85
Medication Reconciliation Preventing Adverse Drug Events One Patient at a Time
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | edward-young |
| View: | 218 times |
| Download: | 0 times |

Medication Reconciliation
Preventing Adverse Drug Events
One Patient at a Time

Today’s Schedule
• Medication Reconciliation Introduction– Break-out session #1: Preparing a Med History
• Best Possible Medication History – Break-out session #2: Interviewing a patient
• Pre-Admission Verification Form– Break-out session #3: Med Reconciliation process
• Verification Coding System & Medication Reconciliation Audit Tool – Break-out session #4: Medication Reconciliation
Audit
• Conclusion

Safer Healthcare Now!
• A campaign to enlist Canadian healthcare organizations in implementing six targeted interventions in patient care
• To improve the safety of our healthcare system in Canada
• A dynamic approach to quality improvement

National Collaborative Effort
• Medication Reconciliation is one of the Safer Healthcare Now Initiatives
1. Medication Reconciliation2. Improved Care for Acute Myocardial Infarction3. Prevention of Central-Line-Associated Infection 4. Rapid Response Teams 5. Prevention of Ventilator-Associated Pneumonia 6. Prevention of Surgical Site Infections

Medication Reconciliation
A formal process of obtaining a complete and accurate list of each
patient’s current medications
At Admission, Discharge
and at all other
Transitions in Care
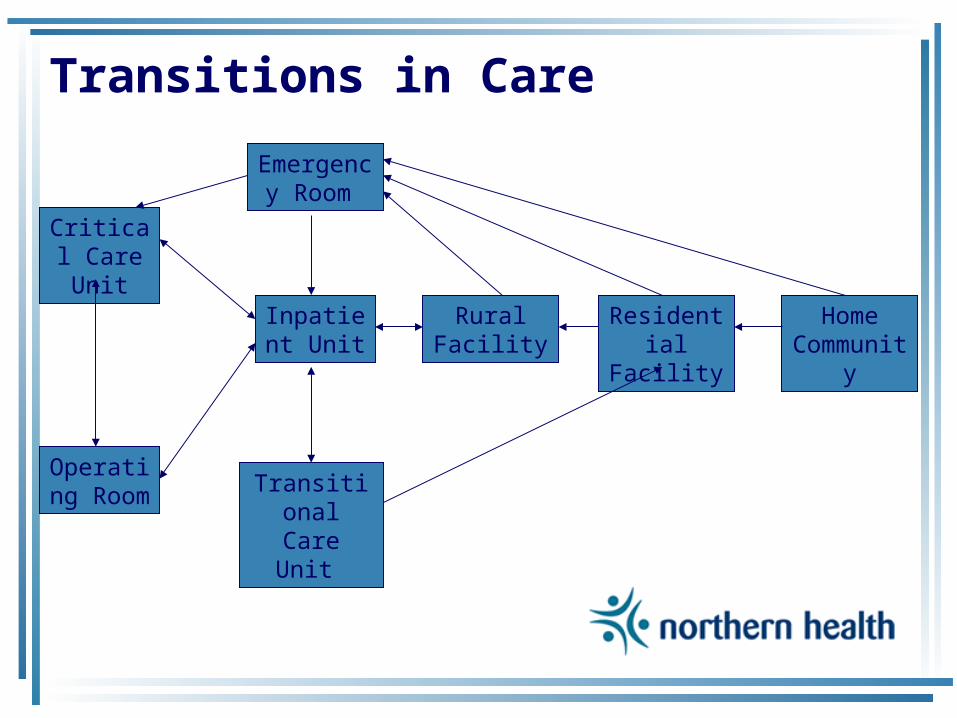
Transitions in Care
Critical Care Unit
Operating Room Transitional
Care Unit
Inpatient Unit
Emergency Room
Rural Facility
Residential Facility
Home Community

Medication Reconciliation
• To prevent Adverse Drug Events (ADE’s) by implementing medication reconciliation in hospitals across Canada
• To eliminate medication discrepancies, at all interfaces of care, for all patients
• To ensure patients receive appropriate medications while hospitalized
• To improve communications at patient transfer points

