THE EFFECT OF POSTURE ON THE MECHANIC, S OF BREATHING DURING INTERMITTENT POSITIVE PRESSURE RESPIRATION* H B F~L~Y, M B, B S, F F A a C S,~ AND DOUG!LAS ]~) HUNTEa, M D CHANCESIN PoSaXr~ during anaesthesia are a well-reqogmzed cause of ventalat embarrassment to the pataent 1,~ Several authorslhavq reported varlataons an v capacity when conscious subieets have been placed m d~fferent surgical p taons ~ r These vanatmns bear a very mdtreet relat~6nshap to changes oeeun m anaesthet.~zed patlents who are not breathing measurement of changes an hdal volume resultang inchoate a change an work-load only very m&reetly mvestagate the magmtude of the changes an the wc maintain satasfaetory ventalataon m the anaesthetaze honed for surgery, using the pressure-volume loqp as~ 9ry ttal )sl- mg max ally S mdarly, from changes m posit1 m2 This study was designed to rk of breathing reqmre d to d subject when he is ppsl- a basis for measurement METHOD They adult pahents, ehmcally normal from the (Iardlopulmonary standpoint, were ehvlded rote three groups of ten The meehaniq~s -- of resp~ratmn were measured an each group, m three different posltaons Group I Supine, s~ttmg, and right lateral positrons Gronp H Supine, hthotomy, and 45 ~ Trendelenburg posxtaons Group III Prone on a Mackay f r a m e 6 well flexed, prone on a Mackay frame flattened but wath abdomen dear of fqae table, and supine AnaesC~hes~a An pataents were premedleated with pantopon an~ hyoscme, anaesthesia was reduced with sodmm thaopentone and maintained wxtth mtrous ox~de oxygen n a proporhon of 2 1 Sufl~clent d-tuboeurmme was given ~o pxevent spontan~ ~us resp~atory efforts, whale ventllahon was maintained at a tLdal volume of 600 twenty tames per minute A 9 5 mm endotraeheal robe was used an all exc three patmnts an whom only a 9 mm tube could be passed A Moreh pls respirator 7 with the a~r retake converted to accept anaesthetm gases from a re, year bag, and a Morch non-return valve, were employc~ an all eases LL, ept ;Oil :er- l ~ t rumentat{on Pressure gradients across the lung-thorax were dgtected by a Statham PI~,3 &ffer~,nha] transducer, one side of which was e0nneeted to a. point immediately pro~amal to the endotraeheal tube. Th~s transducer was calibrated by a w~Lter ~From ~o Anaesthesm Research Laboratory ot &e Umverslty of Toronto § receipt of Medtea] Research Council Grant MBAd213. :~MedleA-Researeh Courted Graduate Student 11l~ Can Anaes See ]', vo] 11, no 2, March, 1964
Transcript
THE EFFECT OF POSTURE ON THE MECHANIC, S OF BREATHING DURING INTERMITTENT POSITIVE PRESSURE RESPIRATION*
H B F~L~Y, M B, B S, F F A a C S,~ AND DOUG!LAS ]~) HUNTEa, M D
CHANCES IN PoSaXr~ during anaesthesia are a well-reqogmzed cause of ventalat embarrassment to the pataent 1,~ Several authorslhavq reported varlataons an v capacity when conscious subieets have been placed m d~fferent surgical p taons ~ r These vanatmns bear a very mdtreet relat~6nshap to changes oeeun m anaesthet.~zed patlents who are not breathing measurement of changes an hdal volume resultang inchoate a change an work-load only very m&reetly mvestagate the magmtude of the changes an the wc maintain satasfaetory ventalataon m the anaesthetaze honed for surgery, using the pressure-volume loqp as~
9ry ttal )sl- mg
max ally S mdarly, from changes m posit1 m 2
