MEASUREMENT AND CONTROL OF BOWEL PRESSURE IN URETERO-COLIC ANASTOMOSIS1 By OWEN DANIEL, M.S., F.R.C.S., and M. L. SINGH, M.S., F.R.C.S. From the Royal Alexandra Hospitaf, Rhyl THE normal bladder is remarkable for its capacity for storing widely differing volumes of urine at a uniformly low pressure and the upper urinary tract for its susceptibility to damage from even slight back pressure. It follows that the relationship between the maximum safe working pressure of the upper urinary tract and pressure within the sigmoid colon is worthy of careful assessment if transplantation of the ureters is under consideration. Measurement of Bladder Pressure.-It is easy to measure pressure within the urinary bladder by means of a catheter connected to a simple manometer or any other recording device such as an electrical transducer. TABLE Bladder Pressure in Retention of Urine 61 82 I I I I h Cause ! ReteqCtion B.P.H. Ca. P. B.P.H. 1 B.P.H. Ca. P. 1 B.P.H. ' Duration I No Yes I 1 12 hours 6-8 weeks 1 :kht only 6-8 weeks Day and night Yes 8 weeks Night only No Blood Urea mg "/b 33 93 31 40 41 75 I.V.P. I Pressure cm/HzO 1 ... ... Normal Hydronephrosis H ydronephrosis Hydronephrosis 86 69 32 21-36 19-38 20-22 B.P.H.-Benign Prostatic Hypertrophy. Ca. P.-Carcinoma of Prostate. Pressure varies in the normal bladder but is generally very little higher than that within the abdominal cavity except in the comparatively short period preceding and during the act of voiding when waves of activity appear (Denny-Brown and Robertson, 1933). The bladder pressure recorded in six men suffering from retention of urine is shown in the Table. Acute retention of under 14 hours' duration was not accompanied by elevation of blood urea or subsequent pyelographic evidence of hydronephrosis although bladder pressure ranged as high as 86 cm. of water. Chronic retention with overflow of six to eight weeks' duration proved damaging to renal function as shown by raised blood urea and the appearance of hydronephrosis (Fig. l), although bladder pressure ranged only from 20 to 38 cm. of water. In one patient in acute retention pressure within the bladder remained almost constant throughout the period of observation, showing only slight rhythmical variation of the same frequency as respiration or the arterial pulse (Fig. 2). In another man in chronic retention the tracing showed slow waves rising from 14 to 28 mm. of Hg every 90 seconds and accompanied by a painful desire to micturate (Fig. 3). 1 Read at the Twenty-fourth Annual Meeting of the British Association of Urological Surgeons at Cardiff, June 1968. 32
Transcript
MEASUREMENT AND CONTROL OF BOWEL PRESSURE IN URETERO-COLIC ANASTOMOSIS1
By OWEN DANIEL, M.S., F.R.C.S., and M. L. SINGH, M.S., F.R.C.S. From the Royal Alexandra Hospitaf, Rhyl
THE normal bladder is remarkable for its capacity for storing widely differing volumes of urine at a uniformly low pressure and the upper urinary tract for its susceptibility to damage from even slight back pressure. I t follows that the relationship between the maximum safe working pressure of the upper urinary tract and pressure within the sigmoid colon is worthy of careful assessment if transplantation of the ureters is under consideration.
Measurement of Bladder Pressure.-It is easy to measure pressure within the urinary bladder by means of a catheter connected to a simple manometer or any other recording device such as an electrical transducer.
TABLE Bladder Pressure in Retention of Urine
61
82
I I I I h Cause ! ReteqCtion
B.P.H. Ca. P. B.P.H. 1 B.P.H. Ca. P. 1 B.P.H.
' Duration
I No Yes
I 1 12 hours 6-8 weeks 1 :kht only 6-8 weeks Day and night Yes 8 weeks Night only No
Blood Urea
mg "/b
33 93 31 40 41 75
I.V.P. I Pressure cm/HzO 1
...
... Normal Hydronephrosis H ydronephrosis Hydronephrosis
86 69 32 21-36 19-38 20-22
B.P.H.-Benign Prostatic Hypertrophy. Ca. P.-Carcinoma of Prostate.
Pressure varies in the normal bladder but is generally very little higher than that within the abdominal cavity except in the comparatively short period preceding and during the act of voiding when waves of activity appear (Denny-Brown and Robertson, 1933).