Why Reconcile?
• Chart reviews have revealed over half of all hospital medication errors occur at the interfaces of care
• Medication errors are one of the leading causes of injury to hospital patients
The Case for Med Reconciliation
• 2004 Canadian Adverse Events Study– Drug and fluid related events were the
second most common type of procedure or event to which adverse events were related
• 2004 Study in Canadian Hospital– 23% incidence of adverse events in patients
discharged from an internal medicine service • 72% were medication related
The Case for Med Reconciliation• 2005 Canadian Study
– 151 General Medicine patients • Prescribed or receiving at least four medications• Not from an extended care facility
– 53.6% - Patients 1 Unintentional Discrepancy • 38.6% - Potential to cause moderate or severe discomfort or clinical deterioration • 46.4% - Omission of regularly used medication
Accreditation Responsibilities
• Canadian Council on Health Services Accreditation
– Patient Safety Goals & Required Organization Practices for 2005
• “Reconcile the patients’ medications upon admission, and with the involvement of the patient”
• “Reconcile medications with the patient at referral or transfer and communicate the patients’ medications to the next provider of service at referral or transfer to another setting, service, service provider, or level of care within or outside the organization”
Seamless Care
• “Desirable continuity of care delivered to a patient in the health care system across the spectrum of caregivers and their environment”
• “When moving between levels of care, patients’ drug information is not always transferred to all care providers in a timely fashion… consequently, the patient may not receive the most appropriate regimen for their condition of this seamless care process”
Medication Reconciliation is a key component of the Seamless Care
process
Medication Reconciliation Process
Easy as 1-2-3
1. Create the most complete and accurate list possible of all current medications
2. Use this list when writing medication orders
3. If using this process after admission orders have been written, reconcile and resolve any discrepancies
Key Benefits
• Prevent inadvertent omission of needed home medications
• Prevent failure to restart home medications following transfer and discharge
• Prevent duplicate therapy at discharge (result of brand/generic) combinations or formulary substitutions
• Prevent errors associated with orders having incorrect doses or dosage forms
Challenges
• No clear owner of med reconciliation process
• May be lack of knowledge and understanding by front line practitioners of the importance of this function
• No standard process to complete the collection of information
• No process to integrate the information obtained in the med history to the prescribing process

Potential Barriers
• Isn’t this physician/nurse/pharmacist job?
• Fear of change• Just another flavour of the week• Staff perceive this as additional work
– Reduce the number of caregivers collecting medication histories
– Build into usual work process

Medication Reconciliation
Best Possible Medication History(BPMH)
Best Possible Medication History
Definition
A medication history obtained by ahealthcare professional which includes
a thorough history of all regular
medication use (prescription and non-prescription)
Information Sources
• Patient – best source if patient competent
• Caregiver • Pharmanet • Prescription vials/Compliance packaging• Medication List • Pharmacy • Family Physician • MAR from previous institution
Med Rec Process at Admission
PREPARATION • Print Pharmanet record • Addressograph Home Medication
Reconciliation form • Determine if patient is capable of
providing med history
Patient Unable to Give Details
• Patient does not know name or details about medication – Obtain a detailed description of
medication • Dosage form (capsule, tablet)• Strength • Size • Shape • Color • Markings
Caregiver
• Good option if patient is not able to provide information
• Obtain information when caregiver is at hospital or call at home
• Helpful only if caregiver has knowledge of patient’s medication history and current use
Pharmanet Record
• Pharmanet record is a “Dispensing History” of past 15 months
• Limitations – Does not indicate medications active
or discontinued– May indicate compliance if consistent
dispensing patterns identified– Will not reflect physician-directed
changes made at doctor appointments
Prescription containers
• Acceptable – Prescription Vials – Pharmacy Blister packaging
• Questionable – Patient packaged cassettes
• Unacceptable – Evidence of mixing meds in one container – Unlabelled and Unidentifiable
medications
Medication List
• A good “supporting” resource if up-to-date
• Always a good idea to confirm accuracy of each item on list with patient
• May be outdated • Potential for transcription errors • Educate patients on the importance
of bringing a Medication List and/or Prescription Vials to the hospital
Pharmacy
• A good source to obtain Pharmanet record if unable to access Pharmanet
• Pharmacist may have additional supporting information – Number of refills left on a prescription – Compliance problems – Economic constraints – Allergy history – Therapeutic successes, failures

Family Physician
• Contact as a “last resort” to obtain information
• “Prescribing information”– Length of therapy – Indications – Distribution of samples
• May not be able to identify problems with compliance
Medication Administration Record
• If patient transferred from another institution – Long Term Care (LTC)– Rural hospital to Prince George
• Important to know if Best Possible Medication History (BPMH) was done at admission
• Important to record time of last doses
Interviewing Patients
• Time commitment – Goal 10min • Introduce yourself and explain
your role – Tell patient you would like to ask
him/her some questions about his/her medication use
– Ask if this is a good time • If not, schedule another time
Interviewing Patients
• Ask questions until you are confident all information is complete and reliable – Pursue unclear answers until they are clarified
• Use open-ended questions – What, how, why, when– Balance with yes/no questions
• Use nonbiased questions – Do not lead the patient into answering
something that may not be true
• Ask simple questions– Avoid using medical jargon
Interviewing Patients
• Prompt the patient to remember all medications– Prescriptions
• Patches, creams, eye drops, inhalers, sample medications
– Over-the-counter (OTC) medications – Herbal and other natural remedies – Vitamins and minerals – Non-drug therapy
• Use “head-to-toe” Review of Systems approach
Review of Systems
• HEENT– Nose, ear or eye drops – Analgesics used for headache or sinus pain– Dental products – Insomnia – Motion sickness – Smoking Cessation aids
• Respiratory tract – Antihistamines – Decongestants
Review of Systems
• GI/GU – Antacids – Antiflatulants – Antidiarrheals – Laxatives – Hemorrhoidal preparations – Vaginal antiinfectives
• Musculoskeletal – ASA – Anti-inflammatory agents – Acetaminophen or combination
Review of Systems
• Dermatological – Psoriatic/Seborrheic – Antiinfective – Analgesic topical preparation – Corns/callus pads or other foot care
• Hematological – Consider iron, B12, folic acid
• Overall/System-wide– Vitamins – Herbal – Homeopathic or other alternative healthcare
products
If Time Permits…
• Indication – This is the patient’s version of the indication
• Efficacy – Tell me how you know this medication is
working for you?
• Toxicity – Are there any problems that you are having
which you think may be caused by this medication?
– If patient says no, probe with a few of the most common side effects