This study was designed to rk of breathing reqmre d to d subject when he is ppsl- a basis for measurement
METHOD
T h e y adult pahents, ehmcally normal from the (Iardlopulmonary standpoint, were ehvlded rote three groups of ten The meehaniq~s -- of resp~ratmn were measured an each group, m three different posltaons
Group I Supine, s~ttmg, and right lateral positrons Gronp H Supine, hthotomy, and 45 ~ Trendelenburg posxtaons Group III Prone on a Mackay f r a m e 6 well flexe d, prone on a Mackay frame
flattened but wath abdomen dear of fqae table, and supine
AnaesC~hes~a An pataents were premedleated with pantopon an~ hyoscme, anaesthesia was
reduced with sodmm thaopentone and maintained wxtth mtrous ox~de oxygen n a proporhon of 2 1 Sufl~clent d-tuboeurmme was given ~o pxevent spontan~ ~us resp~atory efforts, whale ventllahon was maintained at a tLdal volume of 600 twenty tames per minute A 9 5 mm endotraeheal robe was used an all exc three patmnts an whom only a 9 mm tube could be passed A Moreh pls respirator 7 with the a~r retake converted to accept anaesthetm gases from a re, year bag, and a Morch non-return valve, were employc~ an all eases
LL, ept ;Oil
:er-
l ~ t rumentat{on Pressure gradients across the lung-thorax were dgtected by a Statham PI~,3
&ffer~,nha] transducer, one side of which was e0nneeted to a. point immediately pro~amal to the endotraeheal tube. Th~s transducer was calibrated by a w~Lter
~From ~o Anaesthesm Research Laboratory ot &e Umverslty of Toronto § receipt of Medtea] Research Council Grant MBAd213. :~MedleA-Researeh Courted Graduate Student
11l~
Can Anaes See ]', vo] 11, no 2, March, 1964
114
manometer before each measurement Tran: obta_med by connecting the other rode of the balloon, inserted m the lower thud oflth~ eharactenstacs of thas balloon were suc h tered when ~t was fi|!ed wath 0--4 mL ~ of fluctuataons were obtained by inserting the
c~,ma_~ ~STrmTtSTS" s~)ca~rr JOUaNaL
mlmonary pressure gradients were transducer to a 15 em o~sophageal oesophagus The presst~e-volume t no pressure changes were regas- Ltr Mammum resptrator~ pressure ~all~n, open to atmosp~mmc pres-
sure, prior to connecting at to the trmasduc( Asplrataon subsequently showed that negatwe mtrathoramc pressure had flrawJa an 1-1 5 mL of atr Al~- flow was detected by a No 2 Fleasch pneurnotact~ogra?h, placed between the ~on-return valve and the endotracheal tube The screen ~,vas heated by a 5 volt c~rrent The pneumotachograph was cahbrated wath la continuous flow of mr usaag Fasher- Porter flow meters, accmate to ~1% Flqws (lff an were converted to values for 2 1 N20 O~ nuxtures on the basis of th~ dtfference an physical characterastlc~ Thus 100 L ~ram of air = 84 89 L/man N2OtO2, ,at 14 7 P S I A and 70 ~ F The pressure d~fferenhal across the pneurnotachq])graph screen was dete~ted by a Statham PM5 transducer Volumes were denvied by electrical mtegratmn of flow, using a Grass U1-1 rnteglator
Pressure d~fferentml, mr flow, and volume] were recorded continuously on a Grass Polygraph Pressure and volume Changes were displayed on alTektromx dual beam oscilloscope, connected to the output of the Grass driver am~hfiers and cahbrated at the same hme as the latter A slrnple ,,witching device perrmtted the output from the flow channel to be substltutk~d for volume on the Y !~s Thus, either pressure-volume or pressure-flow loops 9ould be &splayed Photographs of loops were made on Polaroid film for measurement purposes, the dd~erence an screen and film cahbrahon was constant, for a gwen camera lens andl screen-to- film dastance, and the appropriate conversmn [factor was apphed to all photogra- phic measurements
