Making Pregnancy Safer Department MATERNAL HEALTH INTERVENTIONS MATERNAL HEALTH INTERVENTIONS FOR REDUCING NEONATAL MORTALITY FOR REDUCING NEONATAL MORTALITY Workshop on building capacity in supporting countries Workshop on building capacity in supporting countries to include newborn health in child survival strategies to include newborn health in child survival strategies Ornella Ornella Lincetto Lincetto WHO WHO - - MPS MPS New Delhi, 5 December 2005 New Delhi, 5 December 2005
Transcript
Making Pregnancy Safer Department
MATERNAL HEALTH INTERVENTIONS MATERNAL HEALTH INTERVENTIONS FOR REDUCING NEONATAL MORTALITYFOR REDUCING NEONATAL MORTALITY
Workshop on building capacity in supporting countriesWorkshop on building capacity in supporting countriesto include newborn health in child survival strategiesto include newborn health in child survival strategies
OrnellaOrnella LincettoLincettoWHO WHO -- MPSMPS
New Delhi, 5 December 2005New Delhi, 5 December 2005
Making Pregnancy Safer Department
BackgroundBackground
• About 50% of neonatal deaths occur in the first day of life, in addition to 3.3 million stillbirths
• Most of these deaths are related to maternal health and survival
• Strengthening maternal services will improve neonatal health and survival
Making Pregnancy Safer Department
OutlineOutline
• Clinical interventions likely to improve neonatal health and survival
• Packages likely to accelerate progress
• Health system and policy interventions
Making Pregnancy Safer Department
MPS list of interventionsMPS list of interventions
