1 MDS 3.0 Training Case Mix Team Office of MaineCare Services Updated May 2015 1 MDS 3.0 Training Agenda Welcome and overview History Chapter 2 Case Mix Implications Chapter 3 – section by section Section S – State only Section X – corrections Questions 2 MDS 3.0 History 3
Transcript
1
MDS 3.0 Training
Case Mix TeamOffice of MaineCare Services
Updated May 2015
1
MDS 3.0 Training Agenda Welcome and overview History Chapter 2 Case Mix Implications Chapter 3 – section by section Section S – State only Section X – corrections Questions
2
MDS 3.0 History
3
2
2
Goals of the MDS 3.0• Resident Voice – MDS 3.0 includes interviews for
Cognitive Function, Mood, Personal Preferences,and Pain.
• Clinical Relevancy – MDS 3.0 Items are basedupon clinically useful and validated assessmenttechniques.
• Efficiency – MDS 3.0 sections are formatted tofacilitate usability and minimize staff burden.
RAI Manual: click on RAI manual on left, scroll downto bottom of page.
Item Set (MDS 3.0 Assessment tool): click on RAItechnical information on left; scroll down to bottom ofpage.
Case Mix Implicationsfor MDS 3.0
6
3
7
Case Mix Payment Items
Certain items coded asRUG III services,conditions, diagnosesand treatments on theMDS 3.0 assessmenthandout .RUG IV refers topayment items for PPSservices.
8
9
MaineCare Case Mix
Maine uses a modified RUG III Code forCase Mix purposes.
PPS / Medicare uses RUG IV codes
Supporting Documentation forCase Mix payment items is
required
4
There are 7 Categories:• Rehabilitation• Extensive• Special Care• Clinically Complex• Impaired Cognition• Behavior• Reduced Physical Function• Default or Not Classified
10
Case Mix Weights
11
12
5
13
14
Case Mix Quality AssuranceReview
About every 6 months, a Case Mixnurse reviews a sample of MDS3.0 assessments and resident
records to check the accuracy ofthe MDS 3.0 assessments.
Insufficient, inaccurate or lack ofdocumentation to support
information coded on the MDS 3.0may lead to an error.
15
Poor Documentation could alsomean…
Lower payment than the facilitycould be receiving, OR
Overpayment which could lead tore-payment to the State
(Sanctions). This is due to eitheroverstating the care a resident
received or insufficientdocumentation to support the
care that was coded.
6
16
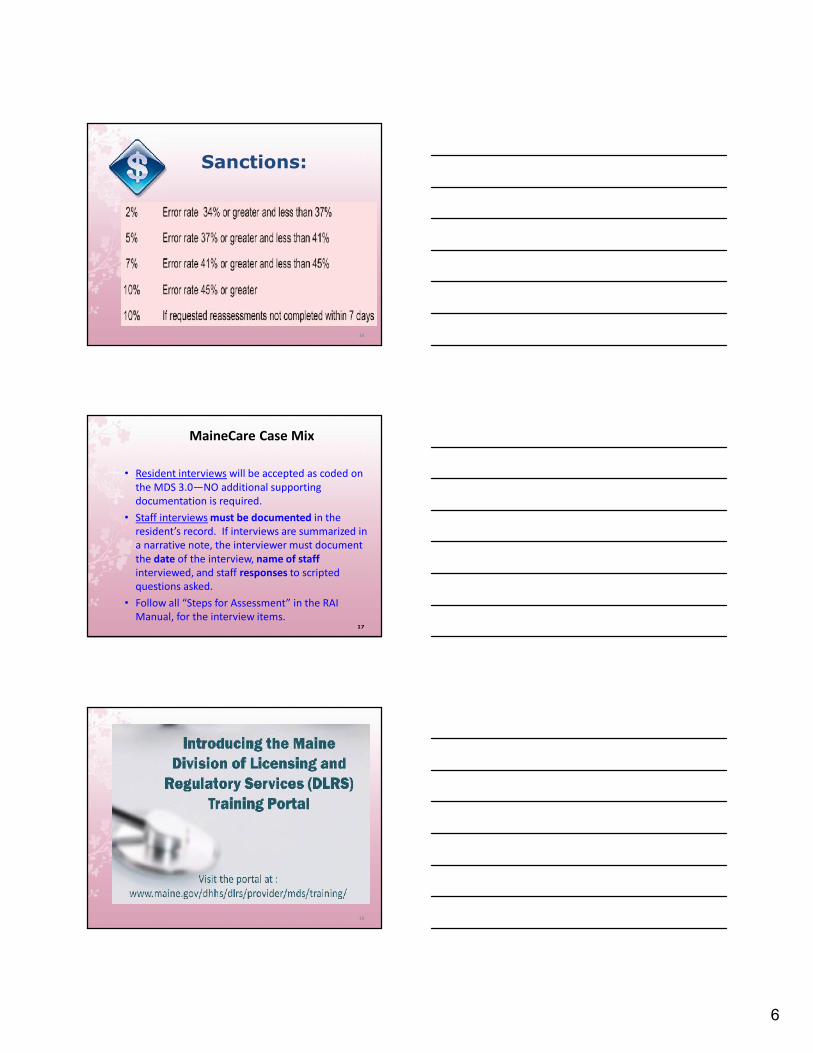
Sanctions:
MaineCare Case Mix
• Resident interviews will be accepted as coded onthe MDS 3.0—NO additional supportingdocumentation is required.• Staff interviews must be documented in the
resident’s record. If interviews are summarized ina narrative note, the interviewer must documentthe date of the interview, name of staffinterviewed, and staff responses to scriptedquestions asked.• Follow all “Steps for Assessment” in the RAI
Manual, for the interview items.17
18
7
MDS 3.0Long Term Care Facility
Resident Assessment Instrument (RAI)User’s Manual
Chapter 2Effective Oct 2014
19
MDS 3.0
Long Term Care FacilityResident Assessment Instrument (RAI)
User’s Manual
Chapter 3Effective Oct 2014
20
Requirement for the 3.0
• Initial and periodic assessments for alltheir residents residing in the facility for14 or more days.
• This includes hospice, respite, andspecial populations such as Pediatric andPsychiatric.
