20
CASE 2 Dr Mohit Goel JR 1 9/7/2012
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | anish-choudhary |
| View: | 35 times |
| Download: | 2 times |

CASE 2
Dr Mohit Goel
JR 1
9/7/2012

HISTORY
56 yrs male ( Mr Bhandarkar Ramesh ) presented with pain and swelling of right lateral side of nose and right lower periorbital area since 2 mnths. There is also redness of right eye with headache since 2 mnths.
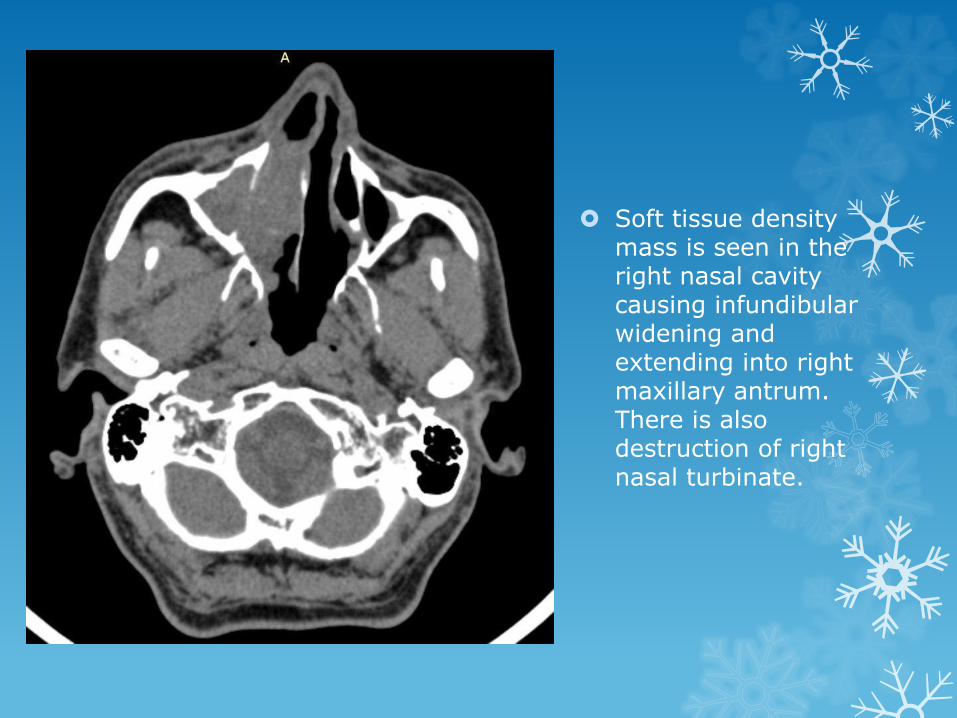
Soft tissue density mass is seen in the right nasal cavity causing infundibularwidening and extending into right maxillary antrum. There is also destruction of right nasal turbinate.

Extension of mass into the ethmoid sinus on both sides with right side lamina papyraceadestruction and invasion of intraorbital fat causing right eye proptosis.

Cranially the mass extends upto the frontal and ethmoidal sinuses on both sides and destroys the floor of anterior cranial fossa on right side, extending intracranially into the frontal region.

The mass shows fairly homogenous enhancement on post contrast images with few small non-enhancing areas within. A well defined non-enhancing area within the right frontal sinus laterally could represent a mucocele.

MRI
The mass appears inhomogenouslyhyperintense on T1 WI.

It turns hypointense with hyperintense areas within, on T2W_FLAIR.

A fairly defined non enhancing area witihinthe right frontal sinus laterally shows peripheral enhancement and could represent mucocele.

