16. Verbal Any Other Business Prof Nigel Ratcliffe 17.20
17. Date of Next Meeting – Wednesday 27 March 2013
Close 17.30
Page 1 of 30
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 01
Subject: Minutes of the Staffordshire and Stoke on Trent Partnership NHS Trust Board Meeting on Wednesday 30 January 2013
Lead: Melanie Print
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT:
The unapproved draft minutes of the Staffordshire and Stoke on Trent Partnership NHS Trust Board meeting held on 30 January 2013 are enclosed for review and approval. KEY POINTS:
An action tracker is attached that shows the status of each action. INTER DEPENDENCIES:
Legal and/or Risk N/A
Clinical N/A
Financial N/A
HR N/A
Social Care N/A
Patient & Public Involvement N/A
Equality Impact N/A
Requirement for further review N/A RECOMMENDATIONS / ACTION REQUIRED: The Trust Board is requested to appraise and approve the minutes of the Trust Board Meeting on Wednesday 30 January 2013.
Page 2 of 30
Page 3 of 30
Meeting of the Trust Board of Directors of Staffordshire and Stoke on Trent Partnership NHS Trust
Wednesday 30 January 2013 Morston House, The Midway, Newcastle under Lyme, Staffordshire ST5 1QG
Key: Overdue On Target Action Complete
ACTION TRACKER Action
No.
Date of
Meeting
Agenda
Item No.
Action Status/
Due Date
Comments (incl. interface with/reference to another Committee/Sub Committee/Working Group)
Responsible Officer
RAG
Rating
2012.260
31 10 12
8
The graph demonstrating ‘harm as a percentage of patients’ within the Quality Report to include numbers to give it some context i.e. the number of patients in community hospitals and the number of patients seen by community nurses.
28 11 12
The Director of Nursing & Quality informed Members that the information reported within the Quality Report for ‘harm as a percentage of patients’ could not be broken down any further. She confirmed that the information reported is in line with benchmarking with comparable services.
Director of Nursing & Quality
2012.274
28 11 12
4
Specialist Rheumatology Service, based in the Haywood Hospital to help share knowledge and train staff based within the Wombourne Clinic that would help.
30 01 13
The Medical Director informed Members that learning and training gained from the patient story has been shared with staff at Wombourne Clinic.
Medical Director
Page 4 of 30
2012.274
28 11 12
4
The Deputy Chief Executive Officer explained that the Pain Clinic that was commissioned for patients living within the Wombourne area was to visit Birmingham, rather than Burton-on-Trent and he confirmed the need for further investigation.
30 01 13
The Deputy Chief Executive Officer reported that arrangements have been discussed and are being formalised to ensure that patients living in the Wombourne area can receive treatment from the Pain Clinic in Birmingham rather than travelling to East Staffordshire.
Deputy Chief Executive Officer
2012.274
28 11 12
4
Contact with the patient representative to discuss the suggestion made re. messages sent to patients in advance.
30 01 13
The Director of Operations confirmed that contact has been made with the patient representative who has requested to link into the Trust on an on-going informal basis.
Director of Operations
2012.276
28 11 12
5
Director of Operations to look at the process of renewing changes as part of the internal report related to the West Midlands Quality Review (WMQR) Service Report – particularly the dementia mechanisms and the link into the Alzheimer’s process.
30 01 13
The Director of Operations informed Members that the internal report related to the Dementia Action Reliance and not the WMQR.
Director of Operations
2012.278
28 11 12
7
Director of Nursing & Quality to meet with Non Executive Director, Jeni Jobson, to discuss end of life care
30 01 13
Meeting took place on 20 02 13.
Director of Nursing & Quality
2012.282
28 11 12
12
The Director of Workforce & Development to develop a ‘grandfather review’ scheme and look into the issues raised by Non Executive Director, Jenny Hendon, re. staff leaving the organisation.
28 03 13
Item will be discussed at the Workforce Matters Sub Committee meeting to be held on 13/03/13.
Director of Workforce & Development
Page 5 of 30
2012.287
28 11 12
18
Deputy Chief Executive to contact Helen Parsons at Staffordshire LINK regarding the recruitment of Voluntary Sector representation.
30 01 13
The Deputy Chief Executive informed Members that Healthlink would like to take one of the voluntary sector seats on the Trust’s Board of Governors. He reported that he will report back progress at a future meeting.
Deputy Chief Executive Officer
2013.290
30 01 13
04
Trust Board Cycle of Business for 2013/14 to be published on the Trust website.
31 03 13
Company Secretary
2013.276
30 01 13
05
Training Academy timeframe to be confirmed at the Trust Board meeting on 27 February 2013.
27 02 13
Paper submitted to the Executive Management Team meeting 18/2/13 and paper to be presented at the Trust Board meeting on 27/2/13.
Director of Workforce & Development
2013.295
30 01 13
08
Context to previous performance to be included throughout future Quality reports to the Trust Board.
27 02 13
Director of Nursing & Quality
2013.295
30 01 13
08
Non Executive Director, David Pearson, to be appraised of the details of the serious incident regarding data.
27 02 13
Director of Finance & Resources
2013.302
30.01.13
14
Trust Board away day to be scheduled to include discussion on the next cycle of strategic objectives.
27 02 13
Deputy Chief Executive Officer
Page 6 of 30
2013.309
30 01 13
21
Director of Finance & Resources to forward an action plan to Elizabeth Jarrett, Development Worker, Staffordshire LINk to show what action is being taken around the delays in social care assessment, in order for her to reassure users/ carers of what is happening and to seek feedback on services.
27 02 13
Director of Finance & Resources
2013.309
30 01 13
21
Chief Executive Officer to ensure that the final policy for the reimbursement of expenses for user/carers to be sent to Elizabeth Jarrett, Staffordshire LINk.
27 02 13
Received at Quality Governance Committee and revised recommendations in relation to reimbursement agreed. Revised policy to be consulted on.
Chief Executive Officer
2013.309
30 01 13
21
Chief Executive Officer agreed to take the issue of: the recruitment of the right calibre of staff to deliver the changes that were discussed at the Trust Board meeting to the Risk Committee for information.
27 02 13
Chief Executive Officer
Page 7 of 30
Present: Prof Roger Evans Non Executive Director Paula Furnival Director of Operations Geraint Griffiths Deputy Chief Executive Director Siobhan Heafield Director of Nursing and Quality Jenny Hendon Non Executive Director Jennifer Ledgar Vice Chair and Non Executive Director
David Pearson Non Executive Director Stuart Poynor Chief Executive Officer Prof Nigel Ratcliffe Chairman Dr John Scarpello Non Executive Director Designate Andrew Talbot Non Executive Director Designate Julie Tanner Director of Workforce & Development Jonathan Tringham Director of Finance & Resources Dr Doug Wulff Medical Director
Apologies: Jeni Jobson Non Executive Director
In attendance: Wendy Dale Corporate Business Manager Dianne Hooley Executive Assistant to the Chairman Melanie Print Company- Secretary
2013.289
Welcome and Apologies The Chairman welcomed Trust Board Members and members of the public to the meeting and noted apologies from Non Executive Director, Jeni Jobson. The Chairman welcomed Giles Tinsley from NHS Midlands & East to the meeting who, he explained, would be observing the meeting. The Chairman informed members of the public that meetings are held at different venues around the county to enable as much representation as possible and he welcomed the following people to the meeting:
• Alison Dowsett GlaxoSmithKline • Martha Keith GlaxoSmithKline • Elizabeth Jarrett Staffordshire LINk • Katie Lee Partnership Trust • Steph Woodhouse Partnership Trust
The Chairman reported that comments were raised at the previous board meeting regarding the order of the meeting agenda and the time taken on items prior to discussing the Trust’s financial report. The Chairman confirmed that the priority of the Trust Board is that of the quality and safety of services delivered hence the reason why Finance is discussed later in the meeting.
MEETING OF THE TRUST BOARD OF STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST
Wednesday 30 January 2013 Morston House, The Midway, Newcastle under Lyme, Staffordshire ST5 1QG
MINUTES
Page 8 of 30
The Chairman also reported that as part of the Trust’s Foundation Trust application the business cycle of the Trust Board for 2013/14 will be published on the Trust website. The Chairman explained when questions would be taken from members of the public. He invited questions at the start of the meeting to enable immediate points in the agenda to be addressed. He added that further questions would be received at the end of the meeting.
MP
2013.290 Declarations of Interest The Chairman asked if Members had any declarations of interest to declare at this meeting. None were raised.
2013.291 Patient Story The Chairman explained that a patient carer or representative is invited to attend every meeting to talk about their experience of receiving Community Health and Adult Social Care Services. He welcomed Mr Brian Lee to the meeting who talked about the services he has received from the Community Intervention Service in Eccleshall. Mr Lee talked about his condition – Emphysema/Chronic Obstructive Pulmonary Disorder - and the journey he has taken to receive services from the Community Intervention Service. He explained that he has lived in Staffordshire for three years, having moved from Manchester to be closer to his family. Having spent a number of periods in an acute hospital setting, whilst living in Manchester, Mr Lee explained that when his GP informed him that he may need to go into hospital for an episode of care, he refused. This is when Mr Lee was introduced to the Community Intervention Service. Mr Lee praised the work and his experience of interactions he has had with the service, the physiotherapy received in his own home, and the medication that has helped to reduce the levels of mucus in his lungs. Mr Lee informed Members that instead of having to visit the health clinic every two weeks for blood tests, he now only attends a monthly Respiratory Clinic. Mr Lee informed Members that he has an emergency pack that contains antibiotics and steroids and should his condition deteriorate, he has the contact details of his community nurse who will visit him at home. Mr Lee talked about the benefits of the care he receives and how his quality of life has improved to such an extent that he is now able to manage his condition. He explained that the service has prevented his admission to an acute hospital setting three times in the last three years. The Chairman thanked Mr Lee for sharing his experience with Members of the Trust Board and asked if anyone had any questions or comments. Non Executive Director, David Pearson, thanked Mr Lee for sharing his experiences with Members and asked him if he has a copy of his care plan at home and if it included a crises plan. Mr Lee informed Members that he has his care plan with him at all times and that he knows who to contact in an emergency. Non Executive Director, Dr John Scarpello, asked Mr Lee how much time, on average, he would spend in hospital previously and how often he was admitted. Mr Lee said that he was admitted every six months or so – anything from a visit that may only last an hour up to five days.
Page 9 of 30
The Director of Nursing & Quality confirmed that Mr Lee’s experience is a great example of how the Model of Care works and one to share with commissioners. The Deputy Chief Executive agreed and noted that the Integrated Locality Team model is predicated on meeting the specific needs of service users within a locality, mapped by reference to the demography of the locality. The Chief Executive Officer thanked Mr Lee for his positive account – an endorsement of what the Trust Board wants to implement under the Model of Care. He confirmed that Mr Lee is confident in the system and understands it well – a real example of self care management. Mr Lee stressed the importance to care for people more in this way and to inform people of what care is available to keep them out of hospital. The Chairman thanked Mr Lee for his time and asked if Mr lee wished to remain for the remainder of the meeting. Mr Lee thanked the Chairman and elected to leave the meeting at that point.
2013.292 Minutes of the meeting and matters arising The Chairman referred Members of the Trust Board to the minutes of the meeting held on 28 November 2012. Members of the Trust Board agreed that the minutes were a true and accurate record of the meeting, subject to the following changes:
• Page 5, 2012.272, the representative from Staffordshire LiNKs name is Hester Parsons and not Helen Parsons.
• Page 10, 2012.278, 2nd para, 3rd line – replace the words ‘rather than a cure’ with ‘and that their families are aware of the Liverpool Care Pathway’.
• Page 10, 2012.278, 7th para, 3rd line – replace the word ‘Therapy’ with ‘Assessment’.
• Page 18, 2012.284, 2nd para, 1st line – replace the word ‘policy’ with ‘medical appraisal’.
Members of the Trust Board reviewed the action tracker and gave the following verbal updates:
• 2012.260 – the Director of Nursing & Quality informed Members that the details, in the graph ‘harm as a percentage of patients’ in the Quality Report, cannot be broken down any further. She confirmed that there are no adverse consequences and that the reporting is in line with benchmarking against comparable services.
• 2012.274 – the Medical Director reported to Members that he has shared the knowledge and training with staff based at Wombourne Clinic following the patient story given at the meeting held on 28 November 2012.
• 2012.274 – the Deputy Chief Executive Officer reported that arrangements are being formalised to ensure that patients living in the Wombourne area can receive treatment from the Pain Clinic in Birmingham rather than travelling to East Staffordshire.
• 2012.274 - the Director of Operations confirmed that contact has been made with the patient representative who has requested that she link into the Trust on an on-going informal basis.
• 2012.276 - the Director of Operations informed Members that the internal report related to the Dementia Action Reliance and not the WMQRS report.
• 2012.278 – the Director of Workforce & Development reported that a date is yet
Page 10 of 30
to be confirmed for her to meet with Non Executive Director
• 2012.282 - the Director of Workforce & Development reported that the issue will be discussed at the next Workforce Matters Sub Committee meeting.
• 2012.287 - the Deputy Chief Executive informed Members that Healthlink has expressed an interest in becoming a voluntary sector governor. He reported that he will report back progress at a future meeting.
Members of the Trust Board accepted the minutes of the meeting held on 28 November 2012 as a true and accurate record subject to the changes noted and received assurance from the Executive Directors from the updates provided from the action tracker.
2012.276 Chief Executive Officer Report The Chief Executive Officer referred Members of the Trust Board to his report and highlighted the following areas:
• Commissioners’ recognition of the system changes required to ensure that people are provided with care and support in community setting in a planned way so as to reduce admissions to hospital.
• Positive discussions having taken place during the round of negotiations for the 2013/14 contract year with commissioners, in relation to additional investment in community services. The Chief Executive Officer informed Members of an expected investment into the Trust to avoid unnecessary admissions.
• Work around the Trust’s Training Academy is progressing and has been covered in the local press and media. The Training Academy will bring about thirty staff into the Trust and enable the organisation to develop its own workforce. The Chief Executive Officer confirmed that timescales will be confirmed at the Trust Board meeting in February.
• The Chief Executive Officer reported back from his visits to frontline services included the work of the Family Nursing Partnership – a personalised service to support young mothers; and time spent with the Adult Care Teams who had put together a role play session to demonstrate the difficulty service users encounter when trying to access support in times of crises. He reported that the Adult Care Teams demonstrated the benefits of integrated health and social care teams.
Vice Chair and Non Executive Director, Jennifer Ledgar, referred Members to page four of the report ‘Government investment to boost health research’ and asked if there is an opportunity for the Trust to be involved. The Medical Director reported that the Trust is looking at the projects available. Vice Chair and Non Executive Director, Jennifer Ledgar, referred Members to page four of the report ‘New figures show wide disparity in dementia diagnosis’ and asked what percentage of people with dementia are diagnosed in Staffordshire and Stoke-on-Trent. The Chief Executive Officer confirmed that the figures are recorded at a Commissioner level. The Chairman asked how patients would benefit from knowing that they were in the early stage of dementia. The Chairman’s concern was to be sure that undue and unnecessary concern was not raised too early with the patient and that there was not an unnecessary reduction, due to concern, in the quality of the patient’s life. The Medical Director confirmed the importance of preparation and support for patients and carers to build memory books/walls that will support them through the different stages of the condition. The Chief Executive Officer confirmed the
JkT
Page 11 of 30
importance for the Trust to work with voluntary services and agencies such as the Alzheimer’s Society. Non Executive Director, David Pearson, confirmed the need to have dementia specialists working in teams Members noted the contents of the report.
2013.293 Minutes of the Finance, Investment & Performance and Quality Governance Committees – Chairs Reports
Audit Committee Vice Chair and Non Executive Director, Jennifer Ledgar, presented the minutes of the Audit Committee meeting held on 23 November 2012 and gave an update on the items of business discussed at the recent meeting of the Audit Committee on 18 January 2013. Vice Chair and Non Executive Director, Jennifer Ledgar reported that Non Executive Director, David Pearson, had attended his first meeting. Vice Chair and Non Executive Director, Jennifer Ledgar, reported the following key points:
• The Committee has met its cycle of business for 2012/13 and will be looking at the cycle of business for 2013/14 at its meeting in March 2013.
• The Director of Workforce & Development provided the Committee with an update on the controls that have been put in place to manage bank and agency spend and informed the Committee of the business case put in place to provide better value for money.
• The Committee was pleased to note that all recommendations in relation to the review of data quality and incident reports, in relation to the tissue viability audit, had all been implemented and directed that Directors will be required to provide assurance that any recommendations made, in consequence of any further reports, will be implemented on time. Directors who are the “owner” of the actions have attended and will be invited to attend, meetings to provide an update on actions of high importance.
• The Committee received adequate assurance in relation to the review of Adult Safeguarding procedures and has recommended that the Quality Governance Committee undertake a review of the proposed improvements into the controls and processes currently in place.
• The Committee received an update on the domiciliary care review and has directed that a written response from the Director of Operations and the Joint Commissioning Unit (JCU) of Staffordshire County Council is provided to support the verbal assurance given at the meeting that the recommendations of Staffordshire County Council’s internal auditors have been implemented.
• No issues of concern in relation to the Trust’s compliance with International Auditing Standards and noted the published timeline for the audit and publication of the Trust’s Audited Accounts for 2012/13. The Trust Board was asked to note the need for an extraordinary Board Meeting on 28 May 2013.
• The Committee had reviewed quarter 2 of the Board Assurance Framework (BAF) noting that a number of thematic reviews have been undertaken by both the QGC and Audit Committee in relation to the effectiveness of the controls and assurance that it and the Trust Board requires in relation to key services and business of the Trust.
• The Committee recommended that the next review of the BAF (Quarter 3) should include control gaps in relation to domiciliary care and adult
Page 12 of 30
safeguarding.
The Chairman thanked Jennifer Ledgar for the update and asked for the meaning of a control gap. Jennifer Ledgar explained that this is when the Committee is not satisfied that there is an adequate control in place to provide assurance. The Chairman asked for clarification on the classification of adequate assurance from the County Council in relation to the review of Adult Safeguarding procedures. The Company Secretary confirmed that the classifications are ones used by the County Council for its audit service.
Members of the Trust Board: • Received the approved minutes of the meeting of the Audit Committee of
23 November 2012; • Noted the Chair’s report and were assured that the Committee is meeting
its Cycle of Business and discharging its Terms of Reference; • Noted the need for an extraordinary Trust Board meeting to take place on
28 May 2013 to receive the audited Annual Accounts for 2012/13. Finance, Investment & Performance Committee The Director of Finance & Resources presented the approved minutes of the Finance Investment & Performance Committee held on 19 December 2012 and gave an update on the items of business discussed at the meeting held on 16 January 2013. The Director of Finance & Resources referred Members of the Trust Board to the following key points:
• The Committee reviewed the month nine financial report, noting that the actual surplus to the end of December 2012 was £1,021k. The (mitigated) forecast gap is £1,324k and the Committee has urged that additional Cost Improvement Programmes (CIPs) be brought on line and that full budgetary control is maintained so as to ensure full delivery of the CIP by the year end.
• The Committee fully supported the additional investment in community services so that additional capacity can be secured to support the local health economy at a time of significant pressure.
• The Committee noted significant improvement in the spend on agency staff, noting that options for the development of a vibrant Trust Bank will be completed in the next quarter.
• The Committee reviewed the Standard Operating Model noting that all performance indicators are now rated green.
• The Committee approved tenders - Staff Wellbeing Service and Linen and Laundry Service – both of which will generate savings, and the Diabetic Retinopathy Service.
• The Committee received, reviewed and noted the quarterly update on Supplies and Procurement.
• The Committee received the first data confidence score assessments and were pleased to note that these assessments will now be applied to other indicators for the remainder of the year.
• The Committee reviewed the Information Management & Technology Strategy noting that it now supersedes the Information Services Strategy approved by the Trust Board in January 2012.
Page 13 of 30
Non Executive Director, Jenny Hendon, added the following key points on behalf of the Committee Chair noting that the Quarterly procurement update had not provided assurance that innovation was being applied to the supplies and products that had been identified in the procurement plan for the Trust. She emphasised the uniqueness of the Data Confidence Score and its benefits to the organisation.
Members of the Trust Board: • Noted the approved minutes of the Finance, Investment & Performance
Committee meeting on 19 December 2012; • Noted the business covered at the meeting held on 16 January 2013; • Were assured that the Committee was being effective in discharging its
Terms of Reference and cycle of business. Quality Governance Committee Non Executive Director, David Pearson, presented the approved minutes of the meeting of the Quality Governance Committee of the 5 December 2012. Non Executive Director, David Pearson, thanked Non Executive Director, Prof Roger Evans, for the progress that had been made since the establishment of the Committee in developing its roles and responsibility. He confirmed Prof Roger Evans’ move to Chair of the Children’s Board. Non Executive Director, David Pearson, reported that more work is being done by the Committee to reinforce the importance of deadlines and completeness of papers to ensure meeting papers are distributed seven days before each meeting. Non Executive Director, David Pearson, referred Members to the following key points:
• Limited assurance provided in relation to the proposed handover of the functions and streams of the Adult Social Quality & Governance Sub-Committee.
• The Committee continues to monitor achievement against Monitor’s Quality Framework so as to secure the required assessment score of 3.5 – to be independently assessed against Monitor’s Quality Governance Framework by KPMG.
• The Committee received update reports on the positive inspections by the Care Quality Council (CQC) of East Staffordshire and Stafford Living Independently Staffordshire and the inspection of HMP YOI Werrington.
• The Committee noted that all actions and recommendations of the Internal Auditors review and audit of the reporting of incidents relating to pressure ulcers had been implemented.
• The Committee had received two thematic reviews.
• The Committee had noted that the Refusal of Care policy has now been implemented in relation to Adult Social Care.
• The Committee agreed that Model B of the new bespoke quality performance indicators, which supplement the Standard Operating Model, should now be developed by the Performance Team.
Members of the Trust Board noted the report and received the minutes of the meeting of the Quality Governance Committee meeting held on 5 December 2012.
2013.294 Board Assurance Framework 2012/13 Quarter 2 Update The Company Secretary presented the Board Assurance Framework (BAF) and
Page 14 of 30
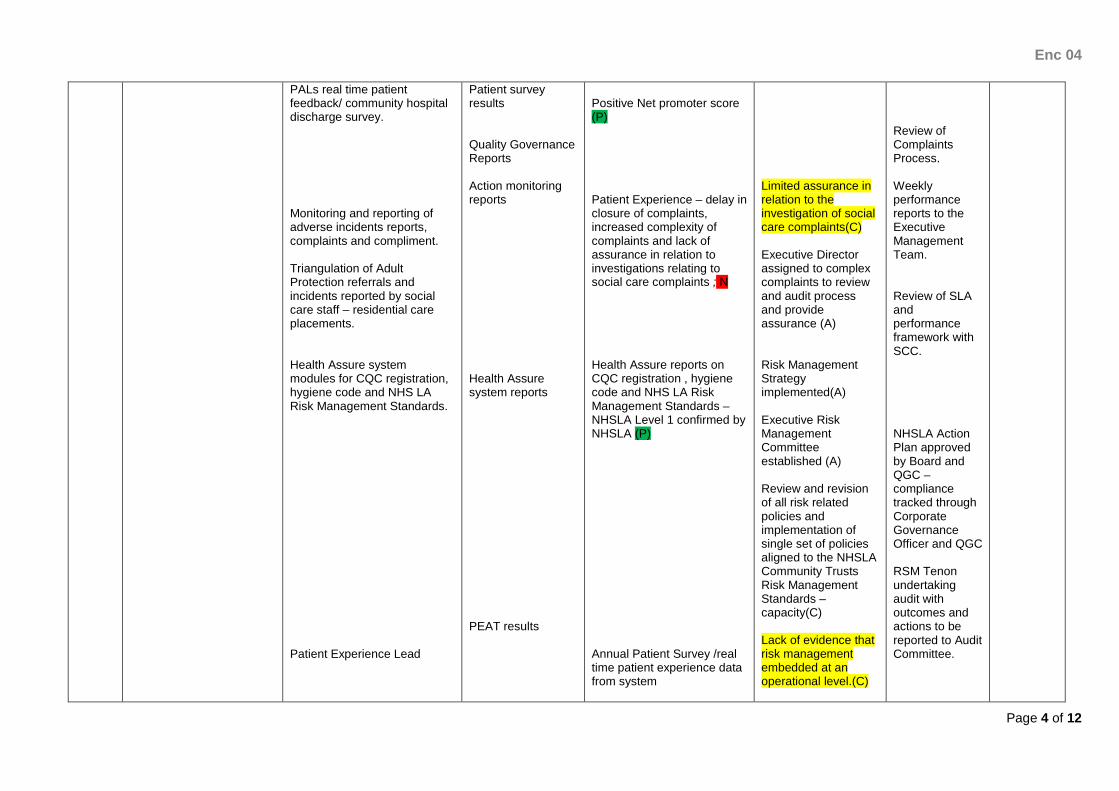
informed Members of the Trust Board that it has been subject to a full review as at the end of Quarter 2. The Company Secretary informed Members that the previously reported key controls and assurances are not static but are aligned to the principal risks to the Trust’s strategic goals, aligned to the risks reported on the Corporate Risk Register and have been the subject of a systematic review. The Company Secretary reported that any gaps in controls and assurance are aligned in the BAF and are the subject of review by the lead Director and the Committee/Sub Committee assigned to relevant strategic goals. The Company Secretary gave additional assurance as to the controls and assurances in place that is provided by quarterly reviews by the Audit Committee with input from the Trust’s internal auditors – RSM Tenon. The Company Secretary informed Members that the next iteration of the BAF, following quarter 3 review, will be presented to the Audit Committee at its meeting on 22 March 2013. The Company Secretary referred Members to areas of the BAF that have been updated, e.g. the Trust has received three positive inspections of the Living Independently Staffordshire and one for HMP YOI Werrington. The Company Secretary reported two additional control gaps to be highlighted, firstly in relation to the limited assurance for Domiciliary Care; and secondly, in relation to the Quality Impact Assessment for the Cost Improvement Programme. She informed Members that the Audit Committee took assurance that the Quality Impact Assessment for Cost Improvement Programme would be presented to the Trust Board at its meeting on 30 January 2013. The Director of Nursing & Quality informed Members that the negative assurance given for the Internal Audit review of pressure ulcers and Route Causes Analysis on page 3 will change in the next iteration. She confirmed that the Tissue Viability Panel has met recently and that there are no remaining serious incidents outstanding for investigation. The Deputy Chief Executive note further updates on page 5 of the report.
Members of the Trust Board: • Noted the quarter 2 review of the BAF in the form appended to the report; • Noted the recommendations of the Audit Committee; • Noted the quarter 3 review will be presented to the next meeting of the
Audit Committee; and • Received assurance that the Audit Committee has reviewed the BAF and
will undertake a further review in March 2013.
2013.295 Quality Report The Director of Nursing & Quality presented Members of the Trust Board with an update on the experience, safety and clinical effectiveness of users and carers during December 2012; and to provide assurance to Members that where there any issues of patient safety identified, then appropriate actions are taken to address and mitigate them. The Director of Nursing & Quality reported the following key points:
• Percentage of users experiencing no harms throughout their care journey has
Page 15 of 30
increased from 87.88% in April 2012 to 92.62% in December 2012. The number of new harms remains low at 3.03%.
• Overall number of incidents reported during December 2012 has declined by 140 and the number of incidents identified at point of admission has fallen by 30 since October 2012. Incidents identified within or attributable to the Trust have further declined by 110 incidents since October 2012. The decline is outside the established control limits but corresponds to previous reporting periods of similar time period over December 2012. The Director of Nursing & Quality confirmed that the Aspirant Community Foundation Trust (CFT) benchmarking tool has been used to compare the Trust’s reported data.
• 23 formal complaints received in December 2012 with 100% compliance for the acknowledgement of all complaints. The Social Care compliancy rate of closures within agreed timescale has increased from 40% to 50%. The Health Care compliancy rate of closure has been sustained at 100%.
• Further work being undertaken to restrict extensions of time to complaint responses and tightening of deadlines.
• 94 Patient, Advice & Liaison (PALs) service contacts were received – 33 relating to services directly provided by the Trust.
• 151 compliments received with a very positive Net Promoter Score of +72.11.
• Dissemination of the Quality Framework is progressing well with work underway with Staffordshire County Council Joint Commissioning Unit to integrate some of the Council’s information and data into the Trust’s Quality Report.
• Summary information included in the report on the Documentation Campaign and the progress made against its five work streams.
• A significant drive on Health Assure training to facilitate the appropriate population and validation of evidence on the system.
The Director of Nursing & Quality informed Members of the unacceptable performance around social care complaints management and assured the Trust Board of work with the Council to improve this. She confirmed that the negotiation of complaint deadlines will only take place with complainants in the future if additional time is required for clinical reasons only. The Chairman thanked the Director of Nursing & Quality for her report and asked Members of the Trust Board for questions. The Chairman asked the Director of Nursing & Quality to explain the net promoter score and how this is calculated. The Director of Nursing & Quality confirmed that the score relates to 10% of footfall within a service. The Chairman asked to see some context to previous performance throughout the report. The Chairman referred Members to the number of compliments received (151) compared to the number of complaints (23) for the month and confirmed that the overall message is a positive one. Non Executive Director, Prof Roger Evans, supported the Chairman and that the number of compliments should be highlighted. Non Executive Director Designate, Andrew Talbot, referred Members to chart 2 on page 32 of the report – Joint Commissioning Unit (JCU) contract monitoring summary dashboard – and asked if the JCU monitors the quality of the teams on behalf of the Trust. He raised concern that the table indicates that only 50% of visits have been completed. The Director of Nursing & Quality confirmed that the JCU performance and quality
SH
Page 16 of 30
reports relate to care provided under the Third Party Contracts (with the County Council) in Care Homes and by Domiciliary Care providers. She noted that this is being addressed and confirmed that the Trust is now copied into the risk register that identifies every organisation that the JCU commissions services from. The Chief Executive Officer reported that the risk register is presented to the Audit and Quality Governance Committees. He reported that he has written to the Chief Executive Officer at Staffordshire County Council expressing his disappointment of progress to-date. The Chief Executive Officer noted that the Trust was triangulating incidents with the reports that had made by the Quality Monitoring Officers of the County Council and the Trust is looking to the County Council to increase the number of visits made by this Team. The Chief Executive Officer noted that CQC retains primary responsibility for the inspection and registration of Care Homes and Domiciliary Care providers; the JCU undertakes quality monitoring and the Trust provides soft intelligence through its staff and the reporting of incidents in Care Homes. He noted that the challenge is to secure consistency in relation to the systems and controls that are in place. He assured the Board that this is being actively addressed with the County Council. Vice Chair and Non-Executive Director, Jennifer Ledgar, noted that the Audit Committee had indicated to the Chief Operating Officer (Social Care) and a representative of the JCU that they were looking for a real step change in the performance monitoring of Third Party Contract providers in Domiciliary Care. Vice Chair and Non-Executive Director, Jennifer Ledgar, referred Members to the development areas outlined on page 30 of the report following a Care Quality Council visit to HMP YOI Werrington and congratulated the team on the clear demonstration of zero tolerance. Vice Chair and Non Executive Director, Jennifer Ledgar, also informed the Director of Nursing & Quality that she found the ‘lessons learnt/recommendations’ listed on page 12 to be useful. Non Executive Director, David Pearson, referred Members to page 12 of the report and the confidential leak of information and asked if the Executive Management Team is assured that processes are safe. The Director of Finance & Resources informed Members that some of the records in the incident were misplaced for a period of time. He agreed to appraise David Pearson of the details outside of the meeting and assured him that controls had been put in place to mitigate the risk of misplaced records. Non Executive Director, David Pearson, asked if the spread of compliments received by the Trust were consistent across the Trust. The Director of Operations confirmed that all compliments and complaints received by the organisation are communicated to teams. The Medical Director noted there is no national measure currently for Community Trusts for mortality. He assured Members that there has not been an increase in deaths across hospitals compared to the increase in the numbers of patients now being received in to the community hospitals. The Chairman asked if there is any concern with the number of staff being trained on the Health Assure system. The Director of Nursing & Quality assured the Board that there had been a recent drive to ensure that the uptake of staff being trained on Health Assure improved.
