25
MERS-CoV: Extent of infection in & transmission to humans Maria Van Kerkhove, PhD Center for Global Health, Institut Pasteur, Paris ESCAIDE 13 November 2015
| Date post: | 18-Feb-2017 |
| Category: |
Health & Medicine |
| Upload: | european-centre-for-disease-prevention-and-control |
| View: | 369 times |
| Download: | 1 times |

MERS-CoV: Extent of infection in &
transmission to humans
Maria Van Kerkhove, PhD
Center for Global Health, Institut Pasteur, Paris
ESCAIDE 13 November 2015

MERS-CoV: What we know
>1611 cases reported from 26 countries, >575 deaths
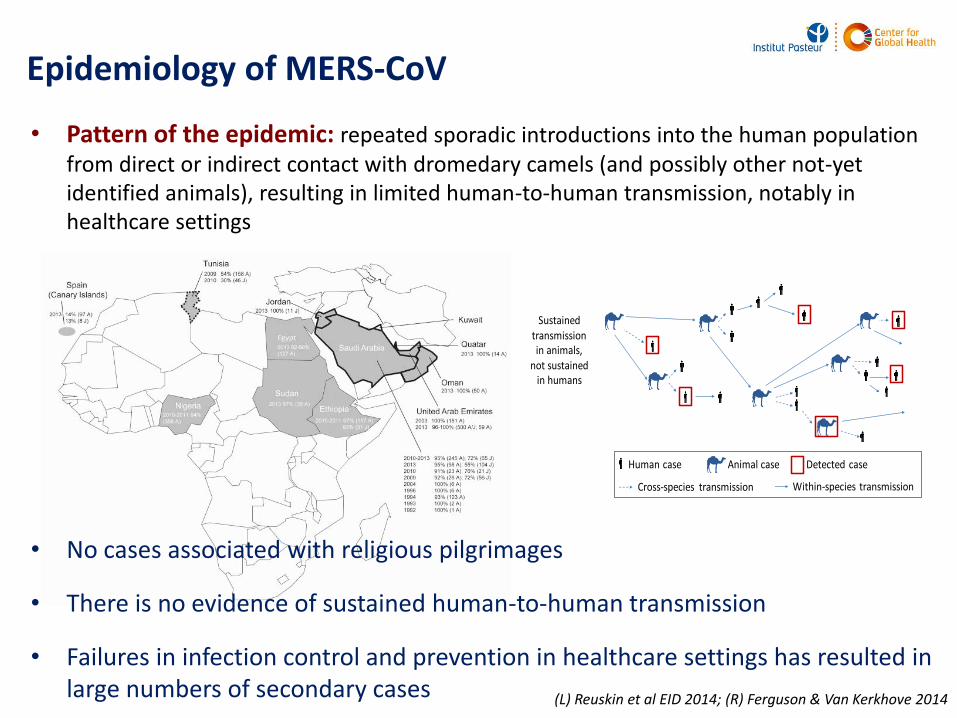
Epidemiology of MERS-CoV
Sustained transmission
in humans
Sustained transmission in animals,
not sustained in humans
Human case Detected case
Cross-species transmission Within-species transmission
Animal case
(L) Reuskin et al EID 2014; (R) Ferguson & Van Kerkhove 2014
• Pattern of the epidemic: repeated sporadic introductions into the human population from direct or indirect contact with dromedary camels (and possibly other not-yet identified animals), resulting in limited human-to-human transmission, notably in healthcare settings
• No cases associated with religious pilgrimages
• There is no evidence of sustained human-to-human transmission
• Failures in infection control and prevention in healthcare settings has resulted in large numbers of secondary cases
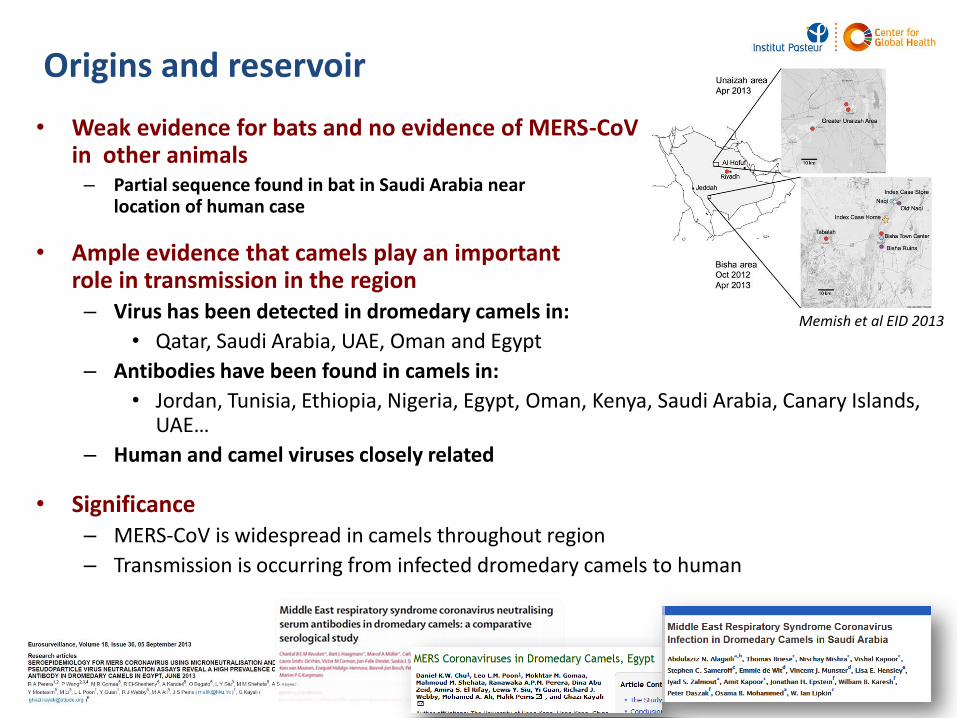
• Weak evidence for bats and no evidence of MERS-CoVin other animals– Partial sequence found in bat in Saudi Arabia near
location of human case
• Ample evidence that camels play an important role in transmission in the region – Virus has been detected in dromedary camels in:
• Qatar, Saudi Arabia, UAE, Oman and Egypt
– Antibodies have been found in camels in:
• Jordan, Tunisia, Ethiopia, Nigeria, Egypt, Oman, Kenya, Saudi Arabia, Canary Islands, UAE…
– Human and camel viruses closely related
• Significance– MERS-CoV is widespread in camels throughout region
– Transmission is occurring from infected dromedary camels to human
Origins and reservoir
Memish et al EID 2013

