67
MENIERE’S DISEASE PRESENTER : DR SHWETA SHARMA
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | shweta-sharma |
| View: | 166 times |
| Download: | 4 times |

MENIERE’S DISEASE
PRESENTER : DR SHWETA SHARMA

• DEFINITION• REVIEW OF LITERATURE (HISTORY)• INCIDENCE• REVIEW OF ANATOMY• AETIOPATHOLOGY• DIAGNOSIS• MANAGEMENT
DEFINITION
Cause unknown
HISTORY150 years & still elusive…..
• Prosper Meniere first described the symptom complex in 1861 and proposed the pathologic site to be in the labyrinth.
• In 1871 Knapp advanced the hypothesis that hydrops was similar to ocular glaucoma : aural glaucoma
• In 1938 Hallpike and Cairns described the underlying pathology endolymphatic hydrops but the precise etiology still remains elusive

INCIDENCE
• The disease seems to be more prevalent among whites, with a variable female-to-male ratio ( ranging from 1:1, 1.3:1, 2:1 ; female preponderance ).
• The peak age at onset is in the fourth and fifth decades of life, although presentation can be at almost any age.
• The incidence of bilateral disease probably is in the range of 19% to 24%.
• Familial occurrence of Meniere’s disease has been reported in 10% to 20% (An AD mode) Migraine is strongly associated in such cases.
• The incidence is elevated in persons with specific major histocompatability complexes (MHCs).
• Human leukocyte antigens (HLA) B8/DR3 and Cw7 have been associated with Meniere’s disease.