21
8
Responsibility of NF forReproducing/Maintaining 3.0
Federal regulatory requirements at42CFR483.20(d) requires NF tomaintain all resident assessmentscompleted within the previous 15months in the resident’s activeclinical record
22
23
Responsibilities of NF forReproducing/Maintaining 3.0
Nursing Homes may:
1. Use electronic signatures for the MDS2. Maintain the MDS electronically3. Maintain the MDS and Care Plans in a
separate binder in a location that iseasily and readily accessible to staff,Surveyors, CMS etc.
24
The Alphabet Soup of MDS
OBRA = Omnibus Budget ReconciliationActPPS = Prospective Payment SystemOMRA = Other Medicare RequiredAssessments (SOT, EOT, COT)ARD = Assessment Reference Date
9
25
Section A
Intent: The intent of this section is to obtainkey information to uniquely identify eachresident, the home in which he or she resides,and the reasons for assessment.
26
Coding Section AA0050 - Type of Record
• Code 1 for a new record that has not beenpreviously submitted and accepted in the QIESASAP system
• Code 2 to modify the MDS items for a record thathas been submitted and accepted in the QIES ASAPsystem
• Code 3 to inactivate a record that already has beensubmitted and accepted in the QIES ASAP system
27
10
33
Section AA0310 Purpose
Documents the reason for completingthe assessment
Identifies the required assessmentcontent information (item set)
28
Section AA0310A Federal OBRA Reason for Assessment
01. Admission02. Quarterly03. Annual04. Significant change in status05. Significant correction to prior comprehensive06. Significant correction to prior quarterly99. Not OBRA required
2929
Significant Change Criteria
• MAJOR change
• Not Self-limiting
• Impacts 2 or more areas ofdecline/improvement (MDS 3.0 RAImanual, pgs. 2-20 through 2-27)
• Requires IDT review and/or revisionof Care Plan
30
11
31
A0310A Hospice Benefit
• Electing or revoking the hospice benefitrequires a significant change in status assessment
31
Significant ErrorSignificant Error – is an error in an assessment
where:1. The resident’s overall clinical status is not
accurately represented (i.e., miscoded) onthe erroneous assessment; and
2. The error has not been corrected viasubmission of a more recent assessment.
32
Assessment Scheduling
33
12
34
Section AA0310B PPS Assessment
Includes scheduled and unscheduled assessments
Medicare PPS Assessments
5 day14 day30 day60 day90 dayReadmission/ReturnSCSASCPAStart of Therapy (SOT)End of Therapy (EOT)Both Start and End of TherapyChange of Therapy (COT)
35
PPS Scheduled Assessments fora Medicare Part A Stay
PPS Unscheduled, OMRA used for aMedicare Part A Stay
36
Coding Section AA0310C PPS Other Medicare Required Assessment - OMRA
Indicates whether the assessment is related totherapy services
Complete this item for all assessments0. Not an OMRA assessment1. Start of Therapy2. End of Therapy when ARD is 1 - 3 days after last dayof therapy services3. Start and End of Therapy4. Change of Therapy Assessment
36
13
37
Section AA0310E Type of Assessment
Is This Assessment the First Assessment(OBRA, PPS, or Discharge) since the MostRecent Admission/Entry or Reentry?
