Meta-analysis shows limited evidence for using Lactobacillus acidophilus LBto treat acute gastroenteritis in childrenHania Szajewska ([email protected])1, Marek Ruszczyński1, Sanja Kolaček2
1.Department of Paediatrics, The Medical University of Warsaw, Warsaw, Poland2.University Department of Paediatrics, Children’s Hospital Zagreb, Zagreb, Croatia
CorrespondenceProfessor Hania Szajewska, MD, Department ofPaediatrics, The Medical University of Warsaw,Dzialdowska 1, 01-184 Warsaw, Poland.Tel/Fax: +48 22 452 33 09 |Email: [email protected]
Received24 September 2013; revised 15 October 2013;accepted 28 October 2013.
DOI:10.1111/apa.12487
ABSTRACTA meta-analysis of four randomised controlled trials of varying methodological quality,
involving 304 children aged 1–48 months, showed that Lactobacillus acidophilus LB (LB)
reduced the duration of diarrhoea in hospitalised, but not outpatient, children compared
with a placebo. The chance of a cure on day three was similar in both groups, but LB
increased the chance of cure on day four.
Conclusion: There is limited evidence to recommend LB for treating paediatric diarrhoea.
INTRODUCTIONAcute gastroenteritis (AGE) is one of the most commondiseases in children. In 2008, the European Society forPaediatric Gastroenterology, Hepatology and Nutrition(ESPGHAN) and the European Society of PaediatricInfectious Diseases (ESPID) introduced evidence-basedguidelines for the management of AGE in children inEurope. The authors of these guidelines concluded that theprimary treatment for AGE is rehydration and nutrition.However, other therapies, including probiotics, are com-monly used. With regard to probiotics, ESPGHAN/ESPIDrecommended that probiotics with documented efficacy,such as Lactobacillus rhamnosus GG or Saccharomycesboulardii, may be considered as an adjunct to rehydration
for the management of AGE in children. Other probiotics,or antidiarrhoeal drugs, also may be used provided theirefficacy is documented in high-quality randomised con-trolled trials (RCTs) or in meta-analyses (1).
In many countries, a product containing lyophilised,heat-inactivated cultures of Lactobacillus acidophilus LB,hereafter, referred to as L. acidophilus LB, plus their spentculture medium is available. Although current guidelines donot provide specific recommendations with regard toL. acidophilus LB (1–3), it is frequently used for the
Abbreviations
AGE, Acute gastroenteritis; CFU, Colony-forming units; CI,Confidence interval; ESPGHAN, European Society for PaediatricGastroenterology, Hepatology and Nutrition; ESPID, EuropeanSociety of Paediatric Infectious Diseases; MD, Mean difference;RCT, Randomised controlled trials; RR, Relative risk.
Key notes� In many countries, a product containing lyophilised,
heat-inactivated L. acidophilus LB (LB) is frequentlyused to treat acute gastroenteritis in children, despite alack of specific recommendations in the current guide-lines.
� This meta-analysis of 304 children shows that LBreduced the duration of diarrhoea in inpatients.
� Given the limited data and the methodological limita-tions of the included trials, the evidence examined inthis article should be viewed with caution.
treatment of AGE in children. The exact mechanisms bywhich L. acidophilus LB might exert its actions on diar-rhoeal diseases are unclear. However, a number of actionshave been postulated. Firstly, L. acidophilus LB, similar toother lactobacilli, has been reported to inhibit adhesion toand invasion of human epithelial cells by enterovirulentmicro-organisms (4,5). Secondly, L. acidophilus LBsecretes a heat-stable antimicrobial compound differentfrom lactic acid (6). It has been documented that both liveand heat-inactivated cultures and a two-fold concentrated,cell-free culture supernatant of L. acidophilus LB showedantibiotic-like activity against enterovirulent bacteria (7,8).Thirdly, L. acidophilus LB stimulates specific immuneresponses to pathogens (6).
