88
Medical Malpractice: How to Cope TIMOTHY CRAIG ALLEN, MD, JD THE UNIVERSITY OF MISSISSIPPI MEDICAL SCHOOL THE UNIVERSITY OF MISSISSIPPI MEDICAL CENTER
Medical Malpractice:
How to CopeTIMOTHY CRAIG ALLEN, MD, JD
THE UNIVERSITY OF MISSISSIPPI MEDICAL SCHOOL
THE UNIVERSITY OF MISSISSIPPI MEDICAL CENTER

Disclosures
Nothing herein should be considered legal advice
Nothing herein necessarily represents the opinions of the University of
Mississippi Medical Center or the College of American Pathologists
Goals to help pathologists cope
Understand the basics of medical malpractice law and discuss specific
legal criteria that determine medical liability
Understand the typical timeline of a medical malpractice lawsuit
Learn how to negotiate a deposition and avoid its pitfalls
Consider ways to minimize the emotional and psychological impact of a
medical malpractice lawsuit on the pathologist and the pathologist's
family

“…ideally…”
“…ideally, [a physician’s post-medical malpractice lawsuit] adaptations
lead to greater competence and a more satisfying personal and
professional life”
Charles SC. Coping with a medical malpractice suit. West J Med 2001 Jan; 174(1): 55-58.

“…predictable hazard…”
“…being sued for medical negligence is a predictable hazard of medical
practice in our times. Education of the sued physician about medical
malpractice stress is the key to dealing with the fear of litigation.”
Sanbar SS, Firestone MH. Medical malpractice stress syndrome. https://www.acep.org/uploadedFiles/ACEP/Professional_Development/Faculty_Development/Medical%20Malpractice%20Stress%20Syndrome%20article%20for%20web.pdf
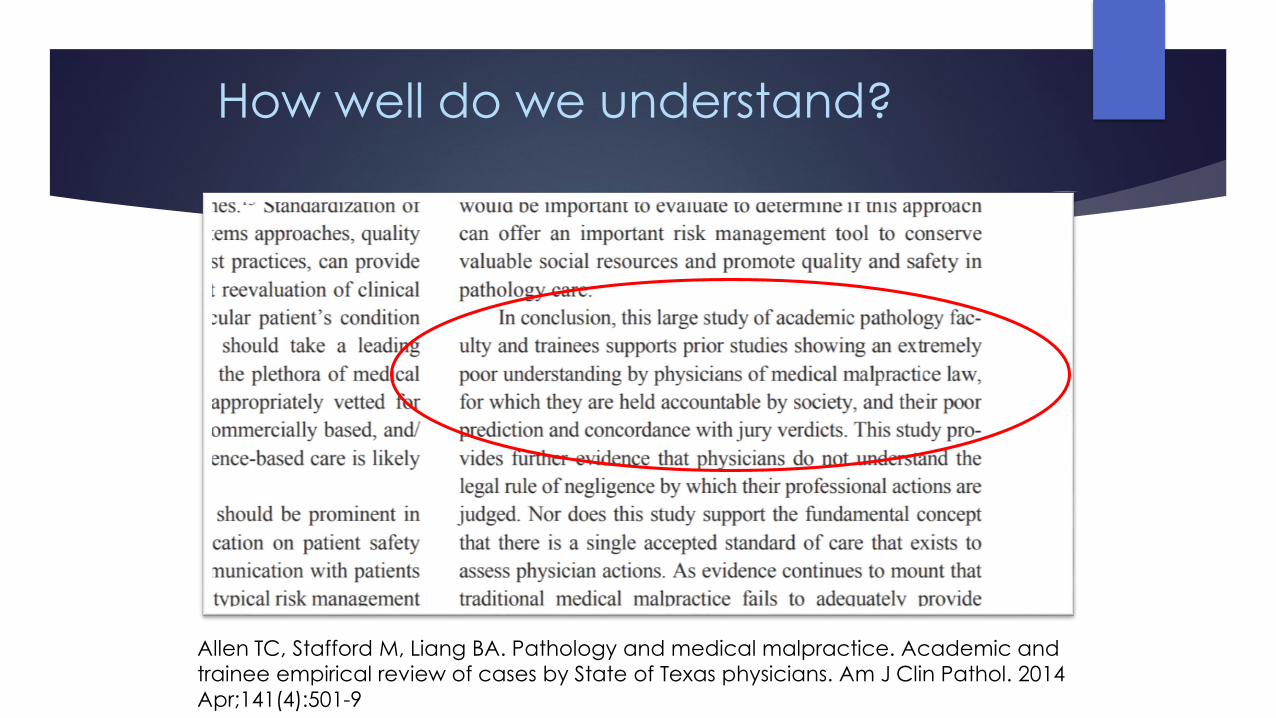
How well do we understand?
Allen TC, Stafford M, Liang BA. Pathology and medical malpractice. Academic and
trainee empirical review of cases by State of Texas physicians. Am J Clin Pathol. 2014
Apr;141(4):501-9