Complete this item for all assessments
37
38
Coding Section AA0310F Entry/ Discharge Reporting
01. Entry tracking record10. Discharge assessment – return not
anticipated11. Discharge assessment – return
anticipated12. Death in facility tracking record99. None of the above
38
Coding Section AA0310G Type of Discharge
Discharge refers to the date a resident leavesthe facility for anything other than atemporary LOA.
A discharge assessment is required for:1. Discharge return not anticipated2. Discharge return anticipated
39
14
40
OBRAAssessment
Schedule AfterDischarge Return
Anticipated
MDS 3.0 Update for 10/1/14
A0410. Unit Certification or LicensureDesignation
42
Section AResident Data
A0500 through A1300Check and doublecheck the accuracyof the name and allnumbers - socialsecurity, Medicareand MaineCarenumbers, Date ofBirth
15
Section AA1500 PASRR/ Medicaid
All individuals admitted to Medicaidcertified NFs must complete a Level IPASRR
If the Level I screen is positive for knownor suspected mental illness, intellectualdisability, developmental disability, or“other related conditions,” a Level IIevaluation is performed
4343
Section AA1510- Level II Preadmission Screening
and Resident Review (PASRR) Conditions
Complete only if at A0310A, Type ofAssessment, you have coded• 01 admission;• 03 annual;• 04 significant change; or• 05 significant correction to prior
comprehensive assessment
44
Section AA1550- Level II Preadmission Screening and
• Designates the end of the look-back periodso that all assessment items refer to theresident’s status during the same period oftime.• Anything that happens after the ARD will
not be captured on that MDS.• The look-back period includes observations
and events through the end of the day(midnight) of the ARD.
48
17
Section BHearing, Speech, and Vision
Intent: The intent of items in thissection is to document the resident’sability to hear (with assistive hearingdevices, if they are used), understand,and communicate with others andwhether the resident experiences visuallimitations or difficulties related todiseases common in aged persons.
49
Section BB0100: ComatoseB0200: Ability to Hear (with hearing aid if normally used)
B0300: Hearing AidB0600: Speech ClarityB0700: Makes Self UnderstoodB0800: Ability to Understand OthersB1000: Vision (with adequate light)
B1200: Corrective Lenses
50
Section CCognitive Patterns
51
Intent: The items in this sectionare intended to determine theresident’s attention, orientationand ability to register and recallnew information. These items arecrucial factors in many care-planning decisions.
18
Section CC0100
Should the Brief Interview for Mental Status (BIMS) beconducted???
Code 0, no: if the interview should not be attempted becausethe resident is rarely/never understood, cannot respondverbally or in writing, or an interpreter is needed but notavailable. Skip to C0700, Staff Assessment of Mental Status.
Code 1, yes: if the interview should be attempted because theresident is at least sometimes understood verbally or inwriting, and if an interpreter is needed, one is available.
52
Section C
C0600: Should the staff assessment be conducted?
C0700-C1000 Staff assessment:C0700 Short-Term MemoryC0800 Long-Term MemoryC0900 Memory/Recall AbilityC1000 Cognitive Skills for Daily Decision Making
C1300 Signs and Symptoms of DeliriumC1600 Acute Onset Mental Status Change
56
Section DMood
57
Intent: The items in this section address mood distress,a serious condition that is underdiagnosed andundertreated in the nursing home and is associatedwith significant morbidity. It is particularly important toidentify signs and symptoms of mood distress amongnursing home residents because these signs andsymptoms can be treatable.