Procedure Each pahent was measured only when the records of pressure, 'fow, and
volume were steady In each posltaon, a presstEFre-volume loop was photographed, switching was performed on the next resplrat0ry cycle and the film w~i~ then re- exposed, this hme to the pressure-flow loop oflthe third cycle Thus th~ I pressure- volume and pressure-flow loops of two s~mala~r cycles were supenmpo~,ed on the same film The cycles from whch the loops were recorded were marked automa- hcally on the polygraph paper, by a switch syhehromzed with the shutlter release cable This prowded the opportumty for subsequent checking of loop measure- ments from the polygraph trace and cor~rmattmn that the two loops Were from comparable cycles In each posltLon, loops ~veCe obtained for lung-thorax and then for lung rneehamcs
Dunng intermittent pomtwe pressure, iunglcomphance falls, and this may be increased by a single, large inflation 8 Sm~darlv, atrway remstanc~i~, may be reduced by a series of large breaths 9 In the pl~esent series, every effort Iwas made to carry out measurements during stable venhlatory circumstances and to avoid such large mflahons Once recordings were strutted, all measurements Were made within as short a hme anterval as posmble
FXltRX~Y & mmTF~. ~ o s r t r ~ AND ~ ~ c ~ oF m ~ T m N C :tJ.5
M e a s u r e m e n t s
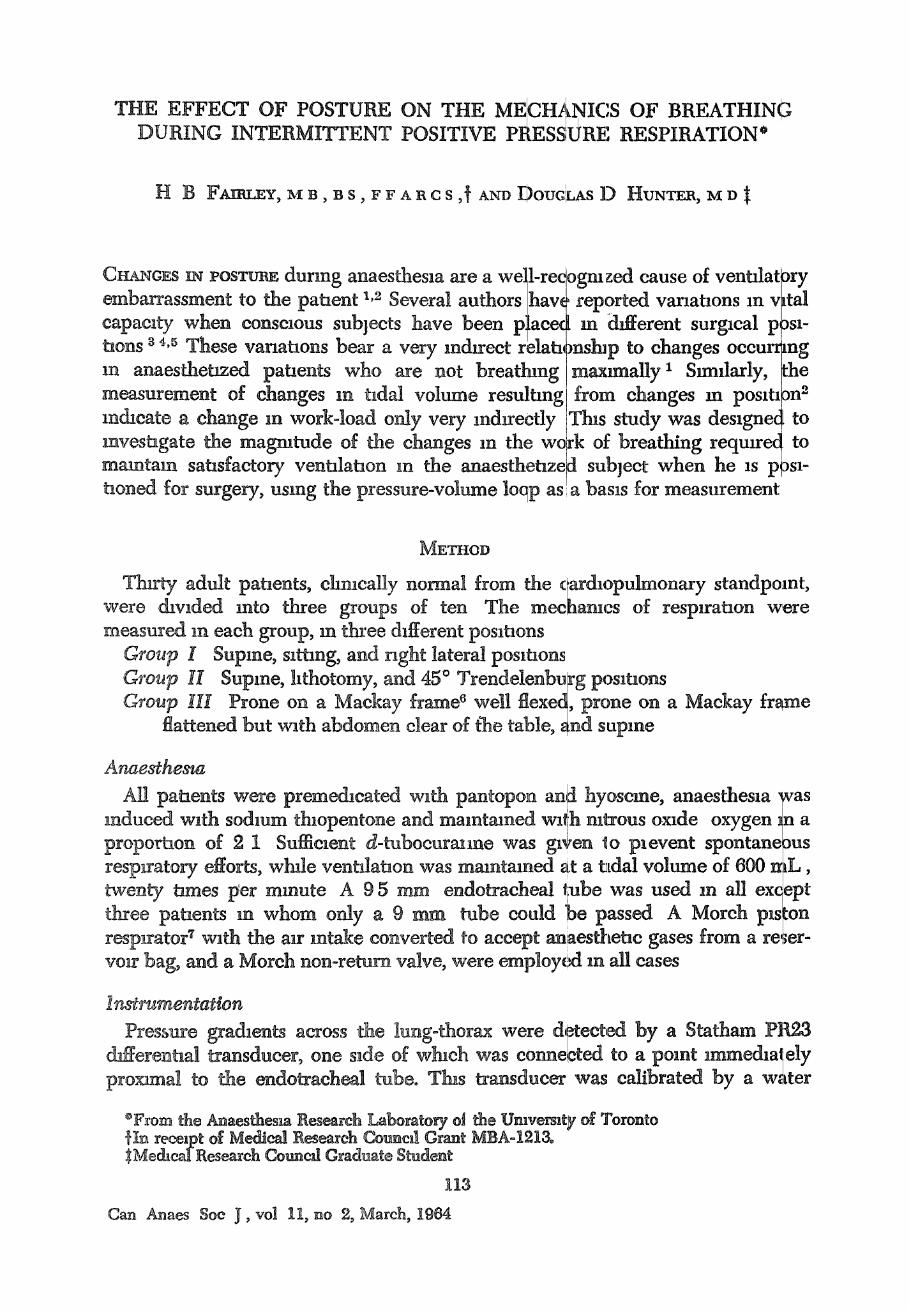
Each loop was traced on rmlhmeter squared graph paper The dynamm com- phance hne was drawn between points of mlfJ,mui and maxmaum volurrLe Where the shape of the loop was such that there wasl pressure change with ao volume change at end-mpzratmn or at end-expnaaoll: the exact points of z~ ro flow w~re ctetermmed by reference to the Grass recording and to the supenln- posed pressure-flow loop, as described by Watson ~'j c see Dl,,cussmn) Elastic work
Vmi
B
y J "
•
h ~ P ~ P cm HzO
F m ~ 1 Ide.xhzed pressure-volume loop 2A~Bu AB repre- sents the dynamm comphance hne
was calculated by measunng the area of the trmngh~ ABW (see Fig 1) Nc elas~c work was measured from the area of the haE tloop ABX When any p~ os the exp,ratory half of the loop crossed the Y aras I~h~s area was added to t non-etasac work Th~s occurred m a few instances m the prone poslaon. keeping w~th the standard s for spontaneous respniatmn, all work values we
n ~
rt le In re
mult~pheA by the resparatory rate and quoted in kg M i/mm Dynamm comphance was obt,~med by dwldmg the volume V' by the pressure dlfferentaal P'
RESULTS
The emthmetm means of the results obtained are ,,hown m Tables I, II, afld tII �9 authors lm2 have shown the lack of vahdity of oesophageal balloon values obtmned m the supine position Consequently, only the results obtmn~d m the sitting, right lateral, and prone posltaons haw been used an calculatmlns separating lung and thoracic wall components from toial lung-thorax values
S tatgstwa~ AnaZys~s Smca the resastances to lung and chest wall expansmn vary markedly w~th bo~]y
saze, ~ each group of ten va]lues showed a large varmhon from the mean. W~tle
116
'_? / I
c xv ,,r socam-Y jotr .
