1 Medical Marijuana Alen Voskanian, MD, MBA, FAAHPM, HMDC, AAHIVS Regional Medical Director, VITAS Healthcare Assistant Clinical Professor of Medicine, UCLA Disclosures • There are no relevant financial relationships to disclose Objectives • Describe the pharmacology of medical marijuana • Describe state laws regarding the use of medical marijuana • Discuss available research studies • Recognize medical risks and side effects • Recommend steps for developing a hospice policy
Transcript
1
Medical Marijuana
Alen Voskanian, MD, MBA, FAAHPM, HMDC, AAHIVS
Regional Medical Director, VITAS Healthcare
Assistant Clinical Professor of Medicine, UCLA
Disclosures
• There are no relevant financial relationships to
disclose
Objectives
• Describe the pharmacology of medical
marijuana
• Describe state laws regarding the use of
medical marijuana
• Discuss available research studies
• Recognize medical risks and side effects
• Recommend steps for developing a hospice
policy
2
Marilyn
• Marilyn is a 68-year-old woman with breast cancer metastatic to the lungs and the thoracic and lumbar spine.
• She is currently undergoing chemo- therapy with doxorubicin.
• She reports having very low energy, minimal appetite, and substantial pain in her thoracic and lumbar spine.
• For relief of nausea, she has taken ondansetron and prochlor- perazine, with minimal success.
• She has been taking 1000 mg of acetaminophen every 8 hours for the pain. Sometimes at night she takes 5 mg or 10 mg of oxycodone to help provide pain relief.