Our aim here was to systematically review data on theeffectiveness of L. acidophilus LB compared with placeboor no treatment in the management of AGE in children.This review was initiated as part of the update of theguidelines for the management of AGE in children (1).
METHODSFor this systematic review, we followed the same method-ology developed by the Cochrane Collaboration (9). Inbrief, RCTs that compared the use of L. acidophilus LBwith a placebo or no treatment were eligible for inclusion.The primary outcome measures were stool output and theduration of diarrhoea, measured by time until permanentcessation. In addition to these outcomes, a priori wedecided to extract other data reported by the investigatorsif clinically relevant to the current review.
The Cochrane Central Register of Controlled Trials(CENTRAL, the Cochrane Library), MEDLINE andEMBASE databases were searched in August 2013. Theprincipal search text word terms and MESH headings usedwere as follows: diarrhea/diarrhoea, diarrh*, gastroenteri-tis, probiotic*, L. acidophilus LB and Lact�eol. No languagerestrictions were imposed. The reference lists from identi-fied studies and key review articles, including previouslypublished systematic reviews with or without a meta-analysis, were also searched to identify any other relevantstudies. The ClinicalTrials.gov website http://clinicaltrials.gov/ and EU Clinical Trials Register website https://www.clinicaltrialsregister.eu were searched for RCTs that wereregistered but not yet published. Certain publication types,such as letters to the editor, abstracts and proceedings fromscientific meetings, were excluded, unless a full set of datawere obtained from the authors. The reviewers used astandardised approach to independently undertake theliterature search, data extraction and quality assessment.The data sought included baseline characteristics of theparticipants, details related to the use of experimental andcontrol interventions including dose and duration, settingand funding. Any disagreements were resolved by discus-sion. The reviewers independently, but without beingblinded to the authors or journal, assessed the risk of biasin the studies that met the inclusion criteria. The CochraneCollaboration’s tool for assessing risk of bias was used,
which includes the following criteria: adequacy of sequencegeneration, allocation concealment and blinding of partic-ipants, personnel and outcome assessors and extent of lossto follow-up. The latter refers to the proportion of patientsin whom the investigators were not able to determineoutcomes, so there were incomplete outcome data. In allcases, an answer of ‘yes’ indicates a low risk of bias and ananswer of ‘no’ indicates a high risk of bias (9).
The dichotomous outcomes, the results from individualstudies and pooled statistics are reported as the risk ratio(RR) between the experimental and control groups with95% confidence intervals (95% CI). The continuous out-comes are reported as the mean difference (MD) betweenthe treatment and control groups with 95% CI. To performa meta-analysis of continuous data using mean differences,one needs to extract the mean values of the outcomes, thestandard deviations of the outcomes and the number ofparticipants in whom the outcome was assessed in each ofthe two groups. In the study by Boulloche et al. (10),missing standard deviations were obtained from a p valueby the method described in the Cochrane Handbook forSystematic Reviews of Interventions (9). If other compar-isons were made, these other arms are not evaluated here.For example, Boulloche et al. additionally compared L. aci-dophilus LB with loperamide.
Heterogeneity was quantified by v2 and I2, which can beinterpreted as the percentage of the total variation betweenstudies that is attributable to heterogeneity rather than tochance. A value of 0% indicates no observed heterogeneity,and larger values show increasing heterogeneity. If heter-ogeneity was not revealed, we present results of only thefixed effects model. If there was substantial heterogeneity(over 50%), all analyses were based on the random effectsmodel. To test for publication bias, we planned to use a testfor asymmetry of the funnel plot proposed by Egger et al.(11). However, the publication bias was not formallyassessed using a funnel plot due to the small number ofstudies (<10) included in the analyses. The data wereanalysed using Review Manager (RevMan) [computerprogram version 5.2. Copenhagen: the Nordic CochraneCentre, the Cochrane Collaboration, 2012].