• Essential: interventions that are absolutely necessary to satisfy the priority health care needs of women and newborn infants in all countries.
• Situational: interventions that are required specifically for women and newborns who live in settings with certain disease patterns
• Routine: interventions for all women and newborn infants to be provided preferably at primary health care level at appropriate times.
• Additional: interventions for women and newborn infants with complications and problems that can be managed at primary healthcare level.
• Specialized / referral: interventions for severe obstetric, newborn and medical complications, and surgical family planning in the hospital.
• Advanced: interventions that are introduced at the primary health care level once quality essential interventions provided to all women and newborn infants. They may be available at the tertiary level of care.
• Immunization against tetanus and rubella• Life style (STIs/HIV prevention, smoke, alcohol,
violence)• Well-spaced and wanted pregnancies
Making Pregnancy Safer Department
Antenatal careAntenatal care
• Essential– Tetanus immunization – Syphilis testing and treatment– Birth and emergency preparedness– Early detection and treatment of maternal and fetal complications – Information and counselling on self care at home, nutrition, safe sex, healthy lifestyle and
breastfeeding– Support for women with special needs e.g. adolescents, women living with violence
• Situational (routine, additional and referral)– Prevention of malaria (IPT and ITN) and treatment of uncomplicated and complicated malaria– Voluntary HIV counselling and testing; PMTCT by ART, infant feeding counselling, mode of
delivery advice; treatment of opportunistic infections
• Advanced– Screening and treatment for asymptomatic bacteriuria and infection with streptococcus B
(GBS)– Screening for rhesus isoimmunization– Selective use of ultrasound for diagnosing/confirming complications– Folic acid supplementation
Making Pregnancy Safer Department
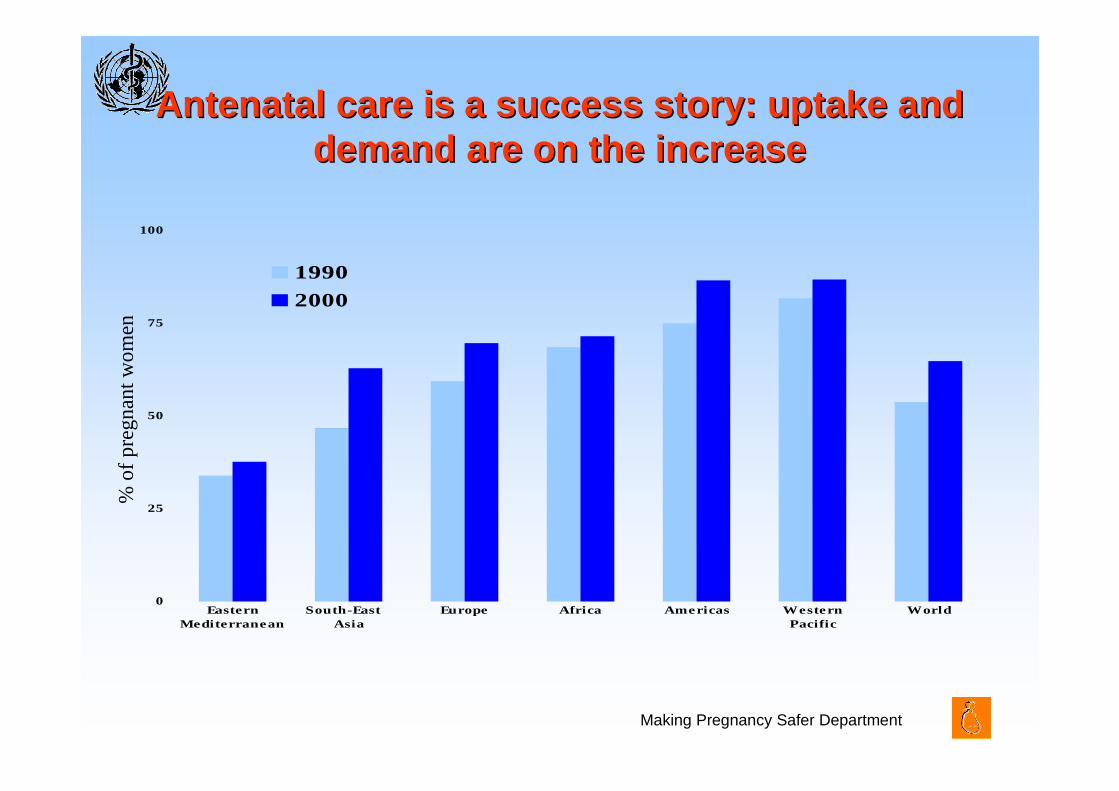
Antenatal care is a success story: uptake and Antenatal care is a success story: uptake and demand are on the increasedemand are on the increase
0
25
50
75
100
EasternMediterranean
South-East Asia
Europe Africa Americas Western Pacific
World
1990
2000
% o
f p
reg
nan
t w
om
en
Making Pregnancy Safer Department
ChildbirthChildbirth
• Routine – Monitoring progress of labour, maternal and fetal well-being with partograph,
provide supportive care and pain relief– Early detection and management of delivery and fetal complications– Promotion of exclusive breastfeeding
• Additional - bEmOC– Treatment of mild to moderate complications (e.g. prolonged labour, including
vacuum extraction; episiotomy, repair of genital tears, manual removal of placenta)
– Pre-referral management of severe complications (e.g. obstructed labour, fetal distress, preterm labour, breech presentation, severe peri- and postpartum haemorrhage)
• Specialized - cEmOC– Treatment of severe complications in childbirth and in the immediate postpartum
