MEDICAL RECORDS: DOB 6/17/11; HOSPITALIZED 1111-11/10/11 PRENATAL Note: I didn't include all basic twin exams - all normal. DATE MED SOURCE NOTES 1110 Med 397- Labs All normal 398 2118 Med 424- MVA reports - 28 yr female 20 wks pregnant, viable twins 433 - MV A just prior to arrival - Moderate abdominal pain - Driving car, wearing lap belt & shoulder harness; impact on front & rear of vehicle, air bag deployed, low impact velocity [rearended, then hit car in front] - No vomiting, headache, etc. - Slight abrasion from airbag - Recommend fetal heart monitoring on L&D - DX: abrasion & contusion to abdomen - Pain level 511 0, lower abdominal - Labs: fibrinogen 496 (150-400; d-dimer 2549 (0-500) - Note: Med 43-48 indicates fetal blood in circulation 2/21 Med 396 Labs Normal except RDW & MPV slightly high. 4/22 Med 395 Labs All normal 5/23 Med406 Twin Active twins, scores 8/8 BPP/Amnio 5/31 Med407 Twin Both fetuses vertex; normal; scores 8/8 BPP/Amnio 5/31 Med 393- Labs Some slight abnormalities; platelets, 394 creatinine, C02, protein, albumin slightly low. Alkaline phosphatase 233 (33-115). Cholic acid 3.7 (under 3.1). 6/2 Med 404- BPP/Amnio Reason for study: dichorionic twin gestation, 405 cholestasis, BPP. Total score 8/8. 6/6 Med 401 Twin basic exam Active twins; appropriate concordant growth, weight discordance 7% 6/13 Med 402 Amnio Active twins, total score 8/8 for each 111 0-6113 Med 422- Ob/gyn records Notes; hard to read; nothing out of ordinary 423 (delivered 6/17) 1
Transcript
MEDICAL RECORDS:
DOB 6/17/11; HOSPITALIZED 1111-11/10/11
PRENATAL
Note: I didn't include all basic twin exams - all normal.
DATE MED SOURCE NOTES 1110 Med 397- Labs All normal
398
2118 Med 424- MVA reports - 28 yr female 20 wks pregnant, viable twins 433 - MV A just prior to arrival
- Moderate abdominal pain - Driving car, wearing lap belt & shoulder
harness; impact on front & rear of vehicle, air bag deployed, low impact velocity [rearended, then hit car in front]
- No vomiting, headache, etc. - Slight abrasion from airbag - Recommend fetal heart monitoring on L&D - DX: abrasion & contusion to abdomen - Pain level 511 0, lower abdominal - Labs: fibrinogen 496 (150-400; d-dimer
2549 (0-500) - Note: Med 43-48 indicates fetal blood in
circulation 2/21 Med 396 Labs Normal except RDW & MPV slightly high. 4/22 Med 395 Labs All normal 5/23 Med406 Twin Active twins, scores 8/8
BPP/Amnio 5/31 Med407 Twin Both fetuses vertex; normal; scores 8/8
BPP/Amnio 5/31 Med 393- Labs Some slight abnormalities; platelets,
Four prior term deliveries (1 prior surrogate) Due date: 7/7 Born: 6/17 37 weeks 1 day 6/23: mother low HGB, HCT Rupture time 7:31 pm Induced with oxytocin
(1 st twin): 7 lbs, 3 OZ; spontaneous vaginal del, 10:02 pm AJ (2nd twin): 6lbs 10.9 OZ; spontaneous vaginal delivery, 11 :05 pm Delivering physician: Providers: birth nurse; Pediatrician Wt 3030 g; length 50.8 cm; hc 35 cm Pediatrician concerned re large swelling on front forehead; shown in pictures. Pediatrician references at Med 8 and 363-4 (he took photo to hospital after admission). Family hx (surrogate) Meds: progesterone, gelestrogen? Prenatals Surrogate hx: UTIs, kidney stones, 2000 cervical cancer, negative after pregnancy - Discharge: twin pregnancy; immediate
postpartum hemorrhage - Problem list: twin pregnancy; immediate
postpartum hemorrhage with delivery; tricuspid regurgitation; acute posthemorrhagic anemia - severe hemorrhage after 2nd twin requiring balloon tamponade of uterus, PRBC
- Hypertension (unclear if from volume overload state or late presentation of eclampsia)
- BP higher than pre-pregnancy - Med hx: varicella, MRSA (pt. thinks
cleared) - Discharge dx (439): twin pregnancy,
immediate postpartum hemorrhage with delivery, acute posthemorrhagic anemia, hypertension
- Ambulating & planned discharge day 2 - Requested spiritual care 6/18 - Lab tests (platelets slightly low, MPV
2
slightly hi) (445) 6/17-6/18 Med 495 Med records Oxytocin infusion 20 units/lOOO mL NS. 12:52 pm Begin at .5-1 mLiminute; increase by 1-2 to 2:05 am mLimin every 30 min. according to fetal
response and uterine activity, avoiding tachysystole or until max of 20 mLimin. is reached; piggyback onto existing IV. Note: oxytocin continued 6/18 1 :20 am-6/19 4:52 pm. Other meds not noted.
6/17 Med447- Anesthesia Complications: excessive maternal bleeding 452 records due to atony of lower uterine segment.
Rec'd 80 units pitocin in IVF, 800 mcg cytotec PR, .25 mg hemabate 1M, .2 mg methergine 1M, which still did not resolve the atony. Tamponnaded; discussed possible need for uterine artery embolization but bleeding slowed on its own.
6/18 Med 399- Surgical Summary of sections (umbilical cord, fetal 400 pathology membranes, parenchyma); full report [I don't
know significance] 6125 Med 514 Problem list, Problem list: (rev'd) Kevin - Twin pregnancy (37 or more wks)
MDPhD - Immediate postpartum hemorrhage - Acute posthemorrhagic anemia - Hypertension - Proteinuria (due to concerns for late
manifestation of eclampsia, underwent 24 hr urine protein collection; 1130 mg/day of protein; no renal failure or neurologic signs; followup BP)
- Resolved: pulmonary hypertension, moderate to severe
BIRTH RECORDS: __
NOT AVAILABLE
3
PEDIATRIC
6/30 Med 363- Well child 2 - Wt. 7.03 lbs (1ih %) 364 week check (Dr. - Ht 20.5 in (47%)
- HC 35 cm (16%) - Good nippIer - frontal presentation swelling way down - anterior fontanelle flat & soft - 37 weeker doing great
Med 366- Discharge from - Admission provider: 367 Legacy Good - Follow up with MD, call in 1
Samaritan day (gives Portland address) Nursery
Med 368- Newborn Normal 9 screenmg
717 Med 370- Weight Wt. 7lbs 14 oz [no hc] 371 checklPKU Excellent growth 37 weeker; expect more
demand, always add a bit more 8115 Med 372- 2 month check 111bs 5 oz (47%)
373 Ht 22.75 in (49%) HC 38.99 cm (31%) Weight for length: 35% Vaccines (see below) Excellent growth, 37 wk twin, recheck 4 mos
10/20 Med 374- 4 mo check 14.691bs (45%) 375 Ht: 26.5 in (93%)
HC: 41.5 cm (29%) AF open & flat Recheck at 6 mos; may start cereal Vaccines (see below)
10/20 Med 376 Vaccine record Pentacel vaccine 1 & 2 (combined DTap, IPV, HIB); pneumococcal vaccine 1&2; rotavirus 1&2 (all 3 on 10/20) ...