• During a visit with her primary care physician she asks about the possibility of using marijuana to help alleviate the nausea, pain, and fatigue. She lives in a state that allows marijuana for personal medicinal use, and she says her family could grow the plants.
• Would you:
– 1. Recommend the medicinal use of marijuana.
– 2. Do not recommend the medicinal use of marijuanaThe New England Journal of Medicine 368;9, Feb 28, 2013
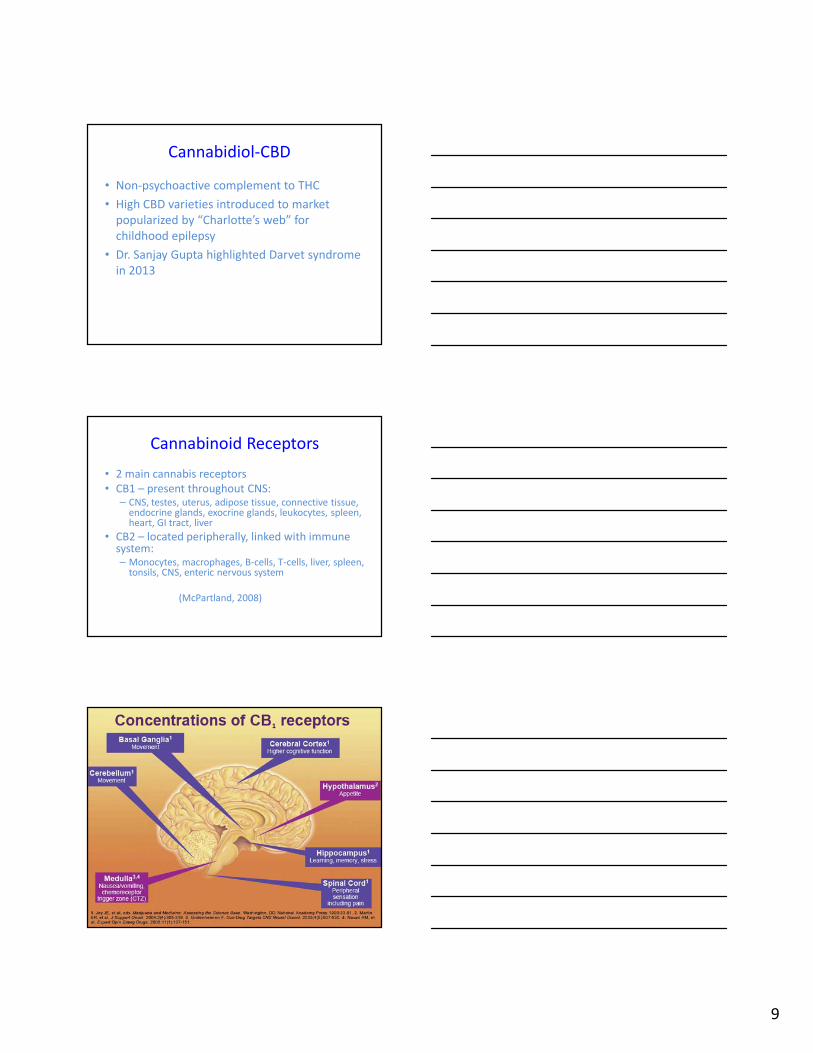
endocrine glands, exocrine glands, leukocytes, spleen, heart, GI tract, liver
• CB2 – located peripherally, linked with immune system:– Monocytes, macrophages, B-cells, T-cells, liver, spleen,
tonsils, CNS, enteric nervous system
(McPartland, 2008)
10
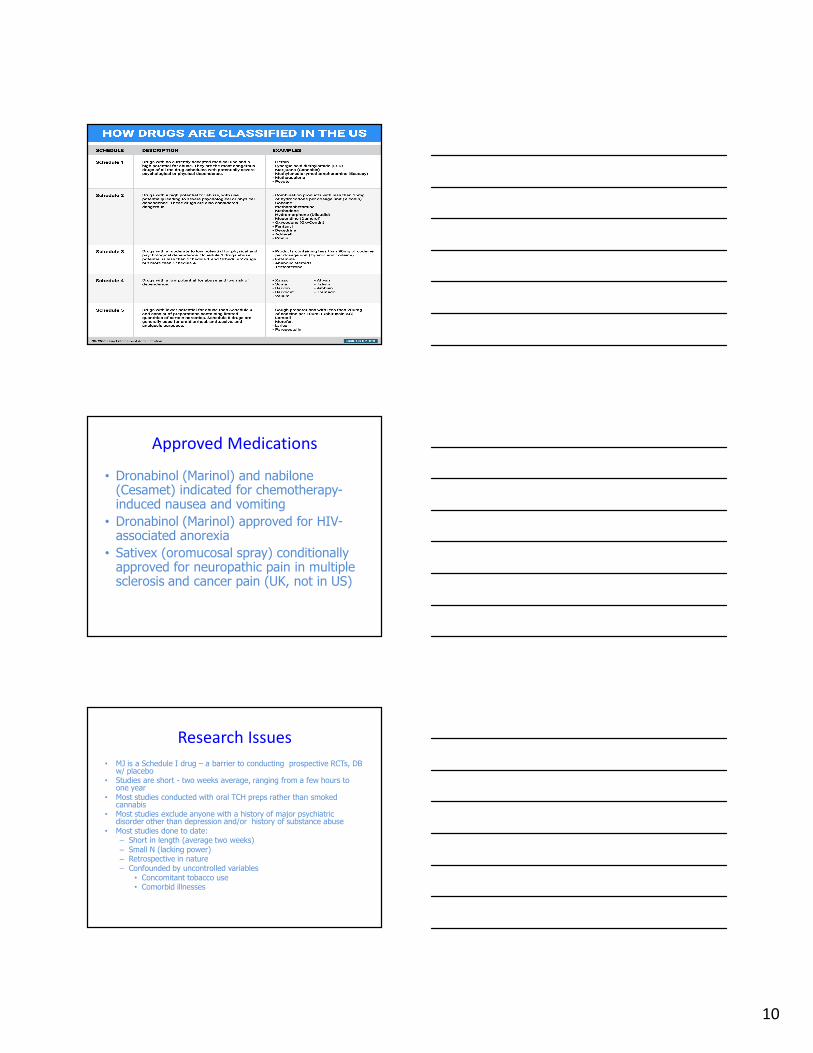
Approved Medications
• Dronabinol (Marinol) and nabilone(Cesamet) indicated for chemotherapy-induced nausea and vomiting
• Dronabinol (Marinol) approved for HIV-associated anorexia
• Sativex (oromucosal spray) conditionally approved for neuropathic pain in multiple sclerosis and cancer pain (UK, not in US)
Research Issues
• MJ is a Schedule I drug – a barrier to conducting prospective RCTs, DB w/ placebo
• Studies are short - two weeks average, ranging from a few hours to one year
• Most studies conducted with oral TCH preps rather than smoked cannabis
• Most studies exclude anyone with a history of major psychiatric disorder other than depression and/or history of substance abuse
• Most studies done to date:– Short in length (average two weeks)– Small N (lacking power)– Retrospective in nature– Confounded by uncontrolled variables
– Jensen B, Chen J, Furnish T, Wallace, M. Medical Marijuana and Chronic pain: A review of Basic Science and Clinical Evidence. Current Pain Headache Rep (2015) 19: 50.