Emergence and transmissibility
• Phylogenetics
– More human and animal genetic sequences are becoming available
– Likely emergence mid 2012 though possible similar virus circulating in animals for decades
– Genetic data support multiple introductions into human populations
• Transmissibility of MERS-CoV
– R0 is likely <1*
– Significant heterogeneity in R
– Higher attack rates in specific settings, e.g., health care settings
R0=reproduction number: the average number of secondary cases generated from 1 case at the start of an epidemic*Brenan et al 2013; Cauchemez et al 2014
Cotton et al 2014
What we don’t know….
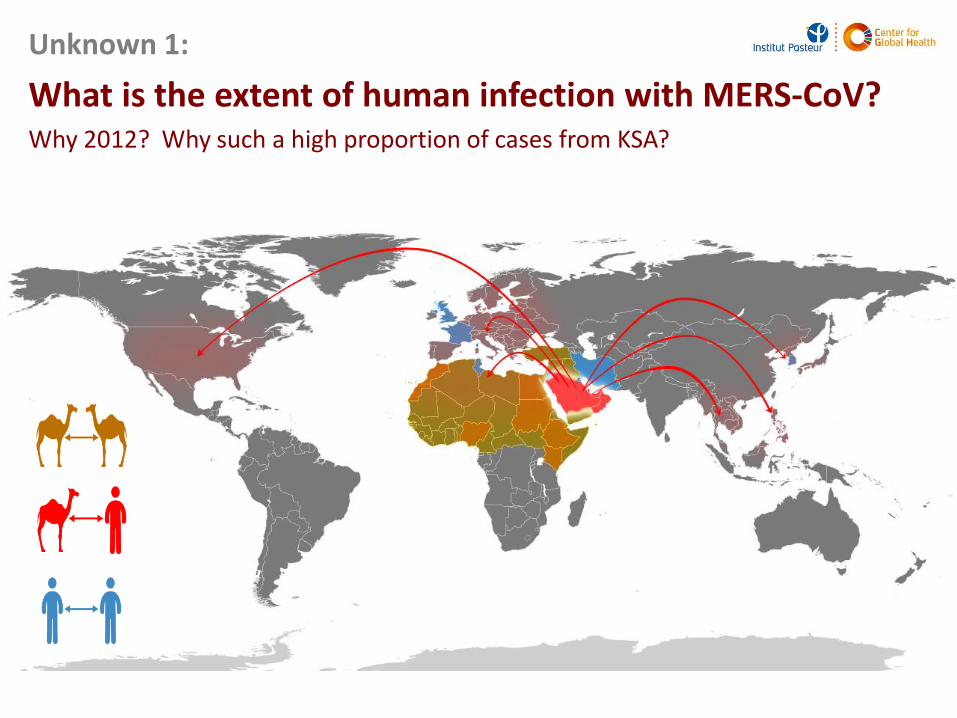
Unknown 1:
What is the extent of human infection with MERS-CoV?Why 2012? Why such a high proportion of cases from KSA?