PEDIATRIC: 1111111
November Med 1-3 Pediatric records 14.8 lbs, 99.7 F 1 Vomiting, dehydration
Very lethargic since vomited 3 pm yesterday 3 pm feeding, about 1 hr later vomited all Vomited 6 pm, 9 pm, 5 am Also vomited during night Cap refill under 2 sec Gave 1 oz pedialyte at exam; vomited forcefully CBC with left shift; WBC 25 (4.5-10.5); Pit
4
1111
1111 9:44 am
Med4-A
Med 379
Ped records
Ped records
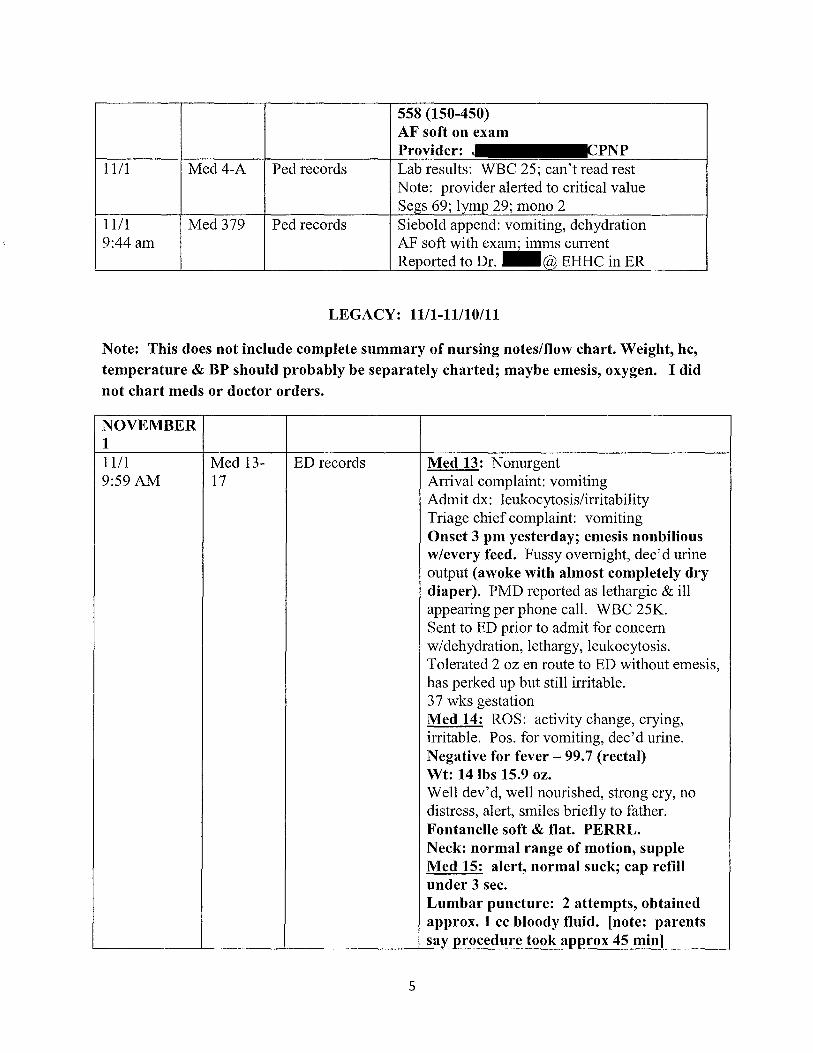
558 (150-450) AF soft on exam Provider: Lab results: WBC 25; can't read rest Note: provider alerted to critical value
69; 29; mono 2 Siebold append: vomiting, dehydration AF soft with exam; imms current
pnnrTPrI to Dr. _ EHHC in ER
LEGACY: 1111-11/10/11
Note: This does not include complete summary of nursing noteslflow chart. Weight, he, temperature & BP should probably be separately charted; maybe emesis, oxygen. I did not chart meds or doctor orders.
NOVEMBER 1 1111 Med 13- ED records Med 13: Nonurgent 9:59AM 17 Arrival complaint: vomiting
Admit dx: leukocytosis/irritability Triage chief complaint: vomiting Onset 3 pm yesterday; emesis nonbilious w/every feed. Fussy overnight, dec'd urine output (awoke with almost completely dry diaper). PMD reported as lethargic & ill appearing per phone call. WBC 25K. Sent to ED prior to admit for concern w/dehydration, lethargy, leukocytosis. Tolerated 2 oz en route to ED without emesis, has perked up but still irritable. 37 wks gestation Med 14: ROS: activity change, crying, irritable. Pos. for vomiting, dec'd urine. Negative for fever - 99.7 (rectal) Wt: 14 lbs 15.9 oz. Well dev'd, well nourished, strong cry, no distress, alert, smiles briefly to father. Fontanelle soft & flat. PERRL. Neck: normal range of motion, supple Med 15: alert, normal suck; cap refill under 3 sec. Lumbar puncture: 2 attempts, obtained approx. 1 cc bloody fluid. [note: parents say procedure took approx 45 min]
5
ED course: alert, active, warm, but prefers to be held. No obvious source of infection; no signs of serious bacterial illness such as lethargy, bulging fontanelle. Will evaluate blood & urine for infection; IV hydration per dec'd wet diapers. LP delayed since pt smiling, waited for labs. WBC 31 K, 66% neutrophils. UA neg. for infection but spec grav 1.020 & + ketones. RN reports very scant wet diaper (1 st since overnight); tolerated 5 oz w/o emesis but parents say seems sick; need inpatient monitoring given dehydration Med 16: disc'd possibility of meningitis; viral illness such as gastroenteritis also possible. Plan LP due to possible meningitis, chest x-ray for occult pneumonia. Low grade fever 37.9 in ED. Traumatic LP with insufficient quantity for cell count; obtained culture. PMD agrees with plan per call. Spoke with peds hospitalist, pending cultures; ceftriaxone while cultures pending. No further LP required as culture available. ED DX: vomiting, irritability, dehydration Med 17: onset of vomiting 3 pm yesterday
1111 Med 382 Note to Dr. - Thank you for referring 10:08 am from - Chief complaint: leukocytosis
Emanuel - Attending: J Childrens - Admit: 10:08 am
1111 Med 214 Nursing notes, - Awakens easily, alert, smiles 10:25 am flow chart 1111 Med 214 Nursing notes, - Took 60 ml at clinic, vomited 10:28 am flow chart - Scant wet diaper now, brick tinged spots in
diaper 1111 Med 236- VA labs - Ketones 3+ (negative); trace albumin; rare 10:55 am 237 bacteria; few amorphous
- Well nourished, healthy appearing, vigorous; easily consoled, making tears. AF normal, flat; PERRL. Deferred ear exam due to no otoscope in room (39)
Nursing notes, flow chart (emesis assessment) (may be Pediatric records
Progress notes, Allison MD [signed by
with addendum]
8
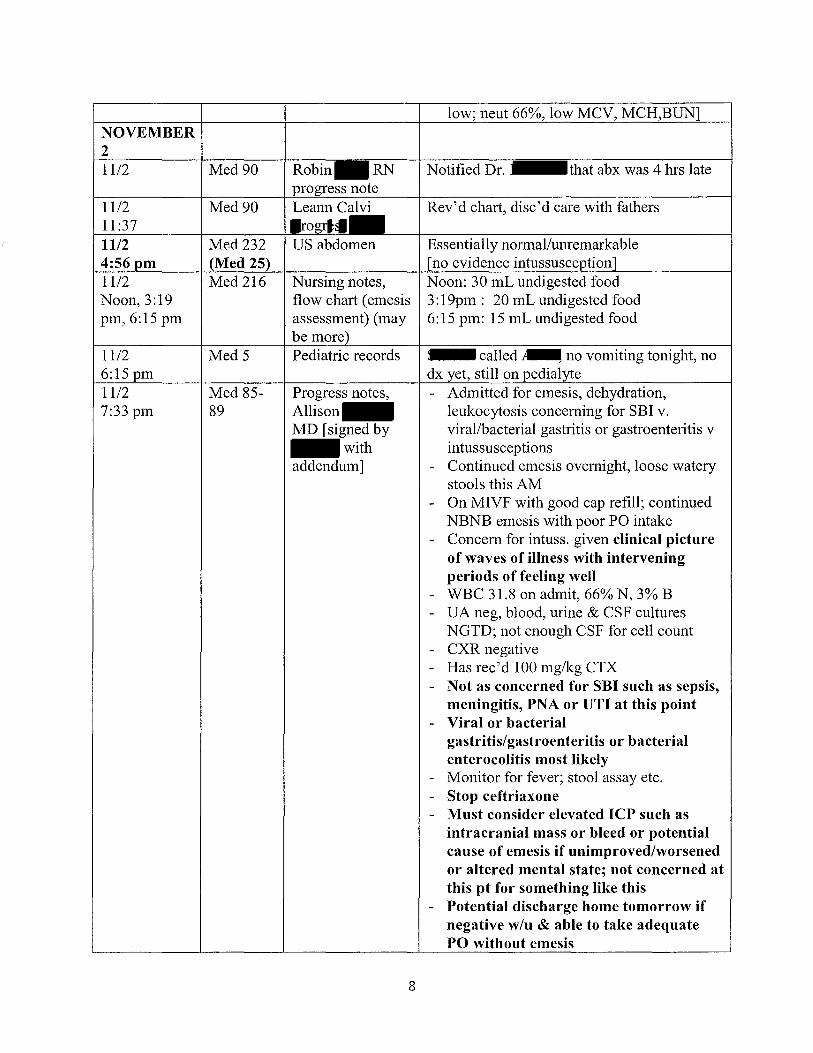
Notified Dr. that abx was 4 hrs late
Rev'd chart, disc'd care with fathers
Essentially normal/unremarkable evidence'
Noon: 30 mL undigested food 3: 19pm: 20 mL undigested food 6:15 pm: 15 mL undigested food
: dx
called ~ no vomiting tonight, no still on
- Admitted for emesis, dehydration, leukocytosis concerning for SBI v. virallbacterial gastritis or gastroenteritis v intussusceptions
- Continued emesis overnight, loose watery stools this AM
- On MIVF with good cap refill; continued NBNB emesis with poor PO intake
