MAVENCLAD® provides a low monitoring burden compared to currently approved disease-modifying drugs for relapsing MS. Pregnancy planning can begin 6 months after the last dose in second year of treatment1, 10-13
M O N I T O R I N G A N DP R E G N A N C Y P L A N N I N G
MAVENCLAD® depletes B and T lymphocytes and selectively reconstitutes the immune system with minimal impact on innate immune function. It was shown to induce a selective and transient lymphocyte depletion followed by a distinct pattern of lymphocyte reconstitution1, 3, 5-9
M E C H A N I S M O F A C T I O N ( M O A )
MAVENCLAD® is a disease-modifying therapy that can deliver clinical and radiological effects with a maximum of 20 days of oral treatment in the first 2 years.Almost 1 of 2 patients had no evidence of disease activity at the end of the 2-year study, after a maximum of 20 days of oral treatment1-4
E F F I C A C Y
What is the clinical evidence for MAVENCLAD®?
MAVENCLAD® use is supported by over 12 years of clinical experience in MS.3, 4, 14-18 Over 2,000 patients were included in the clinical programme, exceeding 10,000 patient-years of experience.3, 16, 18-21
MAVENCLAD® has a well-characterised safety profile, with 8 years of safety registry experience up to August 2017 and no reported cases of PML or risk of secondary autoimmunity.1, 18
• In August 2017, the European Commission granted Marketing Authorization for
MAVENCLAD® for the treatment of adult patients with highly active relapsing multiple
sclerosis (RMS) as defined by clinical or imaging features.1
• MAVENCLAD® is the first short-course oral therapy for relapsing forms of MS.
About MAVENCLAD®
(Cladribine Tablets)
*Patients treated with MAVENCLAD® 3.5 mg/kg in the CLARITY trial
~4 out of 5*Free of relapses
~9 out of 10* Free of disability progression
~1 out of 2* No evidence of disease activity
At 4 years…
~7 out of 10* Remain relapse-free
Date: August 2017
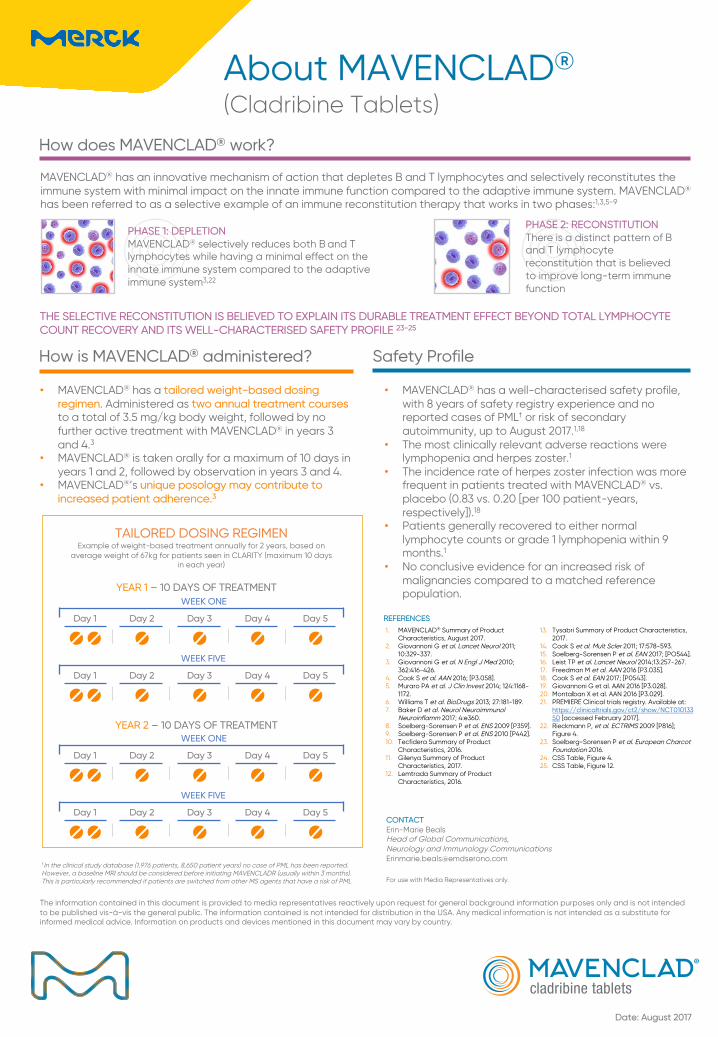
MAVENCLAD® has an innovative mechanism of action that depletes B and T lymphocytes and selectively reconstitutes the immune system with minimal impact on the innate immune function compared to the adaptive immune system. MAVENCLAD®
has been referred to as a selective example of an immune reconstitution therapy that works in two phases:1,3,5-9
PHASE 1: DEPLETION MAVENCLAD® selectively reduces both B and T lymphocytes while having a minimal effect on the innate immune system compared to the adaptive immune system3,22
PHASE 2: RECONSTITUTIONThere is a distinct pattern of B and T lymphocyte reconstitution that is believed to improve long-term immune function
THE SELECTIVE RECONSTITUTION IS BELIEVED TO EXPLAIN ITS DURABLE TREATMENT EFFECT BEYOND TOTAL LYMPHOCYTE COUNT RECOVERY AND ITS WELL-CHARACTERISED SAFETY PROFILE 23-25
About MAVENCLAD®
(Cladribine Tablets)
How does MAVENCLAD® work?
