Page 1
DEPARTMENT OF HEALTH & HUMAN SERVICES
Centers for Medicare & Medicaid Services
Center for Medicare
7500 Security Boulevard
Baltimore, Maryland 21244-1850
MEDICARE DRUG & HEALTH PLAN CONTRACT ADMINISTRATION GROUP
DATE: April 14, 2017
TO: Medicare Advantage Organizations
Section 1876 Cost Plans
FROM: Kathryn A. Coleman, Director
SUBJECT: Contract Year 2018 Medicare Advantage Bid Review and Operations Guidance
The Centers for Medicare & Medicaid Services (CMS) is issuing this memorandum for use in
preparation of contract year (CY) 2018 bid submissions. The purpose of this document is to
provide the following to Medicare Advantage Organizations (MAO), and where specified,
Section 1876 Cost Plans: detailed operational guidance to support plans in their bid
development; highlight key benefit policies; and review of the CY 2018 Plan Benefit Package
(PBP) software for bid submission.
Guidance in this memorandum references the CY 2018 Final Call Letter (specifically Section II,
Part C) issued on April 3, 2017, Chapter 4 of the Medicare Managed Care Manual (MMCM),
and the PBP bid submission module in the Health Plan Management System (HPMS). CMS
recommends MAOs and other Medicare health plans review these resources in addition to this
memorandum when developing bids for CY 2018. Bids are due to CMS on or before Monday,
June 5, 2017 at 11:59 PM Pacific Daylight Time.
Guidance related to the Medicare-Medicaid Plans (MMPs) can be found at
https://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-
Coordination/Medicare-Medicaid-Coordination-Office/index.html and in the HPMS
Memorandum titled “Applicability of CY 2018 Final Call Letter Provisions to Medicare-
Medicaid Plans” issued on April 4, 2017.
For information about the Medicare Advantage Value-Based Insurance Design Model Test (MA-
VBID), please visit http://innovation.cms.gov/initiatives/vbid/.
Bid Review
The following chart displays key MA bid review criteria and identifies which criteria are used in
reviewing the bids of the plan types described in the column headings, and if guidance is also
provided in the CY 2018 Final Call Letter.
Page 2
2
Plan Types and Applicable Bid Review Criteria
Bid Review Criteria
Applies to Non-
Employer Plans
(Excluding
Dual Eligible
SNP)
Applies to
Non-Employer
Dual Eligible
SNP
Applies to
1876 Cost
Plans
Applies to
Employer
Plans
Described in
Call Letter or
this HPMS
Memo
Meaningful Difference 42 C.F.R. §422.254(a)(4)
Yes No No No Call Letter
Total Beneficiary Cost
(TBC) section 1854(a)(5)(C)(ii)
of the Act
42 C.F.R. §422.254
Yes No No No Both
Maximum Out-of –
Pocket (MOOP)
Limits 42 C.F.R. §422.100(f)(4)
and (5) and
§422.101(d)(2) and (3)
Yes Yes No Yes Both
PMPM Actuarial
Equivalent Cost
Sharing 42 C.F.R. §422.254(b)(4)
Yes Yes No Yes Call Letter
Service Category Cost
Sharing 42 C.F.R. §§417.454(e),
422.100(f) and
422.100(j)
Yes Yes Yes1 Yes Call Letter
Part C Optional
Supplemental Benefits 42 C.F.R. §422.100(f)
Yes Yes No No Call Letter
1 Section 1876 Cost Plans and MA plans may not charge enrollees higher cost sharing than is charged under Original Medicare
for chemotherapy administration, skilled nursing care and renal dialysis services (42 C.F.R. §§417.454(e) and 422.100(j)).
CMS has interpreted and applied the regulatory standards for service category cost sharing
standards and amounts, PMPM Actuarial Equivalence factors, and Total Beneficiary Cost (TBC)
requirements for CY 2018 and has provided guidance on these requirements. MAOs must also
continue to comply with statutory requirements, such as the medical loss ratio and health
insurance providers fee, and are expected to do so independently of our requirements for benefits
or bid review. Therefore, CMS is not making specific adjustments or specific allowances for
these changes in the benefits review requirements.
Total Beneficiary Cost (TBC)
As stated in the CY 2018 Final Call Letter, CMS will exercise its authority under section
1854(a)(5)(C)(ii) of the Act to deny MAO bids, on a case-by-case basis, if it determines the bid
proposes too significant an increase in cost sharing or decrease in benefits from one plan year to
the next through the use of the TBC standard. A plan’s TBC is the sum of the plan-specific Part
Page 3
3
B premium, plan premium, and estimated beneficiary out-of-pocket costs. For most CY 2018
bids, CMS will apply a TBC threshold of $34.00. The change in TBC from one year to the next
captures the combined financial impact of premium changes and benefit design changes (i.e.,
cost sharing changes) on plan enrollees; an increase in TBC is indicative of a reduction in
benefits. As in past years, CMS will evaluate TBC for non-employer plans (excluding D-SNPs).