20
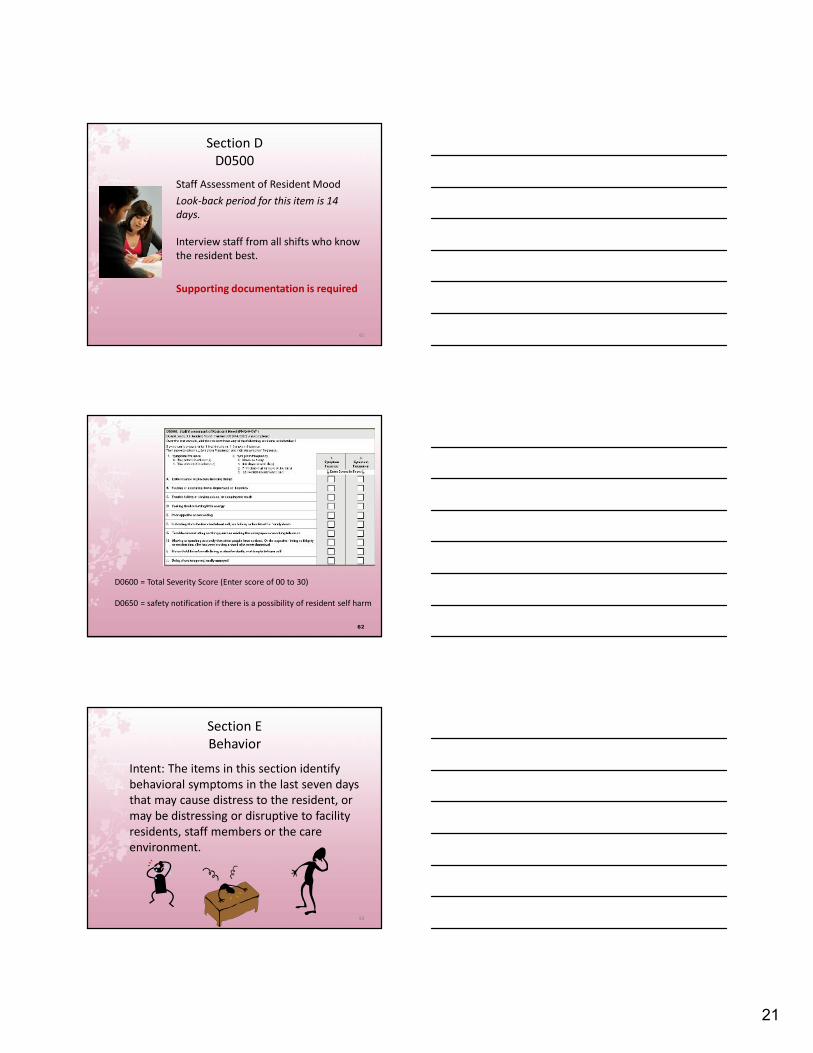
Section DD0100: Should Resident Mood InterviewBe Conducted?
D0300 Total Severity ScoreA summary of the frequency scores thatindicates the extent of potentialdepression symptoms. The score does notdiagnose a mood disorder, but provides astandard of communication with cliniciansand mental health specialists.
Total score must be between 00 and 27
60
21
Section DD0500
Staff Assessment of Resident MoodLook-back period for this item is 14days.
Interview staff from all shifts who knowthe resident best.
Supporting documentation is required
61
D0600 = Total Severity Score (Enter score of 00 to 30)
D0650 = safety notification if there is a possibility of resident self harm
62
Section EBehavior
Intent: The items in this section identifybehavioral symptoms in the last seven daysthat may cause distress to the resident, ormay be distressing or disruptive to facilityresidents, staff members or the careenvironment.
E0200A Physical behaviorsE0200B Verbal behaviorsE0200C Other behaviors
E0800 Rejected care
E0900 Wandered64
Section EE0200
65
E0300: Overall Presence of Behavioral SymptomsE0500: Impact on ResidentE0600: Impact on Others
Section EE0800 and E0900
E0800: Rejection of Care – Presence & FrequencyE0900: Wandering – Presence & Frequency
E1000: Wandering – ImpactE1000A Risk to SelfE1000B Intrusion on others
E1100: Change in Behavior or Other Symptoms66
23
Section FPreferences for Customary Routine and Activities
Intent: The intent of items in this section is to obtaininformation regarding the resident’s preferences for hisor her daily routine and activities.
67
Section GFunctional Status
Intent: Items in this section assess the needfor assistance with activities of daily living(ADLs), altered gait and balance, anddecreased range of motion.