period (obstructed labour, malpresentation, eclampsia, severe infection, bleeding-including caesarean section, blood transfusion and hysterectomy)
– Induction and augmentation of labour
Making Pregnancy Safer Department
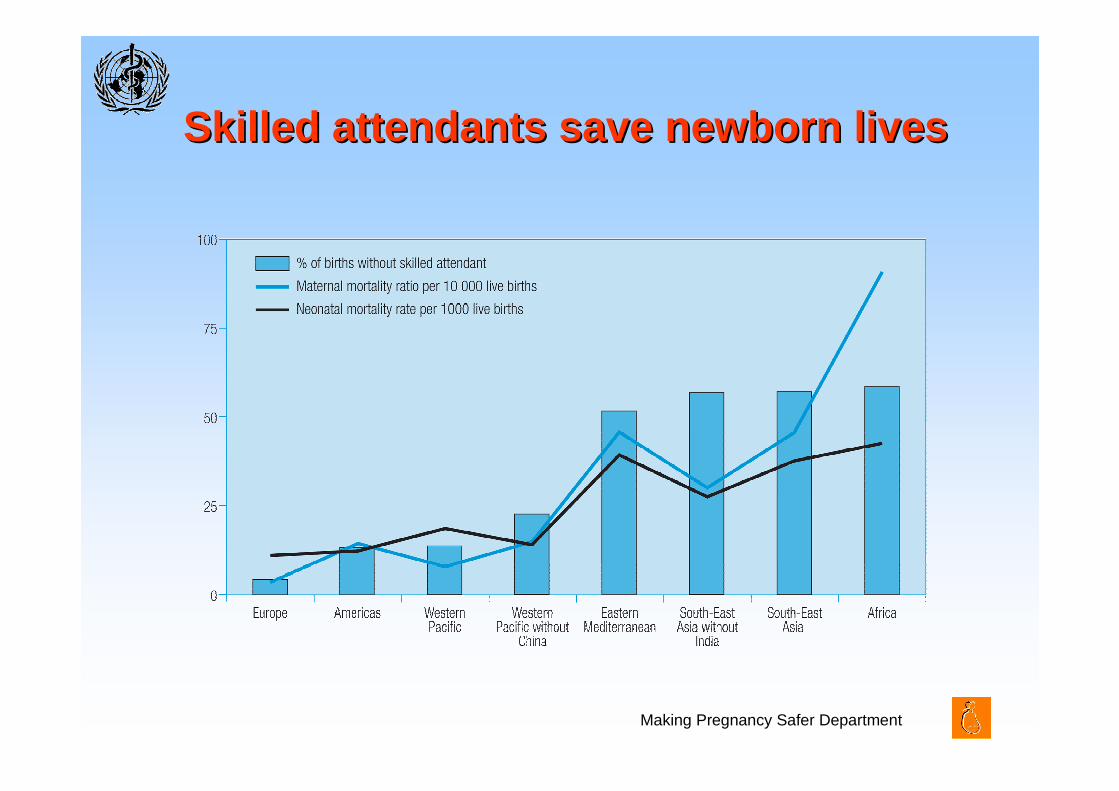
Skilled attendants save newborn livesSkilled attendants save newborn lives
Making Pregnancy Safer Department
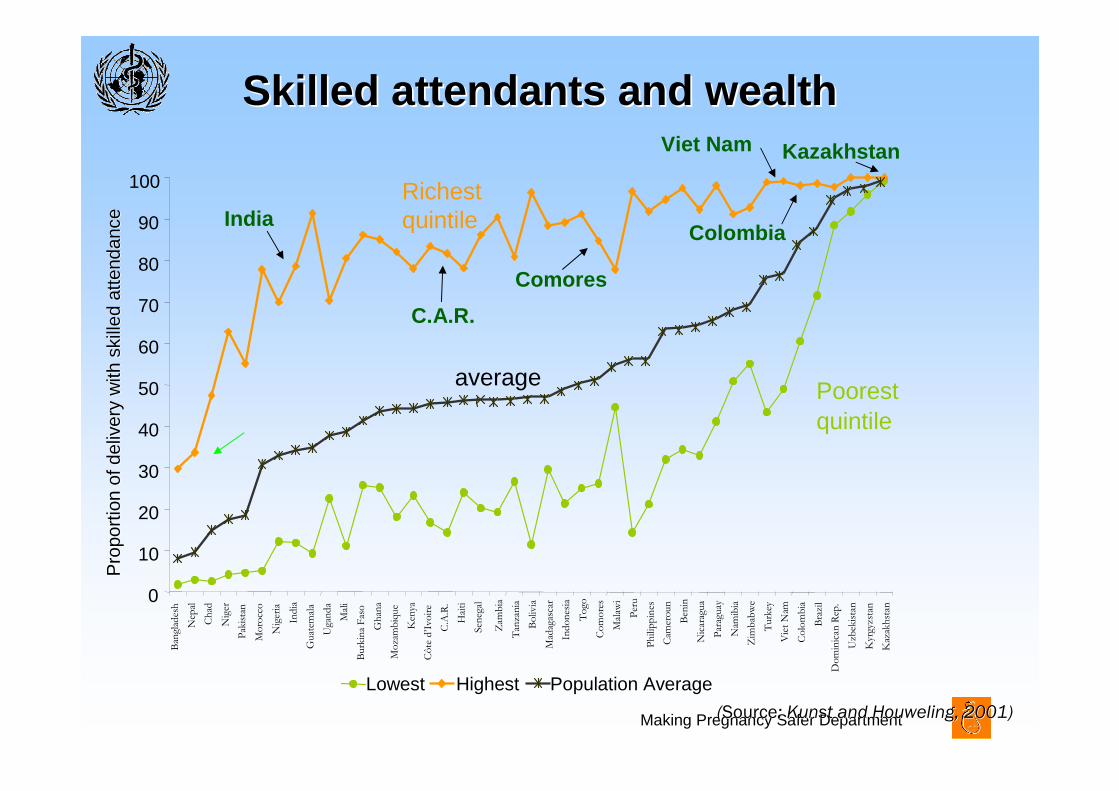
Skilled attendants and wealth Skilled attendants and wealth
((SourceSource: : KunstKunst and and HouwelingHouweling, 2001), 2001)
Poorest quintile
average
Richest quintile
Pro
port
ion
of d
eliv
ery
with
ski
lled
atte
ndan
ceP
ropo
rtio
n of
del
iver
y w
ith s
kille
d at
tend
ance
Zam
bia
Tan
zan
ia
Bo
livia
Mad
agas
car
Ind
on
esia
To
go
Co
mo
res
Mal
awi
Per
u
Ph
ilip
pin
es
Cam
eroun
Ben
in
Nic
arag
ua
Par
aguay
Nam
ibia
Zim
bab
we
Turk
ey
Vie
t N
am
Co
lom
bia
Bra
zil
Dom
inic
an R
ep.
Uzb
ekis
tan
Kyr
gyzs
tan
Kaz
akh
stan
Lowest Highest Population Average
India
C.A.R.
Kazakhstan
0
10
20
30
40
50
60
70
80
90
100B
angl
ades
h
Nep
al
Ch
ad
Nig
er
Pak
ista
n
Mo
rocc
o
Nig
eria
Ind
ia
Guat
emal
a
Uga
nd
a
Mal
i
Burk
ina
Fas
o
Gh
ana
Mo
zam
biq
ue
Ken
ya
Cô
te d
’Ivo
ire
C.A
.R.
Hai
ti
Sen
egal
Colombia
Viet Nam
Comores
Making Pregnancy Safer Department
Increasing the use of antenatal corticosteroids in preterm
pregnancies from 32% to 65%, will:
An Example of advanced intervention
Use of Antenatal Corticosteroids in preterm pregnancies in Latin America
perinatal mortality rate from 102 per 1,000to 88 per 1,000 live births