– Kraft B, Frickey NA, Kaufmann RM, Reif M, Frey R, Gustoff B, Kress HG. Lack of analgesia by oral standardized cannabis extract on acute inflammatory pain and hyperalgesia in volunteers. Anesthesiology. 2008 Jul;109(1):101-10.
– Wallace M, Schulteis G, Atkinson JH, Wolfson T, Lazzaretto D, Bentley H, Gouax B, Abramson I. Dose-dependent effects of smoked cannabis on capsaicin-induced pain and hyperalgesia in healthy volunteers. Anesthesiology 2007 Nov; 107(5):785-96.
• Andreae MH, et al. Inhaled Cannabis for Chronic Neuropathic Pain: A Meta-analysis of Individual Patient Data. The Journal of Pain, Vol 16, No 12, 2015: 1221-1232.
12
Neuropathic Pain- Comparison
• Cannabis– NNT 5.6 (3.4, 14) CI 95%
• Gabapentin for diabetic neuropathy– NNT 5.8 (4.3, 9) CI 95%
• Duloxetine for neuropathic pain in fibromyalgia– NNT 8 (4, 21) CI 95%
• Pregabalin for post-herpatic neuralgia– 5.3 (3.9, 8.1) CI 95%
– Wiffen PJ, et al, Antiepileptic drugs for neuropathic pain and fibromyalgia – an overview of Cochrane reviews. Cochrane Database of Systematic Reviews 2013, Issue 11. Art. No.: CD010567. DOI: 10.1002/14651858.CD010567.pub2.
– Lunn MPT, Hughes RAC, Wiffen PJ. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database of Systematic Reviewes 2014, Issue 1. Art. No.: CD007115.
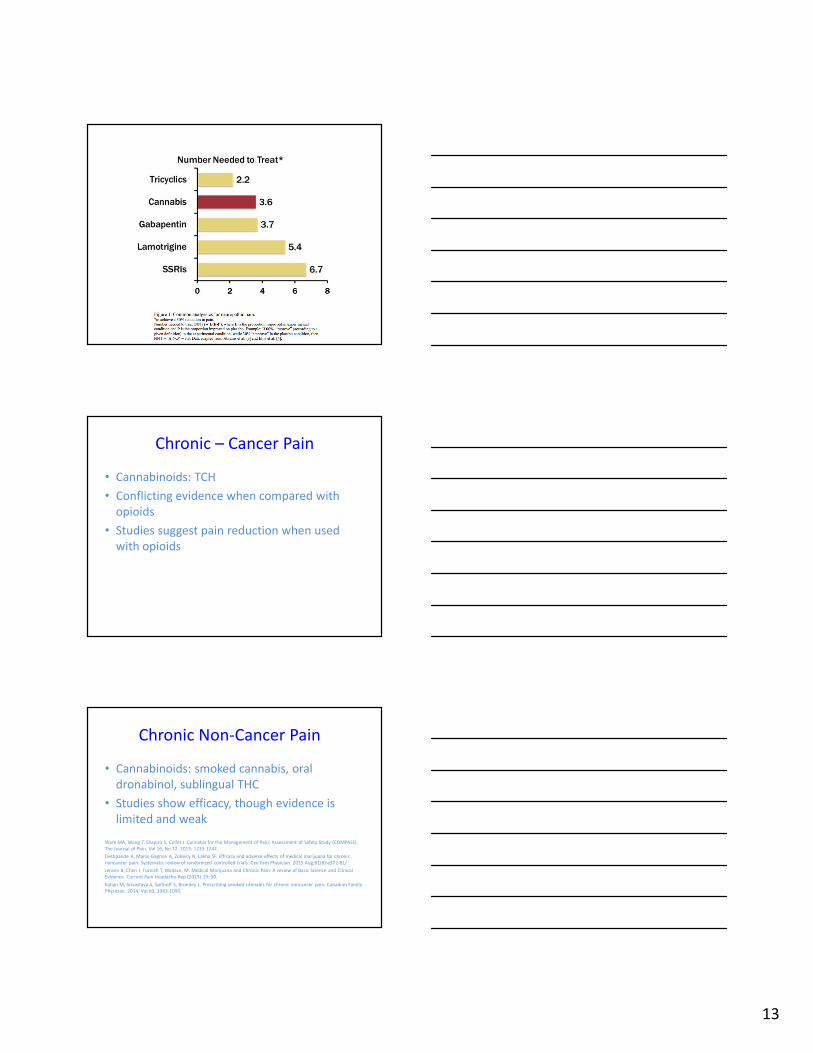
Neuropathic Pain
– 5 studies demonstrated a significant decrease in pain after
cannabis administration
• the magnitude of effect in these studies, expressed as the
number of patients needed to treat to produce one positive
outcome, was comparable to current therapies
13
Chronic – Cancer Pain
• Cannabinoids: TCH
• Conflicting evidence when compared with
opioids
• Studies suggest pain reduction when used
with opioids
Chronic Non-Cancer Pain
• Cannabinoids: smoked cannabis, oral
dronabinol, sublingual THC
• Studies show efficacy, though evidence is
limited and weak
Ware MA, Wang T, Shapiro S, Collet J. Cannabis for the Management of Pain: Assessment of Safety Study (COMPASS).
The Journal of Pain, Vol 16, No 12. 2015: 1233-1242.
Deshpande A, Mailis-Gagnon A, Zoheiry N, Lakha SF. Efficacy and adverse effects of medical marijuana for chronic