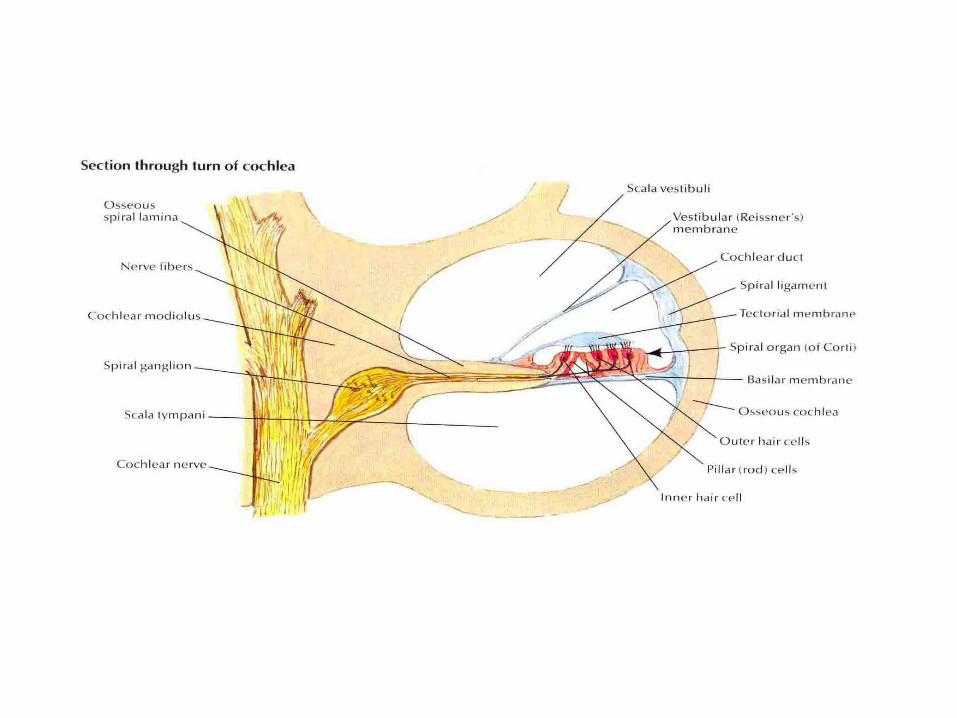
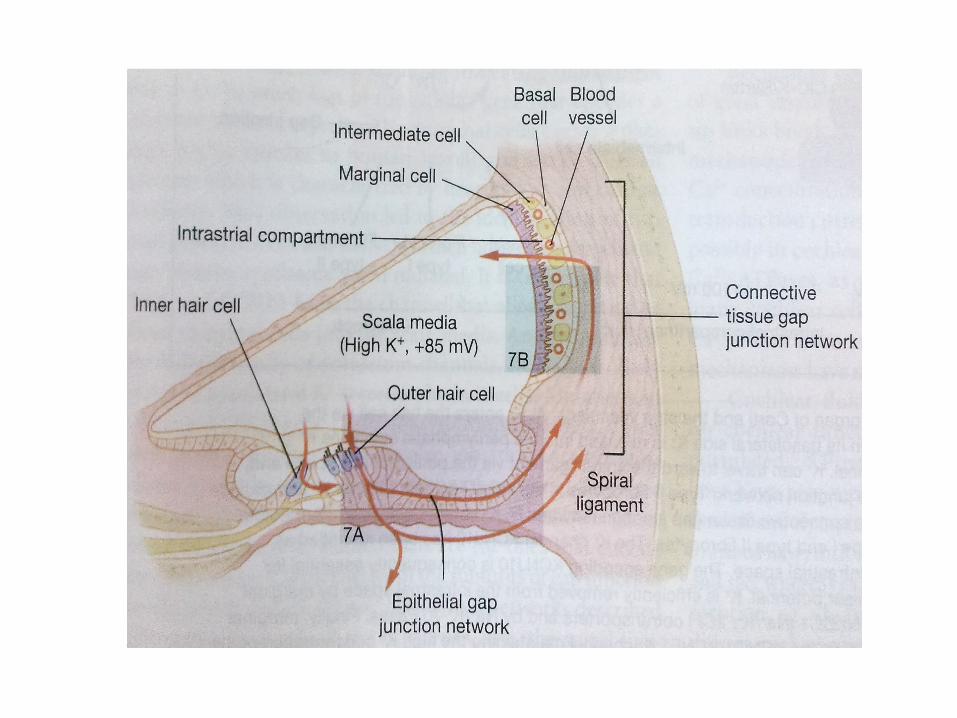
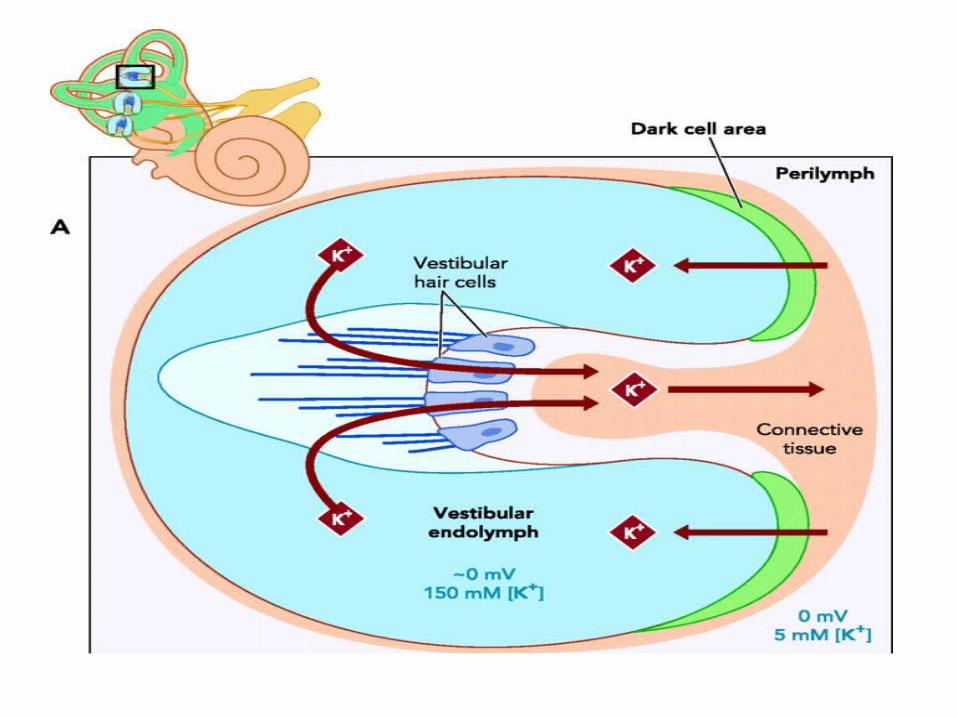
REVIEW OF ANATOMY
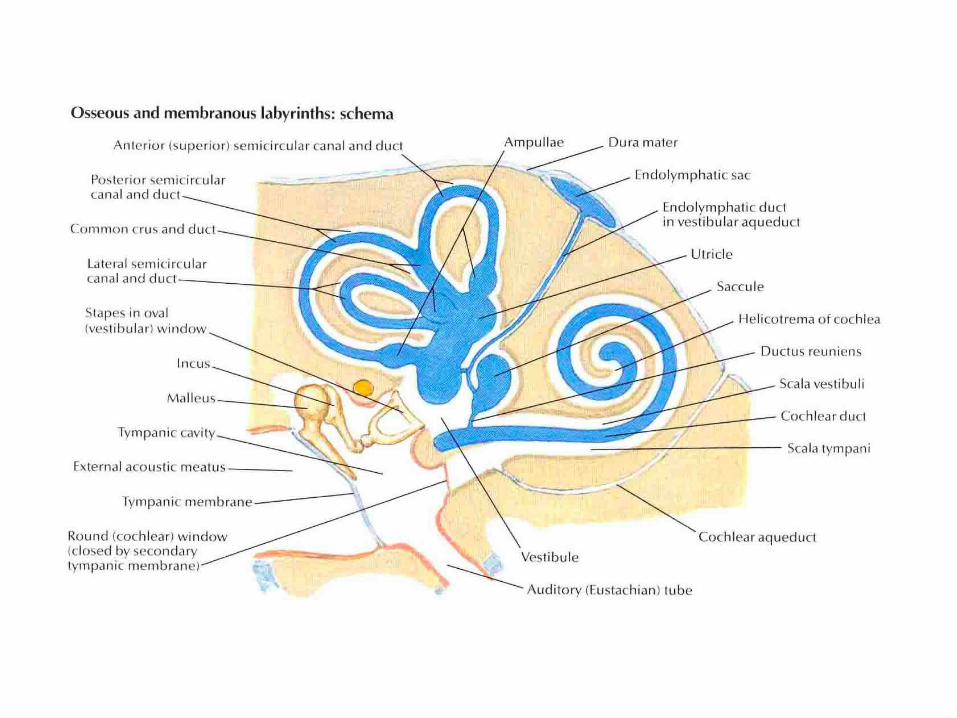
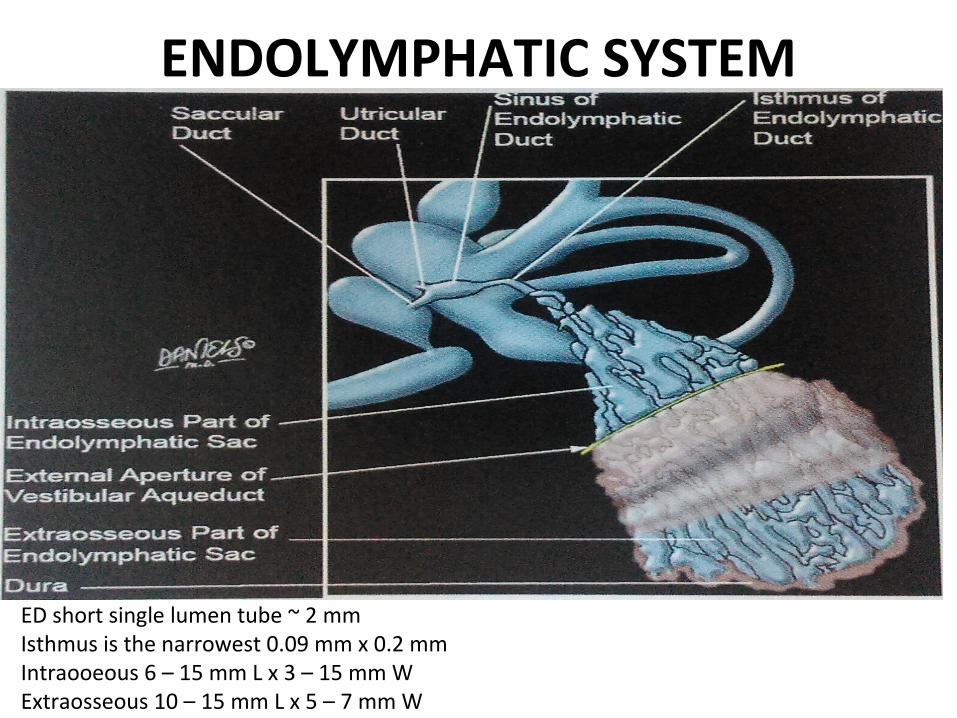
ENDOLYMPHATIC SYSTEM
ED short single lumen tube ~ 2 mmIsthmus is the narrowest 0.09 mm x 0.2 mmIntraooeous 6 – 15 mm L x 3 – 15 mm WExtraosseous 10 – 15 mm L x 5 – 7 mm W
Functions of ENDOLYMPHATIC sac
1. Resorption of the water content of endolymph
2. Ability to participate in some ionic exchanges with endolymph
3. Removal of metabolic and cellular debris, including otoconia
4. Immunodefense function ( perisaccular )
5. Inactivation and removal of viruses
6. Secretion of Glycoproteins to attract extra fluid (Glycoproteins act as a driving force for longitudinal flow)
1. Secretion of Saccin to increase Endolymph production
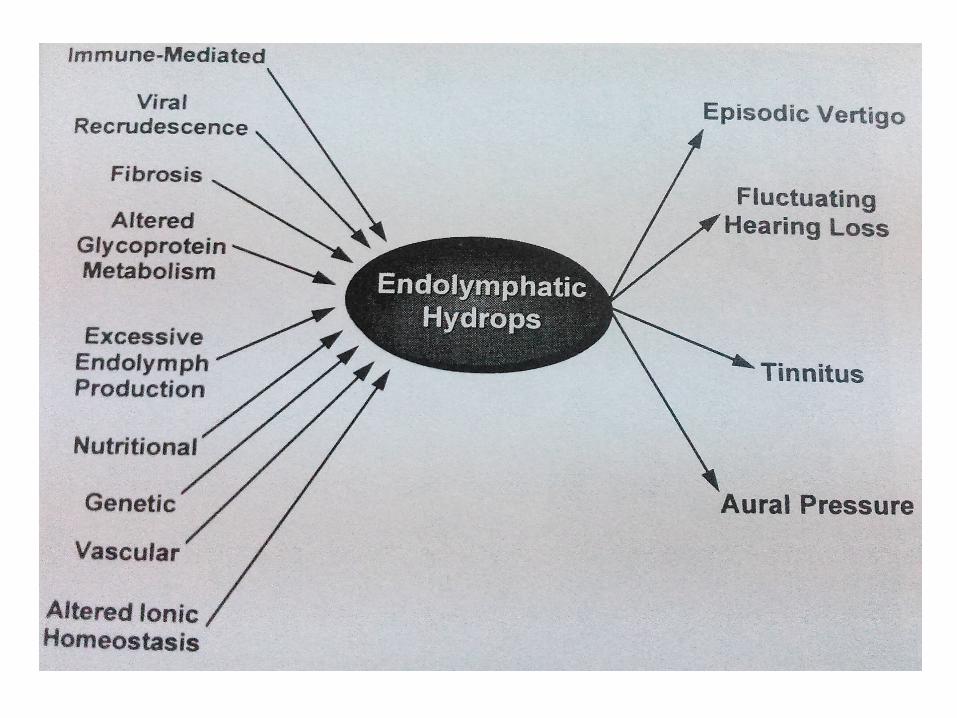
AETIOPATHOLOGY
Aetiology
• Anatomical-abnormalities• Genetic- AD• Immunological - immune complex deposition• Viral-serum IgE to herpes simples virus types I and II,
Epstein-Barr virus and CMV• Vascular-associated with migraines• Metabolic-potassium intoxication
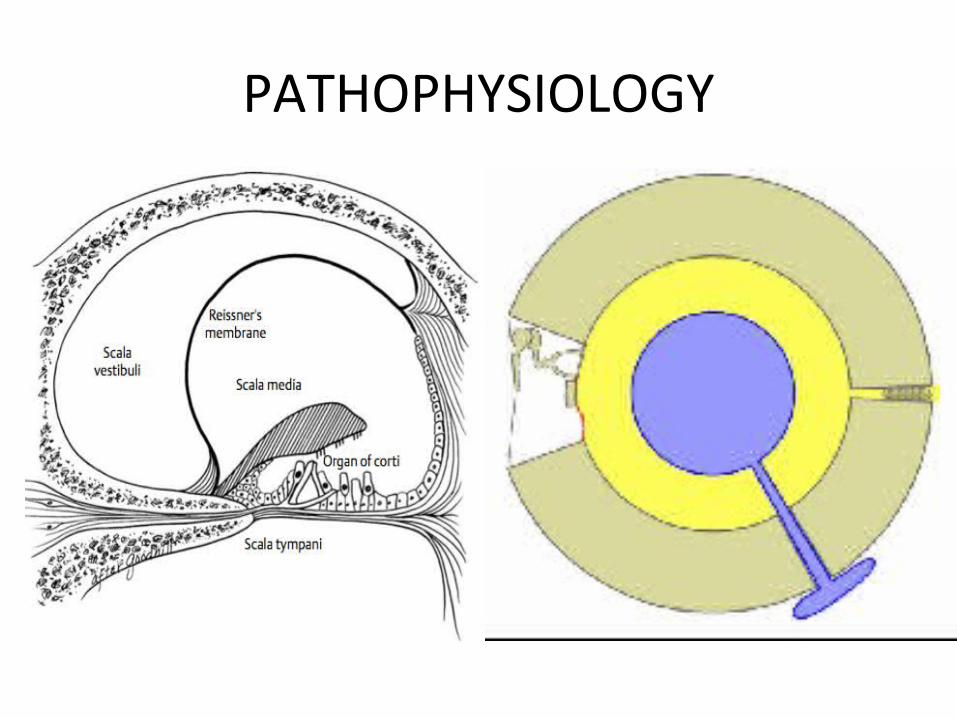
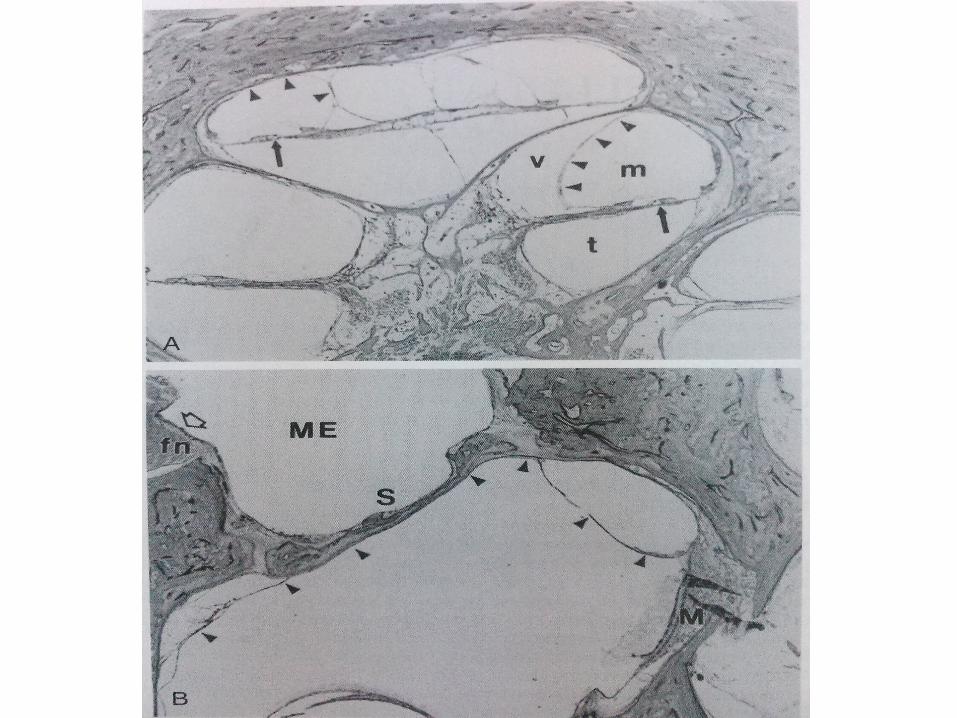
PATHOPHYSIOLOGY
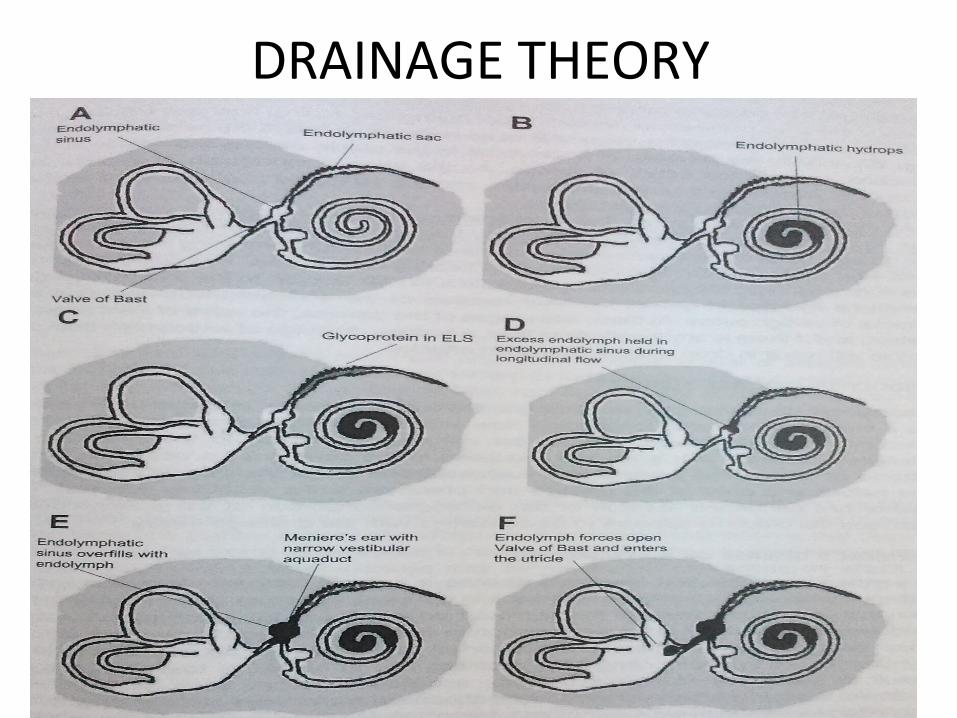
DRAINAGE THEORY
CLINICAL PRESENTATION