avoid 16,000 deaths in LAC per year
Making Pregnancy Safer Department
Postnatal carePostnatal care• Routine
– Assessment of maternal and neonatal wellbeing– Detection of complications (e.g. infections, bleeding, anaemia, postpartum
depression)– Iron & folate supplementation– Information and counselling on nutrition, safe sex, family planning and provision
of some contraceptive methods – Advice on danger signs, emergency preparedness and follow-up– Protection, promotion and support of exclusive breastfeeding
• Additional– Management of mild complications (e.g. infections, bleeding, anaemia,
postpartum depression)– Pre-referral treatment of severe complications
• Specialized– Management of severe complications (e.g. infections, bleeding, anaemia,
postpartum depression)
Making Pregnancy Safer Department
IFC interventionsIFC interventions
• Education activities to increase IFC awareness on MNH needs
• Establish mechanisms to assure community engagement in responding to MNH needs, including transport and finance for emergency situations, and to improving the quality of MNH care
• Support for special groups (HIV positive women, adolescents)
• Support from the family during childbirth and immediate postpartum
• Maternity protection in the workplace
Making Pregnancy Safer Department
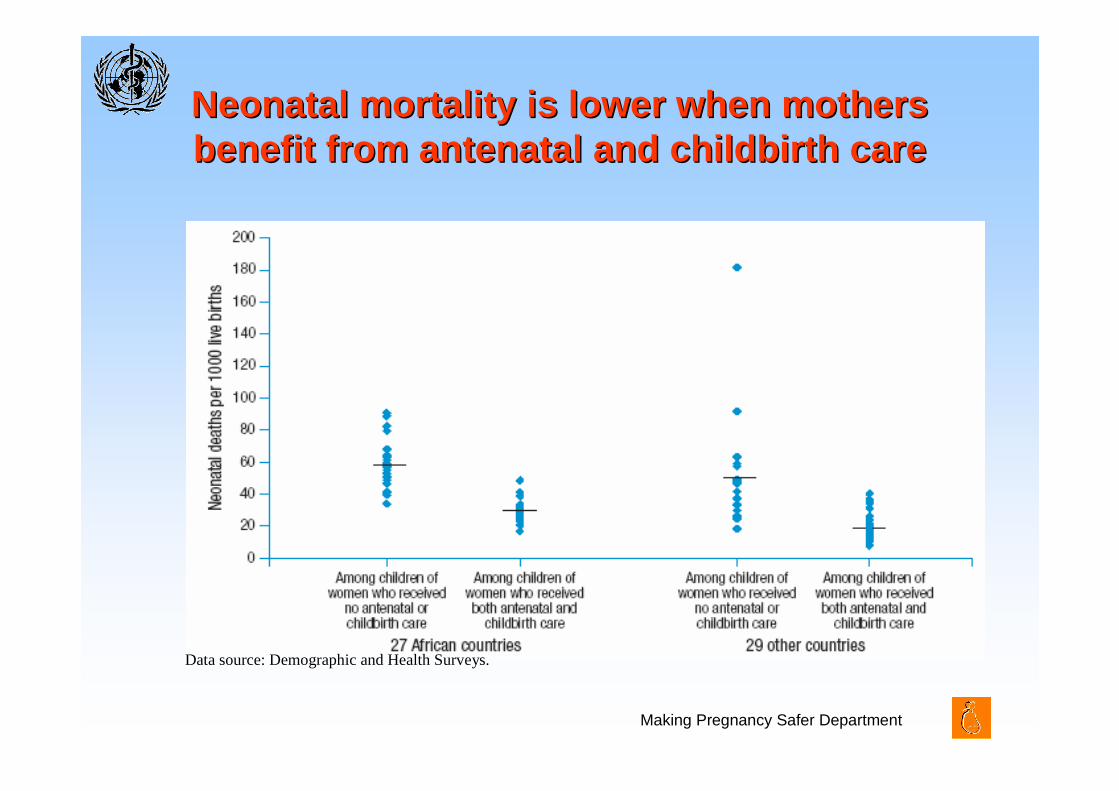
Neonatal mortality is lower when mothers Neonatal mortality is lower when mothers benefit from antenatal and childbirth carebenefit from antenatal and childbirth care
Data source: Demographic and Health Surveys.