For CY 2018, benefits and cost sharing that are offered as part of the Value-Based Insurance
Design (VBID) model test will not be included in the TBC evaluation. The MA plans
participating in the VBID model test will be evaluated under the TBC calculation, including plan
premium and non-VBID benefits and cost sharing. Under 42 C.F.R. §422.254, CMS reserves the
right to further examine and request changes to a plan bid even if a plan’s TBC is within the
required amount.
CMS will continue to incorporate technical and payment adjustments and expect organizations to
address other factors, such as coding intensity changes, risk adjustment model changes, and
payment of the health insurance providers fee independently of CMS requirements for benefits
and bid review. As such, plans are expected to anticipate and manage changes in payment and
other environmental factors to minimize changes in benefit and cost sharing over time. To
provide flexibility for CY 2018 plans, CMS is increasing the TBC threshold from $32.00 PMPM
to $34.00 PMPM for most plans:
In mid-April, as in past years, CMS will provide plan-specific CY 2018 TBC values and
incorporate the following adjustments in the TBC calculation to account for changes from one
year to the next:
Technical Adjustments: (1) annual changes in OOPC model software and (2) maximum
Part B premium buy-down amount change in the bid pricing tool ($4.10 for CY 2018).
Payment Adjustments: (1) county benchmark and (2) quality bonus payment and/or
rebate percentages.
The TBC change threshold for CY 2018 is $34.00 PMPM for most plans. Therefore, a plan
experiencing a net increase in adjustments must have an effective TBC change amount below the
$34.00 PMPM threshold to avoid denial of the bid under section 1854(a)(5)(C)(ii). Conversely,
a plan experiencing a net decrease in adjustments may have an effective TBC change amount
above the $34.00 PMPM threshold. In an effort to support plans that improve quality
compensation and experience large payment adjustments, along with holding plans accountable
for lower quality, CMS will apply the TBC evaluation as follows.
For CY 2018, the TBC change evaluation will be treated differently for the following specific
situations:
Plans with an increase in quality bonus payment and/or rebate percentage, and an overall
payment adjustment amount greater than $34.00 PMPM will have a TBC change
Page 4
4
threshold of $0.00 PMPM (i.e., -1 times the TBC change limit of $34.00 PMPM) plus
applicable technical adjustments.
Plans with a decrease in quality bonus payments and/or rebate percentage, and an overall
payment adjustment amount less than -$34.00 PMPM will have a TBC change threshold
of $68.00 PMPM (i.e., 2 times TBC change limit of $34.00 PMPM) plus applicable
technical adjustments. That is, plans would not be allowed to make changes that result in
greater than $68.00 worth of decreased benefits or increased premiums.
Plans with a star rating below 3.0 and an overall payment adjustment amount less than
-$34.00 PMPM will have a TBC change threshold of $68.00 PMPM (i.e., 2 times TBC
change limit of $34.00) plus applicable technical adjustments.
Plans not accounted for in the three specific situations above will be evaluated at the
$34.00 PMPM limit, similar to CY 2017.
Consistent with last year, CMS will maintain the CY 2017 evaluation process for Special Needs
Plans (SNP) for End Stage Renal Disease (ESRD):
ESRD SNPs with an increase in the overall payment adjustment amount greater than
$34.00 PMPM will have a TBC change threshold of $0.00 PMPM (i.e., -1 times the TBC
change limit of $34.00 PMPM) plus applicable technical adjustments.
ESRD SNPs with a decrease in the overall payment adjustment amount less than -$34.00
PMPM will have a TBC change threshold of $68.00 PMPM (i.e., 2 times the TBC change
limit of $34.00 PMPM) plus applicable technical adjustments. That is, plans are not
allowed to make changes that result in greater than $68.00 worth of decreased benefits or
increased premiums.
As stated in the CY 2017 and CY 2018 Final Call Letters, each individual plan being
consolidated into another plan must meet the TBC requirement on its own merit. Therefore, the
TBC adjustment factors for each plan being consolidated will be part of the calculation as if the
plan were continuing. For example, Plan A is being consolidated into Plan B. Plan A’s TBC
adjustment factors (technical and payment) would be used in the TBC evaluation for Plan A’s
consolidation into Plan B. Plan B’s TBC adjustment factors (technical and payment) would be
used in the TBC evaluation for Plan B. The following describes how the TBC evaluation will be
conducted for organizations that consolidate or segment plans from one year to the next:
Consolidating multiple non-segmented plans into one plan: TBC for each CY 2017 plan
will be compared independently to the CY 2018 plan.
Segmenting an existing plan: TBC for each CY 2018 segmented plan will be compared
independently to the CY 2017 non-segmented plan.
Page 5
5
Consolidating previously segmented plans: TBC of each existing CY 2017 segmented
plans will be compared independently to the non-segmented CY 2018 plan.
Consolidating segmented plans into other segmented plans: TBC of the existing CY 2017
segmented plan will be compared independently to the segmented CY 2018 plan.