Surveillance for MERS
• Significant variation in surveillance for MERS-CoV within and outside of the Middle East– Testing uneven between countries
– Testing uneven over the course of the year
– Noncompliance with surveillance recommendations from WHO
• Notable increases in efforts to monitor for MERS during Hajj– To date, not a single case associated with Hajj (or Umrah)*
– Modelling estimates very few cases associated with Hajj due to reduced amount of time spent in KSA**
• And also due to the nature of activities of pilgrims
– Worry is visits to health care facilities or camel contact
*Waldrom and Doherty 2015; Kumar et al 2015; Barasheed et al 2015; Aberle et al 2015; Annan et al 2015; Barasheed et al 2014; Benkouitenet al 2014; Gautret et al 2014; Memish et al 2014** Lessler et al 2014
Clues from human epidemiologic studies…
• Numerous seroepidemiologic studies have now been undertaken in several countries including KSA, Qatar, Jordan, Egypt, UAE
– Significantly higher seroprevalence in populations with close, regular and direct contact with dromedary camels
– Only one large population based serosurvey (samples from 2012-2013)*
• 0.2% of general population found to be seropositive
• Significance?
– Likely missing mild cases
– Likely these sub-clinical infections play a (silent) role in transmission in the community
*Müller et al Lancet ID 2015
How are humans infected with MERS-CoVfrom contact with dromedary camels?
Unknown 2:
Photo credit: EPA
Photo credit: Green Prophet News

Some answers from epidemiologic studies (1)
• Risk factors for transmission between camels and humans– Case-control study from KSA* 30 primary cases/116 controls matched
on age, sex and neighborhood• found that direct and non-direct contact with dromedary camels are significantly
associated with infection
• Diabetes, heart disease and smoking independently associated with MERS illness
* Alraddadi et al EID 2016
Exposure OR, 95% CI
Univariate
Direct dromedary contact 3.7, 1.4-11.8
Kept dromedaries in or around home 3.3 ,1.04-10.98
milked dromedaries 10.4, 2.5-inf
Visited farm where dromedaries were present 11.6, 2.7-inf
Live in same household as someone who had visited farm with dromedaries or had direct contact with dromedary camel while there
3.95, 1.2-13.75.0, 1.66-16.9
No increased risk for food consumption, unpasteurized animal milk, camel urine ---
Multivariate
Direct dromedary Exposure aOR 7.5, 1.6-35.3

Some answers from epidemiologic studies (2)
• Risk factors for occupationally exposed individuals– Higher seroprevalence among occupationally exposed individuals, but
risk factors for infection not evaluated
– Many more studies have been/are being conducted
• Many studies are not-yet published
• None have addressed this fundamental question