1. When an activity occurs 3 or more times at anyone level, code that level.
2. When an activity occurs 3 or more times atmultiple levels, follow the “Rule of 3” .
Exceptions to the Rule of 3:0 Independent4 Total Dependence7 Activity occurred one or two times8 Activity did not occur
Section GG0120: Bathing
A. Self-PerformanceB. Support
G0300: Balance During Transitions and WalkingG0400: Functional Limitation in Range ofMotion
A. Upper ExtremityB. Lower Extremity
G0600: Mobility Devices (check all that apply)G0900: Functional Rehabilitation Potential
72
25
Section HBladder and Bowel
Intent: The intent of the items in this sectionis to gather information on the use of boweland bladder appliances, the use of andresponse to urinary toileting programs,urinary and bowel continence, boweltraining programs, and bowel patterns.
73
Section HH0100: AppliancesH0200: Urinary Toileting Program
A: Trial of a toileting program?B: Response to trialC: Current toileting program or trial
H0200C and H0500 arepart of the RestorativeNursing Program andwill be reviewed withSection O
75
26
Section IActive Diagnoses
Intent: The items in this section are intended to codediseases that have a direct relationship to the resident’scurrent functional status, cognitive status, mood orbehavior status, medical treatments, nursingmonitoring, or risk of death. One of the importantfunctions of the MDS assessment is to generate anupdated, accurate picture of the resident’s currenthealth status.
76
Section I Active Diagnoses
1. Identify diagnoses in the last 60 days– physician-documented diagnoses
2. Determine status of diagnosis– 7-day look-back period,
– Active diagnoses have a direct relationship tothe resident’s functional, cognitive, mood orbehavior status, medical treatments or nursingmonitoring
– Only active diagnoses should be coded
7777
78
I2300 Urinary Tract Infections
The look-back period for UTI (I2300) differs fromother items– Look-back period to determine an active diagnosis of a
UTI is 30 days
Code for a UTI only if all of the following criteriaare met:– Diagnosis of a UTI in last 30 days
– Signs and symptoms attributed to UTI
– Positive test, study, or procedure confirming a UTI
– Medication or treatment for UTI in the last 30 days
27
DIAGNOSES (Case Mix Items)
I2000 – PneumoniaI2100 - SepticemiaI2900 - Diabetes (If N0300 = 7 and O0700 = 2 or more)
Section JIntent: The intent of the items in this section isto document a number of health conditionsthat impact the resident’s functional statusand quality of life. The items include anassessment of pain which uses an interviewwith the resident or staff if the resident isunable to participate. The pain items assessthe presence of pain, pain frequency, effect onfunction, intensity, management and control.Other items in the section assess dyspnea,tobacco use, prognosis, problem conditions,and falls.
80
Section JPain Assessment
J0100 Pain Management (5-day look-back)J0200: Should Pain Assessment Interview beConducted?Pain Interview: J0300 – J0600J0700: Should the Staff Assessment for Pain beConducted?J0800-J0850: Staff Assessment for Pain
81
28
Section JOther Health Conditions
J1100 Shortness of BreathJ1300 Current Tobacco UseJ1400 Prognosis
82
Section JProblem Conditions
J1550:A. FeverB. VomitingC. DehydratedD. Internal BleedingZ. None of the above
Seven (7) day look-back period
83
Section JHealth Conditions
J1700 Fall HistoryJ1800 Falls since Admission/EntryJ1900 Number of Falls since Admission
84
29
Section KSwallowing/Nutritional Status
Intent: The items in this section areintended to assess the many conditionsthat could affect the resident’s ability tomaintain adequate nutrition and hydration.This section covers swallowing disorders,height and weight, weight loss, andnutritional approaches. The assessorshould collaborate with the dietitian anddietary staff to ensure that items in thissection have been assessed and calculatedaccurately.
85
Section KWeight Loss/Gain
K0100: Swallowing disorderK0200: Height and WeightK0300: Weight LossK0310: Weight gain
86
Section KNutritional Approaches
K0510: ApproachesA. Parenteral / IV FeedingB. Feeding TubeC. Mechanically Altered DietD. Therapeutic DietZ. None of the above
87
30
K0510 Assessment Guidelines
The following items are NOT coded in K0510A: IV medications IV fluids administered as a routine part of
an operative or diagnostic procedure orrecovery room stay IV fluids administered solely as flushes Parenteral/IV fluids administered in
conjunction with chemotherapy ordialysis
RAI Manual pages K-10 through K-12
8888
K0710A Percent Intake by Artificial Route
89
If the resident took no food or fluids by mouth ortook just sips of fluid, stop here and code 3, 51% ormore.
If the resident had more substantial oral intakethan this, consult with the dietician.