noncancer pain: Systematic review of randomized controlled trials. Can Fam Physician. 2015 Aug;61(8):e372-81/
Jensen B, Chen J, Furnish T, Wallace, M. Medical Marijuana and Chronic Pain: A review of Basic Science and Clinical
Evidence. Current Pain Headache Rep (2015) 19: 50.
Kahan M, Srivastava A, Spithoff S, Bromley L. Prescribing smoked cannabis for chronic noncancer pain. Canadian Family
Physician. 2014; Vol 60, 1083-1090.
14
Other Symptoms
• Nausea & Vomiting– Cannabinoids: dronabinol and nabiximols
– Greater benefit of cannabinoids compared to placebo
– Low quality evidence
• Anorexia– Cannabinoids: dronabinol
– Increased weight compared to placebo
– Increased appetite, greater percentage body fat, reduced nausea, improved functional status
– In comparison, megestrol showed greater weight gain
– Low quality evidence
– Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015;313(24):2456-73.
– Suggest cannabinoids are associated with improvements in spasticity
– Moderate quality evidence
Kluger B, Triolo P, Jones W, Jankovic J. The therapeutic potential of cannabinoids for movement disorders. Mov Disord 2015;30(3):313- 27.Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015;313(24):2456-73.
Other Symptoms
• Depression– Cannabinoid: nabiximols (Sativex)
– No difference with placebo
• Anxiety– Cannabinoid: cannabidiol
– Improvement in anxiety as assessed by public speaking
– Very low quality evidence
Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015;313(24):2456-73.
15
Other Symptoms
• Sleep
– Cannabinoids: nabilone, nabiximols
– Suggested improvements
– Low Quality evidence
• Tourette Syndrome
– Cannabinoid: TCH capsules
– Significant improvement in severity of tics
– Low quality evidence
Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015;313(24):2456-73.
Other Symptoms
• Epilepsy
– There is little evidence about the safety or efficacy
– A 2014 Cochrane review did not find enough evidence to draw conclusions about its use
– A 2014 review by the American Academy of Neurology concluded that “data are insufficient to support or refute the efficacy of cannabinoids for reducing seizure frequency.”