MELANOMA
Primary mucosal melanoma of the head and neck is an uncommon neoplasm and accounts for 20% of all malignant melanomas. Within the head and neck region, the most common site of origin is the nasal cavity, where the anterior septum is most often involved, followed by inferior and middle turbinate . The second most common site is the oral cavity, where a predilection for the hard palate and maxillary alveolar gingivae has been found.
The peak age for mucosal melanoma is during sixth to seventh decade. The majority of patients with nasal cavity primaries present with nasal obstruction and epistaxis. Proptosis, diplopia, pain and facial deformity are less common and are indicative of advanced disease.
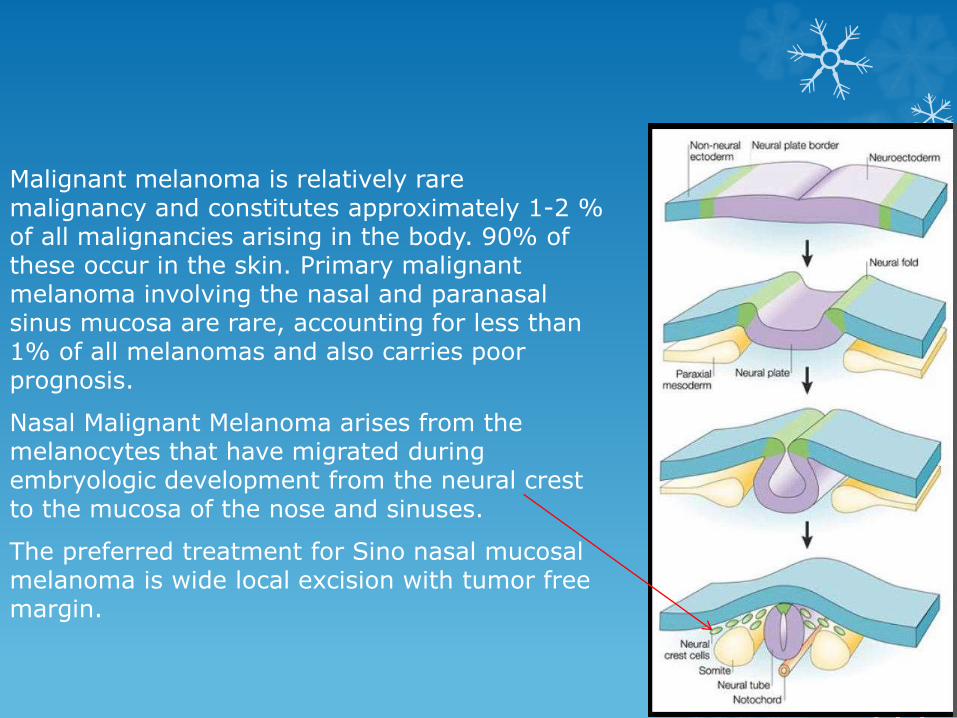
Malignant melanoma is relatively rare malignancy and constitutes approximately 1-2 % of all malignancies arising in the body. 90% of these occur in the skin. Primary malignant melanoma involving the nasal and paranasalsinus mucosa are rare, accounting for less than 1% of all melanomas and also carries poor prognosis.
Nasal Malignant Melanoma arises from the melanocytes that have migrated during embryologic development from the neural crest to the mucosa of the nose and sinuses.
The preferred treatment for Sino nasal mucosal melanoma is wide local excision with tumor free margin.

On CT
Melanomas shows bone remodeling , although element of frank erosions may be present . They are highly vascular tumor so they enhance well on post contrast study.
On MRI
Melanomas have high T1W signal intensities primarily because of the presence of haemorrhage and to a lesser degree because of the paramagnetic melanin.

PNS radiograph shows homogenous opacity in the
right nasal cavity.

CORONAL CT shows the mass involving the ethmoid sinus and extension into the orbit.
POST CONTRAST study shows intense enhancement

CORONAL CT (BONE WINDOW) shows bonydestruction.
AXIAL CECT showing the extent of mass.

The Differential Diagnosis of Nasal melanoma includes-
Anaplastic carcinoma, Lymphoma, Embroyonal rhabdomyosarcoma, Esthesioneuroblastoma and Extramedullary plasmocytoma.
Esthesioneuroblastoma (ENB),
also known as olfactory neuroblastoma, is a rare neoplasm originating from olfactory neuroepithelium. These tumors often display varying biologic activity ranging from indolent growth, with patient survival exceeding 20 years, to a highly aggressive neoplasm capable of rapid widespread metastasis, with survival limited to a few months.
Esthesioneuroblastoma. Coronal CT scan of the orbits and sinuses shows a large, enhancing, and expansilemass occupying the ethmoid air cells that is invading the cribriform plate and breaking through to the left anterior cranial fossa.

Esthesioneuroblastoma. A 39-year-old man presented with 1 month of decreased vision, left facial numbness, and swelling. Physical examination demonstrated left-sided exophthalmos and blindness. He had also lost his sense of smell. Contrast-enhanced T1-weighted MRI demonstrated a large lesion that originated in the paranasal sinuses and extended through the cribriform plate into the anterior cranial fossa.

Esthesioneuroblastoma
The MRI appearance is often that of a large, soft tissue, dumbbell-shaped mass centered within the superior nasal cavity and extending intracranially. The tumor is generally hypointenseon T1-weighted images and iso- to hyperintense on proton density and T2-weighted images. Contrast enhancement is usually mild to marked and can be uniform or mildly heterogenous.
On CT, the tumour is iso- to slightly hyperdense to muscle and enhances homogenously. CT is most useful in demonstrating bone destruction. In addition, calcifications within the mass are reported to be a relatively specific diagnostic indicator of esthesioneuroblastoma.

Solitary extramedullaryplasmacytoma
Extramedullary plasmacytomas are rare neoplastic lesions that can appear in the head and neck. They are characterized by monoclonal proliferation of plasma cells. The nasal cavity and nasal septum are probably the most common locations.
It shows nonspecific CT and MR imaging features. However, features that may suggest the diagnosis are a bulky soft-tissue mass or infiltrative lesion. The tumour does not usually become disseminated, but it may be locally aggressive and demonstrate marked involvement and destruction of the adjacent structures.
SEP should be included in the differential diagnosis of a nasal tract lesion because it has imaging findings similar to those of other more common lesions such as nasopharyngeal carcinoma and lymphoma.

THANK U

