JT
Page 17 of 30
Members of the Trust Board discussed and noted the contents of the Quality Report and were assured that systems and processes are in place to identify patient safety, service user/carer experience and clinical effectiveness for the Partnership Trust.
Members of the Trust Board were assured that all areas are being managed appropriately along with implementation and improvement plans in place to address lessons learnt.
2013.297 Quality Impact Assessment of Cost Improvement Programme The Medical Director informed Members that KPMG had carried out an audit of the Trust’s Quality Governance in the summer of 2012 against Monitor’s Quality Governance Framework. He reported that Quality Impact Assessment of the Trust’s Cost Improvement Programme was highlighted as an ‘amber/red’ alert. The Medical Director highlighted the risks and informed Members of the process put in place to address them. He, and the Director of Nursing & Quality, presented the process schematic representation (see below) and the process in terms of training requirements.
Key:
DMT Divisional Management Team
FIP Finance, Investment & Performance Committee
KPI Key Performance Indicator
QIA Quality Impact Assessment
SEOG Safety, Effectiveness Operational Group
The Chairman thanked the Medical Director and the Director of Nursing & Quality for their presentation and confirmed that the proposed process was a robust one and reported that Members will be kept updated of the implementation of the Quality Impact Assessments of the Cost Improvement Programme. Non Executive Director Designate, Dr John Scarpello, agreed with the Chairman and congratulated the Medical Director, Director of Nursing & Quality and their colleagues for putting the process in place. He confirmed that most of the improvement measures will relate to changes of practice, rather than a change of treatment, and asked how this will be audited and how any improvements in quality are demonstrated.
Page 18 of 30
The Medical Director informed Dr Scarpello that part of the responsibility of service leads and professionals is to identify the quality indicators for each service. The Deputy Chief Executive Officer informed Members that the Finance Investment & Performance Committee and the Quality Governance Committee will incorporate quarterly updates and reviews of the Quality Impact Assessment of the CIP into their Cycles of Business.
Members of the Trust Board noted the update.
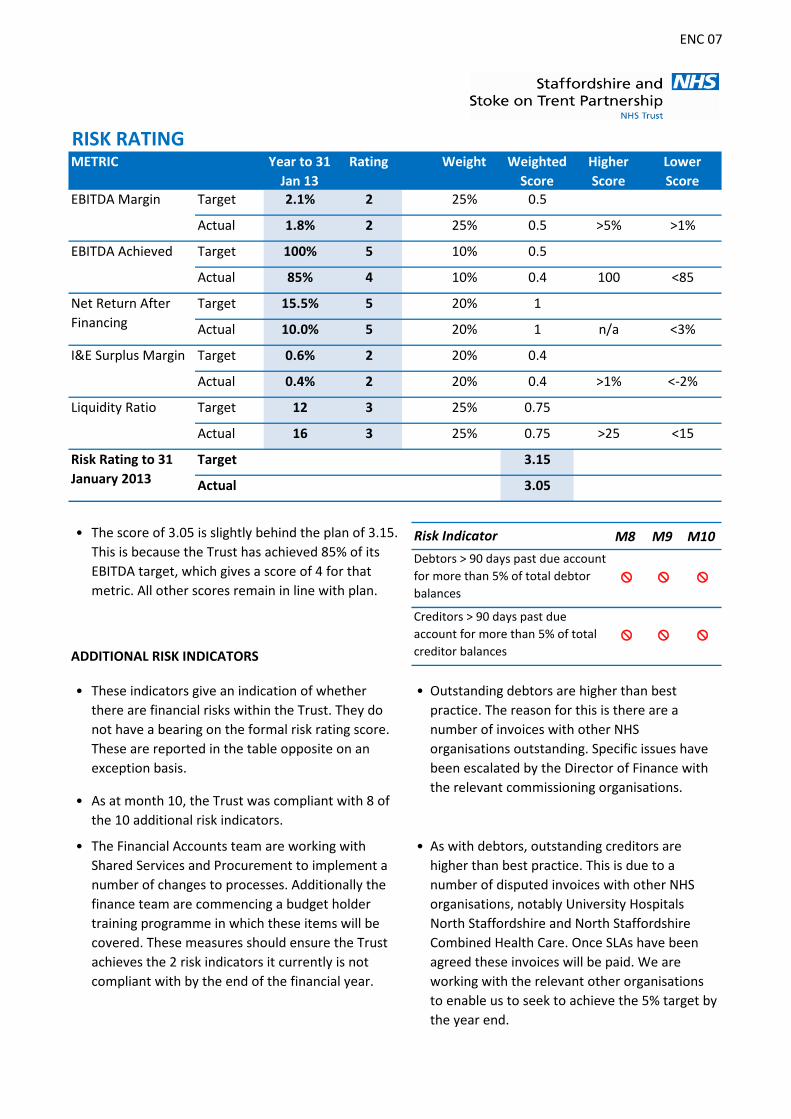
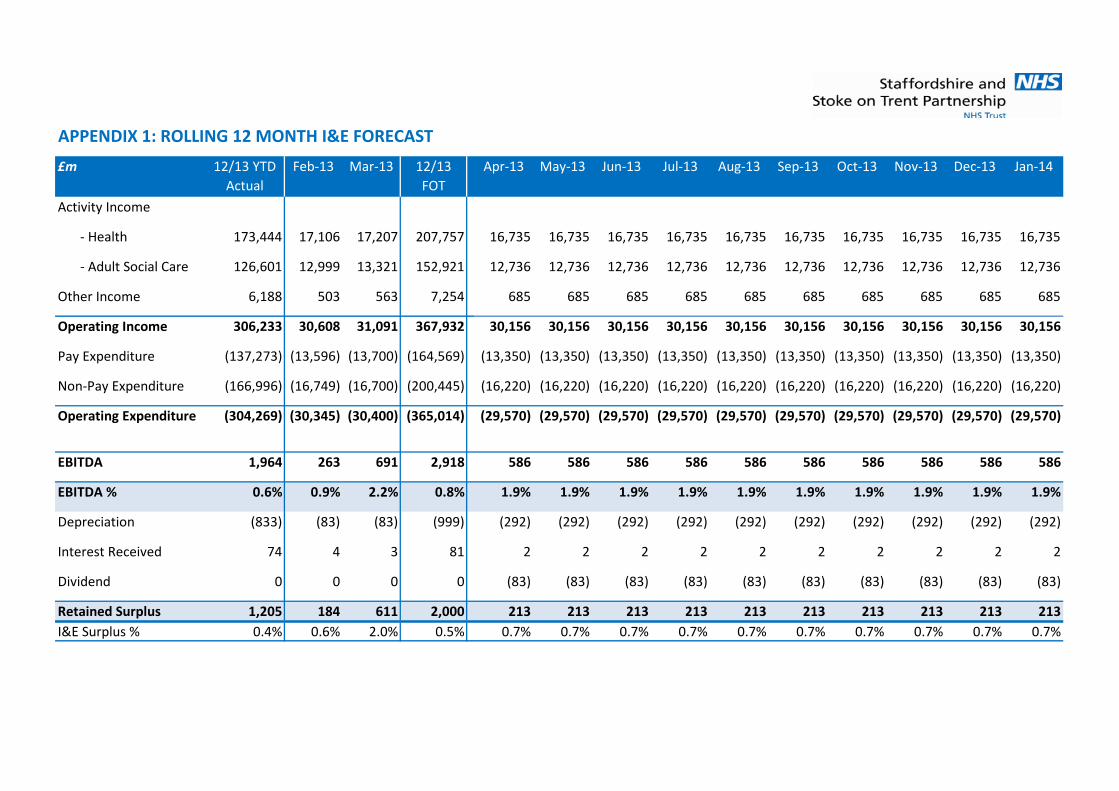
2013.298 Finance Report The Director of Finance & Resources presented the Finance Report for the period ending 31 December 2012. The Director of Finance & Resources confirmed that the new format and style of the report meets the Foundation Trust reporting requirements. He confirmed that the new format was taken to the Finance, Investment & Performance Committee in November 2012. The Director of Finance & Resources reported that the Trust is reporting an actual surplus of £1.021m for the nine months to 31 December 2012 representing an under performance against a plan of £0.64m. The Director of Finance & Resources reported that the Trust is forecasting that it will achieve the required surplus of £2m. He asked Members to note that, as a result of making increased investments to provide sufficient capacity in community services across the health system during the sustained periods of increased pressures, as seen in recent weeks, there has been a negative effect on the level of financial flexibility available to the Trust. This combined with a shortfall against the Cost Improvement Programme leads to a higher degree of risk in achieving our planned surplus. The Director of Finance & Resources gave an outline of the year to date together with an overview:
• of the principal financial risks; • the statement of comprehensive income; • risks and opportunities; and • operational performance. Non Executive Director, Jenny Hendon, referred Members to page 5 of the report – Income – and the Rolling 12 Month I&E Forecast on page 10 and asked why £200k is forecasted for year end and why the variance is greater at year end. The Director of Finance & Resources informed Members that there will be a real drop income in consequence of the tariff deflator of 1.3%. The Director of Finance & Resources informed Jenny Hendon that he would be reporting to the next meeting of the FIP Committee the steps taken to offset the reduction. Non Executive, David Pearson, confirmed that the new format was very clear. He asked what the residual effect will be on the Cost Improvement Programme for 2013/14, in consequence of the application of non-recurrent measures to meet the Cost Improvement Programme for 2012/13. The Director of Finance & Resources reported that this was still being quantified. He informed Members that the Trust built in an additional £2m at month four for 2013/14 however that the actual of that is lower at around £1m. He reported that the £2m would be built into the Cost Improvement Programme for 2013/14 and that
Page 19 of 30
the reconciliation of what is recurrent and what is not will be presented to the Trust Board meeting in February 2013. The Director of Nursing & Quality referred Members to the increase in agency spend noting the need to develop a vibrant Bank within the Trust. The Director of Finance & Resources reported that the level of agency spend in the North Division had not decreased. The Director of Nursing & Quality informed Members of the active recruitment to community hospitals and the difficulties experienced to find the right calibre of staff. Staffside representative, Chris Beswick, informed Members that staff are concerned that savings will not be realised in the Cost Improvement Programme and that the pace of securing savings has been delayed. The Director of Operations agreed that it is difficult and that members of the Executive Management Team have had discussions with the Joint Staffordshire Partnership about the management of the changes. She informed members that she and the Director of Nursing & Quality were meeting with Chris Beswick to discuss podiatry.
Members of the Trust Board noted the financial performance for the period and the increased risk associated with the forecast position.
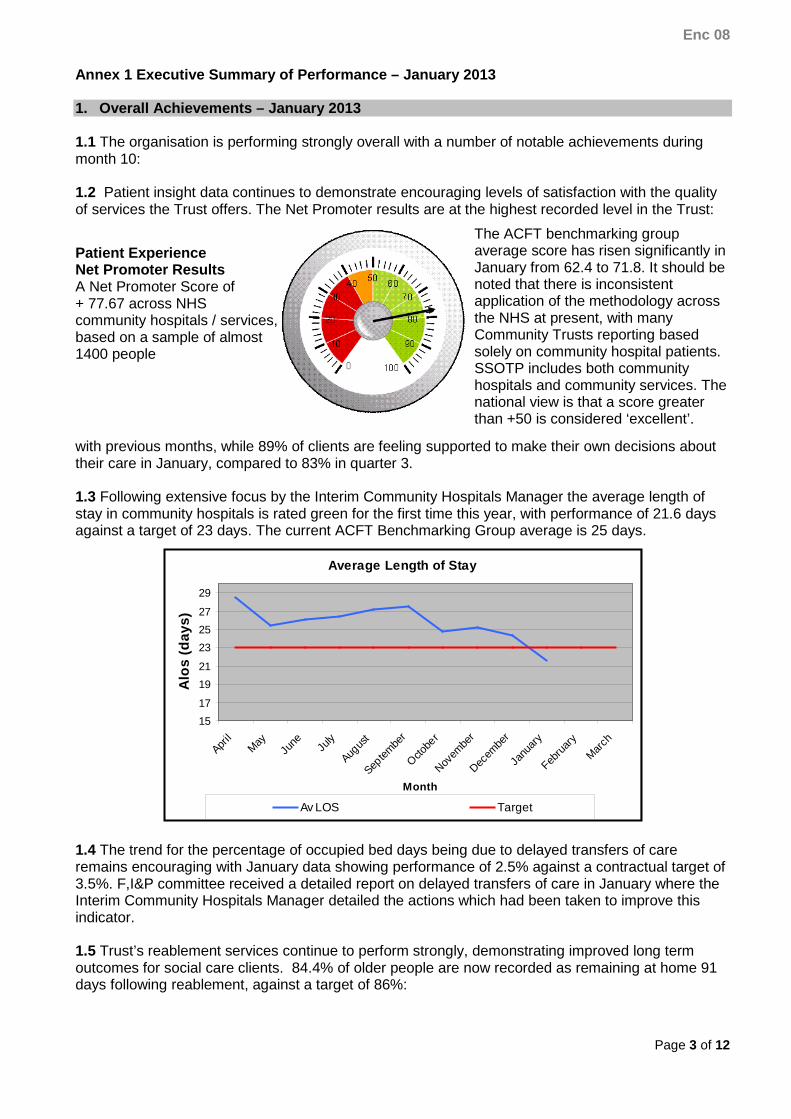
2013.299 Integrated Performance Report The Director of Finance & Resources presented the integrated performance report from 1 April to 31 December 2012. The Director of Finance & Resources reported that Clostridium Difficile is now rated ‘green’; strong performance against reablement teams; improved levels of Delayed Transfers of Care; reduced Average Length of Stay; and continued strong performance against Net Promoter score and customer satisfaction in social care. The Director of Finance & Resources reported a slightly revised Standard Operating Model; the performance against sickness levels remaining in excess of 5%; a declining response to social care complaints within agreed timescales and that the financial performance is behind plan. The Director of Finance & Resources confirmed the core indicators for consideration as follows: • appraisals within health teams dropped below 90%; • statutory and mandatory training; • time from social care assessments to services being implemented – 68.9%; • smoking quitters 9% below plan; and • waiting time performance for physiotherapy and podiatry at 44% and 64.3%. The Chairman confirmed that there is little the Trust can do at the moment to reduce the sickness levels in view of the pace of change that staff are expected to embrace. Non Executive Director, Prof Roger Evans, asked who sets the sickness levels. The Director of Workforce & Development confirmed that the target is national and was set three years ago. She reported that a number of Trusts are finding the target challenging. Non Executive Director Designate, Dr John Scarpello, noted that waiting times in physiotherapy had increased and asked what the rationale for the increase was. The Director of Operations reported increased referrals from the University Hospital of North Staffordshire for post-operative physiotherapy. She noted that there were
Page 20 of 30
on-going discussions with Commissioners about investment to meet demand. Non Executive Director Designate, Andrew Talbot, reported a concern that the Trust will not meet 100% training for staff. The Director of Workforce & Development reported that the target is 95% and confirmed that the new Head of Workforce will start shortly and the achievement of this target will be one of her priorities. Non Executive Director, Jenny Hendon, asked what the action plan for the time for referral to implementation of Social Care services related to. The Director of Operations confirmed that the target is in two parts: from time of referral to completion of assessment; and from assessment to commencement of services. She reported that both of the targets are monitored and action taken to address shortfalls. Where the latter part of the target is under-performing the information is fed back to the County Council to improve the access to and availability of services they commission in the independent sector. The first part of the target is owned by the Trust and staff are often moved around services in order to address demand pressures and to ensure timely responses.
Members of the Trust Board noted the report.
2013.300 Data Quality Update The Director of Finance & Resources provided a verbal update on Data Quality. He reminded Members of the Trust Board that the Trust inherited two informatics providers and three sets of procedures/processes. He confirmed that data quality issues are common in Community Trusts. The Director of Finance & Resources confirmed that a multi-disciplinary data quality group has been established; a policy and strategy developed along with a detailed action plan; the establishment of a single data warehouse and a suite of data validation reports; and the development and implementation of a data quality confidence score. The Director of Finance & Resources reported the following current issues: completeness of timely input by staff; an audit by RSM Tenon had shown some gaps in recording which pointed to the need for training; and that a proportion of community hospital activity FCEs are not captured.
Members of the Board noted the verbal update.
2013.301 Policy for the Development & Implementation of Procedural Documents The Company Secretary informed Members that the Trust will be assessed against compliance with the NHS Litigation Authority Risk Management Standards at Level 1 on 26 and 27 March 2013. She reported that the Policy for the Development and Implementation of Procedural Documents is a critical document to comply with the standards. She confirmed that it will ensure a consistent approach from document inception through to implementation and monitoring of the compliance stage. The Company Secretary informed Members that the development and implementation of the policy is a strategic priority and has been included in the integrated improvement action plan – Quality Governance Framework, Historical Due Diligence and Board Development and Foundation Trust status actions. The Company Secretary confirmed that the Quality Governance Committee has approved the policy and recommended it to the Trust Board for ratification.
Members of the Trust Board ratified the Policy for the Development and Implementation of Procedural Documents for immediate implementation.
Page 21 of 30
2012.302
Strategic Objectives/Annual Plan Quarterly Report The Deputy Chief Executive Officer gave an update to the Board on the performance and assurance of delivery against the organisational objectives for 2012/2013. The Deputy Chief Executive Officer referred to the number of actions that the Trust identified to be achieved in 2012/13. Members noted that following a review of quarter 3, a number of actions had been identified as requiring further input. He referred to these actions and the estimated completion date. The Deputy Chief Executive Officer reported that the Trust-wide implementation of case management was behind schedule and at high risk of non-delivery. He explained that this was due to an adjustment of timescale as commissioners have now agreed to a two year project. The Chief Executive Officer confirmed that a revised approach to setting organisational objectives for 2013/14 was being monitored and reported through the Integrated Performance report. The Chairman asked if a Board Away Day has been scheduled to discuss the next cycle of Strategic Goals. The Deputy Chief Executive Officer informed the Chairman that one will be arranged. The Director of Workforce & Development confirmed that all staff appraisals were aligned to the Strategic Goals of the Board. Non Executive Director Designate, Andrew Talbot, asked for the Executive Directors to be mindful of the number of objectives set so as to allow colleagues the time to fully understand what is required and how it relates to organisational objectives. The Medical Director confirmed that the Trust will be utilising the NHS Trust Development Authority community trust dashboard which will explain any variations in the data collected to support Strategic Goal 1. The Deputy Chief Executive Officer referred Members to the work undertaken by Ernst & Young that had reported a wide variation in activity across certain specialties. This work had been presented as part of the “evidence pack” in support of the Trust’s Historical Due Diligence 1 and we will receive confirmation of the validity of the data at the conclusion of that process. The Director of Nursing & Quality noted that she had not sight of the fully worked up Cost Improvement Programme plans for the next two years and she asked the Deputy Chief Executive Officer as to whether this was a concern. The Deputy Chief Executive Officer confirmed that the Trust Board had sight of the outline of the plans at the Trust Board Away Day held in December 2012. Vice Chair and Non Executive Director, Jennifer Ledgar, asked the Deputy Chief Executive Officer, for assurance that all Strategic Goals would be achieved by the end of the financial year. The Deputy Chief Executive confirmed that action plans were being implemented to secure the targeted completion of the outstanding Strategic Goals.
Members of the Trust Board noted progress to date and received assurance of the delivery of outstanding actions.
GG
Page 22 of 30
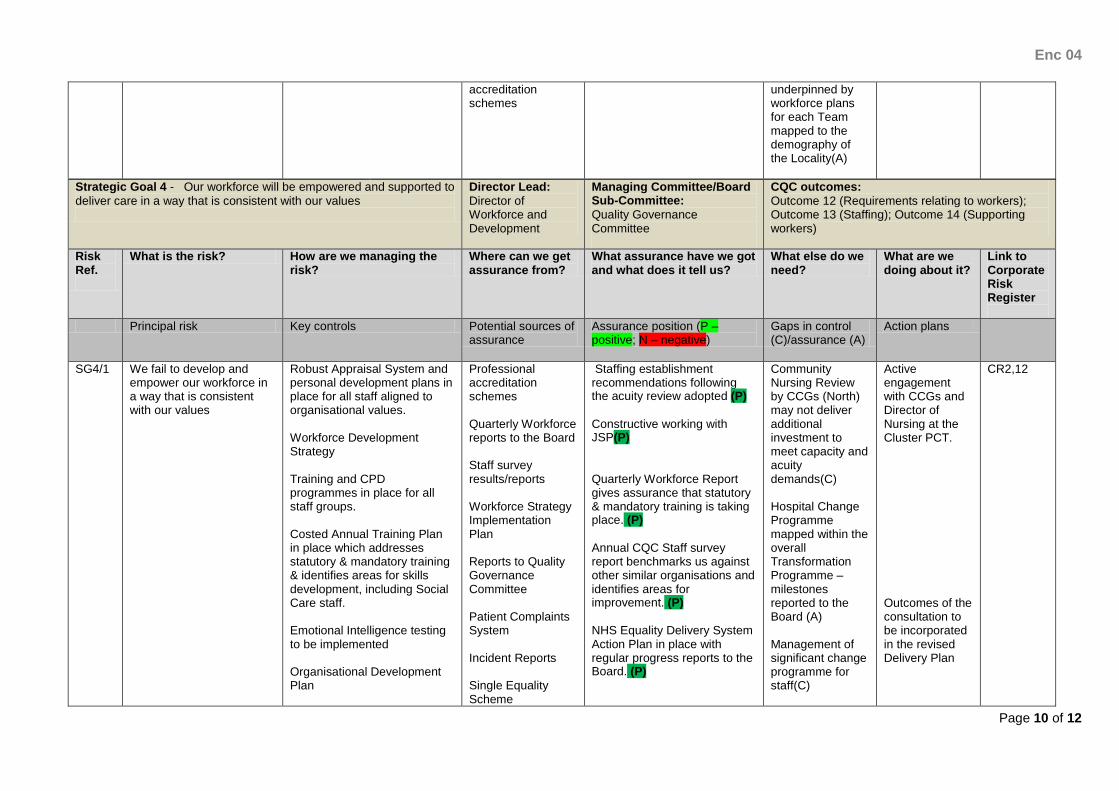
2012.303
Workforce Strategy The Director of Workforce & Development presented the Workforce Strategy. Members acknowledged that the Strategy had been presented to the Trust Board and approved in February 2012. The Director of Workforce & Development informed Members that she was seeking approval from the Trust Board to implement the final version. She gave assurance that the Strategy has been widely circulated and consulted upon, and had been reviewed at the Transformation Programme Board meeting. The Director of Workforce & Development reported that KPMG and the Strategic Health Authority have reviewed an earlier draft of the Strategy and had identified key areas, which had been identified as requiring development. These were being addressed. Members acknowledged that the way forward around recruitment was that we must not recruit ‘like for like’, noting that the Transformation Programme required a change in how people worked and a reduction in the workforce. The Director of Workforce & Strategy confirmed that the Strategy supported the development of the skills of the Workforce and that the launch of the Academy was a signal of the intent of the Trust that it would be actively supporting and investing in the development of Health and Care Support Workers. The Director of Workforce & Development noted that a high proportion of the Trust’s qualified workforce is ageing and she gave assurance to the Board that this was being addressed by looking to recruit apprentices and offer work experience. She explained that the Transformation Team had started mapping exercises to look at how the workforce, within the 28 integrated locality teams, would be mapped to the prevailing health and social care needs, and demography, of the population within the locality. This would mean that the Trust was actively matching the skills of its workforce to the needs of its population. Members noted that the key to success was in engagement with staff and for staff to recognise the opportunities that the Strategy presented to them in changing how they worked. Members noted the positive feedback following discussions with Staff who had been encouraged to come up with ideas and that Trade Unions were fully engaged and supported the Strategy. The Director of Workforce & Development explained that once Trust Board approval is given, it would be necessary to appraise line managers of its content and to gain a better understanding of how they would be expected to deliver the Strategy. The Chairman commented upon the good quality of the report and he addressed Members of the Board asking if there were any questions. Chris Beswick, Staffside Representative agreed that there were benefits from having work experience and employing Students. The Chairman asked Chris Beswick if the workforce were aware of the Strategy and Mr Beswick responded by confirming that this had been put to the test this year and staff recognised that this Strategy and the Transformation Programme was opening up opportunities previously not available, particularly in developing their skills. The Chairman stated we must be mindful that there would be extra demands on
Page 23 of 30
staff and as such workload would increase and there needed to be a realisation that extra pay would not be forthcoming in the current difficult financial climate. The Director of Workforce & Development asked Mr Beswick as to whether Staff had considered this and he responded by stating there were mixed feelings, with some staff not minding, going the extra mile, whilst some staff were showing resistance and required guidance as to why changes were being implemented. Non-Executive Director David Pearson, stated that the key was to ensure that the clinical strategy locally is aligned with the Workforce Strategy and the Estates Strategy and Transformation Programme, with ownership at a Team level. The Deputy Chief Executive Officer confirmed that the locality mapping of the 28 Integrated Locality Teams would achieve this. Non Executive Director, David Pearson, noted that negotiations were currently taking place with commissioners and all agreed that communication was key to help forge good relationships, which would be helped by this strategy.
Members of the Trust Board approved the Workforce Strategy.
2012.304 Information Management &Technology (IM&T) Strategy The Director of Finance & Resources presented the IM&T Strategy which supersedes the previously approved Information Services Strategy 2012-2015. The Director of Finance & Resources explained that the refreshed Strategy had been developed over the last two months following an internal review of: IM&T and Information Governance services and systems across the Trust; National IM&T strategies; and Local Health Economy IM&T strategies. The Director of Finance & Resources informed Members that the Strategy has been reviewed by Non Executive Director Designate, Andrew Talbot, and externally by RSM Tenon. The Director of Finance & Resources confirmed that the Strategy details a number of programmes to support a number of the Trust’s Strategic Goals. The Director of Finance & Resources referred Members to the key points of the Strategy, noting that the 10 IM&T Vision Goals were aligned to the Strategic Goals of the Trust. The Director of Finance & Resources outlined the work programmes that underpinned the Strategy, with the intent being that the Strategy would deliver an integrated IM&T infrastructure supported by a single corporate I.T. infrastructure. The Director of Finance & Resources referred Members to the proposed development of a Primary Clinical System and specialist clinical systems linked together by an Integration Service so that the front end user use a single front end system. The Director of Finance & Resources referred Members to the high level investment plan and the requirement to secure £18m capital funding to deliver the Strategy, noting that for each project a fully costed business case would be developed for approval by the Finance, Investment & Performance Committee and/or the Trust Board. He noted that the revenue costs of the capital schemes have been factored into the Long Term Financial Model. Vice Chair and Non Executive Director, Jennifer Ledgar, asked if the core system would be ‘off the shelf,’ rather than bespoke and the Director of Finance & Resources confirmed that it would not be a bespoke package. The Director of Finance & Resources gave assurance to Members that the Strategy
Page 24 of 30
would improve communication, through the delivery of a range of flexible communication technology and that there were robust information governance arrangements that would ensure that the Trust’s information governance obligations would be met. He informed Members that there is on-going delivery of a number of enabling projects, including I.T. service continuity management, training, finance and procurement. The Chairman confirmed that the Strategy is a comprehensive document and he spoke about the reality staff would face and he noted that that there would be significant training required for staff. The Chairman asked Members to note that this would involve forty projects and he commented upon the scale, time frame and additional stresses to staff. The Chairman referred to the report asking whether staff that were visually impaired or deaf had been consulted with, so as to ensure that all staff would be able to use these new services. The Director of Finance & Resources assured the Board that a wide consultation process had taken place. Non Executive Director Designate, Dr John Scarpello, asked if the proposed Primary Clinical System would be a community clinical system and he suggested that there would be benefits if there were discussions with a Professor John Williams who is looking at community clinical systems. The Chief Executive Officer referred to systems that were already in use within the Community and reiterated to the Board that the Trust was committed to Care Director, noting that it was fundamental that this Strategy delivers a “front end integrated system” which is user friendly, improves data quality and productivity, and demonstrates real improvements in care. Non Executive Director Designate, Andrew Talbot, agreed and confirmed the need for a single data warehouse infrastructure. The Chairman commented upon the scale of the project, in particular the need to implement a full IM&T Department and he queried costs relating to in-house training and the funding support required for an IT helpline service. The Director of Finance & Resources referred Members to page 15 of the Strategy which outlined the scope and scale of the numbers of staff transferring to the Trust and the resources needed to deliver the Strategy and to manage contracts with current and existing providers. Non Executive Director, Prof Roger Evans, welcomed the Strategy and thanked the Director of Finance & Resources for his presentation.
Members of the Trust Board approved the IM&T Strategy and the investment plan detailed in the Strategy.