How is MAVENCLAD® administered?
• MAVENCLAD® has a tailored weight-based dosing regimen. Administered as two annual treatment coursesto a total of 3.5 mg/kg body weight, followed by no further active treatment with MAVENCLAD® in years 3 and 4.3
• MAVENCLAD® is taken orally for a maximum of 10 days in years 1 and 2, followed by observation in years 3 and 4.
• MAVENCLAD®’s unique posology may contribute to increased patient adherence.3
Safety Profile
• MAVENCLAD® has a well-characterised safety profile, with 8 years of safety registry experience and no reported cases of PML† or risk of secondary autoimmunity, up to August 2017.1,18
• The most clinically relevant adverse reactions were lymphopenia and herpes zoster.1
• The incidence rate of herpes zoster infection was more frequent in patients treated with MAVENCLAD® vs. placebo (0.83 vs. 0.20 [per 100 patient-years, respectively]).18
• Patients generally recovered to either normal lymphocyte counts or grade 1 lymphopenia within 9 months.1
• No conclusive evidence for an increased risk of malignancies compared to a matched reference population.
†In the clinical study database (1,976 patients, 8,650 patient years) no case of PML has been reported. However, a baseline MRI should be considered before initiating MAVENCLADR (usually within 3 months). This is particularly recommended if patients are switched from other MS agents that have a risk of PML
CONTACTErin-Marie BealsHead of Global Communications, Neurology and Immunology [email protected]
YEAR 2 – 10 DAYS OF TREATMENT
TAILORED DOSING REGIMENExample of weight-based treatment annually for 2 years, based on
average weight of 67kg for patients seen in CLARITY (maximum 10 days in each year)
YEAR 1 – 10 DAYS OF TREATMENTWEEK ONE
Day 1 Day 2 Day 3 Day 4 Day 5
WEEK FIVE
Day 1 Day 2 Day 3 Day 4 Day 5
WEEK ONE
Day 1 Day 2 Day 3 Day 4 Day 5
WEEK FIVE
Day 1 Day 2 Day 3 Day 4 Day 5
The information contained in this document is provided to media representatives reactively upon request for general background information purposes only and is not intended to be published vis-à-vis the general public. The information contained is not intended for distribution in the USA. Any medical information is not intended as a substitute for informed medical advice. Information on products and devices mentioned in this document may vary by country.
For use with Media Representatives only.
1. MAVENCLAD® Summary of Product Characteristics, August 2017.
2. Giovannoni G et al. Lancet Neurol 2011; 10:329-337.
3. Giovannoni G et al. N Engl J Med 2010; 362:416-426.
4. Cook S et al. AAN 2016; [P3.058].5. Muraro PA et al. J Clin Invest 2014; 124:1168-
1172.6. Williams T et al. BioDrugs 2013; 27:181-189.7. Baker D et al. Neurol Neuroimmunol
Neuroinflamm 2017; 4:e360.8. Soelberg-Sorensen P et al. ENS 2009 [P359].9. Soelberg-Sorensen P et al. ENS 2010 [P442].10. Tecfidera Summary of Product
Characteristics, 2016.11. Gilenya Summary of Product
Characteristics, 2017.12. Lemtrada Summary of Product
Characteristics, 2016.
13. Tysabri Summary of Product Characteristics, 2017.
14. Cook S et al. Mult Scler 2011; 17:578-593.15. Soelberg-Sorensen P et al. EAN 2017; [PO544].16. Leist TP et al. Lancet Neurol 2014;13:257-267.17. Freedman M et al. AAN 2016 [P3.035].18. Cook S et al. EAN 2017; [P0543].19. Giovannoni G et al. AAN 2016 [P3.028].20. Montalban X et al. AAN 2016 [P3.029].21. PREMIERE Clinical trials registry. Available at:
https://clinicaltrials.gov/ct2/show/NCT01013350 [accessed February 2017].
22. Rieckmann P, et al. ECTRIMS 2009 [P816]; Figure 4.
23. Soelberg-Sorensen P et al. European Charcot Foundation 2016.