Making Pregnancy Safer Department
The Lancet Neonatal Survival seriesThe Lancet Neonatal Survival series
• 16 interventions of proven efficacy on neonatal survival
• 3 delivery systems: family-community, outreach and facility-based
• Universal coverage of the 16 interventions could avert 41-72% of global neonatal deaths
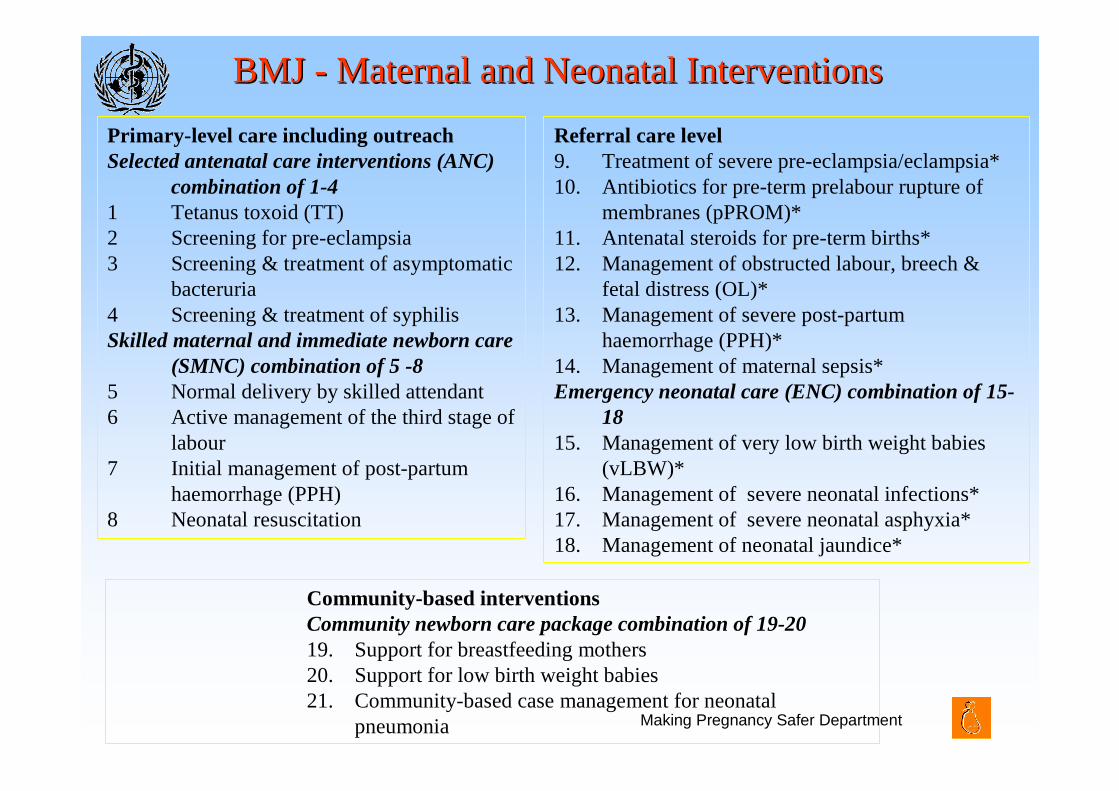
BMJ BMJ -- Maternal and Neonatal InterventionsMaternal and Neonatal Interventions
Primary-level care including outreachSelected antenatal care interventions (ANC)
combination of 1-41 Tetanus toxoid (TT)2 Screening for pre-eclampsia3 Screening & treatment of asymptomatic
bacteruria4 Screening & treatment of syphilisSkilled maternal and immediate newborn care
(SMNC) combination of 5 -8 5 Normal delivery by skilled attendant6 Active management of the third stage of
labour7 Initial management of post-partum
haemorrhage (PPH)8 Neonatal resuscitation
Referral care level9. Treatment of severe pre-eclampsia/eclampsia*10. Antibiotics for pre-term prelabour rupture of
membranes (pPROM)*11. Antenatal steroids for pre-term births*12. Management of obstructed labour, breech &
fetal distress (OL)*13. Management of severe post-partum
haemorrhage (PPH)*14. Management of maternal sepsis*Emergency neonatal care (ENC) combination of 15-
1815. Management of very low birth weight babies
(vLBW)*16. Management of severe neonatal infections*17. Management of severe neonatal asphyxia*18. Management of neonatal jaundice*