If CMS provides an opportunity to correct CY 2018 TBC issues following the submission
deadline, the MAO cannot change its formulary (e.g., adding drugs, etc.) as a means to satisfy
this requirement. The formulary review process has multiple stages and making changes that are
unrelated to CMS identified formulary review concerns negatively affects the formulary and bid
review process. For example, portions of the annual formulary review process are based on
outlier analyses. If an MAO were permitted to make substantial formulary changes after the
initial reviews, these analyses could be adversely impacted. In addition, significant formulary
changes would necessitate additional CMS review, outside of the normal review stages, may
jeopardize the approval of an MAO’s formulary and, as a result, could affect approval of its
contract. To avoid TBC issues, MAOs are strongly encouraged to make sure all Part C and Part
D benefit and formulary changes are considered as part of their TBC evaluation prior to
submitting their final bids and formularies to CMS. We make all of the necessary tools and
information available to MAOs in advance of the bid submission deadline, and therefore expect
all MAOs to submit bids that satisfy our requirements.
The plan-specific data elements that CMS will post on HPMS in mid-April are shown in the
following table. The calculation shown in the table accounts for changes in quality bonus
payment and/or rebate percentage or star rating (as described above) so all plans are evaluated
against a $34.00 PMPM TBC change threshold. Should there be any changes due to the quality
bonus payment appeals process, plan sponsors will be notified of their corresponding revised
TBC adjustment factor. Section 1876 Cost Plans will be included in the HPMS posting so
organizations can review their applicable information for implementation of the enrollment
conversion requirements associated with the cost contract transition.
Page 6
6
Plan-Specific TBC Calculation
Steps Item Item Description
CY 2017
TBC
A OOPC value Each of these plan-specific values will
be provided by CMS through an HPMS
posting
B Premium (net of rebates)
C Total TBC
CY 2018
TBC
D OOPC value Plan calculates using OOPC Model
Tools
E Premium (net of rebates) Bid Pricing Tool, Worksheet 6, Cell
R45 + Cell E14 - Cell L14
F Total TBC Calculation: D plus E
Apply TBC
Adjustments
G Unadjusted TBC Change Calculation: F minus C
Payment adjustments (including county benchmark, quality bonus payment,
and/or rebate percentages)
H Gross Payment Adjustment Plan-specific value will be provided by
CMS through an HPMS posting
I Plan Situation CMS determines whether the TBC
calculation is modified for each plan to
account for changes in quality bonus
payment and/or rebate percentage or star
rating through an HPMS posting
J Payment Adjustment Based
on Plan Situation
Plan-specific value will be provided by
CMS through an HPMS posting
Technical Adjustments
K Part B premium adjustment
for the difference between
the maximum Part B
premium buy-down for CY
2017 ($104.90) and the
amount for CY 2018
($109.00)
Value is $4.10 for all plans
L Impact of changes in OOPC
Model between CY 2017 and
CY 2018
Plan-specific value will be provided by
CMS through an HPMS posting
Evaluation
M Adjusted TBC Change Calculation: G + J - K - L
Plan is likely to pass the TBC evaluation
if M is less than or equal to $34 PMPM
As described in the exhibit above, CMS will provide, through the HPMS posting, CY 2017 TBC
plan-specific information including OOPC value (Item A), Premium (net of rebates) (Item B),
and Total TBC (Item C). Premiums used in this calculation will be inclusive of Part B premium
(full premium or partial as a result of a Part B premium buy-down). Based on the CMS release
of Statistical Analysis Software (SAS) files in early April, MAOs will be able to calculate their
Page 7
7
plan-specific CY 2018 OOPC value (Item D) and combine that with their proposed Premium (net
of rebates) for CY 2018 (Item E). Premium (net of rebates) can be found in the Bid Pricing
Tool, Worksheet 6, Cell R45 + Cell E14 - Cell L14.
The Unadjusted TBC Change between CY 2017 and CY 2018 (Item G) is the difference between
CY 2018 Total TBC (Item F) and CY 2017 Total TBC (Item C) , i.e., G = F - C. The Adjusted
TBC Change amount (Item M) reflects the impact of the payment adjustment and technical
adjustments. CMS will provide payment adjustment information through the HPMS posting.
The Gross Payment Adjustment (Item H) accounts for changes in county benchmark, and quality
bonus payment and/or rebate percentages. The Plan Situation (Item I) defines whether the TBC
calculation will be modified with an alternative Payment Adjustment based on the Plan Situation
(Item J) to account for ESRD SNPs or changes in the quality bonus payment and/or rebate
percentage or star rating as indicated in the following table.
Plan Situation
(Item I)
Payment Adjustment
Based on the Plan
Situation
(Item J)
Plans with an increase in quality bonus
payment and/or rebate percentage, and an
overall payment adjustment amount (Item H)
greater than $34.00 PMPM
Maximized at $34
Plans with a decrease in quality bonus
payments and/or rebate percentage, and an
overall payment adjustment amount (Item H)
less than -$34.00 PMPM
Minimized at -$34
Plans with a star rating below 3.0 and an
overall payment adjustment amount (Item H)
less than -$34.00 PMPM
Minimized at -$34
Plans that are not accounted for in the three
categories above
Same as Gross Payment
Adjustment
ESRD SNPs with an increase in the overall
payment adjustment amount (Item H) greater
than $34.00 PMPM
Maximized at $34
ESRD SNPs with a decrease in the overall
payment adjustment amount (Item H) less
than -$34.00 PMPM
Minimized at -$34
The HPMS posting will also provide Technical Adjustments, including Part B premium
adjustment (Item K) and the Impact of Changes in the OOPC model between CY 2017 and CY
2018 (Item L). It should be noted, however, these elements impact TBC in different directions,
i.e., M = G + J - K - L.