TABLE I LIrNC-THOI~AX M~SUI~M~-NTS
(Each figure represents the anthmeficlme,m of values for ten palaents)
Total Gr, gu p Po~lUons kg M/I
I Supine 0 9'~ ( 10 pataents) Sitting 0 9I
Right lateral 0 9]
II Supine ( 10 patients) Llthotomy
45 ~ Trendelenburg 1
HI Prone flexed 0 9~ ( 10 pattents) Prone flat O 93
Supane 0 8~
Sagmficant dafferences Group I Non-elastm work B Group II Elastic work ]
HI Prone flexed 0 47 0 08 0 39 ( 10 pauents) Prone fiat 0 36 0 05 0 31
'Sagmficant dafferences, Group ~ , elastxc work t Prone flexed > prone fiat
0 189 0 171
~z~u~r.~r a ~ P o S ~ AND M ~ ~ C S oF zaeAT~m~c 117
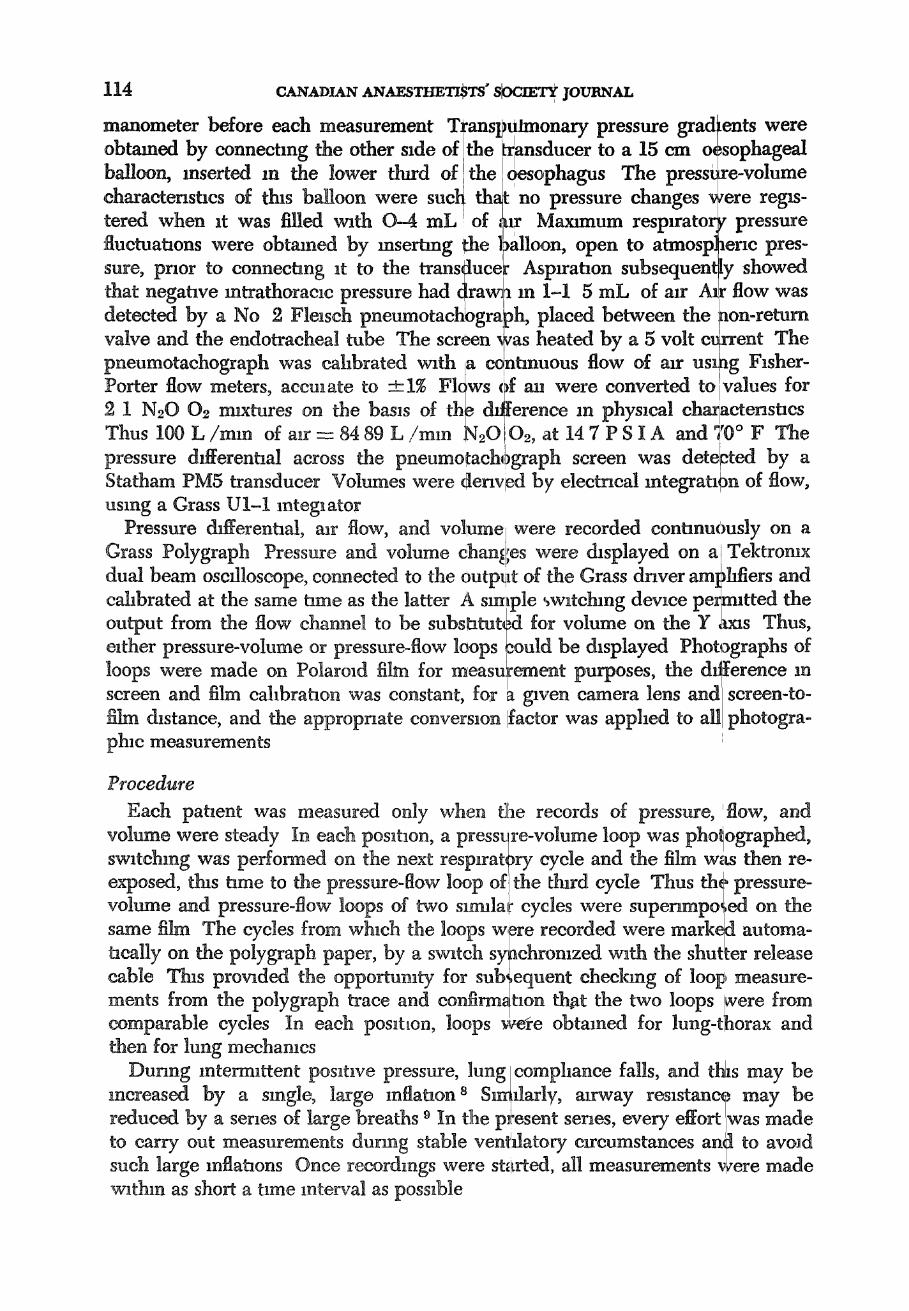
FIG~I~ g Comparison of ant}~rnet~q means of total ~lastlc and non elastic work,' m supine, .~ttmg and nght lateral pombons
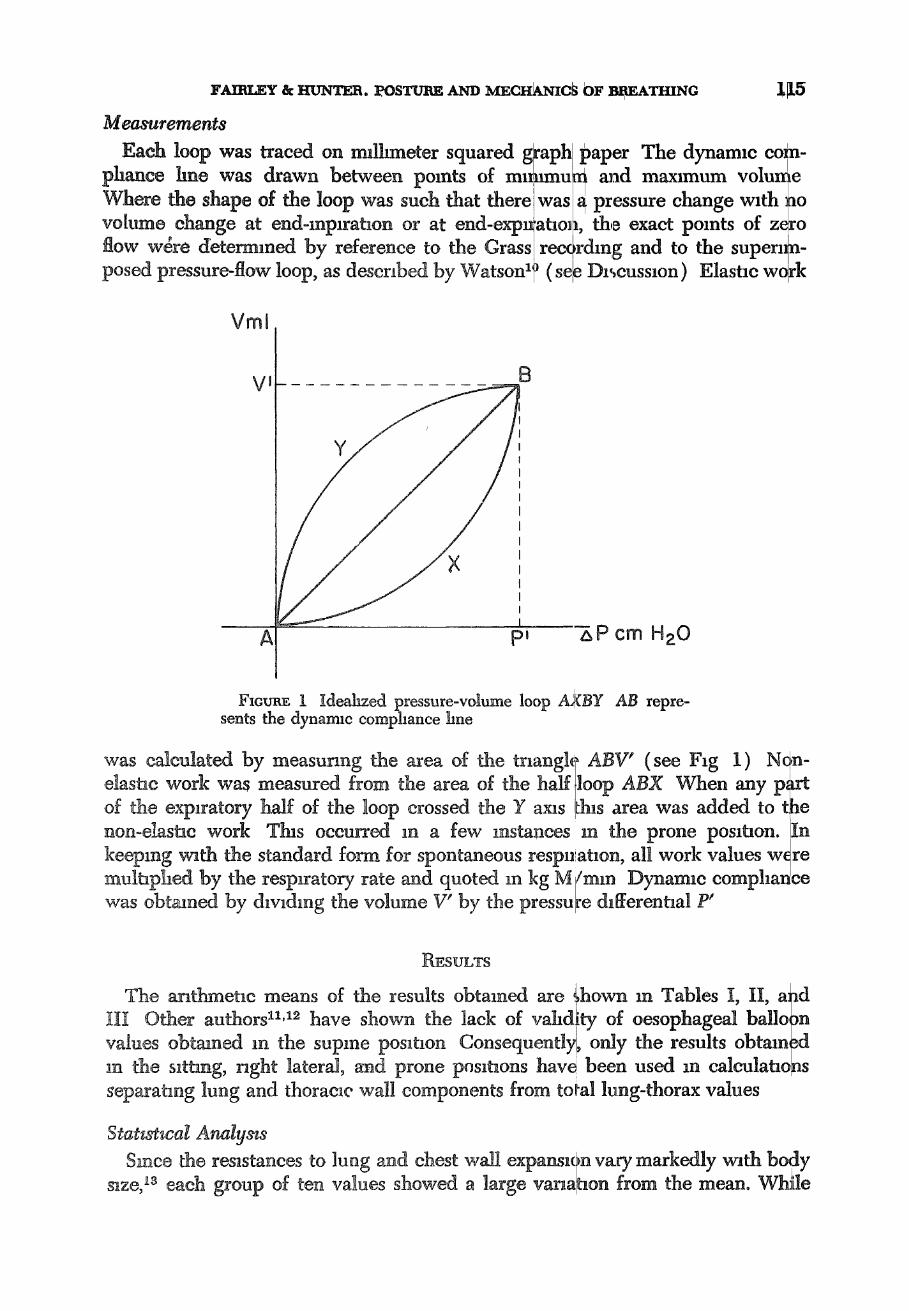
F~cuns 3 Companson of anthmebe mea__us of total, elastle and non elastlc work m supine hthotomy and 45 Trendelenburg poslhons
1!8 r . ~ c ~ . ~ A~,~F.s~m'm~ ~ jotraNxt
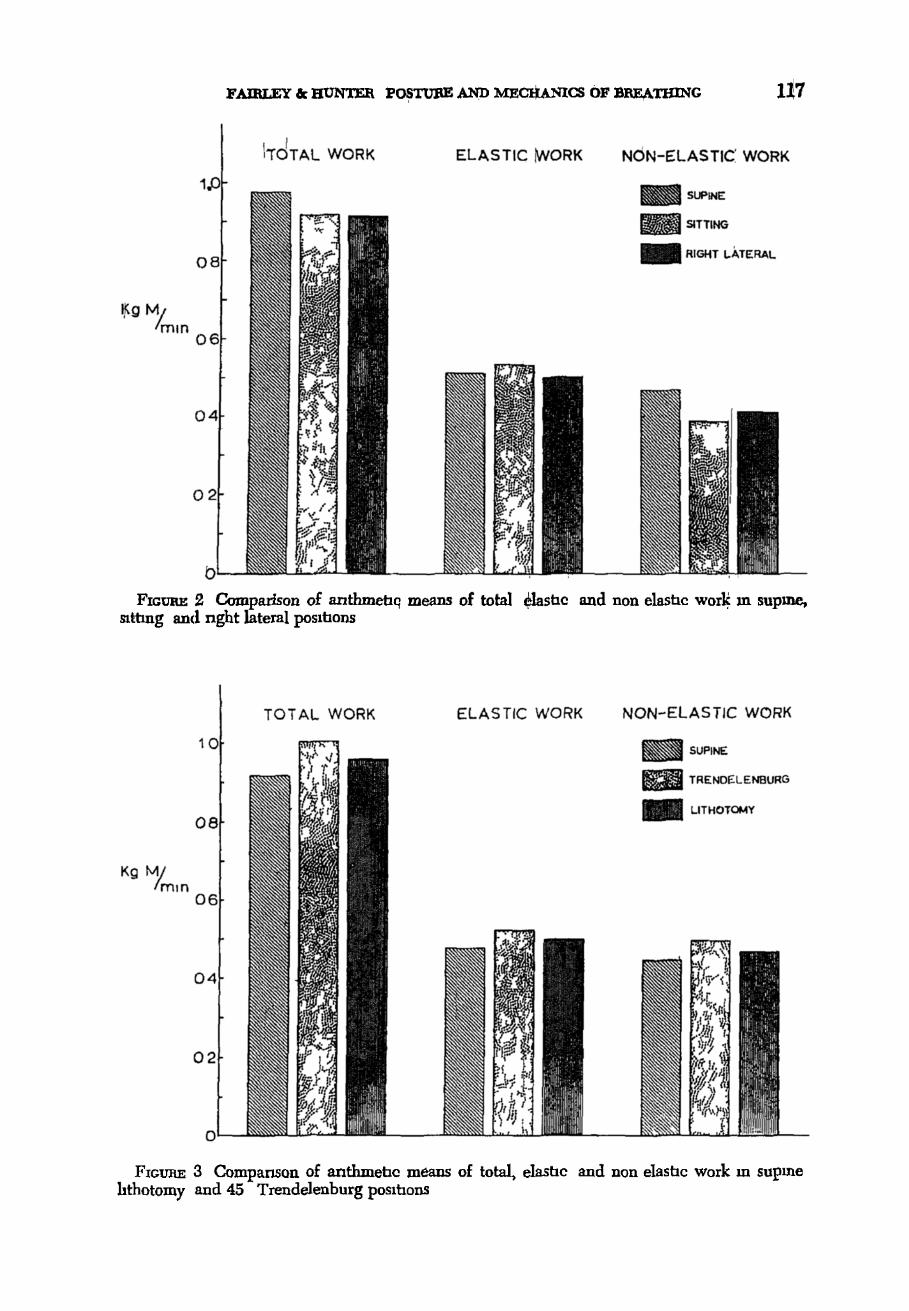
FIdUI~ 4 Comparrson of anthmetae means of total e l~ac and non-elaslac work m prone flexed prone fiat, and supine pOSlhOlaS
tins could have been reduced by relating each value to body weight thas was considered less useful than lettmg each pataent serve as his own control
Lung thorax values (Table I Fags 2 3 and 4) The total raw data were sub- matted to ~an a_n_alysas of variance from whtch it was found that the following means were slgmficantly &fferent at the 5 per cent level
Group 1 Non elastic work was greater in thd supine positron than m either the s l~ng or rtght lateral poslhons
Group H Elashc non elashc and total work were greater and the dynarmc comphance lower m the Trendelenbtrrg than m the supine posluon
Group lII Elastm and total work were greater m both prone posltaons than m �9 e supine position Elastic work was greater when the Mackay frame was flexed than when fiat Dynamic comphance was lower m both prone posl tlons than m the supme posmon
Lung values (Table II) The total raw data were submitted to an analysis of variance and none of the means were found to be slgmficantly different