RESULTSFour RCTs met our inclusion criteria (10,12–14). For thecharacteristics of the included trials, see Table 1. For a flowdiagram, documenting the identification process for eligibletrials, as well as for a table documenting the characteristicsof the excluded trials, with reasons for exclusion, see onlineSupporting Information (Fig. S1 and Table S1).
The four selected studies recruited a total of 304 patients,consisting of 157 in the experimental group and 147 in thecontrol group. One study was performed in Europe(France), and the remaining studies were performed outsideof Europe in Ecuador, Peru and Thailand. Three RCTs werecarried out in inpatients, and one RCT, in outpatients. Thedaily intake of LB ranged from a total of five doses of 1010
colony-forming units (CFU) over 48 h to eight doses of 1010
Szajewska et al. L. acidophilus LB and acute gastroenteritis
CFU over 3 days to nine doses of 1010 CFU for a maximumof four and one half days. In all of the studies, L. acidoph-ilus LB was used in addition to rehydration therapyconsisting of an oral rehydration solution (ORS) and/orintravenous rehydration. All RCTs were placebo-controlled.All included trials had some methodological limitations (seeTable 2). The major limitations were unclear randomisationand no or unclear allocation concealment.
EffectsStool volumeNone of the studies evaluated the effects of L. acidophilusLB on stool volume.
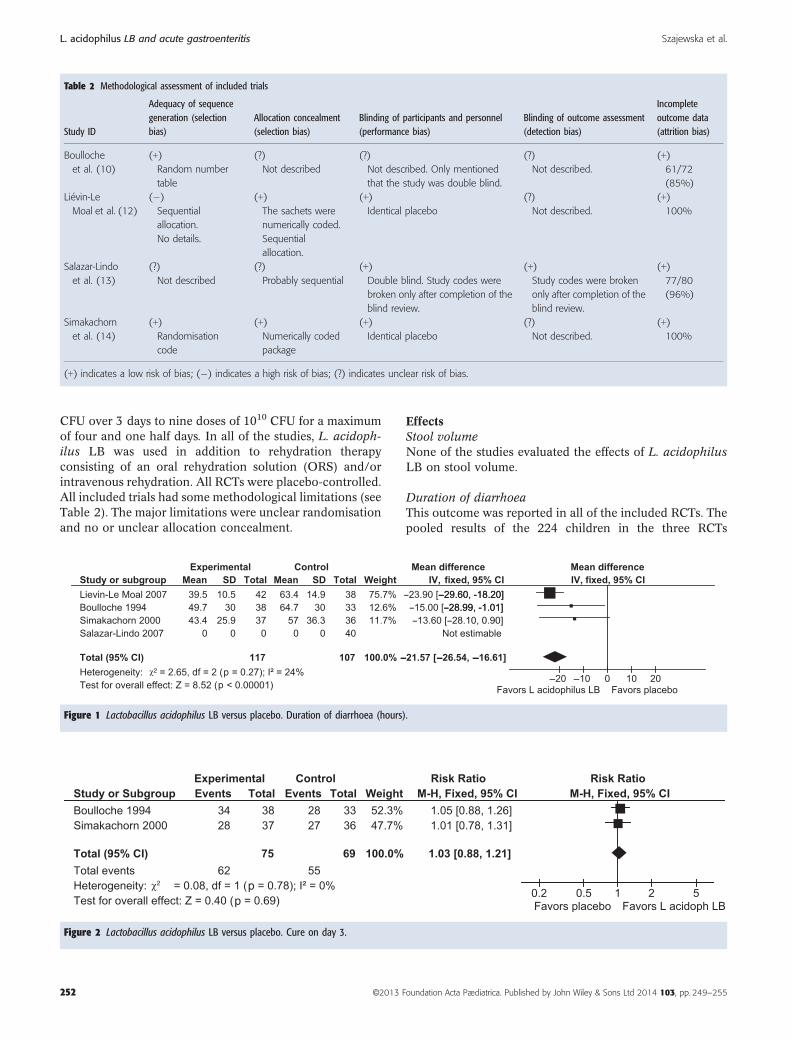
Duration of diarrhoeaThis outcome was reported in all of the included RCTs. Thepooled results of the 224 children in the three RCTs
Table 2 Methodological assessment of included trials
Study ID
Adequacy of sequencegeneration (selectionbias)
Allocation concealment(selection bias)
Blinding of participants and personnel(performance bias)
Blinding of outcome assessment(detection bias)
Incompleteoutcome data(attrition bias)
Boulloche
et al. (10)
(+)
Random number
table
(?)