Page 8
8
Plan bids with an Adjusted TBC Change amount (Item M) equal to or less than $34.00 PMPM
are likely to be accepted. We remind MAOs the Office of the Actuary extends flexibility on
margin requirements so MAOs can meet the TBC standard. Under §422.256, CMS reserves the
right to further examine and request changes to a plan bid even if a plan’s TBC is within the
required amount.
Illustrative Calculation for Payment Adjustments
As described above, CMS adjusts the TBC calculation to reflect payment changes from one year
to the next. The following table provides examples of how the payment adjustment is calculated.
The Payment Adjustment is the CY 2018 rebate minus the CY 2017 rebate. The CY 2017 Bid
Amount and Benchmark are taken from the CY 2017 BPT. For purposes of the illustrative
calculation below, the CY 2017 Bid Amount is assumed to grow by the same MA growth
percentage as was used to develop the CY 2018 ratebook. The CY 2018 Benchmark is the
weighted average of county-specific payment rates using the CY 2018 ratebook and projected
enrollment from the CY 2017 BPT. The rebate percentage is dependent on the plan’s Quality
Bonus Payment (QBP) rating for each year. The rebate is calculated as the Benchmark minus
the Bid Amount (if the Bid Amount is less than the Benchmark the difference is multiplied by
the rebate percentage).
Illustrative Calculation Examples
Bid
ID
2017 Values 2018 Values
Rebate
Difference
Payment
Adj.
TBC
Threshold Star
Rating
Bid
Amt. Benchmark
Rebate
% Rebate
Star
Rating
Bid
Amt. Benchmark
Rebate
% Rebate
Plan
001 3 $1,000 $950 50% ($50.00) 3 1,025.30 $974 50% ($51.27) ($1.27) ($1.27) $35.27
Plan
002 3 $1,000 $1,050 50% $25.00 3 1,025.30 $1,077 50% $25.63 $0.63 $0.63 $33.37
Plan
003 3 $1,000 $1,300 50% $150.00 3.5 1,025.30 $1,333 65% $199.93 $49.93 $34.00 $0.00
Plan
004 3.5 $1,000 $1,300 65% $195.00 3 1,025.30 $1,333 50% $153.80 ($41.21) ($34.00) $68.00
Plan
005 3.5 $1,000 $1,300 65% $195.00 4 1,025.30 $1,398 65% $242.18 $47.18 $34.00 $0.00
Plan
006 4 $1,000 $1,365 65% $237.25 3.5 1,025.30 $1,331 65% $198.89 ($38.36) ($34.00) $68.00
Plan
007 2.5 $1,000 $1,300 50% $150.00 2.5 1,025.30 $1,250 50% $112.35 ($37.65) ($34.00) $68.00
Note: Slight variances in numbers are due to rounding.
Illustrative Calculation Descriptions:
a. Plans 001 through 004 have benchmark growth of 2.53%.
Page 9
9
b. Plan 001 bid amount is greater than the benchmark in both years; therefore the difference is
not multiplied by the rebate percentage.
c. Plan 002 (and plans 003-007) bid amount is less than the benchmark in both years; therefore
the difference is multiplied by the rebate percentage.
d. Plan 003 has an increase in rebate percentage; therefore the payment adjustment is maximized
at $34.
e. Plan 004 has a decrease in rebate percentage; therefore the payment adjustment is minimized
at -$34.
f. Plan 005 has benchmark growth of 2.53% plus 5.0% to simulate gaining a bonus payment;
therefore the payment adjustment is maximized at $34.
g. Plan 006 has benchmark growth of 2.53% less 5.0% to simulate losing a bonus payment;
therefore the payment adjustment is minimized at -$34.
h. Plan 007 has a 2018 star rating below 3.0; therefore the payment adjustment is minimized
at -$34.
We encourage organizations to participate in User Group Calls conducted by the Office of the
Actuary. These calls begin in April and provide organizations with the opportunity to ask
technical questions related to this calculation.
Maximum Out-of-Pocket (MOOP) Limits
As codified at 42 C.F.R. §422.100(f)(4) and (5), and §422.101(d)(2) and (3), all MA plans,
including employer group plans and SNPs, must establish limits on enrollee out-of-pocket
spending that do not exceed the annual maximum amounts set by CMS. The MOOP applies to
Parts A and B services. However, the MOOP also can apply to supplemental benefits.
