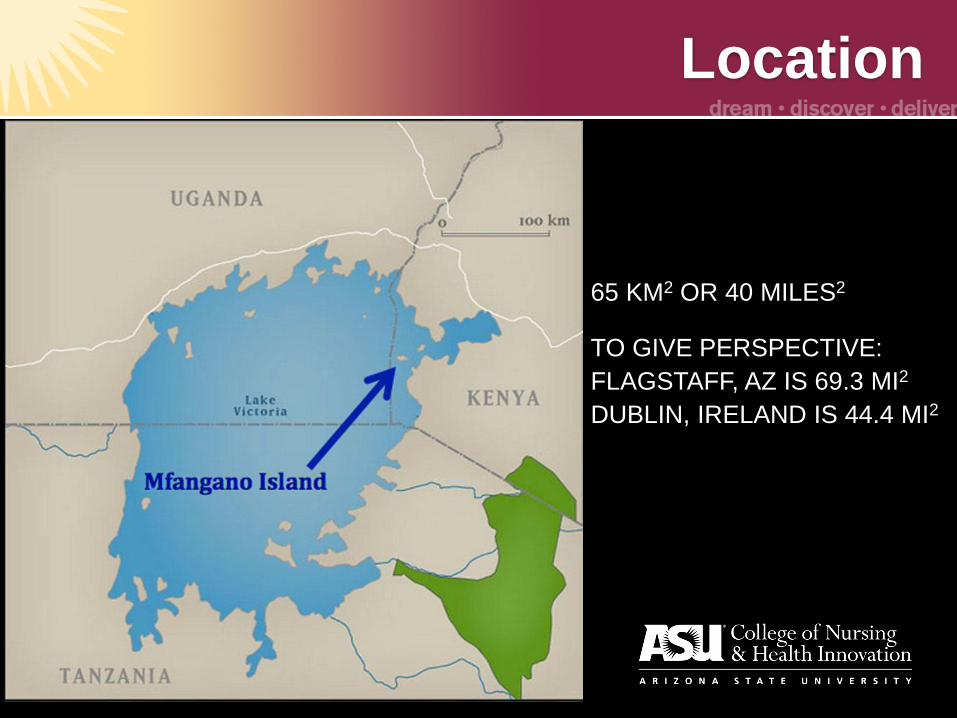
Location
65 KM2 OR 40 MILES2
TO GIVE PERSPECTIVE:
FLAGSTAFF, AZ IS 69.3 MI2
DUBLIN, IRELAND IS 44.4 MI2
Access
Maternal-child nutrition and
the social setting
• Background and significance (KNBS, 2010):
– 35% of children in Kenya are stunted
– 7% of children in Kenya are wasted
– 16% of children in Kenya are underweight
– 6% of all Kenyans have HIV• 36% of the population of Mfangano Island
have HIV/AIDS
– Food for sex industry pervasive among single or widowed women
Female Focus Group Participants
• Average age: 29.5
• Average number of people in the
household: 6
• Average age of children in household:
8
• Large households with many young
children
Maternal-Child Demographics in the
US and Arizona
• 305,388 babies were born to girls 15-19 years of age in 2012 (CDC, 2014)
• Estimated cost is $9.4 billion in taxpayer funds (CDC, 2014).
• Only about 50% of teen mothers receiving a diploma by 22 years of age (CDC, 2014).
• Children of teens are more likely to have increased healthcare needs, require foster care, have an increased chance of incarceration, and lower educational attainment (CDC, 2014).
• Teen pregnancy has been associated with increased medical complications, prematurity, and perinatal mortality (Salihu, Duan, Nabukera, Mbah, & Alio, 2011).
Maternal-Child Demographics in the
US and Arizona
• Non-Hispanic black, Hispanic, Native American, and socio-economically disparate youth are the populations experiencing the highest numbers of births (CDC, 2014).
• Hispanic teen birth rates were more than twice as high as the birth rates of white teens (CDC, 2014).
• Morales (2011) reported that rates of teen pregnancy are still high in the Southwestern states of New Mexico, Arizona, Nevada, and Utah.