- Concern for intuss. given clinical picture of waves of illness with intervening periods of feeling well
- WBC 31.8 on admit, 66% N, 3% B - VA neg, blood, urine & CSF cultures
NGTD; not enough CSF for cell count - CXR negative - Has rec' d 100 mg/kg CTX - Not as concerned for SBI such as sepsis,
meningitis, PNA or UTI at this point - Viral or bacterial
gastritis/gastroenteritis or bacterial enterocolitis most likely
- Monitor for fever; stool assay etc. - Stop ceftriaxone - Must consider elevated ICP such as
intracranial mass or bleed or potential cause of emesis if unimproved/worsened or altered mental state; not concerned at this pt for something like this
- Potential discharge home tomorrow if negative w/u & able to take adequate PO without emesis
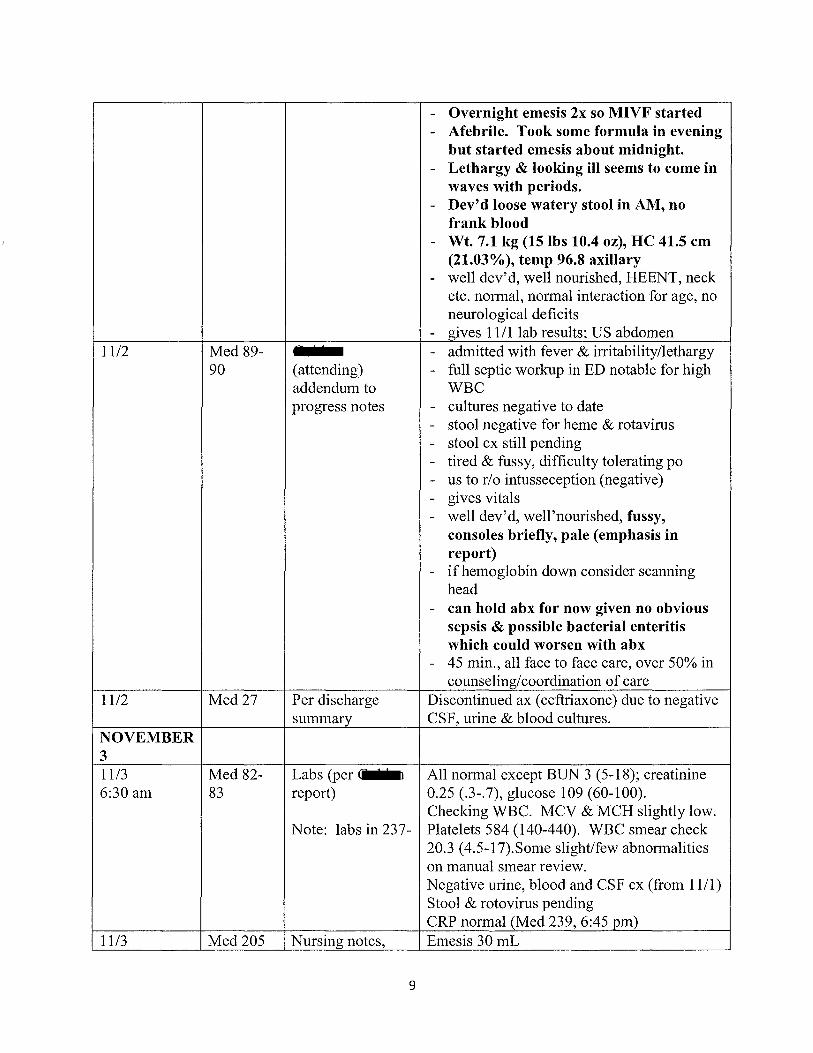
- Overnight emesis 2x so MIVF started - Afebrile. Took some formula in evening
but started emesis about midnight. - Lethargy & looking ill seems to come in
waves with periods. - Dev'd loose watery stool in AM, no
frank blood - Wt. 7.1 kg (15 lbs 10.4 OZ), He 41.5 cm
(21.03%), temp 96.8 axillary - well dev'd, well nourished, HEENT, neck
etc. normal, normal interaction for age, no neurological deficits
- gives 1111 lab results; US abdomen 1112 Med 89- - admitted with fever & irritability/lethargy
90 ( attending) - full septic workup in ED notable for high addendum to WBC progress notes - cultures negative to date
- stool negative for heme & rotavirus - stool cx still pending - tired & fussy, difficulty tolerating po - us to rio intusseception (negative) - gives vitals - well dev'd, well'nourished, fussy,
consoles briefly, pale (emphasis in report)
- if hemoglobin down consider scanning head
- can hold abx for now given no obvious sepsis & possible bacterial enteritis which could worsen with abx
- 45 min., all face to face care, over 50% in counseling/coordination of care
11/2 Med27 Per discharge Discontinued ax (ceftriaxone) due to negative summary CSF, urine & blood cultures.
NOVEMBER 3 11/3 Med 82- Labs (per c.J(~ All normal except BUN 3 (5-18); creatinine 6:30 am 83 report) 0.25 (.3-.7), glucose 109 (60-100).
20.3 (4.5-17).Some slight/few abnormalities on manual smear review. Negative urine, blood and CSF cx (from 11/1) Stool & rotovirus pending CRP normal (Med 239,6:45 pm)
11/3 Med 205 Nursing notes, Emesis 30 mL
9
10 am flow chart 11/3 Med6 Pediatric records: 2:17pm: I
7 " (hospitalist) called _;
2:17 pm, 4:37 phone calls doing better, probably send home today, pm _&~ wanted to go over a few things, not urgent.
4: 37 pm: ret'd call; high blood pressure, kidneys OK, blood & output looking good, smiling; renal artery US for stenosis, abdomen US okay; HC fine; a little spitty. Plan discharge if renal artery scan normal, check BP, consider renal followup
11/3 Med 232 Renal sonogram Clinical: hypertension 5:42pm Findings; impression:
- mostly normal; reflux not excluded on basis of US alone
- 2 right renal arteries, only solitary left renal artery; no evidence for hemodynamically significant unilateral renal artery stenosis as explanation for hypertension
- Minimal left renal pyelectasis of .4cm, WNL variability
- Dependent debris in urinary bladder nonspecific
- Otherwise unremarkable renal study 11113 Med 80- Progress notes, - Emesis, dehydration & leukocytosis
84 , concerning for SBI v. virallbacterial MD, Pediatrics, gastritis or gastroenteritis vs. signed by C J J intussusception with addendum - Most likely etiology at this time is viral
gastroen teritis - Good PO intake, last emesis 6 pm 1112 - Concern for possible intussusception
given clinical picture of waves of illness with intervening periods of feeling well yesterday but abd US negative
- WBC 31.8 on admit, 66% N, 3% B - Has rec' d 100 mg/kg CTX in ED - Not as concerned for SBI such as sepsis,
meningitis, PNA or UTI - Viral AGE most likely but cannot rule
out viral meningitis since not enough CSF for cell count
- Afebrile w/unaltered mental status - Normal BPs on admit & 11/2; elevated
systolic BP this AM of 122; extremity BPs L arm 120/77, R arm 112/76, L le~
10
117/65, R leg 124/95 - Potential discharge to home today pending
results of renal US - Last emesis 6:15 pm 11/2 but lost IV; not
replaced, IVF stopped. Loose stools resolved, baby has more energy.