Thoracw wall values (Table III) Stnndard devaahons znd the standard error of the m ~ n s were calculated for the d~fferences between values for each parr of posllaons These figures were subrmtted to a t test and only one pair of values were found tq be s~gndleantly cltfferent at the 5 per cent level Thus the thoracm wall elashe work was greater when the Mackay frame was flexed than when it was flattened
F ~ Y , ~ : ~ P o s r t r ~ AND I~tECa~CS OF BaEATmNC 119
DISCUSSION
Dunng spontaneous resp~ratmn, m conscmus maintain the artengl carbon dmxxde tensmn volumes and resprratory rate cdmbme to stnkq to overcome dead space-largely a matter of d , elastac reslstance, overcome by changes m respl~ values for work are quoted per minute m order
Dtmng mterrmttent posltave pressure resprrati detern~ned by the resptrator When the latter may deternune has own respiratory frequency but, c thas tc,3 is determined mechamcally Thus, values fc circumstances bear httle comparison w~th thosequt
albjects,/ventalatmn is adjuste vathna I very narrow hrmts '~t~ ~cqmPromase between the .stm Iwork-and vanattons m 'ator~ frequency ~4 Conseque to eJ[acornpass both factors. on, ~he size of the tadal volun as/?atmnt-tnggered, the pat
hmng controlled resprra r work obtamed under
d to 'ldal teed lon- ~tly,
le is rant 21on~ hese
~ ed for spontaneous resl)tra- tmn In thas study, most patients were hyperventdat, A (3/2 L / m m ), even al]o~v- mg for mechamcal dead space Tins accounts m par for the relatwely high v~ork v a ] l . l e $
During spontaneous respara~on, the shape determined by the characteristics of the lungs shape of one patmnt~s loop is comparable with the resparatory pattern as determined by a mech
of !he pressure-volume loo and mrvvay To some extenf. that of another However, v / mmal ventalator, the shape ot
loop also depends on the charactenstacs of the IrespLrator-partmularly , regard[ to its respiratory alr flow pattern ExplratLon ,~nll usually be pas. unless the respirator assists m this phase, but may be modrfied shghtly b)
:} 1S
the hen the
vlth i lve~
the
Vmi
6 0 0 B
A A P cm H20
Fmx~u~ 5 Typmal pressure-volume loo/~ obtained wath Morch piston resparator ('s honzontal]porta?n a t the
" f start of msparatmn as related to the translent surge o aar when tlae Morch valve opens )
12,0 c ~ ~ a ~ ~N~_.s r rm~" socma~ J O ~ A ~