• Recordings were translated into English and transcribed into written format for analysis
• Diagrams and memos will be used as needed to further interpret the setting and sessions
• All data is stored at the EK Center and in a secure online file storage system
Qualitative Data
• Perception of ’good nutrition’
– Balanced diet• Strength
• Disease prevention
• Energy
• Perception of ‘support’ • Food
• Childcare
• Monetary
• Education
Qualitative Data
• Perception of ‘Kanyakla’
– Change
– Health
– Education
– Knowledge sharing/stigma reduction
– Courage
– Friendship
– Freedom
– Confidence
Original Themes
• Nutritional balance: new knowledge of “balanced diet,” diversity of foods, and kitchen gardens
• Multi-dimensional support: community, social network, family, support; reduced incidence of disease; knowledge sharing; increased involvement of partner in choosing food and childcare
• Community collaboration: increased business opportunities for women, increased food trading, and improved childcare
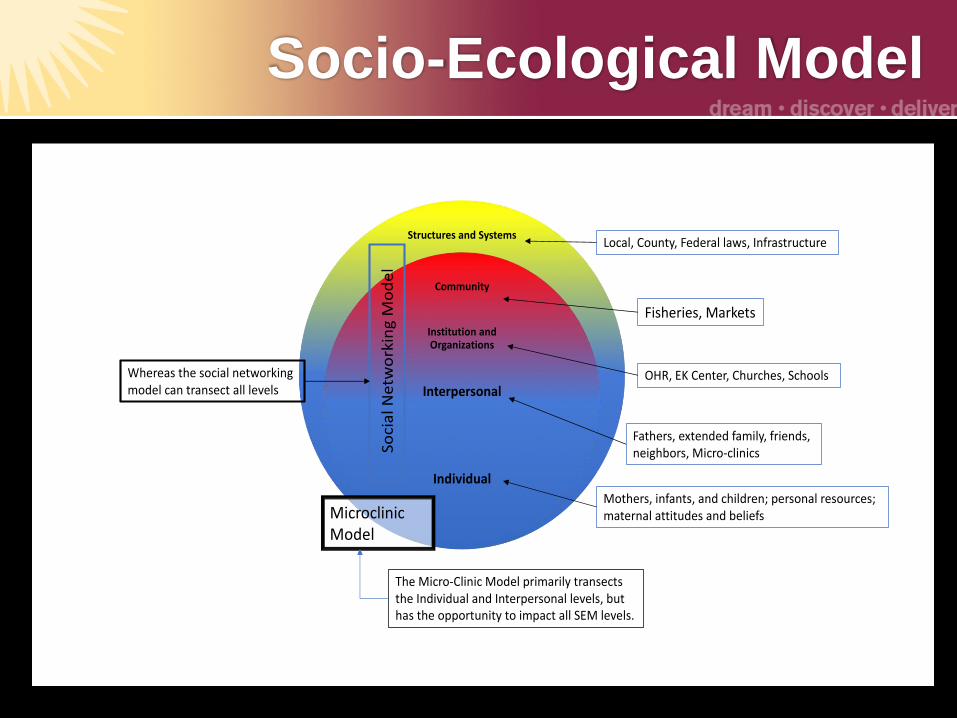
• Premise: Household nutrition among groups of family members and neighbors can influence
– Interpersonal Level: Family practices and behaviors
– Community Level: Norms and behaviors regarding breastfeeding, complementary nutrition, and family planning
– Systems Level: Food production and sustainability, freshwater environmental system, fishing practices and management
• See handout for SEM Level Analysis
Qualitative Data
• Weaknesses:– Support waned after completion
– Lack of financial support
– (perceived) Lack of support from EK center
– Failure of KIVA loan program within Kanyaklas
– Confidence• Nutrition knowledge but no finances
• Breastfeeding knowledge but concerns about storage
– Laziness• Decreased attendance
• Lack of participation in planning/implementation activities
• Discouraged
Similarities
• Food insecurity
– 24%
• Food desert
• Inadequate nutrition
• Social support
• Family units are multigenerational
• History of dependence on the land
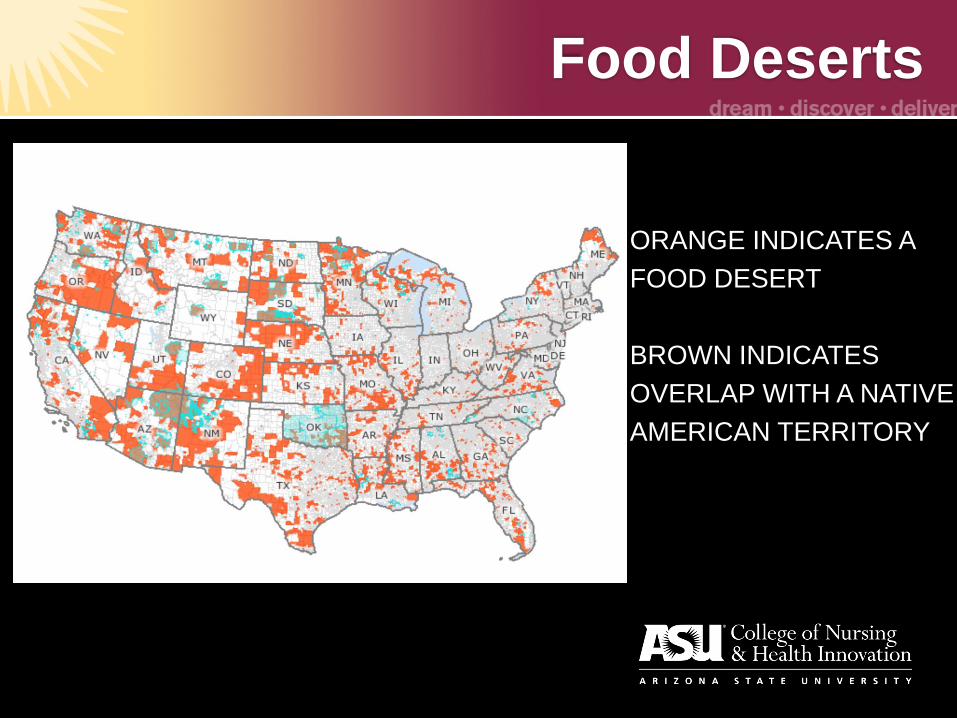
Food Deserts
ORANGE INDICATES A
FOOD DESERT
BROWN INDICATES
OVERLAP WITH A NATIVE
AMERICAN TERRITORY
Scaling out
• Modifying curriculum
• Cultural considerations
• Take home features:
– Community support must be continued
past program presence
• How?
– Planning must be implemented
• Follow up