For CY 2018, we continue to encourage organizations to establish the lower, voluntary MOOP
thresholds. MAOs adopting voluntary MOOP amounts will have more flexibility in establishing
cost sharing amounts for Parts A and B services than those that do not elect the voluntary MOOP
limits. Plans are responsible for tracking enrolled beneficiaries’ out-of-pocket spending and to
alert beneficiaries and plan providers when the spending limit is reached. D-SNPs also must
track enrollee cost sharing, but should include only those amounts the enrollee is responsible for
paying net of any State responsibility or exemption from cost sharing.
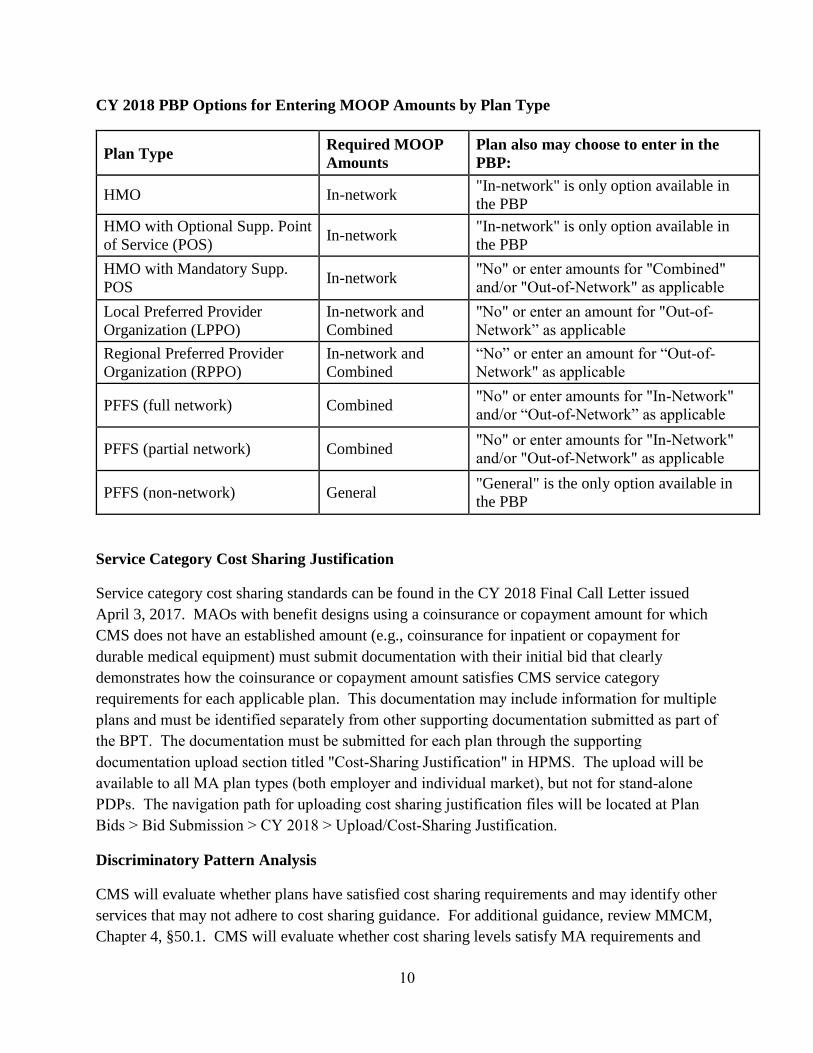
The CY 2018 Final Call Letter defines MOOP requirements by plan type. The following chart
identifies the required MOOP amounts by plan type that are to be reflected in the PBP for CY
2018 for all Parts A and B services.
Page 10
10
CY 2018 PBP Options for Entering MOOP Amounts by Plan Type
Plan Type Required MOOP
Amounts
Plan also may choose to enter in the
PBP:
HMO In-network "In-network" is only option available in
the PBP
HMO with Optional Supp. Point
of Service (POS) In-network
"In-network" is only option available in
the PBP
HMO with Mandatory Supp.
POS In-network
"No" or enter amounts for "Combined"
and/or "Out-of-Network" as applicable
Local Preferred Provider
Organization (LPPO)
In-network and
Combined
"No" or enter an amount for "Out-of-
Network” as applicable
Regional Preferred Provider
Organization (RPPO)
In-network and
Combined
“No” or enter an amount for “Out-of-
Network" as applicable
PFFS (full network) Combined "No" or enter amounts for "In-Network"
and/or “Out-of-Network” as applicable
PFFS (partial network) Combined "No" or enter amounts for "In-Network"
and/or "Out-of-Network" as applicable
PFFS (non-network) General "General" is the only option available in
the PBP
Service Category Cost Sharing Justification
Service category cost sharing standards can be found in the CY 2018 Final Call Letter issued
April 3, 2017. MAOs with benefit designs using a coinsurance or copayment amount for which
CMS does not have an established amount (e.g., coinsurance for inpatient or copayment for
durable medical equipment) must submit documentation with their initial bid that clearly
demonstrates how the coinsurance or copayment amount satisfies CMS service category
requirements for each applicable plan. This documentation may include information for multiple
plans and must be identified separately from other supporting documentation submitted as part of
the BPT. The documentation must be submitted for each plan through the supporting
documentation upload section titled "Cost-Sharing Justification" in HPMS. The upload will be
available to all MA plan types (both employer and individual market), but not for stand-alone
PDPs. The navigation path for uploading cost sharing justification files will be located at Plan
Bids > Bid Submission > CY 2018 > Upload/Cost-Sharing Justification.