Do we practice defensively?
Allen TC, Liang BA. Pathologists and liability: an old medical story needing a new
ending. Am J Clin Pathol. 2015 Dec;144(6):828-9

The Basics of Medical Malpractice
“No matter how much you think you know about medicine, you’re not an
expert on malpractice law. Your lawyer wouldn’t try to take over for you in
the operating room, so don’t tell him how to handle your case. And don’t
assume that you’re smarter than us plaintiffs’ lawyers.
Remember: Once you’re sued, you’re in our OR.”
-Boston Plaintiffs’ attorney
Med Econ. 2000;77(8):94-6, 99, 103-4 passim.

The tort of negligence
“Conduct which falls below the standard established by law for the
protection of others against unreasonable risk of harm”
Typically the tort theory used in medical malpractice cases

Four elements of a negligence lawsuit
An actor owes a DUTY of care to another
There is a BREACH of the applicable standard of care for carrying out the duty
As a PROXIMATE CAUSE of the breach of duty an injury results
Compensable DAMAGES or injury to the plaintiff occurs

If hay is stacked from moist grass, bacterial fermentation may cause high temperatures where a chemical reaction produces flammable gas Farmers must be careful to avoid this "spontaneous combustion”
“Keeping hay fires from spontaneously combusting.” Montana State University Communication Services
Vaughan v. Menlove
Vaughan v. Menlove, 132 Eng. Rep. 490 (C.P.) 1837
Defendant built a haystack near the plaintiff’s land
Defendant, warned over 5 weeks that the haystack was poorly-built and
might catch fire, said he “would chance it”
It caught fire and destroyed the plaintiff’s barn and two rental cottages

“Reasonable Person” standard of care
Vaughan introduced the “Reasonable Person” standard of care
The court held that the defendant’s standard of care was determined by
whether the defendant “proceed[ed] with such reasonable caution as a
prudent man would have exercised under such circumstances”
The “reasonable person standard of care” has become an important part
of negligence law, including medical malpractice law

Legal experts on standard of care
“Ordinary”
“Average”
“Customary”
“Normally-possessed”
“Reasonably competent”
“Minimally competent”
“Interpreted just a little bit differently by everybody”

The expert witness’ job
An expert witness must:
Define a standard of care
Opine as to whether it has been breached
Opine as to whether any perceived injury was caused by the breach

“Battle of the experts”
“Ordinarily, to carry this burden the plaintiff must find a medical expert who is qualified and willing to testify that the standard of care was violated. Typically, defendants, too, must find their own expert to testify that the standard of care was not violated.”
Case studies of settlement failure. In: Vidmar N. Medical Malpractice and the American Jury: Confronting the Myths about Jury Incompetence, Deep Pockets, and Outrageous Damage Awards. University of Michigan Press: Ann Arbor;1995, 59.
The court’s charge
The Court’s goal is to try the case to conclusion in a procedurally correct manner
The Court also is under pressure to control its docket
“[I]t is not the primary goal of the tort system to achieve a scientifically correct conclusion.”
Wick MR, Foucar E. Evidence-based medicine and tort law. Semin Diagn Pathol 2005;22:167-176.