Gloss, D; Vickrey, B (March 5, 2014). “Cannabinoids for epilepsy”. The Cochrane database of systematic reviews (3): CD009270. PMID 24595491.
Koppel, Barbara (April 29, 2014), Systematic review: Efficacy and safety of medical marijuana in selected neurologic disorders, Neurology.
Therapeutic Benefits
• Medical cannabis may be effective for pain, nausea, anorexia, other conditions but the literature is inadequate, and dosage is not well standardized.
• Greatest efficacy when used for management of neuropathic pain, nausea, appetite stimulation, chronic pain, and spasticity associated with MS are the indications supported by high-quality evidence .
Rahn EJ, Hohmann AG. Cannabinoids as pharmacotherapies for neuropathic pain: from the bench to the bedside. Neurotherapeutics. Oct 2009;6(4):713-737. http://www.mbc.ca.gov/Licensees/Prescribing/medical_marijuana_cma-recommend.pdf
16
American Medical Association
AMA
• In 2009, AMA’s House of Delegates put forward a message that marijuana’s Schedule I status was no longer appropriate and interfered with legitimate medical research.
• CA Medical Association’s House of Delegates has also adopted policy urging that marijuana’s status as a federal DEA Status I controlled substance be reviewed. (HOD 102a-10)
Health Risks
• Addiction: Escalating use, inability to cut back, craving, harmful consequences, and physical dependence.
• About 9% of adult cannabis users become addicted and the risk is increased among those who begin using before age 18.
• Amongst adults, incidence of addiction is lower compared to alcohol use (15%), opioids (23%), or nicotine (32%).
Anthony J, Warner L, Kessler R. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances and inhalants: basic ndings from the National Comorbidity Study. Clin Exp Psychopharmacol. 1994;2:244-268.
Health Risks
• Short term cognitive effects: memory, sense of time, sensory perception, attention span, problem solving, verbal fluency, reaction time, and psychomotor control
• Last about 1 – 4 hours
• There are no reported cases of death resulting from cannabis overdose
Welch S, Martin B. The pharmacology of marijuana. In: Graham A, Schultz T, Mayo-Smith M, Ries R, Wilford B, eds. Principles of Addiction Medicine 3rd ed. Chevy Chase, MD: American Society of Addiction Medicine; 2003:249-270.
17
Health Risks
• Long term cognitive effects:
– Results of a meta-analysis showed that there might be decrease in the ability to learn and remember new information in chronic users.
– In medical setting, under more limited exposure, the benefits could outweigh this problematic effect.
Grant I, Gonzalez R, Carey CL, Natarajan L, Wolfson T. Non-acute (residual) neurocognitive effects of cannabis use: a meta-analytic study. J Int Neuropsychol Soc. Jul 2003;9(5):679-689.
Health Risks
• Adolescents and Young Adults:
– Greater vulnerability to the toxic effects of cannabis on the brain, especially when alcohol and cannabis are used together (1)
– Increased use of addiction, and poorer educational outcomes (1)
– Possibility that cannabis increases the risk of developing mental illness in this age group.(2)
1. Hall W. The adverse health effects of cannabis use: what are they, and what are their implications for policy? Int J Drug Policy. Nov 2009;20(6):458-466.
2. D’Souza DC. Cannabinoids and psychosis. Int Rev Neurobiol. 2007;78:289-326.
Health Risks
• Psychiatric Conditions:
– Transient mood, anxiety, and psychotic symptoms.
– Long term risks are less well understood
– Can unmask symptoms among individuals who
have pre-existing vulnerability to schizophrenia
(family history)
Arseneault, Cannon et al. “Causal association between cannabis and psychosis: Examination of the
evidence.” British Journal of Psychiatry. No. 184, 2004: 110-117.
18
Health Risks
• Obstructive Lung Disease:
– Given increased risk of COPD in tobacco smokers, concerns about similar risks for cannabis smokers
– Cannabis smoking by itself probably does not lead to COPD but smoking both cannabis and tobacco is associated with a greater risk of COPD than smoking only tobacco.