Not described
(?)
Not described. Only mentioned
that the study was double blind.
(?)
Not described.
(+)
61/72
(85%)
Li�evin-Le
Moal et al. (12)
(�)
Sequential
allocation.
No details.
(+)
The sachets were
numerically coded.
Sequential
allocation.
(+)
Identical placebo
(?)
Not described.
(+)
100%
Salazar-Lindo
et al. (13)
(?)
Not described
(?)
Probably sequential
(+)
Double blind. Study codes were
broken only after completion of the
blind review.
(+)
Study codes were broken
only after completion of the
blind review.
(+)
77/80
(96%)
Simakachorn
et al. (14)
(+)
Randomisation
code
(+)
Numerically coded
package
(+)
Identical placebo
(?)
Not described.
(+)
100%
(+) indicates a low risk of bias; (�) indicates a high risk of bias; (?) indicates unclear risk of bias.
Figure 1 Lactobacillus acidophilus LB versus placebo. Duration of diarrhoea (hours).
Figure 2 Lactobacillus acidophilus LB versus placebo. Cure on day 3.
L. acidophilus LB and acute gastroenteritis Szajewska et al.
(10,12,14), all carried out in hospitalised children, revealed asignificant reduction in the duration of diarrhoea of�21.6 hfor those treated with LB compared with placebo (MD�21.6 h, 95% CI �26.5 to �16.6, in the fixed effects model).No significant heterogeneity was found (I2 = 24%; Fig. 1).
Data from one trial that presented only the median, withthe inter quartile range (IQR), were not included in themeta-analysis. This RCT conducted in 80 outpatientsshowed no reduction in the duration of diarrhoea for thosetreated with L. acidophilus LB compared with placebo(median: 10.0 h, IQR 6.0–56.7 versus 16.6 h, IQR 7.1–50.3,respectively; p = 0.275) (13).
Cure on day 3This outcome was calculated from two RCTs including 144children (10,14). The chance of cure on day three wassimilar in both groups (RR 1.03, 95% CI 0.88 to 1.2). Nosignificant heterogeneity was found (I2 = 0%; Fig. 2).
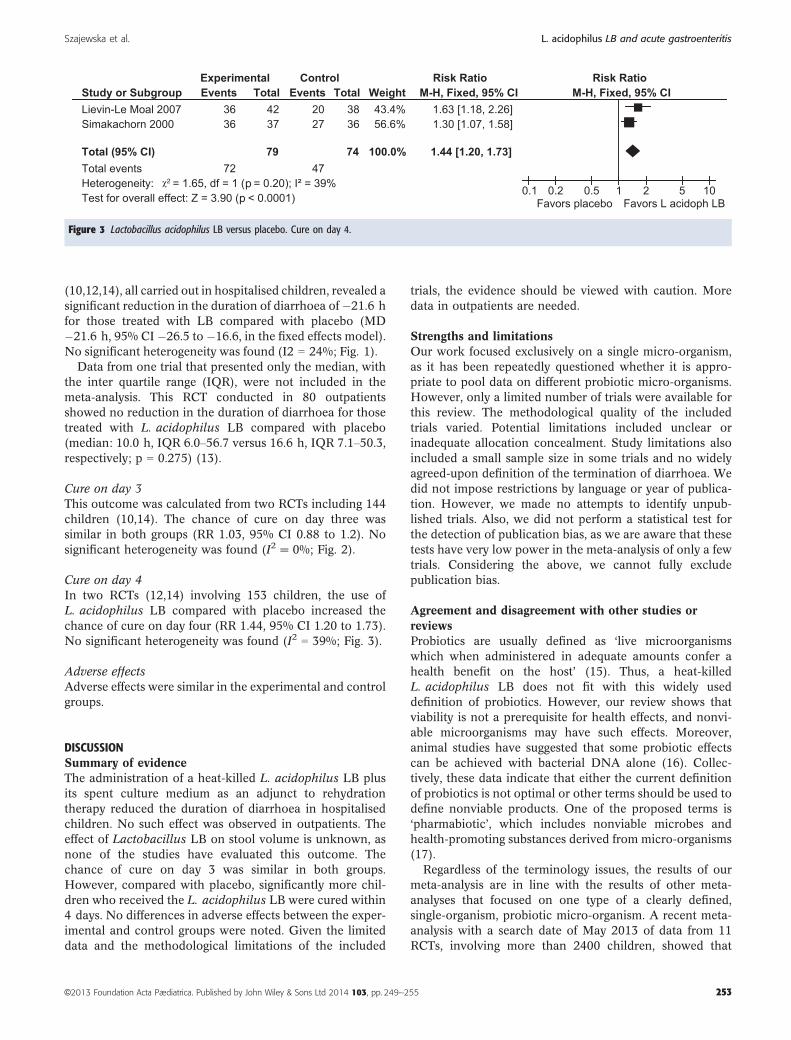
Cure on day 4In two RCTs (12,14) involving 153 children, the use ofL. acidophilus LB compared with placebo increased thechance of cure on day four (RR 1.44, 95% CI 1.20 to 1.73).No significant heterogeneity was found (I2 = 39%; Fig. 3).
Adverse effectsAdverse effects were similar in the experimental and controlgroups.