90
K0710B Average Fluid Intake per Day byIV or Tube Feeding
Code for the average number of cc per dayof fluid the resident received via IV or tubefeeding. Record what was actually receivedby the resident, not what was ordered.
• Code 1: 500 cc/day or less• Code 2: 501 cc/day or more
K0710A and B (column 3) are paymentitems for residents receiving nutrition viaIV or Tube Feeding
31
Section L
Intent: This item is intended to record anydental problems present in the 7-day look-back period.
91
Section MSkin Conditions
Intent: The items in this section document therisk, presence, appearance, and change ofpressure ulcers. This section also notes otherskin ulcers, wounds, or lesions, anddocuments some treatment categories relatedto skin injury or avoiding injury. It isimperative to determine the etiology of allwounds and lesions, as this will determineand direct the proper treatment andmanagement of the wound.
92
Section M
M0100: Determination of Pressure Ulcer RiskM0150: Risk of Pressure UlcersM0210: Unhealed Pressure Ulcer(s)
93
32
Section MM0300 Unhealed Pressure Ulcers
M0300A: Number of Stage 1M0300B: Number of Stage 2
number present on admissiondate of oldest stage 2 if known
M0300C: Number of Stage 3number present on admission
M0300D: Number of Stage 4number present on admission
94
Section MM0300 Unhealed Pressure Ulcers
M0300E: Unstageable Related to Non-removable dressing/device
number present on admissionM0300F: Unstageable – slough and/or eschar
number present on admissionM0300G: Unstageable – Deep Tissue
number present on admission
95
PRESSURE ULCERS(Guidelines)
Do not reverse stage• “If the pressure ulcer has ever been classified at
a deeper stage than what is observed now, itshould continue to be classified at the deeperstage”
• Determine the deepest anatomical stage of eachpressure ulcer
• Enter number of pressure ulcers for each stage• Pressure Ulcers are Case Mix items– 2+ Treatments required
96
33
Section M
M0610: Dimensions of Unhealed Stage 3or 4 or EscharM0700: Most Severe Tissue Type for anyUlcerM0800: Worsening Pressure Ulcer StatusM0900: Healed Pressure UlcersM1030: Number of Venous and ArterialUlcers
97
Section MM1040 Other Ulcers, Wounds, and Skin Problems
98
99
M1200 Skin and Ulcer Treatments
A. Pressure reducing device for chairB. Pressure reducing device for bed• do not include egg crate cushions of any type,
donut or ring devices for chairsC. Turning/repositioning program• Specific approaches for changing resident’s position
and re-aligning the body• Specific intervention and frequency• Requires supporting documentation of monitoring
and periodic evaluationD. Nutrition and hydration
34
M1200 Skin and Ulcer Treatments
E. Pressure Ulcer CareF. Surgical Wound CareG. Non-surgical Dressing (other than feet)
Do NOT include BandaidsE. Ointments/medications (other than
feet)F. Dressings to feetZ. None of the above
100
Section NMedications
Intent: The intent of the items in thissection is to record the number of days,during the last 7 days (or sinceadmission/entry or reentry if less than 7days) that any type of injection(subcutaneous, intramuscular orintradermal), insulin, and/or selectmedications were received by theresident.
101
Section NINJECTIONS
N0300Record the number of days (during the 7-day look-back period) that the residentreceived any type of medication, antigen,vaccine, etc., by subcutaneous,intramuscular, or intradermal injection.
Insulin injections are counted in thisitem as well as in Item N0350.
102
35
Section NMedications
N0350 Insulin: Not a payment item forRUG III (MaineCare).
A. Insulin Injections administeredB. Orders for insulin
Intent: The intent of the items in thissection is to identify any specialtreatments, procedures, and programsthat the resident received during thespecified time periods.
105
36
Section OSpecial Treatments, Procedures, and Programs
Individual minutesConcurrent minutesGroup minutesCo-treatment minutesNumber of DaysStart dateEnd date 108
Section OSpecial Treatments, Procedures, and Programs
37
O0400D Respiratory TherapyTotal minutesDays therapy was administered
at least 15 minutesO0400E Psychological TherapyO0400F Recreational Therapy
109
Section OSpecial Treatments, Procedures, and Programs
O0420 Distinct Days of TherapyO0450 Resumption of Therapy
110
Section OSpecial Treatments, Procedures, and Programs
111
Section ORestorative Nursing Programs
38
Nursing interventions that promote theresident’s ability to adapt and adjust toliving as independently and safely aspossible.