The bladder pressure recorded in six men suffering from retention of urine is shown in the Table. Acute retention of under 14 hours' duration was not accompanied by elevation of blood urea or subsequent pyelographic evidence of hydronephrosis although bladder pressure ranged as high as 86 cm. of water.
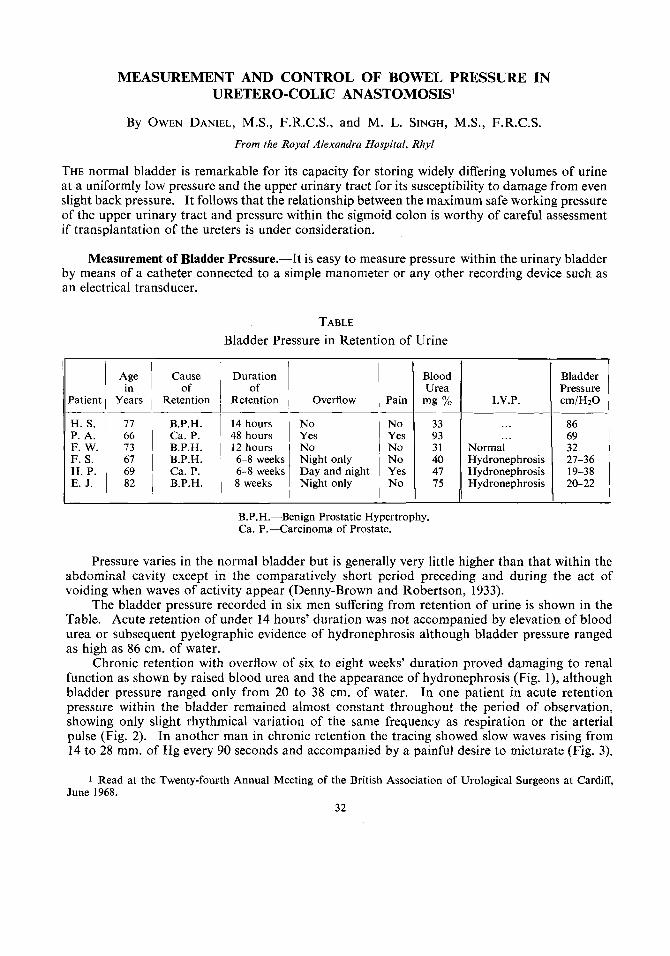
Chronic retention with overflow of six to eight weeks' duration proved damaging to renal function as shown by raised blood urea and the appearance of hydronephrosis (Fig. l), although bladder pressure ranged only from 20 to 38 cm. of water. In one patient in acute retention pressure within the bladder remained almost constant throughout the period of observation, showing only slight rhythmical variation of the same frequency as respiration or the arterial pulse (Fig. 2). In another man in chronic retention the tracing showed slow waves rising from 14 to 28 mm. of Hg every 90 seconds and accompanied by a painful desire to micturate (Fig. 3).
1 Read at the Twenty-fourth Annual Meeting of the British Association of Urological Surgeons at Cardiff, June 1968.
32
B O W E L P R E S S U R E I N U R E T E R O - C O L I C ANASTOMOSIS
FIG. 1 Tomograph of I.V.P. on E.J. showing hydronephrosis after eight weeks of chronic retention.
Residual urine, 30 oz. bladder pressure 20 to 22 cm. HzO.
33
FIG. 2 Bladder and rectal pressure simultaneously recorded after acute
retention of 12 hours’ duration. l c
34 B R I T I S H J O U R N A L OF U R O L O G Y
FIG. 3 Bladder and rectal pressure simultaneously recorded after 6 to 8 weeks chronic retention
with overflow.
