40
Metacarpal Fractures
| Date post: | 14-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | w-thomas-mcclellan-md-facs |
| View: | 420 times |
| Download: | 0 times |

Metacarpal Fractures
Fractures of the Metacarpal
• The most common fracture of the upper extremity
• Involved in 80% of hand Fx
• Incidence peaks between ages 10-40 – Greatest industrial and athletic exposure
• Outer fingers are most frequently injured

Complexity of Functional Anatomy
“hand fractures can be complicated by deformity from no treatment, stiffness from over treatment, and both deformity and stiffness from poor treatment”. !
(Swanson 1970)

!
What is the correct treatment ?
Goal
Full and rapid restoration of function

Fracture treatment should be principle driven
• Anatomic or functionally acceptable reduction !
• Stability !
• Minimizing additional soft tissue trauma !
• Adequate pain control !
• Early functional rehabilitation

Balance
!Injury severity
!Pt. demographics
Joint & tendon motion
Fracture healing
Speed of recovery Safety
BiologyBiomechanics
Stability Implant selection
Blood Supply Surgical dissectionScar tissue

Diagnosis - Hx
• Patient’s age • Past medical history • Dominant hand • Occupational status • Cause and circumstances • Other injuries

Diagnosis
• Area of maximum tenderness • Deformities : location, type ,severity • Soft tissue injuries • Neurovascular status • Tendon injury

Outcome Determinants
• Patient factors • Fracture Factors • Wound Factors • Management factors

Outcome Determinants
• Patient factors – Age ( > 50 ) – Associated disease and arthritis – Socioeconomic status – Motivation and compliance
• Fracture Factors • Wound Factors • Management factors

Outcome Determinants
• Patient factors • Fracture Factors
– Location: intra-articular, flexor tendon Zone 2 – Type : simple, comminuted, impacted, bone loss – Geometry: transverse, oblique, spiral, avulsion – Deformity: angulation, rotation, shortening – Stability
• Wound Factors • Management factors

Outcome Determinants
• Patient factors • Fracture Factors • Wound Factors
– Open Vs. Closed – Associated injuries: tendon, soft tissue, neurovasc. – contamination
• Management factors

Outcome Determinants
• Patient factors • Fracture Factors • Wound Factors • Management factors
– Diagnosis and recognition – Reduction and maintenance – Length of immobilization – Complication management
Freeland’s principles
• Anatomic or functionally acceptable reduction • Stability • Avoiding or minimizing additional soft tissue
trauma • Adequate pain control • Early functional rehabilitation

Open?
Displaced ?
Reducible ? Stable ?
BracingORIF or Ex-Fix
N
Y NY
YN
N
Y
CRIF
Protected motion / Immobilization Rehabilitation
Hand fracture
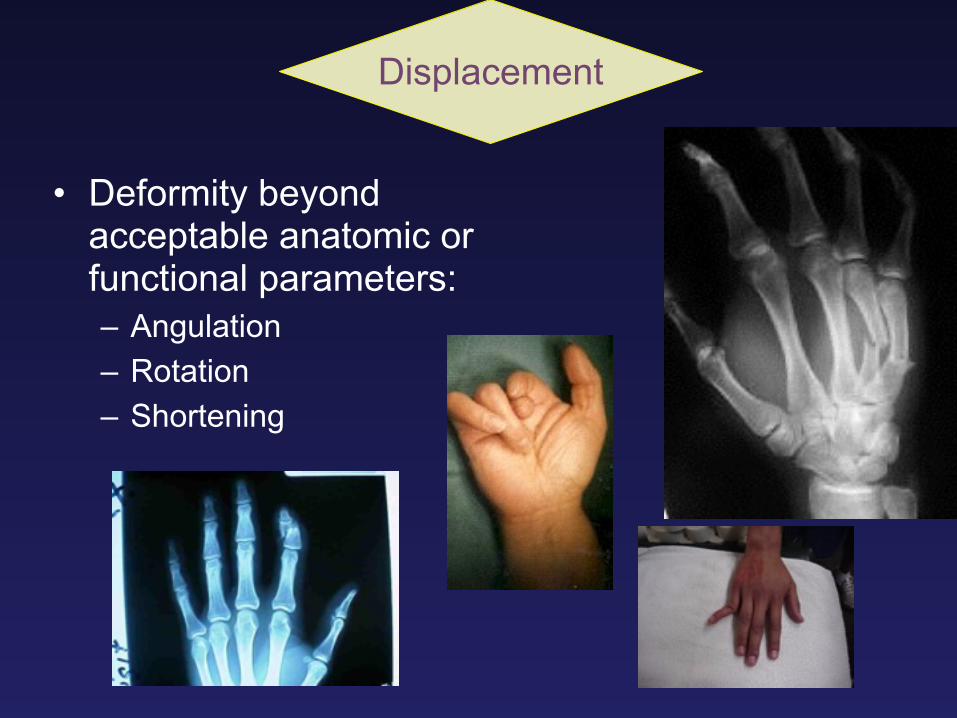
• Deformity beyond acceptable anatomic or functional parameters: – Angulation – Rotation – Shortening
Displacement