Discriminatory Pattern Analysis
CMS will evaluate whether plans have satisfied cost sharing requirements and may identify other
services that may not adhere to cost sharing guidance. For additional guidance, review MMCM,
Chapter 4, §50.1. CMS will evaluate whether cost sharing levels satisfy MA requirements and
Page 11
11
are defined or administered in a manner that may discriminate against sicker or higher-cost
beneficiaries. These analyses may also evaluate the impact of benefit design on beneficiary
health status and/or certain disease states. CMS will contact plans to discuss any issues that are
identified as a result of these analyses and seek correction or adjustment of the bid as necessary.
CY 2018 Part C Benefit Policy
CMS strives to make sure all enrollees receive high quality and effective health care services,
and therefore encourages plans to offer benefits to enrollees that are of value and based on sound
medical practice. The following sections clarify particular policy areas that have generated
questions from stakeholders in previous years.
MA-PD Offerings
As provided at 42 C.F.R. §422.4(c), an MAO cannot offer an MA coordinated care plan in an
area unless that plan or another plan offered by the MAO in that same service area includes Part
D prescription drug coverage. A new validation function has been added to the Service Area
Verification (SAV) in HPMS to ensure that if a legal entity is offering a MA-only plan, it must
offer at least one MA-PD in each county for the legal entity’s service area. Please note that the
following types of plans are not subject to this Part D requirement: EGWP, SNP, PFFS, MSA,
1876 Cost Plans, 1833 Cost Plans, MMPs, PACE, and RFB Local CCPs. The SAV will be
released in late-April and it is important for organizations to verify their service area well in
advance of submitting CY 2018 bids. The navigation path for verifying your service area will be
located at Plan Bids > Bid Submission > CY 2018 > Upload/Verify Service Area.
Smoking and Tobacco-use Cessation
For plans offering Nicotine Replacement Therapy (NRT) as part of their Smoking and Tobacco-
use Cessation benefit, CMS reminds MAOs that these products may be offered through Part C
OTC, Part D OTC, and/or the Part D formulary. If offering NRT under the Part C Smoking and
Tobacco-use Cessation benefit, the plan must specify in the notes section that the NRT does not
duplicate any Part D OTC or formulary drugs.
Maximum Plan Benefit Coverage Amount for Supplemental Benefits
Plans have the flexibility to establish a maximum plan benefit coverage amount for each
supplemental benefit or a combined coverage amount for multiple supplemental benefits. To
establish a maximum plan benefit coverage amount for each supplemental benefit, the plan
would enter the appropriate data in PBP Section B for each benefit. Plans providing a combined
maximum plan benefit coverage amount for multiple supplemental benefits would enter the
combined amount in PBP Section D.
Page 12
12
Cost Sharing for Special Needs Plans Serving Dual Eligible Enrollees (D-SNP)
CMS expects MAOs to communicate MA and State Medicaid benefits to D-SNP enrollees in a
comprehensive and transparent manner. D-SNPs must include Medicare Parts A, B, and Part D
services in their PBP submission, along with approved optional and/or mandatory supplemental
benefits. No Medicaid benefits may be included in the PBP. For example, if a plan offers a
preventive dental benefit for which it receives payment from the State Medicaid agency, that
benefit must not be included in the PBP.
Supplemental benefits that are separately purchased by an employer or union may not be
included in the PBP (See §422.106(a)(2)). This segregation of Medicare-only benefits in the
PBP is necessary so CMS may appropriately account for the Medicare benefit package.
Tiered Cost Sharing of Medical Benefits
MAOs may choose to tier cost sharing of medical benefits to encourage enrollees to seek care
from providers the plan has identified as more efficient or higher quality standards for this type
of tiered plan as described in Chapter 4, §50.1 of the MMCM. The tiered cost sharing of medical
benefits must be applied so all plan enrollees are charged the same cost sharing amount for any
specific provider and all providers are available and accessible to all enrollees in the plan. CMS
reminds organizations they may not exclude any members from being eligible to access tiered
providers.
For CY 2018, CMS expects MAOs to submit a proposal summarizing their intent to tier medical
benefits prior to bid submission. All proposals should be submitted to the mailbox at:
https://MABenefitsMailbox.lmi.org/MedicalTiering.aspx. Submissions will be accepted through
May 4, 2017.
CMS will review all tiering submissions to ensure all MA requirements (including anti-
discrimination requirements and uniform benefit packages) are met. CMS will approve a tiered
medical design meeting the following standards:
The plan fully discloses tiered cost sharing amounts and requirements to enrollees and
plan providers;
The services at each tier of cost sharing are available to all enrollees;
Enrollees may not be limited to obtaining services from providers/suppliers assigned to a
particular tier;
All enrollees are charged the same amount for the same service provided by the same
provider; and
Deductibles, MOOP, and out-of-network benefits are not to be tiered.