expiratory valve resistance Both msptratc,ry and expiratory non-elastic reslstapce will be contributed to by endotracheal lntubahon Thus, loops obtained fr9m patients on resptrators wdl only be c6mp~tmble when identical respirator etrcum- stances have been employed and when ventdation has been delivered through mrways of ~dentmal resistance Thes~ re~ritmrements were met, milan this series, by ventilating all patients ~dentically and letting each pataent ser~e as Ins own control
Watson has descnbed ~:he relatively s resptrator 1~ and his method of determm~ m this series The Morch respirator prod and consequently a more classical press
quare loop produced b 3 lg the points of no flow uces a more smusoadal ure-volume loop, as sho~
, the Radcl/ffe has been used tr flow pattern r in Figure 5
Changes m body position can be expected to miluence the mee] .anlcs of respi- ration m a varmty of ways, such as Iby r m lung voluml, ~ (particularly FRC), 9,15,1~ changes m mtrapulmonary I blood volume, and mh;rference with thoracm wall movements and with chal~hragma~c descent Unf~u-a te ly , the measurement teehmque used ean only separate the lung contribution m certain positions and, m these, any changes /produced were too small toLbe stattstaeally slgmflcant However, the nature of ch~an, g~:s an work-load can be dee~. ected m man~y instances Thus, m the prone positron on bolsters, the additional l~ad is primarily elastm resistance to chest wall expanslon, l~hereas, m the Trendelehburg positron, both elastm and non-elastic work are increased
The magmtude of changes m work of breathing necessary to maintain constant ventilation, despate changes m body posltaon, can be calculate d from Tables I-IH For example, the largest percentag~ change produced was m moving from the prone flexed to the supane posat~on, When the total lung-thor~ elashc work fell by 34 per cent, Mthough the total work changed by only 17 Per cent Tdtmg patients from supane to a 45? Trendelenburg posltaon only nnposed an add~tmnal 9 per cent on the total lung-thorax work (Table I )
Presumably, these percentage change~ would be greater wltll pathological states, such as obesaty, ascates, hydrothorax, pneumothorax, pn/eumoma, pul- monary congestion
In a study on a series of supine paralysed pataents, Watson [was unable to lo n ~rnn o 1 demonstrate any thoxaem wa~ non-elashct resistance During i t 9 trent p s -