“Acceptable” ?Variance in Compensation & accommodation
• The CMC joints of the ring and small finger have 20°-30° mobility in the sagital plain. !
• The CMC joints of the Index and long finger have less mobility. !
• Therefore, in Fractures of the metacarpal necks, angulation can be better compensated for in the ring and small fingers, without compromising hand function.
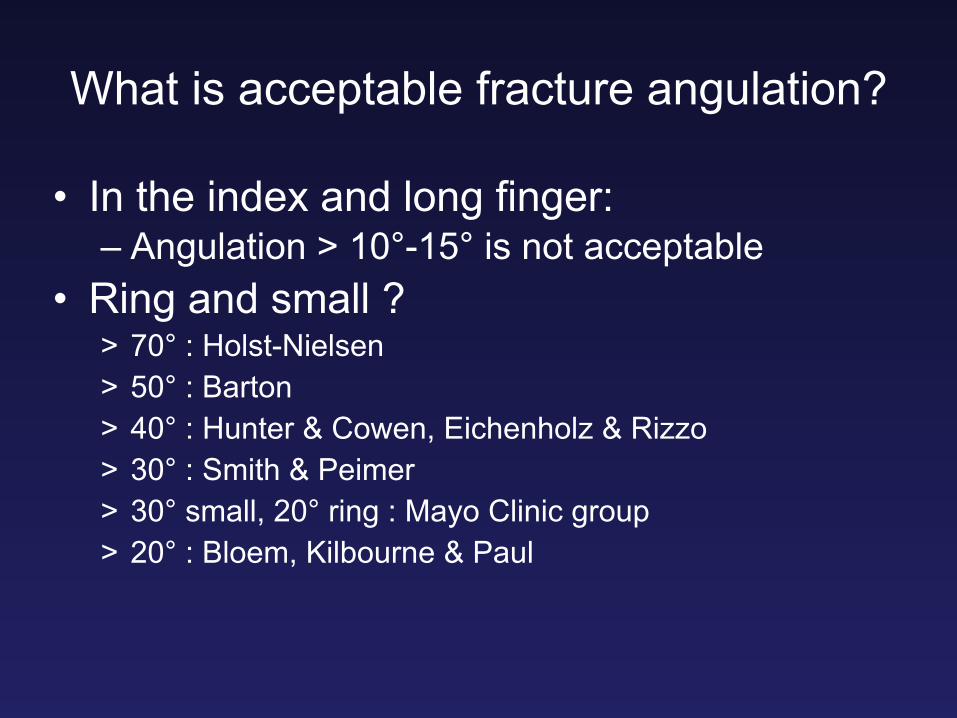
What is acceptable fracture angulation?
• In the index and long finger: – Angulation > 10°-15° is not acceptable
• Ring and small ? > 70° : Holst-Nielsen > 50° : Barton > 40° : Hunter & Cowen, Eichenholz & Rizzo > 30° : Smith & Peimer > 30° small, 20° ring : Mayo Clinic group > 20° : Bloem, Kilbourne & Paul

Displacement
Deformity beyond acceptable anatomic or functional parameters.
Stable fracture: Can be maintained in an anatomic or near anatomic position.
Stability

• Stability determinants – Fracture configuration – Muscle balance – Integrity of periosteum – Integrity of soft tissue – External forces – Integrity of supporting skeletal structures
Stability

Unstable fracture configuration
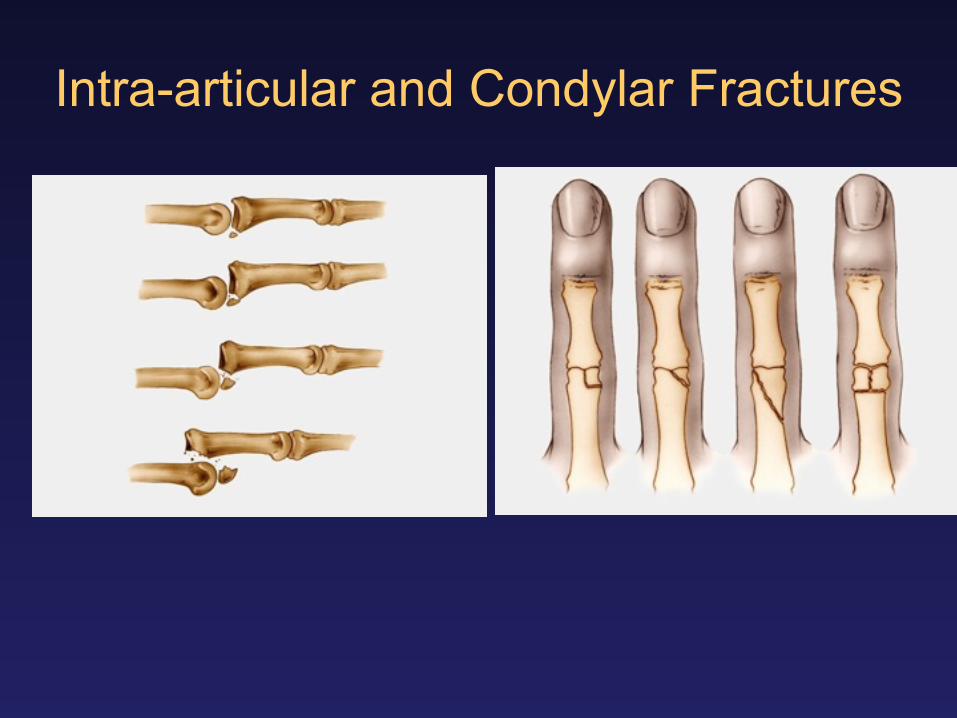
Intra-articular and Condylar Fractures