If Time Permits…• Compliance
– How often do you take this medication?
– Try to verify if cost, dosing frequency, adverse effects, or personal beliefs may be an obstacle
• How do you feel your medications impact your life?• Tell me how you feel about medication use, in
general?
– Inquire about technique and maintenance of devices used to facilitate drug delivery or monitor drug therapy
• Inhalers and Spacers, BP monitors, Blood glucose monitors

Medication Reconciliation
Pre-Admission Medication Verification Form
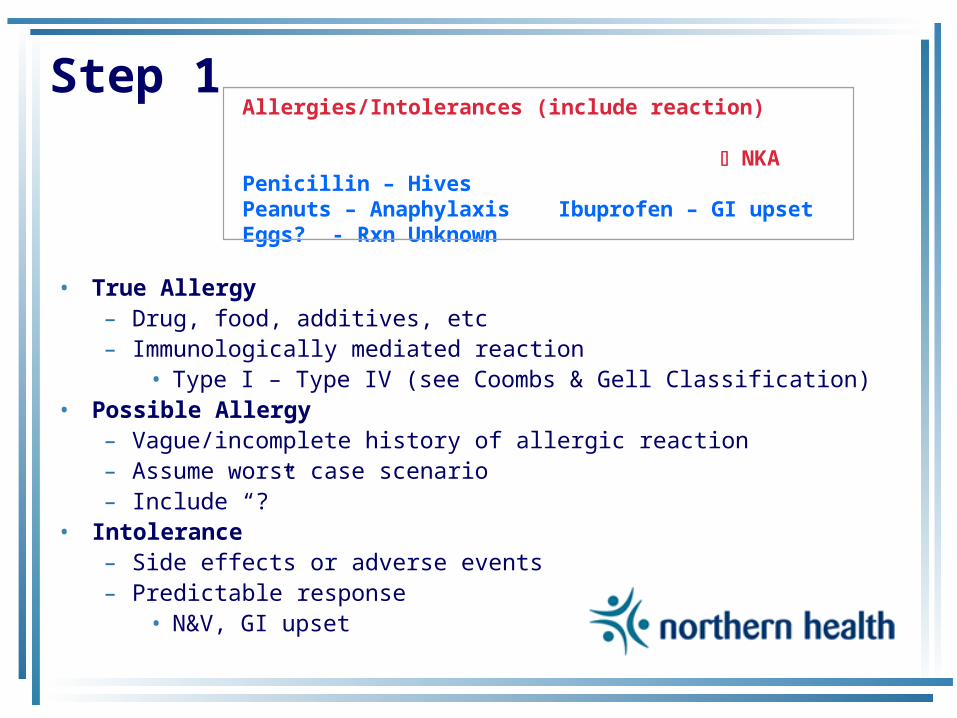
Step 1
• True Allergy – Drug, food, additives, etc– Immunologically mediated reaction
• Type I – Type IV (see Coombs & Gell Classification)• Possible Allergy
– Vague/incomplete history of allergic reaction – Assume worst case scenario– Include “?”
• Intolerance – Side effects or adverse events – Predictable response
• N&V, GI upset
Allergies/Intolerances (include reaction) NKA
Penicillin – HivesPeanuts – Anaphylaxis Ibuprofen – GI upset Eggs? - Rxn Unknown
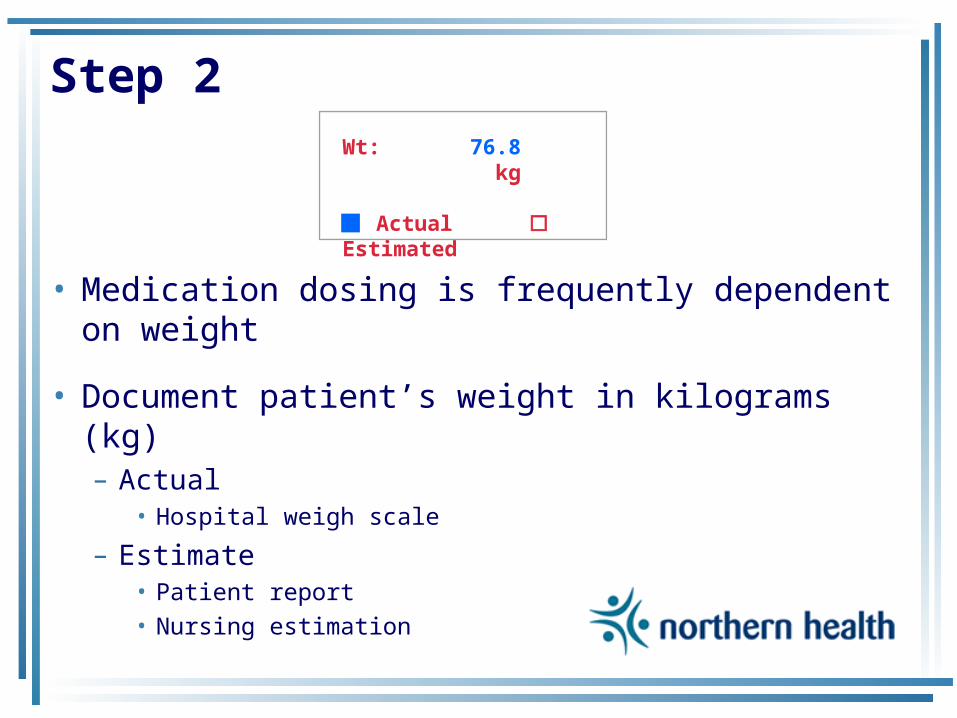
Step 2
• Medication dosing is frequently dependent on weight
• Document patient’s weight in kilograms (kg)– Actual
• Hospital weigh scale
– Estimate • Patient report • Nursing estimation
Wt: 76.8 kg Actual Estimated