Clinical presentation
• The typical history consists of recurring attacks of vertigo (96.2%) with tinnitus (91.1%) and ipsilateral hearing loss (87.7%).
• Attacks often are preceded by an aura consisting of a sense of fullness in the ear, increasing tinnitus, and a decrease in hearing.
• cochlear and vestibular Meniere’s disease

• Otolithic crisis of Tumarkin
• Lermoyez syndrome
Physical Examination• Examination results vary, depending upon the phase
of disease.
• During an acute attack, the patient has severe vertigo.
• Spontaneous nystagmus directed toward affected ear is typical during an acute attack.
1. Irritative nystagmus during the first 20 mins of attack
2. Paralytic nystagmus follows
3. Later recovery nystagmus starts
Hearing Loss and Tinnitus • Sensorineural hearing loss is fluctuating and progressive, with the
sensation of fullness or pressure in the ear.
• In only 1% to 2% of patients does the hearing loss progress to profound deafness.
• Additional features include diplacusis, a difference in the perception of pitch between the ears (43.6%) and recruitment (56%) .
• Tinnitus tends to be nonpulsatile and variously described as whistling or roaring. It may be continuous or intermittent. Tinnitus often begins, gets louder, or changes pitch as an attack approaches. Frequently a period of improvement follows the attack.
• The Romberg test generally shows significant instability and worsening when the eyes are closed.
• The Weber tuning fork test usually lateralizes away from the affected ear.
• The Rinne test usually indicates that air conduction remains better than bone conduction.
• Complete neurologic evaluation is important. New-onset vertigo might be an early sign of stroke, migraine, or brainstem compression that may require emergent evaluation and care.
Particularly helpful to document present hearing acuity and to detect future change.
-The patient may not notice a loss at specific frequencies. Low-frequency or mixed low- and high-frequency insufficiency may be observed.
- Typically, the lower frequencies are affected more severely. This is due to preferential sensitivity of the apex to the hydrops.
- Multiple hearing tests, which document fluctuating hearing loss, are helpful in diagnosing Ménière.
Audiometry