DISCUSSIONSummary of evidenceThe administration of a heat-killed L. acidophilus LB plusits spent culture medium as an adjunct to rehydrationtherapy reduced the duration of diarrhoea in hospitalisedchildren. No such effect was observed in outpatients. Theeffect of Lactobacillus LB on stool volume is unknown, asnone of the studies have evaluated this outcome. Thechance of cure on day 3 was similar in both groups.However, compared with placebo, significantly more chil-dren who received the L. acidophilus LB were cured within4 days. No differences in adverse effects between the exper-imental and control groups were noted. Given the limiteddata and the methodological limitations of the included
trials, the evidence should be viewed with caution. Moredata in outpatients are needed.
Strengths and limitationsOur work focused exclusively on a single micro-organism,as it has been repeatedly questioned whether it is appro-priate to pool data on different probiotic micro-organisms.However, only a limited number of trials were available forthis review. The methodological quality of the includedtrials varied. Potential limitations included unclear orinadequate allocation concealment. Study limitations alsoincluded a small sample size in some trials and no widelyagreed-upon definition of the termination of diarrhoea. Wedid not impose restrictions by language or year of publica-tion. However, we made no attempts to identify unpub-lished trials. Also, we did not perform a statistical test forthe detection of publication bias, as we are aware that thesetests have very low power in the meta-analysis of only a fewtrials. Considering the above, we cannot fully excludepublication bias.
Agreement and disagreement with other studies orreviewsProbiotics are usually defined as ‘live microorganismswhich when administered in adequate amounts confer ahealth benefit on the host’ (15). Thus, a heat-killedL. acidophilus LB does not fit with this widely useddefinition of probiotics. However, our review shows thatviability is not a prerequisite for health effects, and nonvi-able microorganisms may have such effects. Moreover,animal studies have suggested that some probiotic effectscan be achieved with bacterial DNA alone (16). Collec-tively, these data indicate that either the current definitionof probiotics is not optimal or other terms should be used todefine nonviable products. One of the proposed terms is‘pharmabiotic’, which includes nonviable microbes andhealth-promoting substances derived from micro-organisms(17).