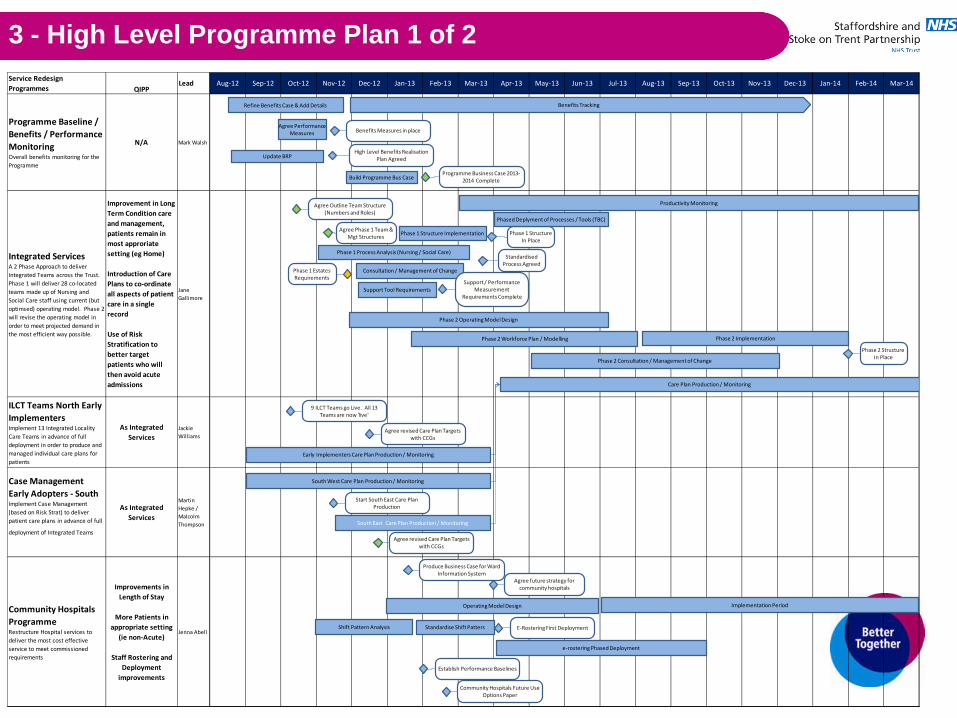
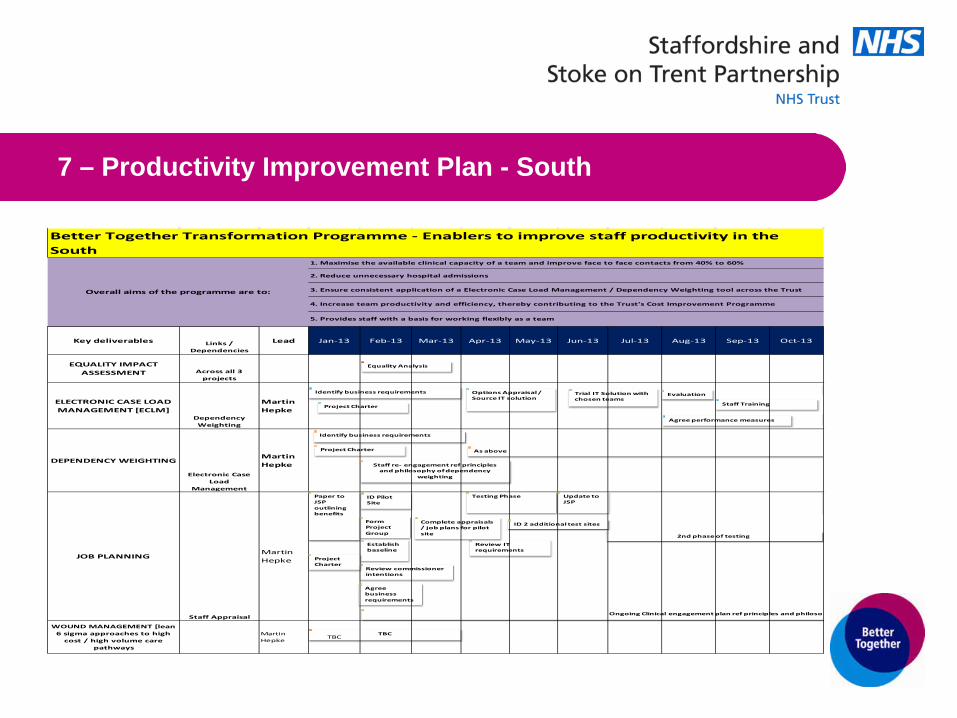
2012.305 Transformation Programme Management Office Report The Deputy Chief Executive Officer referred to the Programme Management Office (PMO) Better Together Transformation Programme. Members noted that this had been produced to provide the Board with an overview of activity and progress for the previous month, along with current timescales, key issues and focus areas. Members were informed that a programme dashboard was included to outline the key component projects and their current delivery status (RAG rated) together with a brief commentary. All noted that there was a draft high level Transformation
Page 25 of 30
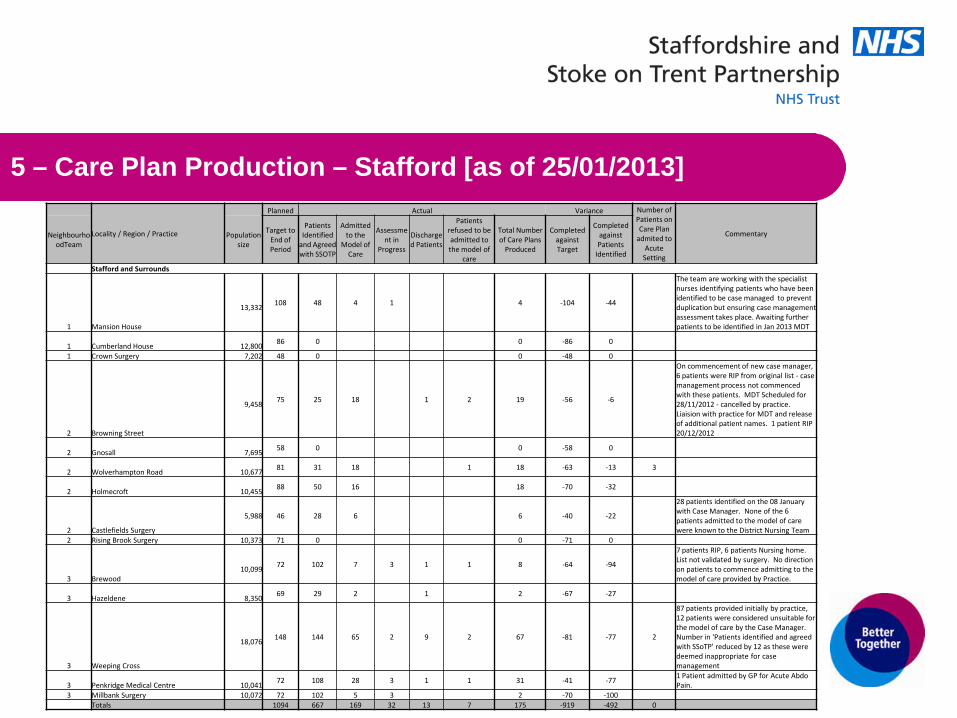
Programme Plan included within the report, to provide the Board with the timelines for projects, contributing to the overall Programme to implement the Model of Care and progress against the care plan targets. The Deputy Chief Executive Officer highlighted the key points around the Transformation Programme Directors update and noted that the Programme was now moving into its delivery phase, in consequence of which the PMO will be streamlined and the completed work streams will be transferred to Implementation Managers. It was established that Phase 1 was now largely complete but that delays in production of the organisational structures had put the 1st April 2013 “go live” date at risk of being missed. Members were informed that at the end of January 2013 Community Hospitals continue to deliver operational improvements and that the average length of stay continues to show significant improvement. All noted that the remote working pilot was experiencing technical difficulties with the digital pen and satellite navigation solutions, but Members noted that these were being investigated with suppliers. It was established that analysis had identified that the number of daily visits to base were not as high as first thought, but any loss of benefit in this area would be off-set by the current inefficiencies in the referral and allocation process that would be removed by a simple technical solution, presently being progressed. The Deputy Chief Executive Officer summarised that there was now a Business Case, which had been developed to ‘operationalise’ standard documentation and he confirmed that this, along with the draft Assistive Technology Strategy, had been circulated and is currently under review. The Deputy Chief Executive Officer outlined the actions planned for the forthcoming month in relation to the planning and risk analysis for the Community Hospitals Programme; agreeing the Transformation structures and the approach for 2013/14; continuing the remote working project and standard assessment pilots; and the need to begin to manage the change process for Integrated Teams and he concluded by confirming that there were permanent PMO staff now in post. Non Executive Director, David Pearson, asked for Members to consider (page 4) - remote working and he asked the Deputy Chief Executive Officer if the Penkridge Case Load Management had been considered. He shared staff feedback with Members about their frustrations when having to travel back to the office to complete documentation. The Deputy Chief Executive Officer assured him that a Business Analyst was at present obtaining data and Staff Side were involved. The Director of Workforce and Development queried whether the Analyst was looking at the payroll system, which would help identify how we implement this into mainstream. The Deputy Chief Executive confirmed that all data received would be reported back to the Board. The Chairman addressed the Non-Executive Directors asking them to focus on communication with staff and to be assured of the governance of the Transformation programme as evidenced by the action tracker within the PMO report.
Page 26 of 30
The Chairman thanked the Deputy Chief Executive for this very informative report, which he commented had been very helpful.
Members of the Trust Board: • Noted the contents of the report and the PMO actions for February 2013; • Noted the Care Plan Targets and the latest high level plan.
2012.306 NHS Constitution The Deputy Chief Executive Officer referred to the update made to appraise the Board on revisions made to the draft Foundation Trust Constitution and the additional engagement with staff and the Joint Staff Partnership, in relation to the division of the Staff Constituency into Staff Classes. Members noted that the Foundation Trust Project Board had approved the change to an “opt out” automatic membership (by default) of the Staff Membership, with support from the Joint Staff Partnership and the proposal to incorporate Staff Classes within the Staff Membership, rather than a single Staff Constituency. The Deputy Chief Executive Officer sought the Board’s approval to the final draft of the Foundation Trust Constitution in the form appended to this Report, prior to its submission to the NHS Midlands & East Strategic Health Authority. The Deputy Chief Executive explained to the Board that highlighted areas within the report were a set of proposals discussed since the first submission to the Board in November 2012, noting that the Trust Board are now recommended to:
• approve the change from a single Staff Constituency to one that comprises five Staff Classes as set out in the Constitution (Annex 2);
• endorse the recommendation of the Foundation Trust Project Board, to approve automatic membership of the staff membership by default, as set out in the Constitution; and
• to note the approval of the Joint Staff Partnership to automatic membership by default and to approve the final draft of the Constitution in the form appended to this report.
The Deputy Chief Executive Officer noted that the Trust Board had agreed (at its November meeting) to:
• increase the number of Elected Patient Governors from four to five;
• to increase the number of appointed governors representing the Voluntary Sector from one to two;
• to reduce the age of the membership from sixteen, to fourteen years of age; and
• to agree the name of the Foundation Trust as the “Staffordshire and Stoke-on-Trent Partnership NHS Foundation Trust”.
Members were assured that substantive discussions had taken place at the Foundation Trust Working Group of Executive and Non Executive Directors (which had been established at the recommendation of the Trust Board at its meeting in November 2012), and with the Staffside in relation to: the Staff Membership and Staff Governors; and the proposed changes to the Constitution as highlighted within the draft Constitution appended to the report. Members noted that next steps were to develop a programme for the election and
Page 27 of 30
induction of a Shadow Council of Governors and to make links with the new Health and the Well Being Board. The Deputy Chief Executive Officer explained this was particularly important as the Trust needed to demonstrate that its membership and the Council of Governors is truly representative of the communities that it serves. He commented upon the implementation of the Membership Strategy, which will provide significant improvement for patient and public involvement within the Trust’s core business. Members were asked to note the final draft of the Constitution with the changes agreed by the Foundation Trust Working Group and the Joint Staff Partnership and to approve the final version of the Constitution prior to submission to the SHA. Non Executive Director, Prof Roger Evans, noted that 450 members of staff have already signed up and the Chairman referred to page 94 (Item 3.2) and he queried as to what constitutes a dispute in relation to the ‘eligibility of membership’. The Company Secretary explained the principles that underpinned the disputes resolution mechanism set out in the Constitution and noted that the discussions Joint Staff Partnership were supportive of a move from a single Staff Constituency to one that comprises of 5 staff classes, particularly as this would enable social workers and care support staff to be represented as Staff Governors within the Council of Governors. The Chairman reiterated that there had also been a robust discussion at November 2012 Trust Board and he addressed both the Deputy Chief Executive Officer and the Company Secretary as to whether there were any further developments, or could the Board be assured that we were where we needed to be as a Trust, at this moment in time. Members were assured that there were no further developments planned and the Chairman asked Members if all agreed with the proposed recommendations and the draft of the Constitution (in the form appended to the report).
Members of the Trust Board: • Approved the change from a single Staff Constituency to one that
comprises five Staff Classes as set out in Annex 2 of the Constitution; • Endorsed the recommendation of the Foundation Trust Project Board to
approve automatic membership of the staff membership by default as set out in the Constitution;
• Noted the approval of the Joint Staff Partnership to automatic membership by default;
• Noted the changes to the Constitution, as approved by the Foundation Trust Working Group, that strengthen the governance of the Council of Governors; and
• Approved the final draft of the Constitution in the form appended to the report.
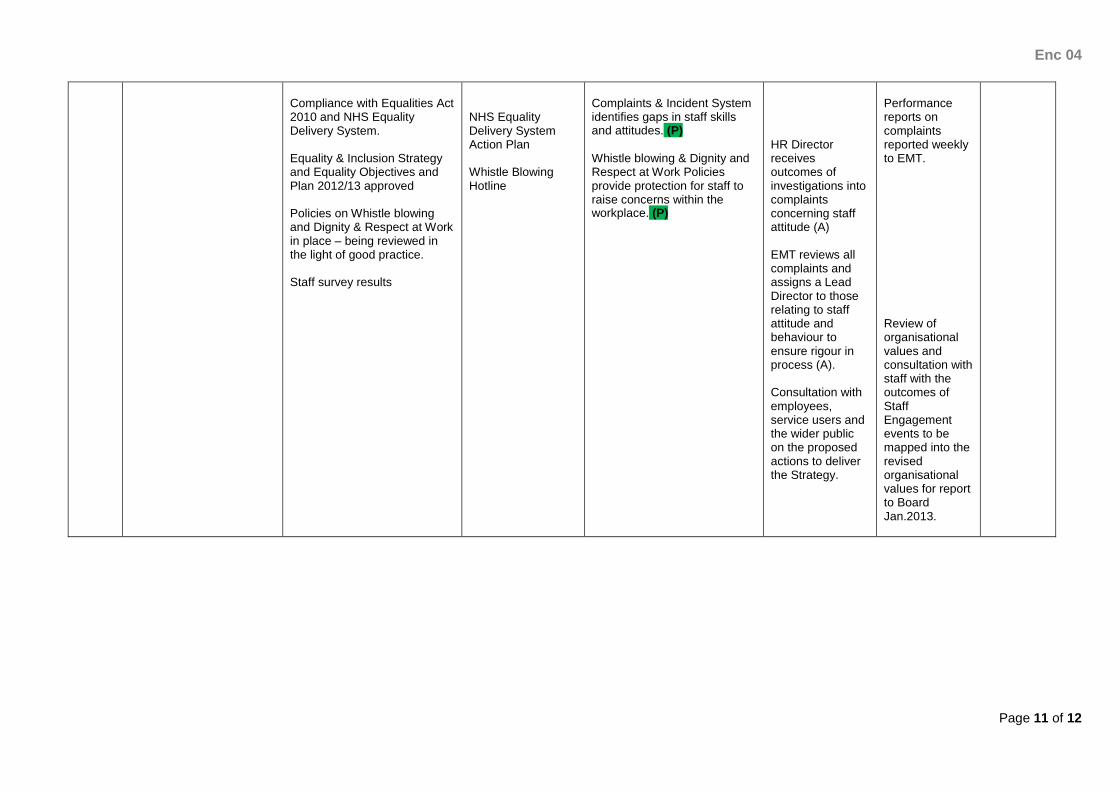
2012.307 Workforce Policies Members of the Trust Board were asked to formally note the Workforce polices submitted by the Director of Workforce & Development, as follows: Recruitment and Selection; Stress Management; Dignity & Respect at Work; Induction; Appraisal; and Work Experience. The Director of Workforce & Development explained that a working group has been established to look at good practice and to positively involve the Staffside forum in workforce matters. The Chairman asked Members if there were any specific questions.
Page 28 of 30
The Chairman confirmed to the Director of Workforce & Development that he never wants to compromise on quality when appointing staff and that staff must have the defined core skills, as a minimum. The Director of Workforce & Development gave assurance that emotional intelligence testing is now being used and that the organisational values are embedded in the recruitment process to ensure that staff are recruited with the right values and attitude. The Chairman welcomed the fact that the Trust has signed up to the ‘Mindful Employer’ charter as this would reduce the stigma that staff felt in reporting stress and depression.
Members of the Trust Board approved the suite of policies referred to in the report.
2012.308 Organisational Values - Distilling and Embedding The Director of Operations explained the purpose to the report, which was to inform Members about the results of staff feedback on reducing the seven values to three more succinct values, and to outline the plan for embedding the values throughout the organisation. The Director of Operations focused upon the three core phrases that simplified the seven values and she gave assurance that these had been discussed and reviewed extensively, through focus groups and staff events, with the final wording having being agreed by the Executive Management Team. She outlined that the Values and Behaviours had been distilled down to become:
• We put Quality first; • We focus on People; • We take responsibility.
Members noted that the approach to the development had focused on considering examples of behaviours, ‘what you will see,’ and ‘what you won’t see,’ by staff and service users. The Board noted that a draft booklet had been designed by the Communication Team. The Director of Operations noted that any additional costs in relation to organisational values training and embedding the new values across the Trust would need to be agreed. The Director of Operations confirmed that Service Users had been involved in the consultation and she explained that their views and ideas had influenced the final proposed 3 core values. Members were informed that good practice had been sought as utilised in other areas e.g. some Trusts had a focused Leadership Forum that had distilled down their values to 3 statements, (identified on page 5) of the report. Members were given assurance that consideration had been given to quality and that people were asked to take responsibility and encouraged to engage, resulting in good feedback from staff. Members noted that 400 staff had taken part within numerous engagement events and noted the importance of embedding these values. Members noted that Social Care colleagues would be equally involved in creating the behavioural framework that underpins the values. Members were informed by the Director of Operations that a detailed behaviour and attitudes framework was to be developed following the approach taken at Guy’s and St Thomas’ and learning taken from this would ensure a greater level of
Page 29 of 30
engagement and sustainability. Members agreed that this detailed framework would be required to help embed the values, particularly at Appraisal and to assist recruitment. Members were made aware that there had been some complaints from staff who had fed back feeling neither engaged and experience had been drawn from this on how these situations could be avoided in future. Moving forward the Board noted that plans had been implemented to utilise team meetings, with good links into the quality team and improved governance, to ensure that a systematic process is being discussed through all teams. The Director of Operations stated staff needed the chance to feel valued, with improved work satisfaction, where Staff had a clarity to their roles, which was linked into their appraisals and personal objectives. The Chairman commented upon the need to have good communication, particularly during appraisal and that staff need to be fully aware and understand what behaviours are expected by all staff, if employed to work for the Trust. Non Executive Director Designate, Andrew Talbot, asked for examples of how the values would make a difference to be included in the roll out of the new values to staff and service users. Vice Chair and Non Executive Director, Jennifer Ledgar, asked that evidence of the changes made as a result of these new values should be visible within the Trust and the Chief Executive Officer encouraged Members of the Board to spend more time out with staff, to both learn from their experiences and to support the roll out of these values.
Members of the Trust Board: • Agreed the final iteration of the distilled values into three core phrases; • Agreed for the generic behaviours and attitudes to be included in a
booklet; • Agreed to the costs involved to produce a booklet and further materials to
support embedding; • Agreed the outline action plan for embedding the values; • Agreed the approach to evaluation.
2012.309 Any Other Business The Chairman asked the members of the public if there were any further questions and Mrs Elizabeth Jarrett, Development Worker from Staffordshire LINk, confirmed that she had three questions that she would like to ask Members of the Trust Board. Mrs Jarrett referred to the performance report, where she stated she had picked up anecdotal feedback about delays in social care assessment. She asked if Staffordshire LINk could have a copy of any action plan in order to both reassure users of what is happening and also, in case LINk seeks feedback, so that they are clear about what users/carers should expect of the service. The Director of Finance and Resources confirmed that he would action this request. Mrs Jarrett made reference to the performance report (Enc 08, annex 2 – 1st objective) where she remarked that the indicators do not appear to measure the strategic objective. Mrs Jarrett suggested that a more relevant indicator would be to measure service integration and look at assessments covering both health and social care needs, or the setting up of joint packages of care.
JT
Page 30 of 30
Members considered Mrs Jarrett’s point, agreeing this was a well-made suggestion. Members acknowledged that the indicators are those which the Trust has to report on and have been allocated to strategic objectives, rather than designed around the objective. Members responded by stating that the intention is to move towards more outcome based indicators, which will better measure the implementation of the strategic objectives. Mrs Jarrett explained that she was a member of the user/carer forum, which has now commented upon two drafts of a policy for reimbursement of expenses, relating to engagement. Members were informed that patient representatives have been unhappy with the mileage rates proposed and have been advised that this has to be dealt with by the Trust Board. Mrs Jarrett did point out that the policy has not been presented to the Trust Board today. The Chief Executive Officer stated that the policy did not need Trust Board approval and he agreed to ensure that it was dealt with. The Director of Nursing and Quality reassured Mrs Jarrett that in the meantime payments to volunteers have been authorised. The Chairman thanked Mrs Jarrett for raising such valid questions, stating that they would be noted and acted upon. The Chairman asked Members of the Trust Board if there were any further risks arising from the discussions today that had not been captured or discussed earlier in the meeting. The Chief Executive Officer referred to the need to recruit the right calibre of staff to deliver the changes that had been discussed during the meeting in relation to: the development of Integrated Locality Teams; the need to improve productivity; and the need to demonstrate a better patient and service experience, with improved outcomes in relation to their care and support. He asked the Director of Nursing and Quality if consideration had been given to have a campaign that encourages working within the NHS as a career choice. The Director of Nursing and Quality gave assurance that University undergraduate students were being approached to look at rotating staff, with integrated teams that would help encourage engagement. The Chief Executive Officer stated he would take this back to the Risk Committee for information. The Chairman thanked Members for their attendance and closed the meeting.
SP
SP
2013.310 Date of next meeting Wednesday 27 February 2013 at The Coton Centre in Tamworth.
Enc 02
Page 1 of 8
REPORT TO STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST
TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 02
Subject: Chief Executive Officer Report
Project Lead: Stuart Poynor
Recommendation: For Approval For Discussion For Information x
PURPOSE OF THE REPORT To provide members of the Trust Board with an update from the Chief Executive Officer. KEY POINTS NATIONAL • Mid Staffordshire NHS Foundation Trust public inquiry report • Changes to quality accounts reporting arrangements for 2012/13 • Whistle blowing: bridging the gap • Consultation on future NICE social care quality standards • NHS Change Day 13 March 2013 • Landmark reform to help people with care and support costs • Alzheimer’s Society launches Dementia Friends information sessions • NHS Friends and Family Test: publication guidance • Local authorities – health and wellbeing boards and health scrutiny regulations • Adults' personal social services: revenue and capital grants final allocations REGIONAL/CLUSTER WIDE • Catalyst for Change • Ministerial Visit to HMP Stafford • Sexual Health Services – Shropshire and Telford & Wrekin LOCAL • Foundation Trust update • Strategic Health Authority Quality Visit • Historical Due Diligence 2 • Board Governance Assurance Framework • Visits to frontline services • Cross Economy Leaders Group Briefing
RECOMMENDATIONS / ACTION REQUIRED Members of the Staffordshire and Stoke on Trent Partnership NHS Trust Board are asked to note the contents of the Chief Executive Officer Report.
Enc 02
Page 2 of 8
Enc 02
Page 3 of 8
CHIEF EXECUTIVE OFFICER REPORT NATIONAL Mid Staffordshire NHS Foundation Trust public inquiry report The Mid Staffordshire NHS Foundation Trust Public Inquiry final report was delivered to the Secretary of State for Health by Robert Francis QC on Tuesday 5 February 2013. The report was published on Wednesday 6 February 2013 and laid before Parliament on the same day. The report details significant recommendations for the NHS to implementwhich will improve the way in which services are delivered. Since the Partnership Trust established we have made the quality of care our top priority and have established a set of values which support the delivery of care with dignity and respect. The Partnership Trust will embrace the recommendations within the report and use them to further improve the care that we deliver. We recognise that we must acknowledge mistakes at the earliest opportunity so that we can take remedial action to reduce any potential harm to patients and service users and that provide the right support for our support. The Director of Nursing & Quality has made a direct pledge to all staff that we will listen to them and if anyone is aware of poor care being delivered they can contact any of the Trust’s Professional Leads, Nursing & Quality colleagues, the whistle blowing service, or a director or directly to myself as Chief Executive Officer. The Secretary of State for Health and NHS Chief Executive published letters to Trust Chairs and Chief Executive Officers asking for staff listening events to be held. The aim of the events is to engage, support, involve and listen to staff to enable them to provide more compassionate care to patients and service users. We must care for staff to care for patients and service users and listen to what patients and family members are saying to us. The report includes 290 recommendations and following an assessment of these early indications would suggest that around 100 are directly relevant to the Partnership Trust. The Executive Management Team is working on a plan to schedule a series of listening events for staff, the creation of a themed list summarising the recommendations and how the Trust Board operates as part of the Trust’s overall response to the recommendations. A proposed methodology for staff listening events has been discussed by the Executive Management Team that will include teams discussing the main issues raised within the report in their own teams and capturing key actions to improve dignity and quality of care and safety; a number of focus groups with a bottom-up approach allocated for a member of the Trust Board to hear at first-hand what staff say; engagement with patients and carers; and a questionnaire or an open request for emails. In each of these approaches and others that the Trust may adopt, the key message to staff will be that their open and honest assessment is being sought and will be acted upon. A clear action plan will be communicated back to staff and actionned. Click here to access the report from the Inquiry website.
Changes to quality accounts reporting arrangements for 2012/13 This joint Department of Health, Monitor, and NHS Trust Development Authority letter sets out important amendments that have been made to the National Health Service (Quality Accounts) Regulations 2010. These amendments come into effect from February 2013 and change the reporting requirements for quality accounts being published in June this year. Click here to read more. Whistle blowing: bridging the gap Many people know about whistle blowing procedures but some do not feel safe using them. Bridging the Gap is a campaign launched by the Government-funded whistle blowing helpline to encourage a culture where all individuals feel safe to raise concerns and where managers are equipped to respond. Free posters and fliers are available on the web link. Click here for further information. Consultation on future NICE social care quality standards The Minister for Care Services, Norman Lamb, has launched a consultation seeking views on an initial proposed list of social care quality standard topics and ideas for new topics. The aim is to establish a full set of NICE quality standards and guidance to improve the quality of social care. Click here for further information. NHS Change Day 13 March 2013 This is one day of individual creativity by NHS staff and their supporters, pledging to do one simple thing to change the way they work and the care they give. It is a grassroots initiative devised and led by the next generation of young and emergent clinical and managerial leaders from primary and secondary care across the NHS. Click here for more information. Landmark reform to help people with care and support costs Jeremy Hunt, Secretary of State for Health, has announced a series of reforms that will provide greater financial support for the elderly, those with disabilities and long-term conditions in paying for their care costs. Local authority chief executives and Directors of Adult Social Services will wish to review the details of these reforms, and discuss with their relevant teams. Click here for more information. Alzheimer’s Society launches Dementia Friends information sessions From this week, people across England will be able to sign up for sessions to become a Dementia Friend. Just over 12,000 people have already registered their interest. Now those people and many more will be able to attend information sessions to find out more about what it’s like to live with dementia and then turn that understanding into action in their local community. Click here for more information. NHS Friends and Family Test: publication guidance The Department has published guidance for providers of NHS funded services on calculating and publishing the NHS Friends and Family Test results. Click here for more information. Local authorities – health and wellbeing boards and health scrutiny regulations The Local Authority (public health, health and wellbeing boards and health scrutiny) Regulations 2013 have now been published. These regulations are intended to help local authorities finalise preparations for health and wellbeing boards and health scrutiny arrangements. Click here for more information.
Adults' personal social services: revenue and capital grants final allocations The Department has published final revenue and capital grants for the period 2013-14 and provisional allocations for 2014-15. The grants will be allocated to local authorities in England. The letter outlines final 2013-14 allocations for each local authority. Click here for more information. REGIONAL/CLUSTER WIDE Catalyst for Change This month I was invited to talk about how positive staff engagement can have an impact on the delivery of front line care at a Customer Service Alliance regional conference ‘Catalyst for Change’ organised by NHS Midlands and East. Delegates heard from two inspirational keynote speakers from Richmond Housing Partnership and Waitrose who had some interesting ideas that we can consider as a Trust. Ministerial Visit to HMP Stafford I joined the Healthcare Team based at HMP Stafford for a visit by Health Minister, Anna Soubrey and the Director of Nursing at the Department of Health, Professor Viv Bennett, who learnt more about the service delivered and of the Trust’s ‘Nurse of the Year’, Johanne Tomlinson. Sexual Health Services – Shropshire and Telford & Wrekin The Trust has successfully bid for the provision of sexual health services in Shropshire and Telford & Wrekin. The service is based on the model which we are currently operating across Staffordshire and will operate as part of our South Division services. LOCAL Foundation Trust Update The Partnership Trust’s overall timetable for its Foundation Trust (FT) application has been amended from 1 April 2013 to 1 June 2013. This is because the NHS Trust Development Authority (which will assume responsibility for the FT pipeline from 1 April 2013) has asked that all Trusts currently within the authorisation process, or shortly to enter it, to have additional time to consider their individual responses to the Mid Staffordshire NHS FT public inquiry report. We are disappointed with the delay but clearly recognise the importance of the Inquiry report and our need to reflect on this as an organisation. We were very aware of the lessons from the first Inquiry when the Partnership Trust was established almost eighteen months ago and the Trust was created as a listening organisation, with a commitment to quality and putting professionals at the heart of everything we do. Strategic Health Authority Quality Visit A Quality Visit led by the Strategic Health Authority (SHA) was held on 12 February 2013. The SHA’s Associate Nurse Director and Associate Medical Director led the visit (which included a team of 17 SHA colleagues) and commented that they were all made to feel very welcome by our staff who were exceptionally helpful to the review team. The SHA team identified no immediate patient safety risks and saw many areas of good practice that will be expanded on in their full report which will also include a number of recommendations for us to action.