- HC 41.5" (21.03%); wt. 15lbs 10.4 oz - Gives vitals; intake/output - Intake 721.67 ml, output 263 m1 (82) - HEENT & neck normal See labs above (11/3, 6:30 AM)
11/3 MED232 CT-Head Clinical: skull fontanelle hypertension 7:17 pm [Med 25) Findings: scattered small volume left cerebral
convexity SDH; no mass effect or midline shift, no IPH or IVH. CSF space at each frontal convexity maintained, normal appearance cortical sulci at vertex. No herniation, no fx. Consider NAT for SDH in child this age. Radiologist discussed with at 7:25 pm. Note: also sees small amt SDH in posterior falx and over tentorium, left greater than rh!ht (Med 362)
11/3 Med84 - Child examined multiple times over day 8:47pm (attending) - Concern re elevated blood pressures
addendum to - Early in day baby smiling, feeding well progress note - Unlikely CNS lesion responsible for
elevated BP; gives BPs for arms/legs - No murmur, good pulses, so renal problem
seemed most likely cause; renal us ordered - Prior to us, more emesis again - After us exam seemed to have changed
markedly: fontanelle full but not tense - Pupils reactive but eyes sundowning to
some extent, less interactive - Tachycardic w/o murmur, abdomen soft,
not tender, tone normal - Given change, ordered stat head CT,
replaced PIV, got a CRP - CT: small left SDH wino midline shift, no
hydrocephalus - Called CARES NW, rec'd skeletal
survey, coags & ophtho consult tomorrow
- & told, understandably upset, no
11
known trauma or falls - Baby in care of nanny Natalie last Fri,
otherwise with - Discussed w/ who will review scan,
unlikely to require neurosurgical interv. - Restart IV, monitor, neurochecks - Strict i/o given risk for SIADH/DI - Recheck lytes in AM
NOVEMBER 4 11/4 Med 7 call to Didn't look right after renal artery study 9:10 am [pediatric Bulging fontanel, urgent CT, SDH
records] Workup to continue 11/4 Med 128 Nursing notes NPO forMRI 10:51 am Had been rec'g Y2 strength similic sensitive
mixed with pedialyte Only tolerating around 1 oz before vomiting
1114 Med 79- Nutrition Progress Pt at nutritional risk secondary to new onset 11:31 80 Note, Tara vomiting & feeding intolerance, etiology
unknown Currently NPO for MRI Growth chart appropriate (15-50th %) Today is day 5 wlinadequate intake Rec's feeding plan w/daily weight checks
11/4, Med240 Blood draw- All normal except creatinine .2 (.3-.7); 12:40 pm metabolic panel glucose 117 (60-100) 11/4 Med 18- Summary/problem Problem list as of 1114:
Note: this may have been when they were considering discharge
1114 Med 145 JM nursing note, Baby happy today and playful 1:30pm flow sheet 11/4 Med 233 MRI Brain Patchy left SDH corr' g to CT. 1:31 pm [Med 26] Smaller focal SDH on right (in retrospect
present on CT). Age: 3 days to 1 week (subacute) Curvilinear area of extra axial signal on posterior left parietal lobe; est. 8 - 72 hrs. No evidence of chronic SDH; no SAH, EDH, IVH, IPH. Brain normal, no edema,
12
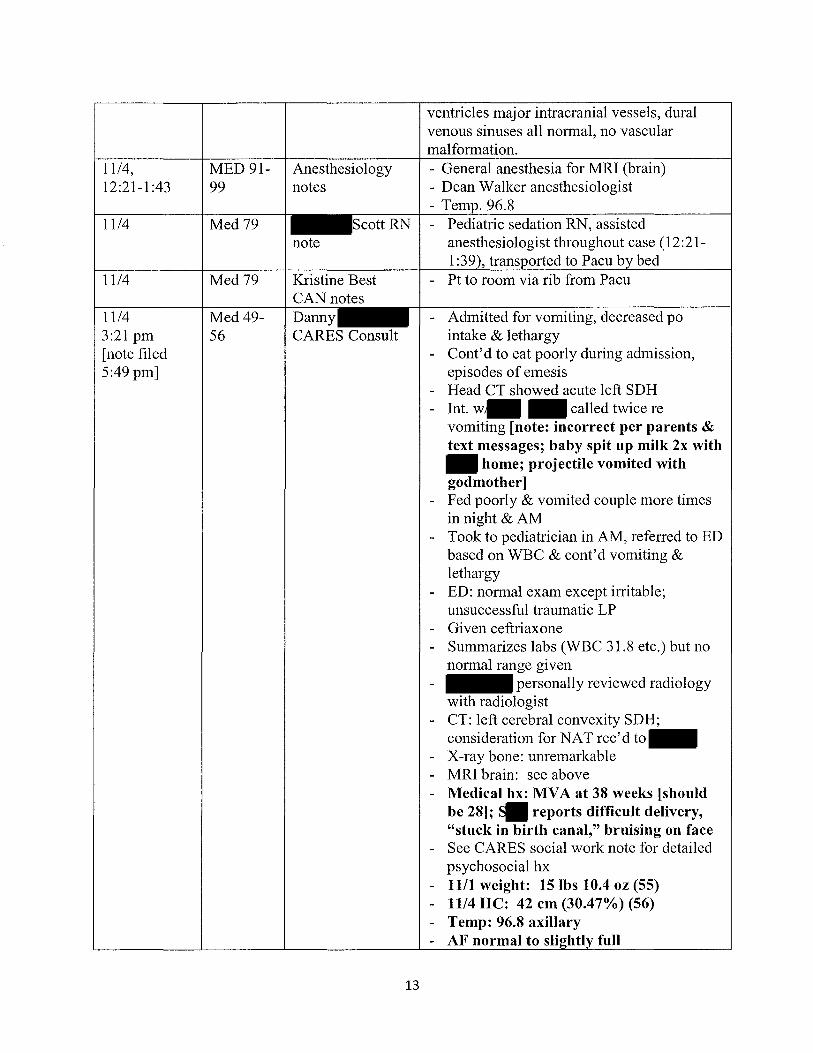
ventricles major intracranial vessels, dural venous sinuses all normal, no vascular malformation.
11/4, MED 91- Anesthesiology - General anesthesia for MRI (brain) 12:21-1:43 99 notes - Dean Walker anesthesiologist
- Temp. 96.8 11/4 Med 79 Scott RN - Pediatric sedation RN, assisted
note anesthesiologist throughout case (12:21-1 :39), transported to Pacu by bed
1114 Med 79 Kristine Best - Pt to room via rib from Pacu CAN notes
11/4 Med 49- Danny - Admitted for vomiting, decreased po 3:21 pm 56 CARES Consult intake & lethargy [note filed - Cont'd to eat poorly during admission, 5:49 pm] episodes of emesis
- Head CT showed acute left SDH - Int. w/ called twice re
vomiting [note: incorrect per parents & text messages; baby spit up milk 2x with
home; projectile vomited with godmother]
- Fed poorly & vomited couple more times in night & AM
- Took to pediatrician in AM, referred to ED based on WBC & cont'd vomiting & lethargy
- ED: normal exam except irritable; unsuccessful traumatic LP
- Given ceftriaxone - Summarizes labs (WBC 31.8 etc.) but no
normal range given - personally reviewed radiology
with radiologist - CT: left cerebral convexity SDH;
consideration for NAT rec' d to - X-ray bone: unremarkable - MRI brain: see above - Medical hx: MVA at 38 weeks [should
be 28]; S reports difficult delivery, "stuck in birth canal," bruising on face
- See CARES social work note for detailed psychosocial hx
- 1111 weight: 151bs 10.4 oz (55) - 1114 He: 42 cm (30.47%) (56) - Temp: 96.8 axillary - AF normal to sli~htly full
13
- Acute/subacute bilateral SDH w/o identifiable medical etiology or significant traumatic hx concerning for AHT, part'ly w/ clinical symptoms
- have rec'd bleeding disorder studies, though SDH & clinical findings would be extremely unusual in isolation as a result of a bleeding disorder
- normal skeletal survey; unfortunately does not exclude AHT since Yz-2/3 infant AHT victims do not have fx; need 2 wk followup
- have disc'd with parents & treating medical team concern that findings are result of AHT; referred to Washington CPS, disc'd concerns with CPS & LEA investigators (57)
- total time: 140 minutes 11/4 Med 109- Lakindra Met w/ alone (109: Note: pg 113 MSW, CARES - reports that called re vomiting; before Med these notes are muddled/incorrect on 109 missing timing (per parents & text messages) so no - says called twice, AJ wouldn't indication of eat around 3 pm, hr later reported time vomiting; unusual, onset of symptoms
rapid, AJ had eaten by time came from work
- sent text saying AJ vomited again; AJ limp & lethargic when arr'd home, new cry (subtle whimper), called godmother & daughter to come over
- Godmother fed around 9 pm, projectile vomiting
- Thought AJ sick, twins not sick before - Up couple times in night, could soothe - Fed AJ in morning, vomited - Went to dr office around 7:45, then ER - Twins only out of care on 10/28 (Fri), LA
Fitness Kids Club; Natalie cared for twins 2-6:30 pm
- Sat. aunt & cousin cared around 2 hrs while & went to class
- Both fine over weekend, no trauma - Met with alone (1l0-1l3} - Normal feeding around 10:30-11, then
napped
14
- At 3, AJ started eating but inconsolable, swaddled, looked lethargic, normal temp. but felt cold/clammy
- Called told him AJ not feeding, not typical
- came home around 4:30, tried to feed, AJ in rocking chair, vomited ( said projectile, never happened before)
- ret'd around 6:30, AJ swaddled in swing, "threw up" down front of shirt
- They thought some sort of virus - Danielle came over around 7:30-8, she was
feeding AJ, projectile vomiting - AJ up off & on during night - talked to mom in AM, got pedialyte - AJ looking pale, took to pediatrician - Everything fine prior to 10/31 at 3 am, no
falls, etc. - Birth hx: conceived in vitro, anonymous
-egg donor, surrogate mom Vaginal delivery 37 weeks; AJ 2nd twin, head stuck in birth canal, slightly deformed
- Healthy, came home 2 days after birth - At 28 weeks of pregnancy, car accident,
car totaled (rear ended), followed by medical providers, everything fine
- again (111): not lot of info re egg donor, no known genetic disorders
- describes routine, fed 5 x day, half breast milk, half formula
- & together about 4 Yz yrs; planning to have children past 3 yrs, considered adoption & foster; took about yr to find egg donor
- chiropractor, teaches yoga - chiropractor asst, teaches yoga - Own clinic together - staying home full time with twins,
went back to work TueslFri afternoon; started teaching yoga about 3 wks ago
- & primary caretakers. Found Natalie through Sitter City; elementary school tchr wl7 yrs experience with children; has been caring for twins past 6 wks. Monday 7 -9 pm; TueslFri 2-6:30
15
pm; last time was 10128) - no concerns with abuse/neglect - no family stressors; enjoys being at-
home dad; good support system - had doula 2 12 wks, then no longer needed
- for 1st 4-6 wks, AJ more cranky; his mother (nurse) thought something not right; uncomfortable, difficult to swaddle/soothe, inconsolable at times. At 6 wks, flipped like light switch. PCP said no need for concern.