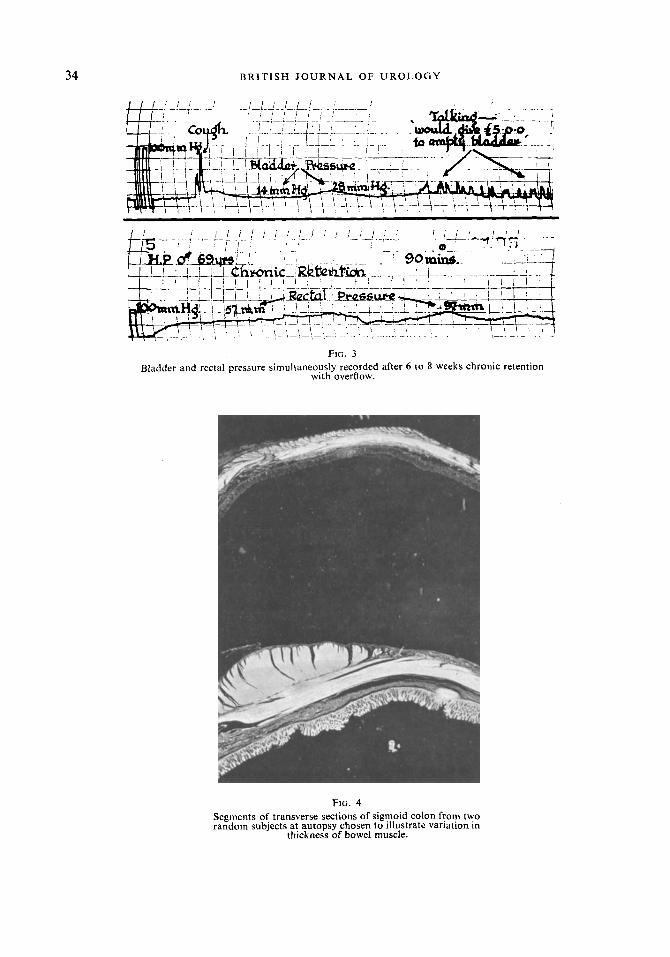
FIG. 4 Segments of transverse sections of sigmoid colon from two random subjects at autopsy chosen to illustrate variation in
thickness of bowel muscle.
B O W E L P R E S S U R E I N U R E T E R O - C O L I C A N A S T O M O S I S 35
It will be noted from Figures 1 and 3 that although chronic retention of urine was producing harmful effects on the kidneys, simultaneous pressure recordings from within the colon were substantially greater than those in the obstructed bladder.
Measurement of Colonic Pressure.-The earliest studies of the motility of the large bowel were based upon measurements made by balloon-kymographs, but such apparatus has been superseded by the system of electrical recording introduced by Brody and Quigley (1947). More recently radio-telemetry has also been used. Both the modern electrical and wireless methods, as well as the older balloon systems require expensive apparatus not normally found outside specialised research departments and also suffer from various other drawbacks. It is, however, possible to make valuable deductions concerning colonic activity either by noting the thickness of the bowel muscle at the time of operation or by means of simple pre-operative flow studies using apparatus readily available.
Laparotomy under general anasthesia usually reveals the colon as a flaccid, inert tube. Only occasionally will waves of spontaneous contraction be observed, but during these the bowel ma) become quite rigid and firm so that no observer could doubt the presence of very high intrd-luminal pressure, indeed, in this condition, diverticula, if present, will bulge tensely from the bowel wall and the mechanism of their formation and occasional rupture can readily be appreciated. Although it is rare to observe activity in the gut of anzsthetised subjects it is common knowledge that there is great individual variation in thickness of the bowel wall. In some individuals the muscle layers are so thin as to be barely noticeable, in others the muscle forms firm, greyish white layers up to 3 or 4 mm. thick (Fig. 4). Experience has shown that thin, atrophic-looking bowel generates low intra-luminal pressure and that thick muscular bowel is capdble of generating very high pressure. The appearance of multiple colonic diverticula, espccially with evidence of previous diverticulitis is further strong evidence of potentially high bowel pressure. Assessment of colonic activity by naked eye observation is however crude, and accurate measurement is possible by studying the rate of flow of water into the bowel.