I would like to thank the patients, partner organisations, members of staff and Staffside representatives for contributing to the following focus groups held on the day: • Social Care • Prison Health • Senior Nurses/Matrons/Allied Health Professions • Advanced Nurse Practitioners • Consultants and Clinical Leads • Junior Nurses/Allied Health Professionals • Patient and Carers • StaffSide • Risk and Governance Managers • Pharmacy Lead Team Historical Due Diligence 2 The Historical Due Diligence 2 review, undertaken by PricewaterhouseCoopers (PwC) will be completed by 25 February 2013 and shared with Members of the Trust Board and the SHA. We have received initial feedback from PwC following some of the interviews that have taken place with Members of the Trust board that indicates that the Trust is progression well in relation to the recommendations PwC issued to the Trust in September 2012 as part of the Historical Due Diligence 1. Board Governance Assurance Framework The independent Board Governance Assurance Framework report produced by Chantrey Vellacott was a positive report which identified that the Trust Board has the ‘capability and capacity’ to progress the Trust’s strategy. Chantrey Vellacott commented that the Partnership Trust is making good progress towards achievement of the governance requirements of the FT authorisation process. Visits to frontline services Following last month’s Trust Board meeting I visited staff, patients and their families and carers on the Sycamore and Bennion Wards at Bradwell Hospital. I spent the evening talking with and listening to the views of family members and carers about the care provided; and spent time with patients who were complimentary about the care they received. Visiting hospital wards gives me an opportunity to hear from staff about the pressures that they face and to listen to suggestions about how the system can work more effectively. I was able to take some of the feedback from my visit to the executive management team for action to be taken and feed back to the staff, patients and family members. This month I have met with the District Nursing team in Uttoxeter and went out to meet three patients who are receiving care from the team, including one patient who resides in a residential home. During one of the visits I saw at first hand the challenges and difficulties being a full time carer can bring and I discussed with one family member how the Trust can provide support to carers who need respite or other support in the future. The District Nursing team shared with me their experiences of work across the local health economy and how we can work together to develop the right culture across the organisation. Whilst in Uttoxeter, I talked to the Health Visiting team, including a Nursery Nurse and Student Health Visitor.
Enc 02
Page 7 of 8
I had the opportunity to meet with a Diabetes Nurse Consultant in Burton to discuss the specialist work of the service in the East Staffordshire area. I was particularly impressed and interested to hear about the work of the service that has been recognised both national and internationally; and discussed how we might bring staff together across the Trust to share best practice. I met with the Social Care team in Burton and saw the support given to ensure the safe discharge of patients from the acute hospital and discussed ideas for schemes and proposals that they feel could have a positive effect in getting more people back to their home environment. Furthermore, we had a useful and open discussion about their concerns regarding the level of bureaucracy and some of the challenges that the team faces. Cross Economy Leaders Group (CELG) Meeting Briefing – January 2013 Matters under discussion in the meeting 1. Briefing on findings of the Community Team Plus locality work in Stoke-on-
Trent
The first part of the January CELG was a broader meeting to receive the findings of the first ‘check’ phase of the Community Team Plus (CT+) initiative in Stoke-on-Trent. CT+ is a health economy-wide drive to support the development of integrated working in the city. CT+ builds upon the existing work on Integrated Locality Care Teams and develops new ways of working to improve outcomes for people who are at risk of preventable deterioration, hospitalisation or residential care admission. It is intended that CT+ will develop the integrated teams to form one local public-facing offer, including NHS, social care, housing, emergency services, community safety and voluntary sector contributors. For this ‘check’ phase, a core multidisciplinary team worked to understand some of the ‘journeys’ people who use services make, and the cost of these journeys. Through this initial analysis, it was established that often services were not ‘joined up’ or complementary, and that sometimes people who used them were confused by the complexity and repetitiveness of the services they experienced. As the services were uncoordinated and episodic, the outcomes were often not as positive for the individual as they could have been. The focus of the ‘check’ phase was on adults with health and social care needs identified at access points across the system, including the Adult Social Care Contact Centre, the NHS Single Point of Care, UHNS referrals to the Complex Assessment Service, and the Willowbank and Belgrave GP practices. The findings reinforced recent evidence for the local health economy, showing that people with complex needs (often with more than one long term physical or mental health condition, experiencing frailty and the issues of old age) were the people that would most benefit from an enhanced integrated service. As a product of this work, the CELG reiterated its commitment to whole economy approaches to make real improvements to the experience of people who use such services, and to further pursue the CT+ work into the next phase of implementation.
Enc 02
Page 8 of 8
2. Cross economy transformation - update on actions
CELG received an update on the post-summit cross-economy activity. The concluding intentions of the summit are being formed into actions upon which the next phase of cross-economy programmed activity is being based.
The key intentions of the summit are as follows. • To make sure that the right care is delivered at the right time in the right place by • addressing over-reliance on acute sector services, • transferring some of the service activity that is at present taking place within the acute
sector be provided within the community, and • focussing that activity on supporting people to remain living independently in their
homes for as long as safely possible. • To ensure that people are supported to acquire the knowledge and capability to take
best care of themselves, to make the most of their health and improve their wellbeing. • To join up the commissioning of services, by adopting methods to ensure that providers
work together to provide better coordinated services, regardless of whether they require an acute or community response.
• To ensure that the range of services that combine to form the local health economy will
be properly coordinated and work well together, providing best value for money, and delivering excellent outcomes for the people that use them, even under circumstances of high pressure.
The summit identified three ‘big ticket’ areas of work (System Coordination, Frail and Complex Approach, and Integrated Intermediate Care). These ‘big tickets’ show the key activity deemed most likely both to have an immediate beneficial effect on the performance of the local health economy, and to set the trajectory for a fuller set of transformational ambitions required to meet the challenges of upcoming years. CELG received an update on the initial draft programmes around these key areas, and discussed how equally important complementary work (such as Locality Working/CT+) will complement this activity. 3. Cross Economy Strategy for Finance and Capacity
In conjunction with the above transformational work, representatives from all of the organisations on the CELG are working together on a commissioner-led process to produce one financial overview of the activity of the local health economy for the next three years. Due to the unpredictable nature of future service demand, the net financial implications of the cross economy transformational plans are difficult to model. CELG agreed however that proper transformational activity will rely on the transfer of responsibility for people’s care from being by default within the acute setting to being pro-active and community-based. Community services will need to be prepared for the diminution of first-line reliance on acute beds, and be able to offer support in people’s localities and homes. This relocating of activity will entail significant shifts in capacity and resource for both community NHS services, social services and other associated activity. This financial overview will form the basis of contractual arrangements to be made between the organisations prior to the next financial year.
Enc 03i
Page 1 of 12
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 03i
Subject: Minutes of the Finance, Investment & Performance Committee and Chair’s Report
Strategic Goal SG5 –“We will make excellent use of our resources and improve levels of efficiency across all services.”
Director Lead: Melanie Print, Company Secretary
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT:
The approved minutes of the meeting of the Finance Investment & Performance Committee of 16 January 2013 are enclosed for information. Redactions have been made in relation to items of business which are commercially sensitive. This report contains a summary report from the Chair of the Committee on the key issues and business of the Committee during its recent meeting of the 20 February 2013. This is made by way of assurance to the Trust Board that the Committee is effectively discharging its Terms of Reference and current Cycle of Business for this year. KEY POINTS: Items of Business / Matters of Assurance discussed February meeting • The Committee reviewed the M10 finance report, noting that the actual surplus to the end of
January 2013 is £1,205k. The (mitigated) forecast gap is £489k and the Committee urged that additional CIPs are now brought on line and that full budgetary control is maintained so as ensure full delivery of the CIP by the year end. The Committee noted that the level of flexibility to close the gap has greatly reduced and that there has been a significant switch in the use of agency staff, as opposed to bank staff, in the Northern Division, with an increase in agency staff engaged to support the Transformation Programme. The Committee noted that the ability of the Divisions to improve their financial performance to the year end is dependent on negotiations with Commissioners.
• The Committee noted that the Northern Division CIP shortfall relates to hospital services, the Southern Division having identified further CIP schemes resulting in over-recovery at Month 10. The Committee noted that whilst there will be a full year achievement of the CIP, achievement if reliant on non-recurrent funding which will impact on the CIP for 2013/14.
Enc 03i
Page 2 of 12
• The Committee reviewed the financial assumptions that underpin the LTFM.
• The Committee received a briefing on the procurement options for a single provider for
Financial Services, Payroll and Procurement.
• The Committee received an update of the work of the Data Quality Group noting that: the compliance rate for Data Timeliness Reports has improved to 81.5% in the Southern Division Health teams, but that there is a lower compliance rate in the Northern Division; the Group considered the results of RSM Tenon’s data quality audit, the recommendations of which have been actionned within an action tracker; and considered the priorities for the Data Confidence Scores. The Committee noted that the Trust continues to build up an “evidence bank” of improving data quality, and confidence in the quality of data that it relies upon in assessing performance against national and bespoke (to the Partnership Trust) indicators.
• The Committee reviewed the IM& T Update Report noting the progress to date in implementing
the 6 key programmes which underpin the IM&T Strategy, and the progress in implementing the successor Health Informatics Service – “Staffordshire and Shropshire Health Informatics Service Transition Programme”, the design of which is being developed with officers of the Trust.
INTER DEPENDENCIES: Legal and/or Risk The Board should maintain an overview of the meetings of the principal
Committees of the Board so as to ensure that, as a matter of good governance, they are discharging their Cycle of Business and their Terms of Reference.
Clinical N/A
Financial N/A
HR N/A
Social Care N/A
Patient & Public Involvement
N/A
Equality Impact N/A Information exempt from Disclosure
Commercially sensitive information in relation to bids made by the Partnership Trust has been redacted from the Report.
Requirement for further review
N/A
RECOMMENDATIONS: The Trust Board is asked to: • Note the approved minutes of the FIP Committee meeting of the 16th January 2013; • Note the business covered at the recent meeting of the Committee on the 20th February 2013; • Gain assurance from the Chair’s summary report as to the ongoing business of the Committee
and its effectiveness in discharging its Terms of Reference and cycle of business.
Enc 03i
Page 3 of 12
Meeting of the Finance, Investment & Performance (FIP) Sub-Committee of Staffordshire and Stoke-on-Trent Partnership NHS Trust
Members and Required Attendees present: Jenny Jobson (JJ) Chair & Non-Executive Director Jonathan Tringham (JT) Director of Finance & Resources Jenny Hendon (JH) Non-Executive Director Geraint Griffiths (GG) Deputy Chief Executive Officer Paula Furnival (PF) Director of Operations In attendance: Susan Fisher (SF) Associate Director of Performance Melanie Print (MP) Company Secretary Julie Tanner (JkT) Director of Workforce & Development (part) Nathan Johnson (NJ) Head of Procurement & Commercial Services Jo Roberts (JR) Strategic Procurement Manager Michelle Bromley (MB) Minute Taker ACTION 1. Apologies
Jenny Ledgar, Stuart Poynor, Andy Talbot and John Scarpello
2. Minutes of Previous Meeting, Matters Arising and Action Tracker The Committee approved the minutes of the previous meeting as being a true and accurate record, subject to the following comments and amendments:- Page 3, Item 4 – Performance – Paragraph 6 – first sentence to be removed. Page 4, Quality Performance Assessment – JH requested that it be noted that she supported Model B. Page 5, Specialist Indicator – first paragraph – “social care service manages will manage” should read “social care service managers will manage”.
MB
MB
MB
Action Tracker The Committee reviewed the Action Tracker and noted the progress made. Action number 90 – JT reported that following discussions with GP, JT was awaiting GP to send a link to JT. Once the link had been received JT would circulate the self assessment questionnaire to all Committee members. Action number 93 – SF stated that identifying suitable targets for bank and agency should be led by HR and Ops and supported by Finance and Performance, with sign off by HR. Matters Arising
JT
Enc 03i
Page 4 of 12
Update on Establishment of Central Bank JkT reported that she had enquired about commissioning someone to work with the Trust to complete a review on the Bank and Agency work which had already taken place. JkT added that the person commissioned to do the work would look at which organisations could provide a centralised service and would be able to provide the services required by the Trust. A business case would be produced to be presented to the FIP Committee for approval. JkT reiterated that some work needed to be carried out on an interim basis to look at areas which need immediate corrective action. The Chair queried the timescales for appointing someone to carry out the work, JkT stated that the individual could start immediately, working two days per week for the Trust. The work should be completed by the end of the February and actions in place in time for the new financial year. SF noted that Action 97 on the tracker should be linked to this work.
3. Tender Process Outcome – Staff Wellbeing Service JkT reported that the report was to advise the Committee of the outcome of the tender process and to seek approval to award the tender to the preferred provider. JkT informed the Committee due to legacy arrangements the Trust was being supplied with occupational health services by four different providers. The service is therefore fragmented and inconsistent and the requirements of the Trust now reach beyond the traditional reactive services. The service specification had been produced in view of recommendations of the Boorman NHS Health and Well-Being report and the Trust’s Health and Wellbeing Strategy. A robust tendering process had been followed, facilitated by the Procurement team, this resulted in two tenders. JkT advised that there had been a marked difference between the presentations and it was proposed that the contract be awarded to Team Prevent. JkT added that only a small saving would be made within the first year, due to set up costs, with more savings in the following years. JkT stated that the Team Prevent had an account manager approach and would attend workforce meetings; they were also very proactive in relation to sickness absence. JkT added that discussions were being held in relation to working in collaboration with UHNS with regards to accommodation, as Team Prevent also worked with UHNS. PF queried whether the service would include Social Care Staff, JkT confirmed that it would. MP queried the length of the contract; JkT stated that it would be for three years. PF asked whether communication would be sent out in relation to any new processes, JkT confirmed that she was liaising with S Quarmby, the Staff Engagement Manager, to arrange for the communications to be sent out at the beginning of February. The Committee discussed whether there were any issues relating to the Section 75 agreement, JkT confirmed that the Trust had already provided notice on the service and the funding would therefore be available for the new service. The Committee approved the awarding of the Wellbeing Service to Team
Enc 03i
Page 5 of 12
Prevent. JkT left the meeting.
4. Quarterly Update on Procurement NJ and JR joined the meeting. NJ reported that the current savings position was that there had been £213k savings at the time of the report, however there were now £233k savings to date. There was a £53k forecast of further savings in the workplan to the end of the year. The Chair asked for confirmation that the total savings for the current year were £286k. NJ advised that the current position for 2013/14 would be £388k savings, which was a slight increase on the initial commitment. The Chair questioned whether this would be the total savings for the full year, NJ stated that it would be, the figure did not include everything, however there was a need to be realistic. JH noted that the majority of the savings were around recruitment and toner cartridges and did not seem particularly innovative. JR stated that these were the savings which had been delivered and there was work being carried out on a further 35 areas of savings. JR added that approximately 70/80 projects were being worked on at any one time. JH queried the completion date of 31/12/12 for the Pharmacy Related Procurement project, where the estimated annual spend was £3m. NR stated that the tender was currently being reviewed, with a view to the Trust joining with UHNS. JH queried whether the Medical Director was involved in a piece of work relating to this and questioned whether there was a link with the two pieces of work. MP stated that there were two issues, one being the redesign of the pharmacy service and the second was around the lack of controls in pharmacy ordering. The Chair asked who was reviewing pharmacy. GG responded that there was some tendering work ongoing and he would request an update. The Chair requested that GG report back to the Committee with the details of who was the lead on this matter and what were the savings/efficiency targets. GG stated that the lead was the Medicines Management team with a link to the transformation team. GG added that he was meeting with them in the near future for an update, the details of which would be included as part of the CIP 2013/14 update. NJ queried whether the work included dispensing; GG stated that the Medical Director would be looking at the whole picture. NJ agreed to discuss with the Medical Director, Doug Wulff. JH queried whether the list of savings produced by Ernst & Young had been shared with the Procurement team; JR confirmed that the savings related to procurement had been shared. PF commented that there was an issue around demand in relation to continence provision. JR stated that the provision for continence in the North and South Divisions was very different. There were three options, which had been provided to the continence leads and decisions were awaited. The two COOs had responded with an agreement to pursue the OJEU route and the service leads
NJ
Enc 03i
Page 6 of 12
had responded that they did not agree with that. JR agreed to contact the COOs for a decision. JR outlined the key points: Estates – the procurement team met with Estates last year and provided the Top 10 spend areas for all Trusts within the LHE, this was currently undergoing analysis by the procurement team. Mobile Telephones – the current suppliers had offered a reduction on line rental which had been accepted. The procurement team continued to engage with the suppliers to try to extract further value for money in the interim. Agency Recruitment – Ancillary, Medical Locums, Nursing and GP Locums were all under review and in the process of being re-let. The procurement team were working closely with the Medical Staffing Officer. The Chair queried whether HR was being involved, JR confirmed that they were. Trust Communications and Training – JR had been working with JT and the finance team to create a new competitive waiver and Breach of SFI procedure, which included more robust control. PF queried whether there was a training need in this area, JR confirmed that training sessions had been set up and were starting this month and would continue in the future. SF queried the process in exceptional circumstances, JR and JT confirmed that exceptional circumstances would be taken into consideration as and when they took place. Systems – A technical authorisation process for the e-requisitioning system had been set up where JT authorises particular categories of expenditure. SF queried whether SCC staff were aware of the process for ordering goods/ services. JR stated that she received many calls from SCC staff, so they did know who to contact with any queries. SF stated that a communication needed to be circulated to SCC staff to inform them of the correct procedure and that they should contact the procurement team. Trust Standardisation – sub groups for all areas of standardisation were being set up and requests for nominations for the sub groups had been circulated and responses were awaited. JR reported that members of the procurement team now attend both the North and South divisional management meetings. Lists of suggestions from front line staff had been received by the procurement team and JR now had closer links with all of the COOs. NJ informed the Committee that he had attended various meetings in London regarding the Department of Health Procurement Strategy. The strategy was due at the beginning of February, therefore a further update would be provided at the next quarterly update. Contract for Linen and Laundry Services JR informed the Committee that the UHNS had served notice on the delivery of the above service; the contract was due to end on 31 January 2013. The linen and laundry service was transported and managed internally by UHNS but the laundering process was actually delivered by Synergy Ltd as part of a contract which runs until 2017. The procurement team had met with the hospital site managers in August to
JR
Enc 03i
Page 7 of 12
begin the review of the service specification. JR stated that following negotiations with Synergy they had agreed to novate the contract with no additional costs to the Trust and the Trust would purchase directly from Synergy but utilise the UHNS contract. This would deliver a £47k saving in the year. The report had been sent to MP for review and a response was awaited. The Chair queried whether there would have been any value in “going it alone”. JR stated that it was better to procure as a consortium and it would not have made financial sense for the Trust to go into the open market alone. JR confirmed that there was not a better deal available. PF queried whether there was a way where demand and usage could be monitored and whether there would be a point during the year where volume could be checked. PF added that it would be useful for her to have this information. The Committee agreed to make a recommendation to the Board for approval of the contract with Synergy Ltd. The Chair requested that in future more notice was required for decisions of this nature. JH commented that if a decision was required on a more contentious contract then it would be very difficult to approve with such short notice. Contract for Software to run the Staffordshire Diabetic Retinopathy Screening Service JR reported that there were a small number of suppliers of this service in the market place. The relevant specifications of service had been obtained from the local and national teams. The PQQ process had been completed and the Trust was currently at the ITT stage. The service is currently operating on a contract extension which expires on 31 March 2013. MP queried whether the unit costs would be recharged to commissioners, JR and GG both agreed to check. The Committee noted the procurement of the Staffordshire Diabetic Retinopathy Screening service. Given the timescales outlined in the paper the Committee again requested that it would be preferable to have more time to review and agree these tender decisions in the future. PF queried the process for renewing contracts in a timely manner and whether the Trust should be doing anything to improve. MP stated that the Trust had inherited lots of spend without contracts and the procurement team were tracking the spend and were engaging with the service leads. PF questioned whether the Trust should be doing anything to capture the contracts which expire in the near future. JT stated that a communication should be circulated to staff, stating that if there were contracts in place, discussions needed to be held with the procurement team well in advance of the end date. NJ stated that there was a database which was being constantly updated. JR agreed to pick this matter up during the procurement meetings and the divisional management meetings. The Chair queried whether there was a need to inform the Quality Governance
JR/GG
JR
Enc 03i
Page 8 of 12
Committee about any contracts; JT stated that the procurement plan would be presented to the QGC. JT noted that a debate needed to take place as a Committee to decide which contracts should be discussed at the FIP meetings in view of the revised SFIs. The Chair requested that this item be added to the agenda for the next meeting. NJ and JR left the meeting.
5. Financial Performance – Month 9 JT reported that the purpose of the report was to present to the Finance, Investment and Performance Committee the financial performance to the end of December 2012. JT highlighted the key points, noting that the Trust continued to forecast the achievement of the required surplus of £2m. JT noted that there would be a higher degree of risk in achieving the required surplus due to the need to make additional investment in the capacity of the Community Services as a result of increased pressures on the Local Health Economy; the level of financial flexibility available to the Trust had been reduced. JT outlined the key issues presented in the report for the North Division. JT reported that the South Division should breakeven; however this was largely dependent on the successful outcome of negotiations with commissioners. Agreement had been reached for funding in certain areas; however it now appeared that some funding was being withdrawn. GG stated that the contract was very clear and this matter had been escalated to the Commissioning Board. JT informed the Committee that the movement with the Corporate Division was consistent with previous months. In relation to Social Care, a balanced position for the year depended on the County Council honouring the funding arrangements agreed in the section 75. JT advised that the agency spend had continued to reduce in December. The year to date expenditure on agency was £3.6m. There were significant reductions in agency spend in the corporate division. JT gave a summary of the Cost Improvement plan (CIP) performance for month 9 by Division. JT confirmed that the Trust would achieve the CIP in full this year and measures had been put in place to ensure this would be the case. The Chair and PF queried the forecast variance as the tabled forecast numbers indicated a variance of £708k. JT clarified that based on existing schemes where funding had been removed from budgets there was indeed a £708k shortfall. However as previously reported to the Board the Trust was forecasting to completely close this gap during the last quarter of the year. The Chair and PF suggested that if JT could add that commentary below the CIP forecast table with an outline of the schemes that would close the gap, it would enhance the understanding of future financial reports. JT outlined the financial outlook for the year and stated that the remaining gap was £1.3m; JT added that there were a number of areas which would contribute to reduce that figure.
Enc 03i
Page 9 of 12
The Committee noted the financial performance for the period and the increased risk associated with the forecast position.
6. Performance Integrated Performance Report SF informed the Committee that the report had been presented to the Board. SF added that an update had been made to the report since the Board meeting. An agreement had been reached with HIS to ensure data was received at day 5 of the month rather than at day 15. SF reported that in relation to the summary quality and safety assessment proposals, subject to comments being received from the Executive Management Team, the preferred option was Model B. The Committee noted the content of the Integrated Performance Report. Data Quality Group Update SF reported that the Data Quality Group was set up and meeting on a monthly basis. The report was to inform the Committee of the process followed. JT commented that the FIP Committee needed to be aware of the processes and how the scoring worked. SF noted that two audits had been carried out on the indicators and this would be formally reported to the Audit Committee. JH commented that the Group had worked extremely hard and gave thanks for this. The Chair reiterated the thanks and SF agreed to forward the comments on to the group. SF noted that these two indicators were very important indicators and whilst the other indicators were important they would not be worked through in as much detail as there was such a large number of indicators. The Committee supported the work of the Data Quality Group in driving improvements in data quality for the organisation. Direct Payments SF reported that the report was to provide the Committee with an overview of the Direct Payments process. The final decision of whether direct payments were offered was made by the relevant Social Worker, as they have the interaction with the individual concerned. SF added that the payments were to give people money in order to achieve their personalised care. SF stated that all payments were reviewed each year. The Chair queried which indicator this item would be listed under – SF confirmed it was under SC32. JH stated that the Committee did need to understand all of the targets. SF agreed to circulate a reduced version of the guidance notes. PF commented that it was important to maximise the independence of people and queried how assurance could be sought that the Trust had control that people have the choice of self directed support. SF noted that the performance against this target was linked to the competency framework for Social Workers. The Committee noted the report and the continued focus on improving
SF
Enc 03i
Page 10 of 12
performance in relation to the Director Payment element of Self Directed Support. Delayed Transfers of Care (DTOC) SF reported that whilst the delayed transfers of care performance had had a varying trend and had increased over the last two/three months, SF now had assurance that there was a more proactive approach rather than reactive approach to this indicator. SF added that she was confident that the Trust would achieve the target by the year end. SF informed the Committee that the most recent figures showed that there was a sustained improvement. PF stated that there were a number of ongoing pieces of work with UHNS to ensure the DTOC target was met. PF added that a clinical and practice task group had been set up to produce a more robust policy for transferring patients out of hospital. PF stated that some of the delays related to care package delays. PF added that some challenge had taken place, although further discussions needed to take place with commissioners. The Chair queried whether the integration of SCC and SSOTP had made an impact on this indicator and how the relationships with the Stoke on Trent City Council were in relation to care on discharge. PF stated that the relationships were good, although the same problems did occur. The integration had not made a difference as the processes were already in place prior to integration. The Chair gave thanks for the report and stated that it was very useful. The Committee noted the report and the continued focus on improving performance in relation to DTOC. Standard Operating Model (SOM) SF reported that the report was to provide the Committee with an early sight of the Trust’s latest submission, which remained incomplete at this stage. The final submission would be presented to EMT on 21 January for review and approval. SF informed the Committee that the only area that had changed was the CDiff indicator rating, which had changed to a Green rating as the Trust was back to its expected levels of CDiff. The Committee noted the content of the provisional submission and acknowledged a complete version would be submitted to and agreed by the Executive Management Team on 21 January 2013.
7. Update on Business Development Activities - CONFIDENTIAL GG advised the Committee that the report detailed the main business activities across the Trust in Quarter 3 2012/13. GG highlighted the tenders which were being prepared for the next stage of competition. GG reported that there was a more robust decision making process in place around which contracts the Trust bid for as a report was presented to the Executive Management Team each month for approval.
Enc 03i
Page 11 of 12
The Committee noted the current position with regards to the level of business activity and the areas of pending submission/outcome.
8. Report on Contractual Process for 2013/14 GG gave the Committee a verbal update. GG reported that in terms of the ongoing work to agree baseline positions with the CCGs for the contract round for 2013/14 the failure to conclude agreement with the contract negotiating teams had required formal escalation to the Commissioning Board. In the South Division, an extraordinary contract meeting had been requested to formally escalate the process. In the North Division, a half day meeting had been requested with senior directors of the CCG to decide on a position. GG added that the deadline to agree a position was the end of February. GG stated that there was more confidence of reaching a satisfactory agreement in the North as the CCGs in the North Division recognised that there was a need to make investment in community services due to continuing capacity problems across the Local Health Economy.
9. IM&T Strategy JT presented the report and the Chair commented that it was a well written and well thought out document. JT stated that this document builds on the previous strategy document which had been presented to the Board a year ago. JT reported that this Strategy will supersede the earlier IS Strategy. Feedback received from consumers, the SHA and others had been taken into account when producing the report. Support had also been given by Andy Talbot. The document had been presented to the Executive Management Team meeting. JT added that the Strategy had been shared with RSM Tenon to receive a view on whether it was fit for purpose and would be presented to the Trust Board on 30 January. JT outlined various aspects of the report and highlighted the ten IM&T visions set out on page 11 of the document. The visions were followed by the goals to support the vision. JT brought the Committee’s attention to page 14 of the report which listed eight broad programmes to be established. JT reported that there were five or six posts in the structure which were critical to the Strategy, and early approval had been received to recruit to these posts. During the recruitment process for these posts, interim support will be brought in. SF pointed out that some work was already taking place in preparation. The Chair commented that the Strategy was very easy to understand and queried whether any engagement with clinical staff had taken place. SF stated that the Chief Information Officer (CIO) had liaised with staff. The Chair commented on the data input/data capture and emphasised the importance of cultural change and the people aspects of the IT programme. SF stated that this was included in the performance strategy and added that she had worked closely with the CIO on this aspect. SF stated that training was ongoing and the emphasis would continue on data quality and data capture.
Enc 03i
Page 12 of 12
JT referred the Committee to page 30 of the document which listed all projects with the timeline for delivery. JT reported that the total capital investment was approximately £18m. JT informed the Committee that the table on page 34 mapped the IM&T goals and visions to the goals and visions of the Trust. The Chair queried when the capital funds would be approved. JT responded that the report would be presented to the Trust Board in January and approval for the funds would be requested at that meeting. The Chair queried whether there was a contingency regarding funding built into the Strategy. JT stated that this was all built into the LTFM; however each individual project would have a business case which would need approval. The Committee noted the much improved IM&T Strategy.
10. Review of Actions/Risks and Key Items for Reporting The Committee agreed that following assurance in the report on Delayed Transfers of Care, this item did not need to be added to the Risk Register.
11. Any Other Business There were no other items for discussion at this time. The meeting closed at 12.56.
12. Date and Time of Next Meeting Wednesday 20 February 2013, 10.00 am – 12.30 pm, Chesterton Room, Morston House.
Enc 03ii
Page 1 of 14
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
Strategic Goal SG5 –“We will make excellent use of our resources and improve levels of efficiency across all services.”
Director Lead: Melanie Print, Company Secretary
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT:
To provide an update and an overview of the actions and business of the recent meeting of the Quality Governance Committee; and to receive the minutes of the meeting held on 9 January 2013. KEY POINTS: Items of Business – February Meeting Governance The Committee is undertaking an effectiveness review of its performance, the results of which will be incorporated into the revised Terms of Reference and Annual Plan for the Committee for 2013/14. All reporting Sub-committees have been tasked with reviewing their membership so as to ensure that all members can attend meetings and support the Sub-committees in discharging their cycles of business and terms of reference. The Committee undertook an in-depth review of the Effectiveness Report noting: the progress to date in developing a bespoke Trust Mortality Review; tasking the Associate Directors of Quality and Performance with a review of the performance reports providing assurance in relation to the management of Third Party Contracts by the JCU; and determining that effectiveness should be prioritised in the order of business of the Committee. The Committee discussed, in depth, the handover of the functions and work streams of the Adult Social Quality & Governance Sub-Committee, and have asked that the designated leads of the assigned functions and work streams provide an assurance report to the Committee, in March, as to the status of the risks and functions assigned to them. The Committee has tasked the Director of Operations, in conjunction with the Adult Safeguarding Sub-committee, to undertake a review of effectiveness of adult safeguarding processes following a referral report from the Audit Committee, the outcomes of which will be reported to the Committee in March with a subsequent report from the Chair of the Committee to the Audit Committee on 22 March 2013.