- AJ happy, bubbly, feisty baby - SDH discovered; in normal health until
10/31; not aware of any falls, drops, accidents, trauma
- Kim Karu is DHS caseworker; DHS has temporary legal custody, will dev. discharge plan; CARES NW will follow
11/4 Med 233 X-Ray Skeletal No fx or dislocations 3:52 pm (Med 25) Survey 11/4 Med 79 CARESNW - met with & separately to gather 4:37 social work note, history
Lakindra - full CARES social note to follow MSW
1114 Med 57- Neurosurgery - healthy 4 12 mo baby admitted 3 days ago 5:20pm 58 consult, Jenny with briefhx dec'd feeding, vomiting,
(?) & decreased urine output, sleepiness, possible low grade fever
- fully worked up for 01 & infectious issues - was improving yesterday to extent
discharge seemed likely but dev'd persistent elevated BP, began vomiting
- CT showed small SDH under left suture - AF soft but somewhat full - Small left frontal SDH evident on MRI;
smaller right frontal SDH, no infarcts - workup underway - no known trauma - SDH do not appear large enough for
drainage; ifbaby doesn't improve, drainage could be considered
1114 Med 48- Pediatric - SDH prompted NAT eval 7:29 PM 49 Ophthalmology - Admitted 3 days prior; reportedly well
Consult, David prior to event; elevated WBC & mildly WheelerMD elevated platelets on admission
- Quiet healthy appearing infant
16
- Extensive RH in posterior pole, both eyes, extending to at least mid periphery
- Most appear intra retinal; some involving NFL
- Peripapillary hemorrhages in both eyes, etc
- Appear to be areas of mild edema along vascular arcades, esp inferiorly, w/mottled appearance of nearly confluent very small hemorrhages; no specific changes suggesting vasculitis; both nerves flat with normal color, sharp borders
- Multiple RH both eyes, somewhat atypical in appearance & distribution for any specific disease process I have seen
1114, Med 74- Progress Notes - Head CT shows small SDH 8:39 pm 78 Allison - Initial eval was gastroenteritis; now with
(signed by confirmed SDH, concerning for NAT v see bleeding d/o v metabolic d/o
addendum) - Will obtain MRI to look for any vascular anomalies
- Monitor mental status, observe BPs/HRs for possible Cushings triad
- Check Schunk's office for past head circs
- Coag panels pending - Assess for metabolic causing spontaneous
bleeds - Initial concern for intussusception given
clinical picture of waves of illness with intervening periods of feeling well; but abd US negative
- Continued emesis; afebrile - Infectious component not as likely given
SDH - Elevated systolic BP on 1113 of 122 (L
arm 120/77, R arm 112/76, L leg 117/65, R leg 124/95)
- Discharge on hold while cause of SDH investigated
- After renal us yesterday evening, dev'd bulging fontanelle conc'g for possible intracranial process causing emesis
- CT showed small SDH - Parents report AJ continues to vomit,
17
IVF restarted - Appears lethargic but responsive - Report surrogate mother in MV A at 28
wks, fetal blood in circulation - HC 41.5 em (21st %); temp 98.4 axillary;
wt 7.1 kg, 151bs 4 oz - Neck supple; AFO and bulging slightly - 1111 urine, blood & CSF cultures negative;
1114 Med 140 Nursing notes, - Report low heart rate by cell 8:45 pm flow chart - Orders rec' d & implemented 11/4 Med 78 Eve - Rev'd MRI & skeletal survey 11:25 pm Addendum - Met with family multiple times, consulted
with & - Still very fussy in day but improving in
evening, taking better PO - MRI confirms SDR, dates 3-7 days - RR unusual from Wheeler's perspective - Family distraught re ART - DRS called, int' g parents - Continuing to work up metabolic (esp GA
type 2) and coag, thought unlikely since no other bleeding in hx
- Trying to support family thru difficult time while remaining open to all diagnostic possibilities
- Wt. 6.965 kg (15 lbs. 5.7 oz); HC 42 em - AF puffy but soft - Continue workup for unexplained
SDH/RH - Spent 60 min
1114 Med 122- Metabolic Panel - All WNL except creatinine .2 (.3-.7), 123 (from 11/7 notes) glucose 117 (60-100)
- Collagen, PT/PTT/INR normal 1114 Med22 MRI discussed - Radiologist (John Gustavsson) discussed 2:20pm with final MRI report with at 2:20
pm NOVEMBER -5 1115 Med 251- Amino Acids - MostlyWNL 5:30 am 254 screen - Pyruvic acid 1143 (0-30)
checking factors 9 & 13. There are several very rare conditions that can present with normal PT/PTT: in absence of family hx & add'l bleeding history, would not pursue at this time. (44) may need to repeat some tests at 6-9 mos when factor levels closer to adult norms; VW may need several repeats (44) Repeats history. Surrogate mo reportedly in MV A at 28 weeks; fetal blood found in her circulation. Meds: zofran; vanponefrin; albuterol; atropine; acetaminophen; dextrose; Benadryl (45-46) Wt: 6.965 kg (151bs 5.7 Oz) He 30.47% percentile Temp: 96.8-99.1 F (46) (47) HEENT: normocephalic, atraumatic,
19
AFO and bulging slightly WBC pending; Plt 584 Summarizes CT, MRI, bone survey (48)
IllS Med 68- Progress notes, - BPs and HRs still somewhat variable clw 9pm 73 Eve some increased ICP, will monitor until
stable - Fontanelle still full but soft - More alert - Reviews ophthal, radiology, etc. - Metabolic: glutaric aciduria is possibility
but certainly quite rare and unlikely - Will be ready for dlc when
hemodynamically stable, normal BP & hr and feeding well
- Improving, better PO but still some emesis & some abnormal bps & lower hrs. No obvious elevated ICP at this time; definitely more alert and interactive
- HC 42 cm, temp 99 (axillary), weight 6.965 kg (l5lbs 5.7 oz), BP 84-125/42-73.
- Labs: fibrinogen, lipase, collagen epinephrine normal (71)
- Spent 45 min, 80% face-to-face with father & grandparents
NOVEMBER 6 11/6 Med8 visit to See IllS (not clear what occurred at which
hospital. visit; written up 11/6) 11/6 Med 42- Danny - Stable overnight wlo doc'd emesis 11:54 am 43 CARES consult - Fibrinogen, platelet function normal
- Waiting on VW, Factor 13, thrombin - Have seen ophthal rpt describing extensive
bilateral RH in posterior pole extending to at least midperiphery; do not see folds of retionoschisis doc' d
- haven't been able to talk to ophthal - based on documentation, remain conc'd
that presentation is result of AHT - RH not specific to AHT, but am't of
hemorrhages & extension to mid periphery is certainly concerning
- Would not expect these hemorrhages to be seen in a coagulopathy or natural disease process
20
- Will wait for coag evals 1116 Med 64- Progress notes, - admitted for vomiting/lethargy; found to 12:57 pm 68 Eve MD have SDH &B BL RH after being
(hospitalist) hypertensive & lethargic - not great po; only % maintenance
yesterday, weight down about 90 grams - BPS and HRs somewhat variable c/w
increased rcp - Fontanelle still full but soft - More alert today - Reviews labs, radiology - Stable but still fussy at times - Brought in video of bouncy seat w/o head
support, wondered if this could cause; didn't think so but defer to
- HC 42 cm; temp 98.1 ancillary - Meds: zofran, Tylenol, dextrose, Benadryl - 30 min. clinical time, over 50% in
counseling & Y coordination of care, 80% face-to-face interaction
1116 Med68 Monica - VSS, total po better today 1:03 pm Neurology/ - More active
1116 Med 133 Nursing notes, - Total vol. 565 ml yesterday. 14 feedings 1:51 pm flow sheets recorded 1115 with max vol. 60 ml at one
feeding. 1116 Med 63- Nutrition progress - high nutritional risk due to poor feeding 2:10pm 64 note, Sarah Lowe - total PO intake yesterday approx 50% of
est. needs - fortification of feeds indicated - wt gain goal of 15-20 g/d average
11/6 Med 137 1M nursing notes, - baby has been happy today and playful 3:45pm flow sheet 11/6 Med42 - Disc'd RH w/ by phone 11:20 pm CARES report - Bilateral RH primarily in posterior pole
but some further into periphery - No retinoschisis or retinal fold - Did not see multilayered too numerous to
count extending to ora serrata, which would have strong association with AHI
- some hemorrhages had atypical appearance, didn't know significance
- agreed that eye findings not dx for AHT but compatible/consistent w/AHT do not feel repeat exam would yield
21
significant new info but will leave decision to treating medical team
NOVEMBER -7 1117 Med 119- Allison - usual repetition (init'ly thought 7:45 am 124 Progress Note, gastroenteritis; confirmed SDH concerning
with for NAT v bleeding dlo v metabolic d/o) addendum - Feel pt may be able to go home today with
safety plan - Today's wt 6.545 kg (down 345 g from
yesterday), reweigh 2 pm - Plan to discharge home with daily weight
checks by pending CARES final recs & wt check this pm (120)
- No acute events; says much more alert & happy, more like himself
- Last emesis 10:30 pm 11/6 - HC 42 em (30.47%) - Reviews labs 1114, 1115; PT/PTT/INR
- Platelets 646 (140-646) - Creatinine .26 (.3-.7) - Glucose 109 (60-100) - Manual smear normal - PT IPTT IINR, thrombin time: normal - All cultures normal