Tashkin DP. Does smoking marijuana increase the risk of chronic obstructive pulmonary disease? Cmaj. Apr 14 2009;180(8):797-798.
Tan WC, Lo C, Jong A, et al. Marijuana and chronic obstructive lung disease: a population-based study. Cmaj. Apr 14 2009;180(8):814-820
Marijuana and Cancer Risk
• Marijuana smoke contains several of the same carcinogens and co-carcinogens as tobacco smoke
• Benzo[α]pyrene, a procarcinogenicpolycyclic aromatic hydrocarbon, is present in marijuana tar at higher concentrations than in tobacco tar
• Marijuana smoking involves inhalation of 3 times the amount of tar as tobacco smoke
Marijuana and Cancer Risk• Case-controlled study of lung cancer in adults
< 55yrs of age in New Zealand• 79 cases of lung cancer and 324 controls• Risk of lung cancer increased 8% for each
joint-yr (1 joint/day for one year) of cannabis smoking after adjustment for confounding variables including tobacco
• Risk increased 7% for each pack-yr tobacco • “Long-term cannabis use increases risk of
lung cancer in young adults”Aldington et al. Eur Respir J. 2008;31:280-286
19
Marijuana and Cancer Risk
• Studies are small in number and are retrospective in nature
• Confounded by concomitant use of tobacco
• Confounded by underreporting of marijuana use because such use is often illegal
Health Risks
• Reproductive:
– Compounds found in cannabis cross the placenta and pass into breast milk
– Affects reproductive physiology in both men and women. Long term consequences are unclear
– Use during pregnancy and early development has been correlated with low birth weight, developmental delay, and behavioral problems.
Schuel, H. “Tuning the oviduct to the anandamide tone.” J Clin Invest 116(8): 2087-90, 2006.
Fergusson, D. M., L. J. Horwood, et al. 2002.
BJOG 109(1): 21-7.
20
Hospice Policy
• Gaining widespread acceptance
• Conflicting clinical evidence
• California Legislation
• Remains Schedule I controlled substance under the Federal Regulation
To Be or Not To Be?
• Hospice plan of care?
• Allow medical marijuana certification?
• Covered or not covered?
• Guideline versus policy?
• Allow medical marijuana on institution’s
campus?
• Employees present when patient is using?
Recommending?
Certifying? Prescribing? Prognosis?
21
Medical Board of CA
• Standards for reasonable physician to recommend or approve any medication:
– History and good faith examination of the patient
– Development of treatment plan with objectives
– Informed consent including discussion of SE
– Periodic review of the treatment’s efficacy
– Consultation, as necessary
– Proper record keeping that supports the decision to recommend the use of medical marijuana
Medical Marijuana Identification Card
• DHS is required to establish & maintain a statewide medical marijuana ID card registry program
• Physician may recommend that a person’s health would benefit from the use of marijuana in the treatment of cancer, anorexia, AIDS, chronic pain, spasticity, glaucoma, arthritis, migraine, or any other illness for which marijuana provides relief.
• I am a qualified patient. How do I apply for
MMIC?