Enc 03ii
Page 2 of 14
Assurance The Committee received the Annual programme of work for Infection Prevention and Control for 2013/14, noted the progress that has been made in implementing the actions, within the Quality Governance Framework, to improve the quality score of Trust, and noted the Q3 review of the implementation and progress in completing the Quality Account priorities for this year. The Committee noted an update on the Quality Circles undertaken within Adult Social Care, noting that they provide an opportunity for reflective practice whilst agreeing that improvements could be made in providing a system of consistent reporting, trend analysis, and review; with a subsequent report to the Committee to provide evidence of the implementation of the agreed improvements. The Committee endorsed and welcomed the success of the Documentation Campaign – “On the Record – Essential Care” and welcomed the refresh of the Professional Forum. The refreshed Professional Forum will provide a forum for multi-disciplinary innovation and development, channelling innovative practice and ideas into the right teams and corporate structure, so that the current gap between frontline staff and the wider organisation is bridged. INTER DEPENDENCIES: Legal and/or Risk The Trust Board should maintain an overview of the meetings of the
principal Committees of the Board so as to ensure that, as a matter of good governance, they are discharging their Cycle of Business and their Terms of Reference.
Clinical N/A
Financial N/A
HR N/A
Social Care N/A
Patient & Public Involvement
N/A
Equality Impact N/A Information exempt from Disclosure
N/A
Requirement for further review
N/A
RECOMMENDATIONS: The Trust Board is asked to: • Note the Chair’s report on the current business of the Quality Governance Committee. • Receive the minutes of the meeting of the Committee of 9 January 2013.
Enc 03ii
Page 3 of 14
Meeting of the Quality Governance Sub-Committee of Staffordshire & Stoke-on-Trent Partnership NHS Trust Board
Sub-Committee members present: David Pearson DP Non-Executive Director (Chair) Roger Evans RE Non-Executive Director Susan Fisher SF Associate Director of Performance Paula Furnival PF Director of Operations Carl Griffiths CG Chief Operating Officer Adult Social Care (North) Rose Goodwin RG Associate Director of Professional Leadership Siobhan Heafield SH Director of Nursing and Quality Jenny Hendon JH Non-Executive Director Becky Monaghan BM Associate Director of Quality Liz Onions LO Chief Operating Officer (South) Stuart Poynor SP Chief Executive Officer Melanie Print MP Company Secretary Nigel Ratcliffe NR Trust Chairman John Scarpello JS Non-Executive Director Doug Wulff DW Medical Director
Apologies: Mandy Donald MD Chief Operating Officer (North) Julie Tanner JT Director of Workforce and Development
In attendance: Sarah Richardson SLR Executive Assistant (minutes)
2012.205 Welcome and Apologies The Chair welcomed Committee members to the meeting giving apologies from Mandy Donald, Chief Operating Officer (North) and Julie Tanner, Director of Workforce and Development
2012.206 Minutes of the last meeting and matters arising The Chairman referred members of the Quality Governance Committee to the minutes of the meeting held on 9 January 2013. The following changes to the minutes and matters arising were raised: P3 of 13, Para 3; amendment to minute – NR queried whether the UHNS tissue viability team depletion would have any impact to SSOTP. P3 of 13 – LO noted that she had raised the issue of the capacity of Best Interest Assessors to meet the current demand for assessments. P4 of 13, re completion of works at Longton Cottage Hospital – SH asked the Committee to note that this was in relation to closing of doors at the hospital. 2012.192 – SH informed the Committee that the Falls Report has been forwarded to the Chairman of the Cluster and that a quarterly executive summary is being developed by the Quality team as per action 2012.177 on the action tracker. A template will be submitted to the March Committee meeting.
Enc 03ii
Page 4 of 14
P9 of 13, Para 5; amendment to minute - LO noted that there is no-one in post to support the increasing number of non-medical prescribers. 2012.194 - JS queried as to where the governance of the refusal of care policy would be considered. BM stated that this would be monitored through the Safety and Effectiveness Sub-Committee and reported back to the Committee in April. 2012.199, Para 2: amendment to minute – SP advised the Committee that the Trust permits extensions to the 30 day investigation period for complaints. He reported that in future this will be only allowed in exceptional circumstances and therefore there may be a dip in the performance of Health Care compliance rate. Members of the Quality Governance Committee accepted the minutes of the meeting held on 9 January 2013 as a true record.
2012.207 Action Tracker 2012.122 – evidence has now been forwarded to CQC; there is likely to be more unannounced visits in the future. 2012.132 – LO apologised for the incomplete action tracker in relation to this action. She advised the Committee that local induction packs are in place across the Trust and that standardisation of the same is currently being developed and will be scrutinised by HR. DP sought an assurance that induction within the Trust is consistent across the Trust especially in relation to when bank and agency staff are receiving induction. SP gave assurance that there is a consistent induction training process in place and that this is mandatory for all staff. 2012.159 – BM reported that discussion has taken place in relation to the outcomes of Quality Visits and consideration was being given as to how this could be put into the public domain. BM noted that the Effectiveness Sub-Committee agreed that dissemination of learning from the quality visits should be reported. The Committee agreed that this should take place on the Trust Website. 2012.175 – The Committee was asked to note that the Community Nursing Project Board relates to the North of the Trust only. 2012.176 – DP requested that ideas for the QGC Quality of Care focus session agenda be forwarded to SLR no later than Friday 8th February. JS submitted his apologies to the session and requested that user experience of domiciliary care be included on the agenda. 2012.183 – Typographical Error: An update re Audit Programme following the review by the Practice Audit Group. Members of the Committee received and noted the Action Tracker.
2012.208 Summary of progress and actions of Sub-Committees DP noted that there could potential confusion in relation to the minutes submitted from the Sub-Committees as the WFM minutes submitted reported exceptions to be escalated but no exception report was circulated. He asked the Committee to note that these matters of exception had been escalated to the Committee at the January meeting enclosure 2v.
Enc 03ii
Page 5 of 14
It was agreed that all Sub-committees and reporting sub-groups should be reminded of the requirement to submit a front cover in the required format; that any matter to be escalated by exception should include a rationale for its escalation and the decision required from this Committee; and that Chairs of Sub-committee should secure a more disciplined approach to the completion of actions of their Sub-committees. User and Patient Experience (UPE) BM outlined the exception report from the User and Patient Experience Sub-Committee and noting that the exception relating to Out of Pocket Expenses Policy has been brought to the Committee for discussion under agenda item 15. BM asked the Committee to note that the Sub-Committee title is incorrect and that it should read User and Carer Experience. Safeguarding Vulnerable Adults Committee (SVAC) RG advised the Committee that the Trust is considering the Pan West Midlands Adult Protection Procedures options paper however the Trust is currently still continuing with local interagency procedures. Concerns were raised that these could be very prescriptive ways of securing effective operational safeguarding. SH reported that feedback has been requested by the Staffordshire and Stoke on Trent Partnership (SSASP) and that she will be meeting with the Independent Chair to discuss the options. Safeguarding Children’s Strategic Sub-Committee (SCSC) RG asked the Committee to note the exceptions reported. Workforce Matters Sub-Committee (WFM) The minutes circulated with the papers were for information. Adult Social Care Governance and Quality Sub-Committee (ASC GQC) The ASC QGC paper was considered by the Committee under agenda item 5. NR raised concerns regarding the amount of apologies received by the Sub-Committees and requested that this be escalated. The Committee concurred and requested that a communiqué be sent on behalf of the Committee to all Chairs ensuring that attendance at the Sub-Committees is greatly improved. The Committee noted that the Action Tracker from the Sub-Committees were inconsistent with the corporate template and requested that the correct template be used. The Committee also enforced that actions are completed in the appropriate timescale and that it was not acceptable for actions that were raised in August for completion in October to be still outstanding in February of the following year. MP reminded members that the revised Action Tracker had been implemented (with instructions) in December and confirmed that she would reiterate the message to all Sub-Committee Chairs. Members of the Committee received and noted the QGC Sub-Committee updates and reports.
SLR
MP
MP
2012.209 Social Care – Handover Legacy Document CG stated that report circulated with the papers came about following the last QGC meeting. An extra-ordinary meeting of the ASC GQC has taken place and has approved the document which outlined the work undertaken to hand over the functions of the ASC GQC to those persons and Sub-committees designated within the Legacy report.
Enc 03ii
Page 6 of 14
NR expressed concerns surrounding the report stating that it was difficult to determine who was accountable for the work streams of the ASC GQC and which function lay with the County Council, the Joint Commissioning Unit or the Partnership Trust. He queried whether there would be any impact on quality and noted that there was no Professional Lead for Social Care at the Trust. CG reiterated that the Legacy report did assign the functions of the Sub-Committee into the corporate functions of the Trust and had addressed the residual risks that are to be assigned to the leads and Sub-committees referred to in the Report. He noted that the appointment of the Professional Lead for Social Care is progressing and highlighted that the document is a ‘point in time’ document; it identifies what actions had been undertaken to mitigate the highlighted risks and where the residual risk would be assigned to within the Trust. RE concurred that the Legacy document was at the ‘point in time’ of the closure of the Sub-Committee. PF asked the Committee to note that social care are currently obligated to carry out quality circles and that professional leadership is embedded within the competency framework of Social Workers. PF assured the Committee that sharing of best practice is taking place with “lessons learnt” being disseminated across the Trust through her Directorate. DP questioned whether it would have been advisable to include the original spread sheet as an appendix so to offer context to the Legacy document. NR commented that he felt a lack of assurance from the document and that he did not feel confident that there was adequate grip on quality in social care. RE said that the approach to social care was different to health as they were different cultures. CG recognised that the risks from the Sub-Committee were still in place. GG noted that new owners would take on these risks following its closure. SH acknowledged that it was a ‘point in time’ document however recommended that it would be useful to see where the actions were coming from as well as the new owners. SP stated that the risks around the quality of the complaints process for social care were being addressed. SP noted that this was a “point in time” document and that the time was right for the winding down of the Sub-committee with the incorporation of the functions into the corporate functions of the Trust. SP requested that a high level assurance map by way of exception report be made to the March meeting of the Committee, with each owner of the transferring functions providing an update on the risk status of the assigned functions and risks; and assurance that transferring function has been transferred to the designated lead and mapped into their portfolio of work and/or the cycle of business of the relevant Sub-committee. JH agreed with NR concerns regarding the legacy report however noted that as an ASC GQC member she felt that it had run its cause and that it should be disbanded. She also agreed that assurance needed to be provided to the Committee that the transferring functions had been embedded into the organisation
Enc 03ii
Page 7 of 14
and that this be provided by the action owners. Members of the Committee agreed that the ASC GQC Legacy Document be revised as discussed; and that a risk assessment spread sheet (in the format presented to the Committee at their January meeting) with completed scores, together with an assurance report in the format referred to above be submitted to the March Committee meeting. Members of the Committee noted that there would no exception to this timeline for any of the persons/Sub-committees to whom the functions of the ASC GQC had been assigned. DW requested that this information to be disseminated through to the Sub-Committees to ensure triangulation.
MD CG RG BM
LO
2012.210 Risk Register The Committee were asked to note the updated Risk Register circulated with the papers and the actions that are being taken to manage the reported risks NR endorsed the robust process that is now in place and asked whether this was now embedded in the Sub-Committees. MP stated that the Trust is now confident that risks are captured at a corporate level and are effectively monitored by the Directors but that further testing of the process at an operational level was required. MP noted that the Internal Auditors were undertaking an audit of how effective and embedded risk management was at operational levels within the Trust. MP noted that the outcome of this audit would be reported to the March meeting of the Audit Committee and the April meeting of this Committee. CG noted that Social Care also has a rigorous system in place for monitoring risks. Members of the Committee received and noted the report and the actions being taken to manage the reported risks, and were assured that the reporting of risks was a standing item of business for all Committees and Sub-committees of the Board.
2012.211 Safeguarding DP advised the Committee that this agenda item has come about from an action and recommendation from the Audit Committee in relation to the Assurance Report into Adult Safeguarding, as reported to the Audit Committee on 18 January 2012, which was circulated with the papers. He requested that the report be submitted to the SVAC for action and to provide an assurance report to the Committee at the next meeting for review prior to submission at Audit Committee in March. LO reported that the issues would in future be picked up at the Safety and Effectiveness Operational (SEOG) meetings. PF raised a concern that this was the first time the Director of Operations had had sight of the Report. MP noted that the Limited Assurance report annexed to the Report had been submitted in draft format to Senior Officers within the Operations Directorate for their comment and review 2 months before the final report had been submitted by SCC Internal Auditors to the Audit Committee.
Enc 03ii
Page 8 of 14
MP reminded members of the Committee of the need to report and map all relevant risks within their Directorates and to be disciplined in highlighting matters of limited assurance so that this Committee had direct line of sight of matters of concern. MP welcomed the fact that the governance between Committees of the Board was working well as evidenced by the referral of this matter to this Committee for its consideration, review and action. MP noted that the lack of assurance noted within the Report had been incorporated into the Board Assurance Framework as a “control gap”; this had been reported to the Trust Board; and that there was an expectation that this control gap would be closed at the next review of the Board Assurance Framework, if the actions and recommendations highlighted within the Report were addressed. DP stated that assurance was required by this Committee and questioned that if the audit had gone to SVAC whether it would have been escalated to this Committee. DP noted that the themes within the Limited Assurance report were a lack of a good document trail which could be audited. DP stated that the Committee must have confidence that procedures are followed and consistent across the Trust. Members of the Committee received: • the Assurance Report into Adult Safeguarding and noted the limited
assurance in relation to the systematic review of investigated cases and non-investigative cases and the completion of investigations;
• agreed that the recommendations within the Limited Assurance Report
are actionned by the Director of Operations; • and that a report is provided to the next meeting of this Committee with an
assurance report to the March meeting Audit Committee as to the implementation of the recommendations.
DP requested that in light of the recommendations that this Committee receive quarterly reports as well as the Annual Report from the SVAC, CSCS and ICC Sub-Committees DW gave his apologies at 09:55
PF
PF
2012.213 Adult Safeguarding Work Programme RG informed the Committee that the Work Programme circulated with the papers was the close down of 2012/13 rather than the work programme for 2013/14 and requested that the item be deferred until the next meeting when the 2013/14 work programme would be submitted. Agenda Item deferred until the next meeting of this Committee.
2012.214 Children’s Safeguarding Work Programme Agenda Item deferred until the next meeting of this Committee.
2012.215 Infection Control and Prevention Annual Work Programme The Committee considered the Infection Control and Prevention annual Work Programme which outlined the evidence and assurance that the Trust has a robust Infection Control and Prevention annual programme of work for 2013/14; the Programme will ensure that the Trust maintains compliance with the ten criteria laid out in the Health and Social Care Act 2008 ‘Hygiene Code’.
Enc 03ii
Page 9 of 14
NR asked how the Trust ensures that the commissioned Care Homes to which adult social care placements are made maintains and meets the same standard of infection control and prevention as the community hospitals. SH stated that these organisations are regulated and inspected by the CQC; that the JCU maintains the framework for Third Party Contracts of Residential Care into which placements are made and that there is triangulation of concerns raised by infection control and tissue viability services with the quality monitoring that is undertaken by the Quality Monitoring Officers of the JCU to triangulate. SH noted that the primary responsibility to secure that good hygiene standards are maintained is that of the registered manager of the Care Home and the CQC. SH referred to “hot spots” of pressure sores in Care Homes which had been noted by District Nurses which had been escalated to both Directors of Adult Social Care within the City and County. DP emphasised that it is professional duty of registered health and social care professionals to report incidents. LO asked the Committee to note that in relation to point 16 with the Programme of Work the CCGs had recently disinvested in the Nursing Homes at Home Service which had provided training and support in relation to hygiene standards and the prevention of pressure sores. LO noted that this may result in an increase in reported pressure sores in Care Homes. JS accepted that it was the professional duty of staff members to report incidents however asked whether high reporting establishments were flagged to provide assurance. SH stated that this was picked up at the SEOG meetings and through the governance of the S75 and triangulated within incident reporting. CG reported that the CQC are invited to the SEOG meetings so as to provide them with “soft intelligence” on incident reporting and poor care in Care Homes, but that attendance was poor. SP noted that this had been a consistent theme at this Committee and requested that an assurance map be provided on the Third Party Contracts with the SCC, setting out which agency or body had primary responsibility and accountability for care in Care Homes and within domiciliary care placements; and what the role of the Trust was. It was agreed that the Company Secretary should provide such a report to the next meeting of the Committee. Members of the Committee received and approved the Annual Programme of Work.
MP
2012.216 Quality Account BM outlined the update on the Quality Account and asked the Committee to note the progress towards achievement of the 2011/12 Quality Account priorities including: • Safety Express • Dementia • Service User Experience • Social Care Integration. RE noted the positive increase in the Catheter Life Chart and patient held Catheter
Enc 03ii
Page 10 of 14
Diary document implementation across the Community Nursing Service. BM noted that joint training is taking place with all Health and Social Care staff in relation to dementia and staff rotation is taking place. PF advised the Committee that the Trust is aligning this training with metrics which measure improved performance. PF noted that the management of the change programme will implement the rotation of professional staff across all specialties. The Committee was advised that the Trust has now received Customer Service Excellence across the South and Social Care and is in the process of getting accreditation across the whole of the Trust. SF requested that for 2013/14 Quality Account, carer reviews by social workers and triangulation from service user feedback / concerns by families and third parties be included in the priorities, so as to ensure that the Trust is actively receiving responses from users and carers. SP referenced a recent visit he had made in which he had received positive feedback from staff members and families on the care that had been provided. SP advocated more engagement of staff with families, visitors and patients at all levels. PF said that she would action this across the Trust. DP asked as to whether the process has begun in relation to the review of the Quality Account for 2013/14 by the local Overview and Scrutiny committees. BM reported that this had not yet taken place however is on the action plan for 2013/14. The Committee received and noted the progress towards the achievement of the 2011/12 Quality Account Priorities.
PF
2012.217 Quality Circles – quarterly report The Committee considered the Quality Circles report which outlines the various improvements and innovations that Quality Circles within adult social care have discussed and actionned with the last quarter. CG acknowledged that there is a wide and varied approach to Quality circles and that there is a lack of consistent recording and reporting. The report highlights the richness and diversity of the themes. GG noted that although they do show good practice there are issues around the audits taking place and assurance in relation to improvements and actions that have been highlighted within Quality Circles. RE noted the positive benefits for frontline staff in improving their own performance and the approach to quality enhancement. JH noted that these need to be Trust wide in both social care and health. BM said that these need to be standardised and consistent across the Trust in ensuring the completion of actions. LO stated that these would feed into the Safety and Effectiveness Sub-Committee through Quality folders. CG concurred and reported that this would be the ideal way of ensuring that lessons learnt are disseminated. The Committee received and noted the report.
Enc 03ii
Page 11 of 14
2012.218 Assurance framework Approval & Review This agenda item was covered under agenda item 7.
2012.219 Self-Assessment against Monitors Quality Governance Framework The Committee was informed that the final report from KPMG in respect of assessment against and compliance with Monitor’s Quality Governance Framework would be issued on Friday 8th February and to gain assurance from the process from the report circulated with the papers. Members of the Committee received and noted the Report.
2012.220 Out of Pocket Expenses BM informed the Committee that this has come about following concerns raised at the UPE and subsequently the Trust Board. The policy circulated with the papers is to ensure that the Trust is line with other organisations in the Region in relation to the rates paid to service users who claim under the ‘help with costs’ scheme. The Trust currently pays 0.26p per mile when using a car and the UPE suggest that this should be increased to 0.45p. JS concurred that the rate paid needs to be in line with the other local organisations. The Committee agreed and approved the 0.45p rate. SF noted that the policy needed to be social care compliant in terms of payments paid to carers. BM advised the Committee that the policy will need a final review and a period of consultation before it can be ratified and implemented. It was agreed that as the Committee had approved the policy in principle once the agreed changes had been made and subject to a period of consultation then the Chair is authorised to take Chair’s Action to ratify the policy and report the same to the Board via the Quality Report. Members of the Committee received, noted and approved the 0.45p rate and the Out of Pocket Expenses for Involvement and Engagement Policy subject to a period of consultation and completion of the conditions stated above.
2012.221 Infection Control Policies for ratification
Members of the Committee approved the Infection Prevention and Control suite of policies relating to infection control and the Trust Compliance with the Hygiene Code.
2012.222 Documentation Campaign update RG informed the Committee that the Documentation Campaign update circulated with the papers is to inform the Committee of the progress of the ‘On the Record – Essential to Care’ campaign. LO asked the Committee to note that the Trust needs to be mindful of the move to becoming electronic when developing reports. SH advised the Committee that Staff Side have been regularly updated on the progress and an article has been included in the Word with a section from Adrian Legan from the RCN in support of the Campaign. The Committee recommended that the positive endorsement of the campaign be reported to Trust Board via the Quality Report.
Enc 03ii
Page 12 of 14
Member of the Committee received and noted the report.
2012.223 Unannounced Inspection of Staffordshire Local Authority for the Protection of Children – 5 November 2012 – 14 November 2012 RG asked the Committee to receive the report and acknowledge the findings of the Staffordshire County Council Unannounced Inspection of Child Protection services and to take assurance that the actions will be monitored through the SCSC. RG advised the Committee that the Inspectors gave positive feedback regarding the MASH in relation to Child Protection. CG asked the committee to note that there are different models for the safeguarding of adults and the safeguarding of children at the MASH. JS questioned as to whether the reduction in the average caseloads within the specialist safeguarding units was achievable within 6 months. RG said that the number of Health Visitors are increasing which will provide more capacity and health input for children. Member of the committee received and noted the report.
2012.224 Patient Safety Report BM gave a brief overview of the Patient Safety Report to the Committee outlining the key points. NR acknowledged the content of the report and questioned how the Trust measures how pressure sores are monitored following a transfer to home. BM stated that this has now been integrated into the report under Community Pressure Ulcers Acquired and noted that these are not collected in the same way for social care therefore the data is reported differently. The Committee received and noted the Report.
2012.225 User and Carer Experience Report BM brought the User and Carer Experience Report to the Committee and highlighted the key points in relation to Complaints, PALS and Patient Experience for health and social care. RE requested that the headline should read 23 formal complaints and 151 compliments. JS expressed concerned relating to the issues with the Sexual Health Services and sought assurance that this had now been rectified. PF agreed to follow up and provide an update to the Committee at its next meeting. LO asked how the Trust would be addressing the complaints that involve Outpatients. BM stated that work is taking place to address this. SH requested that should there be any impact on the quality of patient experience in the reconfiguration of services that this needs early engagement with PALs, Complaints and Patient Experience. DP asked how the Trust gets assurance that the learning actions, as referred to on page 6 of Enc 17, are being cascaded down and that practice is improving as a result. Due to time constraints the Committee agreed that this would be picked up at a later date.
PF
PF/SH
Enc 03ii
Page 13 of 14
Members of the Committee received and noted the Report.
2012.226 Effectiveness Report BM gave a brief overview of the Effectiveness Report to the Committee highlighting that the Effectiveness Group has approved the terms of reference for the Trust’s Mortality Group. The Committee requested that DW provide assurance at the next Committee regarding the Mortality Review at the Trust. SF noted that the Chart 2 on page 17 of 19 of the Effectiveness report is now outdated. This needs to include performance indicators the provide assurance that a schedule of visits to third party providers by JCU risk stratifies those providers where there are concerns. BM and SF will action this at the Performance, Finance and Quality sub-group of the PARG, and report back to this Committee for ratification and assurance. Members of the Committee received and noted the Report.
DW
SF/BM
2012.227 CQUINs BM advised the Committee that the CQUIN report circulated with the papers outlines the quarter 3 update for 2012/13 and the 2013/14 planning process. She asked the Committee to note that the Trust has submitted the Quarter 3 milestones to the Commissioners and these have been agreed as fully compliant. The process for the 2013/14 schemes is taking place and are being set jointly with CCGs. BM expressed concerns with the progress made to date. SF requested that the Associate Director of Business Development and Planning and herself be included in the review process. JS requested that this also involve clinical leads to provide examples. Members of the Committee received and noted the Report and acknowledged the Quarter 3 submission compliance.
2012.228 Professional Forum The Committee was informed that the report circulated with the papers was for information and to agree the Terms of Reference The Committee received and noted the report and approved the Terms of Reference.
2012.229 New items for the Risk Register • CQUINs • JCU Monitoring from PARG
2012.230 Any Other Business The Committee was reminded of the action from Trust Board that all members complete Quality Governance Committee self-assessment questionnaire in preparation for the development of an action plan to address any developmental needs of the Committee. The Committee was asked to ensure that the questionnaire is completed by Wednesday 13 February; this will then enable the Chair and Lead Director for the Committee to collate the results and prepare an action plan for approval by the Committee at its March meeting. The Committee was informed that there has been reported a tenth C-Difficile against the trajectory of 11. There are no further details at present however this will
Enc 03ii
Page 14 of 14
be reported to the Committee at its next meeting. The Director of Operations reported that due to concerns that had been raised in relation to Podiatric Surgery she, the Director of Nursing and the Medical Director had agreed to suspend the service until such time as they could be assured that practices within the service were safe. PF assured the Committee that there had been discussions within the CQC and the Cluster PCT in relation to the decision to suspend the service.
2012.231 Date of next meeting Wednesday, 6 February 2013, 08:30 – 11:30 Brampton Room, 1st Floor, Morston House, The Midway, Newcastle-under-Lyme, ST5 1QG Meeting closed at 11:45
Enc 04
Page 1 of 12
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
The Board Assurance Framework (BAF), annexed to this report, has been the subject of a full review as at the end of Quarter 3. The changes are highlighted. Any gaps in controls and assurance are defined in the BAF and are the subject of review by the Lead Director and the Committee/Sub-committee assigned to relevant Strategic Goal. All Directors are required to provide assurance that they have reviewed the BAF and are actionning the control weaknesses which are assigned to their Directorates. Additional assurance as to the controls and assurances that are in place is provided by quarterly reviews by the Audit Committee with input from the Trust’s Internal Auditors RSM Tenon. KEY POINTS:
This iteration of the BAF, has been the subject of a full review as at Quarter 3, and now incorporates the recommendations of the Audit Committee in relation to SG2/1, where two additional controls gaps have been added - the limited assurance that had been received in relation to the domiciliary care audit and a control weakness that had been highlighted in relation to the closure of adult safeguarding investigations.
The Quality Impact Assessment for the CIP was approved by the Board at its meeting on the 30th January but as there is limited evidence that the Quality Impact Assessments for the CIP has yet been embedded and tested as effective, a control weakness has been added to SG2/3. This control weakness will remain in place until such time as a number of pivotal CIPs have been the subject of a CIP QIA.
Lead Directors have been recommended to address these control gaps and weaknesses. It is anticipated that these control gaps and weaknesses will have been mitigated at the next review – Quarter 4 – of the BAF.
Enc 04
Page 2 of 12
INTER DEPENDENCIES: Legal and/or Risk The BAF for 2012/13 has been aligned with the Strategic Goals of the
Partnership Trust and incorporates the principal risks and related controls for the services and business of the Trust.
Clinical Ditto
Financial Ditto
HR Ditto
Social Care Ditto
Patient & Public Involvement
N/A
Equality Impact N/A
Information exempt from Disclosure
None
Requirement for further review
A further report will be presented to the Audit Committee at its meeting on the 22nd March 2013.
RECOMMENDATIONS: The Board is recommended to:
• Note the Quarter 3 review of the BAF in the form appended to this report; • Note that the Quarter 3 review of the BAF will be presented to the next meeting of the Audit
Committee; and • Receive assurance that the Audit Committee will undertake a further review at its meeting
on 22 March 2013.
Enc 04
Page 3 of 12
Staffordshire and Stoke on Trent Partnership NHS Trust – Board Assurance Framework 2012/13 – Quarter 3 Strategic Goal 2 - We will provide high quality and safe services which provide an excellent experience and best possible outcomes
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG2/1
Our services fail to be of a consistently high and improving quality resulting in patients suffering harm or otherwise having a poor experience when using health & social care services.
Infection Control teams Patient Safety initiatives RCA and Executive Officer Review Panels undertaken for all cases of MRSA Trust wide Zero Tolerance Action plan aligned with training and development of staff. Pressure Ulcer RCA Review Panels. Documentation Audits Quality Framework Action Plans
Care Quality Commission CQC Quality and Risk Profiles (QRP) Internal Audit External Audit Clinical Audit NHS Litigation Authority Royal Colleges LINks National Patient Safety Agency (NPSA)
CQC Registration without conditions all services - health services and social care. (P) All CQC inspections - announced and unannounced completed with positive assurance that the Trust is meeting all essential standards of quality & safety. Minor concerns incorporated into action plans; tracked by the Director of Nursing & Quality with Board assurance being secured through reporting to the Quality Governance Committee and the Board (P) Patient Safety - Increased incident reporting and achievement of the Safety Thermometer degree of harm target (P)
QRP is building up intelligence on the organisation (A). Guidance disseminated to all staff to prepare them for CQC inspections (A) CQC’s Quality and Risk Profiles (A) Action plans and recommendations completed on time(A) Programme of structured quality visits in place supported by Non-Executive Director representation (A)
Revised Clinical Audit Programme agreed. Training of NEDs in relation to Quality Visits.
CR3, CR4, CR5, CR6
Enc 04
Page 4 of 12
PALs real time patient feedback/ community hospital discharge survey. Monitoring and reporting of adverse incidents reports, complaints and compliment. Triangulation of Adult Protection referrals and incidents reported by social care staff – residential care placements. Health Assure system modules for CQC registration, hygiene code and NHS LA Risk Management Standards. Patient Experience Lead
Patient survey results Quality Governance Reports Action monitoring reports Health Assure system reports PEAT results
Positive Net promoter score (P) Patient Experience – delay in closure of complaints, increased complexity of complaints and lack of assurance in relation to investigations relating to social care complaints ; N Health Assure reports on CQC registration , hygiene code and NHS LA Risk Management Standards – NHSLA Level 1 confirmed by NHSLA (P) Annual Patient Survey /real time patient experience data from system
Limited assurance in relation to the investigation of social care complaints(C) Executive Director assigned to complex complaints to review and audit process and provide assurance (A) Risk Management Strategy implemented(A) Executive Risk Management Committee established (A) Review and revision of all risk related policies and implementation of single set of policies aligned to the NHSLA Community Trusts Risk Management Standards – capacity(C) Lack of evidence that risk management embedded at an operational level.(C)
Review of Complaints Process. Weekly performance reports to the Executive Management Team. Review of SLA and performance framework with SCC. NHSLA Action Plan approved by Board and QGC – compliance tracked through Corporate Governance Officer and QGC RSM Tenon undertaking audit with outcomes and actions to be reported to Audit Committee.
