Hospital Acquired Pressure Injuries (HAPI): Getting to the bottom of the problem in the Sydney Local Health District Michelle Barakat-Johnson Dr Catherine Barnett A/Professor Timothy Wand Professor Kate White A collaboration between the SLHD, CNRU and University of Sydney. Disclaimer: Patient permission was obtained for the collection and use of all images in this presentation.
Transcript
Hospital Acquired Pressure Injuries (HAPI): Getting to the bottom of the problem in the
Sydney Local Health District Michelle Barakat-Johnson
Dr Catherine Barnett
A/Professor Timothy Wand
Professor Kate White
A collaboration between the SLHD, CNRU and University of Sydney.
Disclaimer: Patient permission was obtained for the collection and use of all images in this presentation.
The State of Play in 2016
• Pressure Injury research - decades of research
• $ and Strategic Investment into Pressure Injury Research
• $ and Strategic Investment into Pressure Injury Prevention
• Evidence Based Guidelines - Local, National and International
However……..
• Hospital Acquired Pressure Injuries (HAPI) continue to cost the Australian health system up to $ 1billion per annum (Nguyen, Chaboyer, Whitty,
2015)
• Impact an estimated 2.5 million individuals per annum in the US (Agency for
Health Care and Quality Research, 2014)
Prevalence and Incidence of HAPI
• International Prevalence - 0% to 72 % (Paediatric highest)
• National Prevalence - 2.5% to 17.6% (CEC 2016)
• International Incidence – 0% to 59% (Aged care highest)
• US – Over 2.5 million people
• UK – Over 700,000 people (NICE guidelines)
• Australia – Over 100,000 people per year
$ Cost of Pressure Injuries
• Financial Cost – annual • United Kingdom – £ 2.1 billion (Bennett et al.,2004)
• United States – $ US 11.6 Billion (Agency for Healthcare Research and Quality, 2012)
• Australia- $ Aus 983 million (Nguyen et al., 2013)
• Treatment costs: $1082.37 per ulcer (Santamaria & Santamaria, 2014); UK
£1,214 (Stage 1) to £14,108 (Stage IV) (Dealey et al., 2012)
$ Cost of Pressure Injuries
• Cost to the patient (Gorecki et al., 2009)
• Pain and increased suffering
• Prolonged hospital
• Complication
• Premature Death
• Psychological - Social Impact
“ All anyone does is look at my bottom all the time?”
• Impact on general health
• Not often observed by healthcare
Other costs?
Evidence for who is at risk of HAPI?
• Patients at risk of HAPI-
• Three primary risk factors - Mobility/Activity, Perfusion and
oxygenation, Skin Status (Coleman et al., 2015)
• Other risk factors – Skin moisture, haematological factors, nutrition, general health
Is there evidence for HAPI prevention?
• Guidelines for best practice
• Level 2 evidence – Skin Assessment, repositioning, skin clean and dry, continence care, nutritional assessment, off loading heels, support surface - seating and bed, medical device fitting
• Level 3 evidence- prophylactic dressings, microclimate control (NPUAP, EPUAP, Pan Pacific Guidelines, 2014)
Emerging Evidence: HAPI Prevention & Management
• PI Prevention Bundles • Care bundle INTACT
• SSKIN bundle - consistent practice
• Royal Melbourne Hospital Clinical innovation - 6.6% to 2.5% in 2 years
• Prince Charles Hospital –Initiatives decreasing prevalence from 13.3% 2002 to 4% 2012
• United States - Padula et al QA interventions Bundle to decrease HAPU - reduction in early adoption of interventions
• PI Prevention Programs • AHRQ toolkit to assess cost saving in preventing HAPU - $127 per patient
• KPMG - Quality programme to reduce pressure injuries in New Zealand – aim for an overall 70% reduction - 15% per annum
What are care related risk factors?