1117 Med 124- addendum - Initially looked great this AM despite 126 to progress notes some wt loss but later this aft became
fussy again, some emesis, not feeding well - Rechecked CBC & BMP, likely will not
discharge today given wt loss & this picture
- Discussed with odd would still be symptomatic at this point (1 wk out) given small size of SDHs
- BPs improved, HR gen'ly normal, will wait for lab results
- Starting famotidine to see if mild GER is contributing to picture
- Will follow in house another day - HC 42 em - Wt. 6.545 kg (14lbs 6.9 oz) (scale #3) - Reviews 1117 labs (WBC normal; mild
MCV/MCH abnormalities; platelets 646,
22
slightly low creatinine, slightly hi glucose; manual smear normal (labs at 249-250)
1117 Med 100- Danny - looked better this AM, better intake, seems 2:38 pm 101 CARES consult to be approaching baseline
- some emesis this afternoon - 4 mo old with vomiting, lethargy, bilateral
SDH&RH - Coag workup underway though results
not suggestive of blood disorder/coag problem as etiology for SDH/RH
- Urine amino acids pending though newborn screen normal so unlikely there will be any metabolic etiology for clinical findings
- Idea raised findings relating to car accident during pregnancy; no evidence on CT /MRI of any finding suggesting trauma 4 mos ago
- No indication of chronic SDH that could result in rebleeding
- MRI indicate acute/subacute, not even close to time frame
- RH commonly seen in delivery but resolve by 4-6 weeks, not compatible with prenatal or birth trauma
- Based on above, cannot identify how any trauma prior to or at birth would have connection with current findings/symptoms
- Remain concerned victim of AHT - it is my medical opinion that AHT is
most likely explanation for clinical presentation and findings
- Have discussed concern with fathers, CPS, police investigators
- Need followup skeletal survey in 2 weeks; acute fx can be missed due to lack of healing (up to 10-20% of children suspected of physical abuse will have findings not seen on initial skeletal survey)
- Twin should have skeletal survey & neuroimaging (CT or MRI)
- Unfortunately, in young infant, physical exam doesn't help in det'g whether infant has occult skeletal or head injury, can have multiple broken bones or head injury
23
wlnormal exam - This pt is good example as prior to CT had
multiple physical exams with no suspicious of intracranial findings
1117 Med 58- Progress notes, - Admitted for emesis, dehydration, 63 Allison leukocytosis conc'g for SBI, thought due
MD to gastroenteritis - With confirmed SDH & bilateral RH,
concerning for NAT v bleeding dlo v metabolic d/o
- Reviews CT IMRI; ophthal - Observe BPs/HRs for possible dev. of
Cushings triad (59) - Initial concern for possible
intussusceptions given waves of illness wlintervening periods of feeling well but us negative
- Emesis improved, PO better - Weight loss - 6.545 kg today (down 345
g from yesterday) - Goes through labs, radiology - Infectious component not as likely given
SDH - Last emesis 11/6 at 10:30 pm, eating well - Wt 14 lbs 6.9 OZ, AFOSF
1117 Med 9-A call to Will keep another day due to vomiting; was wlupdate looking good, now weight loss. Coag tests
look OK. VSS ok; BP normal. May need second opinion on eyes.
1117 Med 114 DHS custody per Both twins taken into DHS custody 1117 progress notes
1117 Med 119 Katrina Contacted by Jason VanHandel, DHS 6:30 pm RN supervisor; pt taken into legal custody by
progress note DHS but parents allowed to visit at hospital Contact DHS social worker Kim Karu re DHS custody. Fax from VanHandel rec'd, RN contacted worker re terms
NOVEMBER -8 11/8 Med 113- Progress note, - Much repetition (including initial 7:33 am 118 Allison concerns, waxing/waning, Cushings, heme
with addendum by & metabolic followup) - DHS involved, both twins taken into DHS
custody yesterday - CARES physician feels
hemorrhage due most likely to AHT,
24
rec'd twin also have skeletal survey & head imaging (114)
- 1 episode vomiting yesterday afternoon, weight loss, dietician rec' d increased formula 20-24 kcalloz
- Today's weight 6.41 kg (down 85 g from yesterday) (114)
- Plan to go horne on pepcid, 24 kcal formula
- Yesterday return of emesis & lethargy, also few episodes stridor lasting few minutes & self-resolving (115)
- CBC, CMP, coags WNL - DRS took custody of twins, both parents
leaving, godmother stayed at hospital in their place; want placed with family
- This AM, much more alert & vigorous - Eating well w/o emesis overnight - No further episodes stridor overnight - Temp 100.2 rectal - He 42 cm (30.47%) - Wt 6.41 kg (141bs 2.1 oz) (115) - Input/output: 525 intake, 268 output - AFOSF (116) - Meds: zofran, pepcid, Tylenol, Benadryl - Labs from 117 (normal except low MCV,
MCR; high platelets; low creatinine, slightly high glucose; manual smear normal; PT/PTT?INR normal. Cultures & chest x-ray negative. Repeats radiology.
11/8 Med 118 Agree with above note with following: (attending) AJ had better night, still only taking small addendum to volume feeds progress note Still losing weight but no emesis today.
Discussed w/ poss of seizures with SDR, can consider EEG Cont. to monitor wtlfeeding May need ng feeds if continue to lose weight Disc'd with godmother & by phone
1118 Med 161 Nursing notes, Laying in crib, playful (various notes re 5pm flow sheet parents friends present, Jessie, Anna,
godmother, both fathers) NOVEMBER -9 11/9 Med 103- Progress note, - 4 mo male admitted with emesis,
25
8:29 am 108 Whitnee dehydration, leukocytosis concerning for Pediatric resident, SBI, thought initially due to gastroenteritis signed with - Now confirmed SDH and bilateral RH, addendum by concerning for NAT v bleeding dlo v James metabolic dlo MD - CT, small SDH; MRI, bifrontal SDH
- Neurosurgical following, no surgical interventions rec' d
- Mental status waxing & waning yesterday
- Monitor with neurochecks, observe BPs/HRs for possible dev. Cushing's triad
- FlU with Goodman at Casey Eye Institute; referral by
- Coags WNL - Metabolic still pending - CARES consulted due to SDH, DHS
involved, AJ & twin taken into DHS custody; feels hemorrhage most likely due to AHT at this time, rec'd twin have skeletal survey & head imaging
- Same language re waves of illness giving initial concern for possible intussusceptions
- Emesis much improved, better PO despite 1 episode yesterday afternoon
- Weight loss during this admission - Dietician rec'd increased formula from 20
kcalloz to 24 kcal/oz - Today's weight 6.575 kg (up 165 kg
from yesterday) - Plan to discharge home on 24 kcal
formula with daily wt checks by - Afebrile; loose stools resolved with no
stool sent for stool cx - Reviews labs etc. - Infectious component of illness not as
likely given SDH (104) - Temp 98.6 (axillary) (97-99) - HC 43 cm (55.5%) (105) - Wt. 6.575 kg (14 lbs 7.9 oz) (105) - Meds: zofran; pepcid; tylenol; Benadryl - All cultures negative (urine, 2 blood, CSF,
rotavirus, guaiac)
26
- Describes all imaging 11/9 Med 108 Agrees with progress note
addendum Adds: feeding better, will continue to observe and make sure he is tolerating feeds given his brain injury. Plan for discharge tomorrow. Discussed with CARES.
11/9 Med 158 Nursing notes, Rectal temp 10004 (variable from 97 - 100.4) 3:28 pm flow chart 11/9 Med 160 Nursing notes, Fussy, irritable 3:30 pm flow chart NOVEMBER -10 11110 Med 102- Nutrition Progress - Today's weight 235 g below admit 2:30 pm 103 Note, Tara - Current diet order doesn't specify volume
goals (rec. including goals) - Consider nipple/gavage ifunable to meet - Wt. gain goal 15-20 g/d average - Full nutrition assessment documented in
nutrition therapy section of chart 11110 Med 21- Discharge Chief complaint: vomiting
Principal final dx: SDH Other treated dx: SDH (1113), leukocytosis (1111), vomiting (1111), mild dehydration (1111), generalized abdominal pain (1112), bilateral RH (11/5), poor feeding (11/8)
neurosurgery ophthalmology CARES
hematology/oncology
Summarizes radiology (25-27)
Neuro: cont'd emesis on day 2, bulging fontanelle concerning for inc'd ICP with hypertension; CT showed small SDH concerning for NAT v bleeding d/o v metabolic d/o.
27
Summarizes labs & meds (27). WBC 31.8 with 66% N, 3% B; UA unremarkable except for 3+ ketones, trace albumin, rare bacteria. Negative CSF, blood & urine cultures. Total 100 mglkg ceftriaxone, dlc'd 11/2 due to negative cultures. Guaiac & rotavirus assay also negative (11/2). Afebrile throughout admission (27)
Etiology thought to be related to viral gastro but SDH discovered to be cause (27)
Waves of illnessltired with periods of energy & normal behavior; considered intussusception but abdominal US neg.
IV restarted day 2, eventually stopped.
Weight loss from 6.965 kg to 6.89 kg on 11/6; fortified formula. Weight down to 6.565 at discharge (27).