Section ORestorative Nursing Programs
• Measureable objectives and interventions• Periodic evaluation by a licensed nurse• CNAs must be trained in the techniques• Does not require a physician’s order, but a licensed
nurse must supervise the activities
112
• Nursing staff are responsible forcoordination and supervision• Does not include groups with more than 4
residents• Code number of days a resident received
15 minutes or more in each category• Remember that persons with dementia
learn skills best through repetition thatoccurs multiple times per day.
113
Section ORestorative Nursing Programs
114
H0200C Current toileting programAn individualized, resident-centeredtoileting program may decrease or preventurinary incontinence, minimizing oravoiding the negative consequences ofincontinence.
The look-back period for this item is sincethe most recent admission/entry or reentryor since urinary incontinence was firstnoted within the facility.
Section ORestorative Nursing Programs
39
115
H0500 Bowel Training ProgramThree requirements:
• Implementation of an individualized,resident-specific bowel toileting program.• Evidence that the program was
communicated to staff and residentthrough care plans, flow sheets, etc.• Documentation of the response to the
Over the last 14 days, on how many daysdid the physician examine the resident?
Examinations can occur in the facility orin the physician’s office.
Do not include:
• Examinations that occurred prior toadmission/readmission to the facility• Examinations that occurred during an
ER visit or hospital observation stay116
O0700 Physician Order Change DaysAssessment Guidelines
Over the last 14 days, on how manydays did the physician change theresident’s orders?
Do not include the following:• Admission or re-admission orders• Renewal of an existing order• Clarifying orders without changes• Orders prior to the date of admission• Sliding scale dosage schedule• Activation of a PRN order
117
40
Section PRestraints
Intent: The intent of this section is torecord the frequency over the 7-day look-back period that the resident wasrestrained by any of the listed devices atany time during the day or night.Assessors will evaluate whether or not adevice meets the definition of a physicalrestraint and code only the devices thatmeet the definition in the appropriatecategories of Item P0100.
118
119
Section PRestraints
Section QParticipation in Assessment and Goal Setting
Intent: The items in this section areintended to record the participation andexpectations of the resident, familymembers, or significant other(s) in theassessment, and to understand theresident’s overall goals. Discharge planningfollow-up is already a regulatoryrequirement (CFR 483.20 (i)(3)).Interviewing the resident or designatedindividuals places the resident or theirfamily at the center of decision-making.
120
41
Q0100 Participation in Assessment:Who participated??
Whenever possible, the residentshould be actively involved-except inunusual circumstances such as if theindividual is unable to understand theproceedings or is comatose.
121
Section QParticipation in Assessment and Goal Setting
Q0300 Residents Overall Expectation• Overall expectations• Information sourceQ0400 Discharge PlanQ0490 Preference to Avoid Being Asked
Question Q0500B
122
Section QParticipation in Assessment and Goal Setting
Q0500B Return to Community
123
Section QParticipation in Assessment and Goal Setting
The goal of follow-up action is to initiate andmaintain collaboration between the nursinghome and the local contact agency to supportthe resident’s expressed interest in beingtransitioned to community living.
42
Q0550A, Does the resident, (or family or significantother or guardian or legally authorized representativeif resident is unable to respond) want to be askedabout returning to the community on all assessments?(Rather than only on comprehensive assessments.)
Q0500B, what is the source of the information?
124
Section QParticipation in Assessment and Goal Setting
125
Section QParticipation in Assessment and Goal Setting
Who is the Local Contact Agency for Maine?Long Term Care Ombudsman Program
MDS 3.0 Update for 10/1/14
Section SThis section applies to the State of Maine
specific data requirements.
S0120 Residence Prior to AdmissionEnter the zip code of the community
address where the resident last residedprior to nursing facility admission.