• Care delivery factors? • Nurse knowledge • Staff to patient ratio • Environment - Single room • Access to equipment • Culture • Priority
• Risk to Organisation or Health Care Service? • Financial Penalties • Increase in length of stay • Cost of treating pressure injuries
Increase of HAPI in SLHD 2010-2014
544
656
736
820
887
0
100
200
300
400
500
600
700
800
900
1000
Year 2010 Year 2011 Year 2012 Year 2013 Year 2014
SLHD increase in HAPI 2010-2014
District Health Response
• Establish new role: District Lead in Pressure Injury Prevention and Management
• Area Wide Taskforce Chaired by District DON
• Taskforce included Director of Nursing, Senior Clinical Nurse Consultant and Nursing Unit Manager with a special interest in wound care, Occupational Therapy
Suggested Reasons for Increase in HAPI
• Lack of nursing knowledge
• Poor quality nursing care
• Failure for nurses to adhere to clinical guidelines
• Clinical nurses not utilising pressure are prevention equipment
• Increased acuity of patients
Strategy
Area Wide Pressure Injury Task Force Bigger Questions
• Proposed 3-6 months duration
• Presumed knowledge of reasons
• Identification of knowledge gaps
• Area wide nurse education
• Instigation of additional documentation (turn charts)
• Mandate
• Expectations and timelines
• Evidence that these were the underlying cause(s)
• Evidence interventions will address the issues
Research: Beginning Aim
• Aim
To investigate the relationship between HAPI, nursing practice, nurse, patient and carer knowledge, reporting systems and documentation and contribute to knowledge and practice aimed at reducing the incidence of HAPI.
• Setting:
District Health Service in Central Sydney comprising
• Two Tertiary Referral Hospitals
• One Rehabilitation Hospital
• One District Hospital
Why?
• Examine or investigate
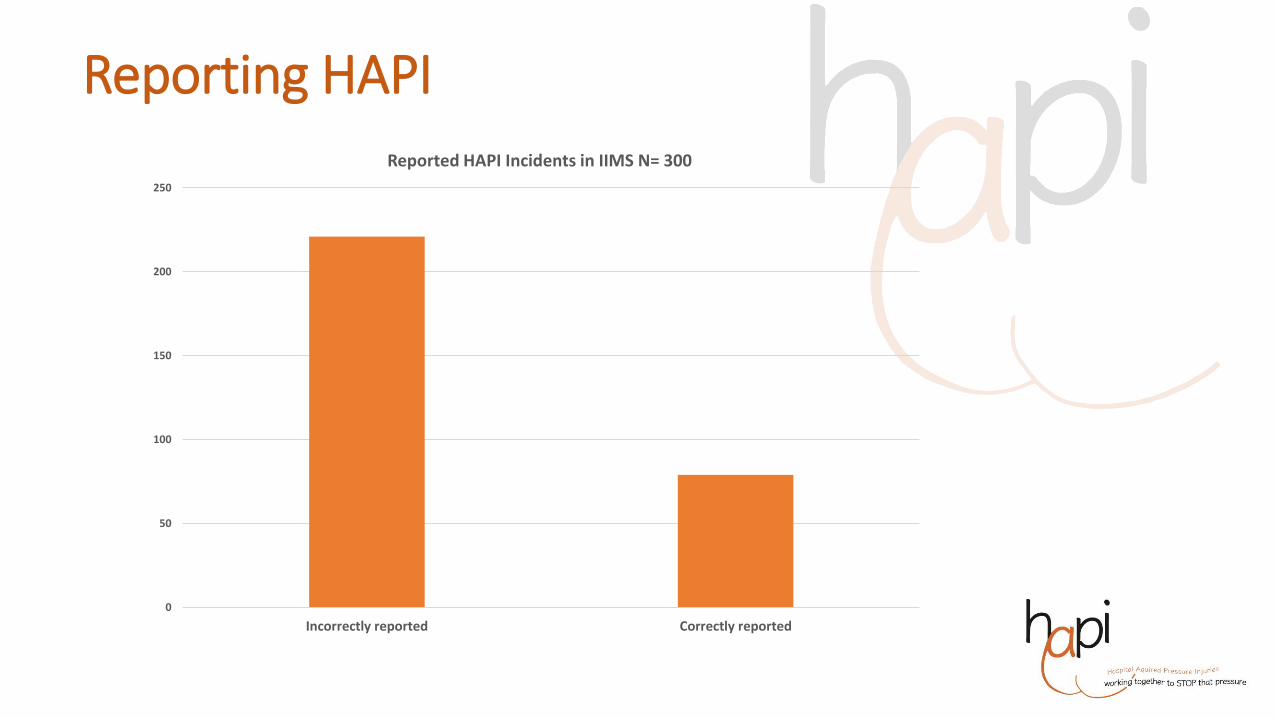
• What is being reported?