Enc 04
Page 5 of 12
Deep Cleaning Programme of Community Hospitals
Director of Nursing & Quality & Director of Operations
Safety walks & Quality Visits. Positive Outcome of Audit of Deep Cleaning Programme (P) Limited Assurance in relation to the effectiveness of contract management and performance – Domiciliary Care; N Limited Assurance received in relation to the systematic review and closure of adult safeguarding incidents; N
Undertake additional audits of programme and training of staff (A). Recommended actions tracked through Audit Committee & QGC with re-test / review by SCC Internal Auditors (A). Recommended actions tracked through Audit Committee & QGC with re-test / review by SCC Internal Auditors (A)
Reviewed by EMT and reported to QGC. Unannounced audit to be undertaken in Q4 Reports by Director of Operations to Audit Committee & QGC.
Strategic Goal 2 - We will provide high quality and safe services which provide an excellent experience and best possible outcomes
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG2/2
The Trust fails to achieve Foundation Trust by 2014 due to inflexibility of licensing regime and the Trust’s status as an Integrated Care Provider.
FT Programme led by the Deputy Chief Executive. FT Project Board led by the Vice-Chair of the Trust tracks delivery of milestones for the
CQC Quality and Risk Profiles. CQC reports/inspection results. Tripartite agreement with SHA/DH.
CQC Registration without conditions and positive outcome from 4 inspections (P) Milestones achieved (P)
Health Economy partnerships strengthened (A). Board development programme delivered (A).
Achievement of service performance objectives/targets Build robust evidence
CR31
Enc 04
Page 6 of 12
FT trajectory with related reports to the Trust Board External support engaged to confirm and challenge assumptions that underpin the IBP, Quality Governance Framework and BGAF. Membership & Engagement Manager reviews membership targets
FT Project Board SOM Returns to SHA Monitor Quality Governance Framework self-assessment. Internal Audit External Audit
Uncertainty as to licensing regime for SSOTP; N Membership numbers – patient, staff and public not on target ; N
IBP approved by Board(A) Integrated Action Plan with identified Executive Leads tracks actions for BGAF; LTFM;IBP and QGF(A) IS Strategy approved by the Board(A) Data Confidence Scoring implemented and reported to FIP & Board (A) Membership numbers tracked weekly with reports from Membership & Engagement Manager to Deputy CEO.
database to support application Engage with Monitor and active engagement with similar Trusts through FTN and leaders at DH/NTDA. Data Quality Group. Membership strategy approved and external support sourced to drive up membership numbers.
Enc 04
Page 7 of 12
Strategic Goal 2 - We will provide high quality and safe services which provide an excellent experience and best possible outcomes –related - Strategic Goal 5 – We will make excellent use of our resources and improve efficiency across our services
Lead Director: Director of Finance & Resources & Deputy Chief Executive
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG2/3
We fail to deliver the CIP 2012/13 and to deliver the CIP for 2013/2017 in a sustainable manner.
CIP incorporated into the Transformation Programme under the leadership of the Deputy Chief Executive Transformation Board established chaired by the CEO reporting to FIP
Performance Reports to FIP and Board External Audit External Support sourced to scrutinise CIP Action monitoring reports
Improved trajectory for achievement of CIP 2012/13 P) Divisional Performance reports and Monthly Finance Reports report CIP for North Division not on course to meet delivery of their milestones N External Support identifies optimal process and route (with confidence rating) for new and existing schemes P) CIP Quality Impact Assessment Process designed and to be implemented once approved by FIP & Board,
Evidence bank of improved trajectory so as to secure CIP - (C) Revised trajectory for CIP and performance management of same(A) New schemes reviewed by CIP Manager (A) Delay in implementation of CIP QIA and limited evidence of its effectiveness as a model for QIA (C).
CIP Manager appointed and action plans being implemented to secure delivery. Implementation and effectiveness to be tracked through FIP & QGC.
CR4, 11
Enc 04
Page 8 of 12
Strategic Goal 2 - We will provide high quality and safe services which provide an excellent experience and best possible outcomes
CQC outcomes: Outcome 4 Care and Welfare of People Who Use Our Services Outcome 6 (Cooperating with other providers)
Risk Ref
What is the risk? How are we managing the risk?
Where can we get assurance from?
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG2/4
We do not have sufficient capacity nor capability to manage the demands of demographics and related acuity inherent in the Local Health Economy
Engagement Plan with key stakeholders and CCGs Development of the Capacity Hub to manage Winter Pressures Participant in Commissioning Board and CLEG forum Impact assessment completed on all service change Implementation of Care Plans and Locality Integrated Teams Transformation Programme Management of demand risk under the MTFS for the Integration
Positive feedback and support of CCGs LINks Local Authority Improved ASCOF reporting CQRMs CQUIN
Fail to achieve Care Plan targets N Initial agreement of the CCGs to variation of targets through CQUINs so as to secure funding over next 2 years P) Demographics modelled and acuity mapped linked to Transformation Programme and implementation of 28 Locality Teams to be aligned with Workforce Strategy P) Additional investment in domiciliary care agreed with SCC P) Limited assurance as to the quality of providers and contract monitoring of the Third Party Contracts – evidenced in Limited Assurance Report to Audit Committee, N
Agreement to vary Care Plan target achieved(A) Early engagement in proposals for the development of integrated commissioning of health & social care(A) Insufficient capacity in the Domiciliary Care marketplace to manage demand and greater acuity (C). Actions tracked by Audit Committee & QGC (P).
Working with the CCGs and GPs to agree to more realistic targets tracked through CQUIN. Development of Integrated Teams enabling more agile working and greater productivity Operational participation in the Dom Care Task & Finish Group to redesign capacity.
CR4/9
Enc 04
Page 9 of 12
Procurement & Contracts Group of PARG reviewing contract monitoring and Performance Framework.
Strategic Goal 3 - Our organisation will develop and deliver sustainable innovative services that support independence – related - Strategic Goal 2 - We will provide high quality and safe services which provide an excellent experience and best possible outcomes
Lead Director: Director of Operations / Director of Nursing & Quality
Managing Committee/Board Sub-Committee: F IP Committee/ Quality Governance / Exec Group & PARG
CQC outcomes: Outcome 4 Care and Welfare of People Who Use Our Services; Outcome 16 Assessing and Monitoring the Quality of Service Provision, Outcome 21 Records
Risk Ref
What is the risk? How are we managing the risk?
Where can we get assurance from?
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG3/1
The implementation of Integrated Teams is delayed and/or fails to deliver the required changes to service delivery.
Portfolio of Director of Operations redesigned to include Health & Social Care (post-Integration) Transformation Programme Board Organisational Development Strategy and Implementation Plan in place
Integrated Performance Reports ASCOF Specialist Indicator Reports – Personalisation Internal Audit External Audit Organisational Development Progress Reports Customer and Patient Experience Surveys Professional
Specialist Indicator Reports demonstrate improvements in personalisation (P) Transformation Programme Board Delivery Plan and Risk Log reported to Board and actions and milestones tracked by the PMO (P) Recognition of significant cultural change in the workforce to achieve single line management for integrated teams. P)
Systems are able to deliver integrated performance reports to the level of granularity which demonstrates improved patient/customer outcomes (C) Mapping of risk and regulatory / professional assurance so as to deliver integrated teams (C) Workforce Strategy will be
Revised IS Strategy prioritises work plans and programmes. Review by Professional Leads. Development of 28 Integrated Team Locality plans
CR13,24
Enc 04
Page 10 of 12
accreditation schemes
underpinned by workforce plans for each Team mapped to the demography of the Locality(A)
Strategic Goal 4 - Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
Director Lead: Director of Workforce and Development
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG4/1
We fail to develop and empower our workforce in a way that is consistent with our values
Robust Appraisal System and personal development plans in place for all staff aligned to organisational values. Workforce Development Strategy Training and CPD programmes in place for all staff groups. Costed Annual Training Plan in place which addresses statutory & mandatory training & identifies areas for skills development, including Social Care staff. Emotional Intelligence testing to be implemented Organisational Development Plan
Professional accreditation schemes Quarterly Workforce reports to the Board Staff survey results/reports Workforce Strategy Implementation Plan Reports to Quality Governance Committee Patient Complaints System Incident Reports Single Equality Scheme
Staffing establishment recommendations following the acuity review adopted (P) Constructive working with JSP(P) Quarterly Workforce Report gives assurance that statutory & mandatory training is taking place. (P) Annual CQC Staff survey report benchmarks us against other similar organisations and identifies areas for improvement. (P) NHS Equality Delivery System Action Plan in place with regular progress reports to the Board. (P)
Community Nursing Review by CCGs (North) may not deliver additional investment to meet capacity and acuity demands(C) Hospital Change Programme mapped within the overall Transformation Programme – milestones reported to the Board (A) Management of significant change programme for staff(C)
Active engagement with CCGs and Director of Nursing at the Cluster PCT. Outcomes of the consultation to be incorporated in the revised Delivery Plan
CR2,12
Enc 04
Page 11 of 12
Compliance with Equalities Act 2010 and NHS Equality Delivery System. Equality & Inclusion Strategy and Equality Objectives and Plan 2012/13 approved Policies on Whistle blowing and Dignity & Respect at Work in place – being reviewed in the light of good practice. Staff survey results
NHS Equality Delivery System Action Plan Whistle Blowing Hotline
Complaints & Incident System identifies gaps in staff skills and attitudes. (P) Whistle blowing & Dignity and Respect at Work Policies provide protection for staff to raise concerns within the workplace. (P)
HR Director receives outcomes of investigations into complaints concerning staff attitude (A) EMT reviews all complaints and assigns a Lead Director to those relating to staff attitude and behaviour to ensure rigour in process (A). Consultation with employees, service users and the wider public on the proposed actions to deliver the Strategy.
Performance reports on complaints reported weekly to EMT. Review of organisational values and consultation with staff with the outcomes of Staff Engagement events to be mapped into the revised organisational values for report to Board Jan.2013.
Enc 04
Page 12 of 12
Strategic Goal 5 - We will make excellent use of our resources and improve levels of efficiency across our services
Lead Director: Director of Finance and Resources
Managing Committee/Board Sub-Committee: Finance, Investment and Performance Committee
CQC outcomes: Outcome 4 Care and Welfare of People Who Use Our Services; Outcome 16 Assessing and Monitoring the Quality of Service Provision, Outcome 21 Records
Risk Ref
What is the risk? How are we managing the risk?
Where can we get assurance from?
What assurance have we got and what does it tell us?
What else do we need?
What are we doing about it?
Link to Corporate Risk Register
Principal risk Key controls Potential sources of assurance
Assurance position (P – positive; N – negative)
Gaps in control (C)/assurance (A)
Action plans
SG5/1
The ICT infrastructure and clinical systems do not support integrated teams.
Implementation of IS Strategy Leadership within the wider LHE review of ICT infrastructure and clinical systems Implementation of Care Director to replace legacy social care systems
Internal Audit External Audit Performance Monitoring of SLA with Providers Financial and Performance reports Action monitoring reports SOM Returns to SHA
Green rating for “data completeness – SOM December 2012. (P) HISS assessment has concluded that the Trust does not currently have information systems that would enable the capture of data in the Community Information Data Set (CIDS) electronically due to limitations within the systems. /N) Care Director on track for “go live” June 2013. (P) Delays in the implementation of Health Assure limits reporting against CQC outcomes/N)
Appointment of CIO (A) CIDs mandated for capture in 2014 – a key area for development.
Develop use of Health Assure To be captured in the revised IS Strategy for reference to the Board in Q3 Data completeness indicator developed within Integrated Performance Reports – November 2012 Revised training programme and ongoing management of legacy systems
CR4, 6, 8
Enclosure:Subject:
Strategic Goal:
Director Lead:Recommendation: For Approval &
AssuranceFor Discussion X For Information
PURPOSE OF THE REPORT:
KEY POINTS:
INTERDEPENDENCIES:Legal and/or Risk
Clinical
Financial
HR
Social CarePatient & Public InvolvementEquality ImpactInformation exempt from DisclosureRequirement for further review
Jonathan Tringham
The purpose of this report is to present to the Trust Board the Trust’s financial performance to the end of January 2013.
The Trust is reporting an actual surplus of £1.205m for the ten months to 31st January 2013 which represents an under performance against plan of £0.754m. The Trust is still forecasting that it will achieve the required surplus of £2m. The Board should however note that the level of financial flexibility available to the Trust has been greatly reduced and there is therefore a higher degree of risk in achieving the planned surplus.
TO BE HELD ON: 27 FEBRUARY 2013
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
07Finance Report for the Period Ending 31 January 20135 - We will make excellent use of our resources and improve levels of efficiency across our services.
Staffordshire and Stoke on Trent Partnership NHS Trust must as a minimum break even at the end of the financial year 2012/13. For the current year the Trust is planning a £2m surplus which will demonstrate that it can operate as a financially viable and sustainable organisation.
Achievement of the forecast surplus and delivery of Quality, Innovation and Productivity and Prevention schemes/Cost Improvement Programmes are essential to reflect good financial management and economic, efficient and effective use of resources to achieve value for money.
Failure to deliver within budget will result in deterioration in the Trust’s financial position.There is an on-going training programme for budget holders within the divisions which is currently being reviewed to ensure all budget holders receive appropriate training.
This report covers financial performance for the whole Trust.
RECOMMENDATIONS:The Board is asked to note the financial performance for the period and the increased risk associated with the forecast position.
ENC 07
EBITDA
CIP Delivery
>5% favourable variance Up to 5% favourable variance On target Up to 5% adverse variance >5% adverse variance
FINANCIAL RISK RATINGSURPLUS •• The Trust has delivered a retained suplus of
£1.205m, which is £0.754m behind plan.•
CIPCASH
This is £4m higher than plan primarily due to:
- Payments yet to be agreed for overperformance against the UHNS contract.
- Invoices have yet to be received from the Staffordshire PCTs for Operating Lease charges for the financial year.
•• The Trust continues to score a 3 for liquidity as
per the financial risk rating.
This is 1.0m behind the SHA plan (£6.4m/2.1%)
Actual vs PlanForecast vs
Plan
EBITDA
Surplus
Risk Rating
Cash
POSITION OVERVIEW
•
•
- The above are offset by a debtor balance of £2.5m with South Staffordshire PCT.
•
Guidance has recently been issued by the Department of Health confirming that Property will not transfer to the Trust until 1st April 2013. This is contrary to the reporting methodology previously agreed with the SHA and will adversly affect the EBITDA achieved percentage referred to above.
The Trust's EBITDA for the ten months ending 31 January 2013 was £5.4m (1.8%). This is an adjusted figure taking into account the expected in year property transfers.
This is primarily due to slippage in the delivery of CIP and increased investment in capacity necessary to meet the growing pressures on community services.
• Overall, the Trust had a cash balance of £32.3m at the end of January.
•
The Trust has spent £6.084m on temporary staff at the end of Month 10. Expenditure on Agency staff was £4.261m (£2.212m in the Northern Division, £0.162m in the South, £0.411m in Social Care and £1.446m in Corporate Services.)
AGENCY EXPENDITURE
•
The Trust's financial risk rating for the year to date is scored at a 3, which is in line with the target set out in the Annual Plan. This is subject to change based on the proposed revised accounting treatment of property assets referred to above.
The Trust has a savings target of £16.9m for 12/13
•
The Northern Division forecast shortfall is £488k, which is 10% of its full year target, however there are plans to assign a further £250k to this shortfall in month 11. The Southern Division forecast is to over-achieve against its target by £198k, with plans to assign £40k of pay savings to CIP in month 11. The month 11 additions will result in the Trust delivering its full year target.
ENC 07
Year to 31 Jan 13
Rating Weight Weighted Score
Target 2.1% 2 25% 0.5
Actual 1.8% 2 25% 0.5
Target 100% 5 10% 0.5
Actual 85% 4 10% 0.4
Target 15.5% 5 20% 1
Actual 10.0% 5 20% 1
Target 0.6% 2 20% 0.4
Actual 0.4% 2 20% 0.4
Target 12 3 25% 0.75
Actual 16 3 25% 0.75
Target 3.15
Actual 3.05
M8 M9 M10
ADDITIONAL RISK INDICATORS
•
• •
>5%
•
•
Higher Score
Lower Score
METRIC
EBITDA Margin
EBITDA Achieved
Net Return After Financing
I&E Surplus Margin
Risk Rating to 31 January 2013
Liquidity Ratio
As at month 10, the Trust was compliant with 8 of the 10 additional risk indicators.
Risk Indicator
Debtors > 90 days past due account for more than 5% of total debtor balances
Creditors > 90 days past due account for more than 5% of total creditor balances
These indicators give an indication of whether there are financial risks within the Trust. They do not have a bearing on the formal risk rating score. These are reported in the table opposite on an exception basis.
Outstanding debtors are higher than best practice. The reason for this is there are a number of invoices with other NHS organisations outstanding. Specific issues have been escalated by the Director of Finance with the relevant commissioning organisations.
•
100 <85
n/a <3%
As with debtors, outstanding creditors are higher than best practice. This is due to a number of disputed invoices with other NHS organisations, notably University Hospitals North Staffordshire and North Staffordshire Combined Health Care. Once SLAs have been agreed these invoices will be paid. We are working with the relevant other organisations to enable us to seek to achieve the 5% target by the year end.
The score of 3.05 is slightly behind the plan of 3.15. This is because the Trust has achieved 85% of its EBITDA target, which gives a score of 4 for that metric. All other scores remain in line with plan.
RISK RATING
The Financial Accounts team are working with Shared Services and Procurement to implement a number of changes to processes. Additionally the finance team are commencing a budget holder training programme in which these items will be covered. These measures should ensure the Trust achieves the 2 risk indicators it currently is not compliant with by the end of the financial year.
>25 <15
>1% <-2%
>1%
ENC 07
Plan Variance Plan Forecast Variance
- Health 171.6 1.8 208.0 207.8 (0.2)
- Adult Social Care 128.2 (1.6) 152.0 152.9 0.9
6.2 (0.0) 7.0 7.3 0.3
306.0 0.2 367.0 367.9 0.9
(139.1) 1.8 (163.9) (164.6) (0.7)
(164.1) (2.9) (199.8) (200.4) (0.6)
(303.2) (1.1) (363.7) (365.0) (1.3)
2.8 (0.8) 3.3 2.9 (0.4)
0.9% -0.3% 0.9% 0.8% -0.1%
(0.8) 0.1 (1.0) (1.0) 0.0
0.1 (0.1) 0.0 0.1 0.1
(0.2) 0.2 (0.3) 0.0 0.3
1.9 (0.7) 2.0 2.0 0.0
0.6% -0.2% 0.6% 0.5% 0.0%
INCOME EXPENDITURE• •
Year to date
Depreciation
Full year
£m
Activity Income
Other Income
Operating Income
Pay Expenditure
Non-Pay Expenditure
Operating Expenditure
EBITDA
EBITDA %
(137.3)
173.4
126.6
STATEMENT OF COMPREHENSIVE INCOME TO 31 JANUARY 2013
1.2
0.4%
Actual
(304.3)
2.0
0.6%
(0.8)
0.0
0.0
Interest Received
Dividend
Health budgets are under pressure due to the level of agency support to the Northern Division community hospitals. Furthermore increased throughput on inpatient wards and the services received from UHNS have cost more than was originally anticipated. Some costs are supported by variable income arrangements, however concerns remain over whether the actual income is enough to support current clinical practices.
Retained Surplus
I&E Surplus %
6.2
306.2
The total planned annual income for the Trust at the end of January 2013 was £367m. This has increased by £1.2m from month 9, predominantly relating to Social Care income streams. Other increases relate to cost and volume activity over performance.
(167.0)
ENC 07
EBITDA STATEMENT OF FINANCIAL POSITION• SUMMARY
•
• •
SURPLUS CASH• •
•
FORECAST SUMMARY•
DEBTORS AND CREDITORS•
•
•
Nov-12 Dec-12 Jan-13 Nov-12 Dec-12 Jan-13
1.2 1.6 1.65 2.1 2.5 1.8
0.38 0.36 0.15 0.27 0.4 0.28
4.6 4.4 4.55 1.8 7.2 3.91.4 1.98 1.9 0.8 1.1 1
5.8 6 6.2 3.9 9.7 5.81.78 2.3 2.1 1.1 1.5 1.3
31% 38% 33% 27% 15% 22%
0.1 0.1 0.1Provision to cover this debt
AGED DEBTORS AGED CREDITORS£m
Non-NHS Debtors
Of which >90 days overdueNHS DebtorsOf which >90 days overdueTotal Debtors
£m
Non-NHS Creditors
>90 days overdue as % of total
>90 days overdue as % of total
Of which >90 days overdue
Total CreditorsOf which >90 days overdue
The EBITDA Achieved target for the period is 5 (100%). The Trust has achieved a rating of 4 (85%).
The Trust has a target to achieve a surplus of £2m at the end of the financial year.
Planned surplus at M10 was £1.959m against which the Trust has achieved £1.205m.
Net assets as at the end M10 are £13.1m.The Trust has achieved it's target EBITDA margin of 2 for the period.
Property assets continue to remain on PCT balance sheets and are forecast to come onto the Trust balance sheet on 1st April 2013.
At 31 January 13 the Trust had £32.3m of cash, £4m higher than plan primarily due to:
Debtors over 90 are significantly above the 5% target. This continues to relate to a small number of debtors with issues having been escalated by the Director of Finance.
Of which >90 days overdue
- The above are offset by a debtor balance of £2.5m with South Staffordshire PCT.
The value of debt >90 days old remains constant at circa £1m but given the decrease in overall Creditor level to circa £5m the % > 90 days old has increased from 15% to 22%.
The constant £1m of creditors >90 days old relate to 3 NHS suppliers with disputes currently being progressed to be resolved before the end of the financial year.
NHS Creditors
- Invoices have yet to be received from the Staffordshire PCTs for Operating Lease charges for the financial year.
The annual plan for the Trust is the achievement of a surplus of £2m which continues to be forecast at the month 10. Given the shortfall against plan to date the £2m surplus remains challenging. The Trust is engaged with its Commissioners to secure income for additional activity, however there remain a number of outstanding items being debated, which could result in considerable gains and losses to the Trust.Included within the forecast position is the shortfall of £290k identified within the CIP plans, noting that this shortfall will be delivered during month 11. All known risks have been identified and have been discussed with COOs to assess the likelihood of occurrence, noting the high number of disputes with commissioners which are yet to reach a resolution.
•
- Payments yet to be agreed for overperformance against the UHNS contract.
Of which >90 days overdue
ENC 07
As at 31 January 2013
Actual Forecast Variance
7.2 7.4 (0.2)
0.2 0.3 (0.1)
7.4 7.7 (0.3)
1.7 1.7 0.0
13.6 5.0 8.6
32.3 28.0 4.3
47.6 34.7 12.9
(41.7) (28.6) (13.1)
(0.1) 0.0 (0.1)
(41.8) (28.6) (13.2)
0.0
(0.1) 0.0 (0.1)
(0.1) 0.0 (0.1)
13.1 13.8 (0.7)
0.0 0.0 0.0
0.0 0.0 0.013.1 12.6 0.5
13.1 13.8 (0.7)
Plan YTD Variance
960 180 (780)
0 393 393
960 573 (387)
CAPITAL PROGRAMME
•
£k
Equipment
IT projects
Total
£m
Current Liabilities
Creditors (>1yr)
Provisions (>1yr)
Land, Buildings and Equipment
Trade and other receivables (>1yr)
Non-Current Assets
Inventories
Trade and other receivables (<1yr)
Cash and Cash Equivalents
STATEMENT OF FINANCIAL POSITION
CAPITAL PROGRAMME
The Capital Resource Limit for 2012/13 is £960k which was set by reference to the forecast depreciation charge for the equipment assets.
Stoke, North Staffordshire and South Staffordshire PCTs continue to hold the capital resource applicable to the building assets. The Trust has full input into the commitment of this resource to ensure it aligns with the Trust's objectives ahead of the buildings transferring on 31 March 2013.
•
• The development of the capital plan has allowed eight schemes to get under way. Three of these are IT related projects. Expenditure at 31 January was £573k.
Non-Current Liabilities
Net Assets
Public Dividend Capital
Revaluation Reserve
Income & Expenditure Reserve
Total Taxpayers' Equity
Current Assets
Creditors (<1yr)
Provisions (<1yr)
ENC 07
• • Within the Southern Division there are a number of risks, all of which are associated with the income contracts and hence are subject to commissioner agreement or escalation:- £150k of income relating to continence products has been assumed.- £405k of income relating to escort and bed watch activity has been assumed, and appears likely that payment will be received.- High cost drug income has been accrued totalling £718k. This is a major risk to the position and is strongly disputed by commissioners.- CIP delivery of £84k assumed relating to occupancy at QHB.
NORTHERN DIVISION
• • The Division’s non pay budgets are £2.7m overspent as at the end of January - £1.2m of which relates to the UHNS SLA. Community hospitals are £901k overspent, including the pharmacy element of the UHNS contract. Other hospitals overspends relate to the increased throughput of patients on the wards. The over spend on heath centre property costs is £433k as a consequence of increased utility costs and rental charges.
•
• Year to date divisional income is over performing by £213k which mainly relates to additional training income to support the training of student health visitors.
RISKS AND OPPORTUNITIESWithin the Northern Division the following opportunities are noted:- The forecast includes a continuation of the UHNS recharges at the highest point in the year. With a focus on clinical practices there is a potential opportunity to reduce this cost over the coming two months. There has been a slight reduction in charges between month 7 and month 10. - There is ongoing negotiation regarding whether commissioners will fund the in-year cost of the new medical model covering community hospitals. This may result in additional income. There are also a number of other commissioning discussions which should result in further income receipts that have not been forecast in the Divisional position.
OPERATIONAL PERFORMANCE
The Division’s financial position has deteriorated from Month 9 to Month 10 in line with the full year forecast. The overspend stands at £2.7m – a shift of £666k. In addition to the continuing trend of over spends against the community hospitals and over performance on the UHNS SLA, there has been a reduction in income relating to the Shropshire PCT SLA, which was set at a lower value than the internal budget allocation. It is in effect a nil impact against the organisational position, with the opposite entry sitting against the corporate income codes.
The pay budget is underspent by £132k at the end of Month 10. This is a £105k improvement compared with month 9, the benefit being the result of further slippage on vacant posts. Within this overall position however, the vacancy savings offset a considerable level of bank and agency use. The Division has spent a total of £3.2m on temporary staff at the end of Month 10.
ENC 07
SOUTHERN DIVISION CORPORATE
• The Southern Division is currently £131k overspent. This adverse month on month movement of £306k is largely due to a reduction in GUM cost and volume income which had been assumed in the position. As there is an on-going debate regarding the value of funding within the original block contract, on the basis of prudence, all cost and volume income has been removed for reporting purposes. The debate with commissioners has however not yet reached a conclusion.
• The Corporate budgets are £1,465k underspent for the year to date compared to an under spend of £701k at Month 9. A transfer between the Corporate and Social Care Divisions led to an improvement of the Corporate position by £916k which was further improved by additional traning income of c£100k but then offset by a £155k overspend against IT contracts, £136k of previously unidentified transformation expenditure and othet minor variances.
• ADULT SOCIAL CARE
• The Month 10 financial position for Adult Social Care (ASC) shows a marginal surplus of £38k against the plan, an improvement over month 9.
• There remains some outstanding issues for resolution with regard to addressing risks around modernisation savings targets and expenditure pressures, which will hopefully be brought to a pragmatic and reasonable conclusion shortly. The reported financial position adopts a fairly prudent judgement with regard to the outcome of the remaining negotiations.
Pay expenditure is below its budget levels by £407k largely as a result of vacancies. Costs in the month are £4.37m and have seen an increase compared to previous months of £153k. This relates to recruitment within the Early Supported Discharge service and single point of access service. Bank and agency costs cost in the month are of £117k which has seen an increase of £18k compared to costs in December of £99k.
Increase/(Decrease) in Movement in non Cash ProvisionsNet Cash Inflow/(Outflow) from Operating ActivitiesInterest Received
(Payments) for Property, Plant & Equipment
Net Cash Inflow/(Outflow) from investing ActivitiesNet Increase/(Decrease) in Cash and Cash Equivalents
Opening Cash & Cash Equivalents balance
Dividend (Paid)/Refunded
APPENDIX 2: ROLLING 12 MONTH CASH FLOW FORECAST
£'000s
Operating Surplus/(Deficit)
Depreciation
Enc 08
Page 1 of 12
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 08
Subject: Integrated Performance Report – February 2013 (Month 10 - January data)
Strategic Goal: All
Director Lead: Jonathan Tringham
Recommendation: For Approval & Assurance x For Discussion For Information
PURPOSE OF THE REPORT:
The purpose of this report is to provide Members of the Trust Board with an integrated view of performance across the Partnership Trust for April – January 2012/13. Annex 1 includes the executive summary of performance including an overview of actions being taken for ‘core’ indicators. The ‘core’ indicators have been identified in consultation with Trust leads on the basis of current strategic importance. Annex 2 details performance against the full suite of Board indicators including direction of travel. Where a ‘core’ is rated red, a reference is included to the section of the main report which identifies whether a formal action plan is in place and provides an overview of actions being taken to remedy performance. Action plans for other under-performing indicators are managed at a Divisional level and are coordinated by the Performance team. The full suite of board indicators is regularly reviewed in consultation with the Trust Board to reflect changes in national and local priorities. The format and content of the report has been developed in consultation with the Executive Team and Finance, Investment & Performance Committee (FIP). The format of this report will continue to be developed to incorporate feedback from both Board and FIP Committee. KEY POINTS: Updates to the report Following feedback from Trust Board the following changes to the report are being: • In the absence of an overall shadow ‘quality’ rating in the Standard Operating Model (SOM)
return to the Strategic Health Authority (SHA), FIP Committee requested a scheme be developed to provide internal assurance for quality indicators. The approach of identifying and weighting key quality indicators is intended to mirror the contract, governance and finance shadow risk ratings contained in the SOM return. Both FIP and Quality Governance
Enc 08
Page 2 of 12
Committees have now considered the options for a new rating system, and the preferred model will be in-place for the March Integrated Performance Report.
• Refreshed benchmarking data has now been released from the ACFT Benchmarking Group
(based on data submitted for December 2012). Where appropriate, benchmarking information has been referenced in the report. It should be noted however that concerns have been raised around the consistent interpretation of methodology and reporting of information by participants, therefore this data should be treated as a high level guide only.
INTER DEPENDENCIES:
Legal and/or Risk The performance information included in the attached report is dependent on the quality of the source data which is taken from a number of information systems. If this data is not of good quality there is a risk that decisions could be made based on flawed performance information, and a risk of adverse audit judgements.
Clinical It is essential that the performance scorecard continues to include clinical quality and safety related indicators to drive continuous improvement and thereby benefit all people with care and support needs across Staffordshire and Stoke-on-Trent.