Page 13
13
The following examples of “differential cost sharing” are allowable, and not considered to be
tiering of medical benefits:
Facility settings for furnishing some services, such as diagnostic imaging services; and
In-network versus out-of-network services.
MAOs are expected to confirm they are tiering medical benefits and the applicable service
categories in Section A-6 of the PBP. MAOs must use minimum/maximum data entry and notes
fields to describe tiering in each applicable section of the PBP.
Section 1876 Cost Plans Entering Supplemental Benefits in the PBP
For CY 2018, Section 1876 Cost Plans must continue to follow the guidance in the February 9,
2016 HPMS memorandum titled “Implementation of the Cost Contract Plan Transition
Requirements under the Medicare Access and CHIP Reauthorization Act of 2015: Star Ratings
and Clarification of Bid Submissions:”
As stated in the December 7, 2015 HPMS memo, “Cost plans are permitted to provide
optional supplemental benefits to enrollees, but not mandatory supplemental benefits. CMS
has permitted cost plans to enter optional supplemental benefits into the Plan Benefit
Package (PBP) as mandatory supplemental benefits for display on Medicare Plan Finder as
an administrative convenience in the past.” We are clarifying that cost plans may continue
this practice unless they intend to convert to an MA plan for the next contract year. Cost
plans intending to convert to an MA plan for the next contract year should submit a PBP to
CMS in which both mandatory and optional supplemental benefits are entered in
accordance with the rules applied to all MA plans. This will allow CMS to appropriately
calculate beneficiary costs (Total Beneficiary Cost) for the converted plan.
Rewards and Incentives
Rewards and incentives are not considered plan benefits or eligible supplemental benefits.
Rewards and incentives are programs plans may offer consistent with regulations at 42 C.F.R.
§422.134 and guidance in Chapter 4, §100 of the MMCM. CMS does not expect to see rewards
and incentives in CY 2018 PBPs. However, the cost of any Rewards and Incentive Program
must be included in the BPT as a non-benefit expense.
CY 2018 Plan Benefit Package (PBP)
Employer Group Waiver Plans
In CY 2017, CMS waived the requirement for MA employer plans to submit a MA or Part D Bid
Pricing Tool (BPT), but employer plans must complete and submit the MA portion of the Plan
Benefit Package (PBP) in accordance with CMS requirements. Organizations should make a
Page 14
14
good faith effort in projecting CY 2018 member months for each plan and place the amount in
Section A-2 of the PBP. The following question must be completed for all MA and 1876 Cost
Plan organizations: “Indicate CY 2018 total projected member months for this plan.”
CY 2018 PBP Data Entry Expectations
Under §422.101(b), MAOs must comply with Original Medicare requirements and guidance as
to benefits coverage. Most PBP sections do not require a note, particularly when an organization
provides benefits in accordance with Chapter 4 of the MMCM. When a note is required,
organizations must ensure it includes all relevant information necessary for CMS review. This
includes ensuring the note:
Is consistent with the data entry in the corresponding section of the PBP.
Includes a brief description of the different cost sharing levels included in the data field
ranges. For example, cost sharing amounts that fall in between the minimum and
maximum for some highly utilized services (if applicable).
Is consistent with guidance in Chapter 4 of the MMCM:
– If PBP notes are required based on Chapter 4 guidance, the note must provide the
necessary information as described in Chapter 4.
– If a plan is offering more extensive services for a particular supplemental benefit,
the note should describe only those services over and above what is described in
Chapter 4.
– If there is no description in Chapter 4 for a supplemental benefit being offered,
the benefit is to be entered in the “Other” (13d, 13e and 13f) category of the PBP
and the note must describe the benefit.
Notes should not include:
Detailed CPT codes or exhaustive lists of every procedure covered by the benefit;
Bid Pricing Tool explanations;
Terms such as "etc., or misc." in the notes field;
Restatement of the PBP question(s);
Terminology that does not follow the current Chapter 4 definitions (such as "prior
authorization" or "referral") or terminology that leaves ambiguity about the benefit
coverage parameters;
Reference to Medicaid benefits;
Page 15
15
Reference to benefits covered under Part D (except in Rx PBP Notes section, where
applicable);
Reference to Model of Care (MOC) Requirements.
Updated Service Category Descriptions
CMS has updated the Medicare benefit and service category descriptions within the PBP
software and encourages MAOs to review this information to make sure proposed benefits are
consistent with CMS definitions and guidance. These service category descriptions can be
viewed within the PBP software. They can also be viewed in early May under the HPMS
"Service Category Report" found in the 2018 Bid Reports section of HPMS (Navigation Path:
Plan Bids > Bid Reports > CY 2018 > Plan Benefit Reports > Service Category Report).