A pattern of low-frequency fluctuating loss and a coincident nonchanging, high-frequency loss is described, resulting in a “peaked” or “tent-like” tracing on the audiogram. This peak classically
occurs at 2 kHz.
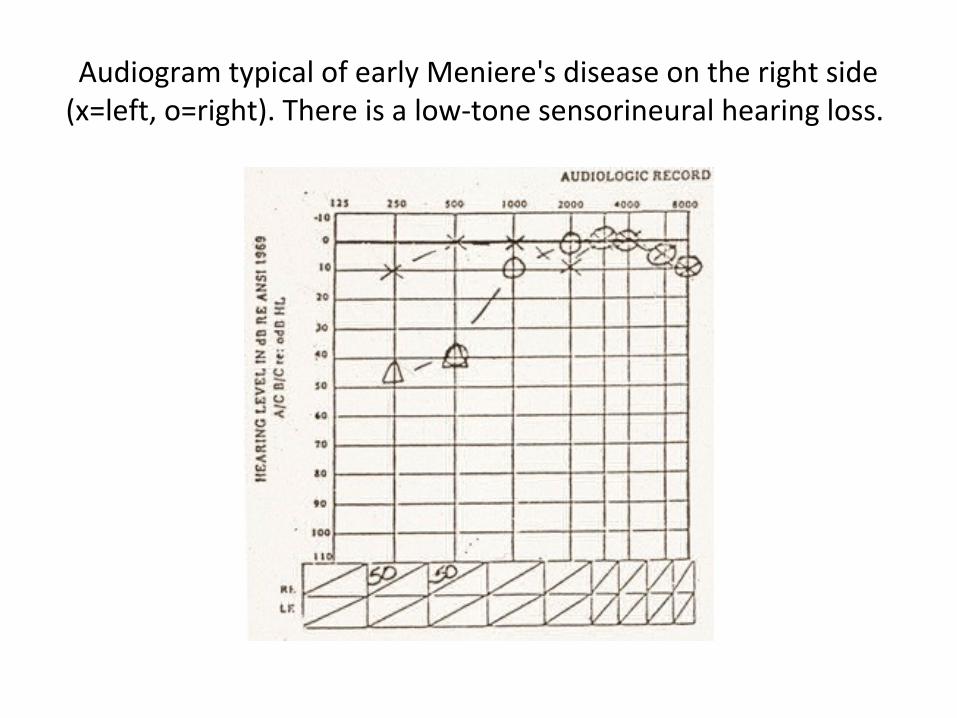
Audiogram typical of early Meniere's disease on the right side (x=left, o=right). There is a low-tone sensorineural hearing loss.
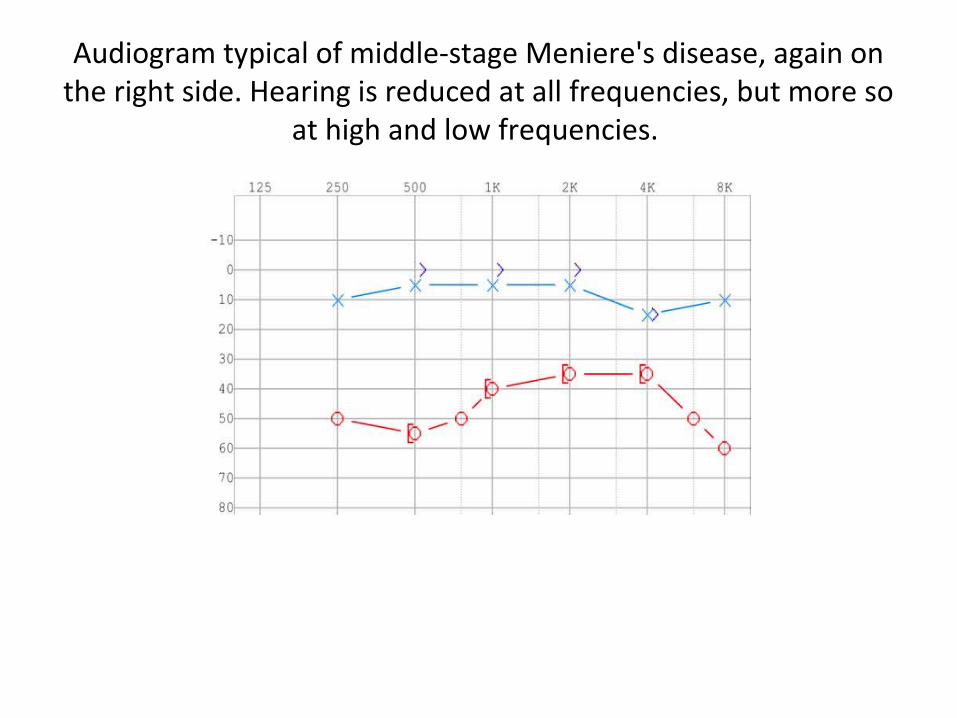
Audiogram typical of middle-stage Meniere's disease, again on the right side. Hearing is reduced at all frequencies, but more so
at high and low frequencies.

Audiogram typical of late-stage Meniere's disease, again on the right side. Hearing is flat, and unaidable on the right side.
Recruitment
•Alternate binaural loudness balance test (ABLB)•Short increment sensitivity index (SISI)
Imaging Studies• Magnetic resonance imaging
- R/o abnormal anatomy or mass lesions. Specifically, acoustic neuromas or CP angle lesions. Other lesions, such as multiple sclerosis or Arnold-Chiari malformations, also can be ruled out.
• CT scans reveal dehiscent superior semicircular canals and/or widened cochlear and vestibular aqueducts
DIAGNOSIS