Loss of chance doctrine
An alternative medical malpractice legal theory of liability

“But for” causation
In traditional medical malpractice cases, the “but for” causation standard sets a clear rule for determining whether the physician’s alleged action was the cause-in-fact for the plaintiff’s injury
Liability occurs where the physician’s action is considered “more likely than not” (51% probability) to have caused the plaintiff’s injury
(In comparison, the “beyond a reasonable doubt” standard, the exclusive standard used in criminal cases, has been considered to be 99%)
When the physician’s action satisfies the “but for” test, and is sufficiently direct (proximate), then the action is considered the legal cause for the plaintiff’s injury
If the physician’s action is found to have a less than 50% probability of having injured the plaintiff, the case fails and the plaintiff “takes nothing”
Relaxed standard of causation
The doctrine relaxes the causation standard of traditional negligence law
Under the loss of chance doctrine, the plaintiff would be compensated for
an injury found to be negligently caused by a physician for the extent to
which the physician’s negligence reduced the plaintiff’s chance of
survival or having a better outcome, if less than 51%
But if greater than 51%, the physician’s extent of negligence is not
considered, and the plaintiff received full (100%) recovery

Ambiguous causation
It is being used more and more in cases where it is difficult to show that a
physician was “more likely than not” negligent under the traditional “but
for” causation standard
These cases often involve elderly and very ill patients, for whom there are
alternative preexisting conditions, giving rise to “ambiguous causation”,
e.g., in a case involving a patient death, whether the patient died from
the physician’s negligence or an alternative preexisting condition
Adequate compensation
The concern is that these patients are not being adequately
compensated for their negligently-induced harms (a reasonable
argument, on its face), and that physicians might therefore not provide
the appropriate standard of care for them (unlikely in my experience, yet
an argument that is put forward)

Smith v. Providence H&S-Oregon, et al.
361 Ore. 456; 2017
P goes to ER with headache, visual disturbances; CT shows no bleeding,
MRI suggested if symptoms persist
P returns to ER with persistent symptoms; D sends P to family MD, with order
for MRI, but not expedited order
MRI at end of week shows substantial brain damage from stroke
Testimony claims failure to order expedited MRI resulted in loss of chance
for treatment which 33% of time reduces or eliminates stroke symptoms
Smith v. Providence H&S-Oregon, et al.
Court determines Oregon adopts the loss of chance theory
“…the defendant’s tortious conduct was the reason it was not feasible to
determine whether or not the more favorable outcome would have
materialized but for the tortious conduct.”
Smith v. Providence, citing King JH. “Reduction of Likelihood” reformulation and Other
Retrofitting of the Loss-of-a-Chance Doctrine, 28 U Mem L Rev 492 (1997)