What improvements are required?
• Improvements in case investigations are urgently needed
– All human cases of MERS-CoV need to be thoroughly investigated
– Including
• Immediate notification of health sector to animal sector if human case reports direct or indirect camel exposure
• Joint animal and human investigations for all community acquired cases
• Monitoring and testing of all contacts regardless of symptoms
• Tracing and testing of animals
• Reporting of follow up for both animal and human investigations
• If PCR positive camel identified, animal sector should inform human sector
– Reporting of PCR positive camels to OIE (Doha Declaration)
• Improvements in prospective studies

Unknown 3:
Nosocomial outbreaks continue to occur, and are unnecessary
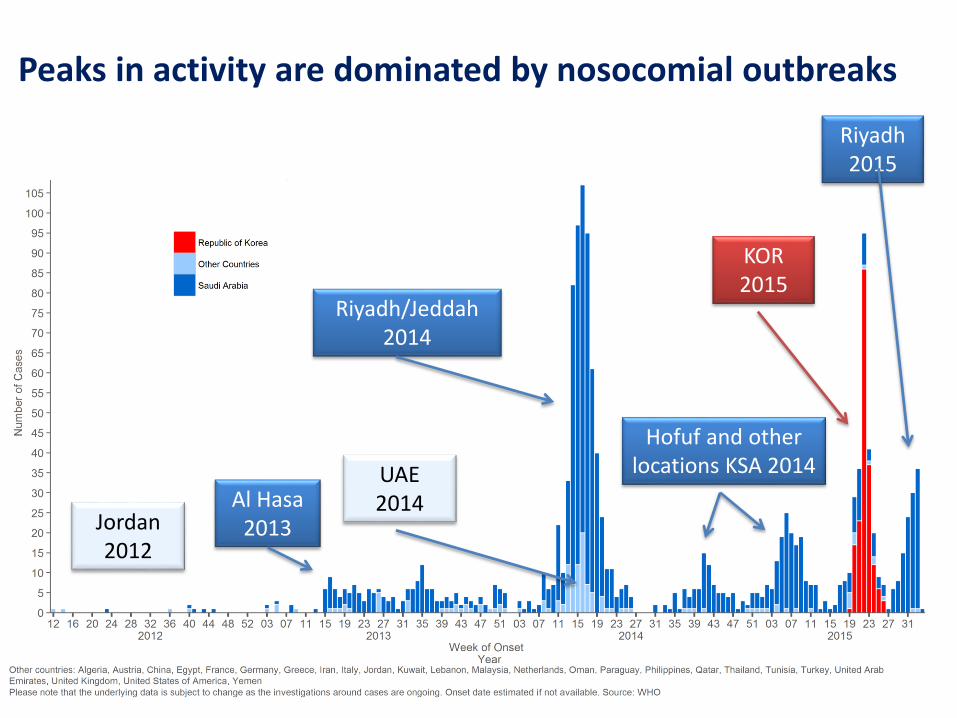
Peaks in activity are dominated by nosocomial outbreaks
Riyadh/Jeddah 2014
UAE 2014
Riyadh 2015
KOR 2015
Hofuf and other locations KSA 2014
Al Hasa2013Jordan
2012

Why are nosocomial outbreaks happening?
• Lack of awareness, slow isolation of suspected patients
– Over crowding in emergency departments
– Basic IPC not adequate
– Slow triage/isolation
• Recommendations not being implemented
• Cultural differences in health seeking behavior
Republic of Korea 14 Health Care
Facilities186 Cases
0
2
4
6
8
10
12
14
16
18
20
8-M
ay
9-M
ay
10-M
ay
11-M
ay
12-M
ay
13-M
ay
14-M
ay
15-M
ay
16-M
ay
17-M
ay
18-M
ay
19-M
ay
20-M
ay
21-M
ay
22-M
ay
23-M
ay
24-M
ay
25-M
ay
26-M
ay
27-M
ay
28-M
ay
29-M
ay
30-M
ay
31-M
ay
1-Jun
2-Jun
3-Jun
4-Jun
5-Jun
6-Jun
7-Jun
8-Jun
9-Jun
10-Jun
11-Jun
12-Jun
13-Jun
14-Jun
15-Jun
16-Jun
17-Jun
18-Jun
19-Jun
20-Jun
21-Jun
22-Jun
23-Jun
24-Jun
25-Jun
26-Jun
27-Jun
28-Jun
29-Jun
30-Jun
1-Jul
2-Jul
3-Jul
Numberofcases
Dateofsymptomonset
RepublicofKorea China Death
Source: Korean Ministry of Health/WHO