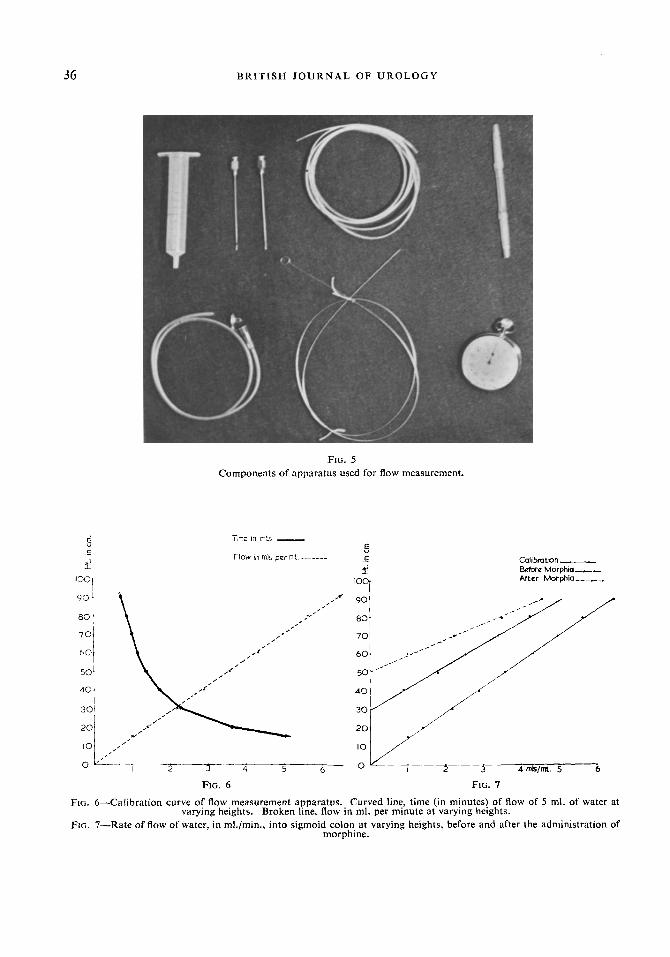
Apparatus and Method for Intra-colonic Flow Measurement.-The apparatus, shown in Figure 5 , comprises a metre ruler, the barrel of a 10-ml. disposable syringe, 150 cm. of polythene tubing of 1 mm. bore1 two 19 G intramuscular needles, a No. 9 Portex infant feeding tube2 with its rip cut so as to present a single, slightly oblique terminal opening, one double-ended or two single-ended Luer fitting tubular connections salvaged from a disposable plastic intravenous infusion set3 and a stop watch.
The intramuscular needles are inserted, one in each end of the long polythene tube into which they will make a comfortably tight fit. One of the needles is attached to the nozzle of the syringe and the other, through the appropriate connecting cannula, to the Portex infant feeding tube. The apparatus is filled with tap water taking great care to exclude air bubbles. The ruler and stop watch are then used to measure the time taken for 5 ml. of water to discharge with the syringe barrel at varying heights above the end of the tube. The results when plotted will show as in Figure 6 that flow varies according to height but is slow and very steady throughout. If time of flow is plotted against height the points will lie along an exponential curve, but if flow in millilitres per minute is plotted against height the points will lie along a straight line, starting from the intersection of the co-ordinates.
To measure intra-colonic pressure the infant feeding tube, stiffened with a lubricated stilette taken from a ureteric catheter, is introduced to the appropriate point through a sigmoidoscope,
FIG. 5 Components of apparatus used for flow measurement.
Calitmtron I_
Betore Morphm-,.- After Morphia ___.__.
- 2 - 5 - 4 5 4mkImt. 5 6
FIG. 6 FIG. 7 FIG. 6-Calibration curve of flow measurement apparatus. Curved line, time (in minutes) of flow of 5 ml. of water at
Fia. 7-Rate of flow of water, in ml./min., into sigmoid colon at varying heights, before and after the administration of morphine.
varying heights. Broken line. flow in ml. per minute at varying heights.
BOWEL PRESSURE I N URETERO-COLIC ANASTOMOSIS 37
secured by external strapping and rejoined to the syringe through the long tube. Again care is necessary to avoid the inclusion of bubbles. The patient is made comfortable and the end of the ruler held at a level corresponding closely with the estimated position of the orifice of the intra- colonic tube. The syringe barrel is raised until a steady flow is established and the time taken for 5 ml. of water to empty into the colon is measured with-the stop watch. Measurements are rtpeated at three or four higher levels and the results converted into flow in millilitres per minute and plotted against height (Fig. 7). The points will form a straight line intersecting the co-ordinate a t a level indicating the mean bowel pressure during the period of observation. The observations are repeated a few minutes following intravenous injection of 10 mg. of morphine sulphate and when the effect of morphine begins to wane 0.5 mg. of prostigmine is administered by injection and flow measurement repeated.