Step 3
• MEDICATION NAME – Document generic name - chemical name of drug
• If two chemical ingredients, list both– Avoid use of brand names
• Exception: multi-ingredient drugs – Sofracort – framycetin/gramicidin/dexamethasone
– Include full name • Erythromycin base, Erythromycin estolate
– Avoid use of abbreviations • Exception: ASA - Acetylsalicylic acid
Generic Name, Strength, & Formulation(Manufacturer or Brand Name)
1 Amoxicillin/Clavulanate
2 Diltiazem
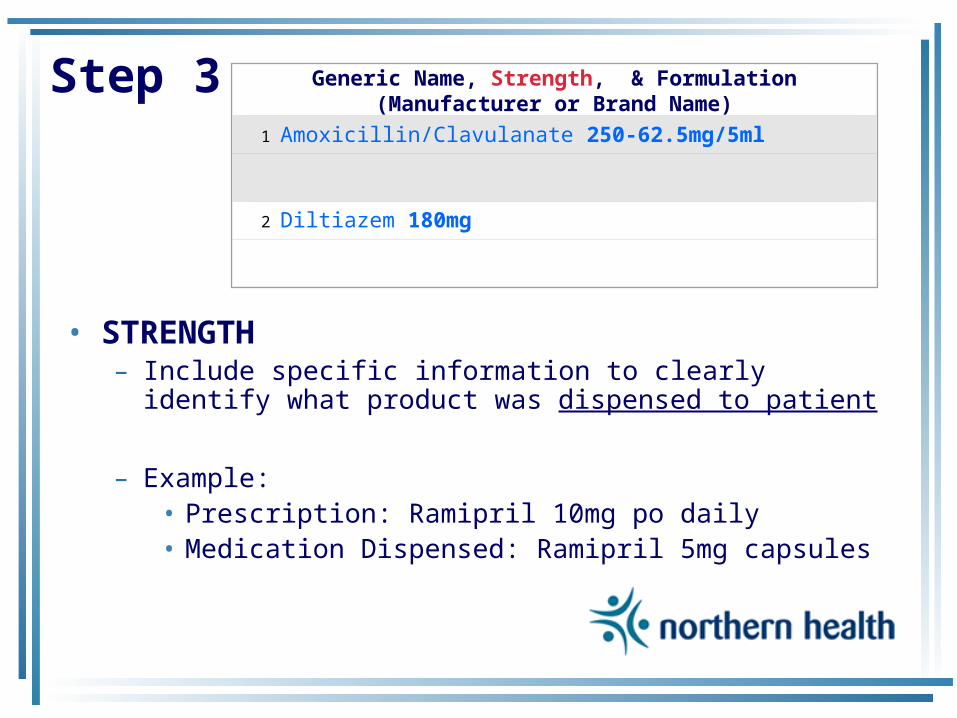
Step 3
• STRENGTH
– Include specific information to clearly identify what product was dispensed to patient
– Example: • Prescription: Ramipril 10mg po daily • Medication Dispensed: Ramipril 5mg capsules
Generic Name, Strength, & Formulation(Manufacturer or Brand Name)
1 Amoxicillin/Clavulanate 250-62.5mg/5ml
2 Diltiazem 180mg
Step 3
• FORMULATION – Acceptable to use abbreviations
• Dosage forms – Susp- suspension – Liq – liquid – Tab or Cap – tablet or capsule – Inj – injectable
• Special formulations – EC – enteric coated – SR – sustained release
Generic Name, Strength, & Formulation(Manufacturer or Brand Name)
1 Amoxicillin/Clavulanate 250-62.5mg/5ml suspension
2 Diltiazem CD 180mg capsule
Step 3
• Prescription labels will include – Generic name PLUS
• Manufacturer OR Brand name OR Drug Identification Number (DIN)
• Additional Resources – Pharmacy or CPS – Drug Product Database http://www.hc-sc.gc.ca/hpb/drugs-dpd/
Generic Name, Strength, & Formulation(Manufacturer or Brand Name)
1 Amoxicillin/Clavulanate 250-62.5mg/5ml suspension
(GlaxoSmithKline or Clavulin-250F)
2 Diltiazem CD 180mg capsule
(Biovail Pharm or Cardizem CD)