AAO-HNS Criteria for Meniere’s Disease Diagnosis
Major Symptoms
1.Vertigo– Recurrent, well-defined episodes of spinning or rotation • Duration from 20 minutes to
24 hours.– Nystagmus associated with attacks– Nausea and vomiting during vertigo spells common– No neurologic symptoms with vertigo
1.Deafness– Hearing deficits fluctuate– Sensorineural hearing loss– Hearing loss progressive, usually unilateral
1.Tinnitus– Variable, often low-pitched and louder during attacks – Usually unilateral– Subjective
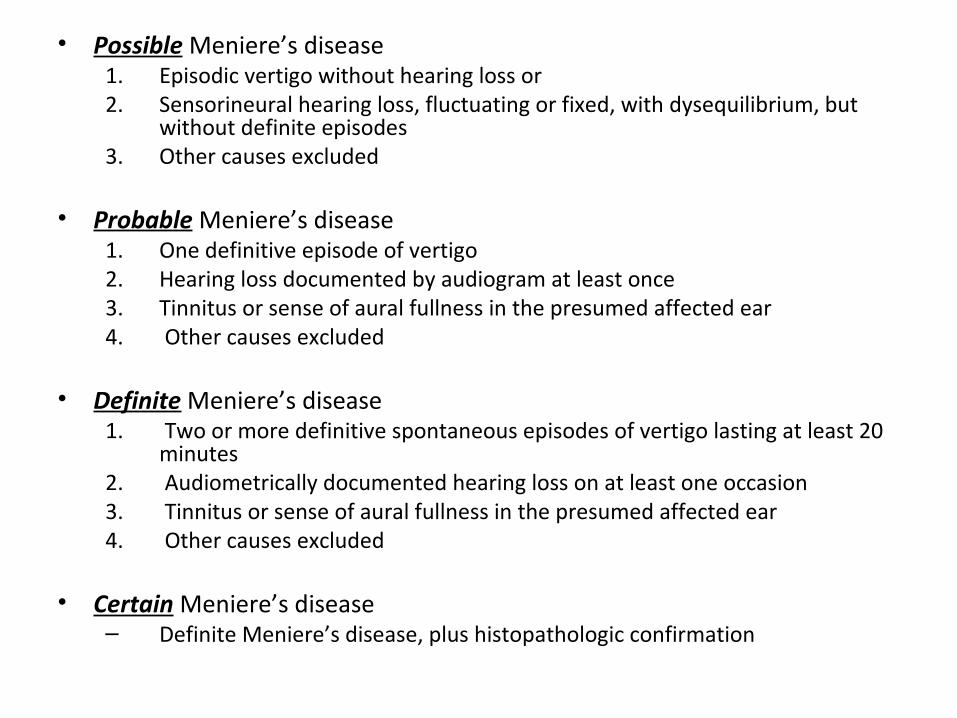
• Possible Meniere’s disease1. Episodic vertigo without hearing loss or2. Sensorineural hearing loss, fluctuating or fixed, with dysequilibrium, but
without definite episodes 3. Other causes excluded
• Probable Meniere’s disease1. One definitive episode of vertigo2. Hearing loss documented by audiogram at least once3. Tinnitus or sense of aural fullness in the presumed affected ear 4. Other causes excluded
• Definite Meniere’s disease1. Two or more definitive spontaneous episodes of vertigo lasting at least 20
minutes2. Audiometrically documented hearing loss on at least one occasion3. Tinnitus or sense of aural fullness in the presumed affected ear4. Other causes excluded
• Certain Meniere’s disease– Definite Meniere’s disease, plus histopathologic confirmation
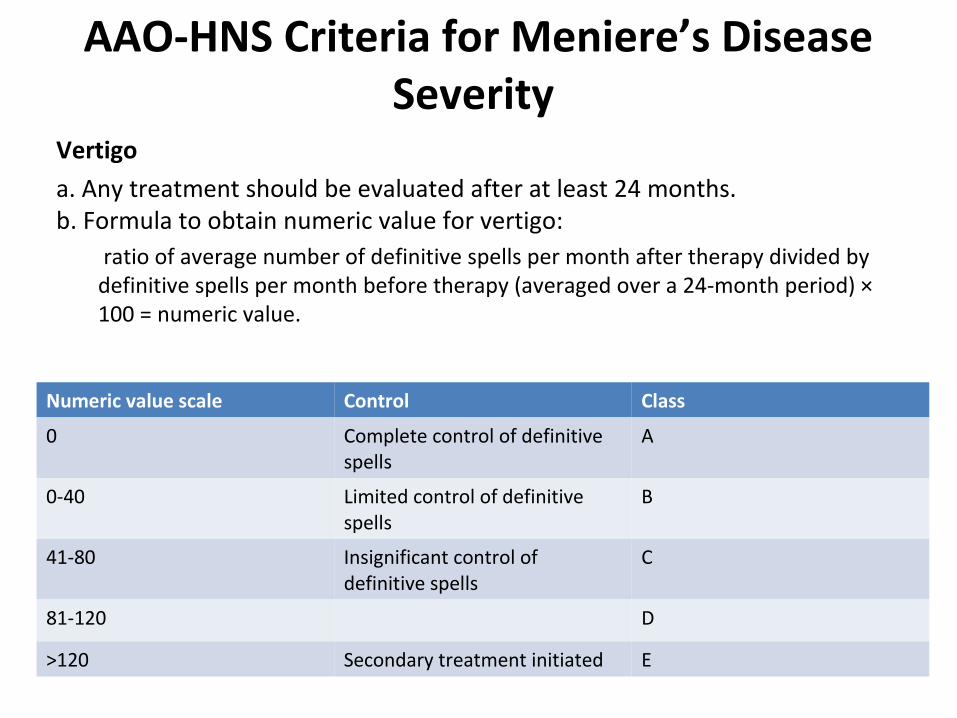
AAO-HNS Criteria for Meniere’s Disease Severity
Vertigo
a. Any treatment should be evaluated after at least 24 months.b. Formula to obtain numeric value for vertigo:
ratio of average number of definitive spells per month after therapy divided by definitive spells per month before therapy (averaged over a 24-month period) × 100 = numeric value.
Numeric value scale Control Class
0 Complete control of definitive spells
A
0-40 Limited control of definitive spells
B
41-80 Insignificant control of definitive spells
C
81-120 D
>120 Secondary treatment initiated E

Disability a. No disability
b. Mild disability: intermittent or continuous dizziness/unsteadiness that precludes working in a hazardous environment.
c. Moderate disability: intermittent or continuous dizziness that results in a sedentary occupation
d. Severe disability: symptoms so severe as to exclude gainful employment
Hearing
• Hearing is measured using a four-frequency pure-tone average (PTA) of 500 Hz, 1 kHz, 2 kHz, and 3 kHz.
• Pretreatment hearing level: worst hearing level during 6 months before therapy
• Post-treatment hearing level: poorest hearing level measured 18-24 months after institution of therapy
• Hearing classification:
i. Unchanged: ≤10-dB PTA improvement or worsening or ≤15% speech discrimination improvement or worsening.
ii. Improved: >10-dB PTA improvement or >15% discrimination improvement
iii. Worse: >10-dB PTA worsening or >15% discrimination worsening

• In 1996, the Committee on Hearing and Equilibrium reaffirmed and clarified the guidelines, adding initial staging and reporting guidelines:
• Initial Hearing Level
Stage Four tone average
1 < 25
2 26-40
3 41-70
4 >70
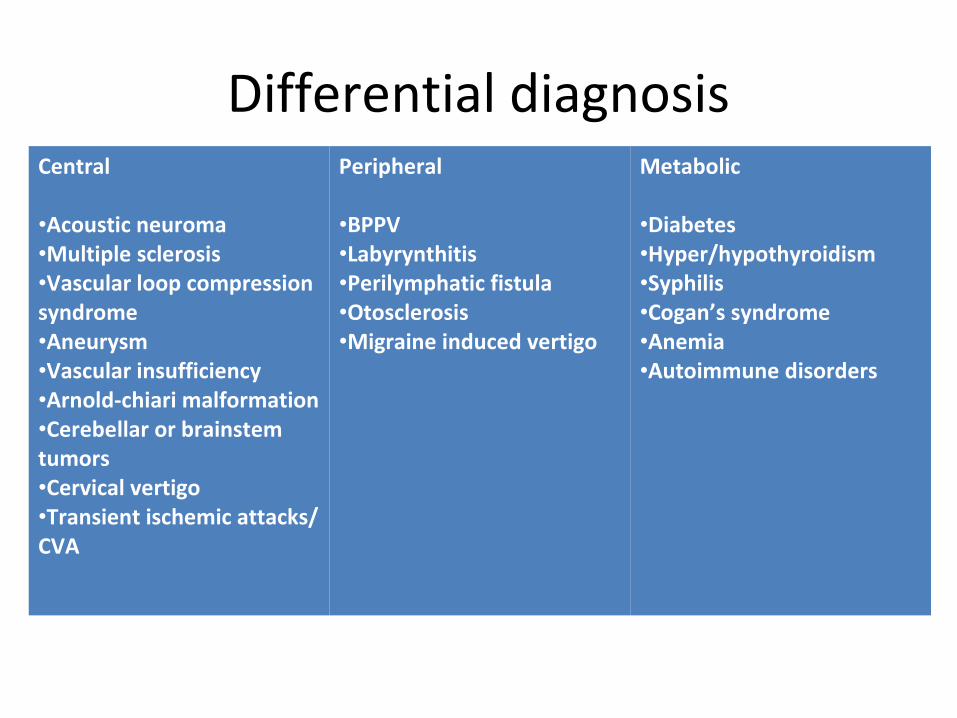
Differential diagnosisCentral
•Acoustic neuroma•Multiple sclerosis•Vascular loop compression syndrome•Aneurysm•Vascular insufficiency•Arnold-chiari malformation•Cerebellar or brainstem tumors•Cervical vertigo•Transient ischemic attacks/ CVA
Peripheral
•BPPV•Labyrynthitis•Perilymphatic fistula•Otosclerosis•Migraine induced vertigo
Metabolic
•Diabetes•Hyper/hypothyroidism•Syphilis•Cogan’s syndrome•Anemia•Autoimmune disorders

MANAGEMENT
Other SPECIAL INVESTIGATIONS
• Electronystagmography • Head Thrust Testing • Electrocochleography • Dehydrating Agents • Vestibular evoked Myopotentials
Electronystagmography
• Electrooculographic recordings of eye movements after caloric and rotational stimulation are a commonly available and reliable method of assessing vestibular function.
• The caloric test often can localize the involved ear. A significant caloric response reduction is found in 48% to 73.5% of patients with Meniere’s disease.
• As many as 25% of meniere’s disease patients have no abnormalities
Head Thrust Testing
• The head thrust test popularized by Halmagyi is very sensitive for detection of unilateral vestibular dysfunction.
• However, in Meniere’s disease, the asymmetry is subtle and present in only 29% of the patients.