Regardless of the terminology issues, the results of ourmeta-analysis are in line with the results of other meta-analyses that focused on one type of a clearly defined,single-organism, probiotic micro-organism. A recent meta-analysis with a search date of May 2013 of data from 11RCTs, involving more than 2400 children, showed that
Figure 3 Lactobacillus acidophilus LB versus placebo. Cure on day 4.
Szajewska et al. L. acidophilus LB and acute gastroenteritis
Lactobacillus GG compared with placebo or no treatmentreduced the duration of diarrhoea by approximately 1 day(MD �1.05 day, 95% CI �1.7 to �0.4) (18). Another meta-analysis showed that compared with the placebo or nointervention group, the use of S. boulardii significantlyreduced the duration of diarrhoea, again, by approximately1 day and the risk of diarrhoea on day 3 by 48% (19).More commonly, all probiotics are pooled together. Forexample, a Cochrane review showed that probiotics as aclass of agents reduced the duration of diarrhoea byaround 25 h and the risk of diarrhoea lasting four or moredays by 59% (20). On the whole, the data show that areduction in the duration of AGE by 1 day with use ofprobiotics is likely.
CONCLUSIONS AND FUTURE RESEARCHThis systematic review and meta-analysis of RCTs documentthat the use of L. acidophilus LB compared with placeboreduces the duration of diarrhoea associated with AGE inhospitalised children. However, given the small number oftrials and participants and the methodological limitations ofthe included trials, the evidence should be viewed withcaution. Data on the effect on stool output, as well as moredata in outpatients, are needed. The role of probiotics,including L. acidophilus LB, in the treatment of AGE in theera of rotavirus vaccination has yet to be established.However, in some countries, such as the United States,norovirus has emerged as the leading cause of medicallyattended AGE (21). If so, the efficacy of probiotics in treatingnorovirus AGE needs to be confirmed. Country-specificstudies to examine the cost-effectiveness of usingL. acidophilus LB for the treatment of AGE are also needed.
ACKNOWLEDGEMENTSThis study was funded in full by The Medical University ofWarsaw.
COMPETING INTERESTSAuthors declare no conflict of interest with regard to thismanuscript.
References
1. Guarino A, Albano F, Ashkenazi S, Gendrel D, Hoekstra JH,Shamir R, et al. The ESPGHAN/ESPID evidenced-basedguidelines for the management of acute gastroenteritis inchildren in Europe. J Pediatr Gastroenterol Nutr 2008; 46(Suppl. 2): S81–122.
2. National Collaborating Centre for Women’s and Children’sHealth. Diarrhoea and vomiting diagnosis, assessment andmanagement in children younger than 5 years. Available at:http://www.nice.org.uk/nicemedia/pdf/CG84FullGuideline.pdf. (accessed on September 1, 2012).
3. Caleb KK, Glass R, Brese JS, Duggan C. Managing acutegastroenteritis among children oral rehydration, maintenance,and nutritional therapy. MMWR Recomm Rep 2003; 52: 1–16.
4. Coconnier M-H, Bernet MF, Kern�eis S, Chauvi�ere G, FourniatJ, Servin AL. Inhibition of adhesion of enteroinvasivepathogens to human intestinal Caco-2 cells by Lactobacillusacidophilus LB strain decreases bacterial invasion. FEMSMicrobiol Lett 1993; 110: 299–306.
5. Chauvi�ere G, Coconnier MH, Kern�eis S, Fourniat J, Servin AL.Adhesion of human Lactobacillus acidophilus strain LB tohuman enterocyte-like Caco-2 cells. J Gen Microbiol 1992; 138:1689–96.
7. Coconnier-Polter MH, Lievin-Le Moal V, Servin AL. ALactobacillus acidophilus strain of human gastrointestinalmicrobiota origin elicits killing of enterovirulent Salmonellaenterica serovar Typhimurium by triggering lethal bacterialmembrane damage. Appl Environ Microbiol 2005; 71:6115–20.