Step 3
• DOSE– Weight
• mg = milligram, g = gram, mcg = microgram – Do not use µg – confused with mg
– Volume • ml = millilitres, L = litres
– Miscellaneous • International Units
– Do not use IU – confused with IV or 10 (ten)• units
– Do not use U or u – confused as zero
Dose
500mg
180mg
Step 3
• Route– po – oral – ng – nasogastric – sc – subcutaneous – im – intramuscular – iv – intravenous
Route
PO
PO
Step 3
• FREQUENCY – daily
• Do not use q.d. or QD
– q2days• Do not use q.o.d. or QOD
– BID, TID, QID– q4h, q6h, q8h – 5 times daily
Frequency
TID
Daily

Step 3
• Duration– How long patient has taken med?
• wks, mths, days, doses…– If medication ordered for specific duration
• Indicate time taken in relation to prescribed duration– 2 doses of 14 days – 17 days of 6 weeks – 2 months of 6 months
Duration
4 of 10 days
4 years
Step 3
• Last dose (date/time)– Use 24hr hospital time– Month and day is adequate
Last Dose Date/Time
1400hrMay 12
0800hrMay 12

Step 3
• Indication/Comments – Indication as reported by patient if known– Adverse events experienced?– Physician directed patient to reduce dose
at last office visit – Non-compliance
Indication/Comment
Acute Sinusitis Non-compliance: taking bid
AnginaExperiencing dizziness
Step 3
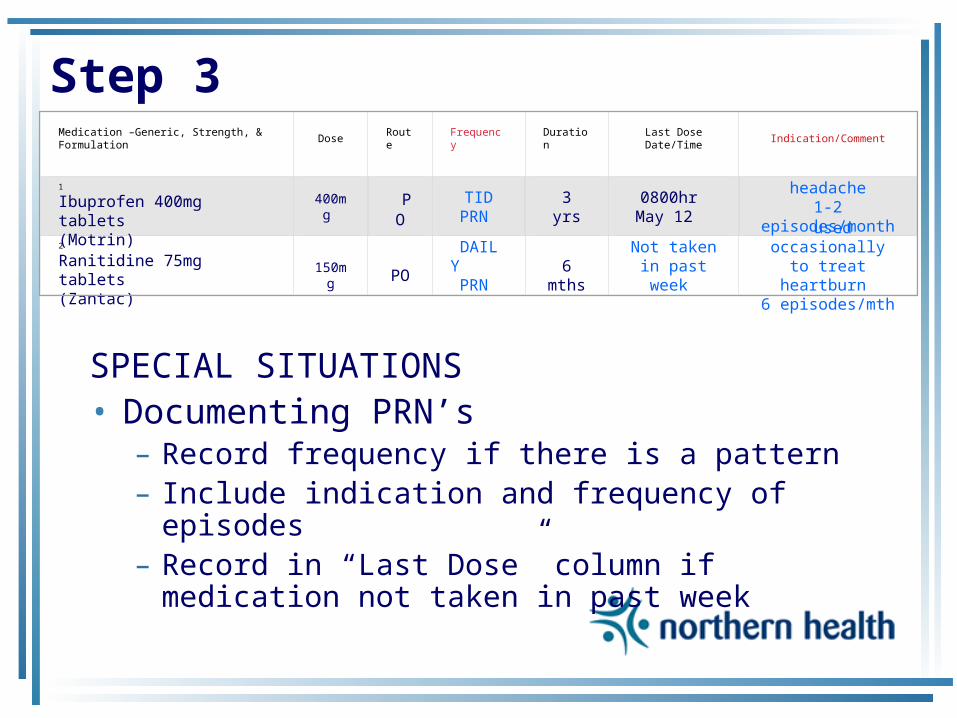
SPECIAL SITUATIONS• Documenting PRN’s
– Record frequency if there is a pattern – Include indication and frequency of episodes– Record in “Last Dose” column if medication
not taken in past week
Medication –Generic, Strength, & Formulation Dose Route Frequency Duration Last Dose Date/Time Indication/Comment
1
Ibuprofen 400mg tablets(Motrin)
400mg POTID
PRN 3 yrs
0800hr May 12
headache1-2 episodes/month
2
Ranitidine 75mg tablets(Zantac)
150mg
PO
DAILY PRN
6 mths
Not taken in past week
used occasionally to treat heartburn 6 episodes/mth