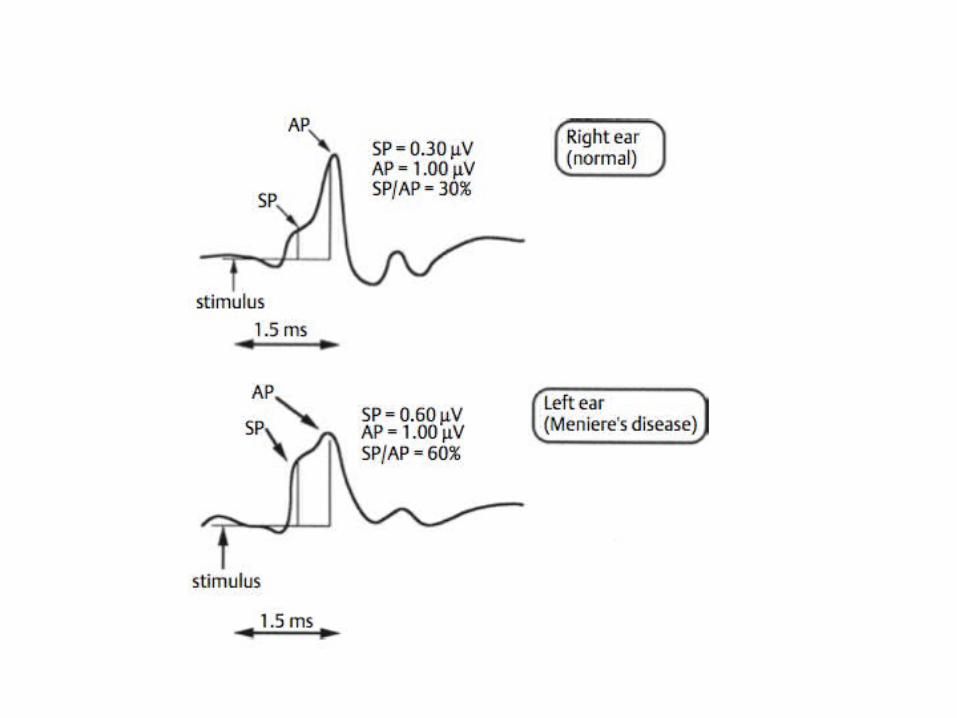
Electrocochleography
• The summating potential (SP) is larger and more negative(( due to distention of the basilar membrane into the scala tympani, causing an increase in the normal asymmetry of its vibration).
• Ratio of amplitudes of the SP and the 8th cranial nerve action potential (AP), the SP/AP ratio.
• The SP becomes relatively larger in hydrops; accordingly, the SP/AP ratio increases; SP:AP > 0.45
• It is not a definitive test, because ratios are elevated in 62% of patients with Meniere’s disease and in 21% of control subjects.

Dehydrating Agents
• Glycerol (1.5ml/kg body weight) : half an hour to one hour intervals with atleast 5dB improvement in three consecutive frequencies.
• Improvement seen with audiometrics, reduction in SP negativity (as recorded with ECoCh), or a change in the gain of the vestibulo-ocular response to rotational stimulation.
Vestibular Evoked Myopotentials
• VEMPs are generated by playing loud clicks in the ear, which move the stapes footplate and stimulate the saccule. This is the start of a disynaptic pathway that passes through the vestibular nuclei and then to synapses that relax the sternocleomastoid muscle.
• The saccule is the second most common site affected by hydrops, which has caused VEMPs to be investigated as a potential diagnostic tool. In the normal ear, the best response is near 500 Hz.
• Ears affected by Meniere’s disease have elevated VEMP thresholds with flattened tuning.
• The interaural amplitude difference in the response has been implicated as a staging tool for Meniere’s disease.
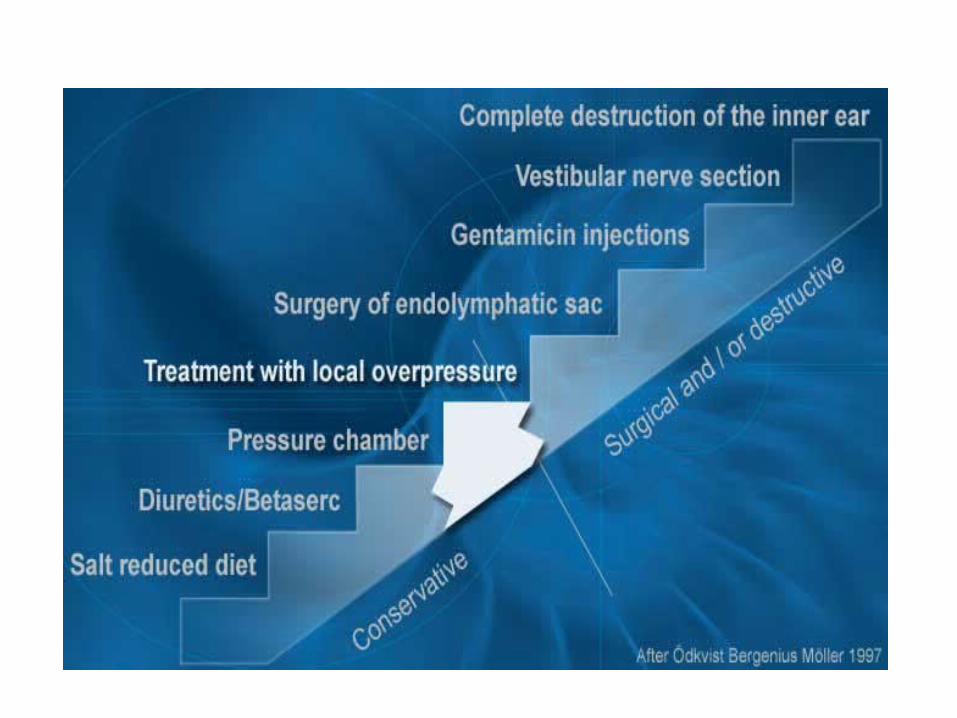

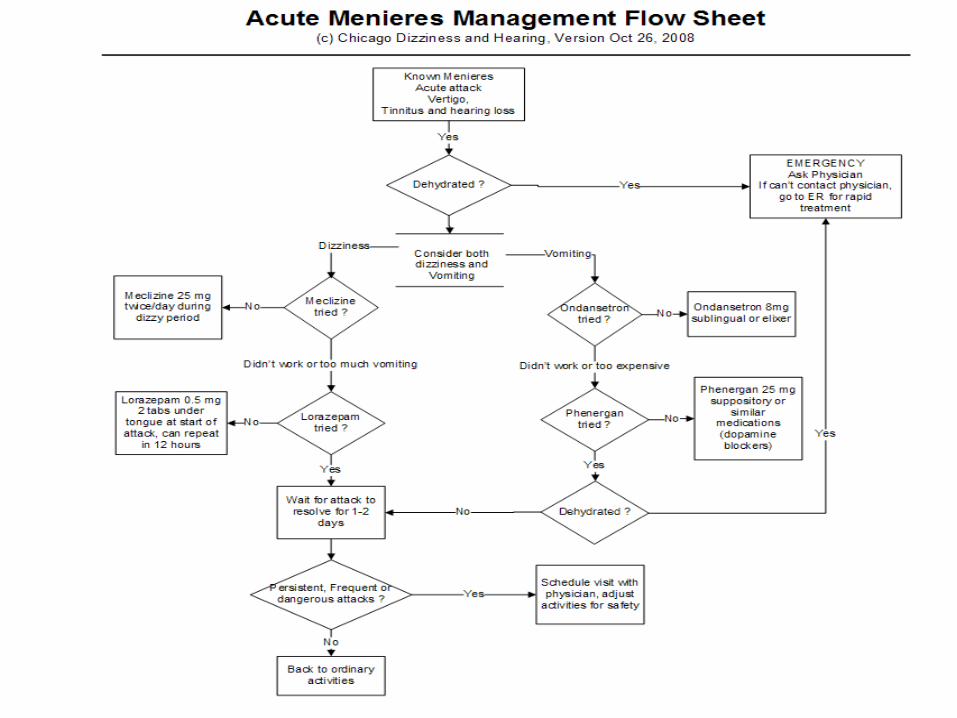
TREATMENT
• Dietary modifications and diuretics• Vasodilators • Symptomatic treatment– Antiverginous medications– Antiemetics– Sedatives– Antidepressants– Psychiatric treament
• Local overpressure therapy
Dietary modifications
• Low sodium (1500 mg) diet (1 month trial)
• Furstenberg diet
• Restriction in caffeine, nicotine and alcohol.
Medications
• Salt wasting diuretic such as diazide (1 month trial)
• Betahistine (2 week trial, often combined with verapamil)– Relaxes the precapillary sphincters and thus improves the
microcirculation of inner ear
– Antivertigo action due to imhibition of massive impulses to the polysynaptic lateral vestibular nucleus)
• Verapamil 30 mg SR (one month trial -- dyazide is stopped)
• Lipoflavins and vitamins ( hypothetical importance )

