May 28 – 30, 2015, Montréal, Québec All Pulmonary Emboli Should Be Treated Carole Dennie MD FRCPC Professor of Radiology and Medicine University of Ottawa Section Head, Cardiac and Thoracic Radiology The Ottawa Hospital The Case AGAINST No Yes
Transcript
May 28 – 30, 2015, Montréal, Québec
All Pulmonary Emboli Should Be Treated
Carole Dennie MD FRCPCProfessor of Radiology and Medicine
University of OttawaSection Head, Cardiac and Thoracic Radiology
The Ottawa Hospital
The Case AGAINST
No
Yes
May 28 – 30, 2015, Montréal, Québec
I do not have an affiliation, financial or otherwise, with a pharmaceutical company, medical device or communications organization.
I have no conflicts of interest to disclose ( i.e. no industry funding received or other commercial relationships).
I have no financial relationship or advisory role with pharmaceutical or device-making companies, or CME provider.
I will not discuss or describe in my presentation at the meeting the investigational or unlabeled ("off-label") use of a medical device, product, or pharmaceutical that is classified by Health Canada as investigational for the intended use.
The Lung is a Natural Filter• Has dual blood supply• Prevents small emboli formed
in systemic venous circulation from travelling to systemic arterial circulation
• Capillary endothelium has complete complement of fibrinolytic enzymes to break down clot without clinical effect
1Goodman LR. Radiol 2005;234(3):654-58 2Storto ML et al AJR 2005;184(1):264-67
3Ritchie G et al. Thorax 2007;62:536-404Schultz DJ et al. J Trauma 2004;56:727-31;discussion 731-33
Wiener RS et al. Ann Intern Med 2011;171:831-37
Time Trends in PE Diagnosis
Additional cases of PE may be associated with a lower severity of illness
72% increase in incidence of PE as primary diagnosis
No change in mortality
36% decrease in case fatality
When a Test is Too Good
Wiener RS et al. Ann Intern Med 2011;171:831-37
Evidence for Overdiagnosis• Anderson DR et al. JAMA 2007
– Randomized controlled trial comparing utility of CTPA and V/Q
– Greater # of PE diagnosed with CTPA than V/Q– Rate of VTE at 3 months identical in untreated patients – Additional PE cases on CTPA clinically unimportant
Anderson DR et al. JAMA 2007;298:2743-2753
Evidence for OverdiagnosisMeta-analysis
22 clinical trials
• Subsegmental PE (SSPE) diagnosis 4.7% for single vs 9.4% for MDCT
• False negative (FN) rate - 0.9% vs 1.1% respectively
• MDCT increases diagnosis of SSPE without change in FN rate SSPE may not be clinically relevant
Carrier M et al. J Thromb Haemosst 2010;8:1716-1722
Donato AA et al.Thrombosis Research 2010;126 ;e266–e270
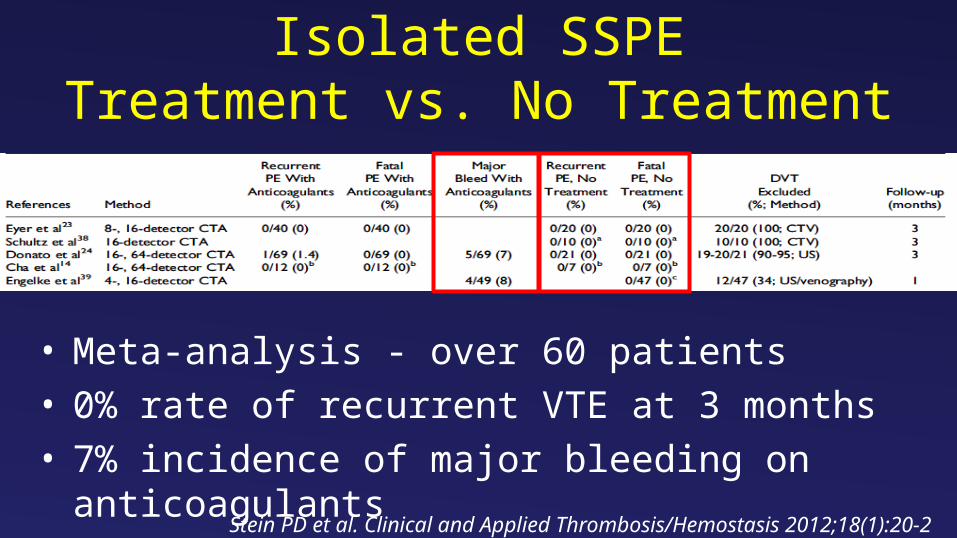
Isolated SSPETreatment vs. No Treatment
• Meta-analysis - over 60 patients• 0% rate of recurrent VTE at 3 months• 7% incidence of major bleeding on anticoagulants
Stein PD et al. Clinical and Applied Thrombosis/Hemostasis 2012;18(1):20-2
Current Guidelines
ACCP guidelines from 2012 do not differentiate between SSPE and more proximal PE
European Society of Cardiology guidelines from 2014 suggest individualized decision if SSPE and negative leg vein ultrasound
Kearon C et al. Chest 2012;2(Suppl):e419S-94SKomstantinides SV et al. Eur Heart J 2014;35:3033-73
SSPE: Who Not to Treat• Adequate cardiopulmonary reserve• No evidence of DVT• Major risk factor for PE no longer present, ie.
surgery, trauma, and no continuing risk factor • No history of central venous catheterization• No history of atrial fibrillation• Compliant and trustworthy patient who would return
for serial noninvasive leg tests
Stein PD et al. Clinical and Applied Thrombosis/Hemostasis 2012;18(1):20-2Hunsaker AR et al. Circ Cardiovasc Imaging 2010;3:491-506
Rebut
tal Rebuttal
• The lung is a natural filter• MDCTPA is too goodOVERDIAGNOSIS!• All dots are not clots• Overdiagnosis leads to overtreatment• Overdiagnosis may lead to more harm• Overdiagnosis costs more• Who not to treatSSPE
SSPE: Who Not to Treat• Adequate cardiopulmonary reserve• No evidence of DVT• Major risk factor for PE no longer present, ie.
surgery, trauma, and no continuing risk factor • No history of central venous catheterization• No history of atrial fibrillation• Compliant and trustworthy patient who would return
for serial noninvasive leg tests
Stein PD et al. Clinical and Applied Thrombosis/Hemostasis 2012;18(1):20-2Hunsaker AR et al. Circ Cardiovasc Imaging 2010;3:491-506
What is the Radiologist’s Role?• Recommend V/Q in patients with normal CXR• SSPE diagnosis on CTPA only when certain
– May recommend leg vein ultrasound in limited negative CTPA for added safety
“Placing the responsibility for overtreatment on the users rather than the providers of diagnostic
information amputates the clinical importance and value of radiologists”
Jha S. Radiol 2014;270(2):628-29
What is the Future of SSPE Diagnosis?
Outcome Trial • Prospective management cohort study
(NCT01455818)– Canada, France, Switzerland– Anticoagulation withheld
• Patients with SSPE diagnosis on CTPA• No DVT on serial leg vein ultrasound