Step 3
SPECIAL SITUATIONS• Medications given in cycles
– Note date next dose due – Didrocal kit – note where patient is in 90 day cycle
Medication –Generic, Strength, & Formulation Dose Route Frequency Duration Last Dose Date/Time Indication/Comment
1
Cyanocobalamin 1000mcg/ml injectable (Sabex)
1000mcg IM q3mths 1 yr
am Mar 21
Anemia Next dose due:Jun 21
2
Etidronate 400mg/Calcium Carbonate 1250mg (Didrocal)
1 tab PO Daily 3 mths0800hr May 12
Osteoporosis 56 tablets left in 90
day kit
Step 4
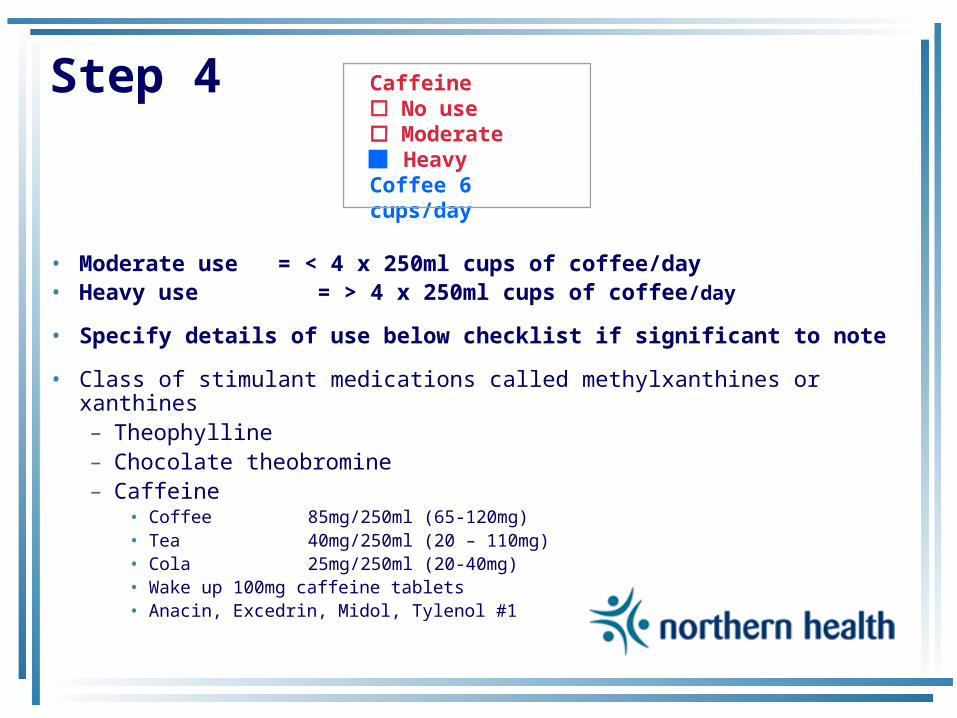
• Moderate use = < 4 x 250ml cups of coffee/day • Heavy use = > 4 x 250ml cups of coffee/day
• Specify details of use below checklist if significant to note
• Class of stimulant medications called methylxanthines or xanthines– Theophylline – Chocolate theobromine – Caffeine
• Coffee 85mg/250ml (65-120mg) • Tea 40mg/250ml (20 – 110mg) • Cola 25mg/250ml (20-40mg) • Wake up 100mg caffeine tablets• Anacin, Excedrin, Midol, Tylenol #1
Caffeine No use Moderate Heavy Coffee 6 cups/day
Step 4
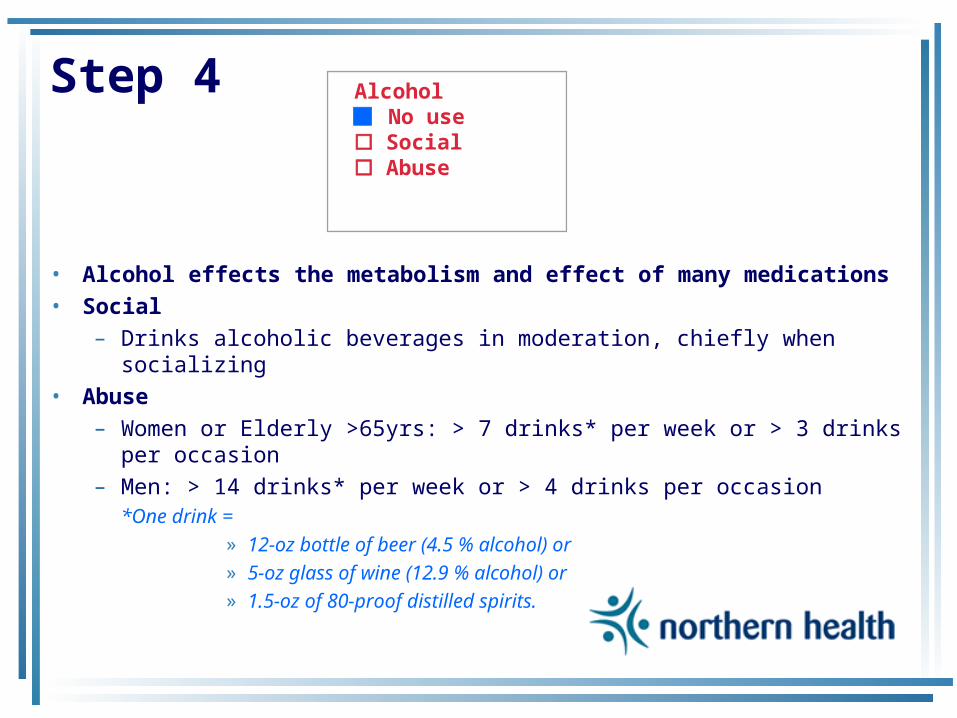
• Alcohol effects the metabolism and effect of many medications
• Social – Drinks alcoholic beverages in moderation, chiefly when
socializing • Abuse
– Women or Elderly >65yrs: > 7 drinks* per week or > 3 drinks per occasion
– Men: > 14 drinks* per week or > 4 drinks per occasion *One drink =
» 12-oz bottle of beer (4.5 % alcohol) or» 5-oz glass of wine (12.9 % alcohol) or » 1.5-oz of 80-proof distilled spirits.
Alcohol No use Social Abuse
Step 4
• Nicotine is a drug that can interact with other medications
• Former smoker – Note quit date
• Current – Note number of cigarettes or packs
smoked per day– Note if smoking cigars
Smoking Former NeverCurrent2 packs/day
Step 4
• Recreational – Illicit drug use
• Marijuana, cocaine, crystal meth, heroine…– Prescription or non-prescription use
• Narcotics - Tylenol #1, Amphetamines, Benzodiazepines
• Interviewing Tips – A lot of people are using recreational drugs these days.
These drugs have a possibility of interfering with the medications you will be receiving in the hospital. Have you tried any? Are you currently using any?
Recreational No use Illicit Rx/OTC