– A copy of your doctor’s recommendation
– Proof of identity. DMV driver’s license or ID
– Proof of residency: Rent/mortgage agreement,
utility bill, or CA DMV registeration
– Apply in person and pay the fee. Typically $100, or
$50 for Medi-Cal beneficiaries
22
The Who, What, Where, When, Why and How of Medical Marijuana in Pediatric Palliative care. Elissa Miller, Tressia Shaw, Matthew Troester, Billie Wiegard
23
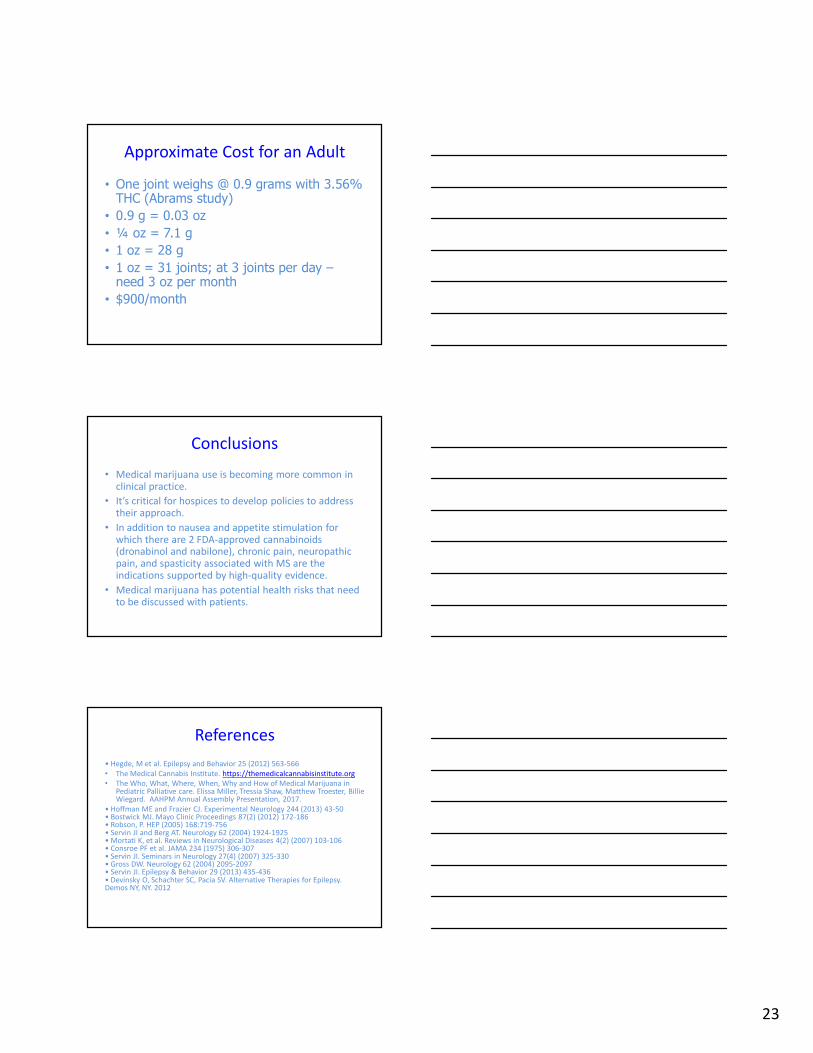
Approximate Cost for an Adult
• One joint weighs @ 0.9 grams with 3.56% THC (Abrams study)
• 0.9 g = 0.03 oz
• ¼ oz = 7.1 g
• 1 oz = 28 g
• 1 oz = 31 joints; at 3 joints per day –need 3 oz per month
• $900/month
Conclusions
• Medical marijuana use is becoming more common in clinical practice.
• It’s critical for hospices to develop policies to address their approach.
• In addition to nausea and appetite stimulation for which there are 2 FDA-approved cannabinoids (dronabinol and nabilone), chronic pain, neuropathic pain, and spasticity associated with MS are the indications supported by high-quality evidence.
• Medical marijuana has potential health risks that need to be discussed with patients.
References
• Hegde, M et al. Epilepsy and Behavior 25 (2012) 563-566
• The Medical Cannabis Institute. https://themedicalcannabisinstitute.org
• The Who, What, Where, When, Why and How of Medical Marijuana in Pediatric Palliative care. Elissa Miller, Tressia Shaw, Matthew Troester, Billie Wiegard. AAHPM Annual Assembly Presentation, 2017.
• Hoffman ME and Frazier CJ. Experimental Neurology 244 (2013) 43-50• Bostwick MJ. Mayo Clinic Proceedings 87(2) (2012) 172-186• Robson, P. HEP (2005) 168:719-756• Servin JI and Berg AT. Neurology 62 (2004) 1924-1925• Mortati K, et al. Reviews in Neurological Diseases 4(2) (2007) 103-106• Consroe PF et al. JAMA 234 (1975) 306-307• Servin JI. Seminars in Neurology 27(4) (2007) 325-330• Gross DW. Neurology 62 (2004) 2095-2097• Servin JI. Epilepsy & Behavior 29 (2013) 435-436• Devinsky O, Schachter SC, Pacia SV. Alternative Therapies for Epilepsy. Demos NY, NY. 2012