• Follow through
Our future…
The team
References
• Brion MJ, Ness AR, Rogers I, Emmett P, Cribb V, Davey Smith G, Lawlor DA. (2010). Maternal macronutrient and energy intakes in pregnancy and offspring intake at 10 y: exploring parental comparisons and prenatal effects. American Journal of Clinical Nutrition, 91(3), p. 748-56. doi: 10.3945/ajcn.2009.28623.
• Corbin, J. & Strauss, A. (2015). Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory (4th ed). Los Angeles, CA: Sage.
• Kenya National Bureau of Statistics (KNBS) and ICF Macro. 2010. Kenya Demographic and Health Survey 2008-09. Calverton, Maryland: KNBS and ICF Macro.
• Glanz, K., Rimer, B. K., & Viswanath, K. (2008). Health behavior and health education :Theory, research, and practice (4th ed.). San Francisco, CA: Jossey-Bass.
• Gordon, A. & Oddo, V. (2012). Addressing child hunger and obesity in Indian Country: Report to Congress. Retrieved from http://www.fns.usda.gov/sites/default/files/IndianCountry.pdf
• McKinney, E., James, S., Murray, S., Nelson, K., & Ashwill, J. (2013). Maternal-Child Nursing, 4th ed. St. Louis, MO: Saunders/Elsevier
• National Campaign to Prevent Teen and Unplanned Pregnancy. (2015). Arizona Data. http://thenationalcampaign.org/data/state/arizona
• Nteff, G.M. (2013). The impact of education on recommended weight gain and selected prenatal outcomes in low income pregnant women. Research in Obstetrics and Gynecology, 2(3), p. 13-27. Doi: 10.5923/j.rog.20130203.01
• Salihu, H. M., Duan, J., Nabukera, S. K., Mbah, A. K., & Alio, A. P. (2011). Younger maternal age (at initiation of childbearing) and recurrent perinatal mortality. European Journal of Obstetrics & Gynecology and Reproductive Biology,154(1), 31-36. doi:http://dx.doi.org.ezproxy1.lib.asu.edu/10.1016/j.ejogrb.2010.08.006
• Smith, K.P. & Christakis, N.A. (2008). Social networks and health. Annual Review of Sociology, 34, 405-429. DOI: 10.1146/annurev.soc.34.040507.134601
• US Census Bureau (2015) State and County QuickFacts. http://quickfacts.census.gov/qfd/states/04/0423620.html
• Whisner, C. M., Young, B. E., Pressman, E. K., Queenan, R. A., Cooper, E. M., & O'Brien, K. O. (2014). Maternal diet but not gestational weight gain predicts central adiposity accretion in utero among pregnant adolescents. International Journal of Obesity, p. 1-6. doi:10.1038/ijo.2014.202 [doi]