Reporting HAPI
0
50
100
150
200
250
Incorrectly reported Correctly reported
Reported HAPI Incidents in IIMS N= 300
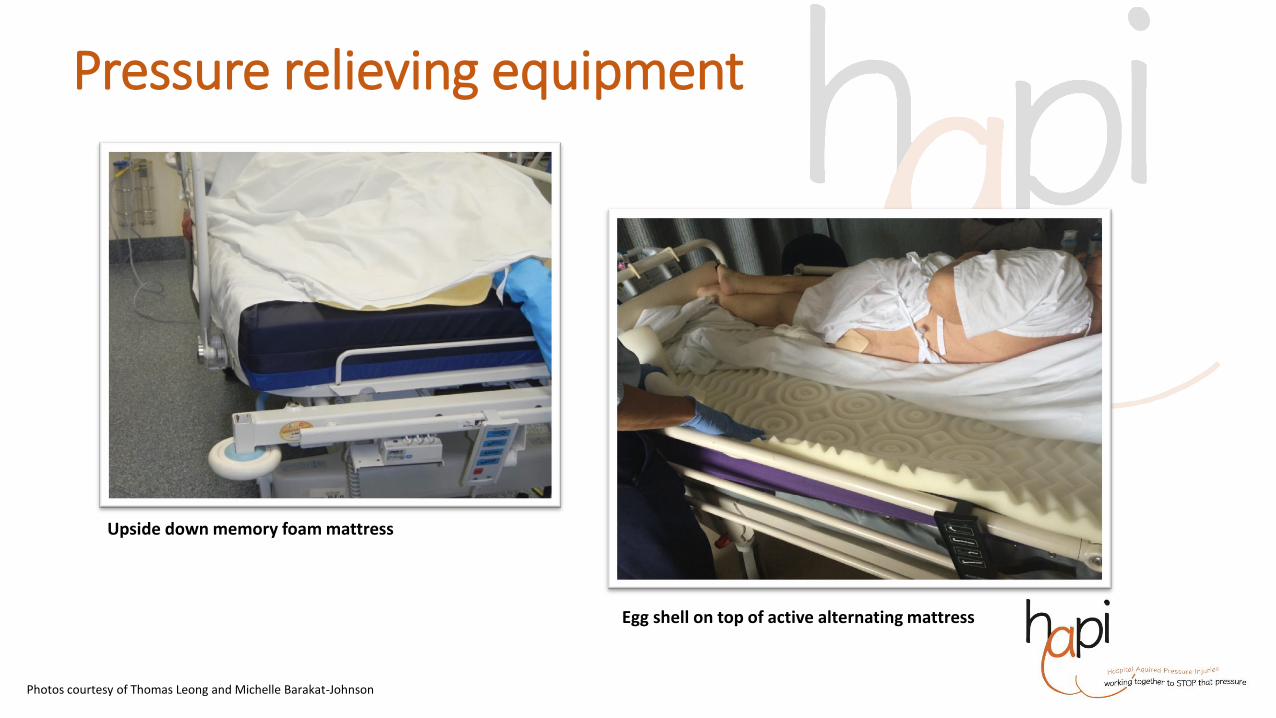
Photos: courtesy of Thomas Leong
Inaccurate Staging: Consequence
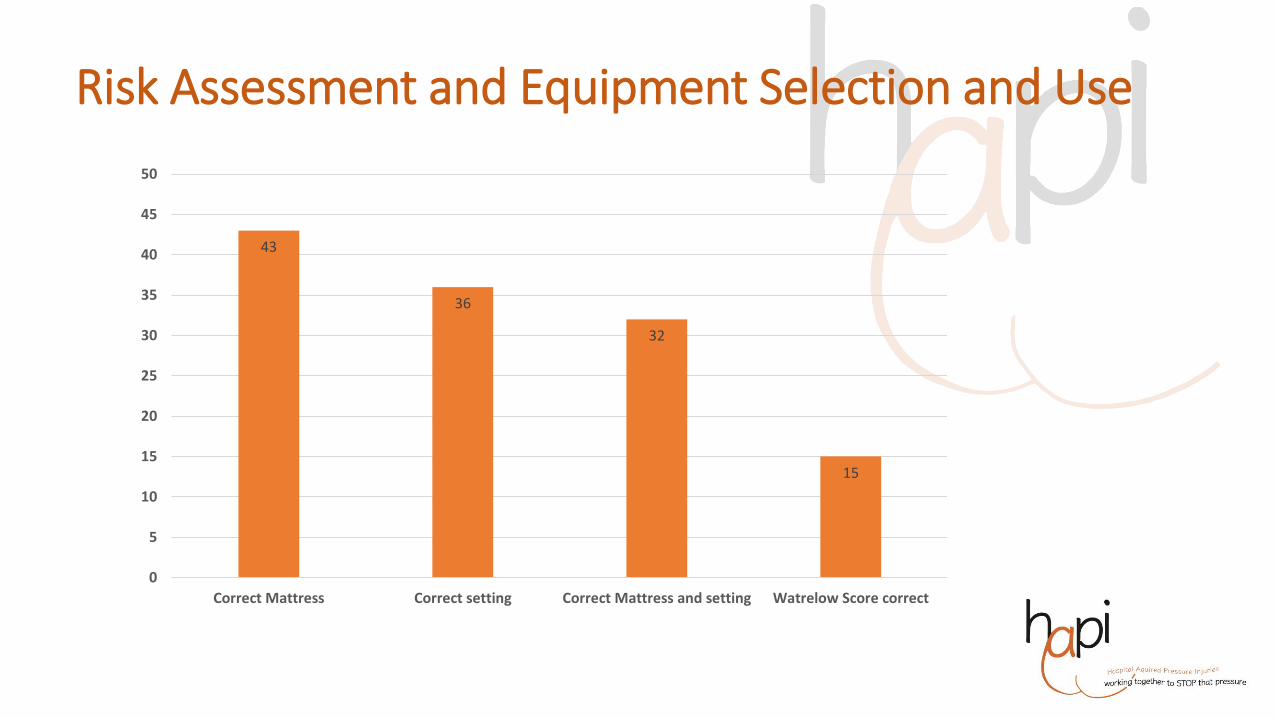
Equipment Audit
• Shortage of essential equipment; specifically pillows and bed cradles to assist with positioning.
• Equipment not in good condition
• This included incorrect use of equipment - heel life devices, active mattresses unplugged or inaccurate setting. Of note 30 of the new memory foam mattresses were incorrectly placed (upside down).
• A number of staff reported a lack of education on how to set and monitor the active mattress being used in their clinical setting.
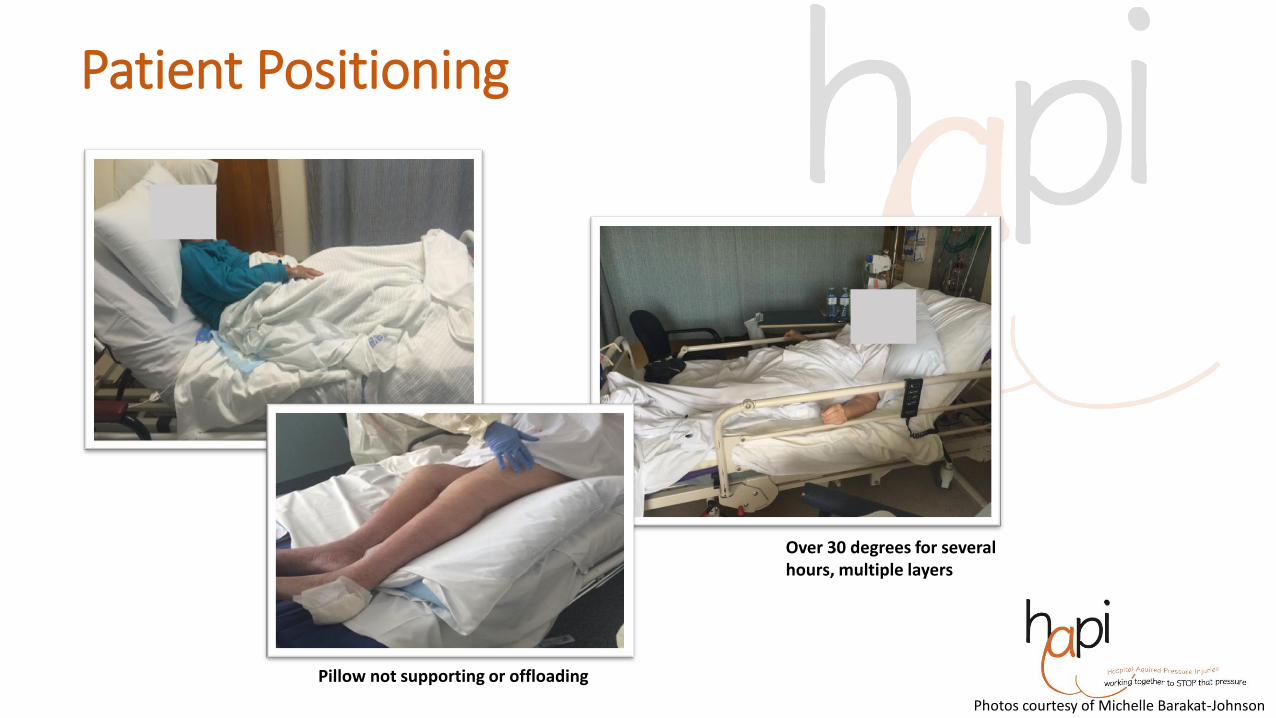
• Poor practices - multiple layers, double pads, antiseptic hand wash, use of zinc
• Nurse not aware, don’t know what it is
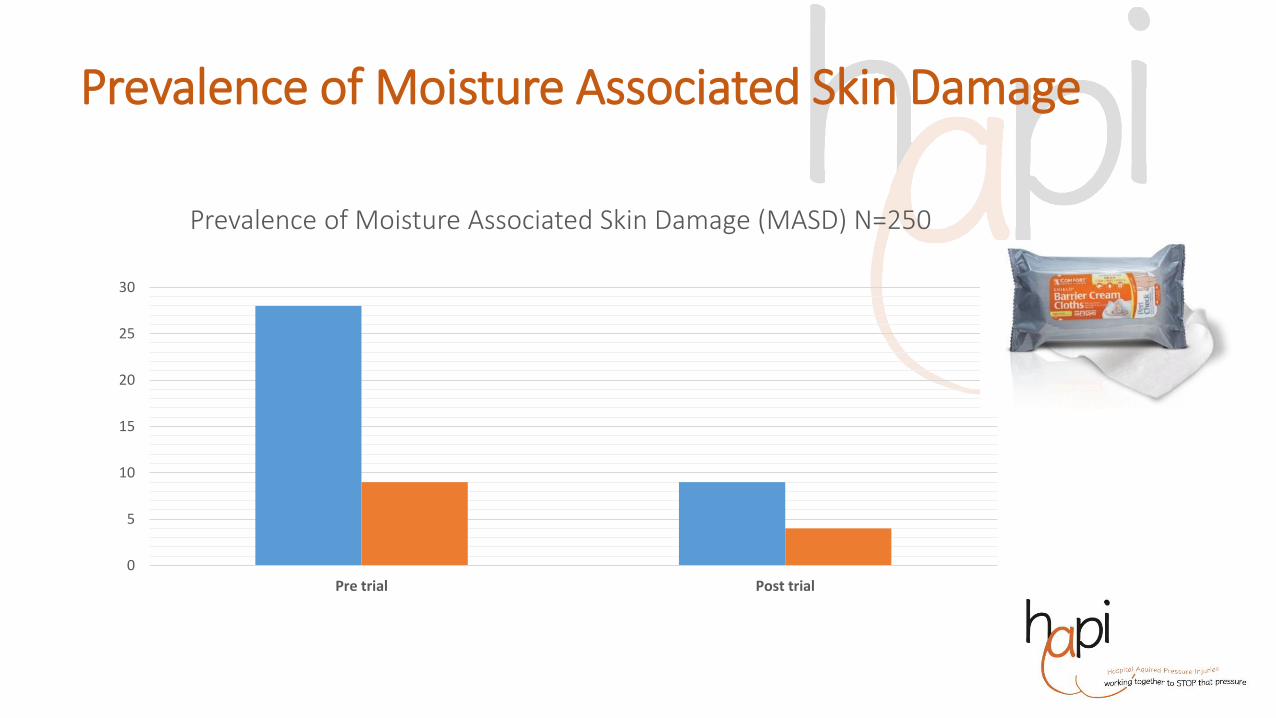
Prevalence of Moisture Associated Skin Damage
0
5
10
15
20
25
30
Pre trial Post trial
Prevalence of Moisture Associated Skin Damage (MASD) N=250