Step 4
• Influenza < 1yr • Pneumococcal < 5yr• Tetanus/Dipth <10yr• Hep B x 3 • Hep A x 2 • MMR x 2 • Meningococcal • Varicella x 2
Immunization Complete History Unavailable
Influenza <1yr Pneumococcal <5yr Tetanus/Dipth < 10yr Hep B x3
MMR x2 Meningococcal Varicella x2 Hep A x2
Step 5
• Indicate Source of Information – Ideal to interview patient
• Limitations if patient:– Confused – Does not speak English – Too ill to interview
– A good idea to document Family Physician, Pharmacy and Caregiver contact info in the event more information is needed later
Patient Pharmanet Caregiver Jane Smith Ph: 987-4321
Prescription vials Pharmacy Wal-Mart Ph: 987-6543
Medication List MAR Family Physician Dr. Green Ph: 987-4444
Step 6
• Sign your name • Record date and time• Insert into patient chart
– beginning of Orders section
DOCUMENTED BY
Alana Froese 1530hr May 12/06Nurse/Pharmacist/Technician Signature Date/Time
Physician Ordering Features • Physician reviews Pre-Admission
Medication list – Continues – Discontinues – Changes
• Verification Codes – Pharmaceutical Care Process
• Eight Drug Related Problems (DRP’s) • A quick way for physicians to indicate reasons for
intentional changes to therapy
• Physician signs and dates order
Order Processing Features • Unit clerk processes orders and
transcribes to MAR – uses yellow highlighter or initials in right
column to indicate order has been processed
• RN initials right column to indicate Unit Clerk has processed order and transcribed to MAR appropriately
• Check “Faxed to Pharmacy” to indicate order has been sent to Pharmacy

Final Touches
CONTINUE
DISCONTINUE
CHANGE
FLOOR USE
1
4
ST
ST
Faxed to Pharmacy Page __1____ of ___1____

Medication Reconciliation
Verification Coding System
Verification Code #1
• INDICATION 1.1 Patient has a diagnosed problem which
requires a drug therapy • New symptoms or indication revealed/presented
1.2 Preventative drug required • Taking a drug for valid indication, but this drug
causes side effects which require prophylactic therapy
1.3 Synergistic drug required • Requires synergistic drug therapy to potentiate
effect of current drug therapy