DISCUSSION
If it is accepted that bowel pressure exhibits wide individual variation (Daniel and Ram, 1965) consideration must be given to the possibility of corresponding variations in ureteral activity, which could potentiate or negate the effect of this variation on the results of uretero-colic mastomosis. The studies of Ross and his co-workers (1965, 1967) show that a pressure of 40 cm. of water is the average maximum pressure in the normal ureters at the height of contraction dnd between contractions the pressure is very much lower.
The observations reported above on the effects of bladder neck obstruction show that serious renal damage can follow chronic retention with overflow when bladder pressure is substantially less than that simultaneously recorded within the sigmoid colon. Clearly, in some men, uretero-colic anastomosis is potentially more damaging to renal function than unrelieved chronic overflow incontinence due to bladder neck obstruction.
The advantage of the simple flow measurement of intra-colonic pressure is that it provides a reliable method for pre-operative assessment of the suitability of an individual for uretero-colic anastomosis. Conventional electrical apparatus is expensive, complicated and difficult to handle as well as to maintain unless in regular, frequent use. Furthermore, although electrical recording apparatus gives a graphic representation of the waves of bowel activity, accurate deduction of mean bowel pressure from these tracings is extremely laborious or demands further expensive complicated apparatus, namely an analogue to digital converter coupled to an electronic computer (Misiewicz et al., 1968). Flow measurement provides from one simple graph a numerical value which expresses the summation of the highly complex waves of bowel activity which have occurred throughout the period of observation. This greatly facilitates classification of results and assessment of the effect of drugs or operative procedures.
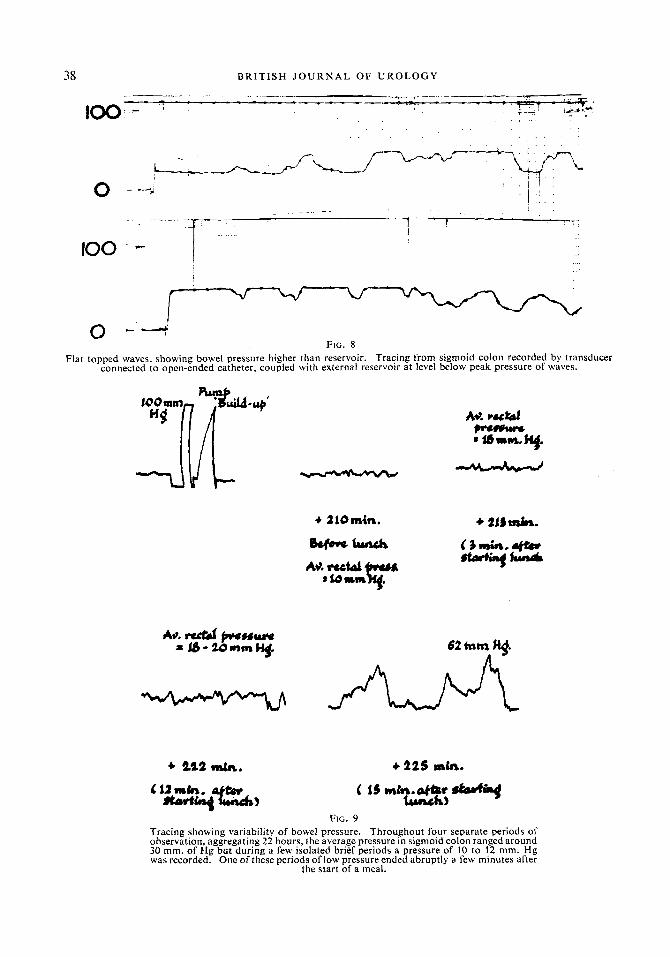
Measurement of flow rate can, with benefit, be combined with the use of an electrical transducer; gravity feed from the syringe barrel, held at various heights, taking the place of the motor driven syringe otherwise a necessary part of the transducer system. If this is done it will be found that when the reservoir is at levels below peak pressure the tracing will show waves with flat tops, indicating that flow has become intermittent, occurring only in the troughs of waves (Fig. 8). It is, however, most unusual for reverse flow to occur from the bowel back into the apparatus. Nevertheless, flow measurement loses its discriminatory value if the level of the reservoir is below peak bowel pressure and observations are valid only when the flow is uninterrupted. The presence of a small air bubble or any extraneous matter within the tube system will seriously affect flow rate. The specified tube dimensions have been selected, after considerable trial, as they provide a uniform slow flow within convenient ranges of height and time. Narrower tubes are readily blo ‘ked by invisible particles of dust or fluff. Doubling the diameter of the long tube wouldincr &r ase the flow rate 16101d.