Knox et al. v. Rana et al.
2016 Tex. App. LEXIS 12381
P “had survived breast cancer and endometrial cancer.” Now
receiving radiation treatment for basal cell carcinoma on the nose
D ordered PET scan based on prior history of cancers; PET report
showed pelvic mass “suspicious for metastatic disease.”
P did not undergo a followup PET scan as ordered; she was later
diagnosed with metastatic cancer and died; testimony showed failure
to get PET scan made no difference in P’s outcome
Court states recovery is barred “if a condition preexists the negligence
of a health care provider and at the time of the negligence, the
condition resulted in the patient having a 50% or less chance of cure or
survival.”
Why now?
“There has recently been a ‘formidable evolution’ of systemic amyloidosestreatments from one of entirely supportive disease management to one dependent upon the specific molecular type of amyloid protein involved, utilizing ‘quite diverse, radical and aggressive treatments,’ including, chemotherapeutic regimens, some with stem cell rescue; stem cell transplantation; liver transplantation; and liver transplantation combined with heart or kidney transplantation...These remarkable therapeutic advances for some specific types of amyloidosis depend upon early, specific, and accurate amyloidosis diagnosis in order to best ensure appropriate patient treatment and optimize prognosis. Hence not only late diagnosis but misdiagnosis of the amyloidosis-type consequently leading to the application of aggressive treatment is dangerous.”
Allen TC. Medicolegal issues of amyloidosis. In: Picken MM, Herrera GA, Dogan A, Eds. Amyloid and related disorders: Surgical pathology and clinical correlations, 2d Ed. Humana Press:New York , 2015; 519.
Why now?
“When treatment options are primarily only supportive or nonspecific, regardless of when a diagnosis is made, and as such early diagnosis does not improve overall survival, showing that misdiagnosis or a delay in diagnosis was the injury’s ‘‘proximate cause’’ could be extremely difficult, or perhaps impossible. The loss of chance doctrine provides the plaintiff no increased benefit beyond the typical medical malpractice negligence doctrine in those situations; the plaintiff probably could not prove ‘‘proximate cause’’ by either method.”
“With the development of new diagnostic and therapeutic regimens; however, many diseases, including cancers, that were once merely treated supportively now have available, or may soon have available, specific therapies, including molecular-based therapies, which, if diagnosed early, provide the patient an improved prognosis. In these cases, the loss of chance doctrine may provide plaintiffs who could not prove that misdiagnosis or a delay in diagnosis was more likely than not the proximate cause of the plaintiff’s injury an avenue through which they might prevail.”
Allen TC. Loss of chance doctrine: An emerging theory of medical malpractice liability. Pathology Case Reviews 2012;17: 172-174.
21st century applications
Molecular testing of cancer
As with amyloidosis, sudden shift to specific, detailed, molecular-driven
diagnoses that must be done quickly and accurately to guide the use of
extremely expensive therapy that has the potential to significantly extend
the life span of cancer patients, e.g., TKIs and late-stage lung cancer
patients
Real world scenario
Multigene predictors of cancer therapy for which evidence-based
literature is still developing
Utilize a new molecular test and recommend a course of action, or do not
utilize it and recommend another course of action:
“In either case, with the advantage of perfect hindsight, the physician
could be portrayed by a skilled trial lawyer as having acted too slowly or too quickly to rely on multigene predictor assays.”
Issa AM, Chaudhari VS, Marchant GE. The value of multigene predictors of clinical outcome in breast cancer: an analysis of the evidence. Expert Rev Mol Diagn. 2015 Feb; 15(2):277-286.

The doctrine is appealing
“…human life is precious and…even the loss of only a small chance of
cure or survival is a significant loss.”
“…acts of negligence…to patients with poor prognoses should not go
unredressed…”
“…fundamentally unfair to permit recovery where the negligence had a
51 percent possibility of producing the harm complained of but denying
any recovery where the proof is only a 50 percent possibility.”
Weigand TA. Loss of Chance in Medical Malpractice: The Need for Caution. Massachusetts Law Review. http://www.massbar.org/publications/massachusetts-law-review/2002/v87- n1/loss-of-chance-in-medical

But
“…the practice of medicine is not an exact science and in most
instances there is more than one acceptable approach…”
“Health care providers could find themselves defending cases simply
because another course of action could possibly bring a better result.”
“To impose liability on physicians based on loss of chance is to impose a
burden that no other professional malpractice defendant carries.”
May encourage “a proliferation of defensive medicine, an escalation of
medical costs, and an unwarranted expansion of liability exposure…”
Weigand TA. Loss of Chance in Medical Malpractice: The Need for Caution. Massachusetts Law Review. http://www.massbar.org/publications/massachusetts-law-review/2002/v87-n1/loss-of-chance-in-medical
Perfect storm
Increasing understanding of disease processes, specifically molecular
pathology
Corresponding increase in therapies for these diseases, often requiring
early diagnosis and fast treatment in order to provide successful results
Increasingly expectant society with less appetite for medical failure
Increasingly cost-conscious medical administrators, with resultant
increased work loads and increased chance of error
Aggressive medical malpractice attorneys exploring options to
advance cases in light of tort reform
Courts becoming more comfortable with using the loss of chance
doctrine