Elevated blood pressure on day 2: left arm 120/77; R arm 112/76; L leg 124/95; R leg 124/95. Renal US normal. BP normalized on discharge (28)
At discharge, stable, tolerating feeding wlo emesis, maintaining hydration. FlU with
on 11114.
Temp 97.9; Wt. 6.565 kg (14lbs 7.6 oz) (22.3%) (28-29)
11110 Med 29- Discharge Meds Meds: famotidine (Pepcid) 30 Flo with 11114
attending addendum: improving with feeds but still below goal of 31/0z day of 24 cal formula; PCP will monitor; will set up repeat skeletal survey; to see ophtho.
11110 Med 30- Discharge Leamer: family eager; many discussions with 37 planning/pediatric godmother, grandmother. Follow
education up with 11114, etc.; seek care if persistent fever, uncontrolled vomitingldiarrhea, cannot stay hydrated with sunken or bulging soft spot & no urine 6-8 hrs, lethargy, altered mental status etc. (37)
28
11110 Med 102 Progress notes, Rev'd discharge instructions w/ & Lisa RN re
discharge 11110 Med 361 report re says too early to be ideal; no
followup skeletal evidence of skeletal injury though lambdoid survey sutures appear wider than in previous
study, suggesting ongoing increased ICP
FOLLOW-UP
11121 Med 9-B- Ophthalmology Followup with Dr. Professor of Med 9-F Ophthalmology, Casey Eye Institute
- 1114 exam showed more extensive RH to at least midperiphery in both eyes
- Exam showed normal range vision response - 2 hemorrhage in left eye, 1 in right - Mild bilateral macular swelling - All changes in posterior pole - Retina completely clear to at least equator - Understand no specific etiology for RH
has been identified - Fortunately eyes are clearing - Recommend eval in 3-4 weeks
12122 Med 10- Pediatric records Well baby 6 mos check 12 Wt 17.281bs (44%)
Height 28 in (92%) HC: 17.91 in (90%) AF open & flat Dev'ly fine; recheck at 9 mos "Development post intracranial bleed is normal adjusted for prematurity; head circ. is on same % since discharge"
, M.D. 12127 Opthalmology RHs gone, normal exam, no residual effects
PROSECUTION TESTIMONY & REPORTS
11115 Med 298- - Educational bkground: general pediatrician 360 testimony 3 12 years; academic position Chicago
Childrens, ass't professor of pediatrics Northwestern; primarily clinical
- 5 yrs child abuse team at Chicago Childrens - moved to CARES NW, employed by
Legacy Emmanual Childrens - CARES is outpatient medical clinic for
29
evaluation & mgt of children referred for concerns of child abuse
- Board cert'd general pediatrics (1998) - Board certified in child abuse pediatrics
(offered 2 yrs ago) - Currently one ofapprox. 200 board cert'd
child abuser pediatricians in the world (301) - Att'd AHT conference in SF this summer;
will go to another in January (SD) - Probably test'd couple hundred times in
child abuse cases - 20-50 on SDH (10) - Contacted by she had some
concerns about vomiting, not getting better so ordered CT, showed SDH
- Realized child abuse was a possibility for SDH, called Keltner, he became involved because of his role in inpatient field
- He rev'd CT with one of their radiologists, made sure really SDH (305)
- Talked to rev'd some medical records, met with parents
- Concern for abuse high enough, had to report to Washington CPS
- Explained to parents (legal mandate), talked about further rec' d tests (MRI, skeletal survey, coag & metabolic tests)
- Social worker stayed talked to he joined in middle, to get info re AJ, timeline of who cared for him, etc.
- Absolutely did not tell that trauma occ'd within 1-3 hrs with something like 99.99% certainty
- Told him this was perhaps most likely possibility, were early in eval process, had other things to look at to see if another explanation other than child abuse
- So could not tell him with this certainty because tests outstanding (14)
- Explained available info indicates children develop symptoms immed'ly after event occurs but somewhat inexact because can't shake children
- Base on clinical experience, medical literature, confession studies
- Don't know where 1-3 hrs comes from
30
- Lakindra went back to get more info from & info pretty much
identical as far as symptoms on Mon, absence of problems before that (309)
- MRI confirmed left SDH, also right SDH - Nothing that would provide info re
different etiology (no structural problem with blood vessels or brain to acct for SDH)
- Eye exam: finally reached Sun night; extensive bilateral RH, some extension to midperiphery in right eye; RH in left eye somewhat unique, didn't know what to make of them
- Agreed RH not diagnostic of AHT but compatible with AHT
- Got hematology consult, based on his recommendation to trying to find any other explanation for findings; bleeding eval all came back normal
- Some disorders can't be completely excluded at his age, absolutely no clinical or lab indication of bleeding disorder
- Metabolic: GAl has strongest association, picked up in newborn screen (normal)
- Some metabolic results had abnormal increases in some acid that could be due to dehydration & vomiting
- No GAl, some amino acid tests still pending
- Most likely explanation for findings & clinical presentation is AHT
- AHT is head injury from abuse: can be hit on side of head, or thrown down; would include child shaken or shaken & Y impact against hard or soft surface
- No evidence of external contact, so concerned shaken and perhaps contact with soft surface but hard to definitively say (20)
- No evidence of external contact: no bump on head, no skull fx, no evidence of any external contact to head; so as far as abusive contact, would be contact against soft surface, mattress or pillow, something that wouldn't leave mark (20-21)
31
- What kind of force involved in shaking? certainly aggressive force, violent force, out of range of normal handling
- Previous AAP statement says anyone seeing this would recognize as harmful
- Kids can get SDH from accident but no trauma described; don't have symptoms like AJ - very rarely have RH, very few in number, not as extensive, & they have signs of contact injury (bump, soft tissue swelling, skull fx) - very common, we dx as nonabusive head trauma (22)
- Reasons for AHT dx: bilateral SDH, absence of any other radiology findings that would be etiology, RH & clinical symptoms (rapid onset, lethargy, vomiting)
- Nothing in clinical presentations or findings that would contradict AHT dx
- Other possibilities? Waiting on tests, can be explained by dehydration & vomiting, so wanted to repeat; don't have another explanation, so AHT most likely, not really alternative I can see based on eval (23-24)
- Had hx of really significant MV A & traumatic delivery - but these don't coordinate with onset of symptoms 4 mos later; absolutely no indication of chronic hemorrhage that could come even close to date of birth
- Ability to pinpoint age limited (e.g., 3 v 7 days old) but ability to say recent v. birth very clear
- His radiologist said absolutely no indication of hemorrhage compatible with birth injury 4 mos prior
- RH common at birth but literature says they all go away by 4-6 mos (25)
- If childbirth hemorrhage has happened, should see on MRI if going to rebleed
- SDH forms membrane that can rebleed from very little to no trauma
- Usually no clinical symptoms; usually find rebleed when checking on kid we know had old SDH, can see new blood & membrane
- No documented cases definitely showing
32
birth hemorrhage persisting to 4 mos, on reimaging, usually resolve by 3-4 weeks
- SDH at birth probably lot more common than we thought, happens in asymptomatic kids but per literature doesn't persist to this age & rebleed
- Absolutely no evidence of this on imaging - High WBC: see in infection (spinal fluid,
blood, urine, viral infections, all can cause); can also be stress response so not uncommon in AHT victims
- Don't have identifiable infectious etiology to explain SDH/RH; all cultures negative, twin didn't have signs of infection -would expect to see these things if any infectious process
- Can't think of any infection that would explain SDH & RH
- Blood on MRI no older than 2 weeks; could be few days; not 4 mos old
- Most likely in last week to 10 days, some debate on issue, have to be careful with timing
- All info we have on AHT suggests will be symptoms immediately after event; so if completely fine then abrupt onset of vomiting & lethargy, if victim of AHT, likely have occurred at onset of symptoms
- Sub specialists trying to help dx & manage (she consulted him, neurosurgeon & her nurse practitioner), hemo consult
- His roletry to help determine whether clinical presentations and findings result from child abuse; not uncommon, probably 160 consults/yr, generally tell people not abuse, unfortunately not the case here
- doesn't have expertise in child abuse, not bd-cert'd child abuse pediatrician; great pediatrician but not expertise in child abuse medicine, that is his
- She would defer to his opinion - Has talked to & explained more
times about this case than any other dr, talked numerous times, so she knows what the findings mean to me - she doesn't want this to be AHT (neither do I) - but no
33
knowledge of her coming to different .. OpInIOn
- Know & Sugar at Harborview? Hard not to; is one of leading experts in world in child abuse & specifically AHT; responsible for much of literature that's been published on it, Sugar not far behind (she is more sexual abuse but also AHT) - they are two of leading child abuse experts in my field
- He's involved in getting slides for them to look at; he will send all images & medical documentation, would listen to him (33)
- AJ needs followup skeletal survey; not definitive, 10-20% have fx not seen on 1st x-ray
- Also want info on twin, or any indication of geneticlbleeding problem, open to testing; but mostly wants traumatic injury eval (neuro & skeletal)
- If you shake child, can lead to rib fx but doesn't have to; absence is piece of info we should look at but doesn't eliminate the dx
Cross-exam: - is att' g, he is consulting attending - Not bd cert'd in pediatric radiology,
neurosurgery, ophthalmology - CARES is supported by combination of
hospitals, located on Legacy campus, he is employed by Legacy & CARES
- Kemp: recognized in field - Aware of risk factors but clinicians don't
make dx based on those - With AHT, he is concerned for certain fx
that have association (rib, metaphyseal) -not seen on initial survey
- Seizures are presenting symptom for AHT [ not present here]
- Not enough concern to do cervical spine MRI, decided not to do, under study
- No apnea, no external bruising - No internal organ damage - No retinoschisis, no multilayered too
numerous to count to periphery RH - RH not diagnostic in and of itself
34
- No surgery needed - VW normal, also factor 13, 9; Gal (also no
clinical signs) - Pyruvic aciduria: some were elevated, could
be metabolic disorder or from vomiting/dehydration (thinks most likely, can repeat)
- Risk factors: economic downturn (Berger) but causation hard to prove ( contributed cases); maybe poor self esteem, hx of violent behavior or poor impulse control, poverty; large support system decreases risk
- All histories same from parents as far as he knows
- He's basing dx on clinical findings (SDH, RH) and presentation (vomiting, lethargy in absence of other medical etiology)
- Risk factors don't change medical dx (53) - called Keltner, Keltner notified
talked to reviewed radiology (not always most experienced radiologist at night; may be brain abnormality that explains)
- Rev'd records, aware vomiting for 5 days prior to involvement, persistent, not getting better
- With high WBC & vomiting, think infection was reasonable dx, would have been his leading dx as well, was presumptive dx throughout most of stay
- A ware 2 doses antibiotics - Possibility ofRH from 5 days projectile
vomiting but RH would be very limited (pyloric stynosis study), maybe 1-2 RH in posterior pole
- Infection in child AJ's age cannot be cause of RH of which he is aware
- Can get minor RH from increased ICP, LP should decrease pressure - don't know of any clinical experience or literature that would support RH & LP
- Suspicious of child abuse when spoke with on the 4th but didn't have tests back
35
- Believe spoke with them late AM on 4tn
- Karen Pfeifer (Lakindra's supervisor) made report to DCS at his request, he wanted to participate in discussions [with
- Shaking: what we believe is that neck muscles very weak, brain content much more watery than older kids, brain & neck & head move back & forth, causing injury to the brain - acc/dec of brain itself - ess'ly whiplash type injury
- Don't know of any diagnostic significance of MRI of neck, only pathological, don't want to do unnecessary tests
- [Absolutely] wouldn't expect to find neck injuries in shaken baby case
Redirect - How significant is absence of bruising etc.