8. L�evin-Le Moal V, Amsellem R, Servin AL, Coconnier MH.Lactobacillus acidophilus (strain LB) from the resident adulthuman gastrointestinal microflora exerts activity against brushborder damage promoted by a diarrhoeagenic Escherichia coliin human enterocyte-like cells. Gut 2002; 50: 803–11.
9. Higgins JPT, Green S (editors). Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0 [updatedMarch 2011]. The Cochrane Collaboration, 2011. Availableat www.cochrane-handbook.org. (accessed on August 1,2013).
10. Boulloche J, Mouterde O, Mallet E. Management of acutediarrhea in infants and toddlers. Controlled study of theantidiarrheal efficacy of killed Lactobacillus acidophilus (LBstrain) versus a placebo and a reference agent (loperamide).Ann Pediatr (Paris) 1994; 41: 457–63. In French.
11. Egger M, Smith GD, Schneider M, Minder C. Bias inmeta-analysis detected by a simple, graphical test. BMJ 1997;315: 629–34.
12. Li�evin-Le Moal V, Sarrazin-Davila LE, Servin AL. Anexperimental study and a randomized, double-blind,placebo-controlled clinical trial to evaluate the antisecretoryactivity of Lactobacillus acidophilus strain LB againstnonrotavirus diarrhea. Pediatrics 2007; 120: e795–803.
13. Salazar-Lindo E, Figueroa-Quintanilla D, Caciano MI,Reto-Valiente V, Chauviere G, Colin P; Lacteol Study Group.Effectiveness and safety of Lactobacillus LB in the treatment ofmild acute diarrhea in children. J Pediatr Gastroenterol Nutr2007; 44: 571–6.
14. Simakachorn N, Pichaipat V, Rithipornpaisarn P, KongkaewC, Tongpradit P, Varavithya W. Clinical evaluation of theaddition of lyophilized, heat-killed Lactobacillus acidophilusLB to oral rehydration therapy in the treatment of acutediarrhea in children. J Pediatr Gastroenterol Nutr 2000; 30:68–72. Erratum in: J Pediatr Gastroenterol Nutr 2000; 30:228.
15. Food and Agriculture Organization of the United Nations(FAO). Health and Nutritional Properties of Probiotics in Foodincluding Powder Milk with Live Lactic Acid Bacteria. 2001.Available at: http://www.who.int/foodsafety/publications/fs_management/en/probiotics.pdf. (accessed on July 30, 2013).
16. Rachmilewitz D, Karmeli F, Takabayashi K, Hayashi T,Leider-Trejo L, Lee J, et al. Immunostimulatory DNAameliorates experimental and spontaneous murine colitis.Gastroenterology 2002; 122: 1428–41.
17. Shanahan F, Collins SM. Pharmabiotic manipulation of themicrobiota in gastrointestinal disorders, from rationale toreality. Gastroenterol Clin North Am 2010; 39: 721–6.
L. acidophilus LB and acute gastroenteritis Szajewska et al.
18. Szajewska H, Sk�orka A, Ruszczy�nski M, Gieruszczak-BiałekD. Meta-analysis: Lactobacillus GG for treating acutegastroenteritis in children – updated analysis ofrandomised controlled trials. Aliment Pharmacol Ther 2013;38: 467–76.
19. Dinleyici EC, Eren M, Ozen M, Yargic ZA, Vandenplas Y.Effectiveness and safety of Saccharomyces boulardii foracute infectious diarrhea. Expert Opin Biol Ther 2012; 12:395–410.
21. Payne DC, Vinj�e J, Szilagyi PG, Edwards KM, Staat MA,Weinberg GA, et al. Norovirus and medically attendedgastroenteritis in U.S. children. N Engl J Med 2013; 368:1121–30.
SUPPORTING INFORMATIONAdditional Supporting Information may be found in theonline version of this article:
Figure S1 Flow diagram.Table S1 Characteristics of excluded trials.