Local overpressure therapy• Since 2000, the Meniett device has been approved
for use by the U.S. Food and Drug Administration (FDA).
• A randomized controlled trial demonstrated that patients using the Meniett device experienced a significant decrease in vertigo symptoms for the first 3 months of therapy but that findings afterward were similar to those with placebo.
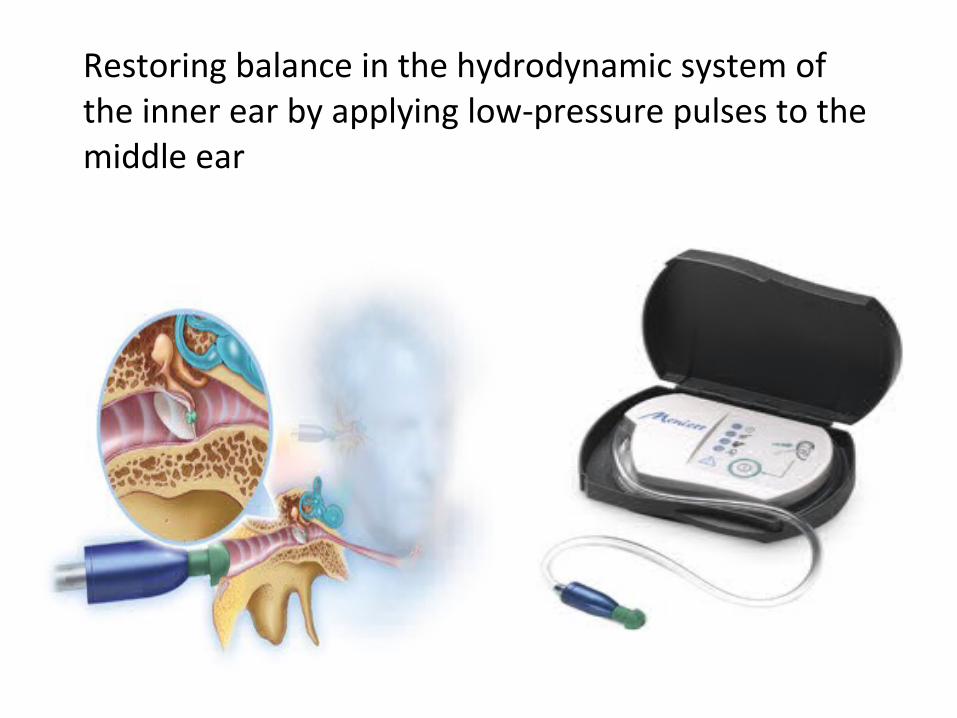
Restoring balance in the hydrodynamic system of the inner ear by applying low-pressure pulses to the middle ear
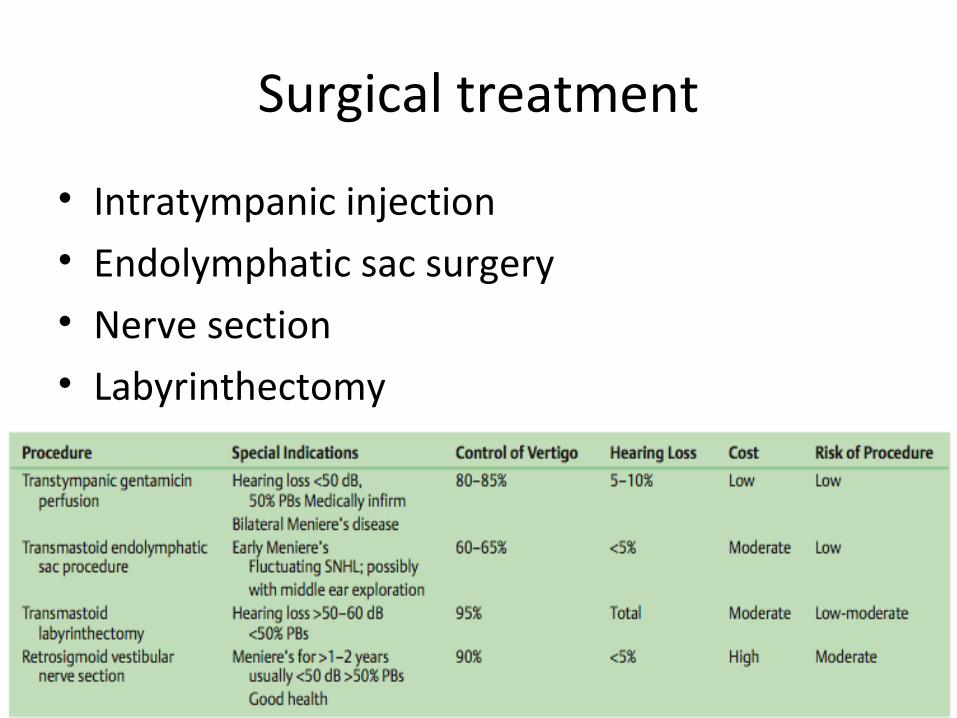
Surgical treatment
• Intratympanic injection• Endolymphatic sac surgery• Nerve section• Labyrinthectomy