Verification Code #2
• NO INDICATION 2.1 No clear indication for drug use
• Improvement of disease state • Receiving drug chronically which was intended for
acute condition • Recreational use, addiction/dependence • Condition can be more appropriately treated by
non-drug therapy
2.2 Receiving a drug to treat an avoidable ADR
2.3 Inappropriate duplication of therapeutic class or active ingredient
Verification Code #3
• DOSE TOO LOW/DURATION TOO SHORT
3.1 Drug dose too low (sub-therapeutic)3.2 Dosage regime not frequent enough3.3 Duration of treatment too short
Verification Code #4
• DOSE TOO HIGH/DURATION TOO LONG
4.1 Drug dose too high (dose dependent toxicity)
4.2 Dosage regime too frequent 4.3 Duration of treatment too long
Verification Code #5
• WRONG DRUG 5.1 Inappropriate drug
• Inappropriate drug or dosage selection • More cost effective drug available • Drug therapy is known to be ineffective for this
indication• Drug therapy is effective for this indication, but not
effective in this patient for unknown reasons 5.2 Inappropriate drug form
• Cannot take the drug product (swallow, taste, administration)
5.3 Contraindication for drug (incl. pregnancy/ breastfeeding)

Verification Code #6
• NON-COMPLIANCE 6.1 Patient is not compliant
• Drug underused, overused or abused • Patient has difficulties reading/understanding
6.2 Drug not taken/administered at all • Patient unable to use drug/form as directed • Patient unwilling to carry financial costs • Prescribed drug not available
6.3 Wrong drug taken/administered • Prescribing error• Dispensing error (wrong drug or dose dispensed)• Administration error (by patient/caregivers)
Verification Code #7
• ADVERSE EVENT
7.1 Side effect suffered at a therapeutic dose (non-allergic)
7.2 Side effect suffered at a therapeutic dose (allergic)
7.3 Toxic effects suffered
Verification Code #8
• DRUG INTERACTION
8.1 Potential or actual Drug/Drug interaction
8.2 Potential or actual Drug/Food interaction
8.3 Potential or actual Drug/Laboratory interaction

Medication Reconciliation
Medication Reconciliation Audit Tool
Purpose
To collect data and measure reduction in “discrepancies”
between home medication list and admission orders
Discrepancies
• Intentional – Physician has made an intentional choice to add,
change, discontinue a medication– Choice is clearly documented
• Undocumented Intentional – Physician has made an intentional choice to add,
change, discontinue a medication– Choice is not clearly documented
• Unintentional – Physician unintentionally changed, added, or omitted
a medication the patient was taking prior to admission
Measurements
• Mean # Undocumented Intentional
Discrepancies = # of undocumented discrepancies
# of patients
• Goal: Reduce the rate of undocumented intentional discrepancies at admission by 75% in 1 year
Measurements
• Mean # Unintentional Discrepancies = # of unintentional discrepancies
# of patients
• Goal: Reduce the rate of unintentional discrepancies at admission by 75% in 1 year
Measurements
• Medication Reconciliation Success Index =
# of NO discrepancies + # of documented intentional discrepancies X100
# of NO discrepancies + total # of ALL discrepancies
• Goal: To increase the effectiveness of the medication admission reconciliation process over time
Recording • Document details of discrepancies:
– Med Reconciliation form
– Patient’s Hospital record • Indicate if OTC medication
– Definition: A medication not prescribed by a physician– OTC medication discrepancies will not be reported to
National Safer Healthcare Now campaign
• Resolve or transfer to pharmacist for follow up
• Record if discrepancies were resolved on Med Reconciliation form • Recorder to sign form
Recording • Record Admission Date/Time
– Defined as time patient was designated to be admitted to hospital
– Not Emergency admission time
• Reconciliation Date/Time– Perform within 24 hours after admission
• Implementation Stage – Baseline – before changes to process – Early Implementation – after changes to process made
by a select team – Full Implementation – when medication reconciliation
process is integrated by all staff on designated ward

Investigator’s Role
• Lead investigator will collect audit forms
• Will be responsible for: – Completing Discrepancy Totals on forms– Calculating & reporting measurements
to National Safer Healthcare Now Campaign
– Reporting findings internally

Medication Reconciliation
Coming to a Hospital Near You!
NH-Wide Implementation
• Initial testing sites – Prince George – Quesnel – Dawson Creek– Burns Lake
• Goal: To standardize the Medication Reconciliation process
• Continue to spread implementation to all healthcare settings in Northern Health
Just Do It!
PUT THEORY INTO PRACTICE
ESTABLISH STANDARD PROCESS
PROMOTE MEDICATION SAFETY
BEGIN IMPLEMENTATION TODAY
Leading the Way
• You are the Trail Blazers – Role Models, Mentors, Educators – Promote cultural change – Lead by Example– Collaborate – Demand Excellence – Do not Compromise
Building it into the Process “The names of the patients whose lives we save
can never be known. Our contribution will be what did not happen to them. And, though they are unknown, we will know that mothers and fathers are at graduations and weddings they would have missed, and that grandchildren will know grandparents they might never have known, and holidays will be taken, and work completed, and books read, and symphonies heard, and gardens tended that, without our work, would never have been.” Donald M. Berwick, MD, MPP
President and CEO Institute for Healthcare Improvement
“Accomplishing the Impossible…
…means only that the boss will add it to your regular duties” – Doug Larson

