Attorneys are aware
Insurer responsibilities
Defend the pathologist in the lawsuit
Retain an attorney for the pathologist
Defend the pathologist during the entirety of the proceeding
Indemnify the pathologist
Pay a settlement up to the policy limits
Pay a judgment on any covered claim
Policy may have a “consent clause” requiring pathologist’s consent to settle the
claim

Pathologist’s responsibilities
Notify the insurer promptly if any potential claims
Failure to do so may jeopardize the insurer’s obligations to the pathologist in the
lawsuit
Cooperate with the defense attorney during the duration of the claim and
subsequent lawsuit
Trust the attorney, be completely candid, and follow the attorney’s advice
Medical Malpractice Lawsuit Timeline
Presuit notice
Lawsuit events
Trial

Presuit notice
No attorney is yet involved
Critical to act promptly
Correct conduct maximizes legal protections
Avoid conduct that is potentially harmful to the pathologist’s case
Notice letter
Patient’s chart
Discussion of the claim

Notice letter
From Plaintiff’s attorney
Advises pathologist of Plaintiff’s intent to sue
Puts pathologist on notice of potential claim
Not a lawsuit
Not filed with the court
State law specific
Required by state to encourage presuit negotiations and settlement

Notice letter
Notify the insurer immediately upon receipt
Provide insurer any additional documentation
Delay in notification can jeopardize coverage
Notify insurer of any notice or service suggestive of or resembling a legal
claim
Discovery request
Deposition notice
If contacted by an attorney, do not discuss the case and immediately
inform the insurer

Patient’s chart
Not as much a concern with electronic medical record
For pathologists, major concern is spoliation of evidence
Place slides and blocks in safekeeping, as instructed by insurer
Do not do additional sections or stains, as such could be argued to be
spoliation

Discussion of the claim
Discuss the claim only with the insurer and the attorney provided by the
insurer
Avoid the temptation to discuss the claim with colleagues
Those discussions are at high risk for being identified and recounted during
discovery
Lawsuit events
Formal beginning of the lawsuit
Statute of limitations
Discovery
Pretrial means of disposition
Mediation

Formal beginning of the lawsuit
Plaintiff’s attorney files a petition with the court
There is then service of the petition and citation on the pathologist
The pathologist is now a defendant in the lawsuit
Immediately call the insurer, then forward copies of the petition and
citation

Formal beginning of the lawsuit
It is typically at this point that the insurer assigns an attorney to the
pathologist
The pathologist must immediately notify the insurer for timely filing of the
lawsuit answer
If answer is not filed by the court’s deadline, Plaintiff may obtain a default
judgement against the pathologist, and proceed to execute on the
pathologist’s assets for the amount of the default judgment

Statute of limitations
State specific
Not uncommonly medical malpractice claims have a two year statute of
limitations
Notice letter may extend it
Discovery rule
Tolls the statute of limitations where Plaintiff is unable to discover the event that
is the basis for the legal claim; otherwise prevents bringing of lawsuit before its
basis is discoverable

Discovery
Filing of the lawsuit initiates the discovery phase
Discovery is broad and includes all documents and information likely to
lead to the discovery of admissible evidence, whether or not that
information or those documents are ultimately themselves admissible
Pathologist often invests significant time and effort into responding to
discovery

Forms of discovery
Interrogatories: written questions served by the parties
Requests for disclosure: state specific requests for basic lawsuit information
such as experts, damages, contentions
Requests for production: requests for written documents