Community-based interventionsCommunity newborn care package combination of 19-2019. Support for breastfeeding mothers 20. Support for low birth weight babies 21. Community-based case management for neonatal
pneumonia
Making Pregnancy Safer Department
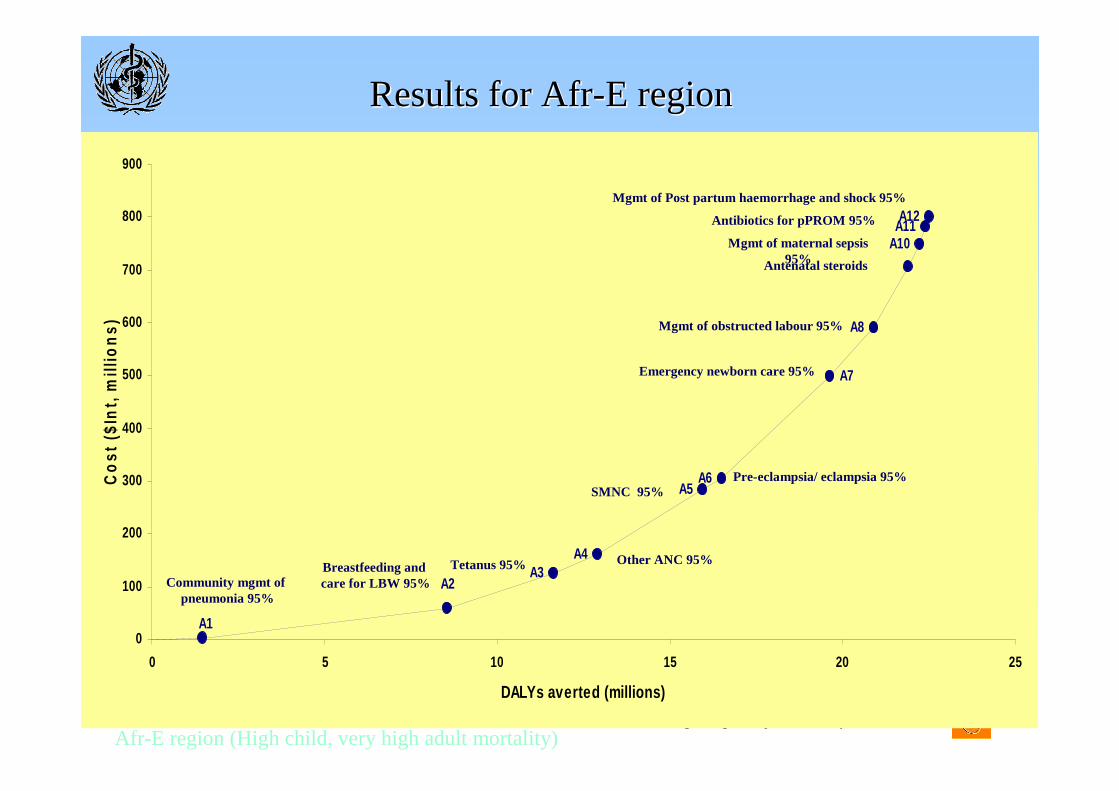
Results for Results for AfrAfr --E regionE region
Afr-E region (High child, very high adult mortality)
Community-based Mgmt of pneumonia (95%)
A3
A5
A8
A11
A1
A2
A4
A6
A7
A10
A12
0
100
200
300
400
500
600
700
800
900
0 5 10 15 20 25
DALYs averted (millions)
Co
st (
$In
t, m
illio
ns)
Breastfeeding and care for LBW 95%
Tetanus 95% Other ANC 95%
SMNC 95%
Antenatal steroids
Antibiotics for pPROM 95%
Pre-eclampsia/ eclampsia 95%
Mgmt of obstructed labour 95%
Emergency newborn care 95%
Mgmt of Post partum haemorrhage and shock 95%
Mgmt of maternal sepsis 95%
Community mgmt of pneumonia 95%
Making Pregnancy Safer Department
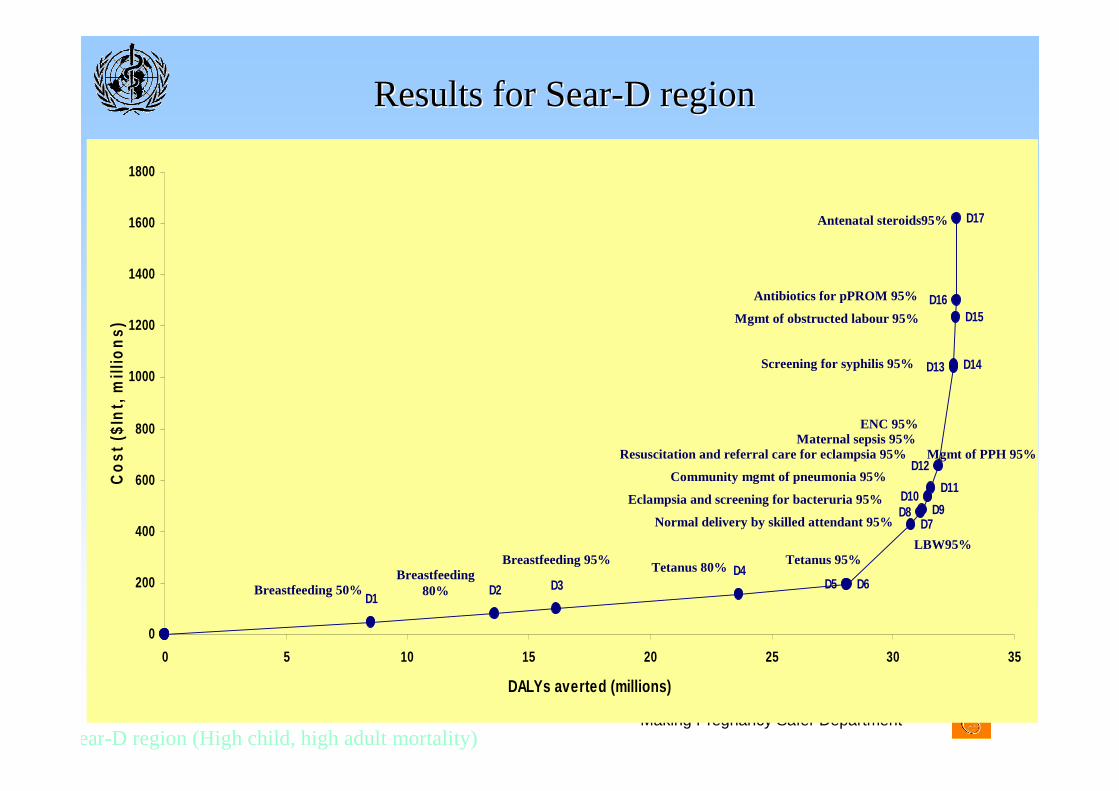
Results for SearResults for Sear--D regionD region
D9D10
D12
D14
D15
D17
D16
D1D2 D3
D4D5 D6
D7D8
D11
D13
0
200
400
600
800
1000
1200
1400
1600
1800
0 5 10 15 20 25 30 35
DALYs averted (millions)
Co
st (
$In
t, m
illio
ns)
Sear-D region (High child, high adult mortality)
Breastfeeding 50%
LBW95%
Breastfeeding 80%
Breastfeeding 95%Tetanus 80%
Tetanus 95%
Normal delivery by skilled attendant 95%
Eclampsia and screening for bacteruria 95%
Resuscitation and referral care for eclampsia 95%
Community mgmt of pneumonia 95%
Maternal sepsis 95%Mgmt of PPH 95%
Screening for syphilis 95%