Financial The financial pressures facing the Trust over the coming years necessitate the development of further ‘value for money’ indicators to include in the monthly scorecard. This will allow the organisation to retain an overall picture of the balance between the financial position and performance.
HR Managing performance outcomes is dependent on its workforce for example training, appraisal and sickness levels.
Social Care The report includes key social care performance indicators to provide Board with an integrated overview of organisational performance.
Patient & Public Involvement
The inclusion of service user feedback in performance reporting is essential for Board assurance.
Equality Impact The use of good data quality to inform decision making and service delivery is key in ensuring vulnerable groups are not discriminated against in any way.
Information exempt from Disclosure
NA
Requirement for further review
Routine reports are provided to the Board, FIP Committee and Operational management meetings to update on performance issues.
RECOMMENDATIONS:
The Board notes the content of the executive summary and performance scorecard, and considers whether corrective actions and planned improvements are appropriate and sufficient.
Enc 08
Page 3 of 12
Annex 1 Executive Summary of Performance – January 2013 1. Overall Achievements – January 2013 1.1 The organisation is performing strongly overall with a number of notable achievements during month 10: 1.2 Patient insight data continues to demonstrate encouraging levels of satisfaction with the quality of services the Trust offers. The Net Promoter results are at the highest recorded level in the Trust:
Levels of customer satisfaction with the social care assessment and support planning experience remain consistent
with previous months, while 89% of clients are feeling supported to make their own decisions about their care in January, compared to 83% in quarter 3. 1.3 Following extensive focus by the Interim Community Hospitals Manager the average length of stay in community hospitals is rated green for the first time this year, with performance of 21.6 days against a target of 23 days. The current ACFT Benchmarking Group average is 25 days. 1.4 The trend for the percentage of occupied bed days being due to delayed transfers of care remains encouraging with January data showing performance of 2.5% against a contractual target of 3.5%. F,I&P committee received a detailed report on delayed transfers of care in January where the Interim Community Hospitals Manager detailed the actions which had been taken to improve this indicator. 1.5 Trust’s reablement services continue to perform strongly, demonstrating improved long term outcomes for social care clients. 84.4% of older people are now recorded as remaining at home 91 days following reablement, against a target of 86%:
Patient Experience Net Promoter Results A Net Promoter Score of + 77.67 across NHS community hospitals / services, based on a sample of almost 1400 people
The ACFT benchmarking group average score has risen significantly in January from 62.4 to 71.8. It should be noted that there is inconsistent application of the methodology across the NHS at present, with many Community Trusts reporting based solely on community hospital patients. SSOTP includes both community hospitals and community services. The national view is that a score greater than +50 is considered ‘excellent’.
Average Length of Stay
1517
1921
232527
29
April
MayJu
ne July
Augus
t
Septem
ber
Octobe
r
Novem
ber
Decem
ber
Janu
ary
Februa
ryMarc
h
Month
Alo
s (d
ays)
Av LOS Target
Enc 08
Page 4 of 12
In addition 49.4% of reablement clients needed no on-going social care services after 91 days, this is rated green against a target of 42%: 1.6 Levels of self directed support continue to exceed the 45% target set by Staffordshire County Council, with over 58% of clients with eligible ongoing services now in receipt of personal budgets and direct payments.
1.7 Core Indicator Achievements 1.8 A set of core indicators have been identified in consultation with Trust leads. These indicators are included within the scorecard (annex 2) and are denoted in the ‘Core PI’ column. The section below details the key performance messages of these indicators: 1.9 National targets for waiting times at walk-in centres / minor injury unites continue to exceed statutory requirements with all patients being seen within four hours in January. The data quality confidence score for this area is amber with a score of 75.0%. 2. Overall Issues for Consideration – January 2013 2.1 The Board is asked to consider the following issues which have been identified from January information: 2.2 The Standard Operating Model (SOM) return was rated green in all areas for the first time in the January submission (December data).
2.3 The Trust continues to achieve the consultant-led completed pathway Referral to Treatment (RTT) waiting time targets, however issues relating to incomplete pathways have been identified. Specifically a draft national return showed a number of people waiting over 52 weeks for treatment. Following a data cleansing exercise all but two cases were validated and removed. In order to comply with the 2013/14 Commissioning Board framework ‘Everyone Counts’ the Trust is adopting a zero-tolerance approach to 52 week RTT breaches – as such additional core indicators have been added to the scorecard. Section 4.2 details the steps being taken to ensure the new target is adhered to.
0
3
Contractual Green
Governance
Financial
<1 Green, 1-1.9 Amber/Green, 2-3.9 Amber/Red, >=4 Red
<3 Red, >=3 Green
Compliance with a set of contractual assessment questions
<30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
R A G
Target
42%
SSOTP
49.4%
< 70 75 80 85 90 95 100
R G
SSOTP
84.4% 86%
Target
A
Enc 08
Page 5 of 12
C.Diff 2012/13
0
2
4
6
8
10
12
April
MayJu
ne July
Augus
t
Septem
ber
Octobe
r
Novembe
r
Decembe
r
Janu
ary
Februa
ryMarc
h
Cumulative Cases Trajectory
2.4 Between April 2012 and the end of January 2013 there were 9 cases of clostridium difficile in the Trust, against an annual trajectory of 11 cases. A further 2 provisional cases have been reported in early February meaning that no further instances can occur during this financial year in order to comply with expected annual levels. Any breach of this target will also have implications for the SOM Governance Risk Rating. The Board is asked to note that the 2013/14 tolerance for C.Diff is likely to be significantly lower. Note: February data is provisional as at 18th February 2013
2.5 Sickness levels for health teams have improved from 5% in November to 4.5% in December, with an overall year to date position of 4.6%. Over the same period social care teams sickness rates have risen from 4.5% to 5.2%, with an annual performance of 3.9%. The latest ACFT Benchmarking data reports an average of 4.7% across all nine participants, indicating that achieving the 3.39% target is extremely challenging for all Community Trusts. Section 4.3 details progress with actions to reduce sickness levels. 2.6 Although the target for acknowledging complaints within three working days was met in both health and social care in January, the target of responding to all complaints within agreed timescales was not met in either area of the Trust. This target has been consistently challenging for social care, however the January data represents a noticeable decline in performance for health. Section 4.4 provides an update on actions being taken to rectify performance. 2.7 Overall financial performance for the year to date is underperforming against planned levels by £754k in January, however the Trust is forecasting that the required surplus of £2m will be achieved by year end. See Section 4.5. 2.8 Core Indicator Issues for Consideration 2.9 Levels of appraisal compliance remain below the 95% target for health teams with 88.9% performance. Social care teams are performing slightly stronger at 92.1%. Section 4.6 provides further detail. SSOTP performance does however compare favourably to the ACFT Benchmarking Group which is showing an average of 73.76% compliance.
2.10 Levels of Statutory & Mandatory Training remain consistent with previous months. NHS compliance is 74%, while Social Care is currently 71%. This performance is in line with the ACFT Benchmarking group which reports an average compliance of 74.84% - further detail is included in section 4.7. 2.11 The timeliness from a social care assessment to services being implemented continues to be challenging with 68.1% of cases being dealt with within 8 weeks, against a target of 80%. It is encouraging to note that the SSOTP component parts of this indicator are now rated green, and discussions are ongoing with Staffordshire County Council to improve the timelines of care packages being put in place, see section 4.8.
Enc 08
Page 6 of 12
2.12 Levels of smoking quitters have improved over the last month but remain slightly below trajectory levels and are currently under-performing by 7%. This equates to 207 less people quitting smoking at their 4 week follow-up appointment than planned. A detailed action plan is in place, which includes recovery trajectories - see section 4.9. 2.13 Due to the emergance of a concerning trend in waiting time performance for physiotherapy and podiatry these indicators were added to the core indicator list in January in order to bring them to the Boards attention. Although improvements are noted, performance remains below target in both areas; physiotherapy is now at 58% against a target of 90% and podiatry is performing at 71.6% aginst a target of 100%. Detailed action plans are in place, and details of the trajectory for recovery are included in sections 4.10 and 4.11. A summary of action plans to address all of these areas are contained in section 4. 3. Contract Activity Performance (Month 10)
2011/12 2012/13 To Month 10
2012/13 Target to Month 10
2012/13 Variance to Month 10
Total number of community contacts 1846016 1290604
Face to face contacts 1739547 1201746 Telephone contacts 106469 88858 New outpatient attendances 48820 68136 FU outpatient attendances 99178 135181 New to follow up outpatient ratio 2.0 2.0 Inpatient FCE's 3050 3635 Daycase 3656 3886 Number of walk in centres and minor injury clinics attendances
97583 66002 52650 13352
Outpatient activity excludes community hospital activity which transferred to Burton in June 2011. All activity excludes cancellations and DNAs. The year-end forecast is a straight projection based on month 10 data.
3.1 In the North division contracted activity levels are generally in-line with targets although there were some areas of variance during January with 67 activity lines over-performing by over 10%, and 17 activity lines underperforming by over 10%. 3.2 Many of these services are currently under block contract arrangements. With regard to PbR based activity (only applicable to rheumatology and limited number of other outpatient specialties in the North Division) there is a projected end of year over-performance against contract in the sum of £223,432 for NHS Stoke-on-Trent and £125,903 for NHS North Staffordshire patients. 3.3 A South division activity schedule has now been shared with Commissioners. The Division has now put a process in place to ensure that this is produced and reported routinely every month. Further work is being carried out to report contract activity at a service, rather than specialty, level from April 2013 onwards. 4. Summary of Action Reports
4.1 Copies of full action reports are available by emailing [email protected], and brief summaries of progress in key areas are set out below: Please note: This section includes an overview of performance issues and planned improvements for each under-performing core indicator, and identifies whether a formal action plan is in place. Action plans for other under-performing indicators are managed at a Divisional level.
4.2 Referral to Treatment: Incomplete Pathways Actions in place – Lead – Paula Furnival – Director of Operations In line with national policy the Trust has adopted a zero-tolerance approach to 52 week referral to treatment target (RTT) breaches. Additional core indicators added to the scorecard include the number of people currently waiting over 26 and 52 weeks and the overall percentage of incomplete pathways within 18 weeks. Although the overall level of incomplete pathways within 18 weeks exceeds the national target of 92% with performance of 96.6%, at the end of January there were 36 patients waiting over 26 weeks and 2 waiting over 52 weeks. Controls in place to ensure the organisation complies with this requirement from April 2013 are: Operational focus on waiting list management through local SMT’s, circulation of current waiting
lists to operational managers and details of all people waiting over 26 weeks being provided to Chief Operating Officers on a weekly basis. This enables routine validation of data to ensure the true waiting list position is reflected in national returns and local monitoring.
The development of a local Waiting List Management policy to set out the Trust’s ‘rules’ for waiting list management; this will provide clear definitions for staff to work to. The policy will sit alongside national guidance to provide consistency across the organisation, and to ensure customers have clear expectations and an equitable experience of Trust services.
The resource dedicated to waiting list management is currently being reviewed in order to ensure adequate provision of training/advice, development of policies/procedures and stringent monitoring of waiting times in order to minimise breaches of RTT targets.
The Data Quality Group will oversee delivery of the actions set out in the RSM Tenon report (which include the need to address accuracy issues in submissions, review the Trusts approach to 18 week RTT training to ensure consistent application of rules, and the need for local documented guidance).
4.3 Sickness rates Action plan in place – Lead – Julie Tanner – Director of Workforce There has been real focus on supporting sickness cases from the HR Business Partners. This includes supporting operational managers to apply absence policies in a proactive way, with a focus on returning people to the workplace. Specific actions include: Use of a tracker system which is monitored at SMT to ensure all cases are being managed
appropriately and individual coaching to Line Managers where necessary; The Staff Support and Counselling Service is now available to managers and/or individuals
Trust-wide; The Staff Physiotherapy Service is also in place with identified pathways for staff needing
secondary-level mental health care interventions. This service will be reviewed early 2013 following user feedback and analysis;
Sickness training has been rolled out across the Trust since the revised policy was introduced in April 2012 and further sessions are being set up to ensure all managers have an opportunity to attend. Additionally sickness absence management is covered in the on-going Management Development Programme.
Sickness Rates
3.00%
3.50%
4.00%
4.50%
5.00%
5.50%
April
MayJu
ne July
Augus
t
Septem
ber
Octobe
r
Novem
ber
Decem
ber
Janu
ary
Febru
aryMarc
h
NHS 11/12 NHS Social Care March 2013 target
Enc 08
Page 8 of 12
4.4 Complaints responsiveness Actions in place – Lead - Siobhan Heafield Director of Nursing & Quality Social Care: 14 formal complaints were closed in January, only 6 of which were within timescale. Of the 8 breaches, 5 were completed by the Investigating Officers (IO) but were delayed due to concerns relating to the quality of the investigations, and the remaining 3 were not concluded within timescale by the appointed IO. Health: The compliance rate of closures for January has declined from 100% to 80%. In December the Executive Management Team (EMT) stated that no further extensions to any complaint timescales should be granted unless it is deemed as an exceptional circumstance. Weekly performance reports have been submitted to EMT in January along with weekly escalations to the Chief Operating Officers. The Trust contacted a number of complainants in January to ask them to participate in a customer satisfaction survey relating to the complaints process. The survey which uses the Net Promoter model (see 1.2) showed a result of +50, indicating that customers are generally satisfied with the process. The graph below illustrates the year to date trend for complaints responsiveness: 4.5 Financial Performance against plan / Percentage of CIPs delivered Monitoring process in place – Lead – Jonathan Tringham – Director of Finance & Resources The Partnership Trust has a target to achieve a surplus of £2m at the end of the financial year. The planned surplus for the first ten months of the year is £1,959k against which the Trust has achieved a surplus of £1,205k, therefore there is a £754k shortfall against the plan at Month 10; this is shown in the graph below that also shows the trajectory over the final months of the year:
Enc 08
Page 9 of 12
A summary of the cost improvement programme (CIP) performance for month 10 by Division is shown in the table below:
The north division CIP shortfall relates entirely to the hospital services. There have been further efficiencies identified within the south division, resulting in an over-recovery at month 10. While there remains a reported shortfall in delivery as at month 10, additional schemes have been identified which will lead to full year achievement of the £16,912k target. 4.6 Staff Appraisals Action plan in place – Lead – Julie Tanner – Director of Workforce A high level action plan is in place to monitor appraisal compliance. January data shows that against a performance target of 95% social care teams are 92.1% compliant and Health teams are currently 88.9.% which is slightly lower than Decembers performance, and continues to be rated red. Actions to improve performance include:
Training sessions have been arranged for January, February and March to assist appraisers and to ensure to ensure that the timeframes set out by the Partnership Trust for completing appraisal are achieved.
Routine compliance reports are sent to departmental managers for action. The quality of appraisals is being assessed through an audit which aims to determine whether
the standards agreed with Staff-side are being met.
4.7 Statutory and Mandatory Training Action plan in place – Lead – Julie Tanner – Director of Workforce
Both NHS and social care levels of statutory and mandatory training remain an area of concern. The Trust rate of 74% for health teams and 71% for social care is in-line with the latest CFT benchmarking data available. A limited action plan is in place which needs to be further developed to include more detailed actions and a trajectory for recovery.
Social Care Health
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
74%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
71%
Social Care Health
Enc 08
Page 10 of 12
4.8 Time from referral to implementation of Social Care services (SC30) Action plan in place – Lead – Paula Furnival - Director of Operations Performance for SC30 is consistent with previous months at 68.1% against a target of 80%. East Staffs and Lichfield remain the only districts meeting the target for this indicator. Part one relates to assessments being carried out in a timely manner, while the second part of the indicator relates to the implementation of services and is shared with Staffordshire County Council (SCC) as the authority is responsible for commissioning contracts. 4.9 Smoking Quitters Action plan in place – Lead - Paula Furnival - Director of Operations The position at the end of January 2013 is showing a performance of 7% below plan. This equates to 207 less people quitting smoking at their 4 week follow-up appointment than planned, and is slightly better than the position reported last month (-9%, 241 screens below target). It should also be noted that the number of 4 week quitters who have remained quit at 12 weeks continues to show better than expected performance. This is a measure that the service being provided is effective and of a high quality, and will also lead to higher than expected tariff income. A marketing plan has been developed with the Business Team and is currently being implemented - it’s impact will be monitored through the new referral recording system. 4.10 Physiotherapy Waiting Times Action plan in place – Lead – Paula Furnival – Director of Operations There are three separate waiting time targets within the north division: Stoke teams have a 2 week target for all referrals
Enc 08
Page 11 of 12
North staffs target of 4 weeks (Adults) North staffs target of 6 weeks (Children)
Stoke teams: Performance in January was 45.6% against a target of 90% for Stoke teams. There has been a 37% increase in the number of referrals received in the period April to September 2012 compared to the referrals received during the same period in 2011 which has had an impact on performance. Recruitment has commenced in order to address this position. North Staffs teams: Performance in January significantly improved to 88.5% against a target of 90%. The service is currently investigating the number of referrals received from UHNS, including post-operative patients and referrals from the fracture clinic, which is reducing capacity to see other community patients. Commissioners have agreed that the UHNS referrals should not be seen by SSOTP physiotherapy services. This should increase capacity within the service, and reduce waiting times.
4.11 Podiatry Waiting Times Action plan in place – Lead – Paula Furnival – Director of Operations 95% of patients referred into the podiatry service should be offered an appointment within 3 weeks. In order to clear the backlog of long-waiters within community clinics, performance against target has remained fairly static for biomechanics during 2012/13 as staff prioritised the community clinic waiting lists. New staffing rotas commenced in September, this saw the percentage offered appointments within community clinics increase but waiting times for biomechanics remain short of the target. An action plan is in place to reduce the wait times for biomechanics. The service has identified the additional capacity required and are in the process of increasing staffing levels in order that additional sessions can take place.
Enc 08
Page 12 of 12
5. Key Performance Risks
5.1 The overall quality of data has remained a risk to the organisation but significant progress has been made over the last year to tackle issues relating to the flow of information through trust systems, and the completeness, timeliness and accuracy of recording. Developments noted in January include: Data Timeliness Reports are being produced and distributed to Operational Leads to improve the
efficiency of the data capture process. For example in the South division health teams data timeliness has improved from 71% to 81.5% of contacts entered within 5 working days during this financial year. This area remains challenging in the north division where there is only a 62% compliance rate at present.
A specification for a new data repository has been provided to the HIS – and a project group is leading the establishment of data flows from key Trust systems into a single data warehouse. This work will encompass a review of spreadsheet based recording with the view to moving data collection onto approved Trust programmes.
The Data Quality group have considered the results from RSM Tenon’s data quality audits of A&E and Referral to Treatment (RTT). The action areas arising from the audits have been built into the groups work programme.
The Data Quality group has agreed a rollout programme of the Data Quality Confidence Scores (currently in place for RTT and A&E waiting times).
6. Scorecard 6.1 Annex 2 includes performance scorecards for quality and safety, operations, finance, and workforce.
Strategic Objective Core PIData
Quality Score
Indicator Type Indicator Outturn
2011/12 Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Direction of Travel March 2013 Forecast
ACFT Benchmark
N Number of formal complaints received Health / Social Care 213 / 233 25 / 12 22 / 25 17 / 14 21 / 13 22 / 12 18 / 8 23 / 9 35 / 19 12 / 11 22 / 21 217/ 144
N Number of compliments received Health / Social Care
SHA Falls (resulting in severe injury or death) 4 4 4 1 3 2 2 5 4 2 31
Our Organisation will develop and deliver
sustainable, innovative services that support
independence
SC
Q18 - Quality Improvement Survey (Question 18) Proportion of people who feel they were supported to make
their own decisions about their social care and/or services?
Trajectory to achieve 85%
by March 201381% 80% 82% 83% 81% 81% 83% 83% 83% 89% 90% 95% N/A 85%
Please note unless otherwise indicated the data on this scorecard relates to the period ending 31st January 2013
Indicator Type - N - National L - Local C - Contractual SHA - Strategic Health Authority SC - Social Care
ANNEX 2: Quality & Safety - Lead Director - Siobhan Heafield - Performance Indicators - January Data
We will work with partners, users and carers
to deliver integrated services
We will provide high quality and safe services
which provide an excellent experience and best possible outcomes
Enc 09
Page 1 of 8
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST BOARD
TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 09
Subject: Response to the publication of the Mid Staffordshire NHS Foundation Trust Public Inquiry published 6 February 2013
Strategic Goal We will provide high quality and safe services which provide an excellent experience and best possible outcomes
We will work with partners, users and carers to deliver integrated services simply and effectively.
Our workforce will be empowered and supported to deliver care in a way that is consistent with our values
Director Lead: Stuart Poynor, Chief Executive Officer and Siobhan Heafield, Director of Nursing & Quality
Recommendation: For Approval & Assurance
For Discussion x For Information
PURPOSE OF THE REPORT:
This report provides the Board with a high level summary of the findings of the Public Inquiry into the failings at the Mid Staffordshire NHS Foundation Trust. The current actions being taken and planned by the Trust are also provided, along with the proposals for a more detailed response after we have had time to reflect on the findings of the Public Inquiry, its recommendations and proposals.
KEY POINTS:
The report sets out the key findings and recommendations of Robert Francis QC and identifies the essential aims of what he suggests would address the issues identified in the Inquiry. Two key recommendations are:
• All commissioning, service provision, regulatory and ancillary organisations in healthcare should consider the findings and recommendations of the report and decide how to apply them to their own work;
• Each such organisation should announce at the earliest practicable time its decision on the extent to which it accepts the recommendations and what it intends to do to implement recommendations it has accepted; and
• Then, on a regular basis at least once a year, publish in public report information regarding the progress that we have made in implementing the recommendations and any related actions.
The importance of an open, transparent and candid culture across the whole of the health system was highlighted as an important factor in the Inquiry Report and has been highlighted both in the Secretary of State’s letter to all Chairs of NHS Trusts and in Sir David Nicholson’s letter to all Chief Executives.
Enc 09
Page 2 of 8
As an organisation we have invested in some of the cultural enablers highlighted in the Report which promote a culture of openness, transparency and candour. These are set out in paragraph 5 and have invested in an independent “Raising Concerns” hotline. We now need to consider how we might best promote listening events for staff, patients, service users and carers, reflecting on the key findings of the Inquiry, and then putting in place actions which are distilled from our listening events; the implementation of which will be reported to the Board and to our Shadow Council of Governors, once elected. INTER DEPENDENCIES: Legal and/or Risk The publication of this report shifts the emphasis of the provision of poor
care from being, not only a matter of professional conduct, but also a matter for the Board by securing the implementation of recommendations relevant to the Trust and learning from the “listening events”, embedding actions into the organisational values and behavioural codes of all employees and the professional standards and Code of Conduct of the Board.
Clinical Clinical leadership will be a key enabler in delivering the required changes to address the relevant recommendations. There is an opportunity for clinical leadership to be strengthened as recommendations are implemented.
Financial There will possibly be financial resource requirements of implementing some of the recommendations. These have not been determined at this stage.
HR As well as the implications of staff failing to meet fundamental standards of care and quality, there is a significant opportunity for Trust staff to have a voice and for significant organisational development.
Social Care Where recommendations are accepted for the Trust they will be applied to all health and social care staff / services.
Patient & Public Involvement
The Francis Report provides a significant opportunity for strengthening patient and public involvement
Equality Impact The implementation of the relevant Francis Report recommendations will improve the quality of care to all groups of patients
Information exempt from Disclosure
N/A
Requirement for further review
The detailed response to the recommendations will be brought back to the Board following the Board development session and in line with the recommendation that a report is made at least once each year on the progress of the implementation of the recommendations accepted by the Trust.
RECOMMENDATIONS: The Trust Board is asked to: • Receive the key points and recommendations of the Public Inquiry; • Approve the actions being taken to commence the listening events; • Advise of any further actions with regard to listening events; and • Agree that a Board development session is dedicated to the consideration of the
recommendations of the report.
Enc 09
Page 3 of 8
Response to the publication of the Mid Staffordshire NHS Foundation Trust Public Inquiry published 6 February 2013 1.0 Introduction
1.1 During 2007, the then Healthcare Commission (HCC), now the Care Quality commission
(CQC) became aware of concerns relating to higher than expected mortality rates at Mid Staffordshire NHS Foundation Trust. The Healthcare Commission Annual Health Check 2007/08 assessed the organisation as being ‘Fair’ for Quality of Services and ‘Good’ for the Use of Resources. The Trust was awarded foundation trust status by Monitor early in 2008.
1.2 In April 2008 a detailed review was undertaken by HCC focusing on mortality rates amongst
those patients admitted as emergency admissions. During the course of the review, further concerns emerged regarding overall clinical care standards, effective systems to support care, leadership and monitoring processes.
1.3 The reasons cited for poor standards of care in the Inquiry Report included too much focus on
finances to the detriment of clinical care, little or no attention to clinical outcomes, inadequate supervision of services by the Executive Team, poor clinical engagement and inadequate staffing levels.
1.4 Further scrutiny of the organisation was undertaken including an independent case notes
review, a review of commissioning practices and emergency care services at the hospital. In response to public concerns regarding the standards of care provided and the assurance provided by the previous reviews the Secretary of State for Health charged Robert Francis QC to undertake an Independent Inquiry into the Trust.
1.5 The findings of this Inquiry were published in February 2010. There were 18 key
recommendations made for both health provider and commissioning bodies. 1.6 A report was provided to the Trust Executive Management Team meeting 14 January 2013 to
provide a position statement and assurance that the 18 recommendations had been considered by the predecessor organisations and implemented on the establishment of the Partnership Trust. This report was provided to Commissioners through the Clinical Quality Review meeting.
2.0 Public Inquiry
2.1 A further, Public Inquiry under the Inquiries Act 2005 was commissioned by the Rt. Hon
Andrew Lansley Secretary of State for Health on 9 June 2010. Robert Francis QC was appointed as Chair to the Public Inquiry. The Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry was published 6 February 2013.
In his letter to the current Secretary of State, Robert Francis QC summarises his findings by
saying:
“Building on the report of the first inquiry, the story it tells is first and foremost of appalling suffering of many patients. This was primarily caused by a serious failure on the part of a provider Trust Board. It did not listen sufficiently to its patients and staff or ensure the correction of deficiencies brought to the Trust’s attention. Above all, it failed to tackle an insidious negative culture involving a tolerance of poor standards and dis- engagement from managerial and leadership responsibilities. This failure was in part the consequence of allowing a focus on reaching national access targets, achieving financial balance and seeking foundation trust status at the cost of delivering acceptable standards of care.”
Enc 09
Page 4 of 8
2.2 It is generally considered that this Report marks a watershed for the NHS with a shift in emphasis of the provision of poor care not only being a matter of professional conduct, but potentially also a legal matter for staff and Trust Boards.
Robert Francis QC made 290 recommendations. He specifically recommended that:
• All commissioning, service provision, regulatory and ancillary organisations in healthcare
should consider the findings and recommendations of the Report and decide how to apply them to their own work;
• Each such organisation should announce, at the earliest practicable time, its decision on
the extent to which it accepts the recommendations and what it intends to do to implement those accepted, and thereafter, on a regular basis but not less than once a year, publish in a report information regarding its progress in relation to its planned actions;
• In addition to taking such steps for itself, the Department of Health should collate
information about the decisions and actions generally and publish on a regular basis but not less than once a year the progress reported by other organisations;
• The House of Commons Select Committee on Health should be invited to consider
incorporating into its reviews of the performance of organisations accountable to Parliament a review of the decisions and actions they have taken with regard to the recommendation in this Report.
3.0 Recommendations from the Mid Staffordshire NHS Foundation Trust Inquiry (2013)
3.1 Robert Francis QC identifies that of the 290 recommendations contained in the Report no
single one on its own provides the solution to the many concerns identified. 3.2 The essential aims of what he suggested are to:
• Foster a common culture shared by all in the service of putting the patient first; • Develop a set of fundamental standards, easily understood and accepted by patients, the
public and healthcare staff, the breach of which should not be tolerated; • Provide professionally endorsed and evidence-based means of compliance with these
fundamental standards which can be understood and adopted by the staff who have to provide services;
• Ensure openness, transparency and candour throughout the system about matters of
concern; • Ensure that the relentless focus of the healthcare regulator is on policing compliance with
these standards; • Make all those who provide care for patients – individuals and organisations – properly
accountable for what they do and to ensure that the public is protected from those not fit to provide such a service;
• Provide for a proper degree of accountability for senior managers and leaders to place all
with responsibility for protecting the interests of patients on a level playing field; • Enhance the recruitment, education, training and support of all the key contributors to the
provision of healthcare, but in particular those in nursing and leadership positions, to integrate the essential shared values of the common culture into everything they do;
Enc 09
Page 5 of 8
• Develop and share ever improving means of measuring and understanding the
performance of individual professionals, teams, units and provider organisations for the patients, the public, and all other stakeholders in the system.”
4.0 Culture
4.1 The importance of the culture across the healthcare system was highlighted as an important
factor which influenced the circumstances which lead to the situation at Mid Staffordshire NHS Foundation Trust.
4.2 Negative aspects of culture in the system were identified as including; a lack of openness to
criticism; a lack of consideration for patients; defensiveness; looking inwards not outwards; secrecy; misplaced assumptions about the judgments and actions of others; an acceptance of poor standards; and a failure to put the patient first in everything that is done.
4.3 To change the influence of any or a combination of these factors on the culture of an
organisation there needs to be “a relentless focus on the patient’s interest and the obligation to keep patients safe and protected from substandard care. This means that the patient must be first in everything that is done: there must be no tolerance of substandard care, frontline staff must be empowered with responsibility and freedom to act in this way under strong and stable leadership in stable organisations”.
4.4 Robert Francis suggests this can be achieved by a re- emphasis of what he describes as truly
important:
• Emphasis on and commitment to common values throughout the system by all within it; • Readily accessible fundamental standards and means of compliance; • No tolerance of non compliance and the rigorous policing of fundamental standards; • Openness, transparency and candour in all the system’s business; • Strong leadership in nursing and other professional values; • Strong support for leadership roles; • A level playing field for accountability; and • Information accessible and useable by all, allowing effective comparison to performance
by individuals, services and organisation. 5.0 Cultural Enablers 5.1 Since the establishment of the Trust in September 2011 the Board has been explicit in the
ambition and determination to develop the organisation as one in which quality is at the heart of everything that is done for patients and service users. Openness, transparency and the empowering of staff to raise concerns have also been an imperative for the Board and the Executive Team.