Intratympanic Injection
• Intratympanic injection commonly is performed with either dexa- methasone or gentamicin for control of vertigo symptoms.
• The term chemical labyrinthectomy often is applied to intratympanic gentamicin treatment, but it may not be an appropriate assessment of the effect of gentamicin on the labyrinth in titrated therapy.
• Instillation of aminoglycosides into the middle ear was described by Schuknecht in 1957 with streptomycin injection through a microcatheter placed through the tympanic membrane.
• Control of vertigo was achieved in these patients, but severe hearing loss in the treated ear also occurred in most patients.
Dexamethasone
• To be offered when vertigo is intractable but the patient still has some functional hearing.
• The risk of hearing loss or other complications from the steroid injection appears to be low.
• A small randomized trial has shown complete resolution of vertigo symptoms in 82% of patients receiving dexamethasone, compared with 57% receiving saline injection.
• Dexamethasone injections may need to be repeated every 3 months to maintain the patient free of vertigo symptoms, although the optimal dosing frequency is variable and unknown.
• Concentrations used have varied from 2 to 24 mg/mL.
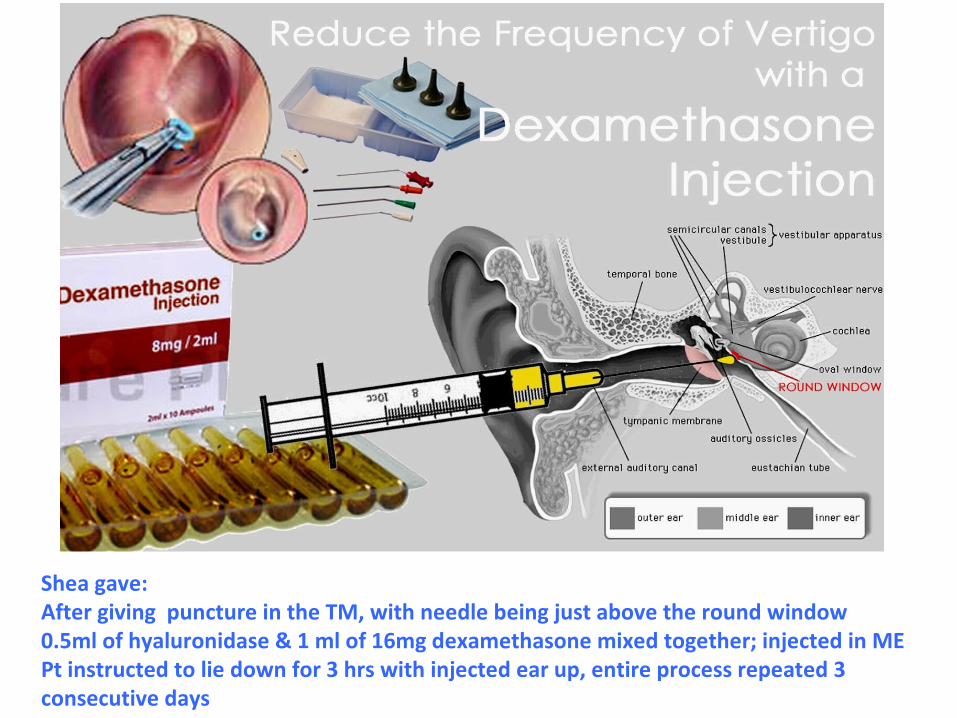
Shea gave:After giving puncture in the TM, with needle being just above the round window0.5ml of hyaluronidase & 1 ml of 16mg dexamethasone mixed together; injected in MEPt instructed to lie down for 3 hrs with injected ear up, entire process repeated 3 consecutive days
Gentamicin
• Has a vestibulotoxicity that is high relative to its cochleotoxicity; accordingly, it can be used to control vestibular symptoms while sparing hearing.
• The gentamicin can be administered through either a tympanostomy tube or directly injected through the tympanic membrane.
• Peripheral vestibular deficits are evident on head thrust testing after even a single dose of gentamicin
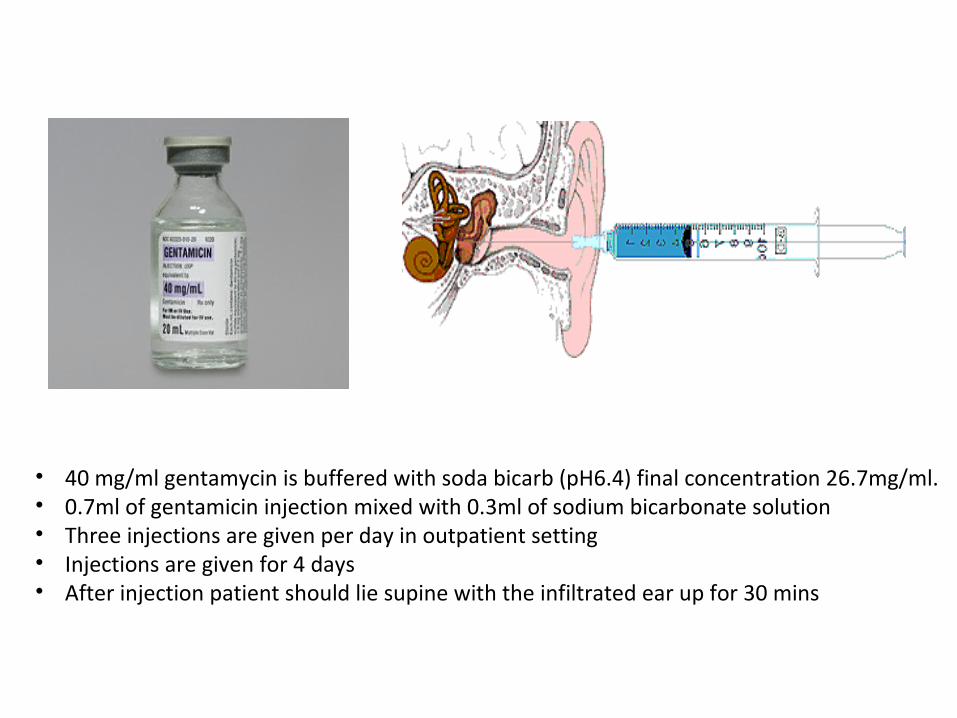
• 40 mg/ml gentamycin is buffered with soda bicarb (pH6.4) final concentration 26.7mg/ml.• 0.7ml of gentamicin injection mixed with 0.3ml of sodium bicarbonate solution• Three injections are given per day in outpatient setting• Injections are given for 4 days• After injection patient should lie supine with the infiltrated ear up for 30 mins
• The current trend is away from multiple doses of gentamicin and toward a single-injection regimen, with additional doses only if needed to control symptoms (so-called titration therapy).
• The risk of hearing loss with gentamicin using many current protocols is similar to that with the natural history of Meniere’s disease.
Nerve section
1.Translabyrinthine vestibular neurectomy
2.Retrolabyrinthine vestibular neurinectomy
3.Retrosigmoid vestibular neurinectomy
4.Middle cranial fossa vestibular neurinectomy
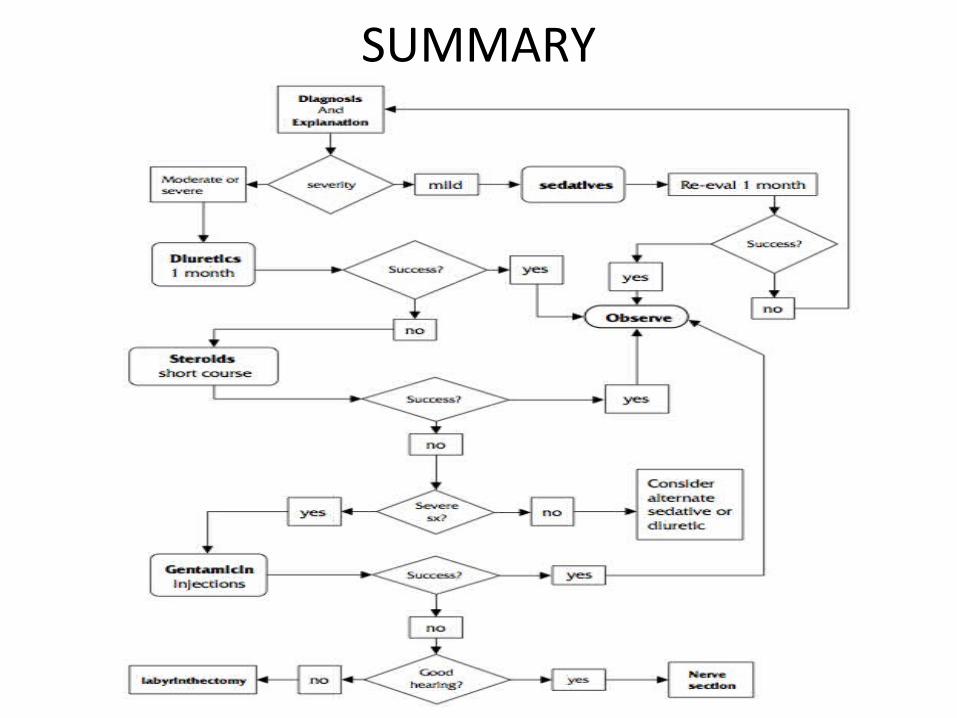
SUMMARY

Prognosis
• Prognosis is variable, since the disease pattern of exacerbation and remission makes evaluation of treatment and prognosis difficult to predict.
– In general, Ménière symptoms tend to stabilize spontaneously with time. With regard to vertigo, about half of patients stabilize over several years.
– Patients tend to "burn out" over time and with residual poor balance and hearing.








![Index [link.springer.com]978-1-4612-4068-6/1.pdf · Index Different species ... effect of ototoxic drugs, 124, 126-129 effects of salicylate, 219-220 ... Meniere's disease animal](https://static.documents.pub/doc/80x56/5b15d6707f8b9a5b4b8baf49/index-link-978-1-4612-4068-61pdf-index-different-species-effect-of.jpg)