The stop watch method is better than measurement of the flow over a predetermined time
38 B R I T I S H J O U R N A L OF U R O L O G Y
100 - ?
FIG. 8
connected to open-ended catheter, coupled with external reservoir at level below peak pressure of waves. Flat topped waves, showing bowel pressure higher than reservoir. Tracing from sigmoid colon recorded by transducer
+ Is2 dn. +22s lab.
FIG. 9 Tracing showing variability of bowel pressure. Throughout four separate periods of observation, aggregating 22 hours, the average pressure in sigmoid colon ranged around 30 mm. of Hg but during a few isolated brief periods a pressure of 10 to !2 mm. H g was recorded. One of these periods of low pressure ended abruptly a few minutes after
the start of a meal.
BOWEL P R E S S U R E I N U R E T E R O - C O L I C ANASTOMOSIS 39
interval signalled by an alarm apparatus (Daniel, 1965) and also obviates the use of a stop cock. When using the stop watch the syringe barrel is filled to above the top mark. The watch is started as the meniscus touches the top mark and stopped as it touches the 5 ml. mark. The stop Hatch is a precise instrument and with very little practice yields accurate results.
Bowel pressure is low at times in all individuals (Fig. 9). The important difference is that activity in some produces far greater intra-luminal pressure than in others. It is therefore essential not to rely on chance observation but always to include an estimate of intra-colonic pressure when the bowel is under maximal stimulation. As far as we are aware, the most reliable stimulants are morphine and prostigmine, but these drugs must not be given following uretero- colic anastomosis as they may then cause a severe attack of pyelo-nephritis.
It is clearly unwise to transplant ureters into bowel without preliminary estimation of activity, and if intra-colonic pressure is found to be higher than 20 cm. of water the operation should not be performed unless accompanied by a procedure known to reduce this pressure to a tolerable level. Sigmoid-myotomy is an effective method of reducing bowel pressure and can be wed in conjunction with uretero-colic anastomosis (Daniel and Ram, 1965). The only dis- advantage is an increased incidence of leakage, leading to post-operative fistula. To avoid this, punctures inadvertently made in the mucosa must be carefully closed with 000 catgut and the whole of the naked mucosa covered by a free peritoneal graft. The use of strips of peritoneum, 1.5 to 2.5 cm. wide, taken from the margin of the abdominal incision or paracolic gutter and used as free grafts to cover the myotomy incision, has greatly reduced the incidence of fistulous discharge. An external drain must also be brought from the site of the myotomy and uretero-colic anastomosis.
SUMMARY
The potential strength of bowel contraction can be roughly assessed during operation by judging the degree of hypertrophy of the colonic muscle. Accurate measurement of mean intra-luminal pressure can be effected with a simple flow meter. Simultaneous measurement of bowel and bladder pressure in chronic retention of urine shows that in some men the intra-colonic pressure greatly exceeds that within the obstructed bladder.
If intra-colonic pressure, following maximal stimulation with morphine and prostigmine, exceeds 20 cm. of water, uretero-colic anastomosis should be accompanied by sigmoid-myotomy.
We are grateful to the Research Committee of the Welsh Hospital Board for generous financial aid and support, and to Mr H. G. Crabtree for the photographs.
REFERENCES
BRODY, D. A., and QUIGLEY, J. P. (1947). Gastroenterology, 9, 570. DANIEL, 0. (1965). Irish J . med. Sci., 6, 415. DANIEL, O., and RAM R. S. (1965). Br. J . Urol., 37, 654, DENNY-BROWN, D., and ROBERTSON, E. G . (1933). Brain, 56, 149. MISIEWICZ, J. J., WALLER, SHEILA, L., HEALY, M. J. R., and PIPER, E. A. (1968). Gut, 9, 232. Ross, J. A., EDMOND, P., COULL, J., and SIMPSON, D. C. (1965). Br. J . Surg., 52, 617. Ross, J. A., EDMOND, P., COULL, J., and GRIFFITHS, J. (1967). J. Urol., 97, 449.