Medical Record Audit
• Twenty five (25) medical records were audited
• Prevention Plan
• Skin assessment
• Five (5) had prevention plans
• One (1) had skin assessment documented on admission
Nursing Knowledge Survey
Nursing Attitude Survey
Interim conclusions
• Complexity
• Revised research question:
How does an organisation effectively implement a strategy to reduce HAPI?
Acknowledgements
• Sydney Research - Grant
• Sydney Local Health District Executive Directors and Taskforce
• Key Stakeholders – Cassandra Chan, Thomas Leong, Megan White, Karen Sherwood, John Sheehy
• University of Sydney – Research Team and Statistician
• A big thank you to all the Patients and Nurse Participants involved in this study
References • Agency for Healthcare Research and Quality. Are we ready for this change?. Content last reviewed October 2014. Agency for Healthcare Research and Quality,
• Bennett G., Dealey. C. and Posnett, J. ( 2004). The cost of pressure ulcers in the UK. Age and Ageing; 33: 230–235
• Chaboyer, W., & Gillespie, B. M. (2014). Understanding nurses' views on a pressure ulcer prevention care bundle: a first step towards successful implementation. Journal of clinical nursing, 23(23-24), 3415-3423.
• Coleman et al. (2013). Patient risk factors for pressure ulcer development: systematic review. International Journal of Nursing Studies; 50,7, 974-1003.
• Gillespie, B. M., Chaboyer, W., Sykes, M., O'Brien, J., & Brandis, S. (2014). Development and pilot testing of a patient-participatory pressure ulcer prevention care bundle. Journal of nursing care quality, 29(1), 74-82.
• KMG. (2015). The case for investment in: A Quality Improvement Programme to Reduce Pressure Injuries in New Zealand. Kpmg.com.nz
• Miles, S., Fulbrook, P., Nowicki, T., & Franks, C. (2013). Decreasing pressure injury prevalence in an Australian general hospital: A 10-year review.
• National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Emily Haesler (Ed.). Cambridge Media: Osborne Park, Australia; 2014.
• Padula, W. V., Makic, M. B. F., Mishra, M. K., Campbell, J. D., Nair, K. V., Wald, H. L., & Valuck, R. J. (2015). Comparative effectiveness of quality improvement interventions for pressure ulcer prevention in academic medical centers in the United States. The Joint Commission Journal on Quality and Patient Safety, 41(6), 246-246.
• Pressure injury in Australian public hospitals: a cost-of-illness study. Nguyen K-H, Chaboyer W, Whitty JA. Australian Health Review, 2015. Clinical Excellence Commission, 2014, Clinical Excellence Commission Pressure Injury Prevention Project Monitoring and Auditing Framework, Sydney: Clinical Excellence Commission. Australian Commission on Safety and Quality in Health Care, National Safety and Quality Health Service Standards (September 2012). Sydney.
• Santamaria et al. (2015). Clinical innovation results from a five-year pressure ulcer prevention project in an Australian university hospital. Wound Internatiomal, 6 (3), 12-16.
• Spetz, J., Brown, D. S., Aydin, C., & Donaldson, N. (2013). The value of reducing hospital-acquired pressure ulcer prevalence: an illustrative analysis. Journal of Nursing Administration, 43(4), 235-241.