CY 2018 PBP Changes
CMS has revised and clarified certain PBP sections to simplify plan data entry, and better reflect
MAO and Section 1876 Cost Plan Organization offerings. CMS strongly encourages MAOs to
review the CY 2018 PBP List of Changes in HPMS (Navigation Path: HPMS > Plan Bids > Bid
Submission > CY2018 > Documentation/View Documentation > PBP Tab). Some of the PBP
changes for CY 2018 are included below:
B-14a: Medicare-covered Zero Dollar Preventive Services and B-14e: Other
Medicare-covered Preventive Services
Preventive services are entered in two sections of the PBP:
B-14a Medicare-covered Zero Dollar Preventive Services: Preventive services in this
section are subject to §422.100(k), which requires MA plans to provide coverage of
certain preventive services in-network at zero cost share in accordance with Original
Medicare. MAOs are responsible for staying up-to-date on which Medicare-covered
zero dollar preventive services must be offered.
B-14e Other Medicare-covered Preventive Services: Five (5) previously blank text
fields have been removed and replaced with an option to select “Other Medicare-
covered Preventive Services” for which cost sharing may apply. Cost sharing fields
have been added for “Glaucoma Screening,” “Diabetes Self-Management Training,”
and “Other Medicare-covered Preventive Services.” Preventive services for which
Original Medicare charges cost sharing are to be placed in this section even if the plan
chooses not to apply cost sharing. For example, “prostate cancer screening - digital
rectal exam” should be included in this section. MAOs are responsible for staying up-
to-date on other Medicare-covered preventive services for which cost sharing may
apply.
Page 16
16
B-14c: Eligible Supplemental Benefits as Defined in Chapter 4
“Remote Access Technologies” has been updated to allow plans to select “Web/Phone
based technologies” and/or “Nursing Hotline.” The “Remote Access Technologies” in
the enhanced benefit picklist (B-14c base 1 of PBP software) contains an “*.” This
indicates a note is required for the Web/Phone based technologies (B-14c base 10 of the
PBP software). A note is optional if a plan is only offering the “Nursing Hotline”
benefit under the “Remote Access Technologies” supplemental benefit.
B-16b: Comprehensive Dental
The enhanced benefits “Endodontics,” “Periodontics,” and “Extractions” are now listed
as separate benefits in this PBP section. In addition, questions related to the type of
benefit (mandatory/optional), specific number or the unlimited number of the visits,
periodicity of visits, and the cost sharing amounts are included for each enhanced
benefit.
B-7b: Chiropractic Services, B-13a: Acupuncture, and B-14c: Alternative Therapies
The PBP now allows MAOs to offer a combined benefit that includes two or three of the
following services: Chiropractic (7b), Acupuncture (13a), and/or Alternative Therapies
(14c). MAOs offering this combined benefit must match the Maximum Plan Benefit
Coverage Amount and/or the number of visits for the services included in the combined
benefit. The Exit Validation will generate an error message if the PBP data entry differs
from the criteria noted above.
Important Administrative Information and Submission of Questions
MAOs must update contact information in the HPMS Contract Management module to ensure
that communication between CMS and your organization includes the correct individuals. In
addition, CMS will use the following email address [email protected] to communicate with MAOs
for MA benefits review. Therefore, please ensure your organization’s email system can receive
emails from this address. CMS may send a test email notification to organizations in April or
May to troubleshoot any email transmission issues.
CMS reminds MAOs that the OOPC model in SAS software is available on the CMS website.
All documentation and instructions associated with running the OOPC model are posted on the
CMS website on the OOPC Resources page: https://www.cms.gov/Medicare/Prescription-Drug-
Coverage/PrescriptionDrugCovGenIn/OOPCResources.html. Prior to uploading a Medicare
Advantage plan bid, MAOs should run their plan benefit structures through the SAS OOPC
model to make sure the plan offerings comply with CMS requirements, such as Meaningful
Difference and Total Beneficiary Cost evaluations.
Page 17
17
CMS encourages MAOs to review the available resources before submitting a question to
confirm the answer has not already been provided. The MA benefits mailbox at:
https://MABenefitsMailbox.lmi.org/ includes links to a variety of reference materials. MAOs
can submit questions regarding policy, cost sharing, and supplemental benefits to this mailbox
for CMS review and response.
Other questions may be directed to the appropriate mailbox or mailbox website as specified
below:
Technical HPMS questions (e.g., PBP download, plan creation, bid upload), please
contact the HPMS Help Desk at 1-800-220-2028 or [email protected] ;
Technical questions about the Out-of-Pocket Cost (OOPC) model, please submit an email
to [email protected] ;
Part C Medicare Advantage policy and Section 1876 Cost Plan transition policy related
questions, please submit to: https://DPAP.lmi.org/DPAPMailbox/;
Crosswalks, plan consolidation and provider specific plan (PSP) questions, please submit
to https://DMAO.lmi.org/DMAOMailbox;
Part D policy questions about meaningful difference, please submit an email
to [email protected] ;
Bid Pricing Tool (BPT) questions, please submit an email to actuarial-
[email protected] ;
Medicare Advantage Value-Based Insurance Design (MA-VBID) model questions, please
submit an email to: [email protected] ;
Medicare-Medicaid Program questions, please submit an email
to [email protected] .