Muscle balance Fracture of the metacarpals
• Under the joint traction of the interosseous muscles and the flexor tendons, the distal fragment of the metacarpal flexes, producing a dorsal angulation.

Reduction & fixationBuddy taping of a fractured finger
• Stabilizing with an intact neighboring finger is the best dynamic splint that ensures a rapid functional result.

Functional bracing
• Splinting the wrist in dorsiflexion and the metacarpophalangeal joints at 90°. !
• The hand is free from the splint in the distal area to allow motion.

Closed reduction and percutaneous pinning with K-wire of a mid-shaft fracture
• Started by the reduction and alignment of the skeleton
• Two oblique K-wires are inserted
• Compression of the bone fragments should be maintained to avoid diastasis.

Jahss manipulation technique and fascicular pinning
• Finger flexion to 90° and force application to the axis of the proximal phalanx for fracture reduction.
• Three K-wires are inserted through a hole made on the lateral side in the proximity of the metacarpal.

Transversal pinning to adjacent metacarpal
!• Transfixation to
adjacent metacarpal !
• Bone loss
ORIF
• Accurate anatomic reduction • Stable fixation
– Pain control – Early mobilization
• Functional recovery

ORIF-cons
• Devascularization of bone fragments • Soft tissue damage • Tendon adherence • Scar formation • Infection • Implant removal - 2° procedure

Open incisions
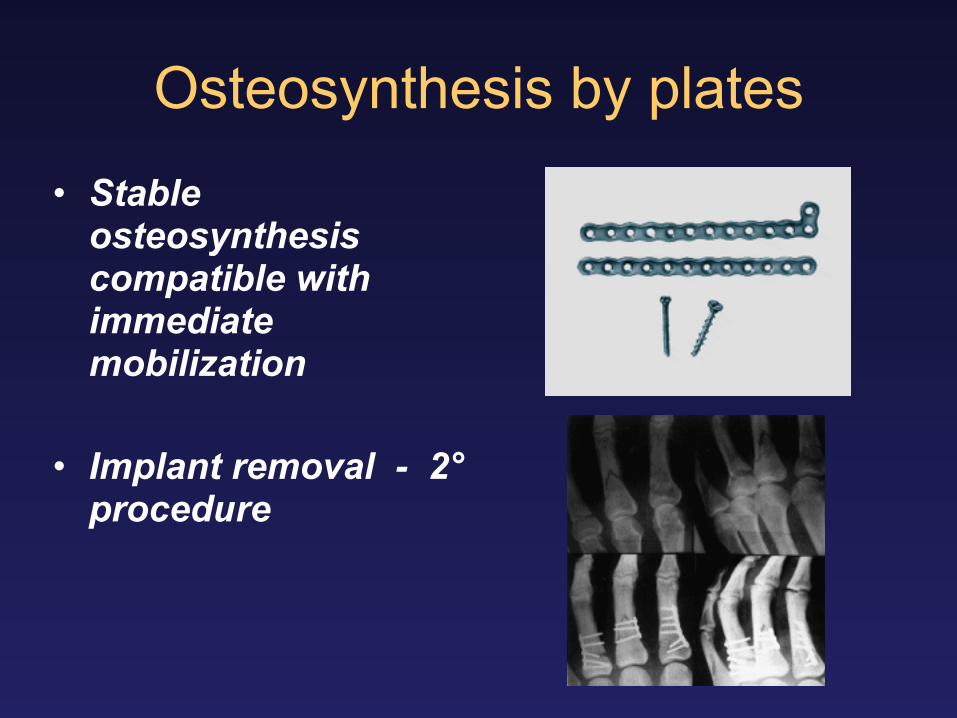
Osteosynthesis by plates
• Stable osteosynthesis compatible with immediate mobilization !
• Implant removal - 2° procedure

osteosynthesis with cortical and cancellous screws



external fixator !
• Comminuted • Small fragments • allows the
preservation of length • allows mobility and
approach to soft tissue injuries.
• Ligamentotaxis

Balance
!Injury severity
!Pt. demographics
Joint & tendon motion
Fracture healing
Speed of recovery Safety
BiologyBiomechanics
Stability Implant selection
Blood Supply Surgical dissectionScar tissue

Complications
• Failure of bone healing – Delayed union, Nonunion, Pseudoarthrosis
• Union with deformity - Malunion • Tendon adhesions • Joint contractures • Post traumatic arthritis • Infection • Implant failure

