Forms of discovery
Requests for admissions: time sensitive requests to admit or deny
contentions or facts
Expert reports: contain the party’s experts’ opinions and bases for those
opinions
Depositions: sworn testimony by witnesses

Pretrial means of disposition
Motion for summary judgement: Dispositive motion; a judgment on the
merits, usually filed asserting defenses such as statue of limitations or
Plaintiff’s inability to produce a qualified expert capable of establishing
negligence
Motion to dismiss: Dispositive motion; usually filed when Plaintiff fails to
produce an expert CV and expert report establishing negligence

Pretrial means of disposition
Settlement: Agreement by parties; often pathologist does not admit
negligence but settles to avoid time and harassment of defending the
lawsuit. The parties execute and file with the court an agreed motion for
nonsuit; judge executes the order
Voluntary nonsuit: Rare; Plaintiff drops claim, often strategically, in order to
refile with a narrower group of defendants

Mediation
Nonbinding
Usually requires a half day or day, with all parties and attorneys present
Insurer must be present or available to authorize settlement
Uses an independent third party mediator
Mediator attempts to persuade parties to resolve the case

Trial
Most medical malpractice lawsuits settle before trial; some settle during
trial
Several years from lawsuit filing to the trial
Trial date is often uncertain until very close to the beginning of trial
Pathologist usually must dedicate two weeks for the trial, be prepared to
testify, and sit with the attorney at the counsel table during the trial

The fact witness deposition
Testimony of a witness under oath before a court reporter
Treated as courtroom testimony
Conducted in accordance with state or federal court rules
A discovery device
One party asks oral questions of the other party or its witness
May be performed in a formal or an informal manner
Locations—attorney’s office, doctor’s office, hotel room, or court reporter’s
office

Deposition
Deponent
Attorneys for parties
Court reporter
Videographer in some cases
Transcript is written
Word by word account of all that is said in the deposition
May be audiotaped and/or videotaped
Witness is entitled to a copy to clarify an answer or correct spelling
Do not waive the right

Plaintiff’s attorney’s goals
Educate herself about the subject
Learn what facts the defendant knows
Learn the defendant’s strategies
Judge the effectiveness of the defendant at trail
Impeach the defendant’s credibility

Plaintiff’s attorney’s goals
Learn the defendant’s strategies
Do not volunteer information
Answer “yes” or “no” or in short sentences
Beware of compound questions
Do not agree to supply any documentation or other information to the
plaintiffs’ attorney
Plaintiff’s attorney’s goals
Judge the effectiveness of the defendant at trial
Dress professionally
Be calm, professional, polite, knowledgeable
Do not appear arrogant (explain medical terms)
Keep emotions in check; do not joke
Plaintiff’s attorney’s goals
Impeach the defendant’s credibility
If unsure, state, “I don’t know” or “I don’t remember.”
Pause before answering to consider the question, and to give your
attorney an opportunity to object
Clarify any mistake

Plaintiff’s attorneys
Pal
Freight train
Butterfly
Time bomb
Ignoramus
Surv Ophthalmol 1995;40:69-72.
Am J Surg Pathol. 2001;25(4):527-537.
Pal
Joking and banter before the deposition
Informal setting
Casual dress

Freight train
Questions the deponent in a rapid-fire manner
Answer before thinking
Answer after a moment, slowly, in complete sentences, to break the
rhythm
Butterfly
Moves from one line of questioning to another
Confusing, attempting to elicit conflicting statements
Ignore and answer consistently

Time bomb
Most difficult, complicated, or contentious questions are presented at the end of the deposition
Hope that fatigue will cause inconsistencies or wrong answers
Ask for a break

Ignoramus
Appears ignorant in an attempt to get deponent to volunteer information
May leave time after an answer to prompt deponent to volunteer more
May use body language to prompt deponent to volunteer information
Common misconceptions
It is not a forum to defend yourself
It is not a forum to tell your story (your defense attorney is not going to elicit
your story then, and the plaintiffs’ attorney is only interested in facts that
help her client
It is not a forum to prove you are a smart doctor
Remember
Remember that a deposition is an adversarial proceeding
Never consider a deposition as “routine”
Listen to the entire question
Make certain you understand the question
Ask that a question be repeated if necessary