126
43
MDS 3.0 Update for 10/1/14
S0170. Advanced Directive
127
MDS 3.0 Update for 10/1/14
S0510. PASRR Level I Screening
Note the skip patterns
128
MDS 3.0 Update for 10/1/14
S0511. PASRR Level I Date:(Complete only if S0510 = 1)
129
44
MDS 3.0 Update for 10/1/14
S0513. PASRR Level I ScreeningOutcome
130
MDS 3.0 Update for 10/1/14
S3300. Weight-based EquipmentNeed
131
MDS 3.0 Update for 10/1/14
S3305. Requirements for Care,Specifically related to Weight
132
45
MDS 3.0 Update for 10/1/14
S6020. Specialized needs specificallyrelated to a resident’s need for a
S8010 Payment Source – To determinepayment source(s) that covers the dailyper diem or ancillary services for theresident’s stay in the nursing facility overthe last 30 days.• C3 – MaineCare per diem. Do not
check if MaineCare is pending• G3 MaineCare pays Medicare Co-pay
S8099 None of the above139
S8510. MaineCare TherapeuticLeave Days
MDS 3.0 Update for 10/1/14
140
Leave of Absence, or LOA, refers to:
• Temporary home visit• Temporary therapeutic leave• Hospital observation stay of
less than 24h where resident isnot admitted to hospital
141
48
S8512. MaineCare Hospital Bed-HoldDays
MDS 3.0 Update for 10/1/14
142
Section VCare Area Assessment Summary
CAAs
Intent: The MDS does not constitute acomprehensive assessment. Rather, it is apreliminary assessment to identify potentialresident problems, strengths, andpreferences.
… and CATS
143
V0100 Items from Most Recent Prior OBRA or PPSAssessment• Reason for assessment (A0310A and/or A0310B)• Prior ARD (A2300)• Prior BIMS score (C0500)• Prior PHQ-9 (C0300 or C0600)
V0200: CAAs and Care Planning
144
Section VCare Area Assessment Summary
49
Section ZAssessment Administration
Intent: The intent of the items in thissection is to provide billing information andsignatures of persons completing theassessment.
145
Section ZAssessment Administration
Majority of this section is completed by yoursoftware.Z0100 Medicare Part A BillingZ0150 Medicare Part A Non-TherapyZ0200 State Medicaid BillingZ0250 Alternate State Medicaid BillingZ0300 Insurance Billing
146
Z0400 Signature of Persons Completing the Assessmentor Entry/Death Reporting.I certify that the accompanying information accurately reflects residentassessment information for this resident and that I collected or coordinatedcollection of this information on the dates specified. To the best of myknowledge, this information was collected in accordance with applicableMedicare and Medicaid requirements. I understand that this information isused as a basis for ensuring that residents receive appropriate and qualitycare, and as a basis for payment from federal funds. I further understandthat payment of such federal funds and continued participation in thegovernment-funded health care programs is conditioned on the accuracyand truthfulness of this information, and that I may be personally subject toor may subject my organization to substantial criminal, civil, and/oradministrative penalties for submitting false information. I also certify that Iam authorized to submit this information by this facility on its behalf.
147
Section ZAssessment Administration
50
Z0400 Signature of Persons Completing theAssessment or Entry/Death Reporting
Z0500 Signature of RN AssessmentCoordinator Verifying AssessmentCompletion
148
Section ZAssessment Administration
Section XCorrection Request
Intent: The purpose of Section X is to identify anMDS record to be modified or inactivated.Section X is only completed if Item A0050, Typeof Record, is coded a 2 (Modify existing record)or a 3 (Inactivate existing record). In Section X,the facility must reproduce the informationEXACTLY as it appeared on the existing erroneousrecord, even if the information is incorrect. Thisinformation is necessary to locate the existingrecord in the National MDS Database.
149
Section XCorrection Request
A modification request is used to correct aQIES ASAP record containing incorrect MDSitem values due to:• transcription errors,• data entry errors,• software product errors,• item coding errors, and/or• other error requiring modification
150
51
Section XCorrection Request
An inactivation request is used to move anexisting record in the QIES ASAP databasefrom the active file to an archive (historyfile) so that it will not be used for reportingpurposes.
151
Section XCorrection Request: Manual Deletion
152
A Manual Deletion Request is required onlyin the following three cases:1. Item A0410 Submission Requirement is
incorrect.2. Inappropriate submission of a test
record as a production record.3. Record was submitted for the wrong
facility.
Section XCorrection Request
X0150 Type of ProviderX0200 Name of ResidentX0300 GenderX0400 Date of BirthX0500 Social Security NumberX0600 Type of AssessmentX0700 Date on existing record
153
52
X0800 Correction numberX0900 Reasons for ModificationX1050 Reasons for InactivationX1100 Name, Title, Signature, Attestation Date
154
Section XCorrection Request
RAI Manual Chapter 5Submission and Correction of MDS
5.1 Transmitting MDS Data:
The provider indicates the submission authorityfor a record in item A0410, SubmissionRequirement.5.2 Timeliness Criteria5.3 Validation Edits5.4 Additional Medicare SubmissionRequirements that Impact Billing Under SNF PPS