in making dx? - He is one of authors looking at association
of bruising with fx from abuse or accident - Majority of shaken babies don't have
bruising - Bruising more from hitting child or
grabbing leg; here no reason to think any of that happened since no physical findings on x-rays
- Spectrum of findings in AHT cases, esp. if shaken (some sleep, fine after few hrs, some fussy & vomiting, some die immediately) -spectrum well described in confessional literature, recent study from France -people said repeat shaking, it works, baby stops crying (358)
- Those are kids we miss, see them back with reinjuries, chronic collecting in head - absence of symptoms doesn't eliminate as possibility diagnosis
- Didn't have blows to abdomen, at least don't have any medical info that would support it
12/14 Med 361- consult - Rec'd radiology images today 362 report - Concern for altered consciousness,
intracranial & retinal bleeding & their causes
- Gestation 38 wks [actually 37] - Failure to progress in birth canal but
36
delivered vaginally hr after sibling - Vital signs okay, some facial bruising - Surrogate in MV A during pregnancy (air
bag hit abdomen, no obvious injuries) - Repeats hx from Lakindra [incorrect per
parents & texts] - Vomiting, slept poorly thru night - Eval 'd & transferred to Childrens ER; exam
okay except for irritability - Spinal tap attempted but traumatic - Rec'd ceftriaxone, admitted for observation - Cont'd decreased oral intake & vomiting
-during hospitalization CT on 3rd day showed small left SDH, later recognized small right SDH
- MRlon 11/4 confirmed these SDH, appeared to be subacute
- No brain abnormality - Skeletal survey felt to be normal - Eye exam had extensive RH to
midperiphery but not to ora serrata; no retinoschisis
- skeletal survey appears normal; follow survey on 11110 too early to be ideal, no evidence of skeletal injury though lambdoid sutures appear wider than in previous study, suggesting ongoing increased ICP
- Also sees small am't SDH in posterior falx and over tentorium, left greater than right
- Normal coag & amino acid screening; newborn metabolic screen also normal
- Injuries such as AJ sustained in absence of obvious serious trauma are almost always result of child abuse
- Eval'd by alternatives to abuse ruled out
- Given available info, no alternative reasonable explanation for the injuries
- Injuries such as these normally result in immediate symptoms following trauma, usually including concussion
- Concussive episode may be brief, followed by irritability & vomiting such as AJ exhibited
37
- Well recognized twin siblings at particular risk
- Multiple cases reported where one twin has abusive injury, other twin later recognized to have asymptomatic intracranial injury
- Dan Lindberg & colleagues are submitting study looking at yield of skeletal surveys in context of injured children: if one twin has sustained child abuse in infancy, other twin 20x more likely to have sustained skeletal injury than non-twin contact children
- Among contact children in general, just under 12 % had unrecognized fx
- Extremely risky for children to remain in care of Mr. as almost certain that he inflicted AJ's injury
- should have cranial imaging & Y full skeletal survey to see if he has also been injured
- If no cranial symptoms, MRI would be highest yield study to identify cranial injuries; cranial CT would be acceptable
PSYCH EV ALS & SUPERVISOR REPORTS
7/6/10 Med 566 Psych - Committed relationship for 3 yrs consultation for - Both always wanted children IVF procedure - Using egg donor & surrogate; one sperm
sample from each child - Very excited - Denied any preexisting mental health issues - Understand risks - Committed; thoughtful about decisions;
appear to bed psychologically ell adjusted and emotionally stable
- Relationship seems to be characterized by mutual respect & healthy communication
Spring Med 567- Testimony of Dr. - PhD 1977; has been CDMHP (county 2011, 583 Albert designated mental health professional Testimony deciding whether people who are dangerous 11111 to themselves or others), involuntary
treatment in Clark County, private practice since 1981
- Works with difficult people & anger
38
- Has testified about 300 times - Saw & last spring (2011) - Centered on plans to have children, handling
stress, each concerned about the other - psychologically very helpful;
concerns with overcommitment (wanted to take care of everybody, helped him set boundaries)
- very mature for age, psychologically healthy, anxious to do everything correctly, doesn't want to say anything that would hurt anyone's feelings
- No concerns about either psychologically - No concerns about anger, both interpunitive
(blame themselves rather than others) - Saw each individually once, together once - No expertise in anger & AHT - comes from rejecting, abandoning
abusive family (verbally abusive because successful, gay, adopting)
- Did not feel need to do testing - In looking at likelihood of violence, looks at
(1) how person deals with stress (people who blame others more likely to be violent) (2) history of violence (3) drug or substance abuse and (4) empathy (putting their needs first)
- None ofthese concerns applicable here - Intrapunitive & empathetic to a fault - Alvin's empathy very deep - Fatigue doesn't change person's personality;
can assess how people would handle stressful situations
- Stresses for them: doing things on their own; with children, will have to do some things on own - does yoga, more athletic
- Some people fly into parenting by seat of pants; & very planful, would do everything they possibly could to be good parent
- Did not have abnormally large amts of stress, were dealing with it ahead of time
11/13/11 Med 560- Report by - Reports on parent visits with twins for 3 561 Marguerite days
MSW, - Fathers meticulous in following instructions
39
ACSW - Very impressed with fathers and handling of Visit supervisor babies; very skilled in assessing needs &
responded appropriately - Very bonded - Never saw either baby cry or act distressed;
when tired, fathers interpreted correctly & helped them fall asleep
- In yrs of experience with parents and infants/children, feel able to interpret if child in danger
- Feel these children very safe with both fathers; do not need supervisor
12/5/11 Med 562 2no report by - Has seen with both babies several times a week, no less than 3 hrs at a time,
one day full 8 hrs - has been stay at home parent,
outstanding job in meeting both babies needs and understanding what they want
- Very bonded, sociable & happy babies - Never seen anything that concerned in
slightest way - Hope lives can return to normal soon
12/9/11 Med 563- Declaration of - Detailed descriptions of visit, 9:15 am to 565 Kelly J. Kelly, 4:59pm
Visitation - very responsive, competent Supervisor - doesn't consider either baby to be
difficult; very easy, slept through night almost from time they came home, rarely fuss. very methodical and organized, considers himself to be a homebody, enjoys cooking, making organic baby food, gardening & decorating. At times, supervisor thought one of babies "fussy",
did not; very relaxed with his children & their care.
Dec. 2011 Med 584- Reference letters - Very strong references 594 from friends, - Nanny (Natalie is a teacher, taught to
nanny, identify signs of abuse; saw no signs, supervIsors, very loving and calm Seth's mother - Doula Teresa babies never cried,
was ahead of dealing with needs (visit supervisor made same point)