HAS THE VIRUS CHANGED?
Unknown 4:
Source: http://dj.kbs.co.kr/resources/2015-06-04/
KCDC, Osong PH Res Perspect 2015

H2H transmission in hospitals
• “Super spreading” events in Korea and in KSA
– 83% of cases in Korea linked to 5 cases
– Not super spreaders – combination of events resulting in amplification in transmission between people
– Role of asymptomatic health care workers
• Role of environmental contamination
– Likely playing a role in nosocomial outbreaks
• Surface contamination
• Air samples
– Likely playing a role in community acquired infections
• Occupationally exposed persons
• Owners/household members of owners
Lee and Wong, IJID 2015
Clustering events
• Clusters of cases among household and “household” contacts
– Limited H2H transmission in households*
– Cluster among expat workers in Riyadh October 2015
*Drosten et al NEJM 2014**KSA CCC Weekly Monitor
Prince Mohammed bin AbdulAziz Hospital
Challenges: Addressing community acquired infections

Epidemiologic investigations in animals and humans are/have been conducted. However…
• Not all results have been publically released and these results are critical
– Develop risk communication materials to protect human health
– Develop specific mitigation measures to prevent human infections from camel exposure
– Design specific epidemiologic studies in at risk populations to evaluate risk factors for camel to human transmission
• Cross-sectional/Longitudinal epidemiologic studies of humans, animals and the environment
– In the Arabian Peninsula and across the region
– Include serology and genetic sequencing in outbreak investigations

How can we stop camel-to-human transmission?
• Active surveillance in animals and humans
• Intensive and joint animal/human investigations for every case (public trust)
• Clear guidance for at risk populations
• Coordinated, multi-site, inter-sectorial human/camel research is needed to better understand transmission patterns
Challenges: Addressing nosocomial outbreaks
• More nosocomial outbreaks are expected – these can be prevented
• Increasing awareness of MERS, especially in countries with close ties to KSA
– for suspicion of MERS
– For early(ier) isolation of suspected MERS patients
• Improvements in basic infection prevention and control procedures, particularly in emergency departments
• More consistent testing of close contacts, especially health care workers and cleaners
• Training in incident management
• Improvement in communication
– Between both public and private hospitals
– In risk communication to general public, to health care providers and to specific occupational groups
Some answers, more questions…
• What is the extent of human infection?– Are asymptomatic laboratory confirmed cases acting as carriers and playing a
significant role in transmission in nosocomial outbreaks? In the community?
– Why 2012 and why so many cases reported from KSA?
• How are humans infected with MERS?– Clues but no definitive answers
– What is the role of environmental contamination?
• How do we stop camel to human transmission?– Is a camel vaccine the answer?
– Can dromedary camels with neutralizing antibodies be re-infected and infectious?
• Why are we still seeing significant nosocomial outbreaks when basic IPC measures can prevent H2H transmission?– Is the virus changing?

Thank you
Special thanks to the WHO MERS-CoV Task Force in HQ/EMRO/WPRO, especially Peter Ben Embarek, Outbreak, Dalia Samhouri, Mamun Malik, Sylvie
Briand, Keiji Fukuda, Ailan Li, CK Lee and many many others
KSA Ministry of Health: Dr Abdul Aziz Bin Saeed, Dr Abdullah Assiri, Hassan Elbushra, FETP Residents









![Molecular aspects of MERS-CoVMERS-CoV overview Middle East respiratory syndrome coronavirus (MERS-CoV) is a betacoronavirus which can cause acute respiratoryillnessinhumans[1].Likeothercoronaviruses,](https://static.documents.pub/doc/80x56/5f2a06d303b0de56cb3de662/molecular-aspects-of-mers-cov-mers-cov-overview-middle-east-respiratory-syndrome.jpg)