Mgmt of obstructed labour 95%
Antenatal steroids95%
Antibiotics for pPROM 95%
ENC 95%
Making Pregnancy Safer Department
LimitationsLimitations
• Not all interventions included, e.g.– Family planning & safe abortion
– Surfactant therapy for respiratory distress syndrome
• Does not measure impact on stillbirths & morbidity from neonatal complications
• Estimates of effectiveness often based on evidence from developed settings
Making Pregnancy Safer Department
DiscussionDiscussion
• Most cost-effective mix of interventions was similar in the two regions:– Community-based newborn care package most CE, followed by:– Antenatal care – Skilled attendance at birth (basic maternal and neonatal care) – Referral-level emergency neonatal and obstetric care
• Coverage of the very CE interventions (ANC, SMNC, community-care) remains low– Where resource availability is extremely limited & unlikely to increase,
scale down less CE interventions & reallocate resources to these more CE options
• However, access to referral-level care will be necessary to achieve the MDGs ─ scaling up all interventions in this analysis to 95% coverage would halve neonatal and maternal deaths
Making Pregnancy Safer Department
Scaling-up will require legal and policy interventions
• To address the human resources crisis
• To achieve universal coverage
• To make it possible for mothers and babies to enjoy the right to survival, the right to health and the right to non-discrimination on the ground of poverty