5.2 Some of the cultural enablers already established and in place or in development within the
Trust:
• Trust Board member visits to front line staff/services, including the Chief Executive spending one day each week working with a frontline team;
• Professional Leadership structure under the auspices of the Director of Nursing & Quality
which sits outside of the operational line management structure; • Monthly drop-in sessions with Directors and Associate Directors held in locations across
the county with an open invitation to all staff to attend to raise issues/ concerns or provide positive feedback of their working experience;
Enc 09
Page 6 of 8
• Quality Visits ( two each month) which includes Non Executive Director involvement; • Raising Concerns Helpline an independently run whistle blowing service for staff to
access; • High percentage rate of appraisal completion aligned to Trust values and strategic goals.
The quality of the appraisals is currently subject of an audit as part of the quality assurance process;
• The use of real-time patient and service user feedback to capture experience and provide
better outcomes; • Front line staff participation in review / challenge panels following incident investigation for
example the Tissue Viability Review Panel; • A Professional Forum facilitated through the Professional Leadership Team which was
established to facilitate two way communication for staff engagement, innovation and clinical change
• Demonstrable actions following staff raising concerns such as the ongoing work with
CCGs with regard to district nursing capacity, subsequent independent review and action plan currently being implemented;
• Plans approved by the Board already in train to develop a Training Academy for health
and social care support workers. The focus of the Academy is to ‘grow our own’ instilling the values and behaviours of the Trust at the onset of training non-clinically qualified support staff.
6.0 Proposal for staff/ patient /carer/ service user listening events following publication of
the Francis Report 6.1 The Executive Management Team has started to consider the next steps required to
implement the recommendations made in the Report of the Public Inquiry. In particular how staff, patients, carers and service users are engaged.
6.2 Consideration is being given to a range of potential methodologies to ensure that these
listening and engagement events are effective and inclusive. 6.3 On the day of the Report publication the Secretary of State for Health and the Chief Executive
of the NHS each published letters to Trust Chairs and Chief Executives respectively, in which the requirement for staff listening events was made clear. The Secretary of State said in his letter:
“We know that staff who feel engaged, supported, involved and listened to are able to provide
more compassionate care to patients. We must care for staff to care for patients. The first step in engagement is listening. To prevent another Mid-Staffs, I believe that we need to start by really listening, to patients and families, and to all the dedicated NHS staff working on the frontline in the NHS whatever their seniority or experience.”
7.0 Organisational context 7.1 The Trust is a very large and complex organisation. It is the largest integrated health and
social care trust in England. The logistical challenges of carrying out listening events will be significant, although arguably no different than those of regular consultation with users,
Enc 09
Page 7 of 8
partners, stakeholders and staff and there are many established forums in place which can be used to undertake the listening events and focus on addressing the recommendations of the Report.
8.0 Report recommendations with direct influence on the Trust 8.1 Whilst all of 290 recommendations will, to some degree or other, impact upon the Trust many
are recommendations for commissioners, regulators and other national bodies. An initial assessment of the 290 recommendations would suggest that the following have a direct influence on the Trust and will require some specific actions in response.
8.3 Clearly the listening events will not be able to address this full range of recommendations in
detail. The Executive Team will be carrying out its own assessment of work already in progress in respect of each of these recommendations so that a report can be made to this Board as part of the Trust’s preparations for a detailed response to the Francis report. It is proposed that a Board development session is dedicated to the consideration of all of the recommendations and the plans to address the actions required
9.0 Proposed methodology for staff listening events 9.1 It is proposed that in addition to the current staff engagement process, that a range of potential
methodologies are utilised by the Trust in order to provide the greatest possibility for staff across the whole organisation to have their say.
9.2 The focus will be to use a bottom up approach and make use of frontline staff with staff skills
and experience in running focus groups and facilitation. This will include a comprehensive communication plan to support the process.
10.0 Listening to patients and service users 10.1 To truly understand the quality of our care we also need to find ways of engaging patients and
their carers either within these groups or in separate focus groups. We will use our membership base to engage with patients, service users and carers which includes the 5,000 public and patient members. This will be lead by the Trust Engagement Manager. She is in the process of developing an engagement plan which includes patients, service users and stakeholders to allow them to offer their input into the development of the actions to address the relevant recommendations. This will be over and above the established engagement processes already in place within the Trust.
11.0 Summary 11.1 The Trust welcomes the findings of the Public Inquiry and is giving due consideration to the
recommendations and the actions that will be put in place to address the findings of the Inquiry. Whilst the response to the recommendations is awaited from the Government, the Trust will continue to act on those findings and recommendations that are not anticipated to be subject to national guidance or change in DH policy.
Enc 09
Page 8 of 8
12.0 Recommendations: The Trust Board is asked to:
• Receive the key points and recommendations of the Public Inquiry; • Approve the actions being taken to commence the listening events; • Advise of any further actions with regard to listening events; • Agree that a Board development session is dedicated to the consideration of the
recommendations of the report.
Enc 11
Page 1 of 2
REPORT TO: STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP NHS TRUST TO BE HELD ON: WEDNESDAY 27 FEBRUARY 2013
Enclosure: 11
Subject: Programme Management Office – Better Together Transformation Programme
Director Lead: Geraint Griffiths, Deputy CEO
Recommendation: For Approval & Assurance
x For Discussion For Information
PURPOSE OF THE REPORT:
The Programme Management Office (PMO) report provides the Board with an overview of activity and progress for the previous month, along with current timescales, key issues and focus areas. It includes a programme dashboard outlining the key component projects and their current delivery status (RAG rated) together with brief commentary. The latest draft of the high level Transformation Programme plan is included within the report, which provides the Board with the timelines for projects contributing to the overall Programme to implement the Model of Care. It also shows progress against the care plan targets.
KEY POINTS:
1. Transformation Programme Director’s Update 2. Programme Summary Dashboard 3. Programme Plan 4. 2012/13 CIP Dashboard & 2013/14 CIP Plans 5. Care Plan Reporting 6. Key points from Operational Transformation Board 08 Feb 2013 7. Productivity Improvement Plan - South 8. Proposed dates for Transformation Workshops
INTER DEPENDENCIES: Legal and/or Risk The programme is extensive in scope and will change the delivery of most
services across the Trust. Each element of the programme will require a separate risk register
Clinical The programme will require extensive clinical debate on the pathways underpinning the model
Financial The productivity assumptions underpinning the revised model of care will be essential to delivery to remain within financial resources in future years
HR There will be extensive changes to service delivery requiring discussions with staff and unions
Enc 11
Page 2 of 2
Social Care The model of care assumes a full integration between health and social care services across the Staffordshire County area, with a more virtual arrangement in Stoke-on-Trent
Patient & Public Involvement
There has been extensive public consultation on most elements of the model of care, including with overview and scrutiny. Further elements of the model will require further consultation both as a Trust and with partner organisations
Equality Impact Equality Impact Assessments will be undertaken as part of each programme area
Requirement for further review
The PMO will provide a monthly progress report to the Board
RECOMMENDATIONS: The Board is asked to: • Note the contents of the report; • Note the PMO actions for March 2013.
‘Better Together’ Transformation
Programme Report
Section 1. Transformation Programme Update 2. Programme Dashboard 3. Programme Plan 4. 2012/13 CIP Dashboard & 2013/14 CIP Plans 5. Care Plan Reporting 6. Key points from the Transformation Operational Group 08 Feb
2013 7. Productivity Improvement Plan – South Division 8. Proposed dates for Transformation Workshops
Transformation Programme Report Contents
Key Issues / Risks 1 – Phase 1 Delay and uncertainly impacts progress for Phase 2 Integrated Services The two phase approach carries inherent risk as the two models may diverge, but whilst Phase 1 Management of Change hasn’t started it is proving difficult to fully engage with staff around the Phase 2 work. 2 – Management of Change Paper Delivery Date unknown Full implementation planning for Integrated Teams (Phase 1) cannot be completed until the Paper is available. Project Team are currently awaiting confirmation of this date. 3 – Transformation Workshops Format First workshop is 28th Feb and current agenda is unclear as we do not know if the Management of Change Paper will have been published in time.
1 - Transformation Programme Director’s Update Overview Team mapping work for Integrated Teams Phase 1 is now complete and the management of change/staff consultation exercise is due to be launched late February 2013 . However there have been significant delays with both elements which means that the 1st April planned go live date is no longer achievable and a revised timetable for implementation needs to be developed. The Integrated Services Programme Board has been tasked with developing this plan. The production of care plans in the North remains below target whilst commissioners digest the implications from the recent District Nursing Review. This could also affect care plan production in the South. The Community Hospitals programme plan and risk log are currently being refreshed and will be presented to the March Transformation Programme Board for agreement. Key features of the plan include the development of a robust Strategy for Community Hospitals and ensuring clear alignment with commissioners’ ‘3 Big Tickets’. The E-Rostering Project Group has been set up; however initial risks and issues have been identified that could hinder implementation; these are being addressed via the Programme Board. Some key benefits that were assumed in the original business case for remote working would seem to be dependent on the implementation of the Strategic Clinical System(s). The final evaluation, due end March 2013, will report on the short and long term benefits realisation potential. A Business Case to ‘operationalise’ the use of the standard documentation set is out for review. Target for forms to be printed and available from the 1st of April is still on track, but a transition period needs to be agreed to phase out existing forms. Implementation plans for improving productivity in the South are currently being developed and focus on electronic case management, dependency weighting and job planning.
Actions for Next Month • Produce revised implementation plan for Integrated Teams • Transformation Programme Board to formally agree the Community
Hospitals Programme Plan • Agree Transformation structures and approach for 2013/14 • Continue Remote Working and Standard Assessment Pilots. • Approve Full Business Case for Standard Documentation set
2 – Programme Dashboard – Service Developments
Jane Gall imore
Jackie Will iams
Martin Hepke /
Malcolm Thomson
Jenna Abell
Case Management Early Implementers (South)
Community Hospitals ProgrammeThe Programme Plan i s being revised in recognition that a more s trategic approach i s required, this wi l l be presented to the March Transformation Operational Group and Programme Board. A performance outcomes framework that a l igns with the CCGs service speci fication i s being developed. Work i s underway to review the average LoS targets for each ward in l ine with contract negotiations . The progress made in community hospi ta ls over the las t 12 months wi l l be presented at the forthcoming Transformation Workshops . The Trust’s Discharge pol icy i s being revised to improve support to Operational teams, particularly in relation to the management choice delays . The Community Hospi ta ls operational management function i s being reviewed to clari fy roles and respons ibi l i ties at each tier. Work i s underway to prepare a case for the implementation of Ass is tive Technology/MyAmego in the hospi ta ls . The DST process i s being reviewed via an LHE project group, internal actions are taking place to review the most appropriate model of del ivery.
The Neighborhood Teams Productivi ty Project Charter i s currently being trans lated into a deta i led implementation plan that wi l l focus on 3 areas : the implementation of electronic caseload management, wide rol l out of the use of a dependency weighting tool for the a l location of DN activi ty and the adoption of the Job Planning Process by community heal th and socia l care s taff. The bus iness requirements for electronic caseload management and dependency weighting are currently being identi fied for review by IT. A pi lot s i te i s currently being identi fied to develop and tria l community job planning.
ILCT Early Implementer Teams (North)The production of care plans in the North remains below target whi l s t commiss ioners digest the impl ications from the recent Dis trict Nurs ing Review.
Team mapping work for Integrated Teams Phase 1 i s now complete and the management of change/staff consul tation exercise i s due to be launched late February 2013 . However there have been s igni ficant delays with both elements which means that the 1st Apri l planned go l ive date i s no longer achievable and a revised timetable for implementation needs to be developed. The Integrated Services Programme Board has been tasked with developing this plan.
Integrated Teams
A A
R
G
2 – Programme Dashboard – Enabling Projects / CIP
Jane Gall imore
Neil Calland
Andrew Errington
Single Assessment Process Remote Working - Proof of Concept Assistive TechnologyAl l of the Ini tia l Assessment Forms have now been received and pi lots of these forms have begun in most of the specia l i s t areas . The Bus iness Case for the future management of the sui te of forms i s complete and awaiting a decis ion. A working group has been set up to look at the documentation needs of the community hospi ta ls . A project update communication has been produced for inclus ion in 'The Word' and 'The Team Brief'.Outstanding actions for this project include agreeing what forms are required from Occupational Therapy and identi fying a budget for printing the forms.
Joint Commissioning Strategy for AT has been produced and is currently out for comments/review both within SSOTP and the wider stakeholder community. Project Board and approach are now in place. Resource requirements have been specified and the TSU are engaged to provide those resources. Work underway to identify environments where AT can be utilized as part of proof of concept. There have been some delays against the original timescales for creating and establishing the overall plan, but these do not currently threaten the overall timescales. Other key challenges are around the design of benefit measures and baselines to allow clear benefit capture of AT intervention and inform SSOTP Strategy and investment plans. Also, project is awaiting confirmation of finances available to SSOTP to allow recruitment to development posts and identification of TSU resource to enable project planning
The project has s tarted to work with 'early adopters ' in digi ta l ly completing care plans in patient's homes, and in sending a range of fax types (e.g. prescription requests ) di rectly from laptops . The Project Board agreed to refocus the use of sat navs , away from us ing the journey data to support mi leage cla ims , and to a l lowing the current locations of practi tioners to be seen to support the a l location of urgent referra ls . The Board a lso decided there was no va lue in pers is ting with the current digi ta l pen solution in the project. An a l ternative software solution i s being investigated which may give better trans lation performance. The fi rs t draft of a user eva luation questionnaire has been created and tested with two users . Some key benefi ts that were assumed in the origina l bus iness case are now looking somewhat tenuous . The fina l eva luation, due end March 2013, wi l l report on the benefi ts del ivered.
A A A
David Morgan
A tota l of 115 schemes have been identi fied within the North divis ion, amounting to an in-year va lue of £3,189k and a ful l year effect va lue of £4,212k.Against the phased target, the divis ion i s under achieving by £336k which i s 9.5% of the year to date plan. In order for this shortfa l l to be del ivered by the year end, an additional £112k of savings needs to be identi fied and del ivered each month for the rest of the financia l year.In the South the CIP target s tands at £3,103k, with del ivery forcast at £2,884k, which equates to a gap of £219k.The Trust’s processes for qual i ty impact assessment of CIP’s has been reviewed and revised, and this revised process has now been s igned-off by the Trust Board. Meetings of the CIP QIA Panel have been arranged for a retrospective review of qual i ty impacts of 2012/13 Cost Improvement Schemes, and of the qual i ty of ini tia l QIA analys is . This process has s tarted, and i t i s expected that a l l cost improvement schemes wi l l have been reviewed by February 7th.
A
3 - High Level Programme Plan 1 of 2 Service Redesign Programmes QIPP
Programme Baseline / Benefits / Performance MonitoringOverall benefits monitoring for the Programme
N/A Mark Walsh
Integrated ServicesA 2 Phase Approach to deliver Integrated Teams across the Trust. Phase 1 will deliver 28 co-located teams made up of Nursing and Social Care staff using current (but optimsed) operating model. Phase 2 will revise the operating model in order to meet projected demand in the most efficient way possible.
Improvement in Long Term Condition care and management, patients remain in most approriate setting (eg Home)
Introduction of Care Plans to co-ordinate all aspects of patient care in a single record
Use of Risk Stratification to better target patients who will then avoid acute admissions
Jane Gallimore
ILCT Teams North Early ImplementersImplement 13 Integrated Locality Care Teams in advance of full deployment in order to produce and managed individual care plans for patients
As Integrated Services
Jackie Williams
Case Management Early Adopters - SouthImplement Case Management (based on Risk Strat) to deliver patient care plans in advance of full
deployment of Integrated Teams
As Integrated Services
Martin Hepke / Malcolm Thompson
Community Hospitals ProgrammeRestructure Hospital services to deliver the most cost effective service to meet commissioned requirements
Improvements in Length of Stay
More Patients in appropriate setting
(ie non-Acute)
Staff Rostering and Deployment
improvements
Jenna Abell
Agree Performance Measures Benefits Measures in place
Programme Business Case 2013-2014 Complete
Benefits TrackingRefine Benefits Case & Add Details
High Level Benefits Realisation Plan AgreedUpdate BRP
Build Programme Bus Case
Agree Outline Team Structure (Numbers and Roles)
Agree Phase 1 Team & Mgt Structures
Consultation / Management of Change
Phase 2 StructureIn Place
Phase 1 StructureIn Place
Phase 1 Structure Implementation
Phase 2 Operating Model Design
9 ILCT Teams go Live. All 13 Teams are now 'live'
Phase 2 Workforce Plan / Modelling
Phase 1 EstatesRequirements
Phase 2 Consultation / Management of Change
Phase 2 Implementation
Early Implementers Care Plan Production / Monitoring
South West Care Plan Production / Monitoring
Start South East Care Plan Production
South East Care Plan Production / Monitoring
Care Plan Production / Monitoring
Productivity Monitoring
Agree revised Care Plan Targets with CCGs
Agree revised Care Plan Targets with CCGs
Establish Performance Baselines
Agree future strategy for community hospitals
Produce Business Case for Ward Information System
Implementation PeriodOperating Model Design
Community Hospitals Future Use Options Paper
Phase 1 Process Analysis (Nursing / Social Care)
Support Tool RequirementsSupport / Performance
Measurement Requirements Complete
Standardised Process Agreed
Phased Deplyment of Processes / Tools (TBC)
Shift Pattern Analysis Standardise Shift Patters E-Rostering First Deployment
Single Assessment Process / Care PlanAgree and deploy a standardised set of documentation for assessment and care planning across the Trust
Improvement Tools
Cost improvement around access to patient information and reduction in duplicated work
Jane Gallimore
Remote WorkingConduct a Proof of Concept to assess the benefits of deploy devices to allow staff to access clinical systems from the field and to reduce duplication of data entry. Based on the outcome, then to deploy the selected solution(s) across the mobile workforce
Improvement Tools
Cost Improvement from reduction in number of journeys and increase volume of patient contact time per staff member
Neil Calland
Assistive TechnologyConduct a full investigation into potential telehealth/telecare solutions and work with commissioners to agree a strategy before creating a deployment project to realise identified benefit
Improvement Tools
Productivity gains as 'maintenance' visits (ie blood pressure measurement) are replace with the technology, thus reducing the number of visits needed
Andrew Errington
Electronic Self Management of Care plansAs part of an SHA Pilot, introduce appropriate patients to the self managed internet based care plan
Improvement Tools
Long term benefits as patients self management delays escalation to managed care
TBC
Single Assessment Process is 'live' in nominated organisations
on a pilot basis
Single Assessment Process Pilot
Single Assessment ProcessDeployed across all
organisations
Updates /Mods to SAP
Final Version of SAP is Completed and Agreed
Review / Audit
Proof of Concept Starts
Effectiveness Review and Benefits Tracking & Assessment
Plan018 0.7% Recurrent CIP Liz Onions 500 366 153 108 Plan019 Wheelchair Service Steve Foster 0 0 129 83
Plan020 GUM Activity recharged to South Staffordshire Commissioners Dr Kundu 0 0 200 150
Plan021 Reduction in Sexual Health Drug expenditure Dr Kundu 0 0 100 75
TOTAL 3,103 2,405 2,884 2,041
Target 3,103 shortfall: (219)
4 – Cost Improvement Programme 2013/14
QIPP Programmes – Currently Identified Projects 2013/14 Status UpdateAdult Services Transformation (Integrated Teams)Community Hospitals TransformationMedicines Management Service Redesign Paper to Executive Team 18th January 2013
AHP Performance Optimisation Review Therapy teams generating responses to Ernst & Young data
Rehabilitation Medicine Service redesign OngoingPharmacy Services Redesign Paper to Executive Team 18th January 2013Prescription Charges Ready to implementSexual Health re-organisation (removal of posts) Scoping underwayDental Services – Contractual AdjustmentsDental Services – Management ReviewPrison Services – Management Restructure and Post Review Awaiting Management of Change paperCommunity Services•Central Booking Implementation underway•Dressings Formulary Commissioner discussions underway•Continence/Enteral feeds Commissioner discussions underwayIntegration – ICT & ProcurementAdult Social Care - Reduction in cost of long term support OngoingEstates Rationalisation OngoingTransport - NEW ADDITION
5 – Care Plan Production - North
As at 01/02/2013
Locality / Region / Practice Population
size
Planned Actual Variance Number of Patients on Care Plan
Totals 6069 406 406 406 28 378 -5691 -28 0 All figures are 'To Date'
5 – Care Plan Production – Stafford [as of 25/01/2013]
Locality / Region / Practice
Planned Actual Variance Number of Patients on Care Plan
admited to Acute
Setting
Commentary NeighbourhoodTeam
Population size
Target to End of Period
Patients Identified
and Agreed with SSOTP
Admitted to the
Model of Care
Assessment in
Progress
Discharged Patients
Patients refused to be admitted to the model of
care
Total Number of Care Plans
Produced
Completed against Target
Completed against Patients
Identified
Stafford and Surrounds
1 Mansion House
13,332
108 48 4 1 4 -104 -44
The team are working with the specialist nurses identifying patients who have been identified to be case managed to prevent duplication but ensuring case management assessment takes place. Awaiting further patients to be identified in Jan 2013 MDT
1 Cumberland House
12,800 86 0 0 -86 0
1 Crown Surgery 7,202 48 0 0 -48 0
2 Browning Street
9,458
75 25 18 1 2 19 -56 -6
On commencement of new case manager, 6 patients were RIP from original list - case management process not commenced with these patients. MDT Scheduled for 28/11/2012 - cancelled by practice. Liaision with practice for MDT and release of additional patient names. 1 patient RIP 20/12/2012
2 Gnosall
7,695 58 0 0 -58 0
2 Wolverhampton Road
10,677 81 31 18 1 18 -63 -13 3
2 Holmecroft
10,455 88 50 16 18 -70 -32
2 Castlefields Surgery
5,988 46 28 6 6 -40 -22
28 patients identified on the 08 January with Case Manager. None of the 6 patients admitted to the model of care were known to the District Nursing Team
2 Rising Brook Surgery 10,373 71 0 0 -71 0
3 Brewood
10,099
72 102 7 3 1 1 8 -64 -94
7 patients RIP, 6 patients Nursing home. List not validated by surgery. No direction on patients to commence admitting to the model of care provided by Practice.
3 Hazeldene
8,350 69 29 2 1 2 -67 -27
3 Weeping Cross
18,076
148 144 65 2 9 2 67 -81 -77 2
87 patients provided initially by practice, 12 patients were considered unsuitable for the model of care by the Case Manager. Number in 'Patients identified and agreed with SSoTP' reduced by 12 as these were deemed inappropriate for case management
3,247 32 0 None Received 0 -32 0 Data Sharing Agreement not returned: practice still to engage with LTC workstream. Delayed approach requested
2
Red Lion House (Dr Berriman)
3,994 40 0 Please see
commentary 0 -40 0
55 patients identified by practice but not validated. Second list produced by Practice and meeting to share list with ACNS Team scheduled for 26 February 2013
2 & 3
GP Suite Cannock Chase Hosptial & Burntwood(Dr Myint)
8642 (Combined
73 30 17/09/2012 23/10/2012 11/12/2012
16 1 16 -57 -14
1 patient refused: 1 patient in hospital. MDT held 11/12/2012. MTD held on 11/12/2012. MDT Scheduled for 22/01/2013 cancelled. 10 patients details released at each meeting.
2 & 4
Nile Practice
5,475 54 14
04/12/2012 and 17/12/2012 PLEASE SEE
COMMENTARY
3 3 -51 -11
Primary and secondary care data have been amalgamated and forwarded to the practice for final validation on 14/11/2012. 04/12/2012 NHT2 received 28 Patient details. 17/12/2012 NHT4 received 14 patient details.
2 Newhall Street (Dr Verma)
2,279 23 23 14/11/2012 4 4 -19 -19
2 Moss Street Surgery (Dr Gibbons) 5,026 50 15 26/11/2012 3 3 -47 -12 2 Chadsmoor Medical Practice 4,014 30 37 28/11/2012 0 0 -30 -37
5 – Care Plan Production – Cannock 2 of 2
As at 25/01/2013
Locality / Region / Practice
Planned Actual Variance Number of Patients on Care Plan
admited to Acute Setting
Commentary NeighbourhoodTeam
Population size
Target to End of Period
Patients Identified
and Agreed with SSOTP
Date patient information
received
Admitted to the Model of
Care
Assessment in Progress
Discharged Patients
Patients refused to be admitted to the model of care
Total Number of Care Plans Produced
Completed against Target
Completed against Patients
Identified
3 Rawnsley Road Surgery
4,066
40 7 05/12/2012 1 1 -39 -6
3 Hednesford Valley Health Centre (Dr Chandra) 2,430
24 0 None Received 0 -24 0 Awaiting practice to validate data
3 Hednesford Valley Health Centre (Dr Murugan)
3,590
36 21 14.12.2012 2 2 -34 -19
3 Hednesford Valley Health Centre (Dr V K Singh)
3,572
26 0 None Received 0 -26 0 Practice still to sign data sharing agreement and release data
3 Hednesford Valley Health Centre (Dr Yi)
3,015
38 0 None Received 0 -38 0 Practice have received data. Practice to validate data. Practice to arrange meeting with SSoTP Case Manager to share list
2 & 3 Dr Gupta (Chase Practice)
10552 Combined
91 21 Additional 4
patients 21/11/2012
19 2 21 -70 0 1 1 Patient admitted as needed a pace maker fitting. 2 patients RIP: Chadsmoor Team.
3 Dr B K Singh (Heath Hayes & Norton Canes)
4,395
36 0 None Received 0 -36 0 Data Sharing Agreement not returned: practice still to engage with LTC workstream. Delayed approach requested
3 Norton Canes health Centre (Dr Jalota)
4,395
30 0 None Received 0 -30 0 Overall approach still to be agreed with practice. Data Sharing Agreement not returned
3 Norton Canes health Centre (Dr Po & Zeya)
3,280 33
0 None Received 0 -33 0 Overall approach still to be agreed with practice. Data Sharing Agreement not returned
4 Great Wyrley Health Centre (Dr Desai)
2,122
21 10 03/01/2013 0 0 -21 -10
4 Great Wyrley Health Centre (Dr A B Patel) 2,038 21 7 05/12/2012 0 0 -21 -7
4
Great Wyrley Health Centre (Quinton Practice)
3,661
37 28
23/10/2012 received
additional 11 patients
21 21 -16 -7 Practice had achieve 0.5% LES as required by CCG. No additional patients needed for the period
4
Dr Kukathasan
3,093
28 8 8 received
14th Jan 2013 0 -28 -8
Meeting held on 14 January 2013. Practice had an initial list of 14 patients. During meeting 6 patients were not deemed as appropriate as patients had either dementia or were in nursing home beds.
4
High Street Surgery (Cheslyn Hay)
5,310
52 25 12/12/2012 0 0 -52 -25
Data Released 07/11/2012 to Case Manager. Further validation of patient list, reduced to 43 patients. ACNS TL contacted practice as patients were still not appropriate for case management. First MDT scheduled for 13 December 2012 at 12:30pm - MDT cancelled by practice
4
Essington Medical Centre
1,965
11 0 None Received 0 -11 0
Data Sharing Agreement returned 20/11/2012. Trajectory indicates practice to commence workstream w/c19/11/2012. List of patients received by practice on 12/12/2012. Practice to validate list in readiness for meeting with ACNT TL and Case Manager.
Totals 1086 353 116 0 2 1 120 -966 -233 0
5 – Care plan Production – East Staffs CCG and South East Staffs CCG
East Staffs CCG: • Bridge practice: of initial 28 patients identified 21 have now opted for case management and have been allocated to staff through initial
MDT meeting. 14 further patients identified and working with practice to identify further patients through manual process as BUPA risk strat tool not in place.
• Yoxall and Barton practices have had their released data validated and have identified that initial patients identified by manual risk strat are not all appropriate for case management.
• Yoxall released 19 patients but only 4 appropriate. Therefore meeting to be arranged with GP and commissioners to identify more appropriate patients. Assessment and care planning underway for those patients identified.
• Barton released 48 patients (one quarter) and undertaking initial assessment and care planning on 15 patients; working on identifying further appropriate patients.
• Alrewas practice data currently being validated on 15 patients and working with practice to identify appropriate patients. • Working with commissioners to support roll out of BUPA risk strat. training to GP practices so that more accurate risk strat. data can be
released to SSOTP. South East Staffs CCG: • Fulfen practice released patient data on 12 patients but data was incomplete so awaiting update from GP practice • Burntwood health and well being centre are still manually collating their data and have not released to SSOTP • No data has been released yet from Stonydelph practice • Meeting with Langton practice for roll out of case management has been arranged for 30.01.2013. • SSOTP met with commissioners on 24.01.13 for further update on roll out trajectory and release of data from practices. SSOTP staff will
continue to meet with practices to discuss case management process as they come on line.
6 - Key points from the Transformation Operational Group 08 Feb 2013 • A meeting of the Integrated Services Programme Board to be convened to agree a detailed
implementation plan for Integrated Services that is informed by a clear strategic vision. • The reporting of case management data in the North will be put on hold until there is clarity on
how the findings and recommendations from the District Nursing review are to be implemented. • A productivity implementation plan has been approved for the South and consists of 3 inter-related
projects: electronic case management, dependency weighting and job planning. • The locality maps for both the North and South will be completed by end February 2013. • The group have asked that a separate CIP governance forum be established due to time
pressures and sheer volume of papers to be covered. • The format and content of the Transformation Workshops need to be agreed as a matter of
3. Ensure consistent application of a Electronic Case Load Management / Dependency Weighting tool across the Trust
4. Increase team productivity and efficiency, thereby contributing to the Trust's Cost Improvement Programme
Better Together Transformation Programme - Enablers to improve staff productivity in the South
5. Provides staff with a basis for working flexibly as a team
2. Reduce unnecessary hospital admissions
1. Maximise the available clinical capacity of a team and improve face to face contacts from 40% to 60%
Overall aims of the programme are to:
Identify business requirements Options Appraisal / Source IT solution
Trial IT Solution with chosen teams
Project Charter
Evaluation
Paper to JSP outlining benefits
ID Pilot Site
Staff Training
Agree performance measures
Identify business requirements
Project Charter
Establish baseline
Form Project Group
Agree business requirements
Review IT requirements
ID 2 additional test sites
2nd phase of testing
Ongoing Clinical engagement plan ref principles and philosop
As above
Complete appraisals / job plans for pilot site
Review commissioner intentions
Testing Phase Update to JSP
Equality Analysis
Staff re- engagement ref principles and philosophy of dependency
weighting
Project Charter
TBC
8 - Proposed dates for Transformation Workshops
Date Area Location 1st March Stafford Yarnfield Park Training & Conference
Centre 6th March Seisdon Wombourne Civic Centre 8th March Cannock Cannock Chase Park & Hockey
Cricket Club 13th March Burton Branston Golf & Country Club 15th March Newcastle Britannia Stadium 20th March Moorlands 3 Horseshoes Leek 21st March Stoke 2 Britannia