tave pressure m the pazalysed patient, the i proportxon of the chest/wall contribu- tion to total resistance probably depends On t~le size of the t~dal volume and the extent to which this passes the neuhal chest wall posltaon In t~s senes, chest wall non-elashc resistance accounted for 6 per cent of the tota~ work m the s ~ n g posat~on, 7 per cent m the right lateral, 8 per cent m the prone flexed, and 3 per cent in the fiat prone position
One unexpected s wa~ the unusmklly low elashe work m from the prone to the supine positron T~. the available data, but at may be relate~ sures necessary an the prone position, volume and an improved mr dlstnbuhon
e reason for this as not ; to the relatwely high resulting low mtrapul~
.xnght account for the sl
,ahents turned pparent, from inflation pres- nonary blood ~bsequent low
elastic work when pahents were turned to tlhe supine posxtmn The reason that the lung-thorax non-el,~shc resistance is higher m the supine
FAtaLlY ~ mmTF~ rOSTtraz AND MECmU~CS Io~ mU~TmNC 1~21 than m the s~ng_ and nght lateral posRmns ~s not ~pp' arent AI, gain' lung ,,apd chest wall components cannot be separated, but! vrobably the "falhng away'lof
m the last two osxtaons, la .., a Sl mfica~t role the abdominal contents, P ~ Y i g ~. Changes an lung volume may be an nnportant factox
From the practmal standpoint, one must conclude tlhat certain changes m p0s~- t~on do ~rd/uence the respiratory work load sagmfieanfl]k" Im |he par~lysed anaesthe- tized patmnt Under such circumstances inflation ~ll,~essure m~st be adjusted appropriately, ff constant ventdahon as to be mam~ame~d~
SUM~At~Y
Mechamcs of breathing have been measured m thlrtY curanzed anaestheta~ed normal adults, ventilated by antermattent posatw~ pressure The magmtude and nature of the changes m work of breathing requned tb maintain constant ventila- tmn despite changes m body positron have bee n as~ess~:l Posstlb]e reasons ~or these changes are suggested
l~Asu~
Chez 30 malades aduites sous anesth6sle, nous awms mesur6 les composan mec -a~xques de la resparatmn en emp]oyant ]es courbes pressrun-volume obten~ au cours de ]a resplratmn avec press~on positive mternuttente Nous avons mes~ le travail total de ]a resplrahon, ]e travail 6lashq~ae, ]e travad non 61ast~que et comphance dynarmque pour ]'ensemble poumon-thoraix et, cela, dans les posxtx~ ~avantes ass~se, ]at&ale dro~te, hthotom~e, Trendelenburg 45 ~ et ventrale part du poumon et de ]a paro~ thorac~que dins ces dom~6es est not6e pour ~sahons ass~se, ]at&ale droxte et ventrale Une analyse .,,tatastaque des r6sul| obtenus a 6t6 Irate et nous avons souhgn6 r~mport,mce des d~ff&ences apF cmbles du travail-ponds respxratoare