Remember
Do not attempt to rephrase a question
Do not accept a summary of facts without considering the accuracy of
those facts
Beware of misstated facts or prior testimony attempting to elicit
information
Look through medical records or other materials at hand
Do not take anything with you to the deposition

Remember
Do not allow yourself to be rushed into answering
Do not volunteer information or speculate
Avoid absolutes such as “always” and “never”
Avoid saying “honestly” or “to be honest”, from which it may be implied
that prior answers were not honest ones
Do not verbally spar with the questioning attorney—you will always lose

Deposition
“The other side would love to hear all of their thinking…because they
will give that to their experts to tear apart and come up with 30 other
reasons why [that explanation] wasn’t right.”
Uraneck K, Proper preparation is the key to a successful deposition, American College of Emergency Physicians News, October 2002.

Deposition
“And the fun part of the deposition is that there isn’t going to be a judge
there to rein you in so you can ask them anything you want.”
“Some deponents have even been asked to empty their pockets at a
deposition.”
Uraneck K, Proper preparation is the key to a successful deposition. American College of Emergency Physicians News, October 2002.

Deposition
“Also, the plaintiff’s attorney can be so punishing in their questioning that
the witness would rather settle than face a repetition of the experience at
trial. These tactics are considered ethical….”
“Everything in the deposition is teased out, taken out of context, used
against you.”
Uraneck K, Proper preparation is the key to a successful deposition. American College of Emergency Physicians News, October 2002.

Coping
Minimizing the emotional,
psychological, and physical
impact on the pathologist
and the pathologist’s family

High stress event
“Becoming involved in a lawsuit can be a significant event for anyone,
including a physician. It can require a great deal of the physician's time
and effort, can be emotionally draining, and can serve a psychological
blow to the physician's professional psyche.”
Berry DB. The physician's guide to medical malpractice. Proc (Bayl Univ Med Cent). 2001 Jan; 14(1): 109–112.
“… a source of much fear…”
“The lawsuit arrives like a modern day version of the ‘Black Spot’…”Sacopulos MJ. Physicians aren’t alone: understanding and dealing with malpractice litigation stress.
http://www.beckersspine.com/orthopedic-spine-practices-improving-profits/item/11117-physicians-arent-alone-understanding--dealing-with-malpractice-litigation-stress
“In the book, pirates are presented with a ‘black spot’ to officially
pronounce a verdict of guilt or judgement. It consists of a circular piece
of paper or card, with one side blackened while the other side bears a
message and placed in the hand of the accused. It was a source of
much fear because it meant the pirate was to be deposed as leader, by
force if necessary—or else killed outright.”Black spot (Treasure Island), Wikipedia. https://en.wikipedia.org/wiki/Black_Spot_(Treasure_Island)

How serious is a medical malpractice lawsuit to a
physician?
Allen TC. Medicolegal issues in pathology. Arch Pathol Lab Med. 2008 Feb;132(2):186-91

“…not a vocation…”
“For many physicians this is not a vocation, this is their life and being sued in an invasion of their life.”
Sacopulos MJ. Physicians aren’t alone: understanding and dealing with malpractice litigation stress. http://www.beckersspine.com/orthopedic-spine-practices-improving-profits/item/11117-physicians-arent-alone-understanding--dealing-with-malpractice-litigation-stress
“…[T]he grinding, drawn-out repercussions of a prolonged lawsuit frequently require…extensive support, including professional mental health resources.”
Coping with the stress of medical professional liability litigation. Committee on Professional Liability, ACOG. https://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Professional-Liability/Coping-With-the-Stress-of-Medical-Professional-Liability-Litigation

“…devastating.”
“…physicians are acutely sensitive to any suggestion that they have failed
to meet the standard of care or are not ‘good’ doctors. Their honor—that
sense of personal integrity that most people cherish—is at issue, and the
threat of its loss is devastating.”
Charles SC. Coping with a medical malpractice suit. West J Med 2001 Jan; 174(1): 55-58.