t6s les
la
ms
La
|es
ats
r~-
REFERENCES
1 Lrrx~,E, D M ,JB Posture and Anaesthesm Canad Ana~tsth See J 7' 2 (1960) 2 JoN~s, J B and JAcoBY, J The Effect of Surgmal Poslelon on Besparatmn Surg Fonnn
5 686 (19~5) 3 CASt:, E H and STmES, J A The Effect of Various Surgical Positrons on the Vlta]
Capacity Anesthesiology7 29 (1946) 4 SzxP~mN, C B The Influence of Posture on Mechames otn Bespxmtmn and Vital CapaCity
Anesthesiology9 134 (1948) 5 So~.LCmm, A, ELLm, D , Hmxox, C, & C~m:::~HF.LMFm, |E IV[ Pulmonary Functmn as
A~ffected by Operative Posxtmn Anesthesxcdogy 10 577 [1949) 6 MAC~Y, I M A New Frame ~or the Positmnmg of P,,~tmnts for Surgery of the Beck
Canad Anaesth Soc J 3 279 (1956) 7 k~.zl~Y~ E E, MORCE, E T, & BIINSON, D "~' Cntmally ICrushed Chests J Thorae Surg
32 9.91 (1956) 8 BEND~N, H H, HrTnLEY-WI~Y2~, j , & LAVEn, M B J~c~t~s~ Physmlogm Shunt~g
dunng Anaesthesm and Surgery Anesthe,,mlogy 24 122 (1963) 9 Bmscoz, W A & D~rnom~ A B Relatmnshlp-~etweenAlrway Reststance, Airway ~on-
ductance and Lung Volumes m Sub]ects of Different Age and Body Size J C,lm ~avestlgataon 37 1279 (1958) _ J _ .. - -
10 WA rsor~, W E Observatmns on the Mechamcal Wor~ ~f Interrmttent v o s l U v e rres~ure ]~tespxratmn Bnt J Anaesth 34. 433 (1962)
122 caNAvL r sArm maszs' socmrY IOtm m
11 MEAD, J & G~ss, .~. E A Esophageal ~ d P]eural Pressures in Man, Upnght and Supine J. AppL PhysmL 14. 81 (1959). , . . . . ~ -" . _1
12 Fzmus, B G, Jl~, M~Av, J , & ~ , IN I~L Effect ot :Body PoMtlon on ~sopnage m Pressure and Measurement of Pulmona~ Comphance J Appl Phenol 14 521 (1959)
13 Coot,, C D, HeH.w~za% P J, & Ao~o6r~lS Relalaon between Me~cl~amcs of Resp~atto~a, Lung $~ze and Body S~ze from Brahe to Young Adulthood J Appl. Physaol 13~. 349 (1958)
14 OTIS, A B, FZN~, W O, & RAm% H Mechm~ics of Breathmg m Mma ] App1 Vhysml 2 599. (1950)
15 MARSHALL, R The Physmal Propektms ~f tho Lungs m Relation t01 the Subdlvislbns 0 f the Lung Volnme Chn Scl 16. 12 (1~t57)
16 Co~moE, J H, JB, Fomvim, R E, IMmo~! A B, Bmscor, W A, and C~mLSr~N, E The Lung 2nd ed Chicago Yearbook Medical Pubhshers (1962)