Just how devastating?
Major depressive disorder:
up to 39%
Adjustment disorder:
up to 53%
Onset or exacerbation of physical illness:
up to 15%
Acknowledge alcohol or drug misuse:
less than 2%
How to cope
“A feeling of being out of control pervades the litigation
process…regaining mastery is central.”
“…the more rapidly this is achieved, the better because chronic stress can
lead to further disability.”
Charles SC. Coping with a medical malpractice suit. West J Med 2001 Jan; 174(1): 55-58.
Knowledge is power
“…an adequate knowledge base about what can be anticipated
psychologically and about the process in which the physician is now a
participant…”
Charles SC. Coping with a medical malpractice suit. West J Med 2001 Jan; 174(1): 55-58.

Social support is critical
“…physicians need to share their feelings and reactions with someone
who is trustworthy, understanding, and sensitive to their concerns…”
“Legal counsel will advise not to talk about the details of the case to
anyone.”
“It is not…good psychological advice.”
Charles SC. Coping with a medical malpractice suit. West J Med 2001 Jan; 174(1): 55-58.

Social support is critical
Discuss with your attorney early in the process
Know the limitations of what can—and importantly what cannot—be
discussed with partner, colleagues, support group, or counselor

Regain control and self-esteem
Use your social support as fully as possible
Take care of yourself
Exercise; spend time with a hobby
Take that much-needed vacation
Understand your litigation process
Get to know your attorney
Learn the anticipated timeline
Learn your role in each step of the process
Schedule enough time off for the trial

Regain control and self-esteem
Change the meaning of the event
You are not a “bad doctor” or “incompetent”; change that narrative
Be objective; acknowledge the “truth” about the event in question
Sued physicians are often the best in their field, taking care of the most high-risk
patients; and most are vindicated in the end
Helpful words of advice
“…think of the lawsuit as a reflection of our times, more than your
competence as a physician.”
“…doesn’t necessarily reflect your competence. Most ethical and
compassionate physicians are sued. This is because they won’t shy away
from caring for the most medically complex patients, or the most
emotionally troubled patients.”
Sacopulos MJ. Physicians aren’t alone: understanding and dealing with malpractice litigation stress. http://www.beckersspine.com/orthopedic-spine-practices-improving-profits/item/11117-physicians-arent-alone-understanding--dealing-with-malpractice-litigation-stress ; adapted from Wang DC. The Kitchen Shrink: A Psychiatrist’s Reflections on Healing in a Changing World.

Helpful words of advice
“Many lawsuits are simply frivolous. [You might be] sued for simply being in
the room.”
“…focus on what’s in your control—such as continuing to practice, and
doing your best for patients. Obsessing about things not in your control
causes anxiety.”
Sacopulos MJ. Physicians aren’t alone: understanding and dealing with
malpractice litigation stress. http://www.beckersspine.com/orthopedic-
spine-practices-improving-profits/item/11117-physicians-arent-alone-
understanding--dealing-with-malpractice-litigation-stress ; adapted from
Wang DC. The Kitchen Shrink: A Psychiatrist’s Reflections on Healing in a
Changing World.

Helpful words of advice
“…the lawsuit will pass.”
“…focus on why you got into medicine in the first place. All the human
improvement and relief you provide should not be marred by some
litigious miscreants.”
Sacopulos MJ. Physicians aren’t alone: understanding and dealing with malpractice litigation stress. http://www.beckersspine.com/orthopedic-spine-practices-improving-profits/item/11117-physicians-arent-alone-understanding--dealing-with-malpractice-litigation-stress ; adapted from Wang DC. The Kitchen Shrink: A Psychiatrist’s Reflections on Healing in a